Embed Size (px)
Citation preview

KBK Psikologi Klinis 14 Februari 2014Henny Wirawan



* Going for a walk in a Thunderstorm.
* Checking the door is locked three times before leaving the house.
* Having five baths every day.
* Betting Rp. 5,000,000 on a horse.

* Having hair dyed pink with green stripes.
* Getting pregnant without being married.
* Being scared of spiders.
* Getting anxious before an examination.
* Writing an extra statement because 13 is an unlucky number.
* Living in isolation without interacting with people.

*Defining a person or behavior as ‘abnormal’ implies something undesirable and requiring change
*Therefore, we must be careful how we use the term
*Psychologists need methods for distinguishing ‘normal’ from ‘abnormal’
www.
psyc
hlot
ron.
org.
uk

*Four definitions of abnormality are:
*Deviation from social norms
*Statistical infrequency
*Failure to function adequately
*Deviation from ideal mental health
www.
psyc
hlot
ron.
org.
uk

There is a difficulty in distinguishing normal from abnormal behavior.
The following are the definitions:Deviation from the averageDeviation from the idealAbnormality as a sense of subjective discomfortAbnormality as the inability to function effectively
Legal definitions of abnormality

*Social norms are a set of rules for behaviour based on a set of moral and conventional standards within society.
*They are judged by the dominant culture

* John Maguire and Laurence Scott-Mackay were the first couple to exchange vows in a civil partnership ceremony in Scotland, with a ceremony in Edinburgh






*social norms vary from one time to another
On 25 May 1895 Wilde was convicted of gross indecencyand sentenced to two years' hard labour.
Wilde and Lord Alfred Douglas in 1893

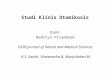
*Under this definition, a person’s trait, thinking or behaviour is classified as abnormal if it is rare or statistically unusual.
*With this definition it is necessary to be clear about how rare a trait or behaviour needs to be before we class it as abnormal
www.
psyc
hlot
ron.
org.
uk

freq
uenc
y
70 100 130
IQ Scores
Average IQ in the population is 100pts. The further from 100
you look, the fewer people you find ww
w.ps
ychl
otro
n.or
g.uk

freq
uenc
y
70 100 130
IQ Scores
A very small subset of the population (<2.2%) have an IQ below 70pts. Such people are statistically rare. We regard them as having abnormally low IQs
www.
psyc
hlot
ron.
org.
uk

20
A very unusual behaviour or trait will be more than 2 standard deviations from the mean. i.e. over 130 or under 70 IQ score.
This statistically ‘rare’ behaviour or trait is likely to be seen as being abnormal.
L2

*From an individual’s point of view abnormality can be judged in terms of not being able to cope with day to day living.

*Under this definition, a person is considered abnormal if they are unable to cope with the demands of everyday life.
*They may be unable to perform the behaviours necessary for day-to-day living e.g. self-care, hold down a job, interact meaningfully with others, make themselves understood etc.
www.
psyc
hlot
ron.
org.
uk


*This definition may be biased by who judges ‘failure to function adequately’ as in the opinion of the individual they may believe that they are functioning adequately even if others do not agree.


*http://nobelprize.org/nobel_prizes/economics/laureates/1994/nash-autobio.html


*Rosenhan & Seligman (1989) suggest the following characteristics:
*Suffering
*Maladaptiveness (danger to self)
*Vividness & unconventionality (stands out)
*Unpredictability & loss of control
*Irrationality/incomprehensibility
*Causes observer discomfort
*Violates moral/social standards
www.
psyc
hlot
ron.
org.
uk

*Suffering
*Maladaptiveness (danger to self)
*Vividness & unconventionality (stands out)
*Unpredictability & loss of control
*Irrationality/incomprehensibility
*Causes observer discomfort
*Violates moral/social standards

*Under this definition, rather than defining what is abnormal, we define what is normal/ideal and anything that deviates from this is regarded as abnormal
*This requires us to decide on the characteristics we consider necessary to mental health
www.
psyc
hlot
ron.
org.
uk

Jahoda states that we identified 6 categories that people need in order to be MENTALLY HEALTHY
*1/ Self attitudes = high self esteem
*2/ Personal growth (Self actualization) = achieve their full potential
*3/ Integration = being able to cope with stressful situations
*4/ Autonomy = making own decisions, being in control
*5/ Accurate perception of reality
*6/ Adaptation to environment = ability to love and solve problems

*Psychologists vary, but usual characteristics include:
*Positive view of the self
*Capability for growth and development
*Autonomy and independence
*Accurate perception of reality
*Positive friendships and relationships
*Environmental mastery – able to meet the varying demands of day-to-day situations
www.
psyc
hlot
ron.
org.
uk

*Marie Jahoda (1958) states that we define physical illness by looking at what is different from ideal physical health. I.e. correct temperature, correct blood pressure
*SO WHY NOT DO THE SAME FOR MENTAL ILLNESS
*SEE IT AS A DOCTOR APPROACH TO DEFINING ABNORMALITY!

