Embed Size (px)
Citation preview

R. Phillip Dellinger, MD, Section EditorConcise Definitive Review
Intensive care unit management of intra-abdominal infection
John C. Marshall, MD; Marilyn Innes, MD
I ntra-abdominal infections are animportant cause of intensive careunit (ICU) morbidity and mortal-ity. Approximately 30% of patients
admitted to an ICU with intra-abdominalinfection succumb to their illness, andwhen peritonitis arises as a complicationof a previous surgical procedure (1, 2), orrecurs during ICU admission (3), mortalityrates exceed 50%. Moreover, their morbid-ity is substantial. Multiple organ dysfunc-tion syndrome was originally described as acomplication of intra-abdominal infection(4, 5), and the association between occultintraperitoneal infection and organ dys-function was deemed sufficiently strong tojustify empiric laparotomy for the patientwith worsening organ dysfunction but nodefined focus of infection (6). The manage-ment of the critically ill patient with intra-abdominal infection can be alternativelygratifying and frustrating for the inten-
sivist. We will review the biologic, clinical,diagnostic, and therapeutic features of thisheterogeneous disorder.
Biologic Considerations
The abdominal cavity is lined by a me-sothelial membrane, the peritoneum,which covers the abdominal viscera andcreates a potential space—the peritonealcavity. The area posterior to the perito-neal cavity is known as the retroperito-neum; its anatomic contents include thekidneys, pancreas, great vessels, and theposterior aspects of portions of the gas-trointestinal tract, specifically the duode-num, ascending and descending colons,and rectum. In health, the peritoneal cav-ity contains �100 mL of peritoneal fluidcontaining scattered macrophages andlymphocytes (7). This fluid circulatesthroughout the peritoneal cavity, drawnby the negative pressures generated bydiaphragmatic contraction upward to-ward specialized fenestrae in the dia-phragmatic peritoneum that, in turn,drain into the lymphatic system (8).
Inflammatory stimuli within the peri-toneal cavity evoke a vigorous inflamma-tory response, with increased vascularpermeability, outpouring of protein-richfluid containing cytokines and chemo-kines (9, 10), and the influx of inflamma-tory cells, particularly monocytes and
neutrophils (11, 12). The activation of aninflammatory response induces tissuefactor expression on peritoneal macro-phages, activating the coagulation cas-cade and resulting in accelerated gener-ation of fibrin that polymerizes to formadhesions and the capsule of an abscess(13, 14). The peritoneum is richly en-dowed with somatic nerve fibers; thus,the onset of peritonitis invokes severepain, localized to the anatomic site ofmaximal inflammation and aggravated bystimuli that result in movement of theperitoneum (the biologic basis for clinicaltests to evoke rebound tenderness). Thenormal innate immune response of theperitoneal cavity is rapid and effective;however, there is evidence that thephagocytic capacity of the neutrophil isimpaired in patients with complicatedperitonitis (15) and that defense mecha-nisms such as fibrin deposition can im-pede microbial clearance (16).
Infections within the peritoneal cavitymost typically arise as a consequence ofdisruption of the adjacent gastrointesti-nal tract, with spillage of the indigenousflora into the peritoneal space. This florais enormously complex and variablethroughout the gastrointestinal tract. Inhealth, the stomach and duodenum aresterile or only sparsely populated withGram-positive organisms, lactobacilli,
From the Department of Surgery and the Interde-partmental Division of Critical Care Medicine, Univer-sity of Toronto; and the Toronto General Hospital,University Health Network, Toronto, Canada.
Address requests for reprints to: John C. Marshall,MD, Eaton North 9-234, Toronto General Hospital,University Health Network, 200 Elizabeth Street, To-ronto, Ontario, Canada M5G 2C4. E-mail:[email protected]
Copyright © 2003 by Lippincott Williams & Wilkins
DOI: 10.1097/01.CCM.0000087326.59341.51
Objective: To review the biologic characteristics of, and man-agement approaches to, intra-abdominal infection in the criticallyill patient.
Design: Narrative review.Setting: Medline review focussed on intra-abdominal infection
in the critically ill patient.Patients and Subjects: Restricted to studies involving human
subjects.Interventions: None.Results: Intra-abdominal infections are an important cause of
morbidity and mortality in the intensive care unit (ICU). Peritonitiscan be classified as primary, secondary, or tertiary, the uniquepathologic features reflecting the complex nature of the endoge-nous gut flora and the gut-associated immune system, and thealterations of these that occur in critical illness. Outcome is
dependent on timely and accurate diagnosis, vigorous resuscita-tion and antibiotic support, and decisive implementation of opti-mal source control measures, specifically the drainage of ab-scesses and collections of infected fluid, the debridement ofnecrotic infected tissue, and the use of definitive measures toprevent further contamination and to restore anatomy and func-tion.
Conclusions: Optimal management of intra-abdominal infec-tion in the critically ill patient is based on the synthesis ofevidence, an understanding of biologic principles, and clinicalexperience. An algorithm outlining a clinical approach to the ICUpatient with complex intra-abdominal infection is presented. (CritCare Med 2003; 31:2228–2237)
KEY WORDS: intra-abdominal infections; morbidity; mortality;multiple organ dysfunction syndrome; peritonitis
2228 Crit Care Med 2003 Vol. 31, No. 8

and, occasionally, Candida (17). Both thevariety and the density of this flora in-crease more distally. Gram-negative or-ganisms are encountered in the proximalsmall bowel, and anaerobes are encoun-tered in the distal small bowel and colon.In total, as many as 600 separate micro-bial species comprise the indigenous floraof the healthy adult, and bacteria are sonumerous that they outnumber humancells of the body by a factor of 10:1 (18).Despite the variety of organisms presentwithin the lumen of the gastrointestinaltract, intraperitoneal infections arising asa result of a breach of gut integrity typi-cally yield a mixed flora whose composi-tion, though complex, is quite predictable(Table 1). Animal models have shownthat differing groups of organisms makedifferential contributions to the outcomeof infection: Gram-negative aerobic or-ganisms are associated with acute lethal-ity, whereas anaerobic flora contributesto abscess formation (19).
The anaerobic flora of the normal gutalso plays an important role in the main-tenance of stable patterns of intestinalmicrobial colonization, a phenomenonknown as “colonization resistance” (20).In experimental animals, ablation of theanaerobic flora of the cecum by oral an-tibiotics such as clindamycin or penicillinresults in a 5-log increase in numbers ofcecal Escherichia coli and translocationof E. coli to adjacent mesenteric lymphnodes in essentially all animals (21).Studies in humans show that the use ofantibiotics with anti-anaerobic activitycan promote gut colonization with Can-dida (22, 23) and vancomycin-resistantEnterococci (24); these effects are partic-ularly prominent when normal coloniza-tion resistance has been disrupted (23).Such changes in the composition of the
normal intraluminal flora can occur overtime in the critically ill patient (25) andexplain the typical flora seen in cases ofrecurrent or tertiary peritonitis discussedin greater detail below.
Although intra-abdominal infectionsare typically polymicrobial, the composi-tion of the infecting flora is influenced bythe clinical setting. Enterococci are iso-lated more frequently in patients withpostoperative peritonitis than in patientswith intra-abdominal abscesses develop-ing outside the hospital (26), and nasalcolonization with methicillin-resistantStaphylococcus aureus is a risk factor forthe acquisition of intra-abdominal methi-cillin-resistant S. aureus infection (27).
