-
YALE JOURNAL OF BIOLOGY AND MEDICINE 74 (2001), pp.
13-20.Copyright C 2001. All rights reserved.
CASE REPORT
Intra-Abdominal Desmoplastic Small RoundCell Tumorc
Jaimie D. Nathana, Cynthia Gingalewski, and Ronald R.
SalemDepartment of Surgery, Yale University School of Medicine, New
Haven, Connecticut
Background: Intra-abdominal desmoplastic small round cell tumor
is a rare malignancy with apredilection for young males. Unique
histological and immunocytochemicalfeatures distinguish
thetumorfrom other members of the family of small round cell tumors
of infancy and childhood. Theaggressive nature oftumor spread,
relative insensitivity to chemotherapy, and generally
incompleteresectability result in a very poor prognosis. The
authors report a case of a 39-year-old man withdiffuse abdominal
and pelvic involvement of intra-abdominal desmoplastic small round
cell tumortreated with aggressive chemotherapy and surgery.
Methods: Computed tomography (CT)-guided biopsy of an omental
mass was performed.Histologically, discrete nests of uniform
closely packed malignant cells were distributed in a back-ground
offocally desmoplastic stroma. Immunocytochemistry demonstrated
positivityfor epithelial,mesenchymal, and neural markers. On the
basis of these unique histological and immunohisto-chemical
characteristics, the diagnosis of desmoplastic small round cell
tumor was made. Thepatient was treated with aggressive neoadjuvant
chemotherapy consisting of a high-dose alkylator-based combination
regimen, followed by surgery.
Results: The patient had a 10 to 15 percent regression in tumor
mass in response to chemotherapy.Laparotomy revealed two large
omental masses, another large mass adherent to the left colon
andpelvic sidewall, and diaphragmatic, peritoneal and mesenteric
studding with small nodules.Complete surgical resection was not
possible.
Conclusions: Intra-abdominal desmoplastic small round cell tumor
remains an aggressive malig-nancy with an extremely poor prognosis.
Although some response to chemotherapy may be possi-ble, complete
resection is rare, and surgical efforts are generally
palliative.
INTRODUCTION
First described in 1987 by Sesterhennet al. [1], intra-abdominal
desmoplasticsmall round cell tumor (IADSRCT)b is a
distinct variant of the small round celltumors of infancy and
childhood. It is anuncommon, highly aggressive tumor witha
predilection for young males [2-15].Predominantly intra-abdominal
in location,
a To whom all correspondence should be addressed: Jaimie D.
Nathan, M.D., Departmentof Surgery, Duke University Medical Center,
PO. Box 3494, Durham, NC 27710; Tel.: 919-684-81 1 1; Fax:
919-681-7934; E-mail: nathaOO2@?mc.duke.edu.b Abbreviations:
IADSRCT, intra-abdominal desmoplastic small round cell tumor; CT,
com-puted tomography; EMA, epithelial membrane antigen; NSE,
neuron-specific enolase;EWS, Ewing's sarcoma gene; WT1, Wilms'
tumor suppressor gene.Submitted: April 6, 1999; Accepted: November
27, 1999.CThis article was originally published in Volume 72 of
this journal in an incomplete form. Asa courtesy to the authors, we
are re-publishing a corrected version of the article.
13
-
14 Nathan et al.: Intra-abdominal small cell tumor
IADSRCT lacks a visceral site of originand spreads diffusely
along serosal sur-faces. Histologically, this tumor is
charac-terized by well-demarcated nests of tumorcells surrounded by
an abundant desmo-plastic stroma. Co-expression of
epithelial,mesenchymal and neural markers is aunique feature of
IADSRCT [2-6, 9, 16],as is its association with a
characteristicchromosomal translocation t(1 1; 12)(pl3;qll.2 or
q12) [17-20]. Prognosis isuniformly poor because the malignancy
isrelatively insensitive to chemotherapy andradiation, and surgical
excision is rarelycomplete. Due to the rarity of this malig-nancy,
optimal treatment regimens haveyet to be defined. We report the
case of a39-year-old man with diffuse abdominaland pelvic
involvement of intra-abdominaldesmoplastic small round cell tumor
treat-ed with aggressive neoadjuvantchemotherapy and surgery.