Mental illness is a complex area, difficult to define, and definitions of normal and abnormal behavior vary over time, from society to society, and in different contexts.

• Are you always worrying?
• Are you unable to concentrate because of unrecognized reasons?
• Are you continually unhappy without justified causes?
• Do you loose your temper easily and often?
• Do you have wide fluctuations in your mood from depression to elation, back to depression, which incapacitate you?

* Do you continually dislike to be with people?
* Are you upset if the routine of your life is disturbed?
* Do your children/parents consistently get on your nerves?
* Are you ‘browned off’and constantly bitter?
* Are you afraid without real cause?

*Are you always right and the other person is always wrong?
*Do you have numerous aches and pains for which no doctor can find a physical cause?
*if the answer is definitely ‘yes’ for any one question it indicates poor mental health)

GRADATIONS OF ABNORMAL AND NORMAL BEHAVIOUR:
DRAWING THE LINE ON ABNORMALITY
*It is better to view abnormal and normal behavior as marking two ends of a continuum rather than as absolute state.
*As such behavior should be evaluated in terms of gradations, ranging from completely normal functioning to extreme abnormal behavior. Obviously, behavior typically falls somewhere between the two extremes.

MODELS OF ABNORMALITY: From Superstition to Science
*For much of the past, abnormal behavior was linked to superstition and witchcraft.
*People displaying abnormal behavior were accused of being possessed by the devil or some sort of demonic god.
*This typically involved whipping, immersion in hot water, starvation, or other forms of torture in which the cure was often worse than affliction.

Contemporary approaches take a more enlightened view, and six major perspectives on abnormal behavior predominate.
They are:
*the Medical Model
*the Psychoanalytic Model
*the Behavioral Model
*the Cognitive Model
*the Humanistic Model
*the Socio-cultural Model

MODELS OF PSYCHOLOGICAL DISORDERS*Medical model – Suggests that physiological causes are
at the root of abnormal behavior ( for ex. a brain tumor or chemical imbalance in the brain or disease)*Psychoanalytic Model – Abnormal behavior stems from
childhood conflicts over opposing wishes regarding sex and aggression.*Behavioral Model – Abnormal behavior is a learned
response – Its emphasis is on here and now.
Both Medical and Psychoanalytic Models look at abnormal behavior as symptoms of some underlying problem.

* Cognitive Model – The model suggests that people’s thoughts and beliefs are central to abnormal behavior. ( the primary goal of treatment using the cognitive model is to explicitly teach new and more adaptive ways of thinking)
* Humanistic Model – It suggests that individuals can, by and large, set their own limits of what is acceptable behavior.
It focuses on the relationship of the individual to society, considering the ways in which people view themselves in relation to others and see their place in the society.

•Socio-cultural Model – The model suggests that people’s behavior – both normal and abnormal – is shaped by family, society and cultural influences.
Social phenomena such as homelessness have been associated with psychological disorders – People from lower classes may be less likely than those from higher classes to seek help until their symptoms become relatively severe and warrant a more serious diagnosis


ABNORMAL BEHAVIOUR
*‘Abnormal’ literally means ‘away from the normal’. It implies deviation from some clearly defined norm.
*In the case of physical illness, the norm is the structural and functional integrity of the body.
*The concepts of ‘normal’ and ‘abnormal’ are meaningful only with reference to a given culture.
*Normal behavior conforms to social expectations where abnormal behavior does not.

NORMAL AND ABNORMAL
I) Psychiatric signs and symptoms are patterns of disturbed human behavior.
Such patterns are also labeled with such terms ‘maladaptive’, ‘disordered’, ‘deviant’, ‘inappropriate’ and ‘abnormal’.
II) Although grossly deviant behavior patterns are readily recognized as abnormal, the distinction between ‘normal’ and ‘abnormal’ can be difficult.
III) A rough definition is ‘Behavior is abnormal if it causes trouble either for the patient or for others’.
Behavior may cause trouble because of its intensity, its frequency, its lack of appropriateness to a given situation.

