Embed Size (px)
Citation preview

INTERESTING CASE PRESENTATIONVCU MCV Grand Rounds
October 11, 2012
Amanda S. Tubbs M.D.

• 55yo M otherwise healthy• September 2009
• Diagnosed with achalasia after many years of progressive dysphagia, regurgitation, chest pains and wt loss (90 to 78kg)
• Laparoscopic Heller myotomy with Dor fundoplication
• December • Lost his job/insurance due to frequent hospitalizations• Presented to the VA with complaint that his symptoms
returned within a month of his surgery• Now only tolerating liquids

Heller Myotomy and Fundoplication

UGI- 3 months post-op

January 2010• GI and Surgery
• EGDs• Endoscopic pneumatic dilatation• Continued sx • Liquid diet
• PCP• URI symptoms• Palpable firm submandibular mass• FNA

Submandibular mass• FNA: squamous cell carcinoma• ENT consulted
• February left tonsil biopsied• Diagnosed with T2N1M0 tonsillar SCC• Underwent tonsillectomy, level II lymph node excisional biopsy left
neck• March PEG placed by GI• Ondontectomy x 10• April-May external beam radiation

August 2010

August 2010• Laparoscopic redo Heller myotomy, partial takedown
of wrap• Dor fundoplication sutures were cut individually to allow for
partial unwrapping of the fundoplication as well as visualization of the myotomy which was done and appeared to be about 6 cm in length
• Only able to pass a 42-French bougie• Myotomy extended both into the cardia and cephalad along
the esophagus

September 2010• Clinic c/o inability to take liquids & solids intermittently • Described a feeling of food sticking in upper pharynx and
difficulty chewing due to loss of teeth• Maintaining weight using ensure in gtube• CT results showing possible residual tonsillar cancer

October 2010-2011• PET likely some residual tonsillar disease• ENT: Laryngoscopy with biopsy
• Path: No cancer
• Continued sx: repeat EGD• Continued chronic dilatation of esophagus and stenosis of the LES• Pneumatic dilation and dilators • No relief• Gaining weight• Offered esophagectomy• Botox

April 2012• ED blood from PEG and dark stools x 1 week• Continued intermittent emesis/PO intolerance
• Dark bloody emesis, coffee ground appearance• Otherwise feeling great, 93kg
• Admitted to medicine• EGD: bleeding esophageal ulcer
• Biopsied• Injected with epinephrine

May 2012
• Biopsies: Moderately differentiated squamous cell carcinoma of the esophagus
• PET scan: Hypermetabolic mid esophageal lesion measuring maximum SUV 5.51• Bilateral hypermetabolic hilar and precarinal lymph nodes are cornering
for metastatic disease• New area of focally increased tracer accumulation in the left floor of the
mouth as described above, which may indicate recurrence of the patient's tonsillar cancer


June 2012• Med/Onc consulted- considering chemoradiation• EUS scope broken
• Referred to MCV in July for EUS• Staged as T3
• Proceeded with chemoradiation July• September repeat PET with increase tracer uptake in the
esophagus, decrease in the floor of the mouth

