Embed Size (px)
Citation preview

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 1
Robert G.Sawyer,M.D.,F.A.C.S.,Jeffrey S.Barkun,M.D.,F.A.C.S.,Robert Smith,M.D.,Tae Chong,M.D.,and GeorgeTzimas, M.D.
19 INTRA-ABDOMINAL INFECTION
The basic principles of rapid diagnosis, timely physiologic sup-port, and definitive intervention for intra-abdominal infectionshave remained unchanged over the past century. Specific manage-ment of these conditions, however, has been transformed of late asa result of numerous advances in technology. Improved radiologicand laboratory techniques have led to more precise preoperativediagnoses, and newer procedures have led to treatment algorithmsthat cause less morbidity and permit faster recovery.Whereas thepathophysiology of these infections remains largely unchanged,their management is now marked by an ever-growing complexity.It is no longer true that the diagnosis of intra-abdominal infection,even in association with a perforated viscus, necessitates urgentexploration, but it remains the case that decisions regarding theultimate course of action for any individual patient are solely theresponsibility of the surgeon.
Clinical Evaluation
HISTORY
The general approach to a patient sus-pected of having an intra-abdominalinfection is much like that to a patientwith any other acute surgical condition.Specific approaches to various intra-abdominal infections are addressed in more detail elsewhere [seeInfections of the Upper Abdomen and Infections of the LowerAbdomen, below].
The first step is an accurate history.To begin with, cases of peri-tonitis are broadly classified as primary, secondary, or tertiary; thisclassification provides a useful framework for suggesting generalapproaches to treatment. Primary peritonitis arises spontaneously,without a demonstrable source of contamination, and is generallytreated with antibiotics alone; an example is spontaneous bacteri-al peritonitis in the setting of ascites. Secondary peritonitis iscaused by a breach in the GI tract that leads to contamination ofa normally sterile space. Control of the source of infection viadrainage, resection, diversion, or some combination thereof isimperative for optimizing outcome.Tertiary peritonitis is a poorlydefined entity associated with recurrence of intra-abdominal infec-tion after the treatment of secondary peritonitis. It frequently fea-tures a diffuse infection in a critically ill patient and may be causedby any of a long list of nosocomial pathogens (e.g., Pseudomonasaeruginosa, Staphylococcus aureus, and Candida albicans). Manage-ment of tertiary peritonitis is complex and must be individualizedfor each patient.
The acuteness and severity of the presenting symptoms mayhelp localize the origin of the infection. More important, however,they allow appropriate triage of these patients, who are frequentlyseen in a crowded emergency department. For example, a patientwith sudden onset of severe abdominal pain and physiologicderangement must take precedence over almost all other patients,
whereas a stable patient presenting with a chronic complaint canbe evaluated in a more deliberate fashion.The specifics of the pre-senting episode (e.g., the onset, location, and nature of the painand any changes in bowel habits) are undeniably crucial, but thepatient’s medical and surgical histories, as well as any previoussimilar illnesses, are equally critical. Many medical problems andtherapies are associated with abdominal pain or discomfort, andan accurate accounting of previous surgical manipulation of theabdomen is vital for refining the differential diagnosis, as well asfor prioritizing further tests.The question of whether a patient haspresented with similar symptoms before (particularly if thosesymptoms led to a diagnosis) may be important for determiningthe timing of any intervention, as well as for putting the currentcomplaint in the context of an ongoing condition. In fact, manypatients arrive for medical treatment with a strong (and frequent-ly correct) concept of the nature of their disease.
PHYSICAL EXAMINATION
Once the history has been obtained, a thorough physical assess-ment is performed, with the emphasis on the abdomen, the pelvis(including the vagina), and the rectum. The usual sequence—inspection, auscultation, percussion, and palpation—should befollowed as traditionally taught.This sequence need not be exten-sively reviewed here; however, certain points should be empha-sized. With the advent of laparoscopy, inspection must include acareful search for scars indicating previous operations, given thatany laparoscopic procedure can be undertaken by way of a varietyof trocar sites. Auscultation, though occasionally helpful, is alsoprobably the least specific form of examination. Percussion is valu-able for assessing tenderness, as well as for differentiating abdom-inal distention caused by intraluminal gas or free air (signaled bytympany) from that caused by fluid in the peritoneum, such asascitic fluid or blood (signaled by dullness).
Proper and humane assessment of the abdomen for tendernessvia palpation can be learned only through extensive experience.Gaining the patient’s trust is fundamental: an anxious or dis-tressed examinee may respond in a hypersensitive manner, there-by hindering the acquisition of information. An individualizedapproach is essential as well. Palpation should not be performed ina uniform manner from patient to patient; rather, the amount oftenderness present ought to be judged by the degree of pressureor indentation required to cause a given patient significant dis-comfort. In the setting of severe abdominal pain, elicitation ofrebound tenderness by means of deep palpation followed by rapidrelease of pressure usually does not improve diagnostic accuracyor alter subsequent evaluation and should therefore be discour-aged. Finally, administration of small doses of narcotics to patientswith abdominal pain is unlikely to alter an experienced examiner’sdiagnostic ability for the worse.
Occasionally, a young patient whose history and physical exam-ination (including vital signs) fit the classic clinical picture ofappendicitis may be taken to the OR without further assessment.
Recognition and Management of Intra-abdominal Infection

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 2
All other patients
Patient has suspected intra-abdominal infection
Obtain history, including previous surgical manipulation of abdomen.Perform physical examination, focusing on abdomen, pelvis and vagina, and rectum (inspection, auscultation, percussion, palpation).
Order blood tests as appropriate.• General tests of systemic response to infection• Specific tests to localize source or focus of infectionOn occasion, a young patient with classic presentation of appendicitis may be taken to OR without blood tests or imaging.
Order abdominal and pelvicCT scans.Treat specific infection as appropriate [see Figure 9].
Order diagnostic imaging as appropriate.
Free peritoneal air is present
Order abdominal and pelvic CT scans (see above, right).
Discharge from surgical care.
History and physical exam warrant exploration of abdomen for peritonitis, but confirmation (free air) is needed first; or index of suspicion for peritonitis is very low
Patient has “certain“appendicitis
Resuscitate, give antibiotics,and take to OR.
Resuscitate, give antibiotics,and take to OR.
Obtain plain abdominal films, includingupright chest film.
Patient has upper abdominalpain, elevated bilirubin level or liver function test results,or history of biliary tract disease
Order upper abdominal US.Treat specific infection as appropriate [see Figure 1].
No free peritoneal air is present, and index of suspicion forperitonitis is low
No free peritoneal air is present, but index of suspicion forperitonitis is high
Recognition and Management ofIntra-abdominal Infection

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 3
Practically speaking, however, almost all patients with significantintra-abdominal infections undergo blood tests, and most alsoundergo some sort of radiologic evaluation.
Investigative Studies
LABORATORY TESTS
Blood work can be divided into twocategories: (1) general tests designed toassess the systemic response to infectionand (2) specific tests designed to localizethe source or site of infection.The formercategory includes serum chemistries and hematology studies.Thelatter category commonly includes amylase and lipase concentra-tions (in patients suspected of having pancreatitis), bilirubin levelsand liver function tests (to evaluate hepatic or biliary tract disease),and lactate levels (when an ischemic bowel is suspected). Thesetests are discussed further elsewhere, in connection with specificinfections (see below). Urinalysis, of course, is necessary wheneverurinary tract infection or urolithiasis is a possibility.
DIAGNOSTIC IMAGING
The use of various radiologic studiesin the diagnosis of intra-abdominal infec-tion continues to evolve rapidly. Outsidethe setting of trauma, it is now very rarefor patients to undergo operations orother major interventions without firstundergoing imaging. At one time, plainfilms of the abdomen (including anupright chest film) were routinely obtained whenever a significantintra-abdominal infection was suspected, principally to detect freeperitoneal air, bowel obstruction, or fecaliths. Abdominal plainfilms proved to lack sensitivity, specificity, and anatomic definitionin this setting and consequently have, in many cases, been sup-planted by abdominal and pelvic computed tomographic scanning.There are, however, two circumstances in which plain films of theabdomen remain a reasonable first study for a patient with sus-pected peritonitis: (1) when the surgeon has almost decided, on thebasis of the history and physical examination, to explore the patientyet needs confirming evidence of perforation (i.e., free air), and (2)when the index of suspicion for peritonitis is so low that the plainfilm studies are intended to rule out an unexpected positive findingand will not be followed by an abdominal CT scan if negative.
Ultrasonography for intra-abdominal infection is useful only forfocused examination of specific organ systems; it is inferior to CTscanning for generalized surveillance of the abdomen because ofthe inability of sound waves to penetrate gas in the bowel. By farthe best-delineated use of ultrasonography is in the diagnosis ofliver and biliary tract disease, for which its ability to demonstratecholelithiasis makes it superior to CT and for which it shouldalmost always be the first radiologic test in the appropriate cir-cumstances (e.g., a classic history of biliary colic or an elevatedserum bilirubin level). Ultrasonography also visualizes the spleen,the kidneys, and the gynecologic pelvic organs well and has theadditional benefit of using no ionizing radiation.
The abdominal and pelvic CT scan, appropriately, has becomethe key diagnostic test for evaluating patients with suspected peri-tonitis. This modality is widely available throughout much of theworld, and newer scanners yield significantly higher resolutionthan older ones, with reduced scanning times and radiation expo-sure. CT is highly sensitive for free air, fluid collections, bowel wall
abnormalities, and inflammatory changes. Now that significantintra-abdominal infections—perhaps even in the setting of a per-forated viscus—are no longer automatically considered to man-date operative intervention, the ability of CT scanning to identifythe source and assess the chronicity of an infection is critical toeffective modern management. Multiple common conditions havenow been defined for which an adequate CT scan allows nonop-erative management either as definitive therapy (e.g., expectanttreatment of a simple perforated duodenal ulcer) or as a means oftemporizing (e.g., percutaneous drainage of a periappendiceal orperidiverticular abscess). In addition, in experienced hands, a neg-ative CT scan of the abdomen and the pelvis virtually excludesany significant acute surgical illness.
It must be noted, however, that a CT scan is not necessary inall patients with abdominal pain, and the decision whether toobtain one should be made on the basis of predefined guidelinesor with the input of a general surgeon.When the need for opera-tive intervention has already been determined, as in a classic caseof appendicitis, imaging is unnecessary. In addition, some patientswith an intra-abdominal infection amenable to nonoperative man-agement (e.g., simple, mild diverticular disease that can be treat-ed with oral antibiotics on an outpatient basis) do not necessarilybenefit from CT scanning.
In selected cases, other forms of imaging may be used.Magnetic resonance imaging, though usually more difficult toobtain in an emergency and logistically more complicated thanCT scanning, yields excellent tomographic images and has theadded benefit of imaging vascular structures and the pancreatico-biliary tree more precisely. Nonetheless, MRI has no significantrole in the evaluation of acute peritonitis. Nuclear medicine scansand fluoroscopic studies, though occasionally useful adjuncts forevaluating biliary tract and upper GI disorders, also play no rolein the assessment of acute peritonitis.
Options for Intervention
Once an intra-abdominal infection is diagnosed, there are mul-tiple options for intervention. Not infrequently, an approach com-bining several modalities is warranted. Occasionally, administrationof systemic antibiotics is all that is necessary (or practical), as incases of spontaneous primary bacterial peritonitis or of multipleinfected fluid collections that are small but too numerous to drain.Single abscesses, particularly those without thick or particulatecontents, can be adequately treated with simple aspiration and ashort course of antibiotics. For discrete infected fluid collections inalmost any setting, placement of a percutaneous indwelling drain(most commonly under radiologic guidance) is currently the treat-ment of choice. Operative management, either open or laparo-scopic, is employed for resection of damaged or inflamed andunsalvageable organs, diversion of enteric contents, or drainage ofcollections that are too thick or numerous for percutaneousdrainage. Beyond these general guidelines, therapy for specificintra-abdominal infections must be individualized (see below).
Infections of the Upper Abdomen
Biliary tract and pancreatic infections present as a systemic sep-tic response or as infections localized in the upper abdomen [seeFigure 1].Typical findings include abdominal pain, a tender upperabdominal mass, fever and leukocytosis, and jaundice. Variouscombinations of these symptoms may occur, but it is convenientto consider three common clinical presentations. In each of thepresentations, one or two symptoms dominate: (1) upper abdom-

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 4
inal pain and fever, (2) fever and jaundice, and (3) an upperabdominal mass and fever.These clinical findings signal the needfor a battery of screening tests, including a complete blood count(CBC); routine blood tests of liver function; determination ofserum amylase level, prothrombin time (PT), and partial throm-boplastin time (PTT); blood culture; chest and abdominal x-rays;and abdominal ultrasonography. When considered together, theclinical findings and the test results allow early differentiation ofthe three most common disease entities: acute cholecystitis, acutecholangitis, and acute pancreatitis.
UPPER ABDOMINAL PAIN AND FEVER
Patients with upper abdominal sepsis may present with epigas-tric or right upper quadrant pain and fever. Only two thirds ofthese patients admitted with a working diagnosis of acute chole-cystitis have acute biliary inflammation.1 In some patients, non-surgical conditions (e.g., pneumonia, acute hepatitis, familialMediterranean fever, herpes zoster of the intercostal nerves, andgastroenteritis) can be distinguished clinically from biliary disease.The most important screening test for acute biliary infection is the
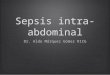
abdominal ultrasound examination: an abnormal image of thegallbladder or bile ducts supports a biliary etiology [see Figure 2].
The differential diagnosis should include acute cholecystitis,biliary colic, acute pancreatitis, and acute cholangitis, each ofwhich requires specific management [see Table 1]. For example, ini-tial management of biliary colic and mild acute pancreatitis is usu-ally nonoperative, whereas severe acute cholangitis and acutecholecystitis are treated by means of surgical, endoscopic, or radi-ologic intervention (see below). Clinical features and blood testresults, though helpful, may be inconclusive.The abdominal ultra-sonogram may provide specific clues. Stones appear in biliary colic[see Figure 2]; stones and thickening of the gallbladder wall, inacute cholecystitis; gallstones and dilatation of the common bileduct (CBD), in acute cholangitis; and pancreatic enlargement andsonolucency, in pancreatitis.
Pancreatitis
Diagnosis Differentiating acute pancreatitis from acutecholecystitis may be difficult.The serum amylase level lacks speci-ficity, but if the clinical findings suggest acute pancreatitis, an ele-
Upper abdominal pain andfever are dominant findings
Fever and jaundice aredominant findings
Fever and abdominal mass are dominant findings
Patient has choledocholithiasisor biliary dilation consistentwith cholangitis
Patient has clinical signs of upper abdominal infection,or serum bilirubin or liver function tests are suggestive
Order abdominal US.
Resuscitate, and give antibiotics.Consider emergency endoscopic, radiologic, or operative biliary drainage.
Patient has liver mass, withor without abscess
Obtain travel history and serologic tests to rule out amebicand echinococcal abscesses. For bacterial abscesses, resuscitate, give antibiotics, seek sources, and perform percutaneous drainage.
Patient has signs of pancreatic infection
Confirm diagnosis via abdominalCT scan.Resuscitate, and give antibiotics if infection is probable or necrosis is noted on CT.Discrete fluid collection: Aspirateor drain.Phlegmon: Attempt medical management. If unsuccessful and percutaneous aspirate positivefor bacteria, perform open drainage.
Stones are seen in gallbladder without evidence of cholecystitis or choledocholithiasis
Evidence of acute cholecystitis is apparent
US is normal
Consider nonbiliarydisease, especiallyacute pancreatitis.Consider abdominaland pelvic CT scans.
If US is equivocal,consider nuclearmedicine scanning.Resuscitate; take to OR for urgent cholecystec-tomy if patient is medi- cally fit, or perform percutaneous drainage if not.
Consider other diagnoses.Evaluate for electivecholecystectomy.
Patient has splenic mass, with or without abscess
Confirm diagnosis via abdominalCT scan.Resuscitate, and give antibiotics. Treat with splenectomy or percutaneous drainage.
Figure 1 Algorithm outlines approach to patient withsuspected upper abdominal infection.

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 5
vated level of serum amylase clinches the diagnosis. In one study,the initial laboratory results in 100 patients with acute pancreati-tis were compared with those in 100 patients with acute abdomi-nal pain caused by acute cholecystitis, perforated peptic ulcer, oracute appendicitis.2 The serum amylase concentrations were ele-vated in 95% of patients with acute pancreatitis but were normalin 95% of patients with acute abdominal pain from other causes.These concentrations peak within the first 48 hours and arealmost always elevated in biliary pancreatitis3; in fact, a serumamylase concentration above 1,000 U/L strongly suggests a biliaryorigin of the pancreatitis.4 In addition, determination of serumlipase levels has been shown to be more specific than and at leastas sensitive as determination of amylase levels for the detection of
acute pancreatitis.5,6 Unless clinical findings and the results of bio-chemical tests and ultrasonography are unequivocal, a contrast-enhanced spiral abdominal CT scan is usually performed to estab-lish the diagnosis and stage acute pancreatitis. It has been sug-gested, however, that CT scanning should be reserved for patientswith clinically suspected severe acute gallstone pancreatitis, on thegrounds that the results would not change the recommendedcourse of action in other patients.7 Occasionally, a very mild pan-creatitis may give rise to no findings on a CT scan, and a normaltechnetium-99m (99mTc)–labeled HIDA (lidofenin) scan may helpdifferentiate this condition from acute cholecystitis.
Treatment Given that pancreatitis encompasses a widerange of diseases with varying degrees of severity, treatment mustbe individualized for each patient. Possible therapeutic strategiesrange from outpatient management with temporary dietary mod-ification (for very mild cases) to open debridement and complexintensive care (for severe cases). It is therefore useful to base pos-sible treatment approaches in particular cases on the cause andseverity of the pancreatitis.
Gallstone pancreatitis. Standard therapy for gallstone pancreatitisincludes I.V. fluids and narcotic analgesics. Nasogastric suction isuseful in patients with significant ileus but need not be used rou-tinely.8 The use of systemic antibiotics is controversial; they are ofbenefit in the 10% to 34% of patients who have concomitantcholangitis.9 Other treatments suggested previously—includingtotal parenteral nutrition (TPN) and various pharmacologic agents(e.g., cimetidine, somatostatin, glucagon, and insulin)—have notproved useful in all cases of gallstone pancreatitis.10 Continuousintraduodenal infusion of an elemental diet has reduced exocrinepancreatic secretions in animal experiments.11 Furthermore, enter-al feeding has been shown to be beneficial and to decrease diseaseseverity in patients with acute pancreatitis.12-14
In clinical practice, the need for further treatment depends onthe severity of the acute pancreatitis. Severity determines both therisk of sepsis, which governs outcome, and the risk associatedwith early cholecystectomy [see 5:21 Cholecystectomy and Bile Duct].The most commonly used clinical prognostic index in NorthAmerica was developed by Ranson and reliably defines the sever-ity of pancreatitis [see Table 2].2 In mild pancreatitis, one or twoRanson signs are present; in more severe pancreatitis, three to fivesigns are present; and in very severe pancreatitis, more than fivesigns are present. This distinction serves to stratify further treat-ment. Other clinical prognostic scores, such as the APACHE-II(Acute Physiology and Chronic Health Evaluation II) andAPACHE-III scores and the Balthazar score, have been shown topossess discriminatory value in identifying patients at high risk forcomplications.15,16
Figure 2 Abnormal abdominal ultrasound examination showscalculi in gallbladder casting shadows on underlying liver tissue.
Table 1—Diagnostic Indicators of Upper Abdominal Pain and Fever
Biliary Colic
Short: 40% < 1 hr
Visceral
Tender
Occasionallyabnormal
Normal
Often normal
Duration
Pathogenesis
Signs
Laboratory testsLiver function tests
Serum amylase
Leukocyte counts
AcuteCholecystitis
Persistent
Somatic
Guarding andspasm
Abnormal
Normal or slightlyincreased
Increased
AcutePancreatitis
Persistent
Retroperitoneal
Guarding andspasm
Abnormal
Increased
Increased
Table 2—Ranson’s Early Objective Signs of Severity of Acute Pancreatitis2
On Admission
Age > 55 yrGlucose > 200 mg/dlWBC > 16,000/mm3
LDH > 350 IU/L
AST > 250 Sigma Frankel U/dl
After Initial 48 Hours
Serum Ca2+ < 8 mg/dlArterial PO2 < 60 mm HgBase deficit > 4 mEq/LBUN increase > 5 mg/dlHematocrit fall > 10%Fluid sequestration > 6,000 ml
Note: < 3 signs = mild pancreatitis; ≥ 3 signs = severe pancreatitis.AST—aspartate aminotransferase—BUN—blood urea nitrogen—PO2—oxygen tension—WBC—white blood cell

