-
8/2/2019 Insulin Definitivo
1/27
1
UNIVERSIDAD DE VALENCIA
BIOCHEMESTRY AND MOLECULAR BIOLOGY
INSULIN AND ITS SIGNALLING
TEAM WORK
AUTHORS:
Maria Teresa Aranda, Arnzazu Arrieta, Brbara
Ballester, Sergio Ballesteros, Marina Belda, Isis Bonilla,Maria
Caams, Macarena Campos
DIRECTED BY:
Jose Enrique OConnor
-
8/2/2019 Insulin Definitivo
2/27
2
INDEX
INTRODUCTION 1
CHAPTER 1: STRUCTURE, BIOSYNTHESIS ANDPHARMACOLOGICAL TYPES OF
INSULIN. .. 4
CHAPTER 2: INSULIN SECRETION BY PANCREAS: SIGNALS
AND RELEASE MECHANISMS. 9
CHAPTER 3: INSULIN SIGNALLING: SIGNAL TRANSDUCTION
PATHWAYS AND METABOLIC EFFECTS. . 15
CHAPTER 4: INSULIN AND DIABETES MELLITUS:COMPARISON BETWEEN TYPE
I AND TYPE II
DIABETES MELLITUS. .. 19
REFERENCES . 26
-
8/2/2019 Insulin Definitivo
3/27
3
INTRODUCTION
Insulin is a hormone that regulates carbohydrate and fat
metabolism in the body. It can
be found in liver, all muscles, and fat tissue in order to take
up glucose from the blood and store
it as glycogen in the liver and muscles. It is produced in the
islets of Langerhans in the pancreas.
Insulin impedes the use of fat as an energy source inhibiting
the release ofglucagon.Its
also a central metabolic control mechanism of other body systems
(such as amino acid uptake
by body cells).
A failure in the control of insulin levels results in diabetes
mellitus. As a consequence,
insulin is medically used to treat some forms of diabetes
mellitus. There are two types of
diabetes depending on the production or not of insulin: type 1
and type 2. In type 1 the hormone
is no longer produced internally while in type 2 insulin is
produced but in a deficiency amount.
The name comes from the Latin insula for "island". Insulin's
structure varies slightly
between species of animals, indeed porcine insulin is especially
close to the human version.
Thanks to several discoveries about insulin, their authors have
won the Nobel Prize
during the 20 century. For instance, insulin was the first
protein to have its amino acid sequence
sequenced, in 1955 by Fred Sanger (Sanger 1988), earning him a
Nobel prize in 1958. It was
also the first peptide hormone, circulating in minute amounts,
to be measured by
radioimmunoassay (Berson and Yallow 1961), earning Yalow a Nobel
Prize in 1977. The
pathway behind the biosynthesis of insulin in pancreatic beta
cells, specifically as a proinsulin
precursor, was determined by Don Steiner in 1967 (Steiner and
James 1992). The three-
dimensional structure of insulin was ultimately solved by
Dorothy Crowfoot Hodgkin and
colleagues in 1969, using X-ray crystallographic methods (Adams
et al. 1969). It was also the
first protein to be synthesized in microorganisms by recombinant
DNA technology in the late
1970s.
http://en.wikipedia.org/wiki/Hormonehttp://en.wikipedia.org/wiki/Fathttp://en.wikipedia.org/wiki/Liverhttp://en.wikipedia.org/wiki/Musclehttp://en.wikipedia.org/wiki/Fat_cellhttp://en.wikipedia.org/wiki/Glucosehttp://en.wikipedia.org/wiki/Bloodhttp://en.wikipedia.org/wiki/Glycogenhttp://en.wikipedia.org/wiki/Islets_of_Langerhanshttp://en.wikipedia.org/wiki/Pancreashttp://en.wikipedia.org/wiki/Glucagonhttp://en.wikipedia.org/wiki/Amino_acidhttp://en.wikipedia.org/wiki/Diabetes_mellitushttp://en.wikipedia.org/wiki/Latinhttp://en.wikipedia.org/wiki/Specieshttp://en.wikipedia.org/wiki/Pighttp://en.wikipedia.org/wiki/Humanhttp://en.wikipedia.org/wiki/Humanhttp://en.wikipedia.org/wiki/Pighttp://en.wikipedia.org/wiki/Specieshttp://en.wikipedia.org/wiki/Latinhttp://en.wikipedia.org/wiki/Diabetes_mellitushttp://en.wikipedia.org/wiki/Amino_acidhttp://en.wikipedia.org/wiki/Glucagonhttp://en.wikipedia.org/wiki/Pancreashttp://en.wikipedia.org/wiki/Islets_of_Langerhanshttp://en.wikipedia.org/wiki/Glycogenhttp://en.wikipedia.org/wiki/Bloodhttp://en.wikipedia.org/wiki/Glucosehttp://en.wikipedia.org/wiki/Fat_cellhttp://en.wikipedia.org/wiki/Musclehttp://en.wikipedia.org/wiki/Liverhttp://en.wikipedia.org/wiki/Fathttp://en.wikipedia.org/wiki/Hormone
-
8/2/2019 Insulin Definitivo
4/27
4
CHAPTER 1 - STRUCTURE, BIOSYNTHESIS AND
PHARMACOLOGICAL TYPES OF INSULIN
1.The Structure of InsulinInsulin is a pedtidic hormone composed
of two polypeptide chains: chain A has 21 amino
acids and chain B has 30 amino acids (in humans). That sums a
total of 51 amino acids linked
by two disulfide bridges (residues A7 to B7, and A20 to B19).
These are covalent bonds that
tether both chains. Chain A also contains an internal disulfide
bridge (between the residues A6
to A11).
This is an endocrine hormone, which means that it is secreted
into the
blood stream through which it travels to affect distant organs.
It has a
compact three-dimensional structure (insulin monomer is
essentially the
same in solution and in solid phase) consisting of three short
helices and
three invariant (conserve) disulfide bridges. This basic fold
(three-dimensional) is present in all members of the insulin
peptide family,
despite divergent sequences.
Due to the fact that insulin is a protein, it has four
structural levels.
Insulin and insulin preparations during storage and use can be
affected by a variety of chemical
changes of the primary structure (yielding insulin derivatives)
and physical modifications of the
secondary to quaternary structures (resulting in "denaturation,"
aggregation, and precipitation).
Insuline mainly exists in two main quaternary conformations that
can adopt a
therapeutically-significant "R" or "T" state (both are hexamers,
therefore they are used in
preparations for therapy). These differ in the extent of helix
in the B chain which is governed bythe presence of phenol or its
derivatives. In acid and neutral solutions (in micromolar
concentrations relevant for pharmaceutical formulation) the
insulin monomer assembles to
dimers while in neutral pH (in the presence of Zinc ions) it
further associates into hexamers.