Surgical Oncology Clinic• CT reviewed



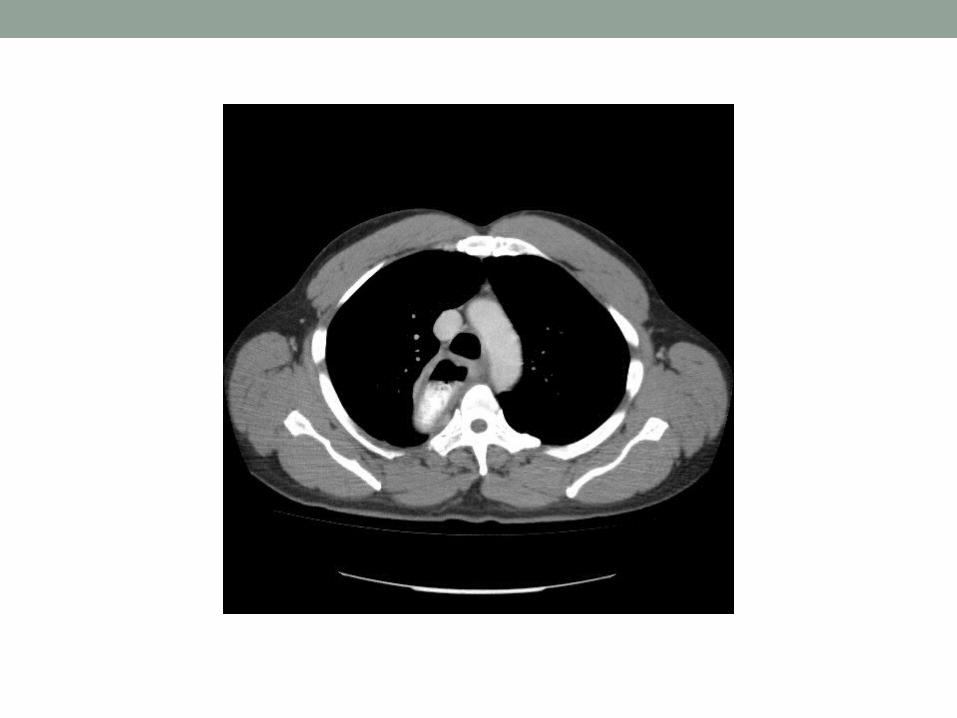
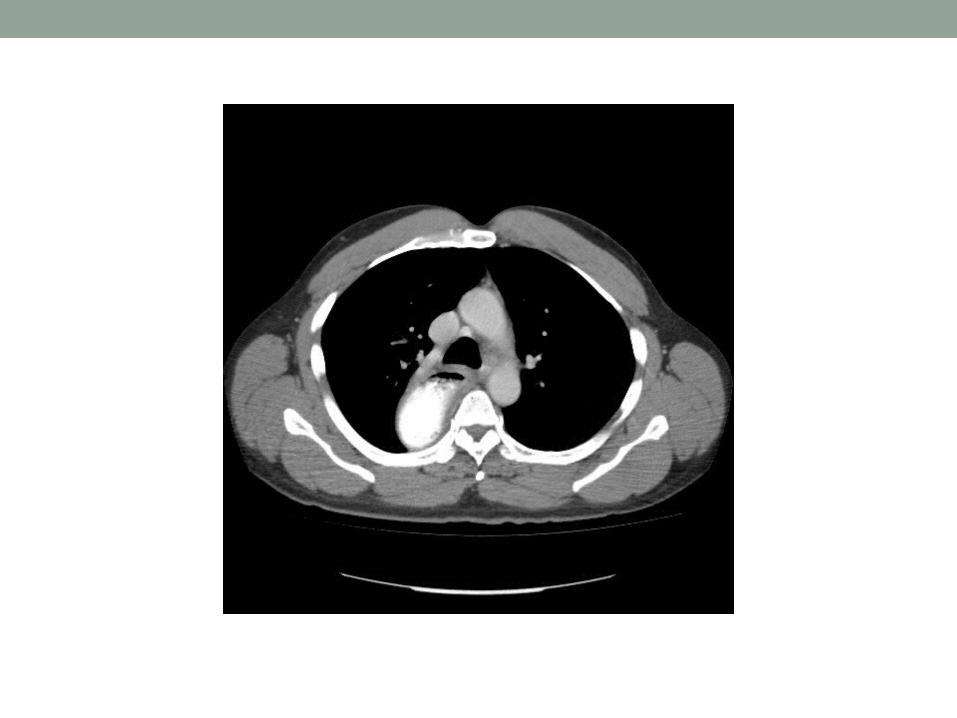










Cardiothoracic Surgery• Transthoracic esophagectomy • Intraop:
• No difficulties with intubation• Right thoracotomy• Extremely vascular megaesophagus about 8cm diameter• Mobilized and divided above the azygous vein which was
also divided• Stapled across at the hiatus• Very thickened edematous tissue• Mobilized as high as possible for cervical esophagostomy• Left neck esophagostomy

Incidence of SCC in Achalasia• Known complication of long-standing achalasia• Middle third of the esophagus • Frequently is reported as an incidental finding on pathology • Early abnormalities are obscured by retained food and
secretions, the presence of leukoplakia, and inflammatory changes of retention esophagitis, all of which are seen in long-standing disease
• Skinner and Belsey provide a concise but comprehensive review of malignancy secondary to achalasia• Belsey's personal series, the incidence of squamous cell cancer was 8%
(12 of 158 consecutive cases followed for more than 6 years)• All 12 cases were at middle third level, and only one patient survived
beyond 5 years

Indication for Esophagectomy in Achalasia
• Disabling obstruction with dysphagia and regurgitation refractory to treatment
• Intractable symptoms of painful retrosternal distress, acid regurgitation, and aspiration despite treatment
• Disabling GERD- intractable peptic ulceration, peptic stricture, and Barrett's esophagus
• Failure of esophagomyotomy• Sigmoid or Megaesophagus• Secondary motor disorder (scleroderma, Chagas disease)• Malignancy
Esophagomyotomy & Esophagectomy• Ruffato and colleagues, from Bologna, reported the long-term results of
extended esophagomyotomy reinforced with a Dor fundoplication• 173 patients, 68 were followed for more than 15 years• Subsequent esophageal cancer in four patients performed 27, 46, 96, and 144 months after
initial myotomy • Poor results were managed by additional surgery in 22 of these patients
• 15 of these 22, failed outcome was due to the development of disabling GERD• 7 of these 22 failures were patients with a grossly dilated sigmoid esophagus• 6 of these seven patients underwent esophagectomy (8%)
• Proposed that primary surgical treatment with esophagectomy may be a reasonable consideration when patients present with advanced degrees of esophageal dilatation and tortuosity

Esophagectomy• Franz Torek (1861–1938)• First esophagectomy for cancer in
1913• 67-year old lady, not only survived
the operation, but also lived without recurrence for 13 years
• 20 years before two surgeons, Garlock and Sweet, were able to report another esophagectomy according to the Torek technique, however, with restoration of the continuity by esophago-gastrostomy

Esophagectomy• Ivor-Lewis• 1950’s• Right thoracotomy with laparotomy
• McKeown • Triple-incision

Esophagectomy• Marc Orringer• 1978 “Esophagectomy without thoracotomy”• AATS Meeting in New Orleans
• Ronald Belsey started the discussion by saying that he was very interested in Orringer's ‘essay on BLIND surgery and his expedition into the DARK AGES’
The original Friedrich-von Petz stapler for gastrointestinal surgery (1934)

