Embed Size (px)
Citation preview
Ménière’s DiseaseSam Maleki, Jordan Braun, Alex Wohl, Rob Whittaker

Etiology
Female Caucasians most prone to disorder. 157/100k in England
46/100k in France
Peak incidence 40-60 y.o. (1.3:1 female to male ratio) 2-50% of symptoms arise in opposite ear
Prevalence rates caused by differences in environment, genetics, or diagnostic criteria is unclear
Familial occurrence reported in 10-20% cases (autosomal dominant mode of inheritance)
Genetics – human leukocyte antigens B8/DR3 & Cw7 have been associated

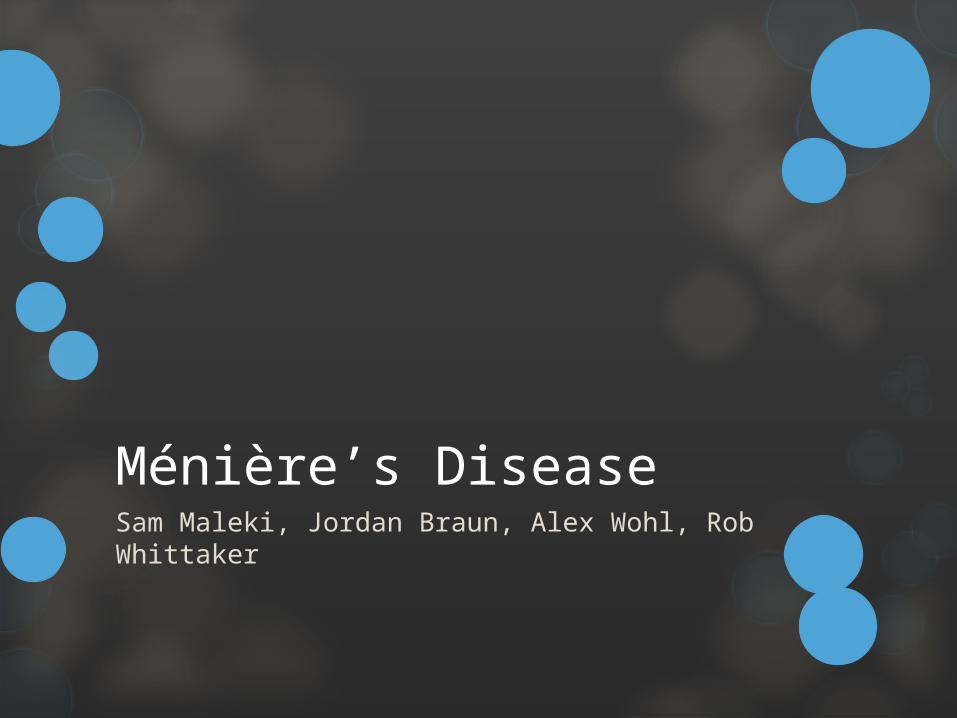
Anatomy/Physiology
Vestibular System Detects forces from gravity & movement, maintains clear vision
during head motion (VOR) by head positioning
Semicircular canals – ring-shaped, fluid filled (endolymph) oriented in 3D provides sensory input to velocity & angular acceleration (ampulla deflected away from direction of head movement by endolymph)
Speed & direction of deflection of hair cells of ampulla determines the rate of firing of the vestibular nerve
Ends of semicircular duct open into otolith (utricle & saccule) – contained hair cells covered in otolithic membrane (otoconia produce shear force)
Signals carried by vestibular nerve - If lesion in vestibular nerve, brain can possibly adapt from intact opposite nerve & recalibrate
Motor output through vesibulospinal reflexes (VSRs) – automatic control of postural muscles in trunk & limbs