When the A chain has an amino-terminal helix (A1-A8) linked to
an antiparallel carboxy-
terminal helix (A12-A20) and the B chain has a central helix
(B8-B19), flanked by extended
amino- and carboxy-terminal strands this arrangement is called
the "T" conformation. On the
other hand "R" conformation exists where the B chain helix
extends from the N-terminus (B1-
B19, versus B8-B19). In the 4-Zn hexamer, three of the monomers
are in the T form and three
are in the R form (R3T3), as a result of a high chloride
concentration. An R6 form exists in
phenol-containing crystals and in solution
An allosteric equilibrium controls the T-R transition, which
plays an important role in the
formulation of therapeutic insulin where chloride is used as an
isotonic agent and phenol is used
as an antimicrobial agent.
Despite the fact that insulin has different conformations, the
biologically active one is the
monomeric conformation.
-
8/2/2019 Insulin Definitivo
5/27
5
Stability of the structure: The insulin hexamer forms a
relatively stable unit but some
flexibility remains within the individual molecules. The
intrinsic flexibility at the ends of the B
chain plays an important role in governing the physical and
chemical stability of insulin. One of
the things that contribute to protein stability is a cluster of
hydrophobic residues that form the
core of the small protein.
2.Biosynthesis of insulinInsulin is synthesized in the pancreas.
This organ can act as an exocrine or an endocrine
system. The endocrine function is executed by a group of small
structures called islet of
Langerhans (1% of the pancreatic mass) which are composed of
different cells that produce
hormones. There are 4 types: (A), (B), (D) and Pp (F).
The cells are localized in the middle of the islet. They are
activated when the organism has
metabolism fuel like glucose, aminoacids These nutrients induce
the release of someproducts: insulin, c-peptide, amylin and
sometimes proinsulin. Although insulin is the main
product, c-peptide is released in the same molar amount as
insulin. Amylin is a small peptide
that appears in diabetis type II and proinsulin appears when it
hasnt be removed (incorrect
process).
The cells are situated in the periphery of the islet. They
become active in stress situation,
that means when the organism has a deficiency of nutrients
(glucose, aminoacids). They
release glucagon to the blood stream in order to mobilize energy
and release glucose from the
liver.
The cells have a suppressor function. They inhibit the release
of products by the and cells by a hormone called somatostatin
(GHIH: growth hormone-inhibition hormone). They are
located overall within the islet.
This inhibition by the cells is due to their innervation. The
artery enters directly in the
middle of the cell irrigating first the cells. Then the
capillaries spread towards the periphery
and the venules take the stream into the veins. This direccion
allows that whatever the cells
produce, passes through the and cells so they can act in
response. This is called a paracrine
regulation.
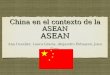
To explain in more detail how the
insulin is synthesized, we must followthe route of synthesis
inside the cell.
Inside the nucleus, the gene that
codifies for insulin is in the
chromosome 11. Once this chromosome
is converted into chromatin and opened
for the transcription, mRNA can be
formed. Then it will go to the
cytoplasm, and several ribosomes will
bind to this chain in order to execute the
translation. When a peptide chain startsto form, ribosomes go to
the
-
8/2/2019 Insulin Definitivo
6/27
6
endoplasmic reticulum (rough endoplasmic reticulum) and the
different chains of aminoacids
enter inside the lumen.
Its inside the lumen where the precursor of the insulin, called
preproinsulin, is formed. It
has an initial segment (signal sequence), an amino-terminal
B-chain, a connector segment (C-
chain) and a carboxy-terminal A-chain. At this place
preproinsuline is exposed to severalspecific endopeptidades
(proteolytic enzymes) that break the signal sequence, therefore the
pre
compartment is lost.
This molecule now called proinsuline has three disulphide bonds:
two between the B and A
chain and one within the A-chain. At this moment the molecule is
folded in a vesicle and
transported to the golgi apparatus. There it is cut again by the
endopeptidases, but this time the
C-chain (which was between the B and the A chains) is deleted.
Now the mature insulin is
formed. It is stored in vesicles (in the cytoplasm) ready to be
released. Finally its in this
secretory granules where the mature insulin and the C-peptides
are and this is the reason why
they are in the same amount. Zinc and proinsulin can also be
found when the maturation hasnt
been completed.
When the beta cell is appropriately stimulated, insulin is
secreted from the cell by exocytosis
and diffuses into islet capillary blood. C peptide is also
secreted into blood, but has no known
biological activity.
As most of the processes in the organism, this endogenous
production of insulin is regulated
in several steps along the synthesis pathway, for example: at
transcription from the insulin gene,
in mRNA stability, at the mRNA translation, in the
posttranslational modifications, etc.
3. Pharmacological types of insulinBovine or porcine insulins
have nearly disappeared from the market, displaced by human
insulin obtained by genetic engineering. All current
preparations have been submitted to a
process of ultrapurification to eliminate any foreign
proteins.
The different types of insulin are categorized according to how
long it takes to begin
working (onset), when it's working the hardest (peak) and how
long it lasts (duration). The types
now available include rapid-, short-, intermediate-, and
long-acting insulin.
Doctors will work in developing an insulin regime that works
specifically for each person,his health and his lifestyle. People
should never make changes in their dosage without first
consulting with their doctor. These insulin regimes consist in
prepared mixtures of fast with
intermediate insulin which are nowadays available on the market,
with the purpose of
obtaining a quick start and long duration medication. These
prepared mixtures are called
biphasic insulins and are basically Humulin, Humalog, Mixtard
and Novomix. Usually people
who take insulin use a combination of a rapid- or short-acting
and intermediate- or long-acting
insulin. This helps keeping blood sugar levels within a range
that is safe for the body throughout
the day.
http://www.news-medical.net/health/What-is-Insulin.aspxhttp://www.news-medical.net/health/Genes-What-are-Genes.aspxhttp://www.news-medical.net/health/Genes-What-are-Genes.aspxhttp://www.news-medical.net/health/What-is-Insulin.aspx
-
8/2/2019 Insulin Definitivo
7/27
7
Nowadays the main types of insulin are:
Rapid-acting
Generic Name Brand Name Action Doing schedule
Insulin aspart Novorapid Onset: 10-15 minutes.
Peak: 60-90 minutes.
Duration: 3-5 hours.
Usually taken right
before eating, or to
lower high blood
glucose.
Insulin glulisine Apidra
Insulin lispro Humalog
Insulin regular Humulin-R Onset: 30 minutes.
Peak: 2-3 hours.
Duration: 6.5 hours.
Taken about 30 minutes
before eating, or to
lower high blood
glucose.
Intermediate-acting
Generic Name Brand Name Action Doing schedule
Insulin NPH Humulin-N Onset: 1-3 hours.
Peak: 5-8 hours.
Duration: up to 18
hours.
Often taken at
bedtime, or twice a
day (morning and
bedtime).
Slow-acting
Generic Name Brand Name Action Doing schedule
Insulin detemir Levemir Onset: 90 minutes.
Peak: none.
Duration: up to 24
hours (Lantus 24 hours,
Levemir 12-24 hours).
Usually taken once or
twice a day.Insulin glargine Lantus
How insulin is taken
The usual way of insulin administration is subcutaneous. The
most common method
of administration is using special syringes graduated in units
of insulin (IU). Injector devices in
the form of pen injector have reached acceptance, because they
facilitate regimes of multiple
-
8/2/2019 Insulin Definitivo
8/27
8
injections per day. There are also prefilled syringes capable of
dispensing with precision in
increments of 2 IU and useful for many applications by changing
the needle. Infusion pumps
administrate continuously a basal insulin dose, supplemented by
extra doses before meals. Some
insulin can be given through a vein but only in a hospital.