MENTAL DISORDERS
The term ‘mental’ springs from a dualistic interpretation of human behavior
The dualistic interpretation holds that the human organism consists of two separate components:
*The body or soma
*The mind or psycheThese two components have impact upon one another –
they are viewed as essentially separate.
MENTAL DISORDERS ARE SIMPLY DISTURBANCES OF BEHAVIOUR

POPULAR MISCONCEPTIONSMental Disorders have been generally characterized by superstition, ignorance and fear.Although successive advances in the scientific understanding of abnormal behavior have dispelled many false ideas, there remain a number of popular misconceptions. They are*The belief that abnormal behavior is always bizarre.*The idea that ‘normal’ and ‘abnormal’ are sharply
differentiated.*The view of mental disorders as a hereditary stigma.*The view of genius as ‘akin to insanity’
*The view of mentally ill persons as incurable and dangerous.*The belief that mental disorder is a disgrace.*An exaggerated fear of one’s own susceptibility to
mental disorder.

General reaction of public to mentally ill persons
The following emotional reactions which directly or indirectly determine our approach to mentally ill are*Fear and suspicion…..that the mentally ill person may be harmful.*Disgust and Dislike….because the mentally ill person is not clean*Anger and Rejection…..because the mentally ill person annoys others.*Sympathy and Pity*Amusement and laughter*Distrust*Indifference

CAUSES OF MENTAL ILLNESSES
Mental illnesses are caused by variety of factors viz.
*Changes in the structure and functioning of the brain.
*Heredity factors.
*Childhood experiences.
*Home/family atmosphere
*Other factors viz. Bad peer-group influence, unemployment, poverty, insecurity, exposure to stressful situations etc.

*Provides a common understanding of a condition and how it is commonly treated
*Aids in treatment planning and medical management
*Aids in patient education
*Fundamental to medical record keeping
*Facilitates data collection, retrieval, and analysis
*Necessary for reimbursement

*DSM-IV published in 1994 was the last major revision of the DSM.
*the culmination of a six-year effort that involved over 1000 individuals and numerous professional organizations.
*Much of the effort involved conducting a comprehensive review of the literature to establish a firm empirical basis for making modifications.
*Numerous changes were made to the classification (i.e., disorders were added, deleted, and reorganized), to the diagnostic criteria sets, and to the descriptive text based on a careful consideration of the available research about the various mental disorders.

*In anticipation of the fact that the next major revision of the DSM (i.e., DSM-V) will not appear until 2010 or later (i.e., at least 16 years after DSM-IV), a text revision of the DSM-IV called DSM-IV-TR was published in July 2000.
*The primary goal of the DSM-IV-TR was to maintain the currency of the DSM-IV text, which reflected the empirical literature up to 1992. Thus, most of the major changes in DSM-IV-TR were confined to the descriptive text. Changes were made to a handful of criteria sets in order to correct errors identified in DSM-IV. In addition, some of the diagnostic codes were changed to reflect updates to the ICD-9-CM coding system adopted by the US Government.

*
*Subtypes define mutually exclusive and jointly exhaustive phenomenological subgroupings within a diagnosis
*Specifiers are not intended to be mutually exclusive or jointly exhaustive
*Both subtypes and specifiers increase specificity in diagnosis

*Mild, Moderate, Severe
*Partial Remission, Full Remission
*PriorHistory, Recurrence
*Principal Diagnosis, Reason for Visit
*Provisional Diagnosis
*Disorder–Not Otherwise Specified

*DiagnosticFeatures
*Subtypesand/orSpecifiers
*Associated Features and Disorders – Associated descriptive features and mental disorders
*Associated laboratory findings
*Associated physical examination findings and general medical condition

*Specific Culture, Age, and Gender Features
*Prevalence
*Course
*Familial Pattern
*Differential Diagnosis

*Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence
*Delirium, Dementia, and Amnestic and Other Cognitive Disorders
*Mental Disorders Due to aGeneral Medical Condition
*Substance-Related Disorders
*Schizophrenia and other psychotic disorders

*Mood Disorders
*Anxiety Disorders
*Somatoform Disorders
*Factitious Disorders
*Dissociative Disorders
*Sexual and Gender Identity Disorders
*Eating Disorders

*Sleep Disorders
*Impulse-Control Disorders Not Elsewhere Classified
*Adjustment Disorders
*Personality Disorders
*Additionally, there is a section on other conditions that may be a focus of clinical attention