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 6
Mild pancreatitis usually subsides within 1 week of onset. Mostsurgeons defer cholecystectomy until then; urgent operation shouldbe reserved for cases complicated by biliary sepsis, and it mayreveal acute cholecystitis in as many as 31% of patients.17
An attack of acute gallstone pancreatitis is initiated by obstruc-tion at the confluence of the lower end of the CBD and the pan-creatic duct by a stone or by edema at the ampulla of Vater result-ing from stone migration. These stones may be found andremoved in 63% to 78% of patients who undergo operation with-in 72 hours of admission17-19 [see 5:22 Biliary Tract Disease]; bycontrast, they are present in only 3% to 33% of patients exploredafter the first week.18-22 A randomized trial exploring the optimaltiming of surgery for gallstone pancreatitis showed that earlysurgery (within 48 hours after admission) was not associated witha significant increase in morbidity or mortality in patients withmild pancreatitis but did not change prognosis.23
Endoscopic retrograde cholangiopancreatography (ERCP). EarlyERCP and sphincterotomy [see 5:18 Gastrointestinal Endoscopy] hasbeen suggested as an alternative to surgery of the CBD in patientswith mild pancreatitis. However, randomized trials comparingendoscopic treatment with conservative treatment within the first72 hours in patients with mild pancreatitis did not find that urgentendoscopic sphincterotomy improved outcome in this group ofpatients.24,25 Other studies showed that delaying surgery beyond 6weeks may lead to a 32% to 57% risk of recurrent pancreatitis.26,27
Therefore, cholecystectomy and cholangiography should bedelayed only until just before patients are discharged from the hos-pital, 5 to 15 days after the onset of symptoms. Laparoscopic
cholecystectomy has facilitated this approach safely without pro-longing hospital stay.
Severe pancreatitis. Patients with three or more Ranson signs areat particular risk for pancreatic sepsis.28 Repeated clinical andradiologic evaluation is required in these patients to ensure earlydetection of complications, because the outcome of an episode ofpancreatitis depends on whether sepsis supervenes. When infec-tion occurs, operative debridement and drainage are required [seeFever and Abdominal Mass, below]. Some surgeons have attempt-ed to alter the course of severe disease by early operation; howev-er, urgent operation is associated with a high mortality in patientswith more than three Ranson signs.19,21,23,29 To avoid the mortali-ty associated with early operative intervention, some cliniciansadvocate early diagnosis by ERCP [see Figure 3], followed by bil-iary decompression by means of endoscopic sphincterotomy andstone extraction. In a randomized trial comparing early ERCP andsphincterotomy with conservative therapy in patients with severeacute pancreatitis, ERCP and sphincterotomy decreased morbid-ity from 61% to 24% and lowered mortality from 18% to 4%.24
The results of this trial, however, have been the subject of debate,and the success of this approach has been attributed by someauthors to the treatment of a concomitant cholangitis rather thanof the actual pancreatitis.25 A well-conducted trial that excludedpatients with concomitant cholangitis was published in 1997;unfortunately, this trial was unable to answer the question defini-tively, because too few patients with severe pancreatitis had beenrecruited.30 It appears that ERCP is warranted mainly in cases ofacute pancreatitis complicated by cholangitis and biliary sepsis.31,32
Use of peritoneal lavage in early severe pancreatitis was advo-cated in one study to decrease morbidity and mortality.33 Use ofstandard lavage over a 2-day period did not improve patient out-come, but use of peritoneal lavage for 7 days (long peritoneallavage) yielded some improvement in outcome.34 Early use ofantibiotics and selective decontamination have been proposed as ameans of reducing septic complications, but neither has convinc-ingly or reproducibly been shown to improve prognosis.35,36
Although prophylactic antibiotics have been shown to decrease therate of infectious complications in severe acute pancreatitis, theyhave not clearly been shown to reduce overall disease mortali-ty.35,37-40 Attempts have been made to modulate the initial systemicinflammatory response seen in early severe acute pancreatitis toreduce the risk of subsequent infection and improve overall prog-nosis; somatostatin has exhibited limited success in this regard.41,42
Another drug in this category, the platelet-aggregating factor(PAF) inhibitor lexipafant, initially yielded promising results inanimal models43,44 and in phase II trials45; however, a 2001 trialusing the same drug did not find it efficacious for treating severeacute pancreatitis.46
Acute Cholecystitis
Diagnosis Acute cholecystitis is the most common diagnosisin patients presenting with upper abdominal pain and fever and ischaracterized by the clinical finding of a midinspiratory arrest onpalpation of the right upper quadrant (Murphy’s sign). As noted(see above), with the widespread availability of ultrasonography,acute cholecystitis can usually be diagnosed rapidly on the basis ofthe findings of gallbladder wall thickening, pericholecystic fluid,and stones. Occasionally, more complex cases must be evaluatedwith nuclear medicine scanning to look for cystic duct obstruc-tion. Concurrent acute obstructive cholangitis must also be con-sidered in all patients with acute cholecystitis. Supportive labora-tory data include a high serum bilirubin level and an increased
Figure 3 Endoscopic retrograde cholangiopancreatographyshows distal CBD stone in acute pancreatitis. Papillotome hasbeen placed through sphincter of Oddi in preparation for endo-scopic sphincterotomy.

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 7
alkaline phosphatase level. Positive blood cultures and dilated biliary ducts on abdominal ultrasonography usually confirm thediagnosis.
Emphysematous cholecystitis. An uncommon and insidious vari-ant of acute cholecystitis, emphysematous cholecystitis is charac-terized by gas in the gallbladder lumen or wall or in the perichole-cystic soft tissue and biliary ducts secondary to gas-forming bac-teria.The key to the diagnosis is the presence of air on abdominalx-ray [see Figure 4] or ultrasound examination. Three stages ofemphysematous cholecystitis have been defined: (1) gas is seenonly in the lumen of the gallbladder, (2) a ring of gas is identifiedin the wall of the gallbladder, and (3) gas is seen in the tissues adja-cent to the wall. Compared with ordinary acute cholecystitis,emphysematous cholecystitis is associated with a fivefold increasein the risk of gallbladder perforation, as well as a 10-fold increasein mortality in patients younger than 60 years [see Table 3].47
Studies from the 1960s noted an increased risk of gangrene andperforation of the acutely inflamed gallbladder in patients withdiabetes mellitus.48,49The mortality for acute cholecystitis was alsoshown to be five to 10 times higher in patients with diabetes thanin other patients. Later studies, however, did not show an in-creased mortality in patients with both diabetes and acute chole-cystitis.50,51 Nevertheless, one third of patients with emphysema-tous cholecystitis also have diabetes.This factor, coupled with thecurrent tendency to perform cholecystectomy early in most pa-tients with acute cholecystitis, may account for the disparity be-tween previous studies and later reports.
Acute acalculous cholecystitis. Another variant of acute cholecys-titis is acalculous cholecystitis; though still rare, it became morecommon from the 1950s through the 1990s.This disease was orig-inally described as occurring after surgical treatment of unrelateddisease but was subsequently identified in patients with multipletrauma, prolonged critical illness, and sepsis. Predisposing factorsinclude gallbladder ischemia (in patients with shock or trauma)and biliary stasis (in prolonged fasting, hyperalimentation, and
sustained narcotics therapy). In addition, focal inflammation maycause biliary colonization or may activate coagulation factor XII,thereby causing severe injury to the blood vessels in the gallblad-der muscularis and serosa. A high index of suspicion is necessary.Acute acalculous cholecystitis should be considered in any post-operative or acutely ill patient with upper abdominal pain andfever or with unexplained fever and leukocytosis. It is particularlycommon 2 to 4 weeks after injury.The diagnosis is confirmed byfindings on abdominal ultrasound examination [see Figure 5] and99mTc-labeled HIDA scanning coupled with infusion of cholecys-tokinin and morphine.52-54
Treatment Standard treatment of acute cholecystitis consistsof I.V. fluid administration, analgesics, and cholecystectomy.Although the timing of operation is somewhat controversial inordinary acute cholecystitis, cholecystectomy should be per-formed at the earliest opportunity [see 5:21 Cholecystecomy/Bile c -Duct]. This approach has been confirmed by at least one ran-domized trial comparing early with late laparoscopic cholecystec-tomy.55 The delayed-surgery group had a greater need for conver-sion to open cholecystectomy (23% versus 11%), as well as a longer
Figure 4 Air outlines gallbladder and bile ducts in emphysema-tous cholecystitis.
Table 3—Comparison of Acute Cholecystitis and Emphysematous Cholecystitis
Gender
Stones
Bile culture positive
Clostridia found
Gangrenous gallbladder
Perforation of gallbladder
Mortality at age < 60 yr
Pathogenesis
EmphysematousCholecystitis
70% male
70%
95%
46%
75%
20%
15%
Ischemia, obstruction
Acute Cholecystitis
70% female
90%
66%
1.2%
2.5%
4%
1.5%
Obstruction
Figure 5 Abnormal abdominal ultrasound examination con-firms diagnosis of acute acalculous cholecystitis. When image iscompared with that in Figure 2, thickening of gallbladder walland intraluminal debris are obvious.

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 8
average total hospital stay and convalescence. Administration ofsystemic antibiotics is not required; however, single-dose antibiot-ic prophylaxis (e.g., cefazolin, 2 g I.V.) can be given at the start ofthe operation [see 1:1 Prevention of Postoperative Infection].56-58
Some patients with acute cholecystitis are at high risk for gan-grene and perforation of the gallbladder. It is crucial to identifythese patients and perform cholecystectomy promptly becausedelay increases morbidity and mortality. Clinically, gangrene andperforation of the gallbladder in this high-risk population are sug-gested by marked systemic toxicity or by the radiologic demon-stration of either emphysematous cholecystitis or acute acalculouscholecystitis.
With ordinary acute cholecystitis, body temperature is slightlyincreased in most patients—averaging 37.8º C (100.04º F)—butis normal in 20% of patients. By comparison, the risk of gangreneand perforation is reportedly higher in patients with marked sys-temic toxicity, manifested by a pulse rate greater than 120beats/min, a body temperature higher than 39º C (102.2º F), anda left shift in the differential white blood cell count, showing morethan 90% polymorphonuclear leukocytes. Unfortunately, findingsof systemic toxicity are frequently absent in elderly patients.
Patients with acute cholecystitis who have signs of systemic tox-icity, emphysematous cholecystitis, or acalculous cholecystitis areat high risk for gallbladder gangrene and perforation and thereforerequire prompt and aggressive treatment. I.V. antibiotic therapywith a single agent (e.g., ceftriaxone, piperacillin, or a quinolonesuch as ciprofloxacin or ofloxacin) can be given.59,60 Early chole-cystectomy is the treatment of choice. Unfortunately, mortalitymay be as high as 20% to 30% with the traditional surgical ap-proach.61 If perforation and gangrene are not suspected but med-ical illness poses a high risk of mortality from operation, nonoper-ative supportive therapy may suffice. If this fails, another treatmentoption is cholecystostomy.
Percutaneous transhepatic cholecystostomy has been recom-mended for these high-risk patients,62 particularly where there is alow risk for perforation of the gallbladder.63 To determine the riskof gallbladder perforation, a risk score can be assigned to each ofseven findings that may be present on the preoperative abdominalultrasound examination: pericholecystic fluid, 7 points; distentionof the gallbladder, 4 points; intraluminal membrane, 4 points;intraluminal debris, 3 points; round gallbladder, 3 points; sonolu-cent zone in the gallbladder wall, 2 points; and a thick gallbladderwall (> 3.5 mm), 1 point.63 A patient with a total risk score of 12or more points requires urgent cholecystectomy; one with a lowerscore who does not respond to conservative treatment may betreated with percutaneous transhepatic cholecystostomy.
A 1997 review of 59 patients exhibiting the septic response whounderwent successful percutaneous radiologic cholecystostomydefined predictors of a successful clinical outcome: localized rightupper quadrant tenderness and gallstones, as well as gallstonesand pericholecystic fluid on ultrasound examination.64 Patientswith more equivocal findings may derive greater benefit frommore invasive techniques that can simultaneously be used fordiagnostic purposes (e.g., laparoscopy, which can even be per-formed at the ICU bedside65).
A few patients with acute cholecystitis will have concurrentacute cholangitis. Cholecystostomy is contraindicated in thesepatients because of its high mortality; adequate drainage of theCBD is required in such cases [see Fever and Jaundice, below].
FEVER AND JAUNDICE
An alternative presentation of upper abdominal infectionincludes patients whose predominant symptoms are fever and
jaundice, with pain a less marked component. Jaundice is almostalways associated with obstruction of the biliary tree, either intra-hepatic or extrahepatic. The combination of fever with jaundicealways suggests acute cholangitis, a condition that can have a ful-minant and fatal course if not treated promptly.
Acute Cholangitis
Diagnosis If a patient presents with a temperature higherthan 38.5º C (101.3º F) in conjunction with jaundice [see 5:3Jaundice], the possibility of acute cholangitis should always beinvestigated. If cholangitis is present, laboratory studies will revealleukocytosis, and blood cultures will often be positive. A finding ofgallstones and dilated biliary ducts on abdominal ultrasound exam-ination supports the diagnosis. Reynolds’ pentad is present in thefull-blown syndrome.66 This syndrome includes upper abdominalpain, fever and chills, jaundice, hypotension, and mental statuschanges. Acute cholangitis is usually related to choledocholithiasis,recent biliary manipulation, or biliary stenting performed for chron-ic obstruction.
Gallbladder infections. Gallbladder empyema can duplicate mostof the findings associated with acute cholangitis. In this condition,acute cholecystitis is complicated by suppuration within the gall-bladder, which then becomes the focus of generalized sepsis.Thedistended gallbladder may be palpable and tender.When jaundiceis associated with empyema of the gallbladder, it is less likely to beobstructive than when it is associated with acute cholangitis.Trueempyema of the gallbladder is rare. Treatment includes adminis-tration of I.V. fluids, systemic antibiotic therapy, analgesics, andearly cholecystectomy.
In some patients with jaundice and inflammation, a stoneimpacted in the cystic duct or in Hartmann’s pouch may suggestcholedocholithiasis, but preoperative diagnosis by ERCP shows anextrinsic compression of the duct known as Mirizzi syndrome.Twotypes of Mirizzi syndrome exist. In type I, a stone impacted in thecystic duct or Hartmann’s pouch compresses the common hepaticduct and causes inflammation, thereby leading to jaundice.Treatment of this type consists of obliteration of the cystic duct andcareful partial cholecystectomy, with the neck of the gallbladder leftin place. In type II, protrusion of the stone into the hepatic ducterodes the septum between the cystic duct and the hepatic ductand causes a cholecystocholedochal fistula.Treatment of this typeinvolves internal biliary drainage to the wall of the cholecysto-choledochal defect, usually with a choledochojejunostomy [see 5:22Biliary Tract Disease], in addition to cholecystectomy.67
Primary sclerosing cholangitis. Patients with primary sclerosingcholangitis, especially those who have undergone internal or exter-nal biliary drainage, are at high risk for recurrent bouts of ascend-ing cholangitis. Primary sclerosing cholangitis predominantly affectsyoung males, particularly those with chronic ulcerative colitis.Thediagnosis is suggested by the dominant cholestatic biochemicalprofile—that is, elevation of the serum bilirubin concentration, theserum alkaline phosphatase level, and aspartate aminotransferaseactivity. Because of the concomitant hepatic scarring, ultrasonog-raphy may not reveal the presence of dilated intrahepatic ducts.Definitive diagnosis requires visualization of the beaded appear-ance of the biliary tree by means of cholangiography. Cholangio-carcinoma and secondary sclerosing cholangitis in patients withCaroli disease or choledochal cysts may mimic these clinical, bio-chemical, and radiologic features, but this is an unusual occur-rence and can be distinguished by careful follow-up of patients.
Currently, magnetic resonance cholangiopancreatography(MRCP) is the imaging modality of choice for elective manage-ment of patients with primary sclerosing cholangitis, in that it yields

