Embed Size (px)
Citation preview

Medicina de precisión en cáncer de ovario: Determinación de BRCA germinal y somático
Dra. Cristina Martin Lorente
Hospital de la Santa Creu i Sant Pau. Barcelona

Introduction
• Ovarian cancer is the fifth leading cause of cancer death in women in
developed countries. Estimated incidence of 225,000 women and
140,000 deaths per year worldwide
• Optimal surgery and platinum-based chemotherapy are the mainstay
of front-line treatment but about 80% will relapse
• Up to 15% of epithelial OC cases are familial. Inherited mutations in
BRCA1/2 account for the majority of familial OC with an increased
lifetime risk of developing OC 40-60% BRCA1 and 11-30% BRCA2
Globocan 2012. Ford D et al Am J Hum Genet 1998. National Cancer Institute 2017. Ford D et al Am J Hum Genet 1998

Ovarian Cancer (OC): Multiples Diseases
• Different types with different behaviour
• Most Common – High grade serous ovarian cancer (HGSOC)
• HGSOC: Associated with characteristics of genomic instability (TP53) and homologous recombination deficiency (BRCA)

Defining BRCAness Phenotype
• Ovarian cancers in women
with BRCA1/2 germline
mutations are characterized by
an improved response to
platinum-based chemotherapy
at first and subsequent
relapses and better outcomes
(PFS, OS)
Tan D JCO 2008; Fong FC JCO 2010; Audeh MW Lancet 2010; Ledermann J Lancet 2014; Fong FC NEJM 2009

Defining BRCAness Phenotype
• BRCA1/2 germline mutated populations have also shown
exceptional sensitivity to PARP inhibitors (PARPi)
Tan D JCO 2008; Fong FC JCO 2010; Audeh MW Lancet 2010; Ledermann J Lancet 2014; Fong FC NEJM 2009

Use BRCA deficiency for treatment
Olaparib
Rucaparib
Veliparib
Niraparib
BMN-673
Tewari Clin Cancer Res 2015

Targeting BRCA in Ovarian Cancer:
An approach for personalizing
management of OC

PARP inhibitors in clinical trials

Response by BRCA status:
ORR 41% with BRCAm vs 24% BRCAwt
Gelmon et al. Lancet Oncol 2011
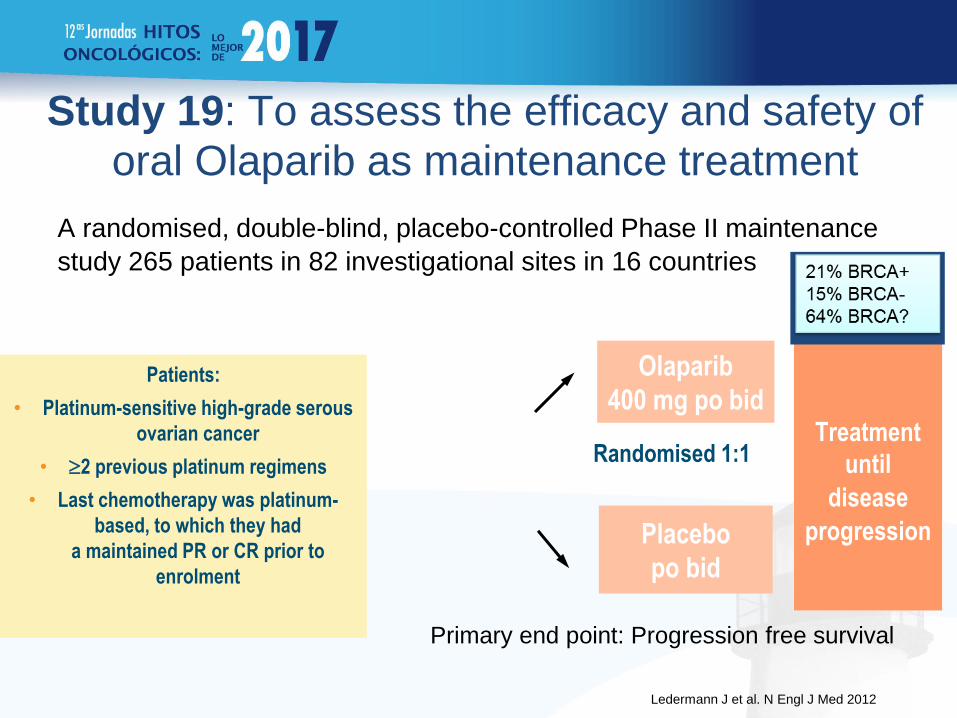
Study 19: To assess the efficacy and safety of
oral Olaparib as maintenance treatment
A randomised, double-blind, placebo-controlled Phase II maintenance
study 265 patients in 82 investigational sites in 16 countries
Olaparib
400 mg po bid
Randomised 1:1
Placebo
po bid
Patients:
• Platinum-sensitive high-grade serous
ovarian cancer
• 2 previous platinum regimens
• Last chemotherapy was platinum-
based, to which they had
a maintained PR or CR prior to
enrolment
Treatment
until
disease
progression
Primary end point: Progression free survival
Ledermann J et al. N Engl J Med 2012