*AXIS I: Clinical Disorders, Other Conditions that my be a focus of attention
*AXIS II: Personality Disorders, Mental Retardation
*AXIS III: General Medical Conditions
*AXIS IV: Psychosocial/Environmental Problems
*AXIS V: Global Assessment of Functioning/Children’s Global Assessment of Functioning

*Adult GAF
*Children’s Global Assessment Scale (CGAS)– For ages 4-16
*GAF and CGAS both assign a specific numerical rating of the person’s overall functioning
*Scales are in 10 point increments with a general description of the level of functioning within the range

*Assigns a numerical rating on a scale from 0-100
*Evaluator to use clinical judgment based upon his/her total experience with the population
*Consider psychological, social, and occupational functioning on a hypothetical continuum of mental health-illness
*GAF/CGAF used to track clinical progress over time

*For adults, a GAF score of 50 or less along with a qualifying SMI diagnosis triggers an SMI Determination.
*(See SMI Determination Addendum of the Assessment)

Mental Retardation (Axis II) 1-2 % of the Population Significantly Below Average Intellectual
Functioning Intellectual Quotient (IQ) below 70 on
standardized testing WISC-R, WAIS III, WPPSI, Stanford-Binet Concurrent Deficits or Impairments in
Adaptive Functioning Communication, Self-care, Home Living, Social
Interpersonal Skills, Use of Community Resources, Self Direction, Functional Academic Skills, Work, Leisure, Health and Safety
Onset Before Age 18 years

*INTELLECTUAL FUNCTIONING
*Borderline Intellectual Functioning – IQ ~70-85
*Normal Intelligence – IQ ~85-115
*Superior intelligence – IQ ~115 or Higher

MENTAL RETARDATION Mild Mental Retardation
IQ~55-69 85% of MR cases
Moderate Mental Retardation IQ~40-55 10% of MR cases
Severe Mental Retardation IQ~25-40 <5% of MR cases
Profound Mental Retardation IQ~25or Below <3% of MR cases

*Reading Disorder
*Mathematics Disorder
*Disorder of Written Expression
*Learning Disorder NOS

*Developmental Coordination Disorder

*Expressive Language Disorder
*Mixed Receptive-Expressive
*Language Disorder
*Phonological Disorder
*Stuttering

Delays or abnormal functioning in: Social Interactions Communication Restrictive Repetitive and Stereotyped
Patterns of Behavior, Interests and Activities
Autistic Disorder Rett’s Disorder Childhood Disintegrative Disorder Asperger’s Disorder Pervasive Developmental Disorder NOS

*DISTINGUISHING ASPERGER’S SYNDROME FROM AUTISM
*Autistic Disorder and Asperger’s Syndrome:
*10-15 / 10,000 population
*Early cognitive and language skills not delayed
*Evidence of disorder has later onset
*Greater motivation for engaging others, but done in an eccentric, one-sided, insensitive manner

*Attention-Deficit/Hyperactivity Disorder
*Attention-Deficit/Hyperactivity Disorder NOS
*Conduct Disorder
*Oppositional Defiant Disorder
*Disruptive Behavior Disorder

*ATTENTION-DEFICIT / HYPERACTIVITY DISORDER
*3–10%ofPopulation
*3:1 Male to Female Ratio
*Clinical Management: Combination of Somatic (Medication) Therapy and Behavioral Management

*DISRUPTIVE BEHAVIOR DISORDERS
*Conduct Disorders: *Repetitive and Persistent Pattern of
Behavior That Violate Rights of Others or Age-Appropriate Social Norms * Aggression to People and Animals
* Destruction of Property
* Deceitfulness and Theft
* Serious Violations of Rules
*10 % of Boys, 2 % of Girls: Often Develops into Adult Antisocial Personality

*Oppositional Defiant Disorder:
*Persistent and Totally Negative, Hostile, and Defiant Behavior

*DELIRIUM
*Disturbance of Consciousness
*Change in Cognition
*Develops Over a Short Period of Time
*Fluctuates
*Look For Underlying Medical Causes

*DELIRIUM, due to…
*Substance Intoxication Delirium
*Substance Withdrawal Delirium
*Delirium Due to Multiple Etiologies
*Delirium NOS

DEMENTIA Alzheimer’s Dementia: Risks: Up to 50 % of First-Degree Relatives by Age 90 Years
Memory Impairment Cognitive Disturbances
Aphasia, Apraxia, Agnosia Executive Functioning: Planning,
Organizing, Sequencing, Gradual Onset and Continuing Cognitive
Decline Pre-Senile (<65 yo) or Senile (>65 yo)
Onset

