Embed Size (px)
Citation preview

Management of Clients with Intestinal Disorders
NRS 108SPRING 2008
LOLA OYEDELE MSN,RN,CTNMAJUVY SULSE MSN, RN, CCRN

General Clinical Manifestations
Hemorrhage Pain Nausea and vomiting Distension Diarrhea Constipation Abnormalities in fecal content

Inflammatory Disorders
Infections and Infestations Viral and Bacterial Infections
Gastroenteritis Appendicitis Peritonitis Diverticulitis Parasitic infections Irritable bowel syndrome Crohn’s disease and ulcerative colitis

Gastroenteritis
Inflammation of the stomach and intestinal tract
Affects primarily the small bowel

Etiology and Risk Factors
Transmitted by the fecal oral route Person to person Ingestion of fecally contaminated food and
water Food is usually the vehicle for transmission Common bacteria sources of contaminated
food include eggs (salmonella), undercooked meat (E. Coli)

The incubation period for all viral and bacterial infections
Ranges from 6 hours to 3 – 4 days.
Gastroenteritis

Pathophysiology
Intestinal flora is disrupted by harmful bacteria and viruses or antibiotic therapy
Pathogens cause tissue damage and inflammation
Release of endotoxins causes greater secretion of water and electrolytes
Inhibition of Na absorption takes place caused by secretion of chloride and bicarbonates

In order to create a Na balance, large amounts of protein rich fluids are secreted in the bowel overwhelming the large bowel’s ability to reabsorb the fluid leading to diarrhea
Pathophysiology

Manifestations
Manifests as diarrhea abdominal pain cramping
Associated symptoms are nausea, vomiting, fever, anorexia, distension, tenesmus (straining on defecation) and hyperactive bowel sounds

Prognosis
Temporarily disabling and self limiting for 2-3 days Resolves in 1-5 days Can be fatal in debilitated, older or very young people Early detection and treatment with fluid and
electrolytes are critical in preventing death or disability
Clients with E. coli may end up with hemolytic uremic syndrome which causes death

Parasitic Infection (Helminths)
The intestinal tract may be infected with any of several helminths or parasitic worms e.g. roundworms, pinworms trichinella spiralis that causes trichinosis and species of tape worm.
Contracted through the skin or ingestion of contaminated food or water
May cause UTI or pruritus ani Susceptible to medications

Outcome management for viral bacterial and parasitic infections Rest the Bowel
NPO until vomiting stops
Decrease diarrhea Obtain stool specimen if unresolved for 2-
3days Anti-Infective agent Avoid meds. that will decrease intestinal
motility

Outcome Management for Viral Bacterial and Parasitic Infections Restore fluids and electrolytes
Small amount of clear liquid as tolerated Electrolyte beverage may be given Advance diet in 24hrs. as tolerated In severe fluid depletion start IV 0.45% NACL A potassium supplement may be ordered if K+
is low.

Nursing Management of the Medical Client Assess the stool for color, odor, consistency,
frequency and amount Assess bowel sounds, muscle weakness and fatigue Examine anal area for irritation, clean the area and
apply moisture barrier Administer anti-infective agent Replace fluid and electrolytes Provide discharge teaching

Appendicitis
An inflammation of the vermiform appendix Most common in adolescence Can occur at any age but rare in children
under 2 years Not common in older adults Rupture occurs mostly in older adults

Etiology and Risk Factors
Caused by a fecalith that occludes the lumen Kinking of the appendix Swelling of the bowel wall Fibrous conditions of the bowel wall External occlusion of the bowel by adhesions

Pathophysiology
Due to obstruction, the intraluminal pressure increases leading to decreased venous drainage, thrombosis, edema and bacterial invasion of the bowel wall
Following initial obstruction, the appendix becomes increasingly hyperemic, warm, and covered with exudates, progressing to gangrene and perforation

Clinical Manifestation
Vomiting which begins after the pain starts Loss of appetite Low grade fever Coated tongue Bad breath Elevated WBC (10 -15,000/mm3) Pain at McBurney’s point confirms diagnosis

APPENDICITIS
DESCRIPTION Inflammation of the
appendix When the appendix
becomes inflamed or infected, rupture may occur within a matter of hours, leading to peritonitis and sepsis
MCBURNEY’S POINT

Surgical Management
Appendectomy Done within 24 – 48hrs. Of onset of
manifestation Can be done through a small incision or a
laparoscope Delay will result in rupture of the appendix
leading to peritonitis