An acute loss of the integrity of thegut wall—for example, after perforationof an ulcer or an uninflamed diverticu-lum, disruption of an anastomosis, ortraumatic perforation of the intestine—results in spillage of intestinal contentsinto the peritoneal cavity and producesgeneralized peritonitis. More commonly,however, the leakage of gut contents is aslow process, accompanied by an inflam-matory response in the surrounding tis-sues, as encountered, for example, in per-forated appendicitis or a postoperativeabscess arising from residual intraperito-neal bacteria or a small anastomotic leak.The result of this interaction between theinfecting bacteria and the defenses of theperitoneal cavity is the formation of anabscess that walls off the infectious in-sult. The abscess lies adjacent to the siteof contamination or in a dependent loca-tion such as the pelvis or subhepaticspace.
Infection within the peritoneal cavityor retroperitoneum evokes a vigoroussystemic response, reflected in elevatedlevels of circulating inflammatory medi-
ators such as tumor necrosis factor andinterleukin-6 (28, 29) and the clinical se-quelae of acute organ system dysfunction(30, 31).
Classification and ClinicalFeatures
Peritonitis can be classified as pri-mary, secondary, and tertiary. Primaryperitonitis, also known as spontaneousbacterial peritonitis, is peritonitis arisingin the absence of a breach of the perito-neal cavity or gastrointestinal tract. Pri-mary peritonitis can arise in otherwisehealthy young girls, in whom the Pneu-mococcus is the typical infecting bacte-rium. In the critically ill patient, it ismost commonly seen in the decompen-sated cirrhotic patient, and it often pre-sents with an acute deterioration in oth-erwise stable advanced liver disease (32,33). Infection is thought to reflect thetranslocation of enteric bacteria across ananatomically intact gut wall, promoted,perhaps, by abnormal overgrowth of or-ganisms in the proximal small bowel (34,35). The infection is characteristicallymonomicrobial, with enteric Gram-negatives and enterococci being the mostcommon isolates; Gram-positive cocciare particularly prevalent when the infec-tion arises in an ICU patient (36) (Table1). Methicillin-resistant S. aureus is acommon isolate when primary peritonitisoccurs as a nosocomial infection in ahospitalized cirrhotic patient (37). Phys-ical findings may be minimal; the diag-nosis can be established by culture of anaspirate of the peritoneal fluid and is sug-gested by demonstration of �500 whitecells/mm3 of ascitic fluid, increased lac-tate, or a reduced glucose, and a declinein polymorphonuclear cell counts to�250 cells/mm3 is associated with suc-cessful resolution (38). Primary peritoni-tis is treated with systemic antibioticsappropriate for the infecting flora, al-though there is no convincing evidencefor the superiority of one regimen overanother nor even for the utility of sys-temic antibiotics at all (39). Mortality isincreased for patients admitted to an ICU(40).
Secondary peritonitis is peritonitis oc-curring as a consequence of egress of gutorganisms through a physical hole in thegastrointestinal tract or through a ne-crotic gut wall (41, 42). Its flora is typi-cally polymicrobial, including both aer-obes and anaerobes when the distalgastrointestinal tract is the site of the
Table 1. Microbiology of peritonitis
Primary Peritonitis Secondary Peritonitis Tertiary Peritonitis
Gram-negative bacteria Gram-negative bacteria Gram-negative bacteriaEschecheri coli E. coli 32–61% PseudomonasKlebsiella Enterobacter 8–26% Enterobacter
Klebsiella 6–26% AcinetobacterProteus 4–23%
Gram-positive bacteria Gram-positive bacteria Gram-positive bacteriaS. aureus Enterococci 18–24% EnterococciEnterococci Streptococci 6–55% Coagulase-negative
Staphylococci 6–16% StaphylococciAnerobic bacteria
Bacteroides 25–80%Clostridium 5–18%
Fungi 2–15% FungiCandida
2229Crit Care Med 2003 Vol. 31, No. 8

perforation (43). In contrast, anaerobesare unusual isolates from perforations ofthe stomach or duodenum. It is impor-tant to keep in mind that secondary peri-tonitis can occur in the cirrhotic patient:a polymicrobial culture, or the presenceof anaerobes in the aspirate, suggest thediagnosis of secondary peritonitis (44).
The typical clinical presentation iswith abdominal pain and tenderness withsigns of peritoneal irritation on physicalexamination. Diffuse pain suggests gen-eralized peritonitis, whereas localizedpain suggests a walled-off process arisingfrom an organ in the immediate ana-tomic vicinity. In the young, otherwisehealthy patient, diagnosis is generallystraightforward. However, in the elderlyor medically compromised patient, theclinical presentation may be quite subtle.Corticosteroids can blunt the inflamma-tory response of the peritoneum and somask the clinical signs. In the patientwith an altered level of consciousness—the sedated patient receiving mechanicalventilation, for example—the only evi-dence of a treatable but life-threateninginfection may be an unexplained septicresponse or an unanticipated deteriora-tion of organ system function.
Tertiary peritonitis is peritonitis in thecritically ill patient that persists or recursat least 48 hrs after the apparently ade-quate management of primary or second-ary peritonitis. Differentiation of this en-tity from secondary peritonitis underlinesits strikingly different microbiologic fea-tures and its generally unsatisfying re-sponse to antibiotics and surgical sourcecontrol measures (45, 46). The microbialflora isolated in tertiary peritonitis isdominated by organisms such as coagu-lase-negative Staphylococci, Pseudomo-nas, Candida, and the enterococcus (3,47) (Table 1). These same species are thedominant floras of the upper gastrointes-tinal tract of the critically ill patient andcommon causes of nosocomial ICU-acquired infection (25, 48). Their preem-inence in tertiary peritonitis suggests arole for bacterial translocation, aided byantibiotic pressures, in the pathogenesisof the disease. The mortality for patientswith tertiary peritonitis is significant,typically in excess of 50%, and optimaltherapeutic strategies are not well de-fined (49).
Diagnosis
Intra-abdominal infection can be par-ticularly difficult to diagnose in the crit-
ically ill patient because an informativehistory is usually unobtainable, and find-ings on physical examination are maskedby changes in level of consciousness.Thus, the diagnosis depends on consider-ation of the clinical setting, the develop-ment of otherwise unexplained signs ofsepsis or organ dysfunction, and defini-tively on the results of radiographic ex-amination (50).
The common causes of secondary bac-terial peritonitis of sufficient severity tonecessitate ICU admission are relativelyfew (Table 2). Perforation of the uppergastrointestinal tract secondary to ulcerdisease or of the lower gastrointestinaltract secondary to diverticular disease orcancer are among the most commoncauses of severe intra-abdominal infec-tion. In the trauma patient, occult injuryto the gut can result in delayed onset ofperitonitis. Gut ischemia secondary to ar-terial intrinsic vascular disease, a low-flow state, or strangulation of obstructedbowel is a relatively common and poten-tially devastating cause of intra-abdomi-nal infection (51, 52). Mesenteric arterialembolism should be suspected in the pa-tient with a potential source of emboli—for example, the patient with atrial fibril-lation, a recent myocardial infarct, or arecent invasive vascular imaging proce-dure. Mesenteric arterial thrombosis typ-ically occurs in the patient with evidenceof peripheral vascular disease at othersites, whereas a history of thrombotic dis-orders should suggest the diagnosis ofmesenteric venous thrombosis. Left-colon ischemia is a relatively commoncomplication of emergency abdominalaortic aneurysm repair and occurs be-cause the inferior mesenteric artery isligated during repair of the aneurysm,rendering the left colon it suppliesacutely ischemic. Previous abdominalsurgery suggests the possibility of an
anastomotic leak, an intra-abdominal ab-scess, or inadvertent and undetected in-jury to the bowel (e.g., caused duringclosure of the abdominal wall). Superin-fection commonly complicates the courseof severe necrotizing pancreatitis.