CASE HISTORY
A 39-year-old white man, previouslywell, presented to his
primary care physi-cian with a six-week history of left lower
quadrant abdominal discomfort, early sati-ety, increasing
abdominal girth, rectalpressure during bowel movements,decreased
caliber of bowel movements,intermittent night sweats and lower
backdiscomfort, as well as a 12-pound weightloss.
On physical examination, theabdomen was moderately distended
withascites, and two large, firm, nontender,mobile masses were
palpable in bothlower abdominal quadrants. Laboratorystudies were
unremarkable except for lac-tate dehydrogenase 287 u/l (normal
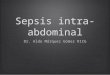
50-240 u/l). Computed tomography (CT)scan revealed an extensive
soft tissuemass filling the pelvis and displacing therectum
posteriorly, as well as severeascites and evidence of peritoneal
carcino-matosis with multiple large solid massesinvolving the
omentum and the bowelwall (Figure 1). CT-guided biopsy of anomental
mass was consistent with desmo-plastic small round cell tumor.
Neoadjuvant chemotherapy was be-gun with intravenous
cyclophosphamide,doxorubicin, and vincristine, alternatingwith
ifosfamide and etoposide. The patientresponded clinically to the
first three
* --j ij Figure 1. Pre-chemotherapycontrast-enhanced CT scanof
the abdomen. Large bulkyintraperitoneal soft tissuemasses (M) are
noted displac-ing bowel loops. Severeascites (A) and peritoneal
nod-ules (arrows) are also evident.
-
Nathan et al.: Intra-abdominal small cell tumor 15
cycles of chemotherapy, requiring para-centesis less frequently.
Subsequent CTscan revealed a 10 to 15 percent regressionin tumor
mass. The patient underwent twoadditional courses of chemotherapy
afterwhich he required stem cell rescue. CTscan showed no further
change in tumormass.
At laparotomy, 2.5 liters of asciteswas found within the
peritoneal cavity.Two large mobile masses were foundattached to the
greater omentum, withtumor very closely adherent to the
splenicflexure. A third large mass was attached tothe left pelvic
sidewall and to the sigmoidcolon and extended between the
bladderand the rectum. The diaphragm was stud-ded with small
nodules, and tumor noduleswere noted throughout the mesentery
andparietal peritoneum. The tumor was mobi-lized from the splenic
flexure and from thesigmoid colon, bladder and rectum andwas
transected at its attachment to the leftpelvic side wall, allowing
en bloc resec-tion of the three masses and the omentum.The parietal
peritoneum was removedwith electrocautery, and the nodules with-in
the small bowel mesentery were maxi-mally resected. Post-operative
course hasbeen uneventful, and subsequent therapeu-tic efforts will
include radiation and fur-ther chemotherapy.
PATHOLOGY
Macroscopic findings
The 2,000-gm specimen consisted ofomentum studded with numerous
tumornodules of variable size, some distinct andspherical and
others confluent. The speci-men measured 20 cm x 20 cm x 11 cm asa
whole, with tumor nodules ranging from0.5 cm to 16 cm in size. The
tumor wasfirm and smooth, and the cut surface of thenodules
revealed firm, white densely
fibrotic areas alternating with soft, gelati-nous myxoid
areas.
Histological findings
The specimen obtained by CT-guidedbiopsy was characterized by
discrete nestsof uniform closely packed malignant cellsdistributed
in a background of focallydesmoplastic stroma (Figure 2). The
nestsof cells varied in appearance from irregu-lar islands to
narrow cords and infiltratingstrands. The tumor cells were small,
withhyperchromatic round to oval nuclei, scanteosinophilic
cytoplasm and indistinctcytoplasmic borders. Nucleoli were
gener-ally inconspicuous. Mitotic figures wererare, and anaplastic
nuclei were not pre-sent. Tubular or glandular foci, rosettes,
orother recognizable signs of differentiationwere absent. The
stroma was dense andcollagenous with occasional
scatteredspindle-shaped fibroblast-like cells. Thetumor
predominantly consisted of malig-nant cells, with the stromal
componentoccupying a smaller portion of the speci-men. In addition
to the characteristics ofthe biopsy specimen, the resected
speci-men revealed cystic changes and somemyxoid areas within the
stroma.
Immunohistochemistry
On immunohistochemical staining,the neoplastic cells were
strongly positivefor the epithelial marker keratin (AEl/AE3and CAM
5.2), diff-usely throughout thecytoplasm. Although positivity for
epithe-lial membrane antigen (EMA) was alsostrong, its distribution
was more patchythan that of keratin. Reactions with anti-vimentin
antibody revealed diffuse cyto-plasmic positivity in the majority
of tumorcells, while staining with desmin was spo-radically
positive and showed a paranu-clear cytoplasmic "dot-like" or
"globoid"pattern of expression. The tumor cellsdemonstrated focal
positivity for alpha-
-
16 Nathan et al.: Intra-abdominal small cell tumor
smooth muscle actin (Figure 3). Stainingfor neuron-specific
enolase (NSE) and S-100 protein, markers of neural
differentia-tion, exhibited a focal pattern of positivity(Figure
4).
DISCUSSION
IADSRCT is a recently describedentity belonging to the category
of smallround cell tumors of infancy and child-hood, including
Ewing's sarcoma, primi-tive neuroectodermal tumor, embryonal
oralveolar rhabdomyosarcoma, neuroblas-toma, malignant lymphoma,
Askin'stumor, and rhabdoid tumor. This group ofneoplasms is
characterized by small uni-form cells with sparse cytoplasm,
diffusegrowth pattern, and high cellularity.
Specific clinical, topographical, mor-phological and
immunohistochemical fea-tures, however, differentiate IADSRCTfrom
other members of its family.Although not as marked as reported in
thefirst series of IADSRCT by Gerald et al. in1991 [3], the male
predominance of thistumor has been described in several subse-quent
reviews (male-to-female ratio,greater than 3:1) [8, 21-23].
Adolescentsand young adults are typically affected,with a mean age
between 18 and 20 years(range 3 to 48) [23], and greater than
70percent of patients present before the ageof thirty in reviews of
larger series [3, 21,22]. The most common presenting symp-toms
ofIADSRCT are abdominal pain anddistention, related to enlarging
tumor bur-den and sometimes to ascites, as in ourcase. The tumor
tends to arise intra-abdominally on serosal surfaces withoutan
obvious visceral primary site. A domi-nant omental or pelvic mass
is commonwith multiple surrounding smaller satellitenodules
adherent to the peritoneum.Grossly, the tumor is firm, smooth
andbosselated, with a gray-white cut surface
and focal necrotic and hemorrhagicregions [2-4].
Histologically, IADSRCT is charac-terized by well-defined nests
or strands ofuniform small round tumor cells surround-ed by an
abundant desmoplastic stroma.Generally, morphologic signs of
differen-tiation are absent. However, tubular lumi-na have been
noted in pathologic speci-mens of IADSRCT [2], and glandular
andneural components have, likewise, beenreported [4, 16, 21, 22].
Although themalignant cells and the stromal compo-nent usually
occupy equal proportions ofthe tumor, the stroma in IADSRCT can
behighly variable, with some tumors beingpredominantly cellular and
others predom-inantly stromal [2, 21, 23]. Within thedense
collagen-rich stroma, spindle cellsresembling fibroblasts or
myofibroblastscan be identified. The stroma may consistof myxoid
areas, cystic degeneration andcalcification [21]. In our case, the
CT-guided biopsy specimen did not revealthese components,
suggesting that themyxoid areas and cystic changes found inthe
resected specimen may have beenassociated with the neoadjuvant
chemo-therapy received. Alternatively, tumor het-erogeneity may
account for the histologi-cal differences.
Although the clinical and histologicalfeatures of IADSRCT may be
sufficientlydistinctive to suggest its diagnosis, IAD-SRCT is most
easily distinguished fromother members of its family by the
uniqueimmunoreactivity for epithelial, mes-enchymal and neural
markers. Immuno-positivity for keratin and EMA, markers
ofepithelial differentiation, is usually diffusethroughout the
cytoplasm and widespread.Some reports have demonstrated, howev-er,
that EMA reactivity is variable, withpatchy or scattered
distribution and local-ization adjacent to the cytoplasmic
mem-branes [6, 24]. The mesenchymal markers,vimentin and desmin,
are consistentlyexpressed in IADSRCT. Vimentin usually
-
Nathan et al.: Intra-abdominal small cell tumor
Figure 2. Histologic appearanceof tumor. The tumor is composed
ofirregular islands and cords of malig-nant cells that are oval and
spindle-shaped with scanty cytoplasm anddark ovoid to round nuclei.
Islandsand cords of tumor cells are sepa-rated by a dense
desmoplastic stro-ma containing occasional spindle-shaped cells. (H
& E, x 250).
Figure 3. Immunostaining forsmooth muscle actin.
Focalcytoplasmic immunopositivity forSMA is present in many
tumorcells. (Immunoperoxidase, x 400).
Figure 4. Immunostaining forS-100 protein. The tumor cellsshow
focally positive cytoplas-mic immunohistochemicalstaining for S-100
protein, amarker of neural differentiation.(Immunoperoxidase, x
400).
17
-
18 Nathan et al.: Intra-abdominal small cell tumor
exhibits widespread, diffuse cytoplasmicstaining, while desmin
positivity has aclassic paranuclear "dot-like" or "globoid"pattern,
though a diffuse, cytoplasmicquality has been noted [16, 22].
Despiteimmunoreactivity for keratin, EMA anddesmin, microscopic
features of epithelialor myoid differentiation are generallyabsent.
In our case, neoplastic cells werefocally positive for alpha-smooth
muscleactin, an uncommonly expressed antigenin IADSRCT [22].
Although neurosecreto-ry dense-core granules, ultrastructural
evi-dence of neuroendocrine differentiation,have been reported only
rarely [3, 4, 16],IADSRCT is usually immunopositive forNSE and
occasionally expresses S-100protein as well [16, 21, 25].
Co-expressionof epithelial, mesenchymal, and neuralantigens in the
same cell suggests thatIADSRCT may arise during developmentfrom a
primitive pluripotential stem cell.However, the histogenesis of
IADSRCTremains unknown.
Evidence demonstrating the associa-tion of a specific
chromosomal abnormali-ty with some cases of IADSRCT may pro-vide
insight into the histogenesis of thistumor at a molecular level. In
most casesanalyzed cytogenetically, the genetic alter-ation
involves a unique reciprocal translo-cation, t(11;12)(pl3;qll.2 or
q12), and isnot the same 11;12 translocation found inother small
round cell tumors, giving fur-ther support to the notion that
IADSRCT isa distinct, yet related, tumor type [17-20].The
breakpoint loci involve the chromoso-mal regions of the Ewing's
sarcoma gene(EWS) and the Wilms' tumor suppressorgene (WTI), which
have been implicated inother malignant developmental neoplasms[26,
27]. Recent studies have demonstratedevidence of expression of
chimeric EWS-WTI RNA in IADSRCT resulting from thefusion of the EWS
and WTI genes [28]. Assuggested by Parkash et al. [29], the
diver-gent differentiation of IADSRCT may bethe result of the
EWS-WTI fusion, allowing
a combination of neural differentiation ofEwing's neoplasms with
the multidirec-tional differentiation of Wilms' tumors.Although
chromosomal analysis has beenconducted in only a small number of
cases,the t(ll;12)(pl3;qll.2 or q12) appears to bea specific
alteration and may prove usefulin the elucidation of the molecular
patho-genesis of IADSRCT and perhaps in themolecular diagnosis of
the tumor.