Olaparib met the primary endpoint of improving PFS
in the OVERALL study population
Ledermann J et al. N Engl J Med 2012

More than 50% patients had a known
deleterious BRCAm (Pre-planned BRCA testing)
Patients with a known BRCA status increased from 98 (37%) to 254 (95.8%) out of 265: • 136 (51.3%) patients had a known deleterious BRCAm (BRCAm dataset) • 118 (44.5%) patients were defined as BRCA1/2 wild type for this analysis • 11 (4.2%) patients had neither a tumour nor a germline result available
Ledermann J et al. N Engl J Med 2012

Olaparib significantly prolonged PFS in
platinum-sensitive relapsed HGSOC –Patients with a BRCA mutation receive greater treatment benefit
–Non-mutation carriers may also benefit from olaparib treatment
0
Time from randomization (months)
0
1.0
Pro
po
rti
on
of
pati
en
ts
pro
gressio
n-f
re
e
3 6 9 12 15
Olaparib BRCAm
Olaparib BRCAwt
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
BRCAm (n=136) BRCAwt (n=118)
Olaparib Placebo Olaparib Placebo
Median PFS,
months
11.2 4.3 7.4 5.5
HR=0.18
P<0.00001
HR=0.53
P=0.007
BRCAm (n=136) BRCAwt (n=118)
Olaparib Placebo Olaparib Placebo
Median PFS,
months
11.2 4.3 7.4 5.5
HR=0.18
P<0.00001
HR=0.53
P=0.007
Placebo BRCAm
Placebo BRCAwt
Ledermann et al. N Eng J Med 2012. Ledermann et al. Lancet Oncol 2014

BRCAness Phenotype
• BRCA germline mutations
• BRCA somatic mutations
• Similar to germline BRCAm, PFS was longer in somatic BRCAm population compared with wildtype
• Germline or somatic HR mutations was highly predictive of primary platinum and PARPi sensitivity and improved overall survival
Hennessy JCO 2010/ Pennington CCR 2014

WHO TO TEST?
In the past we used to refer patients to genetic
counseling based on their family history and personal
history
Nowadays we have a broaden vision of the disease
which supports that this policy is not accurate enough

• Frequency of BRCA1/2 mutations in women with OC is unclear (3-27%). 1001 women enrolled
onto a population-based case-control study were screened
• Germ-line mutations were found in 14.4% of patients (22.6% HGSOC; 8.4% endometrioid;
6%CC; 0% carcinosarcoma)
• 44% had not reported family history of breast or OC
• BRCAm was associated with better outcomes (RR, PFS, OS)
Conclusions: BRCA status has a major influence on survival, treatment outcomes and treatment
selection and SHOULD BE OFFERED TO ALL WOMEN DIAGNOSED WITH NON-MUCINOUS OC
REGARDLESS OF FAMILY HISTORY
Alsop K JCO 2012

WHO TO TEST?