*Vascular Dementia: Multi-Infarct Dementia
*Dementia Due to General Medical Conditions:
*HIV Infection
*Head Injury
*Parkinson’s, Huntington’s, Pick’s, Creutzfeld- Jacob’s Disease
*Brain Tumors, Hydrocephalus
*Substance-Induced Persisting Dementias

*AMNESTIC DISORDERS
*Amnestic Disorder Due to . . .
*Substance-Induced Persisting Amnestic Disorder• Amnestic Disorder NOS

Substance Dependence: Tolerance Develops Characteristic Withdrawal Syndromes Taking Substance in Larger Amounts or
Over Longer Time Than Intended Persistent Desire or Unsuccessful Efforts
to Cut Down or Control Use Spending a Great Deal of Time
Obtaining/Using/Recovering Use Despite Knowledge of
Persistent/Recurrent Physical /Psychological Problems

*Substance Abuse:
*Maladaptive Pattern of Substance use:
* Recurrent Use Results in Failure in Role Obligations (Work/School/Home)
*Use in Hazardous Situations: Driving Under Influence
*Recurrent use-Related Legal Problems (Arrests/Assaults/ Disorderly Conduct)
*Continued Use Despite Persistent/Recurrent Social/Interpersonal Problems

*Multitude of Classifications:
*See pages 16 – 19 of DSM-IV-TR Classification
*Over 100 pages in DSM-IV-TR are substance- related disorder descriptions
*Specific presentation is related to drug(s) of abuse
*Use Core Assessment Substance Abuse section, pages to assist in classification

*• Schizophrenia:– 1 % of Population– Peak Onset: Late Teens, Early 20’s

*Characteristic Symptoms:
*Delusions
*Hallucinations
*Disorganized Speech
*Grossly disorganized or Catatonic Behavior
*Negative Symptoms: Flat/Blunted Affect, Alogia, Avolition, Apathy, Anhedonia

*Social/Occupational Dysfunction:
*Markedly Below Pre-Morbid Functioning in:
*School or Work
* Interpersonal Relationships
* Self Care
*• Duration: Continuous Signs Persist >6 Months

*Subtypes:
*Paranoid Type
*Disorganized type
*Catatonic Type
*Undifferentiated
*Residual Type

*PARANOID TYPE
*Preoccupation with One or More Delusions or Frequent Auditory Hallucinations
*None of the following is Prominent:
*Disorganized Speech, Disorganized or Catatonic Behavior, or Flat or Inappropriate Affect

*DISORGANIZED TYPE
*All of the Following are Prominent:
*Disorganized Speech
*Disorganized Behavior
*Flat of Inappropriate Affect
*The Criteria Are Not Met for Catatonic Type

CATATONIC TYPE The Clinical Picture Is Dominated by at Least Two
of the Following: Motoric Immobility as Evidenced by Catalepsy or
Stupor Excessive Motor Activity Extreme Negativism (Apparently Motiveless
Resistance to All instructions or Maintenance of a Rigid Posture Against Attempts to Be Moved) and Mutism
Peculiarities of Voluntary Movement as Evidenced by Posturing (Inappropriate or Bizarre Postures), Stereotyped Movements, Prominent Mannerisms, or Prominent Grimacing
Echolalia or Echopraxia

*UNDIFFERENTIATED TYPE
*A Type of Schizophrenia in Which Symptoms That Meet Criterion A Are Present,but The Criteria Are Not Met for The Paranoid, Disorganized, or Catatonic Type

*RESIDUAL TYPE
*Absence of ProminentDelusions, Hallucinations, Disorganized Speech, and Grossly Disorganized or Catatonic Behavior
*Continuing Evidence of a Disturbance, as Indicated by The Presence of Negative Symptoms or 2 or More Symptoms Listed in Criterion A for Schizophrenia

*SCHIZOPHRENIFORM DISORDER
*Criteria for Schizophrenia Are Met An Episode of the Disorder Lasts at Least 1 Month but Less Than 6 Months
*Good Prognostic Features:
*Onset of Psychotic Symptoms Within 4 Weeks of 1st Notable Change in Usual Behavior or Function
*Confusion or Perplexity
*Good Pre-morbid Social and Occupational Functioning
*Absence of Blunted or Flat Affect

*SCHIZOAFFECTIVE DISORDER
*During the Same Period of Illness, There Have Been Delusions or Hallucinations for At Least 2 Weeks in the Absence of Prominent Mood Symptoms
*Symptoms of a Mood Episode are Present for a Substantial Portion of the Total Duration of illness