The clinical manifestations of intra-abdominal infection include the other-wise unexplained development of organsystem dysfunction. The differential diag-nosis of unanticipated shortness of breathor new onset of a supraventricular dys-rhythmia arising 3 or 4 days after anabdominal operation includes anasto-motic leakage or other intra-abdominalinfectious pathology, and the diagnosisshould be excluded with the appropriateimaging procedures. New onset of renaldysfunction or elevation of the bilirubinand transaminase levels is also suggestiveof occult intra-abdominal infection.Blood cultures are often negative; in fact,it has been suggested that the absence ofbacteremia in a febrile surgical patientincreases the likelihood of intra-abdomi-nal infection (53). However, polymicro-bial bacteremia (54) or anaerobic bacte-remia should also raise the possibility ofintraperitoneal infection.
Radiographic imaging is the definitivediagnostic approach to patients with sus-pected intra-abdominal infection and canusually characterize the problem beforeplanned intervention (55). Plain filmsmay reveal intraperitoneal free air, bowelobstruction, or subtle signs of intestinalischemia. Contrast studies performed us-ing water-soluble agents can discloseleaks; injection of contrast into drains,fistulas, or sinus tracts can aid in delin-eation of the anatomy of complex infec-tions and help to monitor the adequacy ofabscess drainage.
Ultrasonography performed in the ICUhas the advantage of being portable, andit is an excellent technique for identifying
Table 2. Common causes of intra-abdominal infection in patients in the intensive care unit
Perforation of GI tract Diverticular disease
Peptic ulcer: duodenal, gastricTraumatic: penetrating or bluntIschemicMalignant
Visceral ischemia Small bowel, colon from embolismThrombosis, low-flow state, strangulationGall bladder cholecystitis
Postoperative complication Anastomotic leakIntra-abdominal abscess
Solid organ abscess LiverSpleen
GI, gastrointestinal.
2230 Crit Care Med 2003 Vol. 31, No. 8

intra-abdominal abscesses, detecting freefluid, and evaluating the biliary tree.However it is operator dependent and dif-ficult to perform in patients who haveabdominal dressings or paralytic ileus.Ultrasonography can also be used to as-pirate or drain intra-abdominal fluid col-lections and to obtain fluid for cultureand sensitivity.
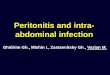
The standard technique for the evalu-ation of the abdomen in the critically illpatient is computerized tomography (CT)(56, 57). With the combined use of intra-venous and oral or rectal contrast, mostcauses of secondary peritonitis can bereadily diagnosed. Abnormal collectionsin the peritoneal cavity or retroperito-neum are readily evident, and infection issuggested by demonstration of intracavi-tary air, inhomogeneity of contents, orthe characteristic rim enhancement of anabscess capsule (Fig. 1, top); inflamma-tion is further suggested by edema andstranding of the mesenteric fat. The CTscan may also show extraluminal passageof contrast medium, indicating a leak, orbowel distension and a point of narrow-ing, indicating an area of obstruction.
Ischemia is suggested by the presence ofgas within the wall of the bowel (pneu-matosis) or mesenteric vasculature (Fig.1, bottom) or the absence of tissue per-fusion; occasionally, an obstructing clotcan be seen. The CT scan is an invaluablediagnostic tool, but it does necessitatetransfer of a potentially unstable patientfrom the ICU. Moreover, radioiodinatedcontrast agents can aggravate renal dys-function, although one report suggeststhat the severity of the injury can beattenuated by premedication with acetyl-cysteine (600 mg, twice daily) (58). Renaldysfunction or paralytic ileus are relativecontraindications to CT scanning; therisks must be weighed against the poten-tial benefits.
Radionuclide scans have only a verylimited role in the diagnosis of intra-abdominal infection in the critically illpatient because they lack specificity anddo not permit image-guided managementof any collections that are found. Thelogistic challenges of transferring a crit-ically ill patient to a magnetic resonanceimaging facility render this test imprac-tical in most circumstances.
Finally, intra-abdominal infection canoften be demonstrated by more invasiveinterventions performed within the ICU.Judicious probing of surgical woundswith a sterile culture swab or a glovedfinger can often identify collections ofinfected material immediately adjacent tothe incision. Diagnostic peritoneal lavageperformed in the ICU may reveal bacteriaand white cells, bile, and intestinal con-tents (59); a bloody lavage return sug-gests the diagnosis of acute intestinalischemia. Laparoscopic evaluation of theperitoneal cavity can be performed at thebedside in the ICU (40) and has beenreported to reduce the need for unnec-essary laparotomy (60). However lapa-roscopy also requires an adequatelyequipped operating suite, and it usuallynecessitates transfer of the patient fromthe ICU. Moreover, adhesions from pre-vious surgery or infection may makevisualization more difficult, and thepneumoperitoneum necessary forproper visualization of the peritonealcavity can compromise venous return.Experience with diagnostic laparoscopyin critically ill patients is largely anec-dotal (61), and although successfullaparoscopic management of intra-abdominal abscesses has been reported(62), CT remains the most useful diag-nostic and therapeutic modality in thecontemporary ICU setting.
Management
The initial management of the patientwith intra-abdominal infection is resusci-tation and physiologic organ system sup-port, combined with appropriate moni-toring. Early fluid requirements may besubstantial because of considerable third-space fluid loss into the peritoneal cavity,the retroperitoneum, and the lumen ofthe gastrointestinal tract. For patientswith extensive intraperitoneal or retro-peritoneal inflammation and significantearly fluid requirements, monitoring ofbladder pressures to detect an abdominalcompartment syndrome should be per-formed (63).
Systemic antibiotics are administeredbased on knowledge of the probable com-position of the infecting flora (Table 1).Coverage is directed against aerobicGram-negative organisms and anaerobeswhen the source of contamination is un-known; however, if the infection is knownto arise from the upper gastrointestinaltract (for example, as a result of a perfo-rated ulcer), coverage directed againstaerobes alone is adequate (64).
The selection of an empiric broad-spectrum antibiotic regimen is guided byconsiderations of patient-specific toxicity,cost, and local patterns of antimicrobialresistance; the many available regimensare of largely equivalent clinical efficacy(Table 3) (65). The optimal duration oftherapy is unknown. When source con-trol has been effective (see below), therole of antibiotics is a purely adjuvant one(66), and the course can be restricted to5–7 days (67).
Although mortality rates are higherwhen the enterococcus is isolated frompolymicrobial intra-abdominal infections(26), there is no compelling evidence thatproviding specific anti-enterococcal ther-apy improves the clinical outcome (68,69). Similarly, although the isolation ofCandida at the time of abdominal abscessdrainage identifies a patient at increasedrisk of mortality (43, 70), there is noconvincing evidence that antifungal ther-apy alters this risk (71).