Anatomy/Physiology Cont’d
Audition Tympanic membrane Ossicles cochlea via oval windows
Scala vestibula & scala tympani (perilymph), Scala media (endolymph)
Pressure waves travels through scala vestibuli, helicotrema, & scala tympani pressure changes onto basilar membrane & into Organ of Corti exits round window at end of scala tympani
Inner ear (cochlea – fluid filled tube dived by organ of Corti)
Fluid incompressible & bony wall rigid, important to maintain fluid volume
Sound through ossicles oval window scala vestibuli (perilymph) scala tympani round window
Endolymph in scala media
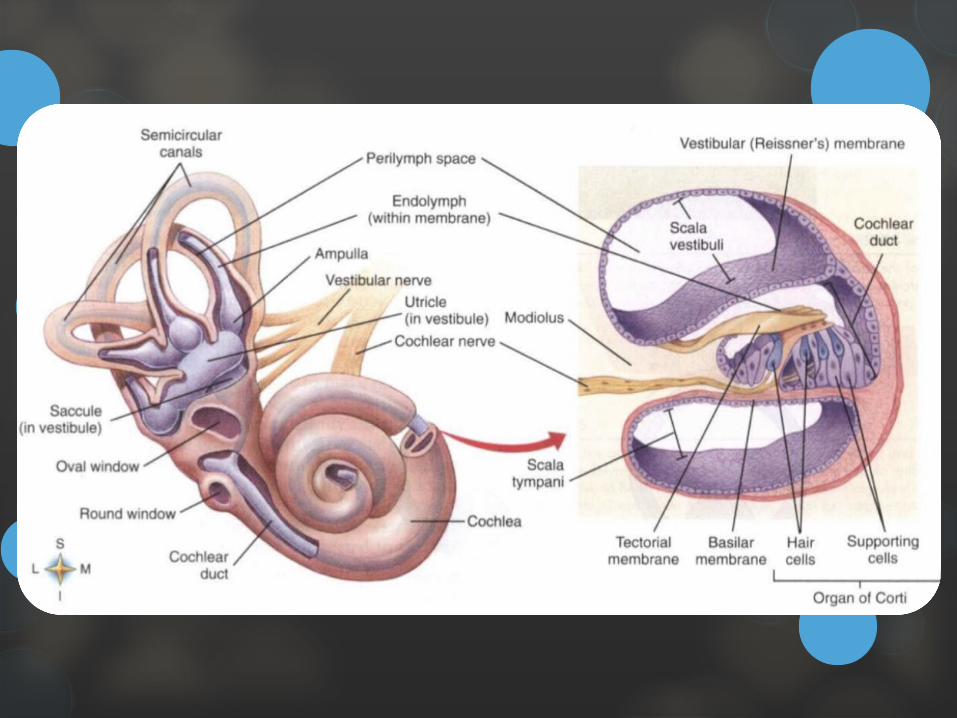

Pathology
Endolymphatic hydrops – over accumulation of endolymph compromising perilymphatic space Lack of absorption of endolymph in endolymphatic duct &
fluid backs up into system
Characterized by episodic vertigo; fluctuating, sensorineural hearing loss; sensation of fullness in the ears; & tinnitus
Vertigo most debilitating symptom with intervals of hours to days
Simultaneous hearing deterioration of involved ear
Reduction in responsiveness of involved peripheral vestibular system can occur
Pathology cont’d
Multifactorial causes Fibrosis, atrophy of the sac, obstruction of the
endolymphatic duct, infection, or the vascularity in the region in the inner ear.
Otosyphilis (involvement of the inner ear in collagen vascular disease)
Immune responses likely within the complex related to allergic reactions & histamine
Viral infection – more susceptible to changes in thyroid, Na+ or hormone dysfunction
Overproduction of endolymph by stria vasularis
Blow to head, a fall, or flexion/extension injury

Pathology cont’d
Pathogenesis of symptoms uncertain
Deficits related to volume/pressure changes within closed fluid system Membranous labyrinth progressively dilate until the wall
makes contact with the stapes footplate & the cochlear duct fills the entire scala vestibula vestibular & cochlear dysfunction
Distension of otoliths can put pressure on the ampulla, creating sensation of spinning that is characteristic of acute unilateral dysfunction
Membrane rupture leak of K+ into endolymph Nerve palsy
Pathology cont’d
Typical attack of hydrops – initial sensation of fullness of the ear, reduction in hearing, & tinnitus Followed by rotational vertigo (30 min – 24 hours), postural
imbalance, nystagmus, & nausea
Permanent loss of hearing over time
Tinnitus is commonly described as low-pitched roaring or seashell like
History
General Questions: Age, date of onset, previous history of falls
Triad of Associated Symptoms: Vertigo
Tinnitus
Fluctuating Hearing Loss
Family History 7-10% affected
Employment: Current work, community, & leisure actions, tasks, or activities