Injectable insulin is packaged in small
glass vials (bottles) and cartridges that hold more than one
dose and are sealed with rubber lids.
The cartridges are used in pen-shaped devices called insulin
pens.
Research is on going to develop not only new forms of insulin
but also insulin that can
be taken in other ways, such as by mouth. These are the
different ways of injecting insulin
nowadays: pen injector, jet injector or external pump.
Dosing guideline
The spread of the idea that strict glycemic control can prevent
long term complications
of diabetes has created a tendency to use dosing schedules aimed
to fit as closely to the
administration of insulin to the diurnal variations of glycemia.
This involves multiple daily
injections regimens and glycemic control by the patient himself.
The most commonly used
guidelines today are:
- Two doses of a mixture of intermediate and rapid insulin. The
popularity of this regime
explains the spread of biphasic insulin preparations.
- A daily dose of long-acting insulin and three insulin
injections per day fast before the
main meals. This regimen requires motivated patients, but has
the advantage of
allowing more flexible meal times. Systems have been introduced
to minimize its
drawbacks; one of them is the use of pens-type injectors.
Side effects
The major side effect of insulin can be a dangerously low blood
sugar level (severe
hypoglycemia). A very low blood sugar level can develop within
10 to 15 minutes with rapid-
acting insulins. Insulin can contribute to weight gain,
especially in people with type 2 diabetes
who already are overweight. Other possible side effects of
long-term insulin use include the loss
of fatty tissue (lipodystrophy) where the insulin is injected
and, in rare cases, allergic reactionsthat include swelling or
edema.
-
8/2/2019 Insulin Definitivo
9/27
9
CHAPTER 2 - INSULIN SECRETION BY PANCREAS:
SIGNALS AND RELEASE MECHANISMS.
Insulin secretion is pulsatile (i.e. increases as needed by
bursts) and is regulated by a
variety of stimulatory and inhibitory factors, most of them
related to glucose metabolism andthe effects of cAMP. This explains
that Insulin secretion is stimulated by high blood glucose
levels and reduced when blood glucose is low. This makes sense
because insulin is in charge of
facilitating glucose entry into cells.
Some neural stimuli (e.g. sight and taste of food) and increased
blood concentrations of
other substances, including amino acids from ingested proteins,
fatty acids, acetylcholine
released from vagus nerve endings (parasympathetic nervous
system), and gastrointestinal
hormones released by enteroendocrine cells of intestinal mucosa
and glucose-dependent
insulinotropic peptide (GIP), also promote insulin
secretion.
These hormons that stimulate insulin secretion are: growth
hormone, placental lactogen,
estrogens, and progestins. These increase its secretion by
increasing the preproinsulin mRNA
and enzymes involved in processing the increased preprohormone.
Inhibitory factors include
somatostatin, norepinephrine (sympathetic stimulation) and
others.
Also, in general, some release takes place with food intake, not
just glucose or
carbohydrate intake, and the -cells are also somewhat influenced
by the autonomic nervous
system.
Our understanding of the mechanisms behind insulin secretion
remains somewhat
fragmentary. Nonetheless, certain features of this process have
been clearly and repeatedly
demonstrated.
The - cells in the islets of Langehans release insulin, mainly
in response to the
presence of high levels of glucose in the blood, in two phases.
The first phase release is rapidly
triggered in response to increased blood glucose levels. The
second phase is a sustained, slow
release of newly formed vesicles triggered independently of
sugar.
These cells are quite dependent upon glucose as its substrate
for energy metabolism.
Neither fatty acids nor amino acids can serve as substrates to
support high ATP levels which
play a significant role in this process.
Also - cells contain several types of channels in their
membranes, each of which
allows a particular type of ion to pass through. These include
channels that let K+
ions pass
through and others that let Ca2+
pass through.
Normally, the K+
channels are open, leaving the K+
ions free to pass through. These
positively charged ions diffuse from inside the cell to outside.
This makes the outside of the cell
positively charged compared with inside. We say that there is a
potential difference across the
membrane. The potential difference across the plasma membrane of
a resting -cell - one which
is not secreting insuline- is about -70 mV.
-
8/2/2019 Insulin Definitivo
10/27
10
However, when glucose enters into the - cell by facilitated
diffusion through the
glucose transporter GLUT2 the concentration of it within the -
cell rise sharply, and this
increase in glucose levels starts off a chain of events which
alters the potential difference of the
resting - cell. In other words, elevated concentrations of
glucose in extracellular fluid leads to
elevated concentrations of glucose within the beta cell, and as
a consequence many processes
related to the secretion of insulin begin. Once the glucose is
inside the - cell it is quicklyphosphorylated by the enzyme
glucokinase. Then, this phosphorylated glucose goes into
glycolysis and the respiratory cycle, where multiple high-energy
ATP molecules are produced
by oxidation.
As a result, the K+
channels which are sensitive to the amount of ATP in the
cell
respond to this increase in ATP levels by closing. So now the
K+
ions cannot diffuse out.
Consequently, the difference in electrical potential on the
inside and the outside of the
memebrane becomes less. It is now only about -30mV, this is
called a depolarization of the
membrane.
On depolarization, voltage-controlled calcium channels (Ca2+
) open and extracellular
calcium flows into the cells. This increase in calcium levels
causes the activation of
phospholipase C, which cleaves the membrane phospholipid
phosphatidyl inositol 4,5-
biphosphate into inositol 1,4,5-triphosphate and diacylglycerol.
Inositol 1,4,5-triphosphate (IP3)
binds to receptor proteins in the membrane of endoplasmic
reticulum (ER). This allows the
release of Ca2+
from the ER via IP3-gated channels, and further raises the cell
concentration of
calcium. A significant increase in the amount of calcium affects
the behaviour of the vesicles in
the cells and causes the release of previously synthesized
insulin, which has been stored in these
secretory vesicles, these vesicles are moved towards the plasma
membrane, where they fuse
with the membrane and empty their contents outside the cell.
This is the main mechanism of
insulin release.
-
8/2/2019 Insulin Definitivo
11/27
11
Clearly, elevated glucose not only simulates insulin secretion,
but also transcription of
the insulin gene and translation of its mRNA.
Stimulation of insulin release is readily observed in whole
animals or people. The
normal fasting blood glucose concentration in humans and most
mammals is 80 to 90 mg per
100 ml, associated with very low levels of insulin
secretion.
The figure to the right depicts the effects
on insulin secretion when enough glucose is
infused to maintain blood levels two to three
times the fasting level for an hour. Almost
immediately after the infusion begins, plasma
insulin levels increase dramatically. This initial
increase is due to secretion of preformed insulin,
which is soon significantly depleted. The
secondary rise in insulin reflects theconsiderable amount of
newly synthesized insulin
that is released immediately.
The exocrine pancreas has a very important rol in the
stimulation of insulin secretion by
intestinal hormones.