For the patient with tertiary peritoni-tis, the role of systemic antimicrobialtherapy is poorly defined. There is littleevidence that antibiotics significantly al-ter the clinical course; moreover, the in-fecting organisms tend to be resistant tothe commonly used empiric regimens (3,47, 72). We favor the use of narrow-spectrum agents, selecting on the basis ofthe results of culture and sensitivity and
Figure 1. Top panel, localized diverticular ab-scess adjacent to the sigmoid colon; note the rimenhancement of the abscess capsule (arrow). Bot-tom panel, CT scan of a 62-yr-old man withintestinal ischemia secondary to low-flow stateafter coronary artery bypass surgery. Intestinalischemia is suggested by evidence of pneumatosisin the intestinal wall (black arrows) and air in theintrahepatic portal vein (white arrow).
2231Crit Care Med 2003 Vol. 31, No. 8

avoiding antibiotics with anti-anaerobicactivity.
The definitive management of intra-abdominal infection must include sourcecontrol—those physical measures thatare undertaken to eradicate a focus ofinfection, to prevent ongoing contamina-tion, and ultimately to restore optimalanatomy and function (73–75). Sourcecontrol measures are based on three prin-ciples—drainage, debridement, and de-finitive management. Because successfulmanagement of even the most compli-cated intra-abdominal infection dependson the optimal application of these prin-ciples, it is instructive to review them ingreater detail (Table 4).
Drainage. The inflammatory responseevoked by intra-abdominal infection (seeabove) results in the local activation ofcoagulation, with the deposition of fibrinand the formation of an abscess—a col-lection of tissue debris, bacteria, neutro-phils and macrophages, and protein-richexudative fluid enclosed within a fibrouscapsule (Fig. 2). Formation of an abscessserves to isolate the infection from thesurrounding sterile tissues but also pre-vents the influx of further host immunecells or antibiotics: the result is a biologicstandoff. Drainage converts an abscess toa controlled sinus (an abnormal commu-nication between a deep space and anepithelial surface) or fistula (an abnormalcommunication between two epitheliallylined surfaces) and, in essence, external-izes the infectious process. Drainage canbe accomplished by several differentstrategies. Open surgical drainage hasbeen the classical treatment strategy, andit permits definition of the extent of thecollection and immediate evacuation ofits contents. Ideally, drainage is accom-plished by the most direct route, mini-mizing contamination of the peritonealcavity (76), although with the use of ad-juvant antibiotics, the benefits of extrase-rous drainage are minimal and often off-set by the advantage that wider exposure
gives for full exploration and manage-ment of the inciting cause of the infec-tion.
More recently, however, with the rec-ognition that the biologic objectives ofdrainage can be accomplished withoutthe need for operative intervention, per-cutaneous drainage guided by ultrasoundor CT has become the initial interventionof choice in the management of a local-ized, radiologically defined infectious fo-cus (77). Initial reports of the efficacy ofpercutaneous drainage for well-demar-cated, unilocular collections (78) led toan expansion of its indications to includemultiple collections, those in relativelyinaccessible anatomic locations, and col-lections containing solid debris or com-municating with the gastrointestinaltract (79). Moreover, percutaneous drain-age can serve as a temporizing measureuseful, for example, in decompressing in-fected retroperitoneal collections in thepatient with necrotizing pancreatitis sothat operative intervention can be de-ferred until it is safer (Fig. 3).
The relative merits of operative andpercutaneous drainage have never beencompared in a formal randomized trial,although case series with historical con-trols (80–82) and an expanding clinicalexperience point to the utility of an initialattempt at percutaneous drainage formost patients with intra-abdominal ab-scesses. Surgical drainage is indicated forfailures of percutaneous drainage, for col-lections with a significant solid tissuecomponent requiring debridement, forsimultaneous management of a source of
ongoing contamination, and when localperitoneal defenses have not containedthe infectious focus, leading to general-ized peritonitis (Fig. 4).
Debridement. In contrast to drainage,which eliminates the liquid component ofan infection, debridement is the physicalremoval of infected or necrotic solid tis-sue. The term encompasses, for example,the excision of necrotic infected peripan-creatic fat in patients with infected pan-creatic necrosis, the removal of feces andintestinal contents from the peritonealcavity of the patient with a perforation ofthe gastrointestinal tract, the excision ofnecrotic intestine in the patient withacute intestinal ischemia, or the excisionof abdominal wall muscle in the patient
Figure 2. Photomicrograph of an intrahepaticabscess. Note dense accumulation of neutrophils(dashed arrow) and fibrous capsule (solid arrow)that walls off the abscess from surrounding nor-mal liver tissue.
Table 4. Definitions and concepts in the management of intra-abdominal infection
Peritonitis Inflammation of the peritoneal lining of the abdominal cavity
Abscess Collection of tissue fluid, neutrophils, and bacteria enclosed in a fibrin capsuleFistula Abnormal communication between two epithelially lined surfacesSinus Cavity communicating with an epithelially lined surfaceDrainage Conversion of an abscess to a controlled sinus or fistulaDebridement Physical removal of infected or necrotic solid tissue
Table 3. Recommended antimicrobial regimens for high-risk patients with intra-abdominal infection
Single agentsImipenem/cilastatinMeropenemPiperacillin/tazobactam
Combination therapyAminoglycoside (amikacin, gentamicin, netilmicin, tobramycin) plus an anti-anaerobe (clindamycin or metronidazole)Aztreonam plus clindamycinCiprofloxacin plus metronidazoleThird/fourth generation cephalosporin (cefepime, cefotaxime, ceftazidime, ceftizoxime, ceftriaxone) plus an anti-anaerobe (clindamycin or metronidazole)
Adapted with permission from Mazuski et al (65).
2232 Crit Care Med 2003 Vol. 31, No. 8

with a secondary necrotizing soft-tissueinfection. It also includes the removal offoreign bodies and such adjuvants forbacterial growth as blood clot and devi-talized tissue.
The need for debridement is encoun-tered less frequently in patients with in-tra-abdominal infection, exceptions in-cluding the patient with intestinalinfarction or infected peripancreatic ne-crosis. Intestinal infarction is a cata-strophic complication, having a prohibi-tively high mortality rate unless thenecrotic bowel is rapidly excised (83). Incontrast, although infected peripancre-atic necrosis is associated with a signifi-cant rate of mortality and major morbid-ity, prognosis is improved if operativeintervention is delayed (84). The reasonfor this discrepancy underlines a funda-mental principle in the source controlmanagement of intra-abdominal infec-
tion—that the benefits of interventionmust be balanced against the risks asso-ciated with intervention. In the case ofintestinal ischemia, leakage of bacteriathrough the necrotic bowel wall is con-siderable, whereas surgical interventionto excise the necrotic bowel is a relativelystraightforward undertaking. The bacte-rial burden in infected retroperitonealnecrosis, on the other hand, is lower, andorganisms sequestered in the necrotictissue are less able to gain access to thecirculation. At the same time, early sur-gical exploration of the retroperitoneumis fraught with hazard because the de-marcation between viable and nonviabletissue is poor, leading to a significant riskof major hemorrhage, and operative ex-posure of this area is difficult (85). Thus,evolving approaches to the managementof infected pancreatic necrosis emphasizethe importance of delayed, rather thanimmediate, intervention (86, 87).