*DELUSIONAL DISORDERS
*Non-bizarre Delusions of at Least 1 Month Duration
*Criterion for Schizophrenia Has Never Been Met
*Apart From the Impact of Delusion(s), Functioning is Not Markedly Impaired/Behavior is Not Obviously Odd or Bizarre
*Concurrent Mood Symptoms are Relatively Brief in Duration

*Erotomanic Type
*Delusions That Another Person, Usually of Higher Status, Is In Love With The Individual
*Grandiose Type
*Delusions of Inflated Worth, Power, Knowledge, Identity, or Special Relationship to a Deity or Famous Person

*Jealous Type
*Delusions That The Individual’s Sexual Partner Is Unfaithful
*PersecutoryType
*Delusions That The Peron (Or Someone Close) Is Being Malevolently Treated In Some Way
*SomaticType
*Delusions That The Person Has Some Physical Defect or General Medical Condition

*BRIEF PSYCHOTIC DISORDER
*Presence of One or More of the Following
*Delusions
*Hallucinations
*Disorganized Speech
*Grossly disorganized or Catatonic Behavior
*Duration of an Episode of the Disturbance is at least 1 day but less that 1Month, and full return to Pre- morbid Functioning

*SHARED PSYCHOTIC DISORDER
*A Delusion Develops In An Individual In The Context of a Close Relationship With Another Person(s), Who Has An Already Established Delusion
*The Delusion Is Similar In Content To That of The Person Who Already Has The Established Delusion

*Depressive disorders
*4.3 % of Population At Any Given Time
*8 – 20% Lifetime Prevalence
*2:1FemaletoMale
*Bipolar Disorder:
*O.5 – 1 % Lifetime Prevalence
*3:2 Female to Male
*Dysthymic Disorder
*3 % Lifetime Prevalence

*RED FLAGS: SUICIDE
*10-15 % of All Hospitalized with Depression
*10-15 % of Persons with Bipolar Disorder
*Epidemic of Suicide Among Adolescents and the Elderly
*Highest Risks for Those With Prior History Of Suicide Attempt; Family History of Suicide; Divorced, Widowed, Separated, or Living Alone; and Currently Abusing Substances

*DEPRESSIVE DISORDERS
*Major Depressive Disorder
*Single episode
*Recurrent
*Dysthymic Disorder
*Depressive Disorder NOS
*

*MAJOR DEPRESSION SYMPTOMS
*Depressed Mood Most of the Day, Nearly Every Day
*For a Child – Can Be Irritable Mood
*Markedly Diminished Interest or Pleasure in All, or Almost All, Activities Most of the Day, Nearly Every Day
*Significant Weight Loss or Weight Gain (5% or more of Body Weight), or Decrease or Increase In Appetite

*Insomnia or Hypersomnia
*Psychomotor Agitation or Retardation
*Fatigue or Loss of Energy
*• Feelings of Guilt or Worthlessness or Excessive or Inappropriate Guilt (Delusional Guilt)

*Diminished Ability to Think or Concentrate, or Indecisiveness
*Recurrent Thoughts of Death, Recurrent Suicidal Ideation Without a Specific Plan, or a Suicide Attempt, or a Specific Plan for Committing Suicide
*Symptoms Cause Significant Distress or Impairment In Functioning

*ManicEpisode:
*Distinct Period of Abnormally and Persistently Elevated , Expansive, or Irritable Mood, Lasting At Least 1 Week
*During the Period, 3 or More Are Present:
* Inflated Self-esteem or Grandiosity
*Decreased Need for Sleep (Feels Rested After Only 3 Hrs.)
*Hyper-talkative or Pressured Speech

*Flight of Ideas or Subjective Experience of Racing Thoughts
*Distractibility
*Increase in Goal-Directed Activities
*Excessive Involvement in Pleasurable Activities That Have a High Potential for Painful Consequences (Spending Sprees, Sexual Indiscretions, Foolish Business Investments)

*Manic episodes:
*Mood Disturbance Is Sufficiently Severe to Cause Marked impairment in Occupational Functioning or in Usual Social Activities or Relationships with Others, or to Necessitate Hospitalization to Prevent Harm to Self or Others or There Are Psychotic Features.