Two of the many gastrointestinal hormones have significant
effects on insulin secretion
and glucose regulation. These hormones are the glucagon-like
peptides (principally glucagon-
like peptide-1, GLP-1) and glucose-dependent insulinotropic
peptide (GIP). Both of these gut
hormones constitute the class of molecules referred to as the
incretins. Incretins are molecules
associated with food intake-stimulation of insulin secretion
from the pancreas.
GLP-1 is derived from the product of the proglucagon gene (gene
symbol = GCG). This
gene encodes a preproprotein that is differentially cleaved
dependent upon the tissue in which it
is synthesized.
Glucose-dependent insulinotropic polypeptide (GIP) is a key
incretin hormone, released
from intestine after a meal, producing a glucose-dependent
insulin secretion. While, the GIP
receptor (GIPR) is expressed on large neurons, and is
synthetised in a subset of neurons in the
brain.
It is also important to explain tthe role of aminoacids in the
secretion of insulin. Specific
amino acids may acutely and chronically regulate insulin
secretion from pancreatic -cells in
vivo and in vitro by altering the b-Cells membrane potencial.
Mitochondrial metabolism is
crucial for the coupling of glucose, alanine, glutamine and
glutamate recognition with
exocytosis of insulin granules.
Mitochondria generate ATP (the main coupling messenger in
insulin secretion) and
other factors that serve as sensors for the control of the
exocytotic process. The main factors thatmediate the key amplifying
pathway over the Ca
2+signal in nutrient-stimulated insulin secretion
-
8/2/2019 Insulin Definitivo
12/27
12
are nucleotides (ATP, GTP, cAMP and NADPH), although metabolites
have also been
proposed, such as long-chain acyl-CoA derivatives and glutamate.
In addition, after chronic
exposure, specific amino acids may influence gene expression in
the -cell, which have an
impact on insulin secretion and cellular integrity. Therefore
amino acids may play a direct or
indirect (via generation of putative messengers of mitochondrial
origin) role in insulin secretion.
Arginine is the amino acid reputed to stimulate the highest
production of both insulin
and glucagon. L-arginine is a potent stimuli for insulin
secretion from pancreatic b-cells.
However, the precise molecular mechanisms of amino acid-induced
insulin secretion have only
partly understood.
Acetylcholine is a neurotransmitter that has a major role in the
function of the insulin-
secreting pancreatic beta cell. Parasympathetic innervation of
the endocrine pancreas, the islets
of Langerhans, has been shown to provide cholinergic input to
the -cell in several species, but
the role of autonomic innervation in human -cell function is at
present unclear. It is known
that the -cells of human islets provide paracrine cholinergic
input to surrounding endocrine
cells. Human -cells express the vesicular acetylcholine
transporter and release acetylcholine
when stimulated with kainate or a lowering in glucose
concentration. Acetylcholine secretion by
alpha cells in turn sensitizes the -cell response to increases
in glucose concentration. It has
beendemostrated by many scientists that in human islets
acetylcholine is a paracrine signal that
primes the -cell to respond optimally to subsequent increases in
glucose concentration. [1]
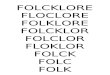
Acetylcholine not only increases the secretion of insuline by
improving the -cells response, but
also increases the granules movement. As show the pictueres
below:
Intracellular movement of secretory granules is a proximal stage
in the insulin secretory
cascade that ends in the release product from cells. The
mechanisms underlying the control of
this movement by acetylcholine has been investigated, thus
trying to clarify how this NT acts.
Acetylcholine activates intracellular movement of secretory
granules as a result of
muscarinic mobilization of intracellular Ca2 +.
Acetylcholine has been reported to exert versatile effects on
the secretory machinery of
the pancreatic -cell. Hydrolysis of phosphatidylinositol
4,5,bisphosphate by activation of PLC
via muscarinic activation positively controls insulin release by
I P3-induced Ca2 +mobilization
-
8/2/2019 Insulin Definitivo
13/27
-
8/2/2019 Insulin Definitivo
14/27
14
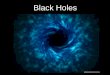
Clockwise from left: the approach of vesicles to the membrane
requires the formation of
a Sec6Sec8 (exocyst) complex (DOCKING). Fusion of docked
vesicles requires an elevation
of Ca2+ concentration and a Ca2+ sensor such as synaptotagmin
V/IX. Fusion is usually
incomplete, releasing only a proportion of the vesicles soluble
cargo and of vesicle membrane-
associated SNARES such as synpatobrevin (brown) (84). Insulin is
released as dimers with
Zn2+ through a fusion pore likely to be less than ~4 nm across,
whereas low molecular massspecies such as ATP (50) and lipid
components of the vesicle membrane are likely to rapidly
associate with plasma membrane lipids . Such "cavity recapture"
events are terminated by the
recruitment of dynamin-1 (RECAPTURE). Vesicles that have passed
through a single round of
exocytosis, but still retain adequate numbers of SNAREs, may
then undergo further fusion
events. Alternatively, vesicles may fuse with the endosomal
network for destruction or may
exchange membrane proteins and soluble cargo with maturing
vesicles (EXCHANGE). The
relative importance in the delivery to mature vesicles of
membrane proteins (SNAREs, Sec6,
phogrin, etc.) of de novo delivery at the TGN, and later
delivery by the recycling mechanisms
above, remains to be established.
-
8/2/2019 Insulin Definitivo
15/27
15
CHAPTER 3 - INSULIN SIGNALLING: SIGNAL
TRANSDUCTION PATHWAYS AND METABOLIC
EFFECTS.
1. Insulin signal transduction pathways.After insulin enters the
bloodstream, it binds to an enzyme (Tyrosine Kinase) that acts as
the
insulin receptor (IR) and is located at the cell membrane.
The insulin receptor (IR) is a tetrameric enzyme comprising two
extracellular -subunits and
two transmembrane -subunits. When insulin binds to the
extracellular port of the IR the
intrinsic tyrosine kinase activity of the -subunits of the IR is
activated. This leads to an
autotransphosphorylation of the IR where one -subunit
phosphorylates the other on several
tyrosine residues.
The union of insulin to its receptor results in: decrease of the
release and production ofglucose, and increase in the uptake of
glucose. The uptake of glucose is caused by the
translocation and exocytosis of GLUT4 storage vesicles and the
activation of enzymes that
activate the insulin transduction pathway and inhibit enzymes
that slow/stop the insulin
transduction pathway.
The activity of the IR enzyme causes phosphorylation
(activation) of two enzymes: Mitogen-
activated Protein Kinase (MSP-Kinase) and
Phosphatidylinositol-3-Kinase (PI-3K).
The activation of MAP-Kinase leads to completion of mitogenic
functions like cell growth
and gene expression.
The activation of PI-3K leads to the main insulin transduction
pathway which intervenes in
the completion of metabolic functions such as synthesis of
lipids, proteins and glycogen. The
PI-3K pathway separates the GLUT-4 vesicle (the main glucose
transporter) from the glucose,
and sends the vesicle to the plasma membrane while the glucose
is sent to the mitochondria to
produce ATP or is stored as glycogen. The steps of this pathway
are:
1. The insulin receptor substrate (IRS1/2) recruits to the
plasma membrane the class Iphosphoinositide 3 kinase which is
activated by this recruitment (PI3K is a
heterodimeric protein composed of a p110 catalytic and a p85
regulatory subunit
which binds to IRS adaptor proteins).