Irrigation of the peritoneal cavity toremove bacteria, devitalized tissue, andfibrin can also be considered a form ofdebridement. Although the practice ispopular with many surgeons, there is noconvincing evidence of its utility (88).Similarly, a randomized trial of perito-neal debridement to remove fibrin at-tached to loops of bowel also failed toshow any evidence of benefit (89).
Definitive Measures. The definitivemanagement of intra-abdominal infec-tion includes measures to remove foci ofongoing contamination and to restore, asmuch as possible, normal structure andfunction. Such measures include, for ex-ample, the excision of an area of divertic-ular disease containing a perforation inthe patient with diverticulitis and restor-ing function either by the creation of anend colostomy of the descending colon(when the distal rectal stump is closedand left in the abdomen, this is known asa Hartmann procedure) or by creating ananastomosis between the two ends of theremaining colon (primary anastomosis).Pooled data from case series indicate thatin patients with perforated diverticulitis,outcomes are improved by excising theinvolved colon (73) and perhaps even byundertaking a primary anastomosis (90–93). The benefits of more extensive inter-vention must be weighed against therisks of that intervention. For the patientwith a contained diverticular abscess, itmay well be preferable to drain the ab-scess percutaneously and to plan an elec-tive sigmoid resection with primary anas-tomosis at a later date. For the critically
ill patient with cholecystitis or even anempyema of the gall bladder, percutane-ous cholecystostomy may be the safer op-tion to surgical cholecystectomy (94–97).
It is important to consider the optionsfor future reconstructive procedures atthe time of the initial source control in-tervention (98). Incisions should be cho-sen to permit maximal flexibility at thetime of re-operation: a midline abdomi-nal incision probably represents the mostversatile approach. Stomas should beplanned and sited to accommodate thedemands of the management of an openwound and to minimize the magnitude ofsurgery required for their subsequentclosure. Rather than creating multiplestomas, for example, it is generally pref-erable to reconstruct the distal gastroin-testinal tract but to protect potentiallytenuous anastomoses with a proximalloop enterostomy: subsequent recon-struction will simply require local closureof the loop enterostomy.
Occasionally, circumstances are suchthat even the most basic of definitive pro-cedures—abdominal wall closure, for ex-ample—are hazardous. In the patientwith loss of the abdominal wall from as-sociated soft-tissue infection or extensiveedema of the viscera and abdominal wall,closure will result in increased intra-abdominal pressure, resulting in abdom-inal compartment syndrome. Open man-agement of the abdomen is advisable,using absorbable mesh or a nonadheringprosthesis to prevent evisceration of the
Figure 3. Percutaneous drainage of the fluidcomponent of a peripancreatic abscess (arrow)facilitated a delay in surgical intervention until 5wks after the onset of disease. Residual infectednecrotic tissue was removed by laparoscopic de-bridement.
Figure 4. Diffuse peritonitis secondary to a leakfrom an unrecognized defect in the rectum afterelective ileocolic resection for Crohn’s disease.Peritoneal inflammation is suggested by en-hancement of intestinal wall (thin arrow). Pres-ence of fluid (large dashed arrow) and air (largesolid arrow) throughout the peritoneal cavityrenders percutaneous drainage ineffective.
T he approach to the
patient with sus-
pected intra-ab-
dominal infection must be
based on a combination of
evidence from the literature
and inference from basic bi-
ologic principles, interpreted
through a combination of
experience and the ability to
adapt one’s approach to a
changing situation.
2233Crit Care Med 2003 Vol. 31, No. 8

intestinal contents. Beyond circum-stances of necessity, however, there islittle evidence that approaches such asscheduled re-laparotomy or an open-abdomen approach improve patient out-come (99–102). Rather, these are asso-ciated with worsening of organdysfunction, amplification and persis-tence of inflammation, and greater useof blood component therapy (103, 104).
Successful source control and antibi-otic management of intra-abdominal in-fection is associated with resolution ofsystemic signs and symptoms of acuteinflammation (105) and reversal of organdysfunction. Conversely, progression orfailure of resolution of organ dysfunctionsuggests persistence of the disease andthe need for further intervention (106).
Although the management of the crit-ically ill patient with peritonitis is com-monly challenging, often frustrating, andinvariably costly, long-term quality of lifein survivors is very good (107, 108), andcost-utility ratios are favorable, with acost per quality-adjusted life years of lessthan $3000 (109), thus, fully justifyingthe efforts expended in this complex pa-tient population.
Approach to the Patient withSuspected Intra-abdominalInfection
The antecedents of intra-abdominalinfection in the critically ill patient are
many, the clinical presentations highlyvaried, and the associated factors thatcomplicate one approach or another inthe individual patient are numerous. It is,therefore, neither possible nor advisableto present a simple management algo-rithm that is likely to define the bestspecific option in a particular patient.Rather, the decision of how to manage aproblem must be individualized andbased on the principles articulated aboveand on the unique features of the partic-ular patient. Nonetheless, it is entirelypossible to outline the elements of thedecision-making process without antici-pating the final decision, and Figure 5provides an algorithm for an approach tothe management of suspected intra-abdominal infection in the critically illpatient.
The suspicion that something is amisswithin the peritoneal cavity arises be-cause of characteristic signs and symp-toms that, however, are often difficult tointerpret in the ICU setting. The develop-ment of new organ dysfunction, particu-larly that involving the gastrointestinalsystem, liver, or hematologic system,raises the possibility of intra-abdominalinfection, as does the development of un-explained metabolic acidosis. However,the paramount consideration is the clin-ical setting. Is the patient at risk for in-fection because of recent abdominal sur-gery? Is there a source of arterial emboli,evidence of peripheral vascular disease, athrombotic disorder, a history of recentarteriography, or a history of reducedsplanchnic flow as a result of the use ofvasopressors or prolonged shock? The ab-sence of such risk factors makes the ab-domen much less likely to be the sourceof an explanation for unexplained clinicaldeterioration.
If a source is readily apparent, for ex-ample, pus or gastrointestinal content isleaking from an abdominal wound, orintraperitoneal free air is demonstratedon a chest radiograph, then interventionshould be undertaken without delay. Typ-ically, this will entail operation ratherthan image-guided therapy. If no sourceis seen, then CT with oral, rectal, andintravenous contrast enhancementshould be performed. The accuracy of theCT scan is such that further decisions aremade on the basis of its findings. A focalor contained collection can be drainedpercutaneously, with a follow-up CT scanor sinogram, injecting water-soluble con-trast medium into the drain, to confirmresolution. If there is evidence of a diffuse
and nonlocalized process, then operativeintervention is indicated. Similarly, ifthere is evidence of ischemia or infarc-tion, then operation should be under-taken, unless there are compellinggrounds for an alternative approach. Theindication for surgery in the patient withgut ischemia is to restore flow or to re-sect dead bowel; for the patient with isch-emia as a result of venous thrombosis ora low-flow state, neither of these optionsmay be possible, and it may be preferableto observe the patient while maximizingsplanchnic flow with anti-coagulants andhemodynamic support.
A negative abdominal CT scan gener-ally indicates a very low probability of aprocess that can be reversed through sur-gical intervention, and if no treatablepathologic process is seen, then contin-ued observation is appropriate. With ad-vances in imaging technology, the era ofblind surgical exploration to diagnose oc-cult infection has almost ended (110).