*PSYCHOTIC FEATURES MIXED EPISODE
*Criteria Are Met for Both a Manic Episode and for a Major Depressive Episode Nearly Every Day During At Least 1 week
*Mood disturbance Is Sufficiently Severe to Cause Marked Impairment

*MAJOR DEPRESSIVE DISORDER
*Single Episode or Recurrent
*With or Without Psychotic Features
*With Catatonic Features
*With Melancholic Features
*With Atypical Features
*With Postpartum Onset

*DYSTHYMIC DISORDER
*Depressed Mood for Most of the Day, for More days Than Not, for At Least 2 Years
*What is the difference between Major Depression and Dysthymic Disorder?

*BIPOLAR DISORDERS
*Bipolar I Disorder:
*Must have had at least One Episode of illness meeting the full criteria for Mania
*Bipolar II Disorder:
*Never has had a Manic Episode
*May have had episode of Hypomania
*• Bipolar Disorder NOS

*CYCLOTHYMIC DISORDER
*For at least 2 Yrs, the presence of numerous periods with Hypomania and Depression
*During the 2 Yr Period, the person has not been without symptoms for more than 2 months
*No episodes of Major Depression, Mania, or Mixed Episodes

*ANXIETY DISORDERS
*Panic Disorder
*Agoraphobia
*Specific Phobia
*Social Phobia
*Obsessive-Compulsive Disorder
*Posttraumatic Stress Disorder
*Generalized Anxiety Disorder

*PANIC ATTACKS/DISORDER
*Discrete Periods of the following: *Palpitations
*Sweating
*Trembling or Shaking
*Sensation of Shortness of Breath
*Feeling of Choking
*Nausea or Abdominal Distress
*Feeling Dizzy, Unsteady, Lightheaded/Fain

*Derealization (Unreality) or Depersonalization (Detached)
*Fear of Losing Control or Going Crazy
*Fear of Dying
*Paresthesias (Numbness, Tingling)
*Chills or Hot Flushes

*AGORAPHOBIA
*Anxiety about being in Places or Situations from which escape might be difficult or embarrassing, or in which help may not be available in an unexpected situation or situation that may lead to panic
*The Situations are avoided or are endured with marked distress, or require the presence of a companion

*SPECIFIC PHOBIA
*Marked or Persistent Fear That Is Excessive or Unreasonable, Cued By the Presence or Anticipation of a Specific Object or Situation:
*Flying
*Heights
*Animals
* Receiving An Injection or Seeing Blood

*SOCIAL PHOBIAS
*A marked or Persistent Fear of One or More Social or Performance Situations In Which the Person Is Exposed to Unfamiliar People or to Possible Scrutiny By Others. The Individual Fears That He or She Will Act In a Way (Or Show Anxiety Symptoms) That Will Be Humiliating or Embarrassing
*Exposure to the Feared Social Situation Almost Invariably Provokes Anxiety or Panic Attack

*The Person Recognizes That the Fear is Excessive or Unreasonable
*Feared Social or Performance Situations Are Avoided or Endured With Intense Anxiety or Distress
*The Avoidance, Anxious Anticipation, or Distress Interferes Significantly With Normal Activities
*Generalized Social Phobia

OBSESSIVE-COMPULSIVE DISORDER (OCD) Obsessions:
Recurrent and Persistent Thoughts, Impulses, or Images That Are Experienced As Intrusive and Inappropriate, and That Cause Marked Anxiety or Distress
The Thoughts, Impulses, or Images Are Not Simply Excessive Worries About Real-Life Problems
The Person Attempts to Ignore or Suppress Them With Some Other Thought or Action
The Person Recognizes That the Obsessions Are From His/Her Own Mind

Compulsions: Repetitive Behaviors (Hand Washing,
Ordering, Checking) or Mental Acts (Praying, Counting, Repeating Words Silently) That the Person Feels Driven to Perform In Response to an Obsession, or According to Rules That Must Be Applied Rigidly
Are Aimed At Preventing or Reducing Distress or Preventing Some Dreaded Event or Situation, But Are Not Connected In a Realistic Way With What They are Designed to Neutralize or Prevent, or Are Clearly Excessive

*At Some Point The Person Recognizes That The Obsessions or Compulsions Are Excessive or Unreasonable
*Obsessions or Compulsions Cause Marked Distress
*Some Persons May Have Poor Insight or Recognition That The Obsessions/Compulsions Are Excessive or Unreasonable

*POST-TRAUMATIC STRESS DISORDER (PTSD)
*The Person Has Been Exposed to a Traumatic Event In Which Both of The Following Are Present:
*The Person Experienced, Witnessed, or Was Confronted With an Event(s) That Involved Actual or Threatened Death or Serious Injury, or a Threat to the Physical Integrity of Self or Others
*The Person’s Response Involved Intense Fear, Helplessness, or Horror

