Embed Size (px)
Citation preview

CASE PRESENTATION
By
Omar Rashid, MD, JD
VCU/MCV
Department of Surgery

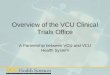
42yr female h/o HTN, protein S def, TIAs x 5, on the OBGYN service w Abd/Pelvis pain for which she underwent an MRI.
4.7cm x 4cm x 3.5cm complex collection





INTERVAL Hx
EUA Path
REPEAT IMAGING
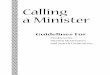
RESECTION

Cephalad

Cephalad

Cephalad
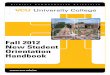
RECTUM
Coccyx


Anatomy

Epidemiology• Rare• 1 – 6 annually diagnosed at major referral centers
» Dunn, 2010
• Incidence estimated at 1:40,000 patients in major referral center.
» Whittaker and Pemberton, 1938
• 50 cases at Cleveland clinic over 50 year period.» Grundfest-Broniatowski et al., 1990
• 39 malignant tumors seen at Memorial-Sloan Kettering over 28 years.
» Cody et al., 1981

Presentation
• Usually incidental finding on pelvic/rectal examination in asymptomatic patients.
• Pain: more common in malignant lesions» Jao et al., 1985
• Recurrent infection; repeated operations for “perirectal abscess/fistula in ano”.
» Singer et al., 2003
• Rectal complaints: sensation of rectal fullness, incomplete evacuation, constipation.
• Headache with straining and during intercourse in women with meningocele.
• Urinary dysfunction


Diagnosis
• Physical Exam:– Inspection: Postanal dimple
suggestive of developmental cyst communicating with the skin. Laxity of sphincter indicates sacral nerve involvement.
– Digital rectal examination: mass displacing rectum anteriorly; smooth intact mucosa.
– Sigmoidoscopy: Typically normal, edema suggestive of infected cyst.

Imaging
• Plain film: “scimitar” sacrum indicates presence of anterior meningocele; bony destruction indicates malignant process.

Imaging• CT scan: Useful in identifying small tumors,
distinguishing solid and cystic lesions, and assessing for invasion of adjacent structures.

Imaging
• MRI: More detailed than CT, useful in delineating nerve/bone involvement in pre-operative planning.

Imaging
• Endorectal ultrasound: May demonstrate rectal wall invasion and differentiate solid from cystic lesions.

To Biopsy or Not…???
• Biopsy of presacral lesions controversial:
Advantages
Tissue diagnosis
Disadvantages
Fistula, Abscess, Tumor Seeding, Meningitis
Always posterior (not transrectal)

Surgical Indication
Resection recommended for all retrorectal tumors:Symptoms worsen with increasing size of lesion.Cystic lesions may become infected, making surgical management difficult.Solid lesions have high malignant potential.Untreated meningocele has high mortality secondary to infection.

Operative Strategies
Operative approach dictated by size and location of lesion:
Abdominal
Posterior
Anteroposterior

• If proximal extent of tumor can be felt on digital exam, posterior approach feasible.
• If ½ of tumor can be palpated, posterior approach may be possible.
• If <1/2 of tumor palpated, anterior or combined approach recommended.

Anterior ApproachAbdomen entered through
midline incision.
Sigmoid colon mobilized and retrorectal space entered anterior to parasympathetics.
Ligation of middle sacral vessels.
Tumor dissected free of surrounding structures.
Rectal involvement may necessitate proctectomy.

Sacral involvement may necessitate sacrectomy through combined anterior/posterior approach. Posterior approach allows for better visualization of sacral nerve roots.
Distal sacral vertebrae and nerve roots can be sacrificed bilaterally without significant functional impairment. S3 nerve root must be preserved unilaterally to preserve continence.

Incision may be paracooccygeal, midline, or transverse depending on surgeon preference.Anococcygeal ligament and pubococcygeus divided and coccyx disarticulated.Cyst dissected free of surrounding structures. En bloc resection with coccyx reduces recurrence rate.
Posterior Approach



Questions???