The diagnosis of IADSRCT is usuallynot made until tissue is
obtained at laparo-tomy, thereby precluding the use of neoad-juvant
therapy. In our case, diagnosis wasmade by CT-guided biopsy, with
obvioustherapeutic consequences. In 1992,Setrakian et al. [30]
described the case ofa 20-year-old man with a subhepatic softtissue
mass biopsied by CT-guided fineneedle aspiration. Cytologic
analysisrevealed small round cells with scarcecytoplasm and
occasional fibroblast-likecells, and immunostaining was positive
forcytokeratin, desmin and NSE, confirmingthe diagnosis of IADSRCT.
The specifici-ty of immunopositivity for epithelial, mes-enchymal
and neural markers makes CT-guided fine needle aspiration a very
usefultechnique in the diagnosis of IADSRCT.
IADSRCT exhibits an extremelyaggressive clinical course and in
general,carries a very poor prognosis. Although astandardized
treatment protocol is lacking,several studies have attempted to
definethe biological behavior of the tumor and itsresponse to
various therapeutic modalities.In the series by Gerald et al. [3]
in 1991, 19patients underwent surgical "debulking,"followed in most
cases by multi-drugchemotherapy with or without
irradiation.Generally, an incomplete surgical resec-tion and
partial response to chemotherapywas followed by rapid,
uncontrollablerelapse. In 1993, Ordonez et al. [22] like-wise
reported only rare complete surgicalresection but initial tumor
reduction withadjuvant multi-agent chemotherapy.Again, however,
progressive tumor growth
-
Nathan et al.: Intra-abdominal small cell tumor 19
was the rule. With evidence in these stud-ies of some degree of
chemosensitivity inthese tumors, Farhat et al. [31] describedfour
patients with IADSRCT who weretreated with an adjuvant
cisplatin-basedmulti-drug regimen following suboptimalsurgical
debulking or biopsy. All fourpatients demonstrated stable disease
afterfour to nine courses of chemotherapy. In aprospective study by
Kushner et al. [9] in1996, five of eight previously
untreatedpatients experienced complete remissionfollowing a
high-dose neoadjuvant alkyla-tor-based regimen and surgical
resection.Another two patients had complete surgi-cal resection at
the time of diagnosis andwere in complete remission
followingadjuvant chemotherapy. With or withoutconsolidative
radiotherapy and/or mye-loablative chemotherapy, five of the
sevenpatients remained in complete remission10 to 39 months from
the start of the alky-lator-based regimen, demonstrating
thatprogression-free survival of prolongedduration is attainable.
In Amato et al. [7],four of five patients treated with
variousmulti-agent chemotherapeutic regimenswith or without
surgical intervention hadevidence of a partial response but
eventu-ally died from their disease within 3.5years from diagnosis.
Treated with a regi-men similar to that described by Kushneret al.,
our patient had an apparent clinicalresponse to therapy, but CT
scan demon-strated only a 10 to 15 percent reduction intumor mass,
and complete surgical resec-tion was not possible. Adjuvant
therapywill include irradiation and additionalchemotherapy.
IADSRCT remains an aggressivemalignancy with an extremely poor
prog-nosis. Although some response to chemo-therapy may be
possible, in particular tohigh-dose alkylator-based regimens,
com-plete surgical resection is rare, and despiteaggressive
therapy, survival rates remainlow due to the refractory nature of
thetumor. Additional studies are necessary to
further elucidate the biology of the diseaseand to optimize
treatment regimens.
REFERENCES1. Sesterhenn, I., Davis, C.J., and Mostofi,
F.K. Undifferentiated malignant epithelialtumors involving
serosal surfaces of scro-tum and abdomen in young males. J.
Urol.137(suppl):214A, 1987.
2. Gonzalez-Crussi, F., Crawford, S.E., andSun, C.J.
Intraabdominal desmoplasticsmall-cell tumors with divergent
differenti-ation: observations on three cases of child-hood. Am. J.
Surg. Pathol. 14:633-642,1990.
3. Gerald, W.L., Miller, H.K., Battifora, H.,Miettinen, M.,
Silva, E.G., and Rosai, J.Intra-abdominal desmoplastic small
round-cell tumor: report of 19 cases of a distinc-tive type of
high-grade polyphenotypicmalignancy affecting young individuals.Am.
J. Surg. Pathol. 15:499-513, 1991.
4. Variend, S., Gerrard, M., Norris, P.D., andGoepel, J.R.
Intra-abdominal neuroectoder-mal tumour of childhood with
divergentdifferentiation. Histopathology 18:45-51,1991.
5. Frappaz, D., Bouffet, E., Dolbeau, D.,Bouvier, R., Carrie,
C., Louis, D.,Pondarre, C., Tabone, E., Philip, T.,
andBrunat-Mentigny, M. Desmoplastic smallround cell tumors of the
abdomen. Cancer73:1753-1756, 1994.
6. Schmidt, D., Koster, E., and Harms, D.Intraabdominal
desmoplastic small-celltumor with divergent differentiation:
clini-copathological findings and DNA ploidy.Med. Pediatr. Oncol.
22:97-102, 1994.
7. Amato, R.J., Ellerhorst, J.A., and Ayala,A.G. Intraabdominal
desmoplastic smallcell tumor: report and discussion of fivecases.
Cancer 78:845-851, 1996.
8. Kretschmar, C.S., Colbach, C., Bhan, I.,and Crombleholme,
T.M. Desmoplasticsmall cell tumor: a report of three cases anda
review of the literature. J. Pediatr.Hematol. Oncol. 18:293-298,
1996.
9. Kushner, B.H., LaQuaglia, M.P., Wollner,N., Meyers, P.A.,
Lindsley, K.L., Ghavimi,F., Merchant, T.E., Boulad F., Cheung,N.V.,
Bonilla, M.A., Crouch, G., Kelleher,Jr., J.F., Steinherz, P.G., and
Gerald, W.L.Desmoplastic small round-cell tumor: pro-longed
progression-free survival withaggressive multimodality therapy. J.
Clin.Oncol. 14:1526-1531, 1996.
10. Barnoud, R., Delattre, O., Peoc'h, M.,Pasquier, D., Plantaz,
D., Leroux, D., andPasquier, B. Desmoplastic small round celltumor:
RT-PCR analysis and immunohis-
-
20 Nathan et al.: Intra-abdominal small cell tumor
tochemical detection of the Wilm's tumorgene WTI. Pathol. Res.
Pract. 194:693-700, 1998.
11. De Lena, M., Caruso, M.L., Marzullo, F.,Mancarella, S.,
Armentano, R., Ventrella,V., and Guida, M. Complete response
tochemotherapy in intra-abdominal desmo-plastic small round cell
carcinoma. A casereport. Tumori 84:412-416, 1998.
12. Gerald, W.L., Ladanyi, M., de Alava, E.,Cuatrecasas, M.,
Kushner, B.H.,LaQuaglia, M.P., and Rosai, J. Clinical,pathologic,
and molecular spectrum oftumors associated with t(l 1 ;22) (p 13;q
12):desmosplastic small round-cell tumor andits variants. J. Clin.
Oncol. 16:3028-3036,1998.
13. Ordonez, N.G. Desmoplastic small roundcell tumor: an
ultrastructural and immuno-histochemical study with emphasis on
newimmunohistochemical markers. Am. J.Surg. Pathol. 22:1314-1327,
1998.
14. Roberts, P., Burchill, S.A., Beddow, R.A.,Wheeldon, J.,
Cullinane, C., and Lewis, I.J.A combined cytogenetic and
molecularapproach to diagnosis in a case of desmo-plastic small
round cell tumor with a com-plex translocation (11 ;22;21).
CancerGenet. Cytogenet. 108:19-25, 1999.
15. Schwarz, R.E., Gerald, W.L., Kushner,B.H., Coit, D.G.,
Brennan, M.F., and LaQuaglia, M.P. Desmoplastic small roundcell
tumors: prognostic indicators andresults of surgical management.
Ann. Surg.Oncol. 5:416-422, 1998.
16. Norton, J., Monaghan, P., and Carter, R.L.Intra-abdominal
desmoplastic small celltumour with divergent
differentiation.Histopathology 19:560-562, 1991.
17. Sawyer, J.R., Tryka, A.F., and Lewis, J.M.A novel reciprocal
chromosome transloca-tion t(l 1; 12)(p l 3;q 12) in an
intraabdominaldesmoplastic small round-cell tumor. Am.J. Surg.
Pathol. 16:411-416, 1992.
18. Shen, W.P.V., Towne, B., and Zadeh, T.M.Cytogenetic
abnormalities in an intraab-dominal desmoplastic small cell
tumor.Cancer Genet. Cytogenet. 64:189-191,1992.
19. Biegel, J.A., Conrad, K., and Brooks, J.J.Translocation (11
;12)(p13;q12): primarychange in intra-abdominal desmoplasticsmall
round cell tumor. Genes Chromo-somes Cancer 7:119-121, 1993.
20. Rodriguez, E., Sreekantaiah, C., Gerald,W., Reuter, V.E.,
Motzer, R.J., andChaganti, R.S.K. A recurring translocation,t(11;
12)(pl 3;q 11.2), characterizes intra-abdominal desmoplastic small
round-celltumors. Cancer Genet. Cytogenet. 69:17-21, 1993.
21. Gerald, W.L. and Rosai, J. Desmoplasticsmall cell tumor with
multi-phenotypic dif-ferentiation. Zentralbl. Pathol. 139:141-151,
1993.
22. Ordonez, N.G., El-Naggar, A.K., Ro, JY.,Silva, E.G., and
Mackay, B. Intra-abdomi-nal desmoplastic small cell tumor: a
lightmicroscopic, immunocytochemical, ultra-structural, and flow
cytometric study. Hum.Pathol. 24:850-865, 1993.
23. Leuschner, I., Radig, K., and Harms, D.Desmoplastic small
round cell tumor. Sem.Diag. Pathol. 13:204-212, 1996.
24. Nikolaou, I., Barbatis, C., Laopodis, V.,Bekir, S., and
Fletcher, C.D.M. Intra-abdominal desmoplastic small-cell
tumourswith divergent differentiation: report of twocases and
review of the literature. Path.Res. Pract. 188:981-988, 1992.
25. Gerald, W.L. and Rosai, J. Desmoplasticsmall cell tumor with
divergent differentia-tion. Pediatr. Pathol. 9:177-183, 1989.
26. Call, K.M., Glaser, T., Ito, C.Y., Buckler,A.J., Pelletier,
J., Haber, D.A., Rose, E.A.,Kral, A., Yeger, H., Lewis, W.H.,
andJones, C. Isolation and characterization of azinc finger
polypeptide gene at the humanchromosome 11 Wilms' tumor locus.
Cell60:509-520, 1990.
27. Zucman, J., Delattre, O., Desmaze, C.,Plougastel, B.,
Joubert, I., Melot, T., Peter,M., DeJong, P., Rouleau, G., Aurias,
A.,and Thomas, G. Cloning and characteriza-tion of the Ewing's
sarcoma and peripheralneuroepithelioma t(l 1; 12)
translocationbreakpoints. Genes Chromosomes Cancer5:271-277,
1992.
28. Ladanyi, M. and Gerald, W. Fusion of theEWS and WTI genes in
the desmoplasticsmall round cell tumor. Cancer Res.54:2837-2840,
1994.
29. Parkash, V., Gerald, W.L., Parma, A.,Miettinen, M., and
Rosai, J. Desmoplasticsmall round cell tumor of the pleura. Am.
J.Surg. Pathol. 19:659-665, 1995.
30. Setrakian, S., Gupta, P.K., Heald, J., andBrooks, J.J.
Intraabdominal desmoplasticsmall round cell tumor: report of a
casediagnosed by fine needle aspiration cytol-ogy. Acta Cytol.
36:373-376, 1992.
31. Farhat, F., Culine, S., Lhomme, C.,Duvillard, P., Soulie,
P., Michel, G.,Terrier-Lacombe, M., Theodore, C.,Schreinerova, M.,
and Droz, J.Desmoplastic small round cell tumors:results of a
four-drug chemotherapy regi-men in five adult patients. Cancer
77:1363-1366, 1996.