Conclusions
Intra-abdominal infection is a com-mon indication for ICU admission and animportant cause of preventable morbidityand mortality after ICU admission. Thedisorders responsible for these infectionsare numerous, and their clinical presen-tation and optimal management arehighly variable. The approach to the pa-tient with suspected intra-abdominal in-fection must be based on a combinationof evidence from the literature and infer-ence from basic biologic principles, inter-preted through a combination of experi-ence and the ability to adapt one’sapproach to a changing situation. Evenwith optimal management, the short-and long-term morbidity can be substan-tial: close collaboration between surgeon,radiologist, and intensivist holds the keyto minimizing these.
REFERENCES
1. Evans HL, Raymond DP, Pelletier SJ, et al:Diagnosis of intra-abdominal infection inthe critically ill patient. Curr Opin Crit Care2001; 7:117–121
2. Bohnen J, Boulanger M, Meakins JL, et al:Prognosis in generalized peritonitis: Rela-tion to cause and risk factors. Arch Surg1983; 118:285–290
3. Nathens AB, Rotstein OD, Marshall JC: Ter-tiary peritonitis: Clinical features of a com-plex nosocomial infection. World J Surg1998; 22:158–163
4. Skillman JJ, Bushnell LS, Goldman H, et al:
Figure 5. An approach to the management of acritically ill patient with suspected intra-abdominal infection. GI, gastrointestinal; CT,computerized tomography; IAP, intraabdominalpressure.
2234 Crit Care Med 2003 Vol. 31, No. 8

Respiratory failure, hypotension, sepsis, andjaundice: A clinical syndrome associatedwith lethal hemorrhage and acute stressulceration in the stomach. Am J Surg 1969;117:523–530
5. Fry DE, Garrison RN, Heitsch RC, et al:Determinants of death in patients with in-traabdominal abscess. Surgery 1980; 88:517–523
6. Polk HC, Shields CL: Remote organ failure:A valid sign of occult intraabdominal infec-tion. Surgery 1977; 81:310–313
7. Heemken R, Gandawidjaja L, Hau T: Peri-tonitis: Pathophysiology and local defensemechanisms. Hepatogastroenterology1997; 44:927–936
8. Hall JC, Heel KA, Papadimitriou JM, et al:The pathobiology of peritonitis. Gastroen-terology 1998; 114:185–196
9. Holzheimer RG, Schein M, Wittmann DH:Inflammatory response in peritoneal exu-date and plasma of patients undergoingplanned relaparotomy for severe secondaryperitonitis. Arch Surg 1995; 130:1314–1320
10. Riese J, Schoolmann S, Denzel C, et al:Effect of abdominal infections on peritonealand systemic production of interleukin 6and monocyte chemoattractant protein-1.Shock 2002; 17:361–364
11. Broche A, Tellado J: Defense mechanisms ofthe peritoneal cavity. Curr Opin Crit Care2001; 7:105–116
12. Finlay-Jones JJ, Davies KV, Sturm LP, et al:Inflammatory processes in a murine modelof intra-abdominal abscess formation.J Leuk Biol 1999; 66:583–587
13. McRitchie DI, Girotti MJ, Glynn MFX, et al:Effect of systemic fibrinogen depletion onintraabdominal abscess formation. J LabClin Med 1991; 118:48–55
14. Hau T, Simmons RL: Heparin in the treat-ment of experimental peritonitis. Ann Surg1978; 187:294–298
15. Holzer K, Konietzny P, Wilhelm K, et al:Phagocytosis by emigrated, intra-abdomi-nal neutrophils is depressed during humansecondary peritonitis. Eur Surg Res 2002;34:275–284
16. Rotstein OD, Pruett TL, Simmons RL: Fi-brin in peritonitis: V. Fibrin inhibits phago-cytic killing of Escherichia coli by humanpolymorphonuclear leukocytes. Ann Surg1986; 203:413–419
17. Lee A: Neglected niches: The microbialecology of the gastrointestinal tract. AdvMicrob Ecol 1985; 8:115–162
18. Savage DC: Microbial ecology of the gastro-intestinal tract. Annu Rev Med 1977; 31:107–133
19. Onderdonk AB, Bartlett JG, Louie T, et al:Microbial synergy in experimental intra-abdominal abscess. Infect Immun 1997; 13:22–26
20. Van Der Waaij D: The ecology of the humanintestine and its consequences for over-growth by pathogens such as Clostridiumdifficile. Annu Rev Microbiol 1989; 43:69–87
21. Berg RD: Promotion of the translocation ofenteric bacteria from the gastrointestinaltracts of mice by oral treatment with peni-cillin, clindamycin, or metronidazole. In-fect Immun 1981; 33:854–861
22. Thomakos N, Maraki S, Liakakos T, et al:Effect of cefamandole, cefuroxime and ce-foxitin on yeast fecal flora of surgical pa-tients. Chemotherapy 2003; 44:324–327
23. Van der Leur JJ, Thunnissen PL, ClasenerHA, et al: Effects of imipenem, cefotaximeand cotrimoxazole on aerobic microbial col-onization of the digestive tract. Scand J In-fect Dis 1993; 25:473–478
24. Donskey CJ, Chowdhry TK, Hecker MT, etal: Effect of antibiotic therapy on the den-sity of vancomycin-resistant enterococci inthe stool of colonized patients. N EnglJ Med 2000; 343:1925–1932
25. Marshall JC, Christou NV, Meakins JL: Thegastrointestinal tract: The “undrained ab-scess” of multiple organ failure. Ann Surg1993; 218:111–119
26. Sitges-Serra A, Lopez MJ, Girvent M, et al:Postoperative enterococcal infection aftertreatment of complicated intra-abdominalsepsis. Br J Surg 2002; 89:361–367
27. Fierobe L, Decre D, Muller C, et al: Methi-cillin-resistant Staphylococcus aureus as acausative agent of post-operative intra-abdominal infection: Relation to nasal col-onization. Clin Infect Dis 1999; 29:1231–1238
28. Riche FC, Cholley BP, Panis YH, et al: In-flammatory cytokine response in patientswith septic shock secondary to generalizedperitonitis. Crit Care Med 2000; 28:433–437
29. Hynninen M, Valtonen M, Markkanen H, etal: Intramucosal pH and endotoxin and cy-tokine release in severe acute pancreatitis.Shock 2000; 13:79–82
30. Fry DE, Pearlstein L, Fulton RL, et al: Mul-tiple system organ failure: The role of un-controlled infection. Arch Surg 1980; 115:136–140
31. Tran DD, Groeneveld ABJ, Van der MeulenJ, et al: Age, chronic disease, sepsis, organsystem failure, and mortality in a medicalintensive care unit. Crit Care Med 1990;18:474–479
32. Conn HO: Spontaneous peritonitis and bac-teremia in Laennec’s cirrhosis caused byenteric organisms. Ann Intern Med 1964;60:568–580
33. Guarner C, Soriano G: Spontaneous bacte-rial peritonitis. Semin Liver Dis 1997; 17:203–217
34. Sola R, Soriano G: Why do bacteria reachascitic fluid? Eur J Gastroenterol Hepatol2002; 14:351–354