History Cont’d
Functional status & activity level: current/prior functional status in self care/home & in work
Medications
Other clinical tests: lab & diagnostic tests, review of available records, review of other clinical findings
Employment: Current work, community, & leisure actions, tasks, or activities
General health status: general health perception, physical function, psychological function, role function, social function
Other clinical tests: lab & diagnostic tests, review of available records, review of other clinical findings
Systems Review
CV: BP, edema, HR, RR
Integumentary: pliability, scar formation, skin color/integrity
Musculoskeletal: ROM, strength, symmetry, height/weight
Neuromuscular: coordination (balance, gait, locomotion, transfers, transitions), motor function
Cranial Nerve Testing Nystagmus testing
Communication, affect, cognition, language, & learning style Ability to make needs known, consciousness, expected
emotional/behavior responses, learning preferences, orientation (person, place, time)

Global outcomes
Functional Limitations – Nottingham health profile, SF – 12/36, Quality of Well being (self administered), dizziness handicap inventory1
Visual analogue scale (VAS), dizziness handicap inventory (DHI), functional disability scale, motion sensitivity quotient (MSQ)2
Gait, locomotion, & balance Elderly mobility scale, Fugl-Meyer assessment scale, functional
standing test, hop tests, obstacle course, seated postural control measure, TUG, trunk control
Berg balance scale, Romberg Tests, sit to stand tests, tilt board balance tests, Tinetti performance-oriented mobility scale
Functional ambulation profile, gait abnormality rating scale, gait speed, Rivermead visual gait assessment

PT tests
Smooth pursuits (nystagmus)
Saccadic eye movements (look back/forth 2 objects)
VOR (focus on an object while turning head)
Head thrusts (quick passive movements by PT)
Head shaking (pt. actively move head quickly)
Dix-Hallpike maneuver (BPPV test)
Lab (by physician) Caloric (air/water injected - alter temp)
Rotational (Barany test, rotate in chair, watch eyes, balance master)
Special Tests
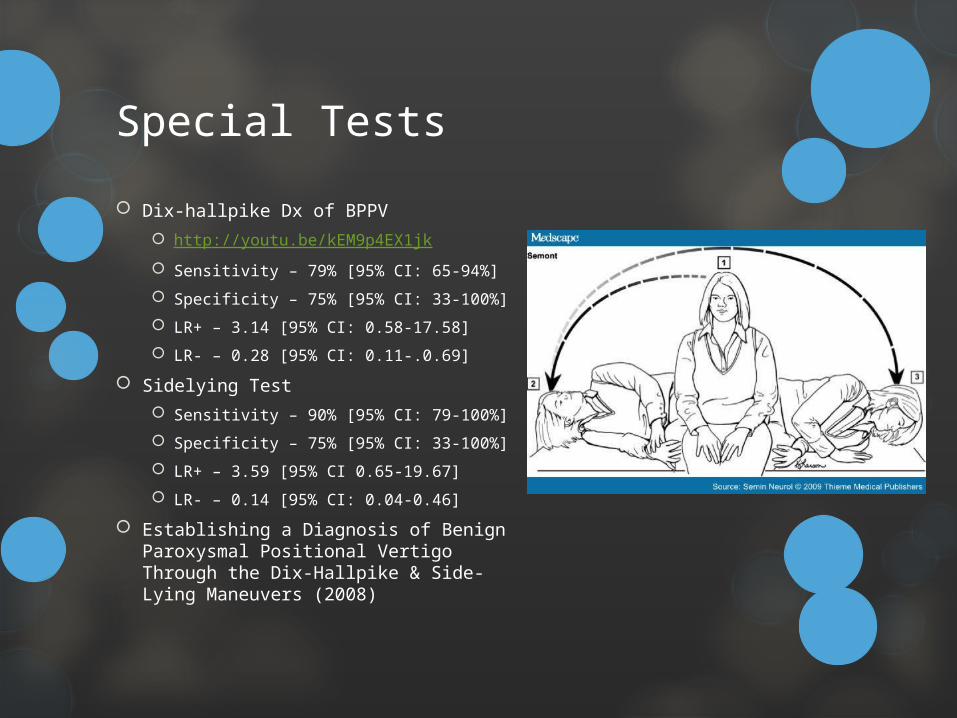
Dix-hallpike Dx of BPPV http://youtu.be/kEM9p4EX1jk
Sensitivity – 79% [95% CI: 65-94%]
Specificity – 75% [95% CI: 33-100%]
LR+ – 3.14 [95% CI: 0.58-17.58]
LR- – 0.28 [95% CI: 0.11-.0.69]
Sidelying Test Sensitivity – 90% [95% CI: 79-100%]
Specificity – 75% [95% CI: 33-100%]
LR+ – 3.59 [95% CI 0.65-19.67]
LR- – 0.14 [95% CI: 0.04-0.46]
Establishing a Diagnosis of Benign Paroxysmal Positional Vertigo Through the Dix-Hallpike & Side-Lying Maneuvers (2008)

