Embed Size (px)
Citation preview

ANNALS OF CLINICAL AND LABORATORY SCIEN CE, Vol. 28, No. 6Copyright © 1998, Institute for Clinical Science, Inc.
Intra-abdominal Desmoplastic Small Round Cell Tumor: Immunohistochemical Evidence for Up-regulation of Autocrine and Paracrine Growth Factors
KENT FROBERG, M.D.,* ROBERT E. BROWN, M .D.,i HARVEY GAYLORD, Ph.D.,§
and CARLOS MANIVEL, M.D.°
*Department o f Pathology and Laboratory Medicine, University o f Minnesota-Duluth,
D uluth, M N 55812 $Departments o f Laboratory Medicine and Pediatrics,
PennState Geisinger Health System, Danville, PA 17822
§R&D Systems, Minneapolis, M N 55413
°Department o f Surgical Pathology, Fairoiew University Hospital
Minneapolis, M N 55455
ABSTRACT
Desmoplastic small round cell tumors (DSRCT) are highly aggressive tumors typically involving the serosal surfaces of the peritoneum. Patients often present with abdominal pain, an abdominal mass, ascites or signs of intestinal obstruction. Cytogenetic and molecular studies have identified a characteristic t(ll;22)(pl3;ql2) translocation within the tumor cells. The fused gene product apparently aligns the NH2-terminal domain (NTD) of the EWS gene to the zinc finger DNA-binding domain of the WT1 gene. This product could lead to loss of the tumor suppressor effect of the WT1 gene as well as to an increase in EWS driven expression of growth factors normally repressed by WT1. We investigated this latter possibility by performing immunohistochemical studies on formalin fixed tissue from 10 cases of DSRCT and five Wilms’ tumors using antibodies to insulin-like growth factor (IGF)-II, the latency associated peptide of transforming growth factor (TGF)-p,, platelet-derived growth factor (PDGF)-AB chain and PDGF-a receptor, respectively. In general, tumor cells were strongly positive for these growth factors in DSRCT, while stromal cells were negative for IGF-II and positive for the other growth factors in parallel with the tumor cells. Wilms’ tumor cells were essentially negative for PDGF-AB chains, but positive for IGF-II, and the latency associated
Address for correspondence: Kent Froberg, M.D., Department o f Pathology and Laboratory Medicine, University o f Minnesota-Duluth, Duluth, MN 55812.
3860091-7370/98/1100-0386 $02.00 © Institute for Clinical Science, Inc.

AUTOCRINE AND PARACRINE GROWTH FACTORS 3 8 7
peptide of TGF-Pj and variably positive for PDGF-a receptor. These findings support the proposed molecular mechanism of tumorigenesis for DSRCT and may help explain this tumor’s poor prognosis.
Introduction
DSRCT is a highly malignant neoplasm with a multiphenotypic immunohistochemical profile usually presenting on the peritoneum of young adult males. Since its definitive description by Gerald et al,1 apparently characteristic cytogenetic and molecular abnormalities have been described.2-9 Karyotypic studies have id e n tif ie d a r e c u r re n t t r a n s lo c a tio n , t(ll;22)(pl3;ql2), in DSRCT.2'3 Band l lp l3 is the site of the WT1 gene, which is deleted or mutated in many Wilms’ tumors.10’11 Band 22ql2 is the site of the EWS gene, which is translocated in Ewing’s sarcoma (EWS), primitive neuroectodermal tumors (PNET), clear cell sarcoma and mesenchymal chondrosarcoma.12’13 Both of these genes have been cloned and their properties studied in vitro. WT1 is a tumor suppressor gene associated with embryonic mesenchymal differentiation necessary for normal nephrogenesis. Target genes include various growth factors including insulin-like growth factor II (IGF-II), transforming growth factor beta (TGF-(3), platelet- derived growth factor (PDGF)-A chain and its receptor (PDGFRot)4 IGF-II and PDGF have been shown to be overexpressed in Wilms’ tumor cells.14-16 Less is known about the EWS gene, although in the tumors in which it is translocated, the NTD of EWS aligns itself with one of several transcription factors, thereby acting as a putative activator of transcription.13 Molecular studies have confirmed the unique translocation described in DSRCT which appears to align the NTD of the EWS gene to the DNA-binding region of the WT1 gene, theoretically activating a number of growth factors normally suppressed by WT1.2-9
The prognosis for DSRCT is worse than either Wilms’ tumor or Ewing’s sarcoma. The role of the t(ll;22)(pl3;ql2) in the poor prognosis of DSRCT is unknown, but could be
related to expression of multiple growth factors by tumoral cells leading to persistent tumor growth. We looked for tumor and stromal cell expression of growth factors normally suppressed by WT1 by performing immunohistochemical studies on DSRCT using antibodies to IGF-II, PDGFRot, PDGF-AB chains and the latency associated peptide of TGF-p!. Immunohistochemical studies using the same antibodies were also performed on Wilms’ tumor to compare the frequency and degree of positive staining between Wilms’ and DSRCT.
Materials and Methods
St u d y C a s e s
Archival formalin-fixed, paraffin-embedded tissue from 10 cases of DSRCT and five cases of W ilms’ tum or was studied. The original histopathologic diagnosis in all cases of DSRCT had been confirmed by immunohistochemical analysis demonstrating the expected m ultiphenotypic expression of epithelial and m esenchym al markers. In two cases, the WT1-EWS translocation was confirmed by Dr. William L. Gerald using a reverse transcriptase, polymerase chain reaction.
I m m u n o h is t o c h e m is t r y
A panel of antibodies was assembled to detect the following antigens: the latency associated peptide (LAP) of transforming growth factor-^! (TGF-P1)§; platelet derived growth factor receptor-alpha (PDGFRa)§; PDGF-AB chain§; and insulin-like grown factor-II (IGF- II)*, respectively.
§ R&D Systems, Inc., Minneapolis, MN* Research Diagnostics, Inc., Flanders, NJ

3 8 8 FROBERG ET AL.
Goat polyclonal antibody reactive with the latency associated peptide (LAP) of TGF-P! (catalog number AB-246-NA)§ was used in these experiments. This antibody against LAP previously has been shown to react with the latent TGF-Pj in immunohisto- chemical applications.17
Mouse monoclonal anti-human PD GFRa (clone 35264.11, IgGlk)§ is reactive in direct enzym e-linked im m unoadso rben t assay (ELISA) with a recombinant extracellular domain of the PDGF receptor alpha expressed either as a monomer (via baculovirus/Sf21 expression) or as a dimeric Fc-fusion protein (via expression in murine NSO cells). It has no detectable reactivity against recombinant human PDGF receptor beta or the VEGF receptor (Flt-1), both of which share some homology with PDGFRa. A neutralization (block-off) experiment was carried out using a known immunoreactive tissue substrate and this anti-PD G FR a-antibody, following prior incubation in a solution containing recom binant human (rh) PD G F receptor alpha in excess. The rh PD GF receptor alpha effectively n eu tra liz ed th e anti- PDGFRa-antibody affirming its specificity in immunohistochemistry.
Mouse monoclonal antibody against human PDGF-AB (clone 10106.3, IgG2b,k)§ was initially detected by screening in direct ELISA on recombinant PDGF dimers of AA, AB or BB type, and found to be reactive with AB or BB, but not AA. It has a marked preference for AB over BB. Although its signal in these experiments theoretically could have been generated by BB homodimers, a neutralization (block-off) study using a known immunoreactive tissue substrate from one of the test cases and this anti-PDGF-AB attested to its specificity. That is to say, prior incubation with rh PDGF-AB in excess neutralized the anti- PDGF-AB antibody. Monoclonal anti-IGF-II antibody is commercially available for use in immunohistochemistry.*
Briefly, the general immunohistochemical procedure involved antigen retrieval methods. For detection of TGF-PX (LAP), PDGFR-a and PDGF-AB antigens, deparaffinized tissues
were pretreated and processed as previously described.18 For IGF-II antigen, slides were steam-treated in citrate buffer prior to antibody exposure. All primary antibodies were used at a concentration of 20 fxg/iriL and sections were processed using the previously referenced procedure or in reaction minus the primary antibody.
A n a l y s is o f I m m u n o s t a i n in g
Stromal and tumor cells were analyzed separately on each slide and immunoreactivities scored from 0 (negative) to 4+ positivity by two pathologists (REB and KF). Parenthetically, stromal cells were identified as those cells away from tumor cell nests, with a typical spindle cell or fibroblastic appearance and without nuclear hyperchromasia. The maximum degree of staining for each case was recorded and used to determine an average degree of staining for each of the aforementioned growth factors in the DSRCT and Wilms’ tumor groups, respectively.
Results
Neoplastic cells in the five cases of Wilms’ tum or showed a m oderate im m unohistochemical signal for the latency associated peptide (LAP) ofTGF-3, and for IGF-II antigens, respectively, with an average maximum staining intensity for each of 2+. Stromal cells gave a weaker signal for both growth factors at 1+. Similar but stronger signals for each of these growth factors was evident in the tumor cells from the 10 cases of DSRCT with average maximum staining intensities at 3+. Stromal cells gave on average a similar 3+ intensity for TG F-Pi (LAP) but no reactivity (0 score) for IGF-II.
A perceptible difference in growth factor expression betw een W ilm s’ tum or and DSRCT cases was evident in the staining intensities for PDGF-AB and PDGFRa. In three out of five cases of Wilms’ tumor, there was no signal (0 score) for PDGF-AB antigen. Two cases exhibited a very weak but probably

AUTOCRINE AND PARACRINE GROWTH FACTORS 3 8 9
real signal recorded at “±” in the tumor cells. If one assigns a 0.5 number to this latter designation, the average maximum score for PDGF-AB in Wilms’ tumor is closer to “0.” Stromal cells, likewise, gave a score of “0” for PDGF-AB. Similarly, in three cases of Wilms’ tumor the neoplastic cells exhibed “±” staining intensity for PD G FR a; one each of the remaining two showed no and 1+ immunore- activity, respectively. The average maximum score for PDGFRa computed to be midway between 0 and 1+, a “±” designation for both the tumor and stromal cells in Wilms’ tumor cases. In contrast, the neoplastic cells in six out of nine cases of DSRCT gave very strong signals for PDGF-AB antigen, either 3 or 4+; two cases had a moderate 2+ reaction and one a 1+ reaction (slides were not available for staining in one case). Similarly nine out of 10 cases of DSRCT showed 3 or 4+ staining reactions for PDGFRa with only one case giving a “±” reaction. The average maximum staining intensity for each of these growth factors in lesional
(tumor) cells was 3+. There was some parallel in staining intensity between the neoplastic cells in DSRCT and the stromal cells for the PDGF-AB and PDGFR-a antigens, albeit on average slightly less at 2+. Finally, it should be noted that in general the majority of tumor and stromal cells in non-necrotic, immunoreactive foci showed some degree of positivity in the cases of DSRCT.
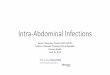
These data are summarized in table I and selected immunoreactivities are illustrated in figures 1 and 2.
Discussion
In recent years specific recurrent translocations have been identified within several malignant neoplasms including Wilms’ tumor, Ewing’s sarcoma and DSRCT. The EWS gene at 22ql2 is involved in translocations seen in ES, PNET, malignant melanoma of soft parts and DSRCT. In most ES and PNET the NH2- terminal domain of the EWS gene is translo-
TABLEIImmunohistochemical Reactivity for Growth Factors in
Desmoplastic Small Round Cell Tumor Versus Wilms’ Tumor
GrowthFactors
StromalCells
WTTumorCells
StromalCells
DSRCTTumorCells
TGF-pi (LAP) 1+a 2+ 3+ 3+PDGFRa ±*> ± 2+ 3+PDGF-AB 0 0 2+ 3+IGF—II 1 + 2+ 0 3+
DSRCT = Desmoplastic Small Round Cell Tumor.WT = Wilms'Tumor.TGF-pi (LAP) = Transforming growth factor - (51 (latency associated peptide).PDGFRa = Platelet - derived growth factor receptor - alpha.PDGF-AB = Platelet - derived growth factor - AB chains.IGF—II = Insulin-like growth factor - II.aNumbers represent the average maximum staining intensity reckoned on a scale of 0 (negative to 4+
(maximum positive reation) and derived from nine or 10 cases of DSRCT or five cases of WT. b±designation refers to an average maximum staining intensity that falls in the mid-range between 0
and 1 +.

390 FROBERG ET AL.
F igure 1. Frame A depicting a desmoplastic small round cell tumor (DSRCT) with nests o f tumor cells in a fibrous stroma (hematoxylin-eosin); Frame B showing strong (3+) im munoreactivity for TGF-(3] (LAP) in DSRCT with slightly less intense staining o f stromal cells (DAB chromogen); Frame C illustrating strong (3+) signal for PDG FR-a antigen in lesional and occasional stromal cells o f DSRCT (HistoMark Red Chromogen); and Frame D with lack of immunoreactivity for PDGFR-a antigen in Wilms’ tumor (HistoMark Red Chromogen; original magnifications x788, A -D ).
cated adjacent to FLI-1, a DNA-binding factor creating a putative dominant oncogene.13 WT1 is deleted or mutated in many Wilms’ tumors and is involved in the recurrent translocation identified in DSRCT. ES, WT and DSRCT share many clinical and pathological features. ES and DSRCT are seen in young adults or adolescents, while WT occurs primarily before the age of five. All are comprised primarily of small, round undifferentiated appearing cells and in the case of WT and DSRCT show mul- tiphenotypic expression of epithelial and mesenchymal markers. However, the poor prognosis of patients with DSRCT is in sharp contrast to that of WT or even ES. Much of
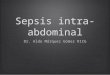
F igure 2. Desmoplastic small round cell (DSRCT) with 4+ immunoreactivity to antibodies for IGF-II and lack of stromal staining (DAB chromogen; original magnification x400).
this difference may depend on primary tumor location or other clinical factors, such as the multifocal presentation usually seen with DSRCT. The role of the genetic abnormalities seen in each neoplasm to tumorigenesis or prognosis is unclear. The recurrent translocation seen in most ES appears to act as a dominant oncogene with few specific alterations in the cell cycle or cell growth identified.13,19,20 In many WT, the suppressor effect of W Tl is lost and over-expression of IG F -II and PDGF-A chain have been reported .14-1(1 Effects of these growth factors may contribute to tumorigenesis in WT. In cell culture, Wilms’ tumor cell line growth is reversibly inhibited by agents that block IGF-II binding to its membrane receptor.21,22
The recurrent translocation between WTl and EWS seen in cases of DSRCT has been studied by Southern and Northern blot, using

AUTOCRINE AND PARACRINE GROWTH FACTORS 3 9 1
probes specific for a portion of the NTD upstream from exon 7 of EWS and exon 8 or 9 of WT1.4"9 Exons 8-10 of WT1 code for zinc- finger regions 2-4, the DNA-binding regions. Exon 7 of EWS-NTD is the most common breakpoint of small round cells in the Ewing’s family.13 Rauscher et al4 conducted assays of the EWS-WT1 fusion gene under conditions where wild-type WT1 functions as a transcriptional repressor, and found this hybrid gene functioned as a potent activator of transcription. Furthermore, the loss of zinc finger 1 appeared to enhance DNA-binding affinity of the remaining three zinc fingers when assayed with an EGR-consensus sequence oligonucleotide, believed to be a normal target gene for WT1. Benjamin et al7 have also shown that EWS-WT1 and WT1 bind similar DNA targets, bu t th a t EWS-W T1 does so w ith increased affinity. Rauscher et al4 studied transcriptional activation of the EWS-WT1 fusion by using EGR-1 fused to the CAT gene as a target for regulation in cell cultures. In cotransfection assays, CMV-WT1 expression vector acted as a potent repressor of the EGR- CAT transcription, while EWS-WT1 titrated into the same assay resulted in activation of transcription. These studies suggest that in DSRCT the EWS-WT1 translocation results in two functional alterations: loss of the repressor activity of WT1 and, secondly, the alignment of the NTD of EWS to the zinc finger region of WT1 creates a potent activator of transcription. Furthermore, it appears that normally repressed WT1 target genes may now be activated by the hybrid gene. Extrapolating these in vitro studies suggests that in native DSRCT, products of WT1 target genes should be expressed at high levels. Several studies have shown that IF G -II, PDGF-A chain and TGF-p are normally repressed by WT1 and in WT, IGF-II and PDGF-A chain are often over expressed. By the molecular model, IGF-II, PDGF-A chain and its receptor, and TGF-(3 should all be expressed by DSRCT cells. The current study supports the molecular model of tumorigenesis in DSRCT by collectively demonstrating strong expression of growth factors normally suppressed by the WT1 gene in the
tumors we studied by immunohistochemical methods. The increased intensity of staining for these growth factors in DSRCT compared to WT also supports the molecular model, ie, that there is activation of transcription in addition to loss of the suppressor effect of WT1 with up-regulation of growth factor expression.
IF G -II , P D G F -cha in and P D G F R -a expression have been documented in several malignancies and may function in an autocrine as well as paracrine manner.23,24 The staining of many of the stromal cells with TGF-(B, PD G FR-a and PDGF-AB in DSRCT, but with lessor intensity than the tumor cells, suggests these growth factors may play a role in formation of the desmoplastic stroma typically seen in these tumors. The expression of PDGFR-a in DSRCT cells and stroma suggests both autocrine and paracrine pathways may be involved in proliferation of tumor and stromal cells. The lack of IGF-II staining in strom al cells is also consistent with this hypothesis and suggests that the tumor cells are the source of IGF-II. PDGF is made up of two homologous polypeptide dimers, A and B chains, and may exist as AA, AB or BB.25 WT1 has been shown to repress the PDGF A-chain gene and only A-chain production has been detected in W ilms’ tum or cells.26,27 The PDGF antibody we used is highly specific for PDGF-AB chains. These findings are consistent with the lack of unequivocal PDGF-AB stain ing in W ilm s’ tum ors we stud ied . PD G FR -a can bind PDGF-AA or -AB.26 PDGF specifically stimulates collagen formation by fibroblasts and PDGF expression has been associated with desmoplasia in some tumors.
The histogenesis of DSRCT is unknown, but Gerald et al,1 in their initial description of 19 cases pointed out that DSRCT shares features with malignant mesothelioma (MM). Each tumor shows diffuse peritoneal spread and demonstrates epithelial differentiation, while fetal mésothélium coexpresses keratin and desmin as is seen in DSRCT. Perturbations of WT1 are uncommon in MM; however, normal mésothélium expresses WT1 and mesotheliomas have been found to express IG F-II,

3 9 2 FROBERG ET AL.
TGF-(B, and PD G F-A and B.27,28 Like DSRCT, the prognosis for MM is poor. The similar pattern of growth factor expression in DSRCT and MM, further supports the idea that DSRCT may be a “mesothelioblastoma.”
In summary, the immunohistochemical demonstration of multiple growth factors in DSRCT lesional and stromal cells with greater staining intensity than seen in cases of WT supports the molecular model of tumorigene- sis of DSRCT and suggests an interplay of autocrine and paracrine mechanisms. Given the poor prognosis for this neoplasm, perhaps therapeutic modalities should be developed that are directed towards agents inhibiting the activity of these cytokines.
Acknowledgment:
The authors wish to thank Glen Kauwell and Kim H agen for their help w ith the im m unohistochem ical studies.
References
1. Gerald WL, Miller HK, Battifora H, et al. Intraabdominal desm oplastie small round-cell tumor. Report o f 19 cases o f a distinctive type o f high-grade polyphenotypic malignancy affecting young individuals. Am J Surg Pathol 1991;15(6):499-513.
2 Sawyer JR, Tryka AF, Lewis JM. A novel reciprocal translocation t(ll;22 )(p l3 ;q l2 ) in an intra-abdominal desmoplastie small round-cell tumor. Am J Surg Pathol 1992;16:411-6.
3. Rodriguez E, Sreekantaiah C, Gerald W, et al. A recurring translocation, t(ll;2 2 )(p l3 ;q ll.2 ) characterizes intra-abdominal desmoplastie small round-cell tumors. Cancer Genet Cytogenet 1993;69:17-21.
4. Rauscher III FJ, Benjamin LE, Fredericsk WJ, et al. Novel oncogenic mutations in the WT1 Wilms’ tumor suppressor gene: a t(ll;22 ) fuses the Ewing’s sarcoma gene EWS1, to WT1 in desmoplastie small round cell tumor. Cold Spring Harbor Symposium on Quantitative Biology. Cold Spring Harbor 1994;59:137-16.
5. Ladanyi M, Gerald W. Fusion o f the EWS and WT1 genes in the desmoplastie small round cell tumor. Cancer Res 1994;54:2837-40.
6. Gerald WL, Rosai J, Ladanyi M. Characterization of the genomic breakpoint and chimeric transcripts in the EWS-WT1 gene fusion of desmoplastie small round cell tumor. Proc Natl Acad Sci USA 1995;92: 1028-32.
7. Benjamin LE, Fredericks W ], Barr FG, et al. Fusion o f EW S1 and W T1 gen es as a resu lt o f th e
t(ll;22 )(p l3 ;q l2 ) translocation in desmoplastie small round cell tumors. Med Pediatr Oncol 1996;27:434-9.
8. de Alva E, Ladanyi M, Rosai J, et al. Detection of chimeric transcripts in desmoplastie small round cell tumor and related developmental tumors by reverse transcriptase polymerase chain reaction. Am J Pathol 1995;147(6):1584-91.
9. Rauscher III FJ. Chromosome translocation-mediated conversion of a tumor suppressor gene into a dominant oncogene fusion o f EWS1 to WT1 in des- moplastic small round cell tumors. Curr Top in Microbiol Immunol 1997;220:151-62.
10. Haber DA, Buckler AJ. WT1: a novel tumor suppressor gene inactivated in W ilms’ tumor. N ew Biol 1992;4(2) -.97-106.
11. Grundy P, Coppes M. An overview of the clinical and molecular genetics o f Wilms’ tumor. Med Pediatr Oncol 1996;27:394-7.
12. Delattre OD, Zucman J, Melot T, et al. The Ewing family o f tumors— a subgroup of small-round-cell tumors defined by specific chimeric transcripts. N Engl J Med 1994;331:294-9.
13. May WA, D enny CT. Biology o f EW S/FLI and related fusion genes in Ewing’s sarcoma and primitive neuroectoderm al tumor. Curr Top in Microbiol Immunol 1997;220:143-50.
14. Scott J, Cowell J, Robertson ME, et al. Insulin-like growth factor-II gene expression in Wilms’ tumor and embryonic tissues. Nature 1985;317:260-2.
15. Reeve AE, Eccles MR, Wilkins RJ, et al. Expression of insulin-like growth factor-II transcripts in Wilms’ tumor. Nature 1985;317:258-60.
16. Frazier GE, Bowen-Pope D F, Vogel AM. Production of platelet-derived growth factor by cultured Wilms’ tumor cells and fetal kidney cells. J Cell Physiol 1987; 133:169-74.
17. Ehrhart EJ, Segarini P, Tsang ML-S, et al. Latent transforming growth factor ¡3, activation in situ: Quantitative and functional evidence after low-dose •y-irra- diation. FASEB J 1997;11:991-1002.
18. Brown RE. Histogenesis o f Reed-Stemberg and dendritic interdigitating cells in nodular sclerosing Hodgkin’s Disease. Immunohistochemical evidence for monocytoid precursors. Ann Clin Lab Sci 1997;27: 329-37.
19. Hirschfeld S, Helman L. Diverse roles o f insulin-like growth factors in pediatric solid tumors. In vivo 1994;8(l):81-90.
20. Hofbauer S, Hajilton G, Theyer G, et al. Insulin-like growth factor-I-dependent growth and in vitro che- mosensitivity o f Ewing’s sarcoma and peripheral primitive neuroectodermal tumor cell lines. Eur J Cancer 1993;29A(2):241-5.
21. Vincent TS, Hazen-Martin DJ, Garvin AJ. Inhibition of insulin-like growth factor II autocrine growth of Wilms’ tumor by suramin in vitro and in vivo. Cancer Lett 1996;103(l):49-56.
22. Qing RQ, Schmitt S, Ruelicke T, et al. Autocrine regulation o f growth by insulin-like growth factor (IGF)-II mediated by type I IGF-receptor in Wilms’ tumor cells. Pediatric Res 1996;39(l):160-5.
23. Fleming TP, Matsui T, Heidaran M, et al. Dem on

AUTOCRINE AND PARACRINE GROWTH FACTORS 3 9 3
stration o f an activated platelet-derived growth factor autocrine pathway and its role in tumor cell proliferation in vitro. Oncogene 1992;7:1355-9.
24. Nister M, Claesson-Welsh L, Eriksson A, et al. D ifferential expression o f platelet-derived growth factor receptors in human malignant glioma cell lines. J Biol Chem 1991;266(25): 16755-63.
25. Ross R, Raines EW, Bowen-Pope DF. The biology o f platelet-derived growth factor. Cell 1986;46:155-69.
26. Gashler AL, Bonthron D T, M adden SL, et al. Human-platelet-derived growth factor A chain is tran
scriptionally repressed by the Wilms’ tumor suppressor WT1. Proc Natl Acad Sci 1992;89:10984-8.
27. Fitzpatrick DR, Peroni DJ, Bielefeldt-Ohmann H. The role o f growth factors and cytokines in the tumorigenesis and immunobiology o f malignant mesothelioma. Am J Respir Cell Mol Biol 1995;12:455-60.
28. Langerak AW, Williamson KA, Miyagawa K, et al. Expression of the Wilms’ tumor gene in human malignant mesothelioma cell lines and relationship to platelet-derived growth factor A and insulin-like growth factor 2 expression. Cancer 1994;12:87-96.