What about SOMATIC Testing?
Ovarian cancer in women with BRCA somatic mutation (BRCAg wt) is also characterized by an improved response to platinum-based chemotherapy and PARP inhibitors and by better outcomes with longer PFS and improved OS
Olaparib approved by EMA as first-in-class treatment for advanced BRCA-MUTATED (germline and somatic) ovarian cancer (January 2015)
BRCA somatic mutation testing expands the number of patients who would benefit from personalized medicine

WHEN TO TEST?
Initial diagnosis preferable
PRO
• Access to pathology
• Biomarker of response to platinum-based chemotherapy
• Prognostic factor
• Likely PARPi will be approved in front-line setting
• Genetic counselling
CON: Evidence supporting temporal heterogeneity in OC

WHICH ONE FIRST?
GERMLINE TESTING
• Well-established
• Lymphocyte DNA more
reliable
• Need for genetic counselling
• Wildtype, still need to test
somatic mutation
SOMATIC TESTING
• Streamline testing
• Less need for genetic
counselling
• Require good quality of DNA
• Technical Considerations

BRCAness Phenotype
• BRCA germline mutations
• BRCA somatic mutations (Hennessy JCO 2010)
• Other Homologous Recombination DNA repair defects (Kristeleit
ECC0 2015. Pennington CCR 2014)
Levine. Nature 2011

HRD Assays: Lines of Research
• Next-generation sequencing assays. Gene expression analysis.
– BROCA: analysis of mutations of key HR genes (BRCA1, BRCA2, ATM, BARD1, BRIP1, CHEK1, CHEK2, FAM175A, MRE11A, NBN, PALB2, RAD51C, RAD51D).
– 60-genes signature of “BRCAness”…
High correlation with response to platinum-based therapy an overall survival. NOT VALIDATED.
• Functional ex-vivo assays: RAD51 nuclear foci formation by immunofluorescence or other DNA repair complexes by immunohistochemistry
• PRO: Dynamic and functional biomarker
• CON: Requires fresh tissue. Reproducibility.
• Genome scars.
– ARIEL 2. Rucaparib and genomic LOH assay (Foundation Medicine)
– NOVA trial. Niraparib and HRD score (myChoice HRDTM Myriad)

HRD Assays: ARIEL 2 • Different mechanisms can lead to HRD with the final result of genomic
instability and large areas of genomic scaring (uniparental deletions)
• HRD causes genome wide LOH that can be measured by NGS
• TCGA and AOCS developed LOH cutoff based on overall survival to
identify patients with HGSOC with BRCA-like signature
McNeish IA ASCO 2015. TCGA Nature 2011. Wang Clin Cancer Res 2012

CONCLUSIONS
• BRCAness profile is now beyond mutations in BRCA germline
• This profile predicts platinum and PARPi sensitivity and better
clinical outcomes
• BRCA testing in the germline and in the tumor expands up to
20% the number of patients who would benefit from targeted
treatments
• Ideally, patients should be tested at diagnosis
• The validation of HRD assays and multiple gene sequencing panels
to guide treatment selection is under evaluation
• Clinical trials on-going will offer additional insight

GRACIAS

ARIEL 2 (Part 1): Phase 2 trial to prospectively
identify OC responders to rucaparib using tumor genetic analysis
Kristeleit et al ECCO 2015

Efficacy Analysis ARIEL 2 (Part 1)
PFS in tBRCAmut and tBRCA-like vs. biomarker negative
patients
Duration of response in tBRCAmut
and tBRCA-like vs. biomarker
negative patients
Kristeleit et al ECCO 2015

ENGOT-OV16/NOVA Phase 3 randomized double-blind of maintenance with niraparib
vs. placebo in patients with platinum sensitive OC
Mirza ESMO 2016

Tesaro. WorldCDx 2015
HRD Assays: HRD Score

HRD Assays: HRD Score
The HRD test does not identify origin of mutation (germline or somatic) It is based on sequencing ~54,000 SNP regions of the genome and the BRCA1/2 genes (myChoice HRDTM Myriad)
Tesaro. WorldCDx 2015

gBRCA Mutated gBRCA Wild Type
NOVA Trial: PFS by gBRCA status
Mirza ESMO 2016

NOVA Trial: Exploratory Analysis PFS in
gBRCAwt Subgroups
Mirza ESMO 2016

• To identify potential biomarker drivers of efficacy is urgently needed
• The presence of HRD may be a valid strategy for selection for DNA repair inhibitors as PARPi
• The actual HRD assays do not seem to be accurate enough to identify patients who don’t benefit from PARPi
Conclusions