Special Tests Cont’d
Vestibular evoked myogenic potentials (VEMPs) Sensitivity – 50.0%
Specificity – 48.9%
LR+ – 1.04
LR- – 1.00
Caloric Test Sensitivity – 37.7%
Specificity – 51.2%
LR+ – 0.75
LR- – 0.72
No significant difference in hearing level between patients appropriately or inappropriately identified by VEMPs, whereas significant difference in those of the caloric test.
Combined VEMP & caloric test increased sensitivity to 65.8%
The diagnostic value of vestibular evoked myogenic potentials in patients with Meniere’s disease (2013)
Evaluation
Rule out differential diagnosis
Potential referral for diagnosis
Describe frequency & duration of symptoms
Refer to previous slides for other testing

Differential Diagnosis
Pathology Implications for the Physical Therapist Presence of neurologic signs or symptoms such as syncope, visual aura,
& motor weakness suggest another diagnosis
Disorders that present with similar symptoms include: migraine, acoustic neuroma, perilmyphatic fistula, dehiscence of the superior semicircular canal, labyrinthitis, autoimmune inner ear disorder, & MS
Vertigo – a feeling of spinning & loss of balance, caused by disease affecting the inner ear or the vestibular nerve
Migraines – a regular aching/throbbing headache that usually affects one side of the head usually goes along with nausea & troubled vision.
Vestibular Neuronitis – Can be a series/single attack of vertigo or a persistent condition that decreases over 6 weeks
Postural muscle weakness, reflex integrity/peripheral nerve
BPPV

Differential Diagnosis Cont’d
Factors that may differentiate Ménière’s disease from benign recurrent vertigo Based on case-control study of 112 patients with Ménière’s
disease & 63 patients with benign recurrent vertigo
Vertigo attacks with unilateral tinnitus & unilateral hearing loss more likely to be Ménière’s disease in multivariate analysis
Earlier age at onset & shorter duration of vertigo attacks, female preponderance, & presence of migraine more common in benign recurrent vertigo
Differential Diagnosis (Reference)
Other problems to be considered include the following: Trauma, Endocrine abnormalities, Thyroid dysfunction, Hyperlipidemia,
Diabetes, Congenital anomalies, Autoimmune problems/inner ear inflammation,
Differential Diagnosis Anterior Circulation Stroke, AVM, Basilar Artery Thrombosis, Benign
Positional Vertigo in Emergency Medicine, Benign Skull Tumors, Brainstem Gliomas, Cerumen Impaction Removal, Ear Foreign Body Removal in Emergency Medicine, HIV-1 Associated CNS Conditions – Meningitis, Hypothyroidism & Myxedema Coma in Emergency Medicine, Inner Ear Labyrinthitis, Intracranial Hemorrhage, Ischemic Stroke in Emergency Medicine, Lyme Disease, Migraine Headache, Multiple Sclerosis, Neurosyphilis, Otitis Media in Emergency Medicine, Polyarteritis Nodosa, Posterior Cerebral Artery Stroke, Primary Malignant Skull Tumors, Rheumatoid Arthritis, Salicylate Toxicity in Emergency Medicine, Subarachnoid Hemorrhage in Emergency Medicine, Syncope & Related Paroxysmal Spells, Temporal Lobe Epilepsy, Transient Ischemic Attack, Vestibular Neuronitis, Viral Encephalitis, Viral Meningitis, Wernicke Encephalopathy
Diagnosis
Practice Pattern 5A: Primary Prevention/Risk Reduction for Loss of Balance & Falling
ICD-9-CM Code – 386.0
Pathology Implications for the Physical Therapist 2 or more definitive episodes of spontaneous rotation
vertigo lasting at least 20 minutes (nausea & vomiting abates by 24 hours)
Low frequency sensorineural hearing loss documented by audiometry
Tinnitus or aural fullness in the affected ear
Exclusion of other causes for the symptoms