35. Cirera I, Bauer TM, Navasa M, et al: Bacte-rial translocation of enteric organisms inpatients with cirrhosis. J Hepatol 2001; 34:150–155
36. Fernandez J, Navasa M, Gomez J, et al:Bacterial infections in cirrhosis: epidemio-logical changes with invasive procedures
and norfloxacin prophylaxis. Hepatology2002; 35:140–148
37. Campillo B, Richardet JP, Kheo T, et al:Nosocomial spontaneous bacterial peritoni-tis and bacteremia in cirrhotic patients: Im-pact of isolate type on prognosis and char-acteristics of infection. Clin Infect Dis 2002;35:1–10
38. Ljubcic N, Spajic D, Vrkljan MMM, et al:The value of ascitic fluid polymorphonu-clear cell count determination during ther-apy of spontaneous bacterial peritonitis inpatients with liver cirrhosis. Hepatogastro-enterology 2000; 47:1360–1363
39. Soares-Weiser K, Brezis M, Leibovici L: An-tibiotics for spontaneous bacterial peritoni-tis in cirrhotics. Cochrane Database SystRev 2001; 3:CD002232
40. Thuluvath PJ, Morss S, Thompson R: Spon-taneous bacterial peritonitis: In-hospitalmortality, predictors of survival, and healthcare costs from 1988 to 1998. Am J Gastro-enterol 2001; 96:1232–1236
41. Marshall JC, Spencer-Netto F: Secondarybacterial peritonitis. Prob Gen Surg 2002;19:53–64
42. Laroche M, Harding G: Primary and second-ary peritonitis: An update. Eur J Clin BiolMicrobiol Infect Dis 1998; 17:542–550
43. Hoerauf A, Hammer S, Muller-Myhsok B, etal: Intra-abdominal Candida infection dur-ing acute necrotizing pancreatitis has ahigh prevalence and is associated with in-creased mortality. Crit Care Med 1998; 26:2010–2015
44. Akriviadis EA, Runyon BA: Utility of an al-gorithm in differentiating spontaneousfrom secondary bacterial peritonitis. Gas-troenterology 1990; 98:127–133
45. Buijk SE, Bruining HA: Future directions inthe management of tertiary peritonitis. In-tensive Care Med 2002; 28:1024–1029
46. Malangoni MA: Evaluation and manage-ment of tertiary peritonitis. Am Surg 2000;66:157–161
47. Rotstein OD, Pruett TL, Simmons RL: Mi-crobiologic features and treatment of per-sistent peritonitis in patients in the inten-sive care unit. Can J Surg 1986; 29:247–250
48. Marshall JC, Christou NV, Horn R, et al: Themicrobiology of multiple organ failure: Theproximal GI tract as an occult reservoir ofpathogens. Arch Surg 1988; 123:309–315
49. Sawyer RG, Rosenlof LK, Adams RB, et al:Peritonitis into the 1990’s: Changing patho-gens and changing strategies in the criti-cally ill. Am Surg 1992; 58:82–87
50. Johnson CC, Baldessarre J, Levison ME:Peritonitis: Update on pathophysiology,clinical manifestations, and management.Clin Infect Dis 1997; 24:1035–1047
51. Kaleya RN, Boley SJ: Acute mesenteric isch-emia. Crit Care Clin 1995; 11:479–512
52. Stoney RJ, Cunningham CG: Acute mesen-teric ischemia. Surgery 1993; 114:489–490
53. Le Gall JR, Fagniez PL, Meakins JL, et al:Diagnostic features of early high post-
2235Crit Care Med 2003 Vol. 31, No. 8

laparotomy fever: A prospective study of 100patients. Br J Surg 1982; 69:452–455
54. Ing AFM, Mclean APH, Meakins JL: Multipleorganism bacteremia in the surgical inten-sive care unit: A sign of intraperitoneal sep-sis. Surgery 1981; 90:779–786
55. Adam EJ, Page JE: Intra-abdominal sepsis:The role of radiology: Baillieres Clin Gas-troenterol 1991; 5(3Pt1):587–609
56. Fry DE: Noninvasive imaging tests in thediagnosis and treatment of intra-abdominalabscess in the postoperative patient. SurgClin North Am 1994; 74:693–709
57. Velmahos GC, Kamel E, Berne TV, et al:Abdominal computed tomography for thediagnosis of intra-abdominal sepsis in crit-ically injured patients: Fishing in murkywaters. Arch Surg 1999; 134:831–838
58. Tepel M, van der Giet M, Schwarzfeld C, etal: Prevention of radiographic contrastagent-induced reductions in renal functionby acetylcysteine. N Engl J Med 2000; 343:180–184
59. Alverdy JC, Saunders J, Chamberlin WH, etal: Diagnostic peritoneal lavage in intra-abdominal sepsis. Am Surg 1988; 54:456–459
60. Gagne DJ, Malay MB, Hogle NJ, et al: Bed-side diagnostic minilaparoscopy in the in-tensive care patient. Surgery 2003; 131:491–496
61. Gorecki P: The role of laparoscopy. In:Source Control: A Guide to the Manage-ment of Surgical Infections. Schein M, Mar-shall JC (Eds). Berlin, Springer-Verlag,2002, pp 350–357
62. Kok KY, Yapp SK: Laparoscopic drainage ofpostoperative complicated intra-abdominalabscesses. Surg Laparosc Endosc PercutanTech 2000; 10:311–313
63. Schein M, Wittmann DH, Aprahamian CC,et al: The abdominal compartment syn-drome: The physiological and clinical con-sequences of elevated intra-abdominal pres-sure. J Am Coll Surg 1995; 180:745–753
64. Nathens AB, Rotstein OD: Therapeutic op-tions in peritonitis. Surg Clin North Am1997; 74:677–692
65. Mazuski JE, Sawyer RG, Nathens AB, et al:The Surgical Infection Society guidelineson antimicrobial therapy for intra-abdomi-nal infections: An executive summary. SurgInfect 2002; 3:161–173
66. Sotto A, Lefrant JY, Fabbro-Peray P, et al:Evaluation of antimicrobial therapy man-agement of 120 consecutive patients withsecondary peritonitis. J Antimicrob Che-mother 2002; 50:569–576
67. Wittmann DH, Schein M: Let us shortenantibiotic prophylaxis and therapy in sur-gery. Am J Surg 1996; 172:26S–32S
68. Barie PS, Christou NV, Dellinger EP, et al:Pathogenicity of the enterococcus in surgi-cal infections. Ann Surg 1990; 212:155–159
69. Röhrborn A, Wacha H, Schöffel U, et al:Coverage of enterococci in community ac-quired secondary peritonitis: Results of a
randomized trial. Surg Infect 2000;1:95–107
70. Calandra T, Bille J, Schneider R, et al: Clin-ical significance of Candida isolated fromperitoneum in surgical patients. Lancet1989; 2:1437–1440
71. Sandven P, Qvist H, Skovlund P, et al: Sig-nificance of Candida recovered from intra-operative specimens in patients with intra-abdominal perforations. Crit Care Med2002; 30:541–547
72. Roehrborn A, Thomas L, Potreck O, et al:The microbiology of postoperative peritoni-tis. Clin Infect Dis 2001; 33:1513–1519
73. Jimenez MF, Marshall JC: Source control inthe management of sepsis. Intensive CareMed 2001; 27:S49–S62
74. Grunau G, Heemken R, Hau T: Predictors ofoutcome in patients with post-operative in-tra-abdominal infection. Eur J Surg 2002;162:619–625