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 9
results comparable to those of ERCP without being invasive.68-71
Other causes of cholangitis. An uncommon cause of recurrentcholangitis in North America is Oriental cholangiohepatitis, whichis characterized by intrahepatic duct scarring, biliary strictures,and hepatolithiasis, as demonstrated by cholangiography. Irrever-sible intrahepatic and extrahepatic liver damage may result be-cause of the overwhelming propensity of these patients to formcalcium bilirubinate stones.
A few patients with cholangiocarcinoma causing bile duct ob-struction or liver metastases causing intrahepatic bile duct obstruc-tion may also present with a clinical picture suggestive of cholan-gitis. CT followed by MRCP can delineate the diagnosis in mostsuch cases.Treatment consists of I.V. antibiotics and biliary drain-age by radiographic or surgical means.
Treatment Once acute cholangitis is diagnosed, resuscita-tion is started with I.V. fluids and antibiotics, such as fluoro-quinolones, mezlocillin, cefoperazone, or piperacillin,59,72-75 partic-ularly in patients with marked hyperbilirubinemia, in whom treat-ment with aminoglycosides may contribute to renal toxicity in upto 33% of cases [see 8:6 Renal Failure].76 These antibiotics arerequired to deal with the various aerobic bacteria, of whichEscherichia coli,Klebsiella species, and enterococci are the most fre-quently encountered in this setting. Anaerobes may be isolated in15% to 30% of patients and are particularly likely to be present indiabetics, the elderly, and patients who have previously undergonebiliary manipulation. In patients with indwelling catheters,Enterobacter,Pseudomonas, and Candida organisms are being isolat-ed with increasing frequency. Indications of high risk include aserum bilirubin concentration higher than 3 mg/dl.
Approximately 75% of patients with acute cholangitis respondto conservative measures,77 and supportive treatment is contin-ued. Subsequent investigations usually include CT followed byMRCP.78,79 Because of their invasive nature, ERCP and needlepercutaneous transhepatic cholangiography (PTC) are reservedfor cases in which a drainage procedure is anticipated or the infor-mation from the MRCP is deemed inadequate.
For the 25% of patients who do not respond to conservativetreatment, early recognition may improve their prognosis. In onestudy, patients who did not respond immediately to antibioticshad a mortality of 62%, compared with a mortality of 1.5% inthose who improved.80 In another study, indicators of high riskwere an arterial blood pH less than 7.4, a serum bilirubin con-centration above 9 mmol/L, a blood platelet count below150,000/mm3, and a serum albumin concentration lower than 3g/dl.102 These high-risk patients often have systemic hypotension,mental confusion, a temperature higher than 39º C (102.2º F), orhypothermia. Occasionally, acute cholangitis is complicated by dis-seminated intravascular coagulation (DIC), which manifests itselfas a tendency to bruise and bleed or merely as prolongation of thePT and the PTT, together with a fall in the blood platelet count[see 1:4 Bleeding and Transfusion]. If DIC is suspected, the diagno-sis should be confirmed and treatment started before biliarydecompression.
Patients with refractory cholangitis who do not improve within24 hours require urgent biliary decompression. Urgent biliarydecompression had traditionally been accomplished via surgicalexploration of the CBD and T-tube drainage [see 5:22 Biliary TractDisease]. Cholecystostomy is an inadequate and often fataloption in this context. Rarely, T-tube insertion alone may be life-saving in a desperately ill patient; generally, however, definitiveinternal decompression is preferable. Unfortunately, any surgical
decompression in these critically ill patients can result in a mor-tality of 30% to 40%.82-85 Furthermore, reoperation is required inone third of survivors because important diagnostic information isnot available at the initial laparotomy. As a result, nonoperativemethods of biliary decompression, including percutaneous trans-hepatic biliary drainage (PTBD) and endoscopic sphincterotomyat ERCP, have gained favor. PTBD was originally developed forpreoperative management of biliary obstruction without cholangi-tis but has not been found to be beneficial in that setting. At pres-ent, it is mainly used for the management of proximal bile ductstrictures or for the treatment of cases not amenable to ERCP; itscomplication rate is less than 10%.86
Although PTBD can reduce the mortality associated with ini-tial biliary decompression, many patients still require a definitiveoperation. Consequently, endoscopic sphincterotomy [see 5:18 Gas-trointestinal Endoscopy] has been proposed for decompression ofthe biliary tree in patients with acute cholangitis from choledo-cholithiasis [see Figure 6]. In a study of 82 patients with acutecholangitis caused by CBD calculi, early operation was employedin 28 patients, endoscopic sphincterotomy in 43, and antibiotictherapy alone in 11.87 Surgical mortality was 21% and morbidity57%; by comparison, mortality for endoscopic sphincterotomywas 5% and morbidity 28%. Others confirmed these findings.81 Inpatients whose gallbladder is still in place, endoscopic sphincter-otomy alone, without cholecystectomy, may even be a reasonablelong-term option. Of 23 patients whose gallbladders were left insitu,87 only two required cholecystectomy in the 1- to 7-year fol-low-up period: one for empyema of the gallbladder and one forrecurrent cholangitis.
An increasingly recognized cause of cholangitis is biliary sepsisafter manipulation of the biliary tree with ERCP or PTBD.Treatment includes I.V. fluids and antibiotics. To prevent thiscomplication, prophylactic antibiotics should be administered be-fore every biliary manipulation.88
FEVER AND ABDOMINAL MASS
A third group of patients with upper abdominal infection pre-sent with fever and an upper abdominal mass identified either byclinical signs or through diagnostic imaging. Even if the mass isonly vaguely palpable, the mass effect is demonstrable on ultra-sound examination of the abdomen. If the abdominal ultrasoundexamination is technically unsatisfactory because of intestinal gas,contrast-enhanced CT of the abdomen will facilitate the diagnosis.
The differential diagnosis is aided by the location of the mass.A mass in the right upper quadrant usually indicates acute chole-cystitis, though the possibility of a liver abscess must also be con-sidered. A mass in the epigastrium or in the left upper quadrantusually signals a pancreatic infection; in rare instances, a solitarysplenic abscess is found. Patients with an intra-abdominal abscessin the subphrenic space or an interloop abscess may also presentin this manner.
Liver Abscess
Diagnosis In the setting of acute upper abdominal sepsis, atender mass in the right upper quadrant is most likely an enlarged,inflamed gallbladder, possibly wrapped with omentum [see UpperAbdominal Pain and Fever, Acute Cholecystitis, above].The nextmost common cause of fever and abdominal mass in the rightupper quadrant, however, is liver abscess.
Pyogenic abscess.Today, pyogenic liver abscess is most common-ly related to biliary tract obstruction from gallstones or malignantdisorders (35% of cases), and the ultrasound examination may

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 10
reveal both the abscess and the dilated biliary ducts. Previously,portal pyemia from diverticulitis, inflammatory bowel disease(IBD), or perforated appendicitis had been the most commoncause; it now accounts for 20% of cases. Even less common ishematogenous spread via the hepatic artery. Approximately 20%of hepatic abscesses are cryptogenic. Ultrasonographic imaging ofthe liver may demonstrate lesions as small as 2 cm in the liver sub-stance. CT scanning, however, is superior to ultrasonography forevaluating the presence of air and abscesses as small as 0.5 cm indiameter, especially near the hemidiaphragms.89 Abdominal CT isalso the diagnostic modality of choice in the postoperativepatient.90 ERCP and PTC are indicated only when gallstone dis-ease or a biliary malignancy is the potential source of the abscess.Most liver abscesses occur in the right lobe: 40% are 1.5 to 5 cmin diameter, 40% are 5 to 8 cm in diameter, and 20% are greaterthan 8 cm in diameter.
Amebic abscess. Although pyogenic abscesses are commonlymultiple, no imaging technique can reliably differentiate themfrom amebic abscesses.The best indication of a parasitic infectionis a history of travel to an endemic area (e.g., Mexico, CentralAmerica, or Southeast Asia). However, when a hepatic abscess isdetected by an imaging technique, serologic tests should be per-formed to rule out active amebiasis or echinococcal infection.Examination of stool for amebae is insensitive; consequently,
isoenzyme analysis, Entamoeba histolytica–specific antigen detec-tion, or even polymerase chain reaction (PCR) is preferred to con-firm the diagnosis of amebiasis.91
Echinococcal abscess. The diagnosis of echinococcal liver abscesscan be confirmed by means of elevated indirect hemagglutination(IHA) titers (> 250). In the late 1980s, a combination of tests thatincluded IHA for Echinococcus granulosus and enzyme-linked im-munosorbent assay (ELISA) using E. multilocularis antigen yieldedan 89% species-specific diagnosis of echinococcal disease.92 Laterwork indicated that IgG ELISA and IHA were the best tests forfollow-up after resection of the abscess. In patients with a favor-able clinical outcome, the specific IgG level decreased toward theend of the first year, though in some cases, a positive serologicresult persisted beyond 6 years.93 Diagnostic aspiration is indicat-ed when a diagnosis of pyogenic or amebic abscess is in doubt, butnot in echinococcal disease. Aspiration may also be beneficial inpatients with left-side abscesses and abscesses greater than 10 cmin diameter. The chest x-ray is abnormal in as many as 50% ofcases of amebic abscess, and the plain abdominal x-ray may showcalcification of an echinococcal cyst with secondary pyogenicinfection.
It is essential to differentiate infected echinococcal cysts frompyogenic abscess: special precautions are required for drainage ofechinococcal cysts because of the risk of spillage and anaphylaxis.
Figure 6 Endoscopic sphincterotomy for acute biliary decompression in acute obstructive cholangitis is shown.At left, stone is visible in common hepatic duct, and papillotome has been passed through sphincter of Oddi. Atright, stone is held within a Dormia basket before extraction.

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 11
Blood cultures are positive in as many as 50% of patients withpyogenic abscess, particularly in those with multiple abscesses; infact, the presence of Streptococcus milleri in the blood suggests a vis-ceral abscess.
Treatment Pyogenic abscess. The preferred treatment of pyo-genic abscess is closed continuous percutaneous drainage guidedby CT or ultrasonography, provided that it is technically feasibleand no other indication for laparotomy exists.94 More than onecatheter may be required for complete drainage. An alternativetreatment is repeated percutaneous needle aspiration, the resultsof which are comparable to those of continuous drainage.95 Oneadvantage to repeated needle aspiration is the elimination of cum-bersome, painful drainage tubes, which are prone to dislodgment.Although initial studies showed a good response rate with repeat-ed needle aspiration,96 the results were not duplicated in a subse-quent randomized trial.97
The abscess cavity dimensions are followed by serial imaginguntil the cavity collapses, and the catheter can usually be removed2 to 3 weeks later. Continuous percutaneous drainage has beenassociated with a complication rate of 4% and a failure rate of15%.98 However, operative drainage is the treatment of choice inpatients with an identified intra-abdominal focus of infection andin patients in whom percutaneous drainage is not feasible or hasfailed.99 Operative drainage, especially via a laparoscopic approach,is a highly effective treatment option that is associated with lowmortality and morbidity.100 In some patients, a limited hepaticresection [see 5:23 Hepatic Resection] may be required to eliminatemultiple abscesses, particularly when an underlying intrahepaticstricture is the source.101
Treatment of pyogenic liver abscess should include systemicantibiotic therapy. Approximately 70% of pyogenic liver abscessesyield polymicrobial isolates,102 and 25% to 45% of the organismsare anaerobic.103 Multiple anaerobic isolates suggest the colon as asource, whereas a single isolate of E.coli suggests a nidus in the bil-iary tree. Antibiotic treatment should include initial coverage ofboth aerobes and anaerobes with either a single agent or multipleagents.The need to cover enterococci has been debated, but theseorganisms clearly are increasingly important nosocomial patho-gens. An acceptable initial treatment regimen consists of a singlebroad-spectrum agent (e.g., ticarcillin-clavulanate or meropenem).It should be noted that significant changes have occurred in the eti-ology, bacteriology, and treatment of liver abscesses. There is atrend toward a higher incidence of pseudomonal and streptococcalinfections, and the frequency of fungal infection is increasing aswell.104 The mortality from this disease remains high, and appropri-ate antibiotic coverage with drainage is of paramount importance.
The duration of antibiotic therapy is controversial105; accordingto one set of guidelines, antibiotics should be continued for 3 to 4weeks when the abscess has been excised, 4 to 8 weeks when a soli-tary abscess has been drained, and 6 to 8 weeks when multiplemacroscopic abscesses have been drained.106 Multiple microscopicabscesses usually require that a biliary source also be treated.85Theoverall prognosis for multiple small hepatic abscesses is not as goodas that for solitary abscesses, and the development of a pyogenicabscess in a patient with an underlying hepatobiliary or pancreaticmalignancy has been identified as a preterminal event associated witha hospital mortality of 28% and survival of less than 6 months.107
Amebic abscess. Medical treatment is now the standard approachto management of amebic liver abscesses. Metronidazole, 750 mgorally three times a day for 10 days, is a highly effective regimen.108
A favorable response to treatment occurs within 4 to 5 days, and
a decrease in the size of the abscess is apparent within 1 week onultrasonographic examination, though a small residual cavity maypersist for as long as 2 years. If the patient’s condition does notimprove, needle aspiration and culture are indicated. Secondaryinfection is treated as a pyogenic abscess. Otherwise, oral emetine,65 mg/day, is added for up to 10 days.
Echinococcal abscess. Symptomatic or secondarily infected echi-nococcal cysts are best treated by means of surgical excision ormarsupialization.The use of oral anthelmintics (e.g., albendazoleand mebendazole) has met with limited success. Nevertheless, pre-operative treatment with albendazole or mebendazole for 1 month,combined with postoperative treatment, is indicated to reduce therisk of intraoperative seeding or postoperative recurrence.109,110
Pancreatic Infection
Diagnosis When the mass is located in the epigastrium or theleft upper quadrant, a pancreatic source is most likely. Prompt andaccurate diagnosis is crucial because severe pancreatic infection isfatal if left untreated.The key to successful treatment is early diag-nosis of infected pancreatic necrosis, infected pseudocyst, and pan-creatic abscess. A high index of suspicion is required to diagnosethese three infectious processes and to differentiate them from apancreatic inflammatory mass or phlegmon,28 in which pancreaticedema and inflammation are present without necrosis or infection.
Correct diagnosis and treatment of infected pancreatic necrosis,infected pseudocyst, and pancreatic abscess require an under-standing of their pathophysiology. It is generally assumed thatinfected pancreatic necrosis develops as a transmural, transductal,lymphatic, or hematogenous infection of a necrotic region of thepancreas. Infection develops in 40% of cases of pancreatic necro-sis, usually in week 2 or 3 after development of the acute pancre-atitis.111 Surgical debridement is required in these cases to preventdeath. Pancreatic abscesses form by liquefaction of infected necro-sis.They usually occur after week 5 of pancreatitis, when the acutephase of the disease has subsided.112 Pancreatic abscesses are asso-ciated with a lower mortality than infected pancreatic necrosis.Like pancreatic abscesses, infected pancreatic collections andpseudocysts present late in the course of pancreatitis. They areassociated with a lower mortality than pancreatic abscesses.Caused by infection in 13% of localized collections resulting fromductal blowout, infected pancreatic collections and pseudocystsmay occur in the pancreas itself, in contiguous peripancreatic tis-sue, or in remote (extrapancreatic) tissue.
Clinical evaluation alone is generally insufficient to diagnosepancreatic infection. A clearly defined upper abdominal mass ispalpable in only 50% to 75% of cases.28 In most patients, thescreening battery of tests reveals leukocytosis with leukocytecounts greater than 15,000/mm3. Blood cultures are positive in50% of cases. CT-guided percutaneous aspiration with Gram stainand culture provides the best method of diagnosing pancreaticinfection. In one study of 75 patients with clinical toxicity sugges-tive of pancreatic sepsis, infection was confirmed in only 40%.113
In another study of 21 patients with pancreatic infection, only fivehad specific signs on abdominal CT scan.114 CT-guided diagnos-tic needle aspiration leads to a correct diagnosis within 72 hoursin two thirds of patients, and the mortality associated with opera-tive intervention is 19%; however, CT-guided needle aspiration isbeneficial only if pancreatic infection is suspected and if the tech-nique is used early in the course of disease.
Several laboratory markers of pancreatic necrosis have beeninvestigated, such as serum methemalbumin, serum ribonuclease,and C-reactive protein. Most of these markers are too insensitive

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 12
for routine clinical practice. However, serum levels of C-reactiveprotein above 10 mg/dl have been reported to be 95% accurate inpredicting necrosis.115
Currently, the best indicators of infected pancreatic necrosis orabscess are a combination of Ranson’s objective prognostic signs[see Table 2] and dynamic abdominal CT scan findings. In Ranson’sseries, the pancreatic findings on CT were graded in five categories[see Figure 7]116: (a) normal, (b) pancreatic enlargement alone, (c)inflammation of the pancreas and peripancreatic fat, (d) one peri-pancreatic fluid collection, and (e) two or more peripancreatic fluidcollections. Only category e was associated with a high (61%) inci-dence of pancreatic abscess. The number of objective prognosticsigns present also predicted the subsequent development of anabscess: fewer than three signs, 12.5%; three to five signs, 31.8%;and more than five signs, 80%. However, the value of this methodwas limited because only five of the 83 patients evaluated had morethan five prognostic signs. By combining the objective prognosticsigns with positive abdominal CT findings, the investigators identi-fied 30 patients who had three or more objective signs and weregraded as category c, d, or e on abdominal CT scan; in thesepatients, the incidence of pancreatic abscess was 56.7%. By con-trast, no patient with fewer than three prognostic signs and gradedas category a or b on abdominal CT scan had a pancreatic abscess.
Treatment Once pancreatic infection is diagnosed, support-ive measures are initiated, including nasogastric suction, with-holding of oral feedings, meticulous attention to respiratory careand fluid and electrolyte balance, systemic antibiotic therapy, andnutritional support. The key to successful treatment, however, issurgical, radiologic, or endoscopic drainage.
Pancreatic necrosis. Sterile pancreatic necrosis alone is not anindication for surgical debridement. In one prospective study, 11patients with sterile pancreatic necrosis were all followed success-fully with conservative treatment.117 However, once infected pan-creatic necrosis is confirmed by Gram stain or culture, surgicaldebridement is required to remove the characteristically thicknecrotic material; radiologic or endoscopic methods alone are notas effective for this purpose.
The choice of drainage technique is nevertheless controversial.Many clinicians prefer operative debridement and sump drainage.The mortality associated with extensive operative debridement (so-called necrosectomy) and sump drainage may range from 30% to40%,118 and this technique may be associated with a 30% to 40%reoperation rate because of sepsis or GI complications.28,119
Open drainage. To reduce the frequency of reoperation and tolower mortality, some clinicians opt for open drainage or marsu-pialization of the infected pancreas. One modification involves theuse of a prosthetic mesh and a zipper to facilitate reexploration inpatients with severe intra-abdominal abscess.120 A 1991 meta-analysis of published surgical studies on infected pancreatic necro-sis found statistically better results with debridement and lavage ordebridement and open packing than with extensive debridementand sump drainage.121 However, surgical treatment should be cus-tomized for each patient. In one study, open packing was used formassive necrosis (more than 100 g removed by debridement atoperation or CT evidence of at least 50% pancreatic necrosis) orfor extrapancreatic necrosis, whereas conventional debridementand sump drainage were used in other cases; the overall mortalityin this study was only 14%.122
Pancreatic abscess. Pancreatic abscess resulting from liquefactionof necrosis is also best treated by surgical drainage because resid-ual necrosis may cause failure of treatment by percutaneous meth-ods.123 On the other hand, infected pancreatic fluid collections and
pseudocysts can usually be treated nonoperatively. In one prospec-tive study, percutaneous and surgical drainage were equally suc-cessful in treating infected pancreatic fluid collections and pseudo-cysts.124 Clinical signs of progress rather than CT findings are thebest indicators of the need for intervention, and nonoperativemethods should be attempted before open surgery is planned.
Adjunctive procedures. In the past, debridement and sumpdrainage were accompanied by the so-called triple ostomy tech-nique, which involved cholecystostomy, gastrostomy, and jejunos-tomy. The role of these ancillary procedures, however, is contro-versial at best, and currently, cholecystostomy is employed only ifgallstones are detected.
Other operative procedures may be required to manage gastricor colonic complications. Gastric bleeding, gastric outlet obstruc-tion, and gastric fistula necessitating reoperation are relativelyinfrequent in this setting. By contrast, colonic necrosis and fistulaformation are relatively common and occur either spontaneouslyor as complications of treatment.The usual site of involvement isthe splenic flexure or upper descending colon.Treatment consistsof colonic resection or a diverting colostomy [see 5:34 Laparo-scopic Coloctomy].
Antibiotic therapy.The role of systemic antibiotic therapy in theprophylaxis of pancreatic abscess is controversial. Experimentalevidence suggests that antibiotics may sometimes decrease theseverity of pancreatitis,125 and endoscopic cannulation of thepancreatic duct has yielded bacteria in pancreatic secretions ofpatients with acute pancreatitis.126 In patients with pancreaticabscess, bacteriologic cultures are usually polymicrobial, themost common organisms being E. coli, enterococci, Klebsiellapneumoniae, P. aeruginosa, S. aureus, Bacteroides fragilis, and Clos-tridium perfringens. There is a growing trend toward early use ofprophylactic antibiotics in cases of pancreatic necrosis, eventhough there are no data that convincingly demonstrate a clini-cal benefit.This trend may be partly responsible for the increas-ing prevalence of Candida species in pancreatitis-related sepsis; a1996 report stated that Candida infection was detected in 21%of patients.127
Nutrition. Nutritional support of patients with pancreatic abs-cesses usually consists of TPN, though small bowel feeding maybe attempted occasionally.These patients have high metabolic de-mands and may experience glucose intolerance or hyperlipi-demia. Nevertheless, they generally tolerate I.V. feeding well. A10-fold increase in mortality (from 2.5% to 21%) was reportedin patients in whom a positive nitrogen balance could not beachieved.128
Splenic Abscess
Diagnosis A splenic abscess should be considered in patientswho present with fever and a left upper quadrant mass, though itremains a rare cause of these symptoms. Most splenic abscessesencountered in clinical practice are solitary; multiple abscesses areusually covert and are typically found at autopsy in patients withdisseminated malignancy, collagen vascular disease, or chronicdebility.
Because splenic abscess is rare, correct diagnosis requires a highindex of suspicion.The main clue is the clinical setting: both bactere-mia and local splenic disease are required to produce splenic abscess.In the preantibiotic period, this combination was seen most frequent-ly in patients with bacterial endocarditis and typhoid. Even today,more than three quarters of splenic abscesses occur in patients whoalready have an infection elsewhere in the body; splenic abscessescan also occur in patients with splenic infarcts, splenic hematomas,or local splenic disease caused by hemoglobinopathies.