Complications and Outcomes
Bowel perforation Antibiotics and surgical drainage is the
treatment Peritonitis D/C within 24-48 hrs. Lifting is restricted for 2-4 weeks Resume all activities in 4-6 weeks

Nursing Management of the Surgical Client Assessment Pain management Fluid and electrolyte replacement Manage the risk for infection

Peritonitis
Inflammation of the peritoneal membrane
Causes sharp well localized pain

Etiology and Risk Factors
May be primary or secondary Sources include G.I., external environment
and blood stream Offending organism is E. Coli No none risk factors

Causes of Peritonitis
Ruptured or gangrenous gall bladder Perforated peptic ulcer Perforated stomach or intestine secondary to
cancer or inflammatory bowel disorder, bowel obstruction, penetrating wounds and acute pancreatitis
Early diagnosis is key

Pathophysiology
The inflammatory response diverts blood to the inflamed area of the bowel
Peristaltic activity of the bowel ceases Fluids and air are retained within the lumen
raising the pressure and increasing fluid secretion into the bowel
Circulating blood volume diminishes

The inflammatory process increases oxygen requirements
Difficulty in breathing results relative to abdominal pain and increased abdominal pressure
Pathophysiology

Clinical Manifestation
Varies according to the cause
Pain – localized or generalized increasing with pressure
Rigidity of the abdominal muscle
Nausea and vomiting
Low grade fever Absence of bowel
sounds Shallow respiration Increased WBC
(20,000mm3) X-ray shows edema and
dilation of the intestines

Outcome Management
Maintain fluid and electrolyte NGT IV fluid
Control infection IV ABT Surgical repair and drainage

Nursing Management
Obtain history Asses the abdomen for positive bowel
sounds, firmness, distension or rigidity IV antibiotics Surgical drainage and repair of perforation

Post Operative Care
Monitor for complications e.g. ARDS, sepsis and shock
Monitor fluid and electrolyte balance
Check vital signs, bowel sounds, urine output, skin tugor, mucus membrane and weight
Report manifestation of sepsis, oliguria, elevated temperature or drop in blood pressure
IV fluid and antibiotics Discharge teaching

Inflammatory Bowel Disease

Crohn’s disease
Chronic relapsing disease Develops discontinuously
(without sequence) in any part of the alimentary tract
Most common location is the terminal ileum
Involves the entire thickness of the bowel wall
Mortality rate is not high Recurrence and complications
can lead to disability More common in whites and
Ashkenazi Jews




Etiology and Risk Factors
The cause of Crohn’s disease is unclear There appears to be a genetic or heredity
predisposition Considered to be autoimmune disease There are no preventive measures for
Crohn’s disease Only risk is genetic

Pathophysiology of Crohn’s disease
Characterized by inflammation of segments of the digestive tract
Inflammation usually extends through all layers of the intestinal mucosa; this can lead to such complications as obstruction, tears, bleeding (anemia), and malnutrition
Consist of quiet (remission) and active (relapse) periods. In quiet periods, the patient is asymptomatic, in active periods, the patient experience symptoms
The cause is unclear although there appears to be a genetic or hereditary predisposition

Diagnosis
Thorough history and physical examination CBC Serum chemistry Stool for occult blood Barium studies Endoscopy with biopsy

Symptom’s of Crohn’s Disease
Stool may be foul smelling and fatty due to malabsorption (Steatorrhea)
Intermittent or chronic abdominal pain Diarrhea, may contain blood or mucous Stool is soft and semi solid Unexplained weight loss Anorexia, anemia Fatigue

Indications for Surgery
Fistula Abscess Obstruction Malignancy Bleeding

Ulcerative Colitis
A disease that spans the entire length of the colon
Involves only the sub mucosa and mucosa
Begins in the rectum and distal colon spreading upward to the sigmoid and descending colon
Causes inflammation, thickening, congestion, edema and minute lacerations that ooze blood

Develops into an abscess Bleeding from minor trauma More common than Crohn’s disease Occurs in all ages Higher incidence among young adults,
women and Jews Familial tendency
Ulcerative Colitis

Etiology and Risk Factors
Bacterial origin Allergic reaction Altered immune state Presence of antibodies in the colon Emotional disturbance can precipitate an
exacerbation or prolong an attack No preventable risk factors