2. Class I phosphoinositide 3 kinase catalyses the conversion of
PIP2 to PIP3, so themain product of PI3K is the PI(3,4,5)P3.
3. The increase of PIP3 induces the recruitment and
co-localizationof protein kinase B(PKB or Akt) and PDK1. Once
recruited to the plasma membrane PKB/Akt is
activated by the action of PDK1 and TORC2. The PKB/Akt
substrates that link insulin
signaling events to GLUT4 translocation are: AS160, TBC1D1 and
PIKfyve.
3.1.AS160: contains two phosphotyrosine binding domains (PTB), a
GAP domainselective for Rab small GTP-binding proteins and seven
potential PKB/Akt
phosphorylation sites. To allow the translocation of GLUT4,
multiple Rab
proteins must be activated. The GAP domain of AS160 suppress the
activity
-
8/2/2019 Insulin Definitivo
16/27
16
of these proteins therefore preventing GLUT4 translocation.
The
phosphorylation of AS160 is thought to render the GAP domain
inactive and,
as a consequence, stimulate GLUT4 translocation.
3.2.TBC1D1: its very similar to AS160 but they differ,
particularly, in theirphosphorylation. Expression of AS160
predominates in both adipose tissueand slow twitch muscle fibres,
whereas TBC1D1 is more abundant in fast
twitch muscle fibres. TBC1D1 also plays an important role in the
stimulation
of muscle glucose uptake in response to contraction and
activators of AMP
kinase.
3.3.PIKfyve: this protein binds to PI3P and phosphorylates PI3P
to yieldPI(3,5)P2. This process might link plasma-derived PIP3
signals to intracellular
PI(3,5)P2 production, and thereby to the control of GLUT4
trafficking
between endosomes and the TGN, from where GLUT4 may feed into
the GSV
pool. The protein PIKfyve is affected not only by insulin but
also by
hyperosmotic stress, being the response independent of
PI3-kinase and
PKB/Akt.
The PI-3K pathway is also involved in the process of glycoysis
as it controls the
phosphorylation, and consequently activation, of PFK-2 which is
a potent stimulator of PFK-1,
the main enzyme-regulating glycolytic flux. To sum up, the
activation of the PI-3K pathways
increases the uptake of glucose and is controlled by different
enzymes (i.e. GSK-3 and PKA,
which constrict its activity, AKT and P70, which stimulate the
pathway). Insulin will, therefore,
increase the action of AKT and P70, and inhibit the activity of
GSK-3 and PKA.
Also important is how insulin controls the GLUT4 translocation
to the plasma
membrane because this vesicle is responsible for passive
diffusion of glucose in the cell. There
are two models of how this process takes place:
Dynamic retention: the GLUT4 pool is in dynamic equilibrium
between the cell surfaceand intracellular compartments. In this
model insulin signalling increases the rate
constants for docking and fusion of GLUT4 with the plasma
membrane to increase the
amount of glucose present at the plasma membrane. GLUT4
translocates to the plasma
membrane via fusion with it, via a cycling pool or a combination
of both routes.
Static retention: the GLUT4 is actively retained within a
storage pool that does notcommunicate with other intracellular
compartments in the absence of insulin. Thismodel requires that
insulin enters deep into the cell to induce the liberation of
GLUT4
from the pool(s) into the cycling system and from there towards
the plasma membrane.
Due to the position of the pool, GLUT4 must transverse the
cytoplasm before arriving
to the plasma membrane, but data suggests that microtubules dont
play an important
role in the movement of GLUT4 vesicles to the plasma
membrane.
Therefore insulin has two effects on GLUT4, it regulates the
release of GLUT4 from
intracellular storage pools and it increases the docking and
fusion of GLUT4 vesicles with the
plasma membrane reducing the mobility of GLUT4 vesicles in order
to allow the fusion of those
vesicles that have docked. Consequently insulin translocates
GLUT4 from the intracellular
stores to the plasma membrane where it increases glucose uptake
by up to 2-fold over basal
levels.
-
8/2/2019 Insulin Definitivo
17/27
17
The signaling pathway that regulates the process of docking and
fusion appears to be PI3K
dependent, as several studies suggest that the stimulation of
PKB/Akt activity at the plasma
membrane is the step in the insulin-sensitive signaling that
ultimately leads to fusion. However,
the movement of GLUT4 vesicles to the cell periphery is
independent of PI3K signaling. The
plasma membrane is an important site of insulin action because
many studies suggest that
insulins main regulation effect is not on GLUT4 vesicles but on
the plasma membrane, butmore investigation remains to be done in
this direction.
The activation of the IR also causes the stimulation of a second
signal transduction
pathways that, although it plays a minor role in
insulin-stimulated GLUT4 translocation, its
involved in the regulation of important processes such as
cortical actin rearrangements, PI(3)P
formation at the plasma membrane, recruitment of the exocyst
complex to the plasma membrane
via Exo70 and the inactivation of Rab31. The steps of this
pathway, known as Wortmannin-
insensitive pathway, are:
1. Recruitment and tyrosine phosphorylation of c-Cbl to the
activated insulin receptor viatwo adaptor proteins (APS and
CAP).
2. c-Cbl recruits the adaptor protein CrKII and the guanine
nucleotide exchange factorG3G to lipid rafts (where c-Cbl is
attached) C3G specifically activates the small GTP
binding protein TC10.
In order to decrease the production of glucose in the cell,
insulin indirectly activates PP-1. It
is an enzyme that dephosphorylates and activates the glycogen
synthase therefore increasing the
synthesis of glycogen, and it also dephosphorylates and
inactivates the glycogen phosphorylase
decreasing, as a consequence, the rate of degradation of
glycogen to glucose and the level of
glucose in the cell.
In conclusion, insulin acts on several intracellular signaling
pathways that regulate
metabolic activity, gene transcription and cell growth, being
its main function the stimulation of
glucose uptake by cells. To know about the components, function
and steps of these pathways is
an important advance in medicine because it will allow us to
regulate them in order to treat
many diseases related to insulin.
2. The metabolic effects of insulin.The pancreas secretes
insulin and equimolar amounts of peptide C. Between 10 to 15%
of
insulin detected by radioimmunoassay (RIA) corresponds to
proinsulin.
The insulin concentration determined by RIA in fasting is from 5
to 15 uU / ml and 30
to 75 uU / ml in the postprandial period. C-peptide has a
peripheral concentration 10 times
higher.
C-peptide levels in fasting is 2 to 4 ng / mL and postprandial 4
to 6 ng / ml.
Measurement of C-peptide concentrations in fasting or post
glucagon stimulation is a good
expression of the synthesis and secretion of insulin, which can
be measured even in patients
who receive insulin, since the latter has no cross-reaction with
peptide C.
The half-life of insulin is 4.8 and the proinsulin is 17.5
minutes.
