Embed Size (px)
Citation preview

CKD and atrial fibrillation: warfarin, NOAC or nothing?
CHRONIC KIDNEY DISEASE (CKD) IN THE PATIENT WITH ATRIAL FIBRILLATION
Tatjana S. Potpara, MD, PhD, FESC Assist. Prof. in Cardiology, School of Medicine, Belgrade University; Head of the Department for arrhythmia intensive care, Cardiology Clinic, Clinical Centre of Serbia, Belgrade, Serbia; President of the Serbian Atrial Fibrillation Association (SAFA); The EHRA Scientific Initiatives Committee co-chair; Past Chair of the Working Group on Cardiac Arrhythmias, Serbian Cardiology Society.
Belgrade University Clinical Centre of Serbia, Belgrade, Serbia
MY CONFLICTS OF INTEREST:
Consultant and speaker for • Bayer, • Pfizer and • Boehringer Ingelheim
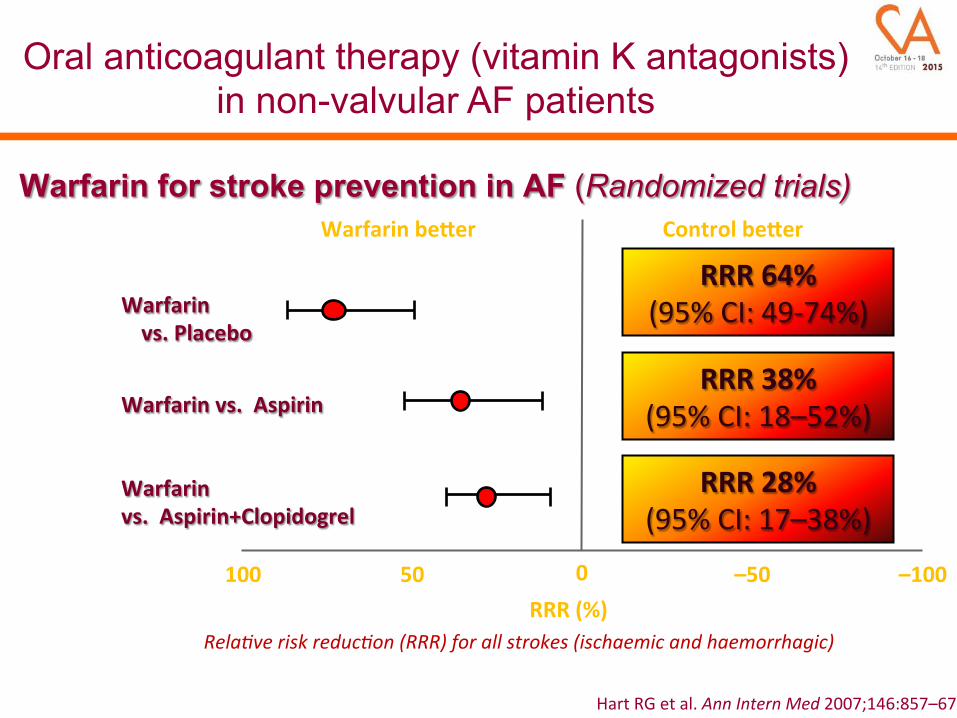
Rela%ve'risk'reduc%on'(RRR)'for'all'strokes'(ischaemic'and'haemorrhagic)'
Warfarin for stroke prevention in AF (Randomized trials) Warfarin'be*er' Control'be*er'
RRR'(%)'100' –100'50' 0' –50'
Warfarin''vs.'Placebo'
RRR'64%'(95%%CI:%49*74%)%
Hart%RG%et%al.%Ann'Intern'Med'2007;146:857–67%
RRR'38%'(95%%CI:%18–52%)%Warfarin'vs.''Aspirin'
Warfarin''vs.''Aspirin+Clopidogrel'
RRR'28%'(95%%CI:%17–38%)%
Oral anticoagulant therapy (vitamin K antagonists) in non-valvular AF patients