Reconstruction• Goal: Restore the elements of normal esophageal function
• Swallow a normal diet comfortably• Retain ability to burp or vomit• Minimize potential for reflux, regurgitation, and aspiration
• Select a conduit that provides minimal morbidity and operative mortality
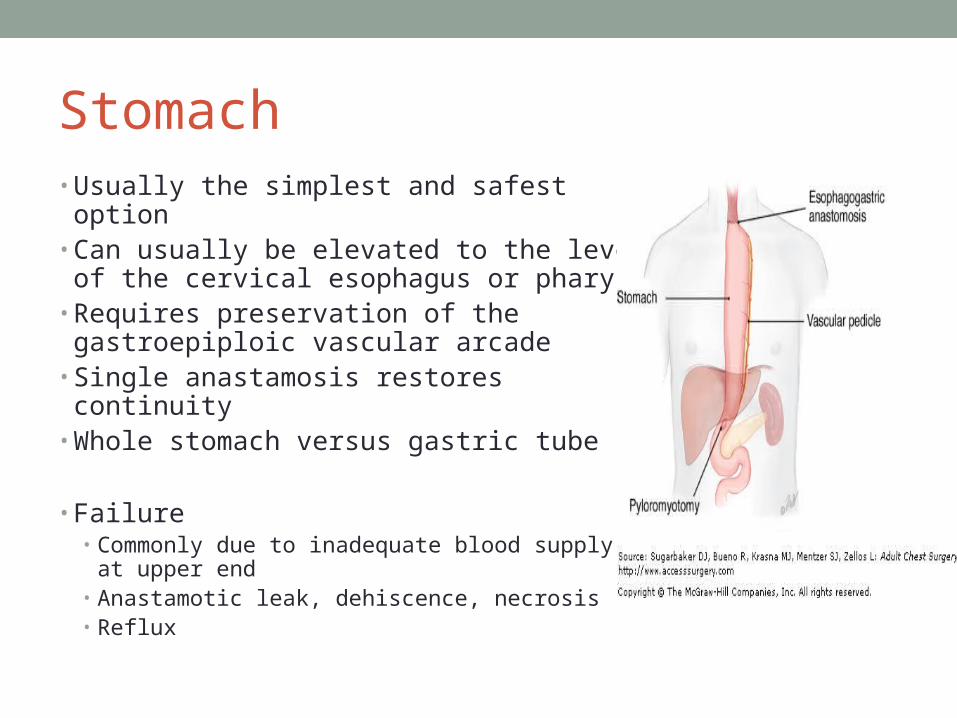
Stomach• Usually the simplest and safest option• Can usually be elevated to the level of
the cervical esophagus or pharynx• Requires preservation of the
gastroepiploic vascular arcade• Single anastamosis restores continuity• Whole stomach versus gastric tube
• Failure• Commonly due to inadequate blood supply at
upper end• Anastamotic leak, dehiscence, necrosis• Reflux


Jejunum• More difficult owing to the complexity of the mesenteric
arcade• Long segments are difficult to fashion without significant
angulation and redundancy• Interposed segment requires 3 anastamoses


Colonic interposition• More versatile and robust• Left colon
• Preserve vascular arcade between the upper left colic and right colic vessels
• Ligate middle colic main branch • Marginal artery is inadequate or missing ~5%• Diverticular disease, stricture, atherosclerosis of the IMA, IMV/splenic
vein thrombosis• Right colon
• More difficult due to bulkier mesentery, larger bowel lumen and thinner bowel wall
• May not reach unless the IC valve and TI are included• Requires 3 anastamoses• Can stretch and become redundant requiring resection


Reconstruction• Posterior mediastinal
• Native space• Infectious, oncological or previous dissection
• Substernal • Plane dissected just behind the sternum• Higher leak rates?
• Subcutaneous• Between the sternum and skin
• Transpleural• Left pleural cavity

Complications• Anastamotic leak• Anastamotic stricture• Recurrent laryngeal nerve
injury• Respiratory
complications/failure• Bleeding• Chyle leak• Impaired conduit emptying• Local recurrence
JD• Postoperative course• Reconstruction

References• Ruffato A, Mattioli S, Lugaresi ML, et al: Long-term results after Heller-Dor operation for
oesophageal achalasia. Eur J Cardiothorac Surg 29:914–9, 2006. [PubMed: 16675239]• Glatz SM, Richardson JD: Esophagectomy for end stage achalasia. J Gastrointest Surg 11:1134–
7, 2007. [PubMed: 17623258]• Pearson FG. Chapter 21. Options for Esophageal Replacement. In: Sugarbaker DJ, Bueno R,
Krasna MJ, Mentzer SJ, Zellos L, eds. Adult Chest Surgery. New York: McGraw-Hill; 2009.http://www.accesssurgery.com/content.aspx?aID=5286927. Accessed October 10, 2012.
• Naef, A. The mid-century revolution in thoracic and cardiovascular surgery: Part 3. Interact CardioVasc Thorac Surg (2004) 3 (1): 3-10. doi: 10.1016/j.icvts 2003.12.003
• Barkley, C, Orringer, M, et al: Challenges in Reversing Esophageal Discontinuity Operations. Ann Thoracic Surg 2003;76;989-95.