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 13
The diagnosis of splenic abscess may be supported by indirectradiologic signs, such as an elevated left hemidiaphragm or thefinding of a left upper quadrant air-fluid level (mimicking the stom-ach). To clinch the diagnosis, an abdominal ultrasound examina-
tion or abdominal CT scan is required.The abdominal CT scan,enhanced with I.V. or oral contrast material, is preferred [see Figure8].129 This technique provides a direct image of the spleen, onwhich abscesses appear as low-density areas that may contain gas.
Abscess
Fluid
Fluid Pancreas
Fluid
PancreasPancreas
Pancreas Pancreasa b
c d
e f
Figure 7 Pancreatic findings on CT scan have been graded by Ranson into five categories: grade A—normal pancreas(a); grade B—diffuse enlargement of pancreas and nonhomogeneous density of gland (b); grade C—diffuse enlargementof pancreas associated with peripancreatic inflammation (c); grade D—high-density fluid collection in left anteriorpararenal space (only head of pancreas is visualized at this level) (d); and grade E—diffuse enlargement of pancreaswith several intrapancreatic small fluid collections and poorly defined fluid collections adjacent to tail and head of pan-creas (e). In final CT scan (f), pancreatic abscess is demonstrated; partially encapsulated fluid collection containingbubbles of air represents large abscess.

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 14
Treatment Treatment of splenic abscess includes I.V. admin-istration of antibiotics and splenectomy [see 5:25Splenectomy].The usual pathogenic organisms found are staphylo-cocci and streptococci, though gram-negative bacilli and anaer-obes may also be present.When splenic abscesses are not drained,mortality approaches 100%.At one time, splenotomy was the pre-ferred operative treatment, but splenectomy is currently the pre-ferred approach. Percutaneous catheter drainage is being per-formed with increasing frequency and appears to be as effective asoperative drainage.8,130.131
Infections of the Lower Abdomen
Although enteric perforations, like pancreatitis and cholecystitis,present most commonly with pain and fever, their diagnosis differsfrom that of upper abdominal infections of the solid organs.The painassociated with enteric perforation frequently is not well localized;consequently, CT scanning is used more frequently than ultra-sonography because it is superior for evaluating the entire abdomen[see Figure 9].Moreover, a perforated viscus may present more acute-ly than other forms of infection do, and it is a common indicationfor emergency exploration.Thus, in the setting of a possible lower
Mass
Figure 8 Abdominal CT scan, enhanced by contrast material, confirms diagnosis of splenic abscess.
Evidence of duodenal perforation is seen, with orwithout free peritoneal air
Patient does not have "certain" appendicitis, signs of upper abdominal infection are not present, and abdominalplain films are not indicated
Order abdominal and pelvic CT scans.
Treat operatively; if upper GI study shows perforation issealed, consider nonoperativetreatment.
No discrete fluid collection is present (pancreatitis, diverticulitis)
Provide nonoperative management,including resuscitation and antibiotic therapy (antibiotics areunnecessary for bland pancreatitiswithout necrosis).
Discrete fluid collection is present (periappendiceal or diverticular abscess)
Resuscitate and give antibiotics.Treatment options:• percutaneous drainage with delayed resection• immediate open resection and drainage• diversion and drainage only
Diffuse infection isobserved; infection is uncontrolled, andsource is unclear
Scans are normal
Consider nonsurgical diagnoses.Consider esophago-gastroduodenoscopy.
Localized infectionis seen
Resuscitate, giveantibiotics, and take to OR.
Free peritoneal air isseen without evidenceof controlled leak (duodenal ulcer,periappendiceal ordiverticular abscess)
Resuscitate, giveantibiotics, and take to OR.
Figure 9 Algorithm outlines approach to patient withsuspected lower abdominal infection.

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 15
abdominal infection, the diagnostic emphasis is on confirming orruling out the presence of an acute condition necessitating opera-tion, rather than on fine localization of a more chronic illness.
PEPTIC ULCER PERFORATION
The incidence of peptic ulcer perforation has decreased signifi-cantly as a consequence of the changes in disease progression andincidence of intractable ulcers brought about by the advent of H2
receptor antagonists and proton pump inhibitors (PPIs). Still, asignificant percentage of all hospital admissions are secondary toperforated peptic ulcers, and the patient population is becomingolder and more evenly balanced between men and women, pre-sumably because of increased use of nonsteroidal anti-inflamma-tory drugs and cigarettes.132
Several studies found a high (80% to 92%) incidence ofHelicobacter pylori infection in patients with perforated pepticulcers.133,134 Although the prevalence of H. pylori infection in thispopulation is well established, the causal role that such infectionplays in peptic ulcer perforations has been questioned.135 In a 1999study involving 50 patients with juxtapyloric perforations related tocrack cocaine use who were successfully managed with simpleomental patch closure, the investigators found that approximately80% of the patients who underwent antral mucosal biopsy at thetime of closure had a positive urease test, a finding that suggested
a role for H. pylori infection in the pathogenesis of these perfora-tions as well.136
Diagnosis
A patient with a perforated peptic ulcer will complain of thesudden onset of intense abdominal pain and will often be able topinpoint the exact time when the symptoms began. If the perfora-tion has not spontaneously sealed or been managed with operativeclosure, the clinical picture can progress to florid sepsis and shock.Evidence of free air on plain upright and left lateral decubitus radi-ographs will be seen in as many as 70% of cases [see Figure 10a].137
Endoscopy should be avoided in the evaluation of peptic ulcer per-foration, but equivocal cases or spontaneously sealed perforationscan be evaluated with water-soluble contrast studies. CT scanningcan be used to localize an infection to the duodenum, particular-ly if communication of air or fluid with the duodenum is estab-lished [see Figure 10b] or if extravasation of contrast is seen [seeFigure 10c].
Treatment
Surgical management centers on control of the site of perfora-tion (via surgical closure or spontaneous sealing), with or withoutan acid-reducing procedure [see 5:20 Gastric Duodenal Disease]. Be-fore this is done, I.V. fluids should be given, metabolic derange-
Figure 10 (a) Upright chest x-ray of patient withsudden onset of diffuse abdominal pain demonstratesfree peritoneal air underneath both diaphragms(black arrows). Emergency exploration was carriedout without further studies, and perforated gastriculcer was excised. (b) Abdominal CT scan of patientwith history of ulcer disease and 1-week history ofincreasing abdominal pain shows retrogastric fluidcollection with air that appears to be in communica-tion with duodenum (white arrow). Patient under-went laparotomy, and perforated duodenal ulcer wasrepaired. (c) Abdominal CT scan of patient with 2- to3-day history of worsening abdominal pain demon-strates extravasation of oral contrast from anterolat-eral aspect of duodenum (white arrow). Patientunderwent laparoscopic omental patch closure.
a b
c

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 16
ments corrected,appropriate antibiotics and an H2 receptor blocker orPPI administered, and a nasogastric tube placed for decompression.
Operative versus conservative management Severalstudies have shown nonoperative management to be safe andeffective for perforations that have sealed spontaneously. A 1989study evaluated 35 patients with acute duodenal perforations—excluding those with a history of chronic ulcer disease who ulti-mately went on to primary repair and acid-reducing surgery—whowere managed nonoperatively after evidence of a sealed perfora-tion was noted on a water-soluble upper GI study.The investiga-tors reported one death, in a patient with a history of metastaticbreast cancer, and one intra-abdominal abscess.138 In a 1989prospective trial of 83 patients with perforated peptic ulcers ran-domly assigned to either conservative or operative management,the two groups experienced similar morbidity and mortality(~5%), and 73% of the patients in the conservatively managedgroup experienced full resolution of their symptoms.139 The onlysignificant difference between the groups was in the length of hos-pital stay. It has been suggested that patients with evidence of asealed perforation confirmed by a Gastrografin upper GI studycan be managed conservatively with a low incidence of reperfora-tion and intra-abdominal abscess formation.140 These patientsmust undergo repeated clinical examination and receive support-ive therapy until clinical symptoms resolve.
Laparoscopic versus open repair A prospective, random-ized trial of perforated peptic ulcers to either open or laparoscopicsuture omental patch repair concluded that for perforations small-er than 10 mm, laparoscopic repair was associated with reducedoperating times, less need for analgesics, fewer postoperative chestinfections, earlier return to normal activities, and shorter hospital-izations.141 An earlier study also demonstrated reduced analgesictimes and earlier return to normal activities but reported longeroperating times.142 These studies confirm that small perforationscan be adequately managed laparoscopically without exacerbationof bacterial sepsis. It must be emphasized, however, that biopsy ofperforated gastric ulcers is critical for ruling out malignancies, andlaparoscopic repair of the perforation may preclude biopsy.
Simple repair with medical management versus repairwith acid-reducing procedure Definitive surgical manage-ment of ulcer disease during repair of a perforated peptic ulcer is contraindicated in patients who are hemodynamically unstable,have diffuse peritonitis, have an abscess, or have multiple under-lying comorbid conditions.143 The significant side effects associ-ated with definitive surgery (dumping and diarrhea) and the suc-cess of medical management (PPIs, H2 receptor blockers, and H. pylori eradication) have further contributed to the reducedpopularity of proximal vagotomy at the time of repair. Now thatfewer acid-reducing operations are being performed, there issome justifiable concern that younger surgeons will not be able toobtain the degree of training they would need to perform a defin-itive operation (highly selective vagotomy) in an urgent or emer-gency scenario.
A 1987 study found that simple closure with a Graham patch,without a concurrent operation to reduce ulcer recurrence, result-ed in a higher recurrence rate than closure with proximal gastricvagotomy did (52% versus 16%; median follow-up, 54 months).144
In a subsequent study of patients with acute perforations whowere randomly assigned to undergo either simple closure or sim-ple closure with proximal vagotomy, ulcer recurrence rates in thetwo groups after 2 years were 36.6% and 10.6%, respectively.145
Both of these studies, however, were performed before PPIsbecame routinely available.
Some 40% of patients with duodenal perforation treated withsimple closure may experience recurrent duodenal ulcer. A 1995series associated such recurrence with H.pylori infection.146To fur-ther study the role of H.pylori eradication in ulcer recurrence afterpeptic ulcer perforation, a randomized study was done in whichpatients with perforated duodenal ulcers and H. pylori infectionafter simple closure received either quadruple anti–H. pylori ther-apy (1 week of bismuth, tetracycline, and metronidazole with 4weeks of omeprazole) or omeprazole alone.133 After 1 year, 38.1%of patients managed with PPIs alone experienced ulcer recur-rence, compared with 4.8% of patients managed with PPIs and H.pylori eradication. A similar study followed patients with perforat-ed duodenal ulcers for up to 2 years after simple closure and ran-domization to either short-term H2 receptor blockers or H2 block-ers with quadruple therapy; ongoing H. pylori infection correlatedwith recurrent ulcers for up to 2 years.147
On the basis of these findings, definitive acid-reducing proce-dures should be reserved for (1) patients in whom medical man-agement of peptic ulcers and H. pylori fails, (2) patients whoseulcer symptoms have persisted for longer than 3 months, and (3)patients with otherwise complicated ulcers (e.g., lesions that arebleeding or causing obstruction).148
Antibiotic therapy In fasting persons, gastric juice containsas many as 103 organisms/ml.These organisms are typically facul-tative gram-positive salivary bacteria (e.g., lactobacilli and strepto-cocci) and fungi (e.g., Candida species). In induced states ofachlorhydria (e.g., from treatment with H2 receptor blockers orPPIs), there is an increase in the total number of organisms,including enterococci and nitrate-reducing organisms. This phe-nomenon suggests a proliferation of salivary and enteric organ-isms, but its clinical relevance is unknown.149
Eradication of H. pylori in patients with uncomplicated ulcersand bleeding ulcers is now the standard of care.150,151 Infection withthis organism is associated with a 1% per year risk of peptic ulcerdisease, a level of risk approximately 10 times that seen in unin-fected patients. Eradication of H. pylori with medical managementtypically results in resolution of the ulcer, and recurrence is rare.Consequently, acid-reducing procedures are not often required.152
SMALL INTESTINAL PERFORATION
Diagnosis
Small intestinal perforation is a very difficult entity to diagnose,in large part because of its relative rarity.There are certain clinicalscenarios (e.g., strangulated hernia and Crohn disease) in whichthe likelihood of this condition is heightened, but in the setting ofblunt small intestinal injury, the low incidental occurrence of per-foration (~1%153) and the complexity of the presentation fre-quently lead to a delay in diagnosis. Such delay is associated withincreases in the morbidity and mortality directly attributable to theinjury.154 The radiographic modality most useful in diagnosis isCT scanning.155
Treatment
The basics of treatment are the same for small bowel perfora-tion as for all perforations: isolation and control of the source ofcontamination. In the acute setting, this is accomplished throughlaparotomy and excision of the disease segment, whether the per-foration is the result of ischemic necrosis, of blunt injury, or ofIBD. Primary reanastomosis is generally accepted in these patients

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 17
[see 5:29 Intestinal Anastomosis]. For patients with Crohn disease,perforation (usually presenting as a fistula) is a risk factor for post-operative disease recurrence156; accordingly, close postoperativefollow-up is indicated.
There are two additional issues regarding small bowel perfora-tions that warrant special mention.The first has to do with smallbowel perforation secondary to obstruction. When this eventoccurs, it is important not only that the perforated segment beresected but also that the cause of obstruction be identified to pre-vent recurrence. The second issue has to do with anastomoticleakage. Not all leaks call for surgical intervention. If the leak is alate complication, it is likely to have walled itself off into anabscess, in which case CT-guided drainage of the abscess is thetreatment of choice. Efforts at reducing the luminal transport arealso made to improve healing.
Nutritional support plays a major supportive role in the treat-ment of patients with small bowel perforation. Many of thesepatients, either because of their underlying pathology (e.g., Crohndisease) or because of their hypermetabolic state (e.g., from trau-ma), lose some of their innate ability to heal and prevent anasto-motic breakdown.The presence of a knowledgeable nutrition staffcan dramatically enhance patient recovery in this setting.
Antibiotic therapy The small bowel flora is typically sparse(103 to 104/ml), with salivary organisms predominating. In condi-tions of stasis, obstruction, or impaired motility, however, colonicflora can proliferate, with E. coli, enterococci, and obligate anaer-obes the dominant organisms. In the distal ileum, there are typi-cally about 106 colony-forming units/ml, with an increasing pro-portion of enteric organisms and anaerobic bacteria, presumablyas a result of backwash through the ileocecal valve.157 Althoughthere are generally far fewer bacteria in the small intestine than inthe colon (which contains about 1012 organisms/ml), the standardantimicrobial therapy remains broad-spectrum coverage (e.g., flu-oroquinolone plus an antianaerobic agent for 5 days).158
APPENDICITIS
Obstruction of the appendiceal lumen by a fecalith, a hyper-plastic lymph node, or a foreign body is typically the inciting eventin the pathogenesis of appendicitis. Luminal obstruction with con-tinued secretion results in progressive distention, proliferation ofluminal microorganisms, ischemia, gangrene, and subsequent per-foration. The clinical history during this evolution is marked bydiffuse epigastric pain with anorexia, nausea, and vomiting. Thepain typically progresses first to the periumbilical region and thento the right lower quadrant (at McBurney’s point). Patients have alow-grade fever and exhibit direct tenderness at McBurney’s pointbut may also manifest rebound tenderness, guarding, rigidity, andmarked temperature elevation if the appendix perforates andresults in diffuse peritonitis.As the viscera and the omentum local-ize and sequester the perforation, the symptoms may subside to adegree, with localized pain and a palpable abdominal mass the pri-mary manifestations remaining.
Diagnosis
Classically, the diagnosis of appendicitis has been made pri-marily through clinical examination, with laboratory tests consis-tent with inflammation (i.e., an elevated leukocyte count with aleft shift and an elevated C-reactive protein level) serving as con-firmation. In as many as 20% of patients with appendicitis, how-ever, the incorrect diagnosis is made, and the incidence of removalof a normal appendix can approach 40%.159-161 Early diagnosis ofappendicitis can decrease the risk of postoperative complications
from 39% to 8%, and one retrospective study found that the useof diagnostic CT lowered the rate of misdiagnosis to 7%.162 CTscanning is reported to be 93% to 98% in diagnosing appendici-tis, with significantly improved accuracy achieved by using anappendicitis protocol after retrograde water-soluble contrastadministration.163 CT findings suggestive of appendicitis [seeFigure 11] include enlargement and dilation of the appendix (to > 6 mm), nonfilling of the appendix, and periappendiceal inflam-mation (fat stranding, abscess, phlegmon, and dependent fluidcollections); these findings do not differ significantly betweenacute appendicitis and chronic, recurrent appendicitis.164,165
Current evidence supports the role of CT scanning in the diag-nostic evaluation of patients with suspected appendicitis. Studieshave demonstrated decreases both in the incidence of normalappendectomies and in the incidence of prolonged, unnecessaryobservations.166,167 Furthermore, alterations in patient manage-ment attributable to diagnostic CT have been shown to decreaseoverall hospital and patient costs. Nevertheless, the utility of CT inyoung men whose history, physical examination, and laboratorytest results fit the classic picture of appendicitis remains unproven;this subset of patients may be managed without confirmatoryCT.166 On the other hand, CT scanning appears to be quite usefulfor diagnosing appendicitis in women, in which setting it decreasesthe incidence of normal appendectomies and facilitates diagnosisof other causes of the symptoms.168,169 Preoperative CT scanningassists in planning an operation, identifying a periappendicealabscess that may delay immediate appendectomy, and recognizingother sources of intra-abdominal pathology.
Treatment
Initial management consists of fluid resuscitation, appropriateprophylactic antibiotics, and preparation for surgery. Currently,acute nonperforated appendicitis, gangrenous appendicitis, andperforated appendicitis without an associated abscess are man-aged with urgent appendectomy [see 5:26 Appendectomy]. Themain dilemmas in management center on the appropriate use of
Figure 11 Pelvic CT scan of patient with distant history of rightlower quadrant abdominal pain with recurrent acute attackdemonstrates inflamed and thickened appendix with surroundingfat stranding (white arrow). Gangrenous appendix was removedlaparoscopically.

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 18
laparoscopic appendectomy and the role of conservative manage-ment for periappendiceal masses with interval appendectomy.
Laparoscopic versus open appendectomy In severalprospective, randomized clinical trials that compared laparoscop-ic with open appendectomy, the consensus was that the formerwas associated with a lower incidence of wound infection,decreased utilization of pain medication, earlier return to normalactivities, and reduced cost of hospitalization (though the datawere conflicting on this last point).170-173 On the other hand, thetrials found the laparoscopic approach to be associated with sig-nificantly longer operating time, equivalent duration of hospital-ization, and a possible increased risk of abscess formation. A ret-rospective review published in 2000, however, found that when adedicated laparoscopic service was established for patients withappendicitis, the rates of intra-abdominal abscess formation afterlaparoscopic appendectomy decreased to levels equivalent to thosereported after open appendectomy.174
Although laparoscopic appendectomy is associated with a high-er incidence of intra-abdominal abscess formation in the setting ofperforated appendicitis, it is not associated with a higher incidenceof wound infection or abscess in patients with gangrenous or non-perforated appendicitis.175 Furthermore, a prospective, random-ized trial found that laparoscopic appendectomy was associatedwith reduced overall cost of hospitalization, decreased use of painmedication, and earlier return to functional status in patients withuncomplicated appendicitis.170
Two groups of patients clearly benefit from laparoscopic appen-dectomy: women and obese patients. In women, laparoscopy aidsin the diagnosis of other pelvic pathologic conditions and lowersthe incidence of negative appendectomies; in obese patients, itresults in less postoperative pain and a shorter recovery time, eventhough it does not significantly reduce the postoperative compli-cation rate.176,177 Patients who present with evidence of perforatedor complicated appendicitis may be better managed with the tra-ditional open approach to minimize the risk of postoperativeabscess formation.178 Improvements in laparoscopic techniques,however, may eventually reduce the incidence of this complicationto a level comparable to that seen with open management.
Periappendiceal abscess and interval appendectomyThe mainstays of conservative management have been parenteralantibiotics, supportive fluid resuscitation, and percutaneousdrainage of radiographically amenable fluid collections. In a 2001review of 155 patients with periappendiceal abscesses, the compli-cation rate was 36% for patients managed with surgical incisionand drainage and appendectomy, compared with 17% for patientsmanaged nonoperatively.179 The recurrence rate was 8% in theconservatively managed patients, and nonoperative managementfailed in five patients. Patients with perforated appendicitis andabscess or phlegmon diagnosed by CT scanning but without apalpable mass were safely managed with conservative therapy. Ina 2002 study, immediate appendectomy was associated with ahigher postoperative complication rate and an increased incidenceof more extensive initial operations (e.g., ileocecal resection, righthemicolectomy, and temporary ileostomy).180
The recurrence rate after conservative management rangesfrom 10% to 20%. In one study of patients managed with intervalappendectomy for periappendiceal mass, histologic evaluationrevealed that a significant majority of samples had a patent appen-diceal lumen and were at risk for recurrent appendicitis.181 In a2002 report, 45.8% of interval appendectomy pathologic samplesshowed evidence of chronic active inflammation.182 The risk of re-
currence and progression to chronic appendicitis supports the useof interval appendectomy in young patients, but in adults, the de-cision algorithm must also consider the incidental diagnosis of tumor.
Interval appendectomy is typically performed between 6 weeksand 3 months after percutaneous intervention and clinical resolu-tion [see Figure 12]. The risk of recurrence is greatest after the 6-month point in the clinical progression of acute appendicitis man-aged conservatively.183 In several retrospective analyses, intervalappendectomy proved to be a safe management plan, but to date,there have been no randomized, prospective trials evaluating itsrole in management.184,185
Antibiotic therapy The pathogenic organisms recovered inperitoneal cultures derive from the colon and consist of aerobic orfacultative bacteria and anaerobes. The most frequently isolatedorganisms are E. coli, enterococci, viridans streptococci, B. fragilis,Lactobacillus species, Prevotella melaninogenica, and Bilophilawadsworthia.186,187 It is noteworthy that the use of intraoperativeperitoneal cultures has not been shown to affect the incidence ofwound infection, abscess formation, or small bowel obstruction ifpatients are presumptively managed with antibiotics that covergram-negative bacteria and enteric anaerobes.188
Appropriate coverage can be obtained with any of the following:ampicillin-sulbactam, piperacillin-tazobactam, ticarcillin-clavu-lanate, cefoxitin, cefotetan, and ciprofloxacin plus metronida-zole.189-192 In a trial involving children with perforated appendici-tis, conversion to oral therapy after parenteral therapy was equiv-alent to parenteral therapy alone.193 In a study of patients withacute nonperforated appendicitis, preoperative administration ofcefoxitin was superior to placebo in reducing the incidence ofwound infection.190 In a study of children with acute nonperforat-ed appendicitis, prolonged antibiotic administration (5 days) hadno advantage over a single preoperative dose with respect to theincidence of wound infection or subsequent abscess formation.194
The duration and timing of antibiotic administration in patientswith nonperforated gangrenous appendicitis have not been shownto correlate with the wound infection rate.195
COLONIC PERFORATION
Diagnosis
Diagnostic strategies for identifying colon lesions associatedwith intra-abdominal infection follow the general approach out-lined earlier [see Clinical Evaluation and Investigative Studies,above]. For unstable patients with generalized peritonitis, there isno need to delay operative intervention to wait for radiologic con-firmation: the pathologic condition will be identified in the courseof the operation. However, for patients who have localized peri-tonitis or those who are stable and whose physical examination isnot conclusive for peritonitis, radiologic evaluation is pivotal inplanning treatment.
Although plain films may reveal free air in the abdomen andprompt surgical intervention, CT scanning may be a more valu-able first study because of its ability to delineate the bowel wall andsurrounding soft tissues with remarkable accuracy. In a 2002study comparing abdominal radiography with CT for the evalua-tion of acute nontraumatic abdominal pain in the ED, the formerwas not nearly as diagnostically sensitive as the latter (a nonspe-cific diagnosis in 68%, compared with a specific diagnosis in80%).196 The investigators concluded that CT was the initial radi-ographic modality of choice for patients with acute abdominalpain in the ED. Another study found that CT scans frequentlychanged physicians’ initial diagnoses, increased diagnostic certain-

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 19
ty, and led to more appropriate treatment in patients with acuteabdominal pain in the ED.197
In view of the relatively high cost of CT scanning, the con-comitant radiation exposure, and the use of I.V. contrast agents toenhance the scans, some have suggested using ultrasonography tomake diagnoses. However, the well-documented dependency ofthis modality on the skill of the individual technician makes it lessattractive to the broader health care community, where full-timesonographers are not always available. Finally, it should be notedthat there is no role for MRI in the acute setting. Although it isboth sensitive and specific, the logistic hindrances associated withits use greatly limit its applicability.
Treatment
Diverticulitis Diverticular disease ranges in severity fromminor to serious.The focus of our discussion will be on manage-ment of complicated (perforated) diverticular disease, for whichresection should be considered after only one attack.
In the past, treatment of perforated diverticular disease involved amultistage surgical approach whereby the patient underwent threeseparate procedures: one for fecal diversion and drainage of theinfection, a second for resection of the diseased segment, and a thirdfor closure of the colostomy.This three-stage approach proved to beassociated with high morbidities, high cumulative mortalities, andprolonged hospitalizations.198-200 Since then, CT-guided percuta-neous drainage, primary resection of the diseased segment, andimproved patient selection for resection and primary anastomosishave improved patient outcomes dramatically. Few adequately pow-ered multicenter, prospective, randomized trials evaluating treat-ment of complicated diverticular disease have been done; accord-ingly, many of the current treatment standards have been derived byconsensus on the basis of thorough review of the literature.
Therapy for perforated diverticular disease depends greatly onthe patient’s condition at the time of presentation and on the stageof the disease.The Hinchey staging system201 [see Table 4] classifiesperforated diverticular disease according to the associated inflam-matory process and is used to guide and compare treatmentoptions.202-204
In stage I disease, a small pericolic abscess [see Figure 13a] in astable and otherwise healthy patient may resolve with conservative
management, including broad-spectrum antibiotics and bowelrest.The patient can be evaluated for definitive surgical treatmentlater, after the episode resolves and the patient is in better condi-tion for surgery. For larger abscesses or stage II disease [see Figure13b], the standard of care is CT-guided percutaneous abscessdrainage, if feasible. After drainage, resuscitation, and bowel prep-aration, a one-stage colectomy can be done (resection of the dis-eased segment with primary anastomosis) so as to avoid the poten-tial increased morbidity of a two-stage procedure.205
For patients who have abscesses that are inaccessible to percu-taneous drainage or who experience persistent symptoms despitedrainage, operative correction is required. If adequate bowel pre-paration can be carried out, primary anastomosis at the time ofsurgery should be considered. If adequate bowel preparation is notpossible, a two-stage approach, including a Hartmann procedureand subsequent stoma reversal, should be considered. Alterna-tively, depending on the patient’s condition, resection with prima-ry anastomosis may be attempted. There is some evidence thatemploying intraoperative colonic lavage to reduce the fecal col-umn and thus allow primary anastomosis may reduce morbidity,especially in patients with stage I or II disease.206-208 However, thestudies supporting this view are not conclusive enough for such aregimen to be considered standard; further investigation is war-ranted before it is generally accepted. Finally, whether to add acovering stoma to a primary anastomosis is a case-by-case decisionthat is usually guided by the presence of risk factors such as poornutritional status, inadequate bowel preparation, blood loss, orintraoperative hypotension.209
a b
Figure 12 (a) Pelvic CT scan of young patient with a 5-day history of right lower quadrant abdominalpain shows fluid collection containing air adjacent to appendix and consistent with appendiceal perfora-tion and abscess formation (white arrow). (b) Pelvic CT scan of same patient after percutaneous ultra-sound-guided placement of drainage catheter shows evacuation of air and much fluid. Patient underwentuneventful interval appendectomy 6 weeks later.
Table 4—Hinchey System for Classification of Perforated Diverticulitis201
Stage
Stage IStage IIStage IIIStage IV
Description
Pericolic or mesenteric abscessPelvic or retroperitoneal abscess that is walled offPurulent peritonitisFeculent peritonitis

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 20
Stage III or IV diverticulitis is a surgical emergency that calls forprompt resuscitation and administration of broad-spectrum anti-biotics, followed rapidly by surgical treatment. The Hartmannprocedure is the most widely accepted operation for this presenta-tion.210-212 It is associated with a substantially lower mortality thandrainage followed by colostomy as a separate, delayed procedure(12% versus 28%).213 In certain circumstances, with appropriatepatient selection and low feculent contamination, primary anasto-mosis, with or without a covering stoma, may be feasible.214-216
The goals of resection are to remove the focus of infection andto prevent recurrent attacks. Recurrent diverticulitis after resectionis the result of incomplete removal of the diseased segment, espe-cially at the rectosigmoid junction. Therefore, when the diseasedsegment is resected, the entire sigmoid must be removed, and thedistal resection margin must extend below the confluence of thetaeniae coli and onto pliable rectum.217 Proximally, the colon ismobilized until a margin of uninflamed bowel is identified. It is not,however, necessary to remove the entire colon affected by diverticuli.
Laparoscopy. Laparoscopic treatment of diverticular disease isbecoming more common but remains controversial. Many feelthat there is no place for laparoscopic-assisted colectomy in thetreatment of stage III or IV disease,202 but there is growing accep-tance of this approach in the treatment of stage I and II disease. Areview of several small studies concluded that laparoscopic colec-tomy had a high potential for reducing hospitalization time andoperative morbidity; however, the cost analysis data were conflict-ing, and some of the trials reported very high conversion rates.218
Right-side disease. Particular mention should be made of right-side diverticulitis. In the past, this condition was often misdiag-nosed as appendicitis before exploration, but today, with theincreased use of CT scanning, this error is less frequently made.Given that diagnosis is difficult and the disease is surgically curable,some authors suggest that it should be treated with aggressiveresection, ranging from simple diverticulectomy to right hemi-colectomy.219,220 Others argue that the disease is relatively benign inthe absence of perforation and suggest leaving the diseased bowelin situ, performing an incidental appendectomy, and then treatingthe patient conservatively.221,222 There is no standard therapy forcecal diverticulitis, mainly because of the small number of patients
it affects annually, which translates into small series reported in theliterature. In the course of follow-up, it is important that thesepatients undergo thorough evaluation for colon cancer.
Antibiotic therapy. Appropriate antibiotic administration is anintegral part of standard therapy for diverticular disease and isstarted at diagnosis. The most frequently isolated organisms areanaerobes, including Bacteroides,Peptostreptococcus,Clostridium,andFusobacterium species. Gram-negative aerobes (predominantly E.coli) and facultative gram-positive bacteria (predominantly strep-tococci) are also associated with these infections.223 Parenterallyadministered broad-spectrum antibiotics are standard. A particu-larly common regimen is ciprofloxacin plus metronidazole, butthere are other regimens that are equally efficacious for treatment.According to a 2002 report from the Surgical Infection Society,the duration of therapy for complicated intra-abdominal infec-tions should be no longer than 5 to 7 days.158 If ongoing infectionis suspected at termination of treatment, investigation into apotential source of infection is warranted.
Other colon lesions associated with perforation and peri-tonitis A number of colonic conditions besides diverticular dis-ease may be manifested by colonic perforation and secondaryperitonitis.Whatever the specific cause, the general goals of thera-py remain the same: (1) to identify and control the source of bac-terial contamination, (2) to reduce the level of peritoneal contam-ination, and (3) to prevent recurrent infections.
Colon cancer. After diverticular disease, colon cancer is the nextleading cause of colonic perforation in uninjured patients. In gen-eral, perforated colon cancer carries a high mortality,224,225 and theoperative technique of choice is controversial. Perforation typical-ly occurs at the site of the lesion but can also occur proximally(e.g., at the cecum) as a result of luminal obstruction.
Generally, perforations at the site of cancer in the ascending andtransverse colon are treated with primary resection and anasto-mosis, with or without a diverting stoma, regardless of whetherlocalized or diffuse peritonitis is present.When perforations occurat the site of cancer in the descending and sigmoid colon, howev-er, there is some debate over the appropriate surgical approach,with some advocating primary resection and others staged proce-
a b
Figure 13 (a) Pelvic CT scan of elderly patient with left lower quadrant abdominal pain of 2 days’ duration showsdiverticulitis with small amount of extraluminal air (white arrow). Patient was treated acutely with resuscitation andantibiotics alone and was discharged home without complications. (b) Pelvic CT scan of middle-aged patient with 1-week history of constipation and moderate pelvic pain shows left lower quadrant fluid collection consistent withperidiverticular abscess (white arrow). Proximal bowel is seen anterior to abscess, distal bowel posterior. Percutan-eous drain was placed, and elective colectomy with primary reanastomosis was performed 12 days later.

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 21
dures.Two studies from the early 1990s suggested improved long-term mortality after primary resection.226,227 A subsequent study,however, suggested that the improved mortality associated withprimary resection was secondary to preselection and thereforecould not be considered conclusive proof of the superiority of thisapproach.The authors of this latter study concluded that primaryresection was appropriate for a select patient population with min-imal comorbidity and that staged resection was beneficial forpatients with a high degree of acute illness and comorbidity (e.g.,elderly patients).228
Less common causes of colonic perforation. Other diagnoses associ-ated with colonic perforation and peritonitis (localized or diffuse)are ischemic necrosis as a result of vasculopathology [see Figure14a] or volvulus, missed traumatic injury, and IBD [see Figure 14b].Except for IBD, the standard therapy is excision of the affected seg-ment and reanastomosis, with or without a covering stoma. Forpatients with numerous comorbidities, a high degree of feculentcontamination, or very severe illness necessitating an extremelyabbreviated operating time, a Hartmann procedure with a mucousfistula or an oversewn distal segment is the primary treatment.Because perforation associated with IBD is typically a self-limiteddisease, treatment is directed at the underlying pathophysiologyand excision of the diseased segment is not always indicated.229
Other Abdominal Infections
PELVIC INFLAMMATORY DISEASE
Because of the diverse clinical presentations of pelvic inflam-matory disease (PID) and the significant sequelae associated withdelayed diagnosis, women with this condition can pose a majordiagnostic dilemma in the ED. In 2002, the Centers for DiseaseControl and Prevention (CDC) updated their established diag-nostic guidelines for initiating therapy in patients with suspectedPID.230 According to these guidelines, empirical treatment shouldbe started if a young sexually active woman or any woman at riskfor sexually transmitted diseases presents with minimal symptoms
[see Table 5] that cannot be attributed to another cause.To reduceundue treatment-associated morbidity, additional criteria are sup-plied to aid in specifying precisely who should receive treatment.
Treatment of PID, according to the CDC, includes broad-spec-trum antibiotics directed toward Neisseria gonorrhoeae, Chlamydiatrachomatis, anaerobes, gram-negative facultative bacteria, andstreptococci [see Table 6]. Hospitalization is suggested when surgi-cal emergencies (e.g., appendicitis) cannot be excluded or whenthe patient is pregnant; does not respond clinically to oral antimi-crobial therapy; cannot follow or tolerate an outpatient oral regi-men; has severe illness, nausea and vomiting, or high fever; or hasa tubo-ovarian abscess. Surgical intervention for PID is generallylimited to patients with symptomatic pelvic masses, ruptured
a b
Figure 14 (a) Abdominal CT scan of elderly patient with history of vascular disease and worseningabdominal pain over a 3-day period shows diffuse inflammation and right upper quadrant extraluminalair (white arrow). Patient underwent emergency exploration, and ischemic perforation of cecum wasfound. Right hemicolectomy and temporary diverting ileostomy were performed. (b) Abdominal CTscan of patient with history of Crohn disease and worsening abdominal pain demonstrates thickening ofcolonic wall with both intramural and extramural air (white arrow). Patient was treated with emergencytotal abdominal colectomy for pancolitis with creation of temporary diverting ileostomy.
Table 5—CDC Guidelines for Diagnosis of Pelvic Inflammatory Disease230
Minimal symptomsUterine/adnexal tendernessCervical motion tenderness
Additional supportive criteria (enhance specificity of minimal symptoms)Oral temperature >101° F (> 38.3° C)Abnormal cervical or vaginal mucopurulent dischargePresence of white blood cells on saline microscopy of vaginal
secretionsElevated erythrocyte sedimentation rateElevated C-reactive proteinLaboratory documentation of cervical infection with Neisseria gonorrhoeae
or Chlamydia trachomatis
Most specific criteriaEndometrial biopsy with histopathologic evidence of endometritisTransvaginal sonography or magnetic resonance imaging techniques
showing thickened, fluid-filled tubes with or without free pelvic fluid ortubo-ovarian complex
Laparoscopic abnormalities consistent with PID

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 22
tubo-ovarian abscesses, or draining abscesses that do not respondto antibiotic therapy. Aspiration has also been considered as atreatment modality; it may limit morbidity and preserve fertility.231
PYELONEPHRITIS
Pyelonephritis is a complication of urinary tract infection; conse-quently, it affects women more often than men.The diagnosis is typ-ically made on the basis of systemic symptoms in the setting of aknown, bacteriologically confirmed urinary tract infection. Pyelo-nephritis may be classified as either complicated or uncomplicated,depending on patient factors (e.g., previous transplantation or ananatomic abnormality) and infectious characteristics (e.g., sepsis).
The typical pathogen in uncomplicated disease is E. coli, and
outpatient treatment with trimethoprim-sulfamethoxazole or afluoroquinolone usually suffices.232 Complicated pyelonephritis,however, often is caused by microbes other than E. coli, includingPseudomonas species and enterococci. Hospitalization is required,and treatment usually involves parenteral administration of ceftri-axone and gentamicin233 or piperacillin-tazobactam234; vanco-mycin is indicated if the patient is allergic to penicillin. More ag-gressive therapies, including percutaneous nephrostomy or ab-scess drainage, may be considered on a case-by-case basis.
SPONTANEOUS BACTERIAL PERITONITIS
In adult patients, primary peritonitis usually accompanies cir-rhosis and ascites235; however, the presentation can be highly vari-able.To diagnose spontaneous bacterial peritonitis, paracentesis isperformed and the fluid sent for Gram stain and culture; pHdetermination; measurement of glucose, protein, lactate, and lac-tic dehydrogenase levels; and a cell count with differential. Accord-ing to a consensus statement from the International Ascites Club,diagnostic paracentesis is recommended for every cirrhotic patientwith ascites upon admission to the hospital.236 Empirical therapyis started if the neutrophil count is higher than 250/mm3, the pHis lower than 7.35, and the lactate concentration is greater than 32ng/ml. If the results of other studies suggest peritonitis, radi-ographic evaluation is indicated to rule out potential causes of sec-ondary peritonitis.
Treatment consists of cefotaxime at a minimum dosage of 2 gevery 12 hours for 5 days, with follow-up paracentesis scheduledfor 48 hours after the start of treatment.237,238 If the neutrophilcount does not decrease significantly (to < 25% of the pretreat-ment value), treatment may be assumed to have failed. Surgicalintervention is undertaken if the patient is refractory to medicalmanagement, the ascitic fluid grows mixed aerobes and anaer-obes, or radiographic studies suggest bowel perforation.
PERITONEAL DIALYSIS CATHETER–RELATED INFECTIONS
Peritonitis is a major cause of failure of peritoneal dialysis inlong-term studies.239 Peritonitis is especially difficult to diagnosein dialysis patients because the presentation is usually vague.Accordingly, it is critical to maintain a low threshold for testing.The definition of peritonitis in this population includes satisfac-tion of two of the following three criteria: (1) a Gram stain demon-strating microorganisms or a positive culture of the dialysis efflu-ent, (2) a dialysate white blood cell count higher than 100/mm3,with at least 50% neutrophils, and (3) peritoneal signs or symp-toms.240 The microbes most commonly identified are S. epider-midis and S. aureus (~ 60% of isolates), followed by gram-negativebacteria (~30% of isolates); the remaining isolates are largelyaccounted for by fungi, anaerobes, and mycobacteria.
Treatment usually includes cefazolin and an aminoglycoside,with or without vancomycin (depending on local S. aureus resis-tance patterns). Antibiotics are administered via the catheter andallowed to dwell intraperitoneally. When treatment is complete,the antibiotic effluent is drained via the catheter. If infection con-tinues despite antibiotic treatment, a recurrent infection with thesame microbe is likely. If fecal contamination occurs, the cathetermust be removed.
Table 6—CDC Guidelines for Antibiotic Treatment of PID230
A
B
Alternative
A
B
Cefotetan, 2 g I.V. q. 12 hror
Cefoxitin, 2 g I.V. q. 6 hr plus
Doxycycline, 100 mg p.o. or I.V. q. 12 hr
Clindamycin, 900 mg I.V. q. 8 hr plus
Gentamicin, loading dose I.V. or I.M. (2 mg/kg body weight)followed by maintenance dose (1.5 mg/kg) q. 8 hr; singledaily dosing may be substituted
Ofloxacin, 400 mg I.V. q. 12 hr or
Levofloxacin, 500 mg I.V. s.i.d. with or without
Metronidazole, 500 mg I.V. q. 8 hr or
Ampicillin-sulbactam, 3 g I.V. q. 6 hr plus
Doxycycline, 100 mg p.o. or I.V. q. 12 hr
Ofloxacin, 400 mg p.o., b.i.d., for 14 days or
Levofloxacin, 500 mg p.o., s.i.d., for 14 days with or without
Metronidazole, 500 mg p.o., b.i.d., for 14 days
Ceftriaxone, 250 mg I.M. in single dose or
Cefoxitin, 2 g I.M. in single dose, and probenecid, 1 g p.o.administered concurrently in a single dose
orOther parenteral third-generation cephalosporin (e.g.,
ceftizoxime or cefotaxime) plus
Doxycycline, 100 mg p.o., b.i.d., for 14 days with or without
Metronidazole, 500 mg p.o., b.i.d., for 14 days
Parenteral Regimens
Enteral Regimens

Controversies and Special Cases
The controversies surrounding the management of intra-abdominal infections are numerous and ongoing, in large partbecause of the relative lack of well-organized, unbiased clinical evi-dence.There are several reasons for this information deficit.
First, although in the aggregate, peritonitis is a common prob-lem seen by general surgeons, any given practitioner sees most ofthe life-threatening forms of the disease (e.g., free perforation fromcolon cancer) infrequently. Second, advances in nonsurgical med-icine and technology (e.g., laparoscopy) have made new forms oftreatment available and have improved outcomes from older tech-niques. As a result, conclusions drawn from older data may nolonger be accurate. Third, many forms of intra-abdominal infec-tion routinely present in such a complex and ill patient population(e.g., elderly patients with multiple comorbidities) that random-ized studies with multiple exclusion criteria can rarely capture ahigh percentage of what is a highly heterogeneous group. Fourth,patients presenting with common causes of intra-abdominal infec-tion that occur in relatively healthy and homogeneous populations(e.g., acute appendicitis and cholecystitis) tend to do well no mat-ter what reasonable therapy is applied. Consequently, it is fre-quently difficult to detect any significant differences between ther-apeutic modalities. For example, despite multiple randomized tri-als, it is still unclear whether a laparoscopic approach has any long-term superiority over an open approach in patients with rightlower quadrant pain and suspected appendicitis: outcomes areexcellent with either method. Finally, for almost any given argu-ment, sufficient supporting data, whether in the form of random-ized trials or—equally valuable—of large observational studiesperformed with statistical rigor, simply do not exist at present.Even simple questions, such as the optimum duration of antibiot-ic treatment for a patient with a single well-drained liver abscess,lack good answers.
In the end, most controversies in this area are not so much amatter of precisely determining the right or the wrong interven-tion for a disease as they are a matter of making a judgmentabout which of many possible interventions is likely to result inthe lowest morbidity and mortality. For example, the decision toperform a primary colon reanastomosis in a patient with a per-forated colon cancer cannot be considered either universally cor-rect or universally incorrect; rather, it is subject to the surgeon’sopinion about the specific patient involved. In what follows, wefocus on several controversial decision points and discuss impor-tant factors that ought to be considered in attempting to opti-mize patient care.
NEW CONCEPTS IN PATHOPHYSIOLOGY OF ACUTE BACTERIAL
CHOLANGITIS
Longmire’s widely accepted classification of acute bacterialcholangitis consists of five categories: acute nonobstructive, acutenonsuppurative, acute suppurative, acute obstructive suppurative,and acute suppurative with intrahepatic abscess. It implies that theseverity of disease parallels the degree of obstruction of biliaryducts.241 This suggestion is well founded. In acute nonobstructivecholangitis associated with acute cholecystitis, infection ascendsalong the intrahepatic and extrahepatic lymphatics. In obstructivecholangitis, the bile duct contains bacteria under pressure.Whenthe pressure is at or above the normal secretion pressure (i.e., 200mm Hg), bacteria pass into the lymphatic system. At a pressure
greater than 250 mm Hg, bacteria may pass directly from the bileductules through the spaces of Mall and Disse and into the hepat-ic sinusoids via cholangiovenous reflux.242 One study confirmedthe clinical significance of increasing ductal pressure by demon-strating a higher ductal pressure and a higher incidence of bac-teremia in patients with proximal ductal obstruction, comparedwith those with distal malignant biliary obstruction.243 However,no correlation exists between the degree of suppuration in theduct and the clinical or pathologic severity of obstructive cholan-gitis.82 Therefore, the terms acute nonsuppurative cholangitis andacute suppurative cholangitis are purely descriptive and do notimply differing degrees of severity.
The source of bacteria in acute cholangitis is most often theduodenum.The ease with which organisms reflux from the duo-denum depends on the degree of obstruction. Thus, in patientswith malignant biliary obstruction, in whom obstruction is usual-ly complete, bile culture is positive in only 10% to 15% ofpatients244; acute cholangitis is seldom spontaneous in this settingbut often follows radiologic intervention.245 By comparison, inpatients with ductal stones or benign strictures, in whom biliaryobstruction is often incomplete, bile cultures obtained on ERCPare positive in 64% to 87% of cases; in these patients, acutecholangitis occurs frequently, both spontaneously and after ductalmanipulation.246
An alternative source of organisms in acute bacterial cholan-gitis is portal venous blood. In patients who have recurrent pyo-genic cholangitis, which occurs frequently in the Far East, a40% incidence of positive portal blood culture has been report-ed.247 In studies of rats with ligated bile ducts, bacteria wereshown to be effectively transmitted to the bile ducts and the liverthrough portal blood.248 Finally, in nonobstructive cholangitisand acute cholecystitis, as well as in the early stages of obstruc-tive cholangitis, infection ascends to the liver through the lym-phatic system.
CHANGING BACTERIOLOGY OF ACUTE BILIARY INFECTION
Most biliary infections are polymicrobial. The organisms mostfrequently cultured are E.coli,Klebsiella species, Enterobacter species,and enterococci. Anaerobic bacteria are infrequently implicated inbiliary infections. Peptostreptococci and clostridia are found occa-sionally; clostridia are especially common in patients with emphy-sematous cholecystitis.47 Gram-negative anaerobic bacilli are rarelypresent in patients with biliary infection. In one study, only two of28 patients with acute cholangitis had anaerobic bacteria in thebile; another investigator found anaerobic bacteria in 3% to 4% ofcultures in similar patients.83 However, a higher incidence of anaer-obic bacteria has been reported in patients who have acute cholan-gitis and acute cholecystitis than in patients who have chroniccholecystitis and cholelithiasis.249
One investigator noted an increased incidence of anaerobic bac-teria in biliary infection and suggested that B. fragilis may play amore important role in the polymicrobial flora of biliary tract infec-tion than was previously appreciated.250These findings remain con-troversial. Bacteroides species are generally considered to be of lim-ited importance in biliary tract infections, except in selected groupsof patients.These groups include diabetics, the elderly,251 and thosewith acute cholangitis who have previously undergone biliary oper-ation252,253; in particular, malfunctioning biliary-intestinal anasto-moses increase the risk of Bacteroides infection.254
© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 23
Discussion

NECESSITY OF DIVERSION AFTER EMERGENCY COLONIC
PROCEDURES
The goal of safely repairing or resecting the colon in an emer-gency setting without leaving a patient with a temporary or per-manent stoma for diversion has been pursued for decades.Through much of the 20th century, largely on the basis ofwartime experience, diversion was routinely performed. Today,however, it is apparent that this approach is not always necessaryeither for trauma or for intrinsic colon disease. Thus, the ques-tion is no longer whether primary repair or reanastomosis can beachieved safely but, rather, in which individual patient a giventreatment is prudent.
Traditionally, clinical studies have attempted to define patientcharacteristics associated with complications after attempted pri-mary repair or reanastomosis. Not surprisingly, hypotension, bloodloss, delay before treatment, and extensive contamination have allbeen associated with postoperative complications after primaryrepair; however, these risk factors are associated with complica-tions after diversion as well.The nature of the colon injury is clear-ly an important consideration: multiple studies now support aone-step approach to traumatic colon injury in all except the mostill patients, but primary resection and reanastomosis for othercauses of perforation (e.g., diverticulosis and cancer) remain con-troversial. Many nonrandomized studies have demonstrated thatfor nontraumatic causes of perforation, on-table lavage and pri-mary resection yield outcomes equivalent to those of theHartmann procedure, which suggests that both approaches aresafe and that surgeons are capable of identifying the patients bestsuited to each one.
Perhaps more important than determining how likely a patientis to experience a complication after a given operation, however, isassessing how well the patient is likely to tolerate that complicationin the early postoperative period.Thus, elderly patients with mul-tiple comorbidities might be better off undergoing diversion andthus avoiding the potential significant physiologic stress posed byan anastomotic leak in the early postoperative period, even thoughthey will face the additional risk associated with reoperation if theysubsequently choose to have a stoma reversed.
ROLE OF LAPAROSCOPY IN MANAGEMENT OF PERITONITIS
Laparoscopy has altered the surgical landscape by offering aminimally invasive approach that reduces the morbidity associat-ed with a large incision, generally decreasing convalescence timeand hastening return to normal activity. Nonetheless, laparoscop-ic management of intra-abdominal infection is still hinderedsomewhat by the difficulty of inspecting the entire bowel, thedecreased tactile sensation, and the significantly greater expertiserequired for laparoscopic resection and reanastomosis of the bowel.These obstacles notwithstanding, almost every intra-abdominalprocedure used to treat infection has been performed laparo-scopically with acceptable results.
The single most important factor in the decision whether totake a laparoscopic approach is the skill and experience of thesurgeon. From a theoretical point of view, it is almost always pos-sible to treat a patient with peritonitis laparoscopically; the realquestion is whether the attending surgeon can perform the pro-cedure most safely and efficiently via an open or a minimallyinvasive approach.The answer to this question will rely to a largeextent on preoperative imaging studies. In addition, even if thesurgeon does not plan to complete the operation laparoscopical-ly, initial placement of the scope may aid in planning the mostappropriate open incision and procedure by localizing the lesionof interest.
MANAGEMENT OF ANASTOMOTIC LEAKS
Dehiscence of a gastrointestinal anastomosis is a common andtoo frequently fatal complication of modern GI surgery. Again,there is little debate regarding which therapeutic options are avail-able to surgeons managing this problem.The options include thefollowing: supporting the patient with medical care only, in thecase of a tiny radiographically evident but clinically insignificantleak seen on fluoroscopic study; reoperating and performing pri-mary repair and drainage, in the case of a small early leak from anenteroenterostomy with minimal soilage; performing percuta-neous drainage, in the case of a moderately symptomatic leak pre-senting in a delayed manner with an abscess; and reexploring andperforming a diverting procedure, in the case of complete disrup-tion of an anastomosis with widespread fecal contamination.Theonly controversy has to do with which course (or combination ofcourses) to take in an individual patient.
Some general guidelines for the management of anastomoticdehiscence may be recommended, with the caveat that they havenot yet been rigorously tested. Leaks diagnosed in the immediatepostoperative period are easily approached because the relevanttissue planes have been dissected free. After 1 to 2 weeks, howev-er, early adhesion formation makes reoperation more difficult,especially if the initial operation was for an infectious or inflam-matory process, and increases the risk of complications, particu-larly inadvertent enterotomy and enterocutaneous fistula forma-tion. Small, contained leaks, if accessible, frequently respond topercutaneous drainage and antibiotics alone, with the small fistu-la resolving spontaneously. Medical management in such casesgenerally includes TPN, though enteral nutrition is occasionallyfeasible if it is shown to have no effect on drain output. Largerleaks, on the other hand, are more likely to call for direct operativerepair, resection and reanastomosis, or diversion. Once it is decid-ed that surgical treatment is warranted and is not precluded by thestate of the abdomen, definitive management should not bedelayed. Exactly which operation is to be performed depends onthe health of the bowel, the severity of abdominal contamination,and the level of overall physiologic dysfunction.
MANAGEMENT OF ENDOSCOPIC BOWEL PERFORATION
Large rents in a peritoneal portion of the bowel generally call foroperative repair (most commonly to the colon), though it shouldbe noted that simple repair or resection without diversion is almostalways all that is required. Extraperitoneal or retroperitoneal per-forations, however, can be managed nonoperatively with antibi-otics and I.V. fluids if the patient is stable. This situation occursmost frequently after ERCP or with low rectal perforations.Typically, CT scanning demonstrates retroperitoneal air with min-imal free peritoneal air. In these circumstances, patients can besafely observed as long as their condition does not deteriorate; oralintake can be restarted after 5 to 7 days. Endoscopic perforationsof a normal distal esophagus can also be managed nonoperative-ly, though a perforation proximal to a tumor or stricture is unlike-ly to heal and almost always must be treated operatively.
NONOPERATIVE MANAGEMENT OF INFECTED FLUID
COLLECTIONS
It is axiomatic that abscesses are best treated with drainagerather than with antibiotics, but there are certain circumstances inwhich drainage may not be possible. Pyogenic liver abscesses maynot be amenable to either percutaneous or open drainage if theyare multiple and involve both lobes. In such circumstances, aspi-ration or drainage of the largest abscess, followed by a long courseof antibiotics, is generally successful. It has been argued that this
© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 24