0.5% 1.0% 2.0%
Favours'NOAC' Favours'warfarin'
Warfarin''(events)'
NOAC''(events)'
RE*LY%1*%
ROCKET%AF%2†%
ARISTOTLE%3‡%
ENGAGE%AF*TIMI%484§%
Combined'(random)'
134/6076%
269/7081%212/9120%296/7035%911/29'312'
199/6022%
306/7090%265/9081%337/7036%1'107/29'229'
RR'(95%'CI)% p%
0.66%(0.53–0.82)%
0.88%(0.75–1.03)%0.80%(0.67–0.95)%0.88%(0.75–1.02)%0.81'(0.73–0.91)'
0.0001%0.12%0.012%0.10%<0.0001'
NOACs for STROKE PREVENTION in AF
Stroke'or'systemic'embolic'events'
*Dabigatran%150mg%twice%daily;%†Rivaroxaban%20mg%once%daily;%‡Apixaban%5mg%twice%daily;%§Edoxaban%60mg%once%daily.%
1N%Engl%J%Med%2009;361:1139*1151;%2N%Engl%J%Med%2011;365:883*891;%3N%Engl%J%Med%2011;365:981*992;%4N%Engl%J%Med%2013;369:2093*2104.%
A'19%'RR'reducQon'in'stroke'or'SE'

0.5% 1.0% 2.0%%Favours'NOAC' Favours'warfarin'
NOAC''(events)%
Warfarin''(events)%
RR'(95%'CI)% p%
RE*LY%5*%%%ROCKET%AF%6†%
%%ARISTOTLE%7‡%%%ENGAGE%AF*TIMI%488§%
''Combined'(random)'
375/6076%395/7111%327/9088%444/7012%1'541/29'287'
397/6022%386/7125%462/9052%557/7012%1'802/29'211'
0.94%(0.82–1.07)%1.03%(0.90–1.18)%
0.71%(0.61–0.81)%0.80%(0.71–0.90)%0.86'(0.73–1.00)'
0.34%0.72%
<0.0001%0.0002%0.06'
NOACs for STROKE PREVENTION in AF
Major'bleeding'
*Dabigatran%150mg%twice%daily;%†Rivaroxaban%20mg%once%daily;%‡Apixaban%5mg%twice%daily;%§Edoxaban%60mg%once%daily.%
1N%Engl%J%Med%2009;361:1139*1151;%2N%Engl%J%Med%2011;365:883*891;%3N%Engl%J%Med%2011;365:981*992;%4N%Engl%J%Med%2013;369:2093*2104.%
A'14%'RR'reducQon'in'major'bleeding'

0.2% 0.5% 1.0% 2.0%%
Favours'NOAC' Favours'warfarin'
Pooled'NOAC'(events)'
Pooled'warfarin'(events)'
Efficacy%Ischaemic%stroke%Haemorrhagic%stroke%Myocardial%infarcbon%All*cause%mortality%Safety%Intracranial'haemorrhage'GastrointesQnal'bleeding'
665/29%292%130/29%292%413/29%292%2022/29%292%
204/29'287'751/29'287'
724/29%221%263/29%221%432/29%221%2245/29%221%
425/29'211'591/29'211'
0.92%(0.83–1.02)%0.49%(0.38–0.64)%0.97%(0.78–1.20)%0.90%(0.85–0.95)%
0.48'(0.39–0.59)'1.25'(1.01–1.55)'
RR'(95%'CI)' p'
0.10%<0.0001%0.77%0.0003%
<0.0001'0.043'
NOACs for STROKE PREVENTION in AF
Secondary'efficacy'and'safety'outcomes'
*Dabigatran%150mg%twice%daily;%†Rivaroxaban%20mg%once%daily;%‡Apixaban%5mg%twice%daily;%§Edoxaban%60mg%once%daily.%
1N%Engl%J%Med%2009;361:1139*1151;%2N%Engl%J%Med%2011;365:883*891;%3N%Engl%J%Med%2011;365:981*992;%4N%Engl%J%Med%2013;369:2093*2104.%
A'51%'RR'reducQon'in'haemorrhagic'stroke'A'10%'RR'reducQon'in'allZcause'mortality'
Do not cause BLEEDING
Prevent THROMBOSIS
The use of oral anticoagulant therapy for stroke prevention in atrial fibrillation