The Traumatic Eventis Persistently Re- experienced In One or More of the Following Ways: Recurrent and Intrusive Distressing
Recollections of the Event Recurrent Distressing Dreams of the Event Acting or Feeling As If the Traumatic Event
Were Recurring Intense Psychological Distress at Exposure
to Internal or External Cues That Symbolize or Resemble Aspects of the Event
Physiological Reactivity on Exposure to Internal or External Cues

*Persistent Avoidance or Numbing
*Persistent Symptoms of Increased Arousal
*Course:
*Acute: <3 Months
*Chronic: >3 Months
*Delayed Onset: Onset of Symptoms >6 Months After the Trauma

GENERALIZAED ANXIETY DISORDER Excessive Anxiety and Worry The Person Finds It Difficult to Control
the Worry The Anxiety and Worry Are Associated
With 3 or More of the Following: Restlessness or Feeling Keyed Up or On
Edge Being Easily Fatigued Difficulty Concentrating or Mind Going Blank Irritability Muscle Tension Sleep Disturbance (Falling Asleep, Staying
Asleep, or Restless Sleep)

*Somatization Disorder
*Conversion Disorder
*Pain Disorder
*Hypochondriasis
*Body Dysmorphic Disorder

*DISSOCIATIVE DISORDERS
*Dissociative Amnesia
*Dissociative Fugue
*Dissociative Identity Disorder
*Multiple Personality Disorder

*Intense Sexually Arousing Fantasies, Urges, or Behaviors / Perversions
*The Person Acts On These With Resulting Significant Distress or Impairment in Social, Occupational, or Other Important Areas of Functioning

PARAPHILIAS Exhibitionism: Exposing Fetishism: Use of Non-Living Objects Frotteurism: Touching, Groping Pedophilia: Involving Children (Often
13 y.o. or Younger) Sexual Masochism: Made to Suffer
(Beating, Bondage, or Humiliation) Sexual Sadism: Inflicting Suffering Transvestic Fetishism: Involving Cross-
Dressing Voyeurism: Observing Unsuspecting
Person’s Nudity

*Anorexia Nervosa
*Bulimia Nervosa

*ANOREXIA NERVOSA
*Refusal to Maintain Body Weight At or Above Minimally Normal Weight For Age and Height (<85% of Expected)
*Intense Fear of Gaining Weight or Becoming Fat, Even Though Underweight
*Disturbance In Perception of Body Weight or Shape, or Denial of the Seriousness of Current Low Weight
*Amenorrhea (No Menses for 3 or More Consecutive Months)

*Restricting Type:
*No Binge-Eating or Purging Behaviors
*Binge-Eating/Purging Type:
*Regularly Engages in Self-Induced Vomiting or the Misuse of Laxatives, Diuretics, or Enemas
*Death Rate 10-20%: One of the Most Lethal Disorders

BULIMIA NERVOSA Recurrent Episodes of Binge Eating; Within a Discrete Period (e.g., <2
hours), Eating Food in Larger Amounts Than Most People Would Eat
Sense of Lack of Control Over Eating – Recurrent Inappropriate Compensatory
Behavior In Order to Prevent Weight Gain: Self-Induced Vomiting; Misuse of Laxatives, Diuretics, Enemas,
or Other Medications; Fasting; or Excessive Exercise

*IntermittentExplosiveDisorder:
*Sudden Violent Aggression
*Kleptomania:
*Impulsive Stealing
*Pyromania
*Fire Setting
*PathologicalGambling:
*Trichotillomania
*Hair pulling/May Eat Hair

*Enduring Pattern of inner experience and Behavior That Deviates From the Expectations of the Individual’s Culture Manifested In:
*Cognition (Perceiving and Interpreting Self, Others, and Events
*Affectivity (Range, Intensity, Lability, and Appropriateness of Emotional Response
*Interpersonal Functioning
*Impulse Control

*Enduring Pattern of Personality Is Inflexible and Pervasive Across a Broad Range of Personal and Social Situations
*Enduring Pattern Leads to Significant Distress or Impairment In Social, Occupational, or Other Important Areas of Functioning
*Enduring Pattern Is Stable and Of Long Duration, and Its Onset Can Be Traced Back At Least To Adolescence or Early Adulthood

Cluster A: Paranoid Schizoid Schizotypal
Cluster B: Antisocial Borderline Histrionic
Narcissistic
*Cluster C:
*Avoidant
*Dependent
*Obsessive-Compulsive