Embed Size (px)
Citation preview

Susan England, MSN , RNLloyd Preston, MSN, RN APRN-BC
Riza Mauricio, MSN, RN,CCRN, CPNP-ACJennifer McWha, MSN, RN

A 20 year old white male presented to the EC unconscious 5 minutes after missing the pole vault pit and landing with the occipital region of his head hitting the ground.
Neurologic evaluation on admission as follows: patient’s eyes opened to the sound of his name, and when asked where he was, the patient responded with “my shoes to change.” The patient moved all of his fingers and toes when prompted.
What is this patient’s score on the Glasgow Coma Scale?

Developed by neurosurgeons in 1974 Quantifies level of consciousness
◦ Acute brain damage: traumatic and/or vascular injuries or infections
◦ Metabolic disorders: hepatic or renal failure, hypoglycemia, diabetic ketosis, toxic ingestion
Assess initial level of consciousness Assess changes in level of consciousness Helps guide treatment and predict outcome

Category Response Points
Eye opening
Spontaneous, open with blinking at baseline 4
Opens to verbal command, speech, or shout 3
Opens to pain, not applied to face 2
No response 1
Verbal response
Oriented conversation 5
Disoriented, confused conversation, able to answer questions 4
Inappropriate responses, words discernible 3
Incomprehensible speech 2
No response 1
Intubated 1T
Motor response
Obeys commands for movement 6
Purposeful movement to painful stimulus 5
Withdraws from pain 4
Abnormal (spastic) flexion, decorticate posture 3
Extensor (rigid) response, decerebrate posture 2
No response 1

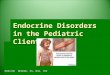
Decorticate◦ Upper extremity flexion with lower extremity extension◦ Mesencephalic region or corticospinal tract damage
Decerebrate◦ Upper and lower extremity extension◦ Brainstem damage below the red nucleus
Progressive◦ Uncal or tonsilar herniation


Eye opening◦ Name spoken loudly
Verbal response◦ Person, place, time
Motor response◦ Fingernail bed pressure◦ Supraorbital pressure
Hand crosses midline and above clavicle
◦ Sternal rub

Score range◦ Extubated: 3 – 15◦ Intubated: 3 –
11T Clinical presentation
◦ Normal: GCS =15
◦ Comatose: GCS ≤ 8◦ Dead: GCS = 3
Grading of head injury◦ Minor: GCS ≥13◦ Moderate: GCS 9
-12 ◦ Severe: GCS ≤ 8
Example report◦ GCS 9 = E2 V4 M3 at
07:35

Highest score observed during
1st 24 hours after
injury
Good recovery or
Moderate disability
Vegetative or Dead
3-4 7% 87%
5-7 34% 53%
8-10 68% 27%
11-15 82% 12%

Past medical history◦ Age, previous neurological problems
Injury◦ Type and location, depth, duration of coma, presence of
low blood pressure, oxygen levels after the injury
Current findings ◦ Physical examinations, radiological studies of
the brain

The patient’s eyes initially closed, opened to the sound of his name. ◦ Eye opening◦ 3
When asked where he was, the patient said “my shoes to change.” ◦ Verbal response◦ 3
The patient moved all of his fingers and toes when prompted.◦ Motor response◦ 6

◦ SCORE
◦ GCS 12 = E3 V3 M6 at 16:34
Head injury severity
◦ Moderate

Numerous researchers have investigated the use of the GCS score in predicting outcomes in head injury patients.
Cumulative findings: GCS scores are most accurate at predicting outcome in head-injured patients when they are combined with patient age and pupillary response and when broad outcome categories are used.
Knowledge of potential outcomes for head-injured patients based on these early GCS scores is valuable for nurses and other healthcare professionals who care for and support these patients and their loved ones throughout the recovery process.
J Neurosci Nurs 20

Greenberg,M. (2006). Coma: Handbook of Neurosurgery, (154-160) New York, NY:Thieme. ISBN 1-588890 457 1).
McNett, M. (2007). A Review of the Predictive Ability of Glasgow Coma Scale Scores in Head-Injured Patients. The Journal of Neuroscience Nursing,392(2),68-75.
Weir, C.J., Bradford, A.P., and Lees, K.R. (2003). The Prognostic values of the components of Glasgow Coma Scale following acute stroke. QJMedicine: An International Journal of Medicine, 96, 67-74.