Prognosis
Expected Range of Number of Visits Per Episode of Care
2-18 visits
Range affected by: accessibility/availability of resources, adherence, age, cognitive status, co-morbidities, concurrent medical interventions, level of impairment/physical function, living environment, nutritional status/overall health status, psychological & socioeconomic factors, social support, stability of condition
Prognosis Cont’d
Highly variable, Attacks increase in frequency in first years then decrease
Clusters of attacks may be separated by periods of long remission – balance function between attacks can be normal, although a sense of disequilibrium often persists later in the disorder
2-6% of patients experience “drop attacks” (otolithic crisis of Tumarkin) – abruptly thrown to the ground without LOC & with little/no vertigo
Initially 1 ear – bilateral disease ranges from 2-78% with an average incidence of 45%
If bilateral involvement has not occurred within 5 years of onset of first ear, then unlikely will occur
Hearing loss fluctuating, low-frequency sensorineural loss early becomes irreversible often progressing in severity with higher frequencies & loss of speech discrimination

Problem list/Symptoms
Inner ear condition of vestibular & cochlear systems Recurrent vertigo
Hearing loss & tinnitus in one year
Feeling of pressure differences in ears
Nausea
Balance deficits
Risk of fall
Goals
Patient will reduce the risk of falling through therapeutic exercise, balance training, & lifestyle modification within 4-6 weeks to improve quality of life.
Reduce nystagmus
Improve dizziness
Increase smooth pursuit
Independent HEP
Increase balance
Improvement via functional test (Berg, MiniBEST, ect.)
Surgical Intervention
Cochlear implant Improved hearing reported with cochlear implantation in case
series of 9 patients (mean age 61 years) with Ménière’s disease for at least 10 years & severe sensorineural hearing loss
Vertigo may decrease with/without surgical intervention
Endolymphatic sac surgery does not appear effective for Ménière’s disease
Endolymphatic sac shunt & ventilating tube insertion appear similarly effective both treatments associated with significant reductions in dizzy spells at 6 & 12 months, but no significant differences between groups
Middle ear injections Gentamicin
Steroids
Post-Surgical Timeline
Goal: 30 days before return to work
Physician will assess need for continued interventions, or possible use of medications
PT may be utilized to address any functional limitations Neuromuscular Reeducation
Strengthening
Aerobic Conditioning
PT will continue to monitor for signs/symptoms that indicate referral back to a physician is necessary
Intervention Cont’d
Patient will need referral from Physician PT alone cannot diagnose Ménière’s Disease
Precautions/Contraindications Sudden loss of hearing
Increased feeling of pressure or fullness to discomfort in ears
Severe ringing in ears
Severe increase in symptoms
Severe nausea
Intervention
Addressing required functions, collaboration & coordination with agencies (equipment, payers, home care), communication (education/documentation), data collection/analysis, documentation
Therapeutic exercise – aerobic/endurance training, balance/coordination/agility, body mechanics/postural stabilization, flexibility, gait training Treatment
Diuretics can control vertigo & stabilize hearing in more than ½ of individuals
Restricting salt, caffeine, alcohol, & nicotine (reduces endolymph volume by fluid removal)
Antivertiginous meds, antiemetic, sedatives, antidepressants, & psychiatric treatment
Corticosteroid infusion of the middle ear via a transtympanic route – autoimmune & inflammatory injury
Intratympanic gentamicin used for chronic unrelenting unilateral hydrops
Surgery for endolymphatic decompression

Inpatient/Outpatient Care (nonsurgical) Balance/Vestibular training program progressions
Gaze stabilization exercises
Hip, knee, & ankle strategies
Therapeutic Exercises Aerobic
Strength
Assess Vertigo if needed
Gait analysis
Patient Education Home analysis
HEP
The use of different devices (hearing, AD)

Surgical Intervention
Vestibular nerve section: Selective vestibular nerve section (AKA vestibular
neurectomy)
Goal is to disconnect diseased labyrinth from brainstem while preserving hearing
Complications may include hearing loss, facial nerve injury, CSF leak, & headache
Retrosigmoid approach of vestibular nerve section reported to control vertigo in patients with Meniere's disease
Translabyrinthine vestibular nerve section may be superior to labyrinthectomy for improving balance, but appears to have similar efficacy for vertigo