75. Seiler CA, Brugger L, Forssmann U, et al:Conservative surgical treatment of diffuseperitonitis. Surgery 2000; 127:178–184
76. Spain DA, Martin RC, Carrillo EH, et al:Twelfth rib resection: Preferred therapy forsubphrenic abscess in selected surgical pa-tients. Arch Surg 1997; 132:1203–1206
77. van Sonnenberg E, Wittich GR, GoodacreBW, et al: Percutaneous abscess drainage:Update. World J Surg 2001; 25:362–372
78. Gerzof SG, Robbins AH, Johnson WC, et al:Percutaneous catheter drainage of abdomi-nal abscesses: A five-year experience. N EnglJ Med 1981; 305:653–657
79. Gerzof SG, Robbins AH, Johnson WC, et al:Expanded criteria for percutaneous abscessdrainage. Arch Surg 1985; 120:227
80. Olak JO, Christou NV, Stein LA, et al: Op-erative versus percutaneous drainage of in-tra-abdominal abscesses. Arch Surg 1986;121:141
81. Hemming A, Davis NL, Robins RE: Surgicalversus percutaneous drainage of intra-abdominal abscesses. Am J Surg 1991; 161:593–595
82. Bufalari A, Giustozzi G, Moggi L: Postoper-ative intraabdominal abscesses: Percutane-ous versus surgical treatment. Acta ChirBelg 1996; 96:197–200
83. Raymond DP, May AK: Acute mesentericischemia. In: Source Control: A Guide tothe Management of Surgical Infections.Schein M, Marshall JC (Eds). Berlin,Springer-Verlag, 2003, pp 178–190
84. Mier J, Leon EL, Castillo A, et al: Earlyversus late necrosectomy in severe necro-tizing pancreatitis. Am J Surg 1997; 173:71–75
85. Urbach DR, Marshall JC: Pancreatic abscessand infected pancreatic necrosis. Curr OpinSurg Infect 1996; 4:57–66
86. Dellinger P: Pancreatic infection. In:Source Control: A Guide to the Manage-ment of Surgical Infections. Schein M, Mar-shall JC (Eds). Berlin, Springer-Verlag,2003, pp 154–166
87. Fernandez-del Castillo C, Rattner DW,
Makary MA, et al: Debridement and closedpacking for the treatment of necrotizingpancreatitis. Ann Surg 1998; 228:676–684
88. Platell C, Papadimitriou JM, Hall JC: Theinfluence of lavage on peritonitis. J Am CollSurg 2000; 191:672–680
89. Hudspeth AS: Radical surgical debridementin the treatment of advanced generalizedbacterial peritonitis. Arch Surg 1975; 110:1233–1236
90. Schilling MK, Maurer CA, Kollmar O, et al:Primary vs. secondary anastomosis aftersigmoid colon resection for perforated di-verticulitis (Hinchey Stage III and IV): Aprospective outcome and cost analysis. DisCol Rect 2001; 44:699–703
91. Gooszen AW, Tollenaar RA, Geelkerken RH,et al: Prospective study of primary anasto-mosis following sigmoid resection for sus-pected acute complicated diverticular dis-ease. Br J Surg 2001; 88:693–697
92. Biondo S, Jaurrieta E, Marti Rague J, et al:Role of resection and primary anastomosisof the left colon in the presence of perito-nitis. Br J Surg 2000; 87:1580–1584
93. Zeitoun G, Laurent A, Rouffet F, et al: Mul-ticentre, randomized clinical trial of pri-mary versus secondary sigmoid resection ingeneralized peritonitis complicating sig-moid diverticulitis. Br J Surg 2000; 87:1366–1374
94. Hamy A, Visset J, Likholatnikov D, et al:Percutaneous cholecystostomy for acutecholecystitis in critically ill patients. Sur-gery 1997; 121:398–401
95. Boggi U, Candio G, Campatelli A, et al:Percutaneous cholecystostomy for acutecholecystitis in critically ill patients. Hepa-togastroenterology 1999; 46:121–125
96. Melin MM, Sarr MG, Bender CE, et al: Per-cutaneous cholecystostomy: A valuabletechnique in high-risk patients with pre-sumed acute cholecystitis. Br J Surg 1995;82:1274–1277
97. Boland G, Lee MJ, Mueller PR: Acute cho-lecystitis in the intensive care unit. CritCare Med 1993; 1:246–250
98. Rotstein OD: Reoperation after source con-trol surgery for intra-abdominal infection.In: Source Control: A Guide to the Manage-ment of Surgical Infections. Schein M, Mar-shall JC (Eds). Berlin, Springer-Verlag,2003, pp 300–311
99. Christou NV, Barie PS, Dellinger EP, et al:Surgical Infection Society intra-abdominalinfection study: Prospective evaluation ofmanagement techniques and outcome.Arch Surg 1993; 128:193–198
100. Schein M, Hirshberg A, Hashmonai M: Cur-rent surgical management of severe intra-abdominal infection. Surgery 1992; 112:489–496
101. Hau T, Ohmann C, Wolmershauser A, et al:Planned relaparotomy versus relaparotomyon demand in the treatment of intra-abdominal infections. Arch Surg 1995; 130:1193–1197
102. Lamme B, Boermeester MA, Reitsma JB, et
2236 Crit Care Med 2003 Vol. 31, No. 8

al: Meta-analysis of relaparotomy for sec-ondary peritonitis. Br J Surg 2002; 89:1516–1524
103. Zugel N, Siebeck M, Geissler B, et al: Cir-culating mediators and organ function inpatients undergoing planned relaparotomyvs conventional surgical therapy in severesecondary peritonitis. Arch Surg 2002; 137:590–599
104. van Goor H, Hulsebos RG, Bleichrodt RP:Complications of planned relaparotomy inpatients with severe general peritonitis. EurJ Surg 1997; 163:61–66
105. Stone HH, Bourneuf AA, Stinson LD: Reli-ability of criteria for predicting persistent orrecurrent sepsis. Arch Surg 1985; 120:17–20
106. Paugam-Burtz C, Dupont H, Marmuse JP,et al: Daily organ-system failure for diagno-sis of persistent intra-abdominal sepsis afterpostoperative peritonitis. Intensive CareMed 2002; 28:594–598
107. Scheingraber S, Kurz T, Dralle H: Short-and long-term outcome and health-relatedquality of life after severe peritonitis. WorldJ Surg 2002; 26:667–671
108. Bosscha K, Reijnders K, Jacobs MH, et al:Quality of life after severe bacterial perito-nitis and infected necrotizing pancreatitistreated with open management of the abdo-men and planned re-operations. Crit CareMed 2001; 29:1539–1543
109. Welcker K, Lederle J, Schorr M, et al: Sur-gery and adjuvant therapy in patients withdiffuse peritonitis: Cost analysis. WorldJ Surg 2002; 26:307–313
110. Bunt TJ: Non-directed relaparotomy for in-traabdominal sepsis: A futile procedure. AmSurg 1986; 52:294
2237Crit Care Med 2003 Vol. 31, No. 8







![Intra-Abdominal and Abdominal Wall Desmoid Fibromatosis · intra-abdominal and involving the small bowel mesentery [2]. TREATMENT Surgery Margin-negative resection has historically](https://img.pdfslide.us/doc/110x75/5e5a290071d21b380f5b7e74/intra-abdominal-and-abdominal-wall-desmoid-fibromatosis-intra-abdominal-and-involving.jpg)