Pathophysiology of Ulcerative Colitis
Appearance depends on the stage, activity and severity
Characterized by a crypt abscess (Inflammatory)
Secretions from crypt abscess result in purulent discharge from the bowel mucosa.
Abscess becomes necrotic and ulcerates
Inflammation reaction due to secondary infection leads to scarring, fibrosis, narrowing, thickening and shortening of the colon

Clinical Manifestation
Abdominal pain Diarrhea (20x/day) Fluid imbalance Weight loss Metabolic acidosis Rectal bleeding Tenesmus Bloody stool
Sense of urgency Cramping Colicky pain in the LLQ Nausea, vomiting,
anorexia Anemia Low potassium May recur with
emotional distress

Medical Management
Decrease diarrhea Replace fluid, electrolytes and blood as
needed Restrict physical activity during attack to
decrease intestinal motility Keep record of loose stool, consistency, color Bowel rest/parenteral hyper alimentation Restore immuno competence Correct nutritional deficiency Relieve bowel edema and inflammation

Pharmacological Agents
Antidiarrhea medications e.g. Imodium, Lomotil
Metamucil may improve consistency of stool and control incontinence
Aminosalicylates – inhibits prostaglandin synthesis e.g. Azulfidine, Mesalamine and Olsalazine
Anti infective agents – prevent or control infection
Corticosteroids – reduce body’s response to inflammation e.g. prednisone, hydrocortisone
Give folic acid supplement Immunosuppressive
agents Anticholinergics – relieve
abdominal cramp and control diarrhea

Nutritional Support
Increase nutritional intake Diet and supplement – High protein, high
calorie, low residue diet. TPN Avoid cocoa, chocolate, citrus fruit,
carbonated drinks, nuts, seeds, popcorn and alcohol

Nursing Management
Assessment Control diarrhea Altered nutrition Pain management Ineffective individual coping

Surgical Management
Surgery is the only cure Indicated when medical management fails Total Proctocolectomy
Permanent ileostomy is formed Ileorectal Anastomosis Continent ileostomy Surgical resection of the small bowel

Continent Ileostomy
Reservoir is constructed from a loop of colon Advantages
No need for external pouch Minimal skin problems No flatus or leakage of stool
Client drains the pouch several times a day using a catheter usually in response to a feeling of fullness

Contraindications
Crohn’s disease Malnutrition

Complications
Suture line leakage Peritonitis Fistula formation Obstruction by food residue

Outcomes
Resume activity in 4-6weeks Improved nutritional status Improved quality of life

Ileal Pouch-Anal Anastomosis
Preferred surgical procedure for clients with ulcerative colitis
Colon is removed Ileoanal reservoir is created Temporary loop ileostomy is formed Heals in 3-4 months Ileostomy is revised so that stool drains
into the reservoir

Contraindications Crohn’s disease Malnutrition
Complication Anastomotic leakage Pouchitis - inflammation of the pouch Bowel obstruction
Outcome Resume regular activities in 4 – 6 weeks Improved nutritional status Improved quality of life
Ileal Pouch-Anal Anastomosis

Surgical Resection of the Small Bowel Indication
Crohn’s disease to treat complications Contraindication
Malnutrition – give TPN Complications
Impaired absorption of vit.B12, glucose, fat and protein Loss of body protein or lean body mass Anemia Paralytic ileus

Outcome Return to regular activities and complete
wound healing Adequate nutritional in 4-6weeks after
surgery
Surgical Resection of the Small Bowel

Nursing Management
Assessment – Nutritional status and start TPN if needed
Pre – op. teaching visit from a member of the ostomy association Wear pouch for 1-2 days before surgery
Post – op teaching Monitor stoma Advance diet Monitor for complications

Critical Thinking
What are the signs of intestinal obstruction? Anorexia Abdominal cramps Absence of ileostomy drainage Foul brown watery discharge in the pouch Visible peristalsis

Risk for body image disturbance Confront the stoma Integrate function and appearance into their
body image Help client look at the stoma and touch it as
soon as possible Discuss clothing options Discourage wearing a tight waist band Verbalize feelings
NURSING DIAGNOSIS

Ineffective Management of Therapeutic Regimen Self care Stoma assessment Prevent skin irritation Reduce odor Discuss medications Emphasize fluid intake Prevent urolithiasis
Encourage follow up visits
Maintain ileal drainage Continent ileostomy:
Reservoir Catheterization
Continent ileostomy Explain dietary
recommendations

Risk for sexual dysfunction Verbalize concerns Empty pouch before intimacy Use different positions Pregnancy and vaginal delivery is possible
for clients with ileostomy
NURSING DIAGNOSIS