Home Program
Hearing Aid
Meniette device-positive pressure device administer 3x/day for five min/session. Equalizes pressure in patient with persistent problems
Home assessment
Continue inpatient/outpatient care
Dietary Changes Limit Caffeine & sodium
Lifestyle changes Stop smoking
Manage stress/anxiety
Eat regularly

Patient Education
Who’s affected/prevalence
What causes the disease
How the disease impacts function (hearing/balance?)
Identifying signs/symptoms
Options for treatment (refer/balance training)
HEP
Potential of extra help
Secondary complications in life
Three systems that control balance Somatosensory, visual, vestibular
Discharge
Occurs when anticipated goal & expected outcomes have been achieved Patient has met goals
Improved functional ability
Improved quality of life
Dependent on medical/psychosocial status
Significant improvement on functional assessments
PT determines pt. will no longer benefit

References
1. Guide to physical therapy practice. 2nd ed. APTA; 2003.
2. O'Sullivan SB, Schmitz TJ. Physical rehabilitation. F a Davis Company; 2007. 3. Kisner C, Colby LA. Therapeutic exercise: Foundations and techniques. F a Davis Company; 2007.
3. Goodman CC, Fuller KS. Pathology: Implications for the physical therapist. SAUNDERS W B Company; 2009.
4. Alexander TH, Harris JP. Current epidemiology of meniere's syndrome. Otolaryngol Clin North Am. 2010;43(5):965-970. doi: 10.1016/j.otc.2010.05.001; 10.1016/j.otc.2010.05.001.
5. Egami N, Ushio M, Yamasoba T, Yamaguchi T, Murofushi T, Iwasaki S. The diagnostic value of vestibular evoked myogenic potentials in patients with meniere's disease. J Vestib Res. 2013;23(4-5):249-257. doi: 10.3233/VES-130484; 10.3233/VES-130484.
6. Guidetti G, Monzani D, Rovatti V. Clinical examination of labyrinthine-defective patients out of the vertigo attack: Sensitivity and specificity of three low-cost methods. Acta Otorhinolaryngol Ital. 2006;26(2):96-101.
7. Saeed SR. Fortnightly review. Diagnosis and treatment of Meniere's disease. BMJ. 1998 Jan 31;316(7128):368-72
8. Vassiliou A, Vlastarakos PV, Maragoudakis P, Candiloros D, Nikolopoulos TP. Meniere's disease: Still a mystery disease with difficult differential diagnosis. Ann Indian Acad Neurol. 2011;14(1):12-18. doi: 10.4103/0972-2327.78043; 10.4103/0972-2327.78043.
9. Meniere's society. Meniere's Society Web site. http://www.menieres.org.uk/. Updated 2013. Accessed February 26, 2014.
10. Li J, Lorenzo N. Meniere disease (idiopathic endolymphatic hydrops) Differential diagnoses. Medscape Web site. http://emedicine.medscape.com/article/1159069-differential. Updated 2014. Accessed February 26, 2014.
11. Meniere's disease. Mayo Clinic Web site. http://www.mayoclinic.org/diseases-conditions/menieres-disease/basics/definition/CON-20028251. Updated 2012. Accessed February 24, 2014.

References
12. Rauch, SD. Clinical hints and precipitating factors in patient’s suffering from Meniere’s disease. Otolaryngol Clin North Am. 2010 Oct; 43(5): 1011-7
13. Minor LB, Schessel DA, Carey JP. Meniere's disease. Curr Opin Neurol. 2004 Feb;17(1):9-16
14. Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Menière's disease. American Academy of Otolaryngology-Head and Neck Foundation, Inc. Otolaryngol Head Neck Surg. 1995 Sep;113(3):181-5, commentary can be found in Otolaryngol Head Neck Surg 1996 Jun;114(6):835
15. Syed I, Aldren C. Meniere's disease: an evidence based approach to assessment and management. Int J Clin Pract. 2012 Feb;66(2):166-70
16. Enticott JC, O'leary SJ, Briggs RJ. Effects of vestibulo-ocular reflex exercises on vestibular compensation after vestibular schwannoma surgery. Otol Neurotol. 2005;26(2):265-269.