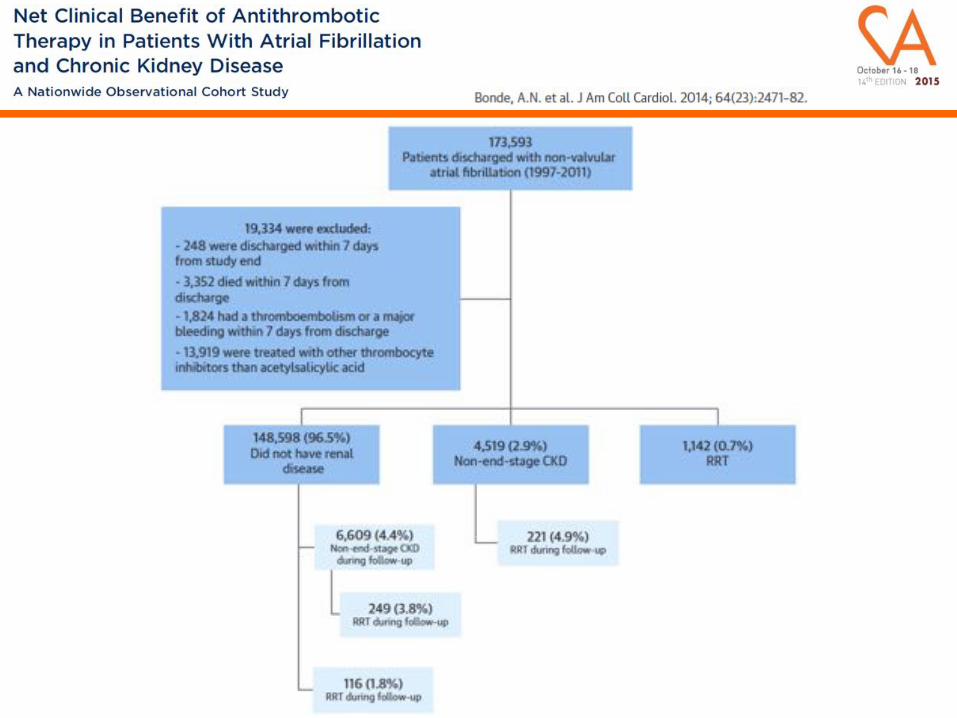
Olesen JB, Lip GYH, Kamper A., et al. NEJM 2012;367:625.



The value of vitamin K antagonists in patients with less advanced CKD and AF resembles that of non-CKD patients

No'relevant'data'from'randomized'clinical'trials!'Large'database'analyses'(a'number'of'limitaQons!):'%• Chan%et%al.%J'Am'Soc'Nephrol'2009;20:2223:%in%1671%incident%hemodialysis%pabents%with%preexisbng%AF%(mean%follow*up%of%1.6%years),%warfarin'use'was'associated'with'a'significantly'increased'risk'for'new'stroke%(HR'1.93;'95%CI,1.29Z2.90).'%Study%limitabons:%INR%monitoring,%INR%reporbng,%drug%disconbnuabon,%etc.%%• The'DOPPS*'data'(1996*2004)%on%2188%pabents%with%prevalent%AF:%increased'risk'for'stroke'with'warfarin,%parbcularly%in%pabents%aged%≥75%y%(HR'2.17;'95%CI,'1.04Z4.53).%%• Winkelmayer%et%al.%Clin'J'Am'Soc'Nephrol'2011;6:2662:%No%difference%in%ischemic%stroke%risk%(HR%0.92;%95%CI,%0.61*1.37)%in%237%pabents%with%incident%AF%and%taking%warfarin%vs.%948%propensity%matched%non*anbcoagulated%pabents,%but%significantly'increased'risk'for'haemorrhagic'stroke'with'warfarin%(HR'2.38;'95%CI,'1.15Z4.96).%%
Vitamin K antagonists in end-stage CKD patients with AF
*Dialysis'Outcomes'and'PracQce'Pa*erns'study'

A retrospective analysis

307,351 AF patients identified in national
Patient register
294,312 remaining
283,969 remaining for study 13,435 with renal failure
270,534 without renal failure
10,343 exluded because of death
<14 days from index
13,039 excluded because of mitral
stenosis or valvular surgery




A Danish AF cohort 1997-2008
N=132,372




All patients with any CKD compared to no CKD Stroke or SE
HR (95%CI) P Major bleeding
HR (95%CI) P
Warfarin 0.76 (0.64-0.91) 0.003 1.33 (1.16-1.53) <0.001 Aspirin 1.17 (1.01-1.35) 0.04 1.17 (1.02-1.34) 0.03 Warfarin plus aspirin 0.74 (0.56-0.98) 0.04 1.61 (1.32-1.96) <0.001




All NOACs are partly eliminated via the kidneys Dabigatran has the greatest extent of renal elimination

Prolongation of the NOACs half-lives is proportional to the degree of renal dysfunction

A pre-specified sub-analysis Estimation of GFR: 1. Cockcroft-Gault formula 2. CKD-EPI equation (Chronic Kidney
Disease Epidemiology Collaboration) 3. Cystatin C equation 4. MDRD equation (Modification of Diet in
Renal Disease)
eGFR Cockcroft-Gault
CKD-EPI
≥ 80 mL/min 5844 (32.6%) 3880 (21.6%)
50-79 mL/min 8553 (47.6%) 10697 (59.6%)
30-49 mL/min 3554 (19.8%) 3374 (18.8%)
eGFR <30mL/min (Cockcroft-Gault) was an exclusion criterion in the RE-LY


Patients with atrial fibrillation receiving oral anticoagulation exhibited a decline in renal function that was greater in those taking warfarin versus DE, and it was amplified by diabetes and previous vitamin K antagonist use
Changes in Renal Function in Patients With Atrial Fibrillation: An Analysis From the RE-LY Trial
Bohm M, et al. J Am Coll Cardiol 2015;65(23):2481-93.

A pre-specified secondary analysis • Renal function was estimated using the Cockcroft-Gault equation • 2950 of 14264 patients (20.7%) had a CrCl of 30-49mL/min
• Rivaroxaban dose was reduced to 15mg once daily • Patients with a CrCl of 30-49mL/min on warfarin (n=1476) had a median TTR of 57.7 (IQR 42.2-69.9)
eGFR <30mL/min (Cockcroft-Gault) was an exclusion criterion in the ROCKET AF


A pre-specified secondary analysis Apixaban dose was reduced to 2.5 bid if 2 of 3 of the following criteria were met: • age of ≥80 years • body weight of ≤60kg • serum creatinine of ≥1.5mg/dL (133µmol/L)
eGFR Cockcroft-Gault
CKD-EPI
> 80 mL/min 7518 (42%) 5190 (29%)
51-80 mL/min 7587 (42%) 10151 (56%)
30-50 mL/min 3017 (15%) 2843 (16%)
Serum Cr >2.5mg/dL or calculated CrCl <25mL/min (Cockcroft-Gault) was an exclusion criterion in the ARISTOTLE


Edoxaban 60mg and 30mg once daily Edoxaban dose reduction criteria (at least one of the following): • CrCl <50mL/min (30-49mL/min), • body weight ≤60kg or • concomitant therapy with verapamil or quinidine or dronedarone
CrCl <50mL/min at randomization: n=1361 patients (19.3%)


Qamar A, Bhatt, D. L. Nat. Rev. Nephrol. 2015; doi:10.1038/nrneph.2015.14
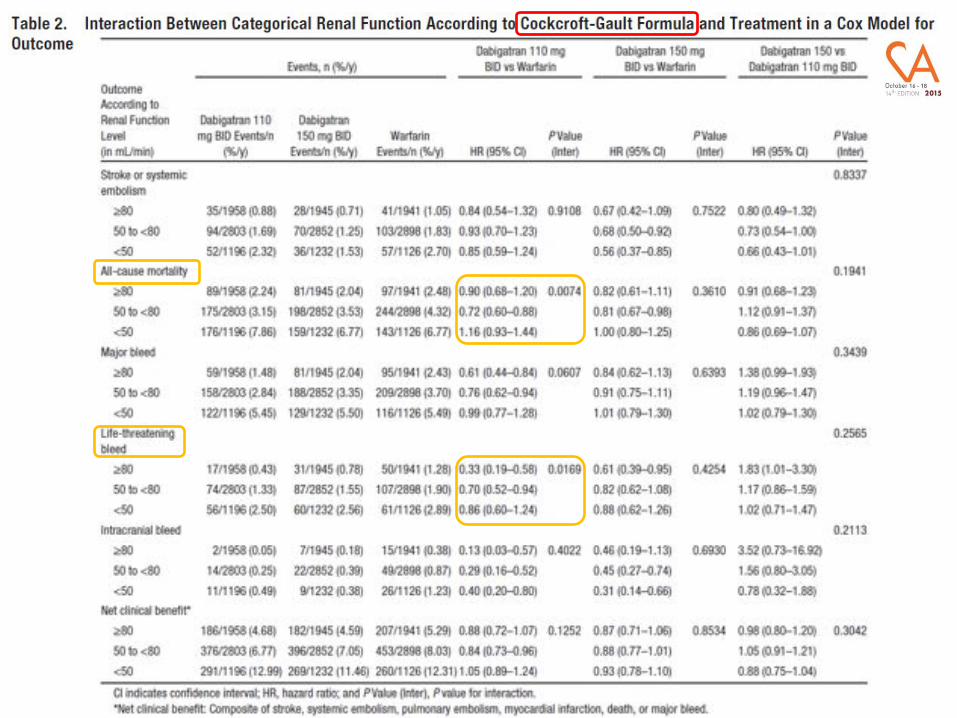
Efficacy and safety of NOACs vs. warfarin in patients with moderate CKD

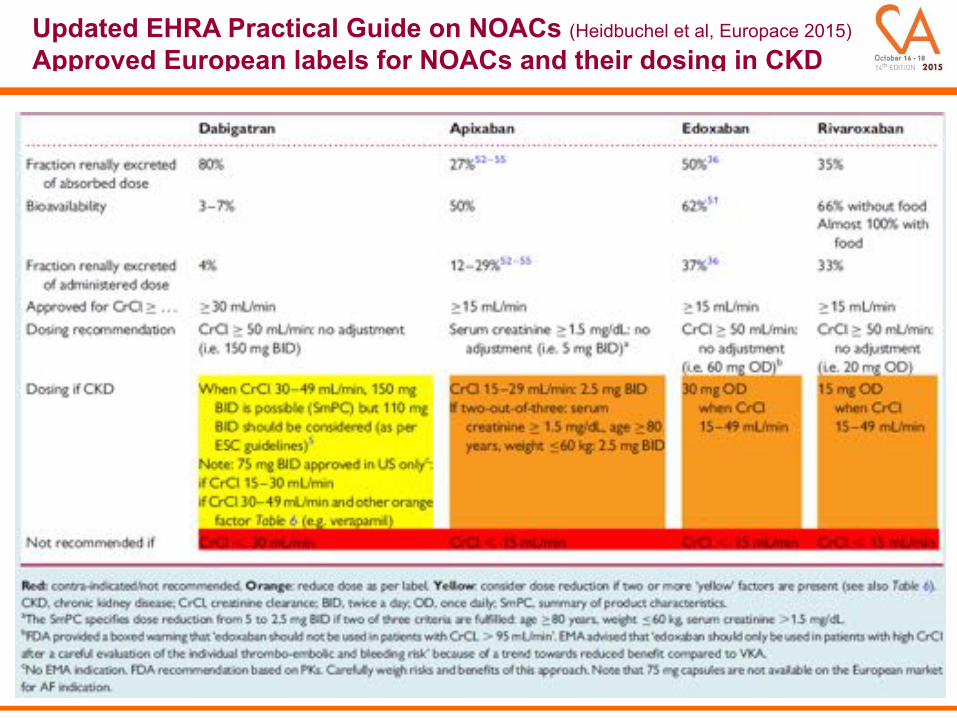
Updated EHRA Practical Guide on NOACs (Heidbuchel et al, Europace 2015) Approved European labels for NOACs and their dosing in CKD

Camm AJ et al. Eur Heart J 2012;33:2719–47
ESC 2012 focused update: NOACs in patients with renal impairment
Recommendation Class Level
Baseline and subsequent regular assessment of renal function (by CrCl) is recommended in patients following initiation of any NOAC, which should be done annually but more frequently in those with moderate renal impairment where CrCl should be assessed 2–3 times per year
IIa A
NOACs (dabigatran, rivaroxaban, and apixaban) are not recommended in patients with severe renal impairment (CrCl <30 mL/min)
III A
ESC 2012 focused update: NOACs in patients with renal impairment



Component PointsS Sex (female) 1A Age (<60 years) 1Me Medical history* 1T Treatment (interacting drugs, e.g.,
amiodarone)1
T Tobacco use (within 2 years) 2R Race (non-Caucasian) 2
*More than two of the following: hypertension, diabetes mellitus, coronary artery disease/myocardial infarction, peripheral arterial disease, congestive heart failure, previous stroke, pulmonary disease, and hepatic or renal disease.
Patient already taking a VKA?
NO
YES
SAMe%TT2R2 ≤2*** SAMe%TT2R2 >2***
VKAs*(or*NOACs)***
NOACs***
Labile INR(TTR<70%)
TTR≥70%, patient
satisfied with VKA
VKAs***

Conclusions: 1. Patients with AF and CKD taking OAC have increased rates of
stroke and bleeding compared with non-CKD patients, irrespective of the OAC type (VKAs or NOACs)
2. Benefits of OAC are evident for patients with a non-end-stage CKD, and NOACs broadly offer additional net clinical benefit over VKAs in these patients
3. More data are needed to guide the use of OAC in patients requiring RRT. Whilst available data suggest that these patients may benefit from VKAs, experience with NOAC is lacking
4. Patients with advanced CKD taking OAC require close and regular clinical follow-up and monitoring of renal function, and achieving a good TTR in CKD patients taking VKA is essential.



