Self care Teach stoma care before discharge Join united ostomy association Know nearest ostomy supply center Visiting nurse or enterostomal therapy nurse
should visit the client at home to follow up on learning needs
Wear a medical alert identification bracelet
NURSING DIAGNOSIS

Colorectal Cancer
Etiology and Risk Factors Cause is unknown Related to low residue, high fat and highly refined
foods with inadequate intake of fruits and vegetables
Higher incidence in cities and industrialized countries
Genetic mutation in hereditary form of colon cancer Familial tendency Increased risk with age and ulcerative colitis or
familial polyps

Pathophysiology
Develops from adenomatous polyps Increases in size and invade bowel wall. Tumors in the right intestine tend to be bulky and
cause necrosis and ulceration Left tumors are small that cause ulceration of the
blood supply Spread by direct extension to nearby organs Lymphatic and hematogenous channels usually the
liver Seeding of cells into the peritoneal cavity

Clinical Manifestations
Rectal bleeding Change in bowel habits Abdominal pain Weight loss Anemia Anorexia

Prognosis
Depends on the health of the client Early diagnosis Effective treatment Early diagnosis and treatment are
essential for a good outcome

Outcome Management: Colorectal Cancer Medical Management
Decrease Tumor Growth, Chemotherapy, & Radiation
Surgical Management Colostomy Abdominal-Perineal Resection

Colostomy



Complications
Suture line leakage Peritonitis Hemorrhage Stomal necrosis Retraction Prolapse Stenosis

Outcome
Resume usual activities within 4 – 6 weeks Able to perform self care of the stoma Radiation and chemotherapy may be
continued if indicated

Outcome Management of Patient with Colorectal Cancer
Nursing Management Risk for Injury Risk for Ineffective Management of
Therapeutic Regimen: Ostomy Care, Irrigations, Minimizing Flatus

Nursing Management of the Surgical Client
Pre – Operative care History taking High calorie, protein, carbohydrate and low
residue diet TPN may be necessary Decrease risk of infection Treat anxiety if present Provide enterostomal education

Post Operative care Assessment Gastric suction Ensure patency of NGT Monitor colostomy output Assess stoma for signs of ischemia Assess incision site
Nursing Management of the Surgical Client

Risk for Injury
Monitor vital signs Advance diet Decrease cramping Apply rectal dressing Reduce pain Monitor stoma drainage Prevent thrombophlebitis

Risk for Body Image Disturbance
Provide emotional support and extensive teaching
Involve family and significant other in teaching

Risk for Ineffective Management of Therapeutic Regimen
Teach self care Teach client to empty pouch when it is about
½ full Teach stoma irrigation – done to regulate the
colostomy Minimize flatus

Herniations
Abnormal protrusion of an organ, tissue or part of an organ through the structure that normally contains it.
Occurs commonly in the abdomen

Etiology and Risk Factors
Occurs due to a defect in the integrity of the muscular wall
Increased intra – abdominal pressure. Obesity Heavy lifting and straining

Pathophysiology
Defects in muscular wall and increased intra abdominal pressure leads to herniation
Muscle weakness can be congenital, due to trauma or wide space at the inguinal ligament
Intra abdominal pressure increases with pregnancy, obesity, heavy lifting, coughing and trauma from blunt pressure

Types of Hernia
Reducible Irreducible or incarcerated Strangulated – surgical emergency

Classification
Indirect Inguinal hernia Direct Inguinal hernia Femoral hernia Umbilical hernia Incisional or ventral
hernia


Medical, Surgical, and Nursing Management Medical management
Reduction and truss Surgical management
Herniorrhaphy Nursing management
Check for voiding Return to general diet No lifting for 4-6weeks Apply ice pack to reduce pain and swelling

Diverticular Disease
Two diseases Diverticulitis
Blind out – pouching or herniation of intestinal mucosa through the muscular coat of the large intestine (sigmoid colon)
Diverticulosis The presence of non inflamed
diverticula

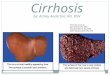
DIVERTICULA
From Ignatavicius, D. & Workman, M. (2002). Medical-surgical nursing: Critical thinking for collaborative care, ed 4, Philadelphia: W.B. Saunders.

COMPLICATIONS OF DIVERTICULITIS
From Beare PG, Myers JL. Adult Health Nursing, ed. 3, St. Louis, 1998, Mosby.

Etiology and Risk Factors
Low fiber diet Presence of muscle weakness Diverticulitis occurs when undigested food
blocks the diverticulum

Pathophysiology
Weak points in the muscle of bowel exist where branches of blood vessels penetrate the colon wall
These weak points create areas for bowel protrusion when there is increased intraluminal pressure
It frequently develops in the sigmoid colon May be acute or chronic

Clinical Manifestations
Discomfort – dull, episodic or steady, left quadrant or mid abdominal pain
Alteration in bowel habits Increased flatus Anorexia Low grade fever Rectal bleeding Stool may contain mucus Tender mass on digital rectal exam

Outcome Management
Medical and Nursing Management Diet modification Increase fiber and prevent constipation Notify physician of change in bowel
habit Rest the colon Antibiotic therapy

Surgical Management Indicated when there is bleeding,
obstruction, abscess and perforation Colon resection with colostomy
Outcome Management

Obstructions
Partial or complete impairment of the forward flow of intestinal content

Etiology and Risk Factors:
Inflammation, Neoplasm, Adhesions, Hernia, Volvulus, Intussusception Food blockage
Compression from outside the intestine,
Paralytic ileus, Vascular problems such
as mesenteric embolus and thrombus,
Hypokalaemia may result in obstruction

Other Causes
Diverticulitis Ulcerative colitis Previous abdominal surgery

Causes of Intestinal Obstruction
Mechanical – Adhesions, hernias, Volvulus, Intussusceptions, cancers
Neurogenic – paralytic ileus Vascular
Interruption of blood flow Obstruction of blood flow Complete occlusion Partial occlusion

Clinical Manifestations
Vomiting Abdominal pain Visible peristalsis Toxemia High pitched tinkling
sound Hypoxia
Peritonitis Vomit may contain dark
fecal material (Small bowel)
Dehydration Metabolic acidosis

Diagnosis
X – ray shows gas shadows Barium or radiopaque studies CBC Leukocytosis ( Bowel Strangulation)

Outcome Management: Bowel Obstruction Medical
Decompress the bowel
NGT Nursing
Management Assessment Replace fluid and
electrolyte
Decompress the bowel Discharge teaching
Surgical Management Bowel resection Colostomy Bypass procedure

Irritable Bowel Syndrome
A functional disorder of motility of the intestine
Also called spastic colon or irritable colon

Etiology and Risk Factors
High fat diet High intake of fresh fruits, gas producing
foods, carbonated beverage and alcohol Smoking Lactose intolerance High stress Alteration in sleep and rest

Pathophysiology
A disorder of GI motility Motility may be altered by any number of
factors including diet and emotions. The alteration in motility can cause diarrhea,
constipation or alternating diarrhea and constipation

Clinical Manifestation
Abdominal pain Altered bowel function Constipation or diarrhea Hyper secretion of colon
mucus Flatulence Nausea Anorexia
Anxiety or depression Fiber, fruits, alcohol and
fatigue may aggravate or precipitate manifestation
Stool with mucus Foul breath Diagnosis is made by
excluding other diseases

Outcome Management:
Medical and Nursing Management Modify Diet – Increase bulk Modify Lifestyle – reduce stress Administer Medications – sedatives and
antispasmodic Alternative Treatments Provide empathy and support

Hemorrhoids
Perineal varicose veins May be external or
internal

Etiology and Risk Factors
Caused by Increased intra abdominal pressure
Pregnancy Constipation with prolonged straining Obesity CHF Prolonged sitting or standing Cirrhosis with portal hypertension

Pathophysiology
Tenesmus increases intra abdominal and hemorrhoidal veins pressure leading to distension of the veins
When the rectal pouch is filled with formed stool, venous obstruction occurs
The repeated and prolonged increase in this pressure and obstruction causes the hemorrhoidal veins to become permanently dilated.
As a result, thrombosis and bleeding may occur

Clinical Manifestations
Enlarged mass at the anus Bleeding and prolapse Rectal itching and constipation Pain Bright red blood in the stool

Outcome Management: Hemorrhoids Surgical Management
Sclerotherapy & Ligation
Cryosurgery & Laser Hemorrhoidectomy
Nursing Management Promote Healing,
Prevent Complications, & Relieve Pain
Medical Management Prevent complications Relieve pain

Complications
Bleeding Thrombosis Hemorrhoidal strangulation Iron deficiency anemia Severe pain, extreme edema and
inflammation when strangulated