-
8/2/2019 Insulin Definitivo
18/27
18
The degradation of insulin was performed in liver and kidney,
but preferably in the liver
and proinsulin C-peptide and the kidney. Insulin in a high
percentage is captured in its first pass
through the liver, but not C-peptide
The catabolism begins with the breaking of the disulfide bridges
by the action of
glutathione insulintransferasa, then start proteolysis,
releasing inactive peptides.
The biological activity of proinsulin is 10% of insulin and
C-peptide is completely
inactive.
Insulin receptors:
The biological action of insulin is mainly done through its
interaction with specific
receptors. Alpha units are recognized, responsible for
recognition of the insulin molecule and
beta units, location within the membrane, with the function of
transmitting the message to the
intracellular effectors. The receptors are degraded and
resynthesized continuously now been
identified the gene responsible for its synthesis.
The number of counter regulatory receptors are negatively by the
concentration of
insulin and its affinity is reduced by the action of other
hormones, among which
catecholamines, glucagon, growth hormone, corticosteroids,
estrogens, progesterone and
placental lactogen.
It has been established that the maximum insulin bioeffects can
be maintained even with
a concentration of 10% of recipients.
Post-receptor effects of insulin:
Although not known the exact the effects of the interaction
between insulin receptor-
transport systems and enzymes effector, is postulated as the
most likely mechanism of action
units autophosphorylation and activation of protein kinase beta,
which would have the effect of
second messenger.
The second messengers, activate and inhibit gene transcription
and action of enzymes
involved in the metabolism of substrates, induce translocation
of proteins, stimulate protein
synthesis and transport of glucose, amino acids and ions.
Thus, insulin activates glucose transport across the cell
membrane of adipose tissue and
muscle. We have identified a transporter located in the interior
of the cell called Glut 4, the
synthesis and translocation to the membrane is
insulin-dependent. The transporter Glut 4 is also
glucose-dependent, showing a negative counter-circulating
glucose levels.
Insulin increases hepatic action of stimulating glucokinase gene
transcription of the
enzyme and directly activates pyruvate dehydrogenase, acetyl CoA
carboxylase and laglicgeno
synthetase. On the other hand, directly inhibits the
intracellular lipase and phosphorylases
responsible for the mobilization of endogenous substrates.
-
8/2/2019 Insulin Definitivo
19/27
19
CHAPTER 4 - INSULIN AND DIABETES MELLITUS:
COMPARISON BETWEEN TYPE I AND TYPE II
DIABETES MELLITUS
Diabetes mellitus is a group of metabolic diseases in which a
person has problems with sugar
levels in blood because theres an insulin resistance in the
tissues or the body is partially or
completely unable to produce. According to the American Diabetes
Association, the
classification of diabetes includes four clinical classes: Type
1 Diabetes, Type 2 Diabetes, other
specific types of diabetes due to other causes and Gestational
Diabetes Mellitus.
1. Type 1 Diabetes MellitusIt is a metabolic disease in which
beta cells of Langerhans Islets in the pancreas are
destroyed and the body losses the capacity to segregate insulin,
so there is an insulin deficiency.
This diabetes is also known as IDDM (insulin dependent diabetes
mellitus) or juvenile diabetes,
because it usually appears before the age of 25 years old.
Causes and factors
The main cause seems to be an autoimmune reaction. This process
of self-destruction
starts several years before clinical features of diabetes are
diagnosed in a routine blood sugar
test. At birth, the beta cell mass is normal and then the
destruction starts to develop because of
the autoimmune process , however the effects are not noticeable
until the 80% of the beta cell
are destroyed.
This autoimmune process starts due to the pathological situation
of insulitis - an
inflammation of the islets of Langerhans of the pancreas- .
Pancreatic -cells become infiltrated
by mononuclear cells, leading to inflammation. This lymphocyte
infiltration can result in
destruction of the insulin - producing beta cells of the
pancreas without the involvement of the
glucagon-secreting cells (- cells of Islets of Langerhans) as a
result of the attack of
lymphocytes T together with macrophages. Also B lymphocytes are
involved in this process by
producing autoantibodies against -cells.
However, as collateral effects, the destruction of beta cells
can impair the activity of
cells. In turn this results in an impairment in glucagon
production. In fact, surveys involved in
the effect of the destruction of cells into cells have
demonstrated that the production of
glucagon is affected by two main things: the destruction of the
sympathetic nervous system dueto the autoimmune mechanism and
directly by the loss of beta cells, because some substances
that they produce, such as GABA, Zinc and even insulin it-self
,have inhibitory effects on
glucagon production.
Genetic factors: Most individuals with type I diabetes have the
HLA DR3 and / or the
HLA DR4 haplotype. Refinemens in genotyping of HLA loci have
shown that the haplotypes
DQA1*0301,DQB1*0302 and DQB1*0201 are associated with type I
diabetes .On the other
hand haplotypes DWA1*0102,D1B1*0602 provide protection against
type I diabetes.
Environmental factors: some viruses (such as coxsachie virus and
rubella virus), bovine
milk proteins and nitrosourea compounds could be involved in the
pathogenesis of diabetes but
this has not been proven yet.
http://en.wikipedia.org/wiki/Inflammationhttp://en.wikipedia.org/wiki/Islets_of_Langerhanshttp://en.wikipedia.org/wiki/Pancreashttp://en.wikipedia.org/wiki/Lymphocytehttp://en.wikipedia.org/wiki/Insulinhttp://en.wikipedia.org/wiki/Beta_cellhttp://en.wikipedia.org/wiki/Beta_cellhttp://en.wikipedia.org/wiki/Insulinhttp://en.wikipedia.org/wiki/Lymphocytehttp://en.wikipedia.org/wiki/Pancreashttp://en.wikipedia.org/wiki/Islets_of_Langerhanshttp://en.wikipedia.org/wiki/Inflammation
-
8/2/2019 Insulin Definitivo
20/27
20
Idiopathic diabetes type I
Diabetes type I can be idiopathic, meaning, that there isnt a
known cause. This
idiopathic diabetes is mostly present in African or Asian
people. This form of diabetes is
strongly inherited and has permanent insulinopenia (insufficient
production of insulin by the
pancreas) and it is prone to ketoacidosis without antibodies
against -cells.
As we can see, ethnical factors are also involved in diabetes
type I, which supports the
theory of genetic factor involved in the disease: in Asian and
African people the incidence of
diabetes is the lowest one and the Caucasian are the most
affected people by DMTI.
Singns and symtomes : Before DMT-I is diagnosed the
hyperglycemia situation presents
the following main effects-: polyuria with glycosuria (frequent
urination with the presence of
sugar in the urine), polydipsia ( increased thirst), polyphagia
(increased hunger), weight loss,
nausea , vomiting ,abdominal pain and tiredness.
Diagnosis: The diagnosis of DMTI in a person who presents these
symptoms includes:
Presence of immunological-involved molecules against beta cells:
islet cells antibodies(ICAs), autoantibodies against insulin
(IAAs), autoantibodies against glutamic acid
decarboxylase (GAD65) and against tyrosine phosphatases (IA-2
and IA-2). These
molecules are part of beta cells.
Hyperglycemia and low blood insulin levels: the blood sugar
under fasting condition ismore than 126 mg/dL and the aleatory
blood sugar (that means, without fasting
conditions) reaches more than 200 mg /dL.
Glycated proteins and glycated haemoglobin: the excess of sugar
causes the glycation ofdifferent proteins in the body. Glycated
haemoglobin is the most easy way to check
what level of hyperglycemia has suffered or suffers the
patient.
Most of the symptoms can lead to a diabetic ketoacidosis, which
is a dangerous situation
due to hyperglycemia that is characterized by an abundant
present of ketone bodies in the urine
and blood. This for instance, can cause abdominal pain and
hyperventilation even leading to
death if the treatment is not given in time.
Treatment: Objectives in the treatment of any kind of diabetes
are orientated to have a
good management of the disease until arriving to the most
permanent state of euglycemia
(balanced and no pathological blood sugar levels ), to avoiding
future complications (specially
micro and macrovascular complications) and to live a life as
normal as possible. The treatment
of any diabetes have three points in common: diet, exercise and
self-controlling of blood sugar
levels. When it comes to diet and self-monitoring of blood sugar
levels, treatments are different
between DMTI and DMTII.
Diet: The diabetic type I diet consists on a balanced diet, with
the correct caloric support toensure a correct growth and
development, without any lack of nutrients. The most
important issue here will be the distribution of carbohydrates
during the day. This
distribution has to be personalized and have to take into
account the number and type of
insulin injections during the day. The nutritional indications
in diabetes type II will be
discussed later.
Exercise: It helps in the maintenance of correct blood sugar
levels ( controlling thuseuglycemia) and also preventing
overweight.
-
8/2/2019 Insulin Definitivo
21/27
21
Self-monitoring of blood sugar levels: In the case of DMTI this
is the most importantmeasure because ,if there is something that
really characterize diabetes type I, is the insulin
dependence . Controls of blood sugar levels will be done with a
blood-glucose metters,
that offers an easy and fast way to have an idea of blood sugar,
with a very low margin of
error in calculation. From 3 to 6 times per day, the diabetic
patient will need to check his
blood sugar in order to adjust insulin doses.
Hypoglycemia situation
On the other side, a diabetic patient can present a hypoglycemia
situation, showing a so
low blood sugar levels (under 50 mg/dL) that can cause the
diabetic comma , leading even to
death. This hypoglycemia condition can be achieve by injecting
an extra doses of insulin, a hard
or prolonged exercise or under fasting conditions, also an
inadecuate balance between meals and
insulin injected can provoke hypoglycemia.
Hypoglycemia will be treated depending on its gravity: once the
first symtomes appear
(sweating, sickness, hunger or nausea) the patient must take
some high-sugar containing food,
as juice, sugar drinks or plain sugar. In severe hypoglycemias,
the patient can convulsionate, so
he will need an injection of glucagon hormone (it has been
discussed above the effect in
glucagon secretion in diabetes type I) very quickly. So,
glucagon is essential to revert extreme
hypoglycemia situations.
Long term consequences and effects
The bad control of glucose levels in blood has several important
effects, due mostly to
the glycation of proteins what in turn leads to general problems
such as: nerve damaging
(neuropathy), mainly in peripheral nerves; macrovascular
diseases ( the excess blood sugar canprovoke atherosclerosis, which
can lead to a bad circulation, and cerebro-vascular
problems,and
also to heart arrest); microvascular diseases (the damage in
capillaries and the increasement of
density in blood sugar can cause escapes of sugars to the
extracellular place, so black stains can
appear in the skin; vision diseases (over all retinopaties),
renal complication, feet ulceras,
sexual complications.
Future treatments and studies which are orientated to cure the
disease
Treatments are underway investigated following two different
ways:
Treatment of diabetes type I with stem cells: Nowadays, surveys
with stem cells are beingdone. The transplant of stem cells of one
patient to another one need an immunosupressor
treatment, due to the rejection typical of an exogenous protein,
so, this is a problem. But,
most recently studies use the autotransplant that is ,stem cells
from the patient- to try to
cure diabetes and the results, so far, are being positive, but a
lot of questions remain yet
under debate.
Islets Langerhans transplants: A promising alternative to
insulin injections is cellulartransplantation. In this case, the
treatment consists in harvesting beta cells from a cadaver
and in introducing them into the blood stream of the patient.
However, this also needs an
immunosupressory treatment because of the rejection and to the
attack of the immunitary
system to the new beta cells, which , in the long-term, are
destroyed again.
-
8/2/2019 Insulin Definitivo
22/27
22
2. Type 2 Diabetes Mellitus2.1.Background.
Diabetes Mellitus: Diabetes Mellitus (DM) represents a
heterogeneous collection of
metabolic diseases of very different etiopathogenesis,
characterized by the common featureof chronic hyperglycemia, there
being two basic physio-pathological disorders underlying
any etiologic type of DM: 1- a defect in insulin secretion, 2- a
defective insulin action or
both, either one predominating at a given time.
Endoplasmic Reticulum (ER) Stress:Many disturbances of the cell
homeostasis cause
accumulation of unfolded-misfolded proteins in the ER,
triggering an evolutionarily
conserved response, termed the unfolded protein response (UPR).
The initial intent of the
UPR is to adapt to the changing environment, and reestablish
normal ER function. These
adaptive mechanisms enhance the protein folding capacity of the
ER, and promote ER-
associated protein degradation to remove misfolded proteins.
Excessive and prolonged ER
stress triggers apoptosis.
Insulin resistance (IR) is defined as the decreased tissue
response to insulin-mediated
cellular actions and is the inverse of insulin sensitivity. The
term insulin resistance, as
generally applied, refers to whole-body reduced glucose uptake
in response to physiological
insulin levels and its consequent effects on glucose and insulin
metabolism.
The most accepted hypothesis for insulin resistance is that it
develops as a consequence
of the effects of inflammatory and hormonal factors, ER stress,
and the accumulation of by-
products of nutritional overload on insuling-sensing tissues,
such as adipocytes, hepatocytes,
skeletal muscle and pancreatic -cells.
Deposition of amyloid is the single most typical islet
alteration in type 2 diabetes, where
almost all of the islets are converted to amyloid. The amyloid
formed may cause -cell
apoptosis and dysfunction of remaining cells.
2.2. What is type II diabetes mellitus (dmII)?:Type II diabetes
mellitus is classified by the WHO under Endocrine, nutritional
and
metabolic diseases category. Its code is ICD-10 E11. According
to the American Diabetes
Association, Type II Diabetes Mellitus (DMII) is one the 4
clinical presentations of diabetes.
Formerly called adult-onset or non-insulin-dependent diabetes,
is the most commonform of diabetes. It is a complex, polygenic
disease characterized by both hyperinsulinemia
and hyperglycemia, at least early in its pathogenesis.
Therefore, the term type II diabetes
Mellitus designates not a single disease, but a heterogeneous
collection of hyperglycemic
syndromes phenotipically and genotypically different.
It is thought to be the result of an imbalance between insulin
sensitivity and secretion,
with failure of pancreatic -cells to compensate for the
increased insulin requirement created
by IR leading to hyperglycemia.
-
8/2/2019 Insulin Definitivo
23/27
23
2.3. SymptomsOften, people with DMII have no symptoms at
firsteven for years. The early
symptoms of diabetes may include: bladder, kidney, skin, or
other infections that are more
frequent or heal slowly; fatigue; hunger; increased thirst;
increased urination. The first
symptom may also be: blurred vision; erectile dysfunction; pain
or numbness in the feet orhands.
2.4. PrevalenceDMII has already reached epidemic proportions,
affecting over 200 million people
worldwide, being its prevalence of 6% in most developed
countries.
2.5.Risk factors: gene-enviroment interactions predisposing to
dmIIDMII is strongly influenced by inheritance. Unlike type I
diabetes, where a large
component of heritability is found within a single locus (the
HLA region), the heritability of
DMII appears to be composed of many variants, each of modest
impact on disease.
It appears that IR and secretory deficiencies are necessary, but
not sufficient to reach the
levels of hyperglycemia that yield a clinical diagnosis. On the
other hand, there is
overwhelming evidence for the influence of genetic factors
combined with a permissive
environmental setting that determines risk of development of
DMII.
Clearly, epigenetics play a role in insulin resistance and in
turn in DMII development as
can be appreciated, for instance, by the fact that 80% of those
with DMII reach a Body Mass
Index (BMI)>30 Kg/m2. Moreover, people with BMI>35
Kg/m
2(morbid obesity) have 100-
fold greater risk for developing DMII than those with BMI
-
8/2/2019 Insulin Definitivo
24/27
24
IR and PD usually have no symptoms. People with a severe form of
IR may show
acanthosis nigricans (Dark patches of skin, usually on the back
of the neck, but sometimes
on other possible sites). Other typical signs of IR syndromes
include hyperinsulemia or
polycystic ovary syndrome.
Two physiopathological defects underlie DMII: defective -cell
function and insulinresistance. Therefore, pathophysiologically
DMII may range from predominantly IR with
relative insulin deficiency, to predominantly an insulin
secretory defect with IR.
In DMII, islets of Langerhans dont show autoimmune destructive
changes as in type I
Diabetes (DMI), although amyloid deposits are frequently found
in the islets.
Natural history of DMII is variable resulting from long duration
of silent
hyperglycemia, often clinically reveled by symptoms and signs of
specific macrovascular
(e.g .stroke) and/or microvascular complications such as renal
disease, retinopathy or
obesity, among others.
Ketoacidosis of acute onset as a complication of trauma, surgery
or infection is rare
compared to its frequent incidence in DMI, being more frequent
in particular clinical
phenotypes of keto-prone DMIIparticulary in Afro-Americans.
The cornerstone of DM diagnosis is the unequivocal demonstration
of plasma glucose levels
higher than those accepted as normal. In the absence of
unequivocal hyperglycemia
diagnosis must be confirmed on a later date by any of the
following three methods:
1. Fasting Plasma Glucose (FPG)>=126 mg/dl Fasting defined as
no caloric intakefor at least 8 hours.
2. Symptoms of hyperglycemia and a casual plasma glucose>=200
mg/dlCasual isdefined as any time of day without regard to time
since last meal. The classic
symptoms of hyperglycemia include polyria, polydipsia and weight
loss.
3. 2-h plasma glucose >= 200 mg/dl during an Oral Glucose
Tolerance Test (OGTT):This test measures blood glucose after people
fast for at least 8 hours and 2 hours
after they drink a sweet liquid provided by a doctor or
laboratory.
A blood glucose level between 140 and 199 mg/dL means glucose
tolerance is notnormal but is not high enough for a diagnosis of
diabetes.
Hemoglobin A1C measurement (A1C) or glycated hemoglobin is a
form of hemoglobin
that is measured primarily to identify the average plasma
glucose concentration over
prolonged periods of time. It is routinely used as a tool for a
metabolic control of DM,
although its utility in the diagnosis has been a matter of
debate for a long time. The cut-off
point accepted for the diagnosis of DM is set at an A1C value of
6.5%.
2.7. TreatmentThe primary goals of hyperglycemic management
should be different depending on
whether the patient has primarily -cell deficiency (AKA
insulin-sensitive DMII), or
whether the patient has IR leading to -cell insufficiency (AKA
insulin-resistant variant of
DMII).
-
8/2/2019 Insulin Definitivo
25/27
25
In the case of insulin-sensitive DMII, the treatment of choice
is drugs which stimulate
insulin secretion. If these patients have severe -cell
deficiency, they may need insulin
replacement therapy.
The insulin-resistant variant of DMII is the most common type of
DMII in Western
societiesdirectly related with the increase in ovesity. The
initial approach to regulating theplasma glucose is to implement
life-style changes with dietary intervention and increased
physical activity. The objective is to maintain A1C
-
8/2/2019 Insulin Definitivo
26/27
26
REFERENCES
1. Catlogo de Medicamentos (2009). Consejo General de Colegios
Oficiales deFarmacuticos.
2. Bolli GB, et al. (2009). Comparison of a multiple daily
insulin injection regimen (basalonce-daily glargine plus mealtime
lispro) and continuous subcutaneous insulin infusion
(lispro) in type 1 diabetes. Diabetes Care, 32(7): 11701176.
3. Types of insulin. National Institute of Diabetes and
Digestive and Kidney Diseases.. Accessed Aug.
20, 2010.
4. Insulin basics. American Diabetes Association. Accessed Aug.
20,
2010.
5. Types of insulin. American Diabetes Association. . Accessed
Aug. 20,2010.
6. Diabetes Control and Complications Trial/Epidemiology of
Diabetes Interventions andComplications Study Research
Group.Intensive diabetes treatment and cardiovascular
disease in patients with type 1 diabetes . 2005, New England
Journal of Medicine,
353(25): 26432653.
7. Adams, M. J., T. Blundell, E. Dodson, G. Dodson, M. Vijayan,
E. Baker, M. Harding,B. Rimmer and S. Sheat. "Structure of
Rhombohedral 2-zinc Insulin Crystals." Nature
224: 491 (1969).
8. Bentley, G., E. Dodson, G. Dodson, D. Hodgkin and D. Mercola
. "Structure of insulinin 4-zinc insulin." Nature 261(5556): 166-8
(1976).
9. Berson, S. A. and R. S. Yallow. "Immunochemical distinction
between insulins withidentical amino-acid sequences." Nauchni Tr
Vissh Med Inst Sofiia 191: 1392-3
(1961).
10.Chang, X., A. M. Jorgensen, P. Bardrum and J. J. Led .
"Solution structures of the R6human insulin hexamer." Biochemistry
36(31): 9409-22 (1997).
11.Derewenda, U., Z. Derewenda, E. J. Dodson, G. G. Dodson, C.
D. Reynolds, G. D.Smith, C. Sparks and D. Swenson. "Phenol
stabilizes more helix in a new symmetrical
zinc insulin hexamer." Nature 338(6216): 594-6 (1989).
12.Mirmira, R. G., S. H. Nakagawa and H. S. Tager. "Importance
of the character andconfiguration of residues B24, B25, