Embed Size (px)
Citation preview
1
International Forum on the Development of
Social Health Protection in Southeast Asian
Region
27-28 October 2014, Hanoi, Vietnam
CAMBODIA Country Team
LO Veasnakiry, M.D.; MA(HMPP), MoH
Sum Sophorn, NSSF
1. Basic Data
2. Health System Organization
3. Health Financing and Coverage
4. Challenges
5. SHP: Ways moving forwards
6. Concluding Remark
2
Source: NSDP 2014-2018, RGC
• Total geographical areas 181,035 Sq. Kms
• Total population 14.7 M (Nov. 2013 CIPS)
• Annual growth rate 1.46%
• Total fertility rate 2.8
(per 1,000 live births)
• Life expectancy at birth M 67.1/F 71
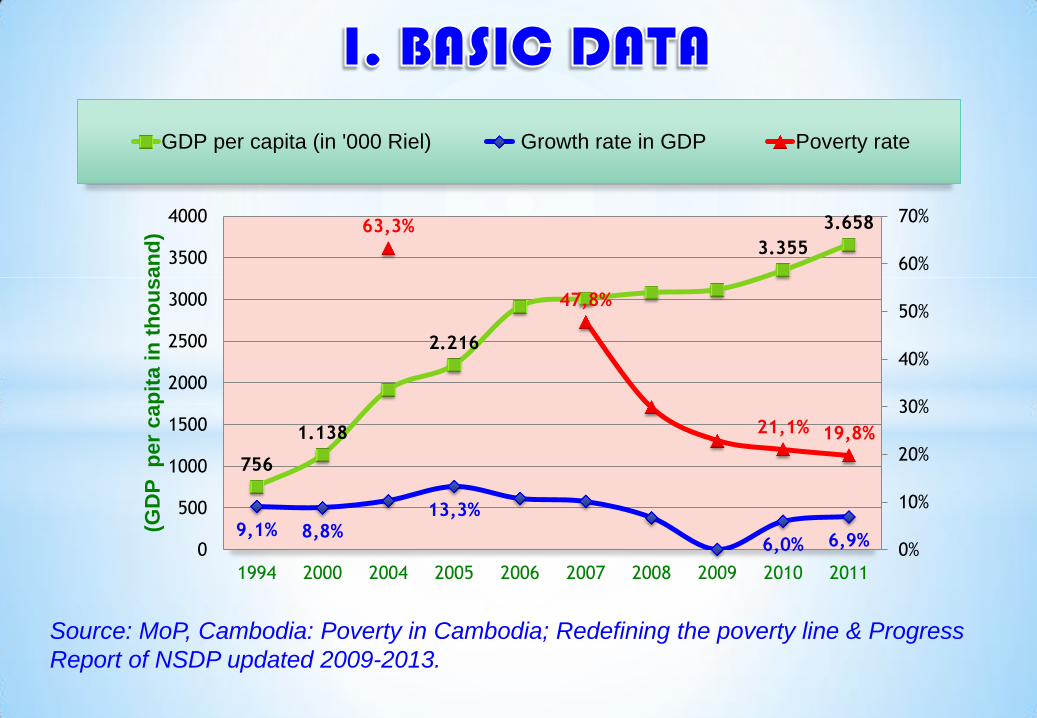
756
1.138
2.216
3.355
3.658
9,1% 8,8% 13,3%
6,0% 6,9%
63,3%
47,8%
21,1% 19,8%
0%
10%
20%
30%
40%
50%
60%
70%
0
500
1000
1500
2000
2500
3000
3500
4000
1994 2000 2004 2005 2006 2007 2008 2009 2010 2011
(GD
P
pe
r ca
pit
a i
n t
ho
usan
d)
GDP per capita (in '000 Riel) Growth rate in GDP Poverty rate
Source: MoP, Cambodia: Poverty in Cambodia; Redefining the poverty line & Progress
Report of NSDP updated 2009-2013.
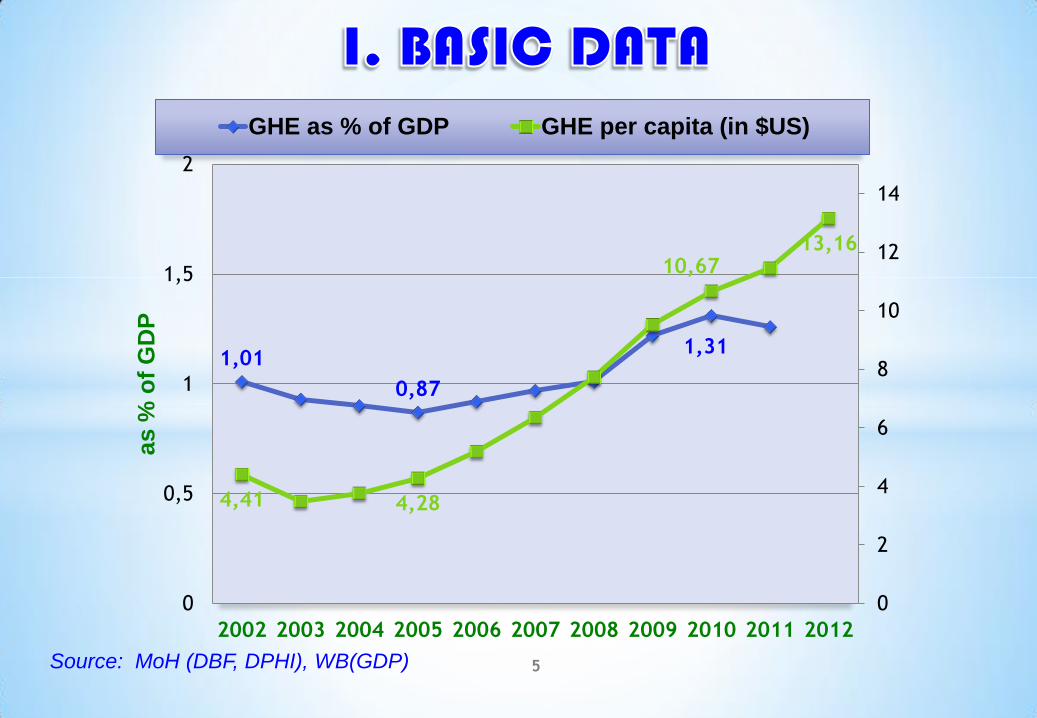
1,01
0,87
1,31
4,41 4,28
10,67 13,16
0
2
4
6
8
10
12
14
0
0,5
1
1,5
2
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
as %
of
GD
P
GHE as % of GDP GHE per capita (in $US)
Source: MoH (DBF, DPHI), WB(GDP) 5

6 “Operational District level (81)”
Central Level
Provincial Level provincial hospitals
(24)
Referral Hospitals (68)
1000,000-200,000 J
Health Centers (1.024)
JKLJKL
Community
J8,000-10,000
Health Post (121)
1
2
3
National
hospital (8)
Health Sector Reform (HSR) in post conflict
setting
• Initiated 1993, implemented in 1995
• The reform implies entails important
transformations, both organizational
(including human resources) and financial
Changing from administrative to
population base system organization—
Population size and accessibility criteria.
Redefine management & service delivery
functions of each level, HC-MPA and RH-
CPA
Reallocation and training health workforce:
pre-service training, in-service training
(Health Service Management)
Introducing new ways of health system
financing (Health Financial Charter)
7
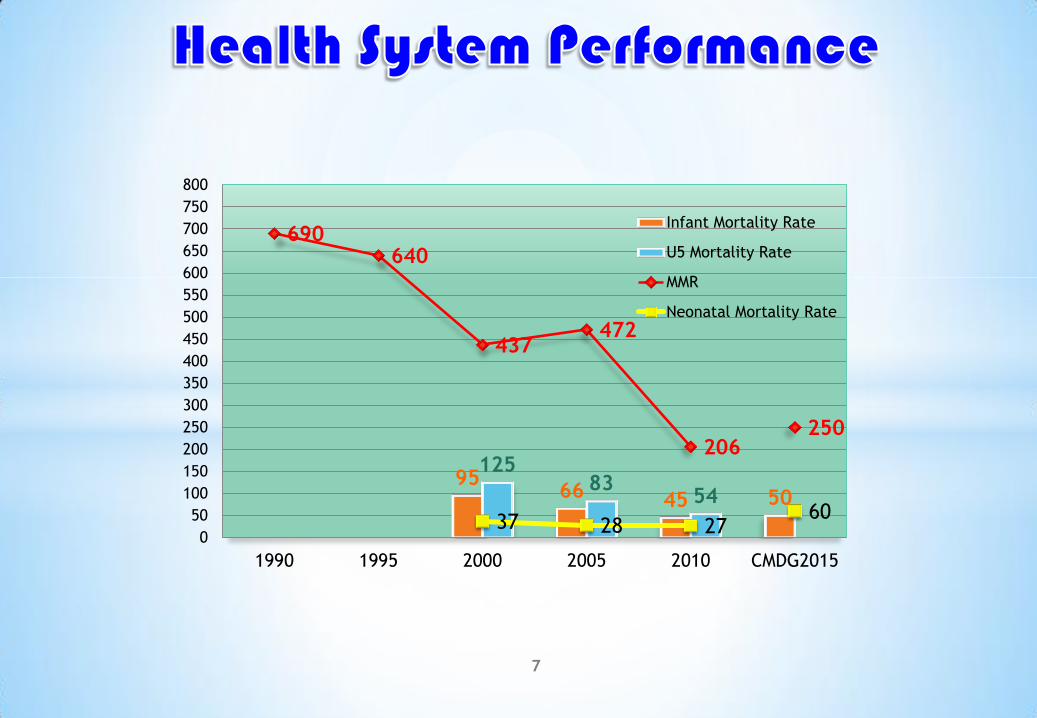
95 66 45 50
125 83
54
690 640
437 472
206 250
37 28 27 60
0
50
100
150
200
250
300
350
400
450
500
550
600
650
700
750
800
1990 1995 2000 2005 2010 CMDG2015
Infant Mortality Rate
U5 Mortality Rate
MMR
Neonatal Mortality Rate
MMR development in Cambodia 1990-2010. Estimates for 1990 and 1995 from WHO, the remainder from CDHS
For 2005 and 2010 with 95% confidence intervals. Analyzed CSES 2004, 2007 and 2009 using methods developed by the World Health Organization (MoH, WHO,
GIZ), 2010, 2011
8
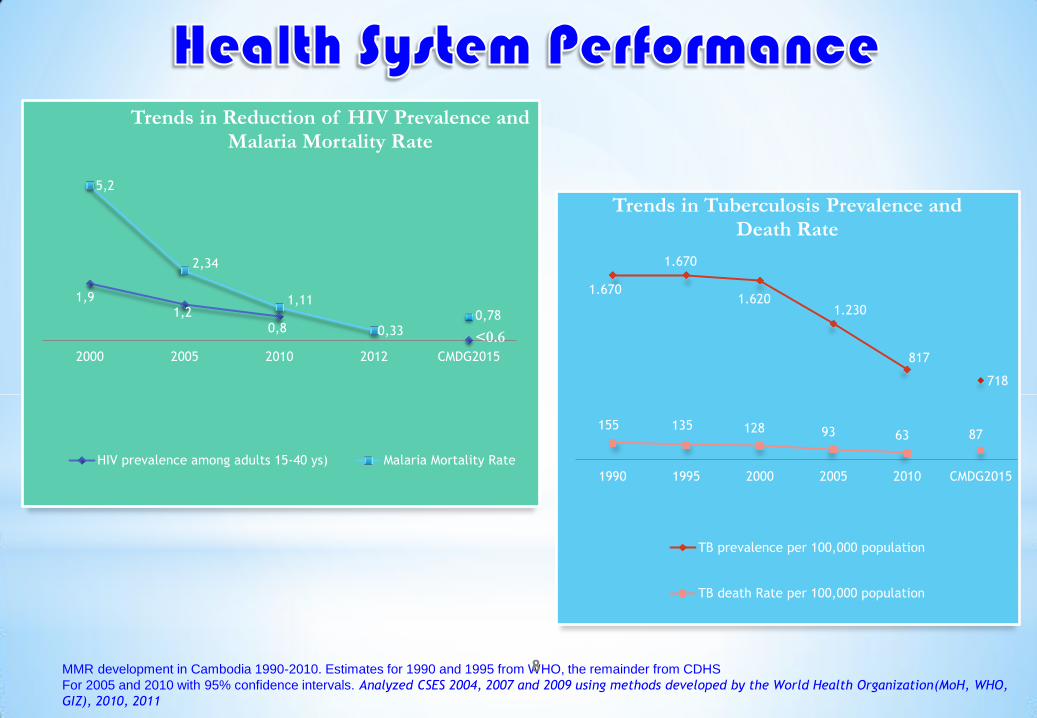
1,9 1,2
0,8 <0.6
5,2
2,34
1,11
0,33 0,78
2000 2005 2010 2012 CMDG2015
Trends in Reduction of HIV Prevalence and Malaria Mortality Rate
HIV prevalence among adults 15-40 ys) Malaria Mortality Rate
1.670
1.670
1.620 1.230
817
718
155 135 128 93 63 87
1990 1995 2000 2005 2010 CMDG2015
Trends in Tuberculosis Prevalence and Death Rate
TB prevalence per 100,000 population
TB death Rate per 100,000 population
9
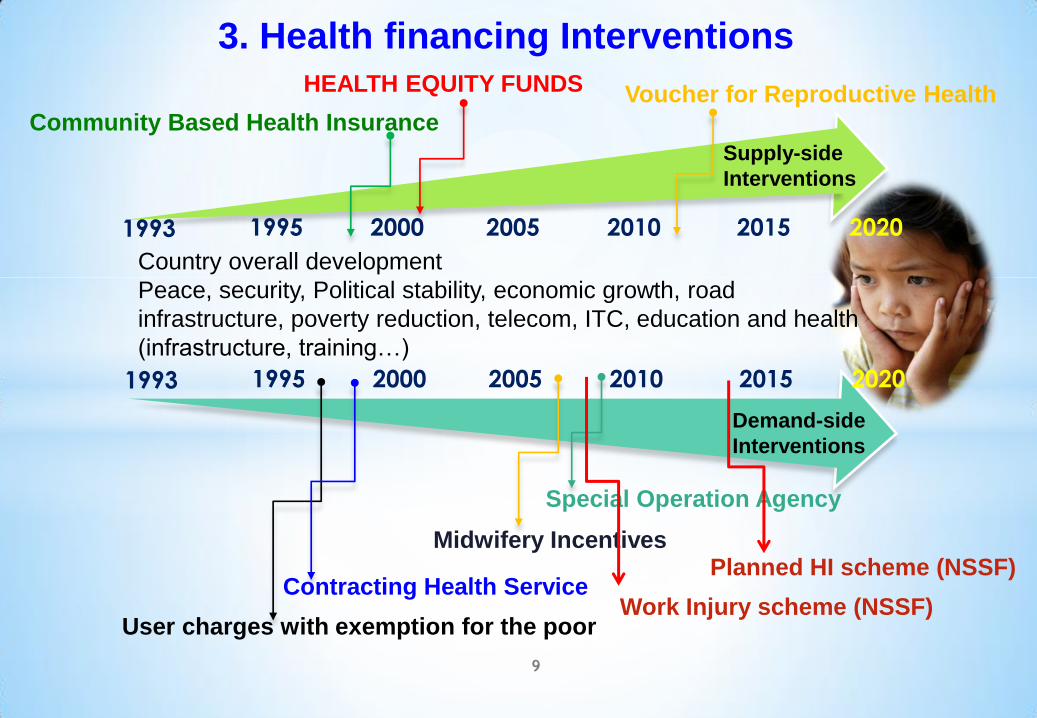
Country overall development
Peace, security, Political stability, economic growth, road
infrastructure, poverty reduction, telecom, ITC, education and health
(infrastructure, training…)
Supply-side
Interventions
Demand-side
Interventions
1993 1995 2000 2005 2010 2015 2020
1993 1995 2000 2005 2010 2015 2020
User charges with exemption for the poor
HEALTH EQUITY FUNDS
Contracting Health Service
Special Operation Agency
Community Based Health Insurance
Midwifery Incentives
Voucher for Reproductive Health
3. Health financing Interventions
Work Injury scheme (NSSF)
Planned HI scheme (NSSF)
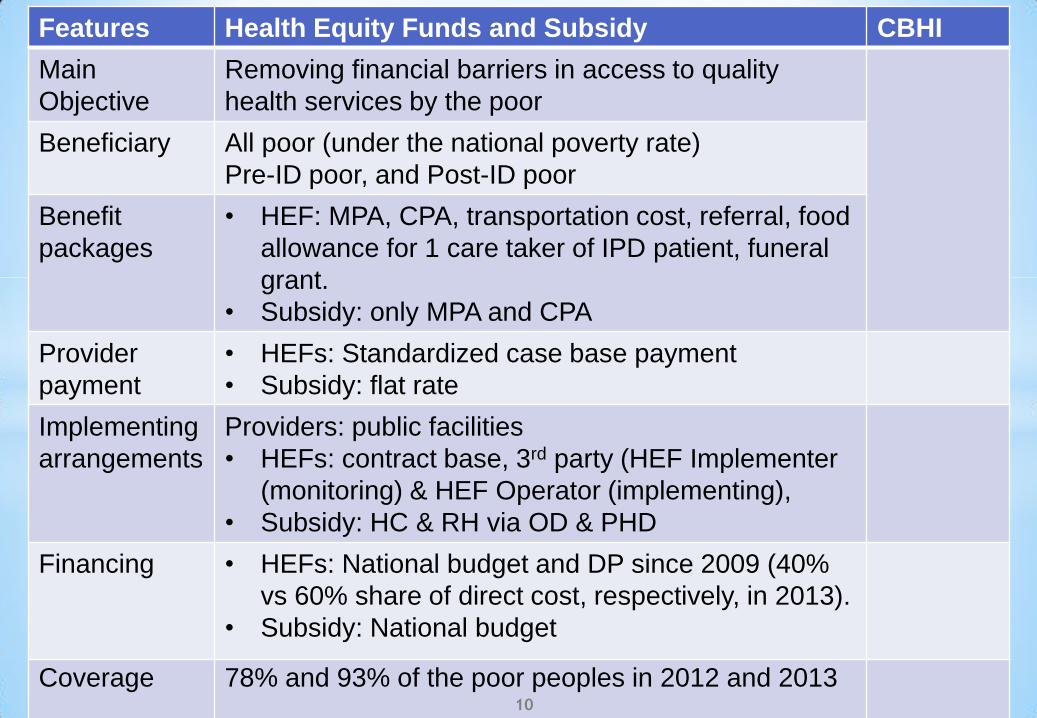
Features Health Equity Funds and Subsidy CBHI
Main
Objective
Removing financial barriers in access to quality
health services by the poor
Beneficiary All poor (under the national poverty rate)
Pre-ID poor, and Post-ID poor
Benefit
packages
• HEF: MPA, CPA, transportation cost, referral, food
allowance for 1 care taker of IPD patient, funeral
grant.
• Subsidy: only MPA and CPA
Provider
payment
• HEFs: Standardized case base payment
• Subsidy: flat rate
Implementing
arrangements
Providers: public facilities
• HEFs: contract base, 3rd party (HEF Implementer
(monitoring) & HEF Operator (implementing),
• Subsidy: HC & RH via OD & PHD
Financing • HEFs: National budget and DP since 2009 (40%
vs 60% share of direct cost, respectively, in 2013).
• Subsidy: National budget
Coverage 78% and 93% of the poor peoples in 2012 and 2013 10
MoH: Annual Performance Report 2012, Analyzed CSES 2004, 2007 and 2009 using methods developed by the
World Health Organization(MoH, WHO, GIZ). CDHS 2010. MoH, Health Financing Policy final draft. May 2013.
11
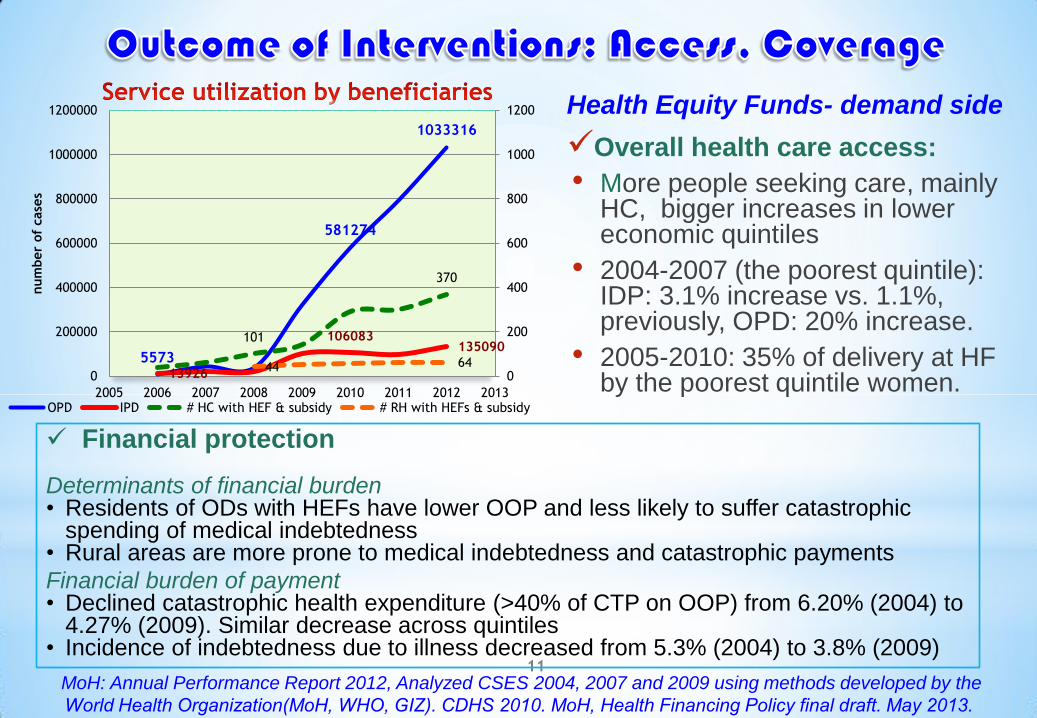
5573
581274
1033316
13926
106083 135090
101
370
44 64 0
200
400
600
800
1000
1200
0
200000
400000
600000
800000
1000000
1200000
2005 2006 2007 2008 2009 2010 2011 2012 2013
num
ber
of
case
s
OPD IPD # HC with HEF & subsidy # RH with HEFs & subsidy
Financial protection Determinants of financial burden • Residents of ODs with HEFs have lower OOP and less likely to suffer catastrophic
spending of medical indebtedness • Rural areas are more prone to medical indebtedness and catastrophic payments
Financial burden of payment • Declined catastrophic health expenditure (>40% of CTP on OOP) from 6.20% (2004) to
4.27% (2009). Similar decrease across quintiles • Incidence of indebtedness due to illness decreased from 5.3% (2004) to 3.8% (2009)
Health Equity Funds- demand side
Overall health care access:
• More people seeking care, mainly HC, bigger increases in lower economic quintiles
• 2004-2007 (the poorest quintile): IDP: 3.1% increase vs. 1.1%, previously, OPD: 20% increase.
• 2005-2010: 35% of delivery at HF by the poorest quintile women.
1. Epidemiological view point
•Despite significant reduction, maternal and child mortality in
Cambodia remain high if compared with countries in the
region.
•HIV/AIDS, TB and Malaria continue to pose a major public
health problem and require sophisticated clinical expertise
and considerable financial resources.
•The most important areas that deserve attention are non-
communicable and chronic diseases that increase burden on
health system - to provide better primary prevention, improve
detection and management, and improve treatment and care
for acute events- and other health related problems.
2. Health system perspective
• Improving equitable access to quality health services need to pay
attention to service delivery expansion and quality improvement, and
financial protection for the poor and vulnerable.
• Requiring considerable investment in physical infrastructure, medical
technology, ICT, clinical expertise.
• Adequate staffing and skills of health personnel, appropriate
remuneration and right incentive with improved accountability and
performance monitoring.
• licensing, accreditation, quality control mechanisms-well regulated
private sector participation linked to a national accreditation and quality
improvement system.
• Scaling up the coverage of Health Equity Funds, and integrating social
health protection mechanism by rationalizing, harmonizing and
transforming the existing financing schemes- Universal Health
Coverage.

Historical Development Process of Social Security for Formal Sector
The current Labour Law of Cambodia was passed in 1997 by
amending the 1992 Labor Law. The first Social Security Law was passed by the Parliament in
September 2002. In 2004 the ILO experts came to study the feasibility of the
scheme and the administrative design. In 2007 the sub-degree concerning the establishment of the
National Social Security Fund (NSSF) was adopted. NSSF was fully functional at end of 2008
Administration
Legal entity with autonomy in administration and self-
financing.
Administers the schemes of Social Security protection in
accordance with the National Social Security Law and the
provisions of the Social Security related Sub-Decrees.
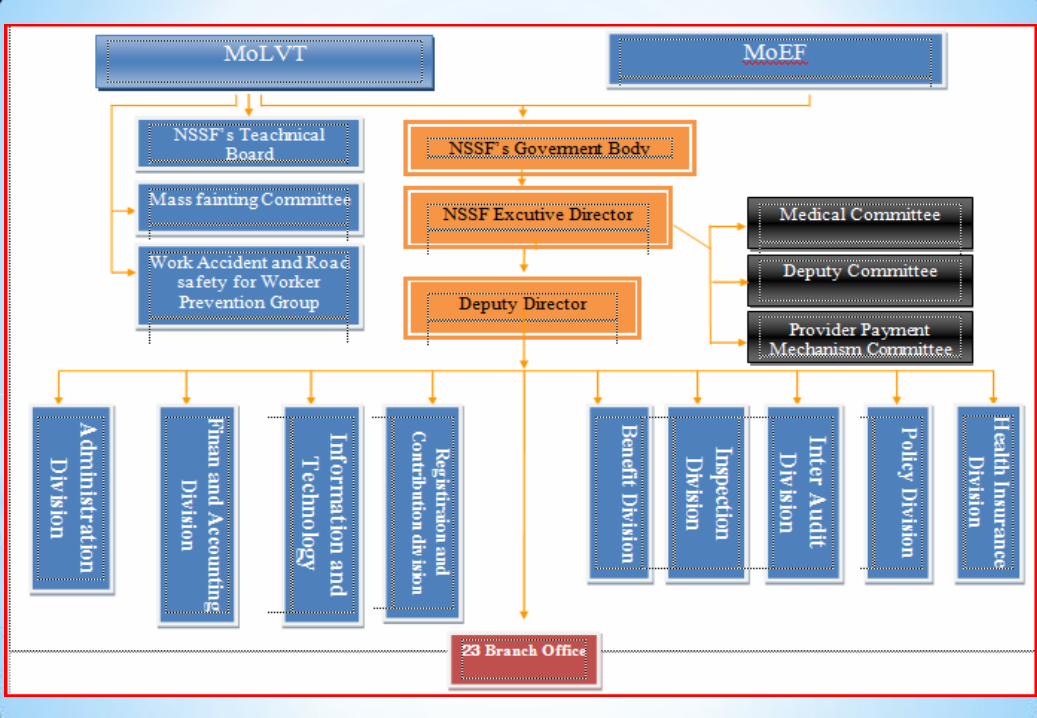
All technical issues are under the supervision of the Ministry
of Labor and Vocational Training (MoLVT), while the Ministry of
Economy and Finance (MEF) needs to approve all finance
related issues.
Role of the Governing Body
NSSF is guided and monitored by the Governing Body, which consists of a
tripartite representation of employers, employees, and the government.
The chairman of the board gets nominated by the Minister of Labor. The
NSSF Director is an ex-officio Member (automatic).
Other representatives get nominated by their related organization.
They must have never been convicted of misdemeanor or criminal
charges.
The chairman and members of the Governing Body except ex-officio
member (permanent member) are appointed by sub-degree for a 3-year
mandate issued by MoLVT as request from the organization they represent
*Member:
*1,019,130 Members (September of 2014)
*6,915 Employers
*Coverage in 24 Provinces
*Premium: Employers pay 0.8% of each average
staff’s salary.
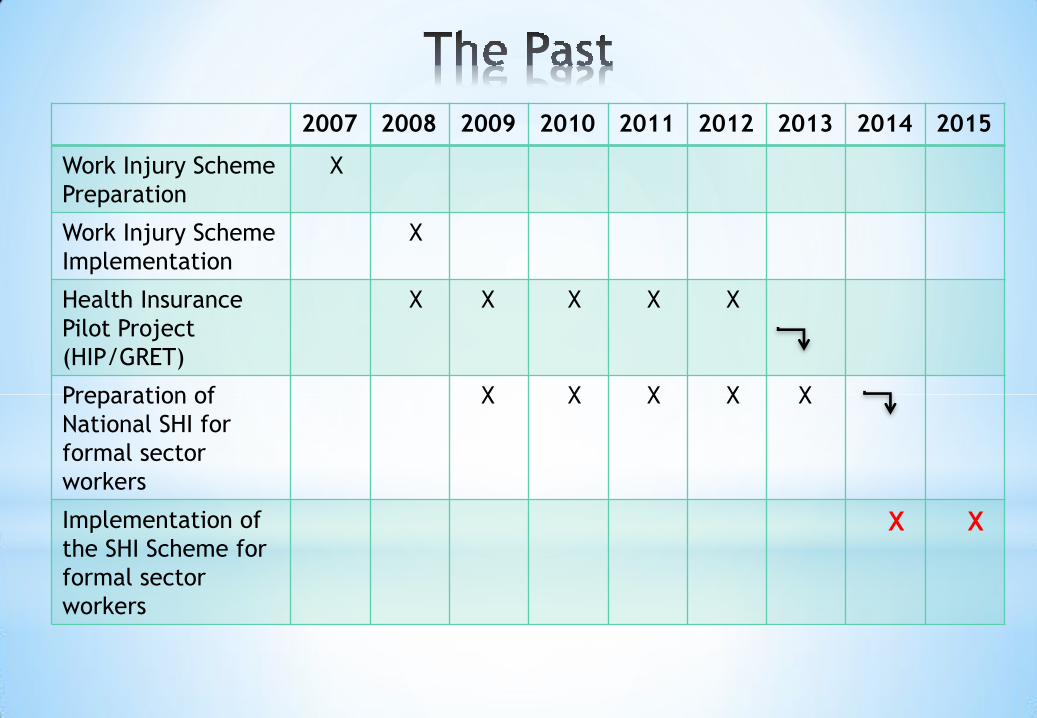
2007 2008 2009 2010 2011 2012 2013 2014 2015
Work Injury Scheme
Preparation
X
Work Injury Scheme
Implementation
X
Health Insurance
Pilot Project
(HIP/GRET)
X X X X X
Preparation of
National SHI for
formal sector
workers
X X X X X
Implementation of
the SHI Scheme for
formal sector
workers
X X
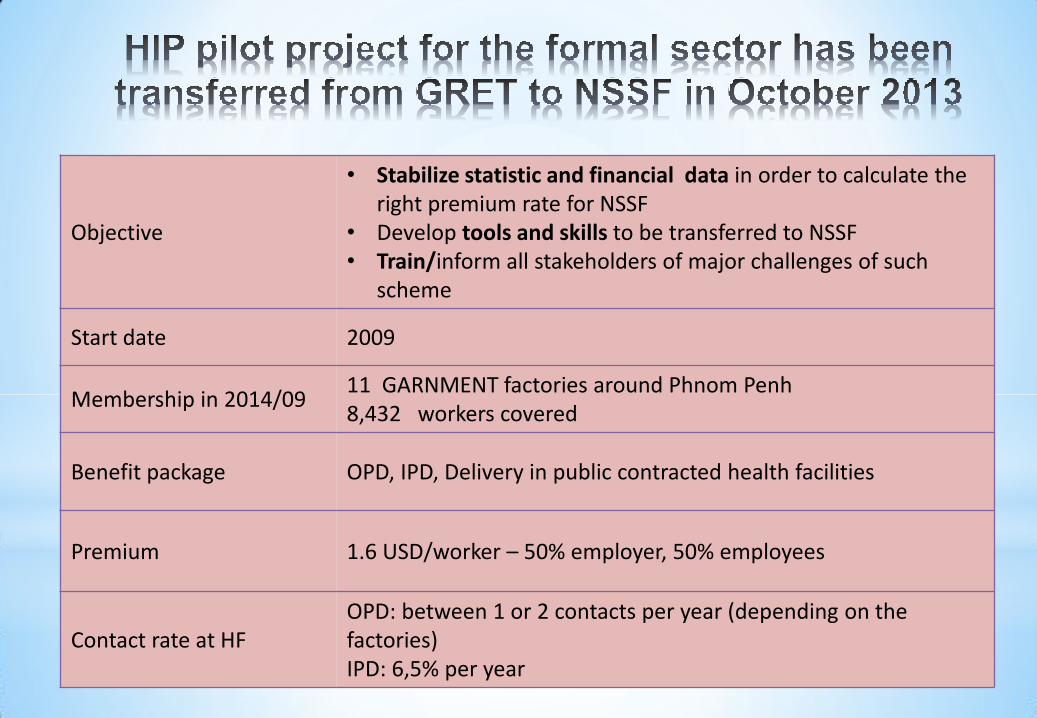
Objective
• Stabilize statistic and financial data in order to calculate the right premium rate for NSSF
• Develop tools and skills to be transferred to NSSF • Train/inform all stakeholders of major challenges of such
scheme
Start date 2009
Membership in 2014/09 11 GARNMENT factories around Phnom Penh 8,432 workers covered
Benefit package OPD, IPD, Delivery in public contracted health facilities
Premium 1.6 USD/worker – 50% employer, 50% employees
Contact rate at HF OPD: between 1 or 2 contacts per year (depending on the factories) IPD: 6,5% per year
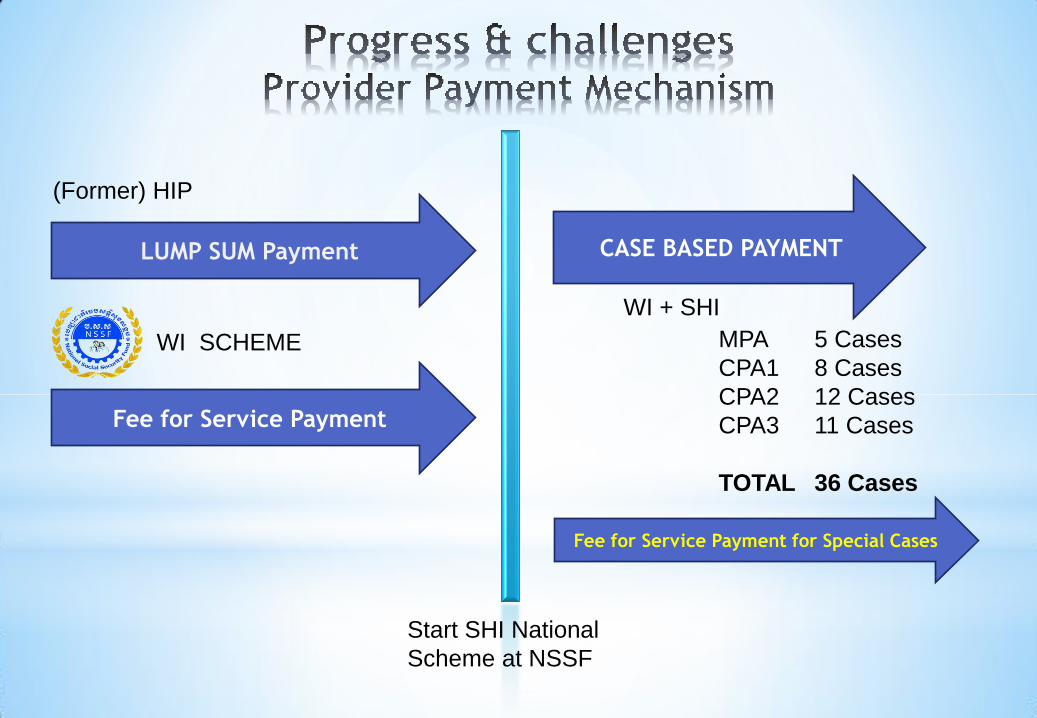
LUMP SUM Payment
(Former) HIP
Fee for Service Payment
WI SCHEME
CASE BASED PAYMENT
WI + SHI
Start SHI National
Scheme at NSSF
MPA 5 Cases
CPA1 8 Cases
CPA2 12 Cases
CPA3 11 Cases
TOTAL 36 Cases
Fee for Service Payment for Special Cases
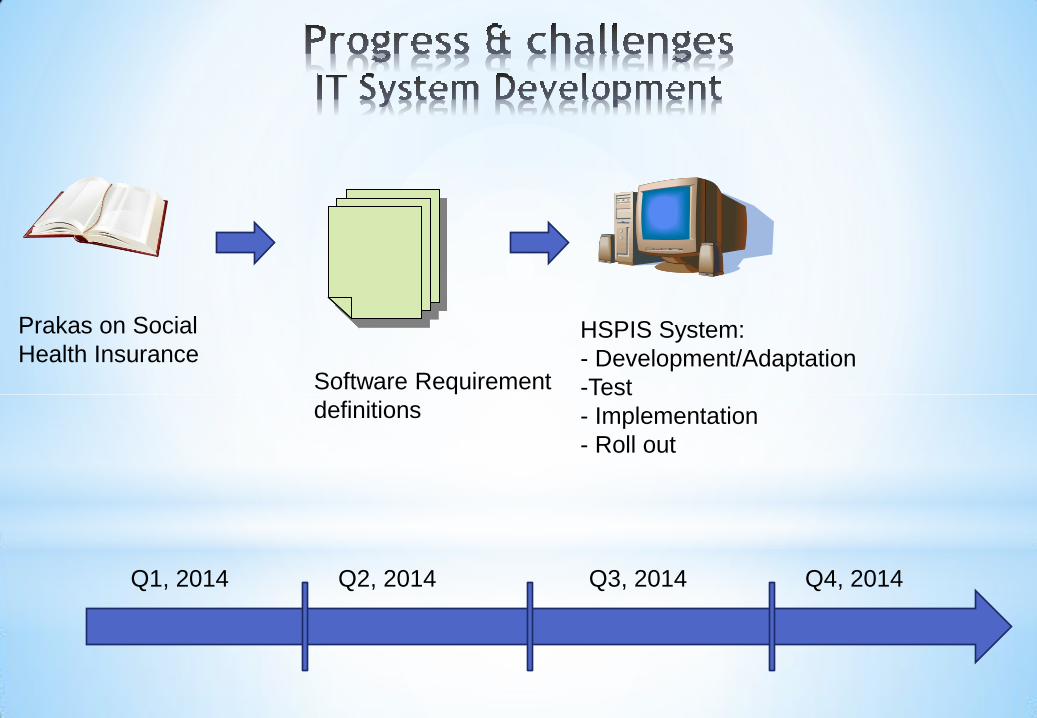
Prakas on Social
Health Insurance HSPIS System:
- Development/Adaptation
-Test
- Implementation
- Roll out
Software Requirement
definitions
Q1, 2014 Q4, 2014 Q3, 2014 Q2, 2014

SOUND HEALTH FINANCING STRATEGY IN THE CONTEXT OF PUBLIC FINANCIAL MANAGEMENT REFORM AND DECENTRALIUZATION & DECONCENTRATION
Moving forwards: Social health Protection
1. Financial risk
protection
2. Equitable and fair
funding
3. Efficiency of
service delivery
4. Quality services
5. Transparency
• Resource
mobilization
• Pooling: who will
manage them
• Purchasing: buy
services (supply or
demand)
• Stewardship:
regulation and
monitoring
1. Medium term
• Along policy
objectives and
Financing functions
2. Long term
Considering:
• UHC of Social
health Protection
Health Financing Strategic Components
• Institutions: NSSF (private sector), NSSF-C (civil servants), Informal
sector (MoH)--enrolment
• Universal population coverage: risk pooling and financial protection
against the cost of illness--
• Benefit package (criteria for quality of care)- risk pooling and financial
protection against the cost of illness
• Purchasing services: ensure quality of health services that are conducive for
good health while making optimal use of available resources
• Sources, level and management of funds: raise sufficient funds to allow for
the delivery of essential health services and enabling their purchase
• Regulation: ensure the delivery of quality health care and establishment of
rules and regulations with clarifications of stakeholders’ roles

• The Royal Government of Cambodia’s strong political
commitment to achieving MDGs, esp. reducing maternal
and childhood mortality and to reducing poverty and
development of social health protection.
• Evidence base policy interventions – country specific choices
• A combined set of both supply-side interventions (service readiness) and demand-side interventions (removing barriers in access to and utilization of health services, geographically, financially, bureaucratically).
• Technical & financial support of Development Partners
25

26