approach works because of the liver’s luxurious dual blood supply.On the other hand, multiple peritoneal fluid collections (with-
out a natural blood supply) are not infrequently seen even aftersuccessful management of diffuse or fecal peritonitis yet can occa-sionally be managed without drainage. Even if these collectionsare subsequently proved to be infected, they may be too numer-ous to approach percutaneously, and ongoing inflammation of thebowel may render an operative approach unsafe. Again, drainageof the largest accessible collection to establish a diagnosis andguide antibiotic management, followed by long-term antibiotictherapy, is the most feasible course. In this case, sampling is imper-ative because a hospital-acquired intra-abdominal infection ismore likely to involve less common but more resistant pathogens,including fungi. Regardless of the situation, though, the optimalduration of antibiotic therapy for small undrained abscessesremains to be established.
ADJUNCTIVE MEDICAL THERAPIES
Until recently, it could be said that advances in surgical therapyfor intra-abdominal infection were outpacing other aspects ofpatient management. Too often, operations were technically suc-cessful, yet patients died afterward as a result of their systemic
response to the original insult. Such deaths are still attributed tooverwhelming sepsis, to multiple organ dysfunction syndrome, orto any number of other terms used to describe an irreversiblesequence of organ failure and death [see 8:13 Multiple OrganDysfunction Syndrome].
Multiple attempts over the years to alter this downward trajec-tory by using novel therapies to target this generalized inflamma-tory response proved unsuccessful. In the past few years, however,both recombinant human activated protein C and corticosteroidreplacement therapy (for those with sepsis-associated adrenalinsufficiency) were shown to improve survival in randomized,placebo-controlled trials involving mixed populations of patientswith sepsis. Although the number of patients with intra-abdomi-nal infection was relatively small in each study, there was no indi-cation that these agents would not be similarly effective in this spe-cific subgroup. The overall benefit of each of these treatmentsappears to be small, but the results of these trials are highlyencouraging in that they suggest that related agents might be ableto achieve further decreases in mortality.These possibilities, com-bined with significant improvements in general critical care, por-tend a future in which significant reductions in mortality may berealized even in the most severely infected patients.
© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 25
References
1. Schofield PF, Hulton NR, Baildam AD: Is itacute cholecystitis? Ann R Coll Surg Engl 68:14,1986
2. Ranson JH: Acute pancreatitis. Curr Probl Surg16:1, 1979
3. Winslet M, Hall C, London NJ, et al: Relation ofdiagnostic serum amylase levels to aetiology andseverity of acute pancreatitis. Gut 33:982, 1992
4. Patti M, Pellegrini CA, Way LW: Serum amylaseis useful in the differential diagnosis of acuteabdominal pain. Gastroenterology 90:1580,1986
5. Yadav D, Agarwal N, Pitchumoni CS: A criticalevaluation of laboratory tests in acute pancreati-tis. Am J Gastroenterol 97:1309, 2002
6. Smotkin J, Tenner S: Laboratory diagnostic testsin acute pancreatitis. J Clin Gastroenterol 34:459, 2002
7. Toosie K, Chang L, Renslo R, et al: Early com-puted tomography is rarely necessary in gallstonepancreatitis. Am Surg 63:904, 1997
8. Sarr MG, Sanfey H, Cameron JL: Prospective,randomized trial of nasogastric suction inpatients with acute pancreatitis. Surgery 100:500, 1986
9. Bradley EL 3rd: Antibiotics in acute pancreatitis:current status and future directions. Am J Surg158:472, 1989
10. Steinberg WM, Schlesselman SE: Treatment ofacute pancreatitis: comparison of animal andhuman studies. Gastroenterology 93:1420, 1987
11. McArdle AH, Rosenberg M, Fried GM, et al:Pancreatic exocrine secretion in response to con-tinuous and bolus feeding (abstract), 19th Annu-al Meeting, Association for Academic Surgery,Cincinnati, Ohio, 1985
12. Erstad BL: Enteral nutrition support in acutepancreatitis. Ann Pharmacother 34:514, 2000
13. Scolapio JS, Malhi-Chowla N, Ukleja A: Nutri-tion supplementation in patients with acute andchronic pancreatitis. Gastroenterol Clin NorthAm 28:695, 1999
14. Windsor AC, Kanwar S, Li AG, et al: Comparedwith parenteral nutrition, enteral feeding attenu-ates the acute phase response and improves dis-ease severity in acute pancreatitis. Gut 42:431,1998
15. Chatzicostas C, Roussomoustakaki M, Vardas E, et al: Balthazar computed tomography se-verity index is superior to Ranson criteria andAPACHE II and III scoring systems in predict-ing acute pancreatitis outcome. J Clin Gastro-enterol 36:253, 2003
16. Liu TH, Kwong KL,Tamm EP, et al: Acute pan-creatitis in intensive care unit patients: value ofclinical and radiologic prognosticators at predict-ing clinical course and outcome. Crit Care Med31:1026, 2003
17. Stone HH, Fabian TC, Dunlop WE: Gallstonepancreatitis: biliary tract pathology in relation totime of operation. Ann Surg 194:305, 1981
18. Acosta JM, Rossi R, Galli OM, et al: Earlysurgery for acute gallstone pancreatitis: evalua-tion of a systematic approach. Surgery 83:367,1978
19. Kelly TR: Gallstone pancreatitis: the timing ofsurgery. Surgery 88:345, 1980
20. Dixon JA, Hillam JD: Surgical treatment of bil-iary tract disease associated with acute pancre-atitis. Am J Surg 120:371, 1970
21. Ranson JH:The timing of biliary surgery in acutepancreatitis. Ann Surg 189:654, 1979
22. Paloyan D, Simonowitz D, Skinner DB:The tim-ing of biliary tract operations in patients withpancreatitis associated with gallstones. SurgGynecol Obstet 141:737, 1975
23. Kelly TR, Wagner DS: Gallstone pancreatitis: aprospective randomized trial of the timing ofsurgery. Surgery 104:600, 1988
24. Neoptolemos JP, Carr-Locke DL, London NJ, etal: Controlled trial of urgent endoscopic retro-grade cholangiopancreatography and endoscopicsphincterotomy versus conservative treatmentfor acute pancreatitis due to gallstones. Lancet2:979, 1988
25. Fan ST, Lai EC, Mok FP, et al: Early treatmentof acute biliary pancreatitis by endoscopic papil-lotomy. N Engl J Med 328:228, 1993
26. Williamson RC: Early assessment of severity inacute pancreatitis. Gut 25:1331, 1984
27. Srinathan SK, Barkun JS, Mehta SN, et al: Themanagement of gallstone pancreatitis in the lap-aroscopic era. J Gastrointest Surg (in press)
28. Ranson JH, Spencer FC: Prevention, diagnosis,and treatment of pancreatic abscess. Surgery82:99, 1977
29. Osborne DH, Imrie CW, Carter DC: Biliarysurgery in the same admission for gallstone-asso-ciated acute pancreatitis. Br J Surg 68:758, 1981
30. Folsch UR, Nitsche R, Ludtke R, et al: EarlyERCP and papillotomy compared with conserv-ative treatment for acute biliary pancreatitis.TheGerman Study Group on Acute Biliary Pan-creatitis. N Engl J Med 336:237, 1997
31. Chang L, Lo S, Stabile BE, et al: Preoperativeversus postoperative endoscopic retrogradecholangiopancreatography in mild to moderategallstone pancreatitis: a prospective randomizedtrial. Ann Surg 231:82, 2000
32. Nitsche R, Folsch UR, Ludtke R, et al: UrgentERCP in all cases of acute biliary pancreatitis? Aprospective randomized multicenter study. Eur JMed Res 1:127, 1995
33. Kozarek RA, Patterson DJ, Ball TJ, et al:Endoscopic placement of pancreatic stents anddrains in the management of pancreatitis. AnnSurg 209:261, 1989
34. Ranson JH, Berman RS: Long peritoneal lavagedecreases pancreatic sepsis in acute pancreatitis.Ann Surg 211:708, 1990
35. Pederzoli P, Bassi C, Vesentini S, et al: A ran-domized multicenter clinical trial of antibioticprophylaxis of septic complications in acute nec-rotizing pancreatitis with imipenem. Surg Gyn-ecol Obstet 176:480, 1993
36. Luiten EJ, Hop WC, Lange JF, et al: Controlledclinical trial of selective decontamination for the

NECESSITY OF DIVERSION AFTER EMERGENCY COLONIC
PROCEDURES
The goal of safely repairing or resecting the colon in an emer-gency setting without leaving a patient with a temporary or per-manent stoma for diversion has been pursued for decades.Through much of the 20th century, largely on the basis ofwartime experience, diversion was routinely performed. Today,however, it is apparent that this approach is not always necessaryeither for trauma or for intrinsic colon disease. Thus, the ques-tion is no longer whether primary repair or reanastomosis can beachieved safely but, rather, in which individual patient a giventreatment is prudent.
Traditionally, clinical studies have attempted to define patientcharacteristics associated with complications after attempted pri-mary repair or reanastomosis. Not surprisingly, hypotension, bloodloss, delay before treatment, and extensive contamination have allbeen associated with postoperative complications after primaryrepair; however, these risk factors are associated with complica-tions after diversion as well.The nature of the colon injury is clear-ly an important consideration: multiple studies now support aone-step approach to traumatic colon injury in all except the mostill patients, but primary resection and reanastomosis for othercauses of perforation (e.g., diverticulosis and cancer) remain con-troversial. Many nonrandomized studies have demonstrated thatfor nontraumatic causes of perforation, on-table lavage and pri-mary resection yield outcomes equivalent to those of theHartmann procedure, which suggests that both approaches aresafe and that surgeons are capable of identifying the patients bestsuited to each one.
Perhaps more important than determining how likely a patientis to experience a complication after a given operation, however, isassessing how well the patient is likely to tolerate that complicationin the early postoperative period.Thus, elderly patients with mul-tiple comorbidities might be better off undergoing diversion andthus avoiding the potential significant physiologic stress posed byan anastomotic leak in the early postoperative period, even thoughthey will face the additional risk associated with reoperation if theysubsequently choose to have a stoma reversed.
ROLE OF LAPAROSCOPY IN MANAGEMENT OF PERITONITIS
Laparoscopy has altered the surgical landscape by offering aminimally invasive approach that reduces the morbidity associat-ed with a large incision, generally decreasing convalescence timeand hastening return to normal activity. Nonetheless, laparoscop-ic management of intra-abdominal infection is still hinderedsomewhat by the difficulty of inspecting the entire bowel, thedecreased tactile sensation, and the significantly greater expertiserequired for laparoscopic resection and reanastomosis of the bowel.These obstacles notwithstanding, almost every intra-abdominalprocedure used to treat infection has been performed laparo-scopically with acceptable results.
The single most important factor in the decision whether totake a laparoscopic approach is the skill and experience of thesurgeon. From a theoretical point of view, it is almost always pos-sible to treat a patient with peritonitis laparoscopically; the realquestion is whether the attending surgeon can perform the pro-cedure most safely and efficiently via an open or a minimallyinvasive approach.The answer to this question will rely to a largeextent on preoperative imaging studies. In addition, even if thesurgeon does not plan to complete the operation laparoscopical-ly, initial placement of the scope may aid in planning the mostappropriate open incision and procedure by localizing the lesionof interest.
MANAGEMENT OF ANASTOMOTIC LEAKS
Dehiscence of a gastrointestinal anastomosis is a common andtoo frequently fatal complication of modern GI surgery. Again,there is little debate regarding which therapeutic options are avail-able to surgeons managing this problem.The options include thefollowing: supporting the patient with medical care only, in thecase of a tiny radiographically evident but clinically insignificantleak seen on fluoroscopic study; reoperating and performing pri-mary repair and drainage, in the case of a small early leak from anenteroenterostomy with minimal soilage; performing percuta-neous drainage, in the case of a moderately symptomatic leak pre-senting in a delayed manner with an abscess; and reexploring andperforming a diverting procedure, in the case of complete disrup-tion of an anastomosis with widespread fecal contamination.Theonly controversy has to do with which course (or combination ofcourses) to take in an individual patient.
Some general guidelines for the management of anastomoticdehiscence may be recommended, with the caveat that they havenot yet been rigorously tested. Leaks diagnosed in the immediatepostoperative period are easily approached because the relevanttissue planes have been dissected free. After 1 to 2 weeks, howev-er, early adhesion formation makes reoperation more difficult,especially if the initial operation was for an infectious or inflam-matory process, and increases the risk of complications, particu-larly inadvertent enterotomy and enterocutaneous fistula forma-tion. Small, contained leaks, if accessible, frequently respond topercutaneous drainage and antibiotics alone, with the small fistu-la resolving spontaneously. Medical management in such casesgenerally includes TPN, though enteral nutrition is occasionallyfeasible if it is shown to have no effect on drain output. Largerleaks, on the other hand, are more likely to call for direct operativerepair, resection and reanastomosis, or diversion. Once it is decid-ed that surgical treatment is warranted and is not precluded by thestate of the abdomen, definitive management should not bedelayed. Exactly which operation is to be performed depends onthe health of the bowel, the severity of abdominal contamination,and the level of overall physiologic dysfunction.
MANAGEMENT OF ENDOSCOPIC BOWEL PERFORATION
Large rents in a peritoneal portion of the bowel generally call foroperative repair (most commonly to the colon), though it shouldbe noted that simple repair or resection without diversion is almostalways all that is required. Extraperitoneal or retroperitoneal per-forations, however, can be managed nonoperatively with antibi-otics and I.V. fluids if the patient is stable. This situation occursmost frequently after ERCP or with low rectal perforations.Typically, CT scanning demonstrates retroperitoneal air with min-imal free peritoneal air. In these circumstances, patients can besafely observed as long as their condition does not deteriorate; oralintake can be restarted after 5 to 7 days. Endoscopic perforationsof a normal distal esophagus can also be managed nonoperative-ly, though a perforation proximal to a tumor or stricture is unlike-ly to heal and almost always must be treated operatively.
NONOPERATIVE MANAGEMENT OF INFECTED FLUID
COLLECTIONS
It is axiomatic that abscesses are best treated with drainagerather than with antibiotics, but there are certain circumstances inwhich drainage may not be possible. Pyogenic liver abscesses maynot be amenable to either percutaneous or open drainage if theyare multiple and involve both lobes. In such circumstances, aspi-ration or drainage of the largest abscess, followed by a long courseof antibiotics, is generally successful. It has been argued that this
© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 24

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 27
98. Gerzof SG, Johnson WC, Robbins AH, et al:Intrahepatic pyogenic abscesses: treatment bypercutaneous drainage. Am J Surg 149:487,1985
99. Seeto RK, Rockey DC: Pyogenic liver abscess:changes in etiology, management, and outcome.Medicine (Baltimore) 75:99, 1996
100. Herman P, Pugliese V, Montagnini AL, et al:Pyogenic liver abscess: the role of surgical treat-ment. Int Surg 82:98, 1997
101. Klatchko BA, Schwartz SI: Diagnostic and ther-apeutic approaches to pyogenic abscess of theliver. Surg Gynecol Obstet 168:332, 1989
102. Gyorffy EJ, Frey CF, Silva J Jr, et al: Pyogenicliver abscess: diagnostic and therapeutic strate-gies. Ann Surg 206:699, 1987
103. Sabbaj J, Sutter VL, Finegold SM: Anaerobicpyogenic liver abscess. Ann Intern Med 77:627,1972
104. Huang CJ, Pitt HA, Lipsett PA, et al: Pyogenichepatic abscess: changing trends over 42 years.Ann Surg 223:600, 1996
105. Schein M,Wittmann DH, Lorenz W: Duration ofantibiotic treatment in surgical infections of theabdomen. Forum statement: a plea for selectiveand controlled postoperative antibiotic adminis-tration. Eur J Surg Suppl (576):66, 1996
106. Rubin RH, Swartz MN, Malt R: Hepatic ab-scess: changes in clinical, bacteriologic and thera-peutic aspects. Am J Med 57:601, 1974
107. Yeh TS, Jan YY, Jeng LB, et al: Pyogenic liverabscesses in patients with malignant disease: areport of 52 cases treated at a single institution.Arch Surg 133:242, 1998
108. Cohen HG, Reynolds TB: Comparison of metro-nidazole and chloroquine for the treatment ofamoebic liver abscess: a controlled trial. Gastro-enterology 69:35, 1975
109. Turkcapar AG, Ersoz S, Gungor C, et al: Sur-gical treatment of hepatic hydatidosis combinedwith perioperative treatment with albendazole.Eur J Surg 163:923, 1997
110. Saimot AG: Medical treatment of liver hydatido-sis. World J Surg 25:15, 2001
111. Stiles GM, Berne TV, Thommen VD, et al: Fineneedle aspiration of pancreatic fluid collections.Am Surg 56:764, 1990
112. Bittner R, Block S, Buchler M, et al: Pancreaticabscess and infected pancreatic necrosis. Dif-ferent local septic complications in acute pancre-atitis. Dig Dis Sci 32:1082, 1987
113. Banks PA, Gerzof SG, Chong FK, et al: Bacte-riologic status of necrotic tissue in necrotizingpancreatitis. Pancreas 5:330, 1990
114. Crass RA, Meyer AA, Jeffrey RB, et al: Pancre-atic abscess: impact of computerized tomographyon early diagnosis and surgery.Am J Surg 150:127,1985
115. Buchler M, Malfertheiner P, Schoetensack C, etal: Sensitivity of antiproteases, complement fac-tors and C-reactive protein in detecting pancre-atic necrosis: results of a prospective clinicalstudy. Int J Pancreatol 1:227, 1986
116. Ranson JH, Balthazar E, Caccavale R, et al: Com-puted tomography and the prediction of pancre-atic abscess in acute pancreatitis. Ann Surg 201:656, 1985
117. Bradley EL 3rd, Allen K: A prospective longitu-dinal study of observation versus surgical inter-vention in the management of necrotizing pan-creatitis. Am J Surg 161:19, 1991
118. Warshaw AL: Pancreatic abscesses. N Engl JMed 287:1234, 1972
119. Frey CF, Lindenauer SM, Miller TA: Pancreaticabscess. Surg Gynecol Obstet 149:722, 1979
120. Hedderich GS, Wexler MJ, McLean AP, et al:The septic abdomen: open management with
Marlex mesh with a zipper. Surgery 99:399,1986
121. D’Egidio A, Schein M: Surgical strategies in thetreatment of pancreatic necrosis and infection.Br J Surg 78:133, 1991
122. Stanten R, Frey CF: Comprehensive manage-ment of acute necrotizing pancreatitis and pan-creatic abscess. Arch Surg 125:1269, 1990
123. Rotman N, Mathieu D, Anglade MC, et al: Fail-ure of percutaneous drainage of pancreatic absces-ses complicating severe acute pancreatitis. SurgGynecol Obstet 174:141, 1992
124. Lang EK, Paolini RM, Pottmeyer A:The efficacyof palliative and definitive percutaneous versussurgical drainage of pancreatic abscesses andpseudocysts: a prospective study of 85 patients.South Med J 84:55, 1991
125. Williams LF Jr, Byrne JJ: The role of bacteria inhemorrhagic pancreatitis. Surgery 64:967, 1968
126. Gregg JA: Detection of bacterial infection of thepancreatic ducts in patients with pancreatitis andpancreatic cancer during endoscopic cannula-tion of the pancreatic duct. Gastroenterology73:1005, 1977
127. Farkas G, Marton J, Mandi Y, et al: Surgicalstrategy and management of infected pancreaticnecrosis. Br J Surg 83:930, 1996
128. Grant JP, James S, Grabowski V, et al: Total par-enteral nutrition in pancreatic disease. Ann Surg200:627, 1984
129. Johnson JD, Raff MJ, Drasin GF, et al: Radiologyin the diagnosis of splenic abscess. Rev Infect Dis7:10, 1985
130. Sones PJ: Percutaneous drainage of abdominalabscesses. AJR Am J Roentgenol 142:35, 1984
131. Berkman WA, Harris SA Jr, Bernardino ME:Nonsurgical drainage of splenic abscess. AJR AmJ Roentgenol 141:395, 1983
132. Espinoza R, Rodriguez A: Traumatic and non-traumatic perforation of hollow viscera. SurgClin North Am 77:1291, 1997
133. Ng EK, Lam YH, Sung JJ, et al: Eradication ofHelicobacter pylori prevents recurrence of ulcerafter simple closure of duodenal ulcer perfora-tion: randomized controlled trial. Ann Surg231:153, 2000
134. Tokunaga Y, Hata K, Ryo J, et al: Density ofHelicobacter pylori infection in patients with pep-tic ulcer perforation. J Am Coll Surg 186:659,1998
135. Matsukura N, Onda M, Tokunaga A, et al: Roleof Helicobacter pylori infection in perforation ofpeptic ulcer: an age- and gender-matched case-control study. J Clin Gastroenterol 25(suppl1):S235, 1997
136. Feliciano DV, Ojukwu JC, Rozycki GS, et al:Theepidemic of cocaine-related juxtapyloric perfora-tions: with a comment on the importance of test-ing for Helicobacter pylori. Ann Surg 229:801,1999
137. Cho KC, Baker SR: Extraluminal air: diagnosisand significance. Radiol Clin North Am 32:829,1994
138. Berne TV, Donovan AJ: Nonoperative treatmentof perforated duodenal ulcer. Arch Surg 124:830, 1989
139. Crofts TJ, Park KG, Steele RJ, et al: A random-ized trial of nonoperative treatment for perforat-ed peptic ulcer. N Engl J Med 320:970, 1989
140. Donovan AJ, Berne TV, Donovan JA: Perforatedduodenal ulcer: an alternative therapeutic plan.Arch Surg 133:1166, 1998
141. Siu WT, Leong HT, Law BK, et al: Laparoscopicrepair for perforated peptic ulcer: a randomizedcontrolled trial. Ann Surg 235:313, 2002
142. Lau WY, Leung KL, Kwong KH, et al: A ran-domized study comparing laparoscopic versus
open repair of perforated peptic ulcer usingsuture or sutureless technique. Ann Surg 224:131, 1996
143. Feliciano DV: Do perforated duodenal ulcersneed an acid-decreasing surgical procedure nowthat omeprazole is available? Surg Clin NorthAm 72:369, 1992
144. Christiansen J, Andersen OB, Bonnesen T, et al:Perforated duodenal ulcer managed by simpleclosure versus closure and proximal gastric vago-tomy. Br J Surg 74:286, 1987
145. Boey J, Branicki FJ, Alagaratnam TT, et al: Prox-imal gastric vagotomy: the preferred operationfor perforations in acute duodenal ulcer. AnnSurg 208:169, 1988
146. Sebastian M, Chandran VP, Elashaal YI, et al:Helicobacter pylori infection in perforated pepticulcer disease. Br J Surg 82:360, 1995
147. Kate V, Ananthakrishnan N, Badrinath S: Effectof Helicobacter pylori eradication on the ulcerrecurrence rate after simple closure of perforatedduodenal ulcer: retrospective and prospectiverandomized controlled studies. Br J Surg88:1054, 2001
148. Kauffman GL Jr: Duodenal ulcer disease: treat-ment by surgery, antibiotics, or both. Adv Surg34:121, 2000
149. Ruddell WS, Axon AT, Findlay JM, et al: Ef-fect of cimetidine on the gastric bacterial flora.Lancet 1:672, 1980
150. Hosking SW, Ling TK, Chung SC, et al: Duo-denal ulcer healing by eradication of Helicobacterpylori without anti-acid treatment: randomisedcontrolled trial. Lancet 343:508, 1994
151. Sung JJ, Leung WK, Suen R, et al: One-weekantibiotics versus maintenance acid suppressiontherapy for Helicobacter pylori–associated pepticulcer bleeding. Dig Dis Sci 42:2524, 1997
152. Sung JJ, Chung SC, Ling TK, et al: Antibacterialtreatment of gastric ulcers associated with Helico-bacter pylori. N Engl J Med 332:139, 1995
153. Wisner DH, Chun Y, Blaisdell FW: Blunt intesti-nal injury: keys to diagnosis and management.Arch Surg 125:1319, 1990
154. Fakhry SM, Watts DD, Luchette FA: Currentdiagnostic approaches lack sensitivity in the diag-nosis of perforated blunt small bowel injury:analysis from 275,557 trauma admissions fromthe EAST multi-institutional HVI trial. J Trauma54:295, 2003
155. Malhotra AK, Fabian TC, Katsis SB, et al: Bluntbowel and mesenteric injuries: the role of screen-ing computed tomography. J Trauma 48:991,2000
156. Lautenbach E, Berlin JA, Lichtenstein GR:Risk factors for early postoperative recurrence ofCrohn’s disease. Gastroenterology 115:259,1998
157. Walker AP, Krepel CJ, Gohr CM, et al: Micro-flora of abdominal sepsis by locus of infection. JClin Microbiol 32:557, 1994
158. Mazuski JE, Sawyer RG, Nathens AB, et al: TheSurgical Infection Society guidelines on antimi-crobial therapy for intra-abdominal infections:an executive summary. Surg Infect (Larchmt) 3:161, 2002
159. Reynolds SL: Missed appendicitis in a pediatricemergency department. Pediatr Emerg Care 9:1,1993
160. Rothrock SG, Green SM, Dobson M, et al:Misdiagnosis of appendicitis in nonpregnantwomen of childbearing age. J Emerg Med 13:1,1995
161. Izbicki JR, Knoefel WT, Wilker DK, et al:Accurate diagnosis of acute appendicitis: a retro-spective and prospective analysis of 686 patients.Eur J Surg 158:227, 1992
162. Rao PM, Rhea JT, Rattner DW, et al: Intro-

© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 28
duction of appendiceal CT: impact on negativeappendectomy and appendiceal perforation rates.Ann Surg 229:344, 1999
163. Rao PM, Boland GW: Imaging of acute rightlower abdominal quadrant pain. Clin Radiol53:639, 1998
164. Rao PM, Rhea JT, Novelline RA, et al:The com-puted tomography appearance of recurrent andchronic appendicitis. Am J Emerg Med 16:26,1998
165. Rao PM, Rhea JT, Novelline RA: Sensitivity andspecificity of the individual CT signs of appen-dicitis: experience with 200 helical appendicealCT examinations. J Comput Assist Tomogr 21:686, 1997
166. Rao PM, Rhea JT, Novelline RA, et al: Effect ofcomputed tomography of the appendix on treat-ment of patients and use of hospital resources. NEngl J Med 338:141, 1998
167. Walker S, Haun W, Clark J, et al: The value oflimited computed tomography with rectal con-trast in the diagnosis of acute appendicitis. Am JSurg 180:450, 2000
168. Rao PM, Feltmate CM, Rhea JT, et al: Helicalcomputed tomography in differentiating appen-dicitis and acute gynecologic conditions. ObstetGynecol 93:417, 1999
169. Wilson EB, Cole JC, Nipper ML, et al: Com-puted tomography and ultrasonography in thediagnosis of appendicitis: when are they indicat-ed? Arch Surg 136:670, 2001
170. Long KH, Bannon MP, Zietlow SP, et al: Aprospective randomized comparison of laparo-scopic appendectomy with open appendectomy:clinical and economic analyses. Surgery 129:390, 2001
171. Pedersen AG, Petersen OB, Wara P, et al: Ran-domized clinical trial of laparoscopic versus openappendicectomy. Br J Surg 88:200, 2001
172. Ortega AE, Hunter JG, Peters JH, et al: Aprospective, randomized comparison of laparo-scopic appendectomy with open appendectomy.Laparoscopic Appendectomy Study Group. Am JSurg 169:208, 1995
173. Frazee RC, Roberts JW, Symmonds RE, et al: Aprospective randomized trial comparing openversus laparoscopic appendectomy. Ann Surg219:725, 1994
174. Katkhouda N, Friedlander MH, Grant SW, et al:Intraabdominal abscess rate after laparoscopicappendectomy. Am J Surg 180:456, 2000
175. Krisher SL, Browne A, Dibbins A, et al: Intra-abdominal abscess after laparoscopic appendec-tomy for perforated appendicitis. Arch Surg 136:438, 2001
176. Larsson PG, Henriksson G, Olsson M, et al:Laparoscopy reduces unnecessary appendicec-tomies and improves diagnosis in fertile women:a randomized study. Surg Endosc 15:200, 2001
177. Enochsson L, Hellberg A, Rudberg C, et al: Lap-aroscopic vs open appendectomy in overweightpatients. Surg Endosc 15:387, 2001
178. Horwitz JR, Custer MD, May BH, et al: Shouldlaparoscopic appendectomy be avoided for com-plicated appendicitis in children? J Pediatr Surg32:1601, 1997
179. Oliak D,Yamini D, Udani VM, et al: Initial non-operative management for periappendiceal ab-scess. Dis Colon Rectum 44:936, 2001
180. Tingstedt B, Bexe-Lindskog E, Ekelund M, et al:Management of appendiceal masses. Eur J Surg168:579, 2002
181. Mazziotti MV, Marley EF, Winthrop AL, et al:Histopathologic analysis of interval appendecto-my specimens: support for the role of intervalappendectomy. J Pediatr Surg 32:806, 1997
182. Hoffmann J, Lindhard A, Jensen HE: Appendixmass: conservative management without interval
appendectomy. Am J Surg 148:379, 1984
183. Samuel M, Hosie G, Holmes K: Prospective eval-uation of nonsurgical versus surgical manage-ment of appendiceal mass. J Pediatr Surg 37:882,2002
184. Lasson A, Lundagards J, Loren I, et al: Appen-diceal abscesses: primary percutaneous drainageand selective interval appendicectomy. Eur JSurg 168:264, 2002
185. Lidar Z, Kuriansky J, Rosin D, et al: Laparo-scopic interval appendectomy for periappendicu-lar abscess. Surg Endosc 14:764, 2000
186. Bennion RS, Baron EJ, Thompson JE Jr, et al:The bacteriology of gangrenous and perforatedappendicitis—revisited. Ann Surg 211:165, 1990
187. Bennion RS, Thompson JE, Baron EJ, et al:Gangrenous and perforated appendicitis withperitonitis: treatment and bacteriology. Clin Ther12(suppl C):31, 1990
188. Bilik R, Burnweit C, Shandling B: Is abdominalcavity culture of any value in appendicitis? Am JSurg 175:267, 1998
189. Ferzoco LB, Raptopoulos V, Silen W: Acutediverticulitis. N Engl J Med 338:1521, 1998
190. Bauer T,Vennits B, Holm B, et al: Antibiotic pro-phylaxis in acute nonperforated appendicitis.The Danish Multicenter Study Group III. AnnSurg 209:307, 1989
191. Liberman MA, Greason KL, Frame S, et al:Single-dose cefotetan or cefoxitin versus multi-ple-dose cefoxitin as prophylaxis in patientsundergoing appendectomy for acute nonperfo-rated appendicitis. J Am Coll Surg 180:77, 1995
192. Salam IM, Abu Galala KH, el Ashaal YI, et al: Arandomized prospective study of cefoxitin versuspiperacillin in appendicectomy. J Hosp Infect26:133, 1994
193. Rice HE, Brown RL, Gollin G, et al: Results of apilot trial comparing prolonged intravenous anti-biotics with sequential intravenous/oral antibiot-ics for children with perforated appendicitis. ArchSurg 136:1391, 2001
194. Gorecki WJ, Grochowski JA: Are antibiotics nec-essary in nonperforated appendicitis in children?A double blind randomized controlled trial. MedSci Monit 7:289, 2001
195. Almqvist P, Leandoer L, Tornqvist A: Timing ofantibiotic treatment in non-perforated gangren-ous appendicitis. Eur J Surg 161:431, 1995
196. Ahn SH, Mayo-Smith WW, Murphy BL, et al:Acute nontraumatic abdominal pain in adultpatients: abdominal radiography compared withCT evaluation. Radiology 225:159, 2002
197. Tsushima Y, Yamada S, Aoki J, et al: Effect ofcontrast-enhanced computed tomography ondiagnosis and management of acute abdomen inadults. Clin Radiol 57:507, 2002
198. Rodkey GV, Welch CE: Surgical management ofcolonic diverticulitis with free perforation orabscess formation. Am J Surg 117:265, 1969
199. Byrne JJ, Garick EI: Surgical treatment of diver-ticulitis. Am J Surg 121:379, 1971
200. Graves HA Jr, Franklin RM, Robbins LB 2nd, etal: Surgical management of perforated divertic-ulitis of the colon. Am Surg 39:142, 1973
201. Hinchey EJ, Schaal PG, Richards GK: Treat-ment of perforated diverticular disease of thecolon. Adv Surg 12:85, 1978
202. Kohler L, Sauerland S, Neugebauer E: Diagnosisand treatment of diverticular disease: results of aconsensus development conference.The Scientif-ic Committee of the European Association for En-doscopic Surgery. Surg Endosc 13:430, 1999
203. Farthmann EH, Ruckauer KD, Haring RU:Evidence-based surgery: diverticulitis—a surgicaldisease? Langenbecks Arch Surg 385:143, 2000
204. Wong WD, Wexner SD, Lowry A, et al: Practice
parameters for the treatment of sigmoid divertic-ulitis—supporting documentation. The Stan-dards Task Force. The American Society of Co-lon and Rectal Surgeons. Dis Colon Rectum43:290, 2000
205. Ambrosetti P, Robert J, Witzig JA, et al: Inci-dence, outcome, and proposed management ofisolated abscesses complicating acute left-sidedcolonic diverticulitis: a prospective study of 140patients. Dis Colon Rectum 35:1072, 1992
206. Koruth NM, Krukowski ZH, Youngson GG, etal: Intra-operative colonic irrigation in the man-agement of left-sided large bowel emergencies.Br J Surg 72:708, 1985
207. Lee EC, Murray JJ, Coller JA, et al: Intra-operative colonic lavage in nonelective surgeryfor diverticular disease. Dis Colon Rectum40:669 1997
208. Murray JJ, Schoetz DJ Jr, Coller JA, et al:Intraoperative colonic lavage and primary anas-tomosis in nonelective colon resection. DisColon Rectum 34:527, 1991
209. Belmonte C, Klas JV, Perez JJ, et al: TheHartmann procedure: first choice or last resortin diverticular disease? Arch Surg 131:612, 1996
210. Nagorney DM, Adson MA, Pemberton JH:Sigmoid diverticulitis with perforation and gen-eralized peritonitis. Dis Colon Rectum 28:71,1985
211. Illert B, Engemann R,Thiede A: Success in treat-ment of complicated diverticular disease is stagerelated. Int J Colorectal Dis 16:276, 2001
212. Tucci G, Torquati A, Grande M, et al: Majoracute inflammatory complications of diverticulardisease of the colon: planning of surgical man-agement. Hepatogastroenterology 43:839, 1996
213. Krukowski ZH, Matheson NA: Emergencysurgery for diverticular disease complicated bygeneralized and faecal peritonitis: a review. Br JSurg 71:921, 1984
214. Gooszen AW, Gooszen HG, Veerman W, et al:Operative treatment of acute complications ofdiverticular disease: primary or secondary anas-tomosis after sigmoid resection. Eur J Surg167:35, 2001
215. Maggard MA, Chandler CF, Schmit PJ, et al:Surgical diverticulitis: treatment options. AmSurg 67:1185, 2001
216. Wedell J, Banzhaf G, Chaoui R, et al: Surgicalmanagement of complicated colonic diverticuli-tis. Br J Surg 84:380, 1997
217. Benn PL, Wolff BG, Ilstrup DM: Level of anas-tomosis and recurrent colonic diverticulitis. Am JSurg 151:269, 1986
218. Wexner SD, Moscovitz ID: Laparoscopic colec-tomy in diverticular and Crohn’s disease. SurgClin North Am 80:1299, 2000
219. Fang JF, Chen RJ, Lin BC, et al: Aggressiveresection is indicated for cecal diverticulitis. AmJ Surg 185:135, 2003
220. Lane JS, Sarkar R, Schmit PJ, et al: Surgicalapproach to cecal diverticulitis. J Am Coll Surg188:629, 1999
221. Oudenhoven LF, Koumans RK, Puylaert JB:Right colonic diverticulitis: US and CT find-ings—new insights about frequency and naturalhistory. Radiology 208:611, 1998
222. Graham SM, Ballantyne GH: Cecal diverticuli-tis: a review of the American experience. DisColon Rectum 30:821, 1987
223. Brook I, Frazier EH: Aerobic and anaerobicmicrobiology in intra-abdominal infections asso-ciated with diverticulitis. J Med Microbiol49:827, 2000
224. Runkel NS, Schlag P, Schwarz V, et al: Outcomeafter emergency surgery for cancer of the largeintestine. Br J Surg 78:183, 1991

225. Welch JP, Donaldson GA: Perforative carcinomaof colon and rectum. Ann Surg 180:734, 1974
226. Nespoli A, Ravizzini C, Trivella M, et al: Thechoice of surgical procedure for peritonitis dueto colonic perforation. Arch Surg 128:814, 1993
227. Anderson JH, Hole D, McArdle CS: Electiveversus emergency surgery for patients with co-lorectal cancer. Br J Surg 79:706, 1992
228. Koperna T, Kisser M, Schulz F: Emergencysurgery for colon cancer in the aged. Arch Surg132:1032, 1997
229. Nathens AB, Rotstein OD: Therapeutic optionsin peritonitis. Surg Clin North Am 74:677, 1994
230. Sexually transmitted diseases treatment guide-lines 2002. Centers for Disease Control andPrevention. MMWR Recomm Rep 51:1, 2002
231. Cohn DE, Rader JS: Gynecology. Surgery: BasicScience and Clinical Evidence. Surgery: BasicScience and Clinical Evidence. Norton JA,Bollinger RR, Chang AE, et al, Eds. Springer,New York, 2001, p 1923
232. Nickel JC: The management of acutepyelonephritis in adults. Can J Urol 8(suppl1):29, 2001
233. Roberts JA: Management of pyelonephritis andupper urinary tract infections. Urol Clin NorthAm 26:753, 1999
234. Naber KG, Savov O, Salmen HC: Piperacillin 2g/tazobactam 0.5 g is as effective as imipenem0.5 g/cilastatin 0.5 g for the treatment of acuteuncomplicated pyelonephritis and complicatedurinary tract infections. Int J Antimicrob Agents19:95, 2002
235. Conn HO: Spontaneous bacterial peritonitis:variant syndromes. South Med J 80:1343, 1987
236. Rimola A, Garcia-Tsao G, Navasa M, et al:Diagnosis, treatment and prophylaxis of sponta-neous bacterial peritonitis: a consensus docu-
ment. International Ascites Club. J Hepatol32:142, 2000
237. Runyon BA, Antillon MR: Ascitic fluid pH andlactate: insensitive and nonspecific tests indetecting ascitic fluid infection. Hepatology13:929, 1991
238. Felisart J, Rimola A, Arroyo V, et al: Cefotaximeis more effective than is ampicillin-tobramycin incirrhotics with severe infections. Hepatology5:457, 1985
239. Kawaguchi Y: Peritoneal dialysis as long-termtreatment: comparison of technique survivalbetween Asian and Western populations. PeritDial Int 19(suppl 2):S327, 1999
240. Vas SI: Infections of continuous ambulatoryperitoneal dialysis catheters. Infect Dis ClinNorth Am 3:301, 1989
241. Longmire WP: Suppurative cholangitis. CriticalSurgical Illness. Hardy JD, Ed.WB Saunders Co,Philadelphia, 1971, p 400
242. Stewart L, Pellegrini CA, Way LW: Cholangio-venous reflux pathways as defined by corrosioncasting and scanning electron microscopy. Am JSurg 155:23, 1988
243. Lygidakis NJ, Brummelkamp WH: Bacteremia inrelation to intrabiliary pressure in proximal v.distal malignant biliary obstruction. Acta ChirScand 152:305, 1986
244. Flemma RJ, Flint LM, Osterhout S, et al:Bacteriologic studies of biliary tract infection.Ann Surg 166:563, 1967
245. Weissglas IS, Brown RA: Acute suppurativecholangitis secondary to malignant obstruction.Can J Surg 24:468, 1981
246. Elson CO, Hattori K, Blackstone MO: Polymi-crobial sepsis following endoscopic retrograde cho-langiopancreatography. Gastroenterology 69:507,1975
247. Ong GB: A study of recurrent pyogenic cholan-gitis. Arch Surg 84:199, 1962
248. Jackaman FR, Triggs CM, Thomas V, et al:Experimental bacterial infection of the biliarytract. Br J Exp Pathol 61:369, 1980
249. Lewis RT, Goodall RG, Marien B, et al: Biliarybacteria, antibiotic use, and wound infection insurgery of the gallbladder and common bileduct. Arch Surg 122:44, 1987
250. Finegold SM: Anaerobes in biliary tract infec-tion. Arch Intern Med 139:1338, 1979
251. Shimada K, Inamatsu T, Yamashiro M:Anaerobic bacteria in biliary disease in elderlypatients. J Infect Dis 135:850, 1977
252. Shimada K, Noro T, Inamatsu T, et al:Bacteriology of acute obstructive suppurativecholangitis of the aged. J Clin Microbiol 14:522,1981
253. Lee WJ, Chang KJ, Lee CS, et al: Surgery incholangitis: bacteriology and choice of antibiotic.Hepatogastroenterology 39:347, 1992
254. Bourgault AM, England DM, Rosenblatt JE, etal: Clinical characteristics of anaerobic bactibilia.Arch Intern Med 139:1346, 1979
Acknowledgments
Figures 2 through 5 Dr. L. Stein, Montreal, Quebec.
Figure 6 From “Computed Tomography and thePrediction of Pancreatic Abscess in AcutePancreatitis,” by J. H. C. Ranson, E. Balthazar, R.Caccavale, et al, in Annals of Surgery 201:656, 1985.Used by permission.
Figure 7 From “Nonsurgical Drainage of SplenicAbscess,” by W. A. Berkman, S. A. Harris Jr., and M. E.Bernardino, in American Journal of Roentgenology141:395, 1983. Used by permission.
© 2010 Decker Intellectual Properties8 CRITICAL CARE
ACS Surgery: Principles and Practice19 Intra-Abdominal Infection — 29
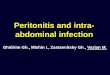













![Alternative models to study bacteria-fungi interaction · wound and surgical-site infection, and intra-abdominal and urinary tract infection [3,8,9]. In dentistry, they are frequently](https://img.pdfslide.us/doc/110x75/5e5403d3d10c0b57ca30aeb8/alternative-models-to-study-bacteria-fungi-interaction-wound-and-surgical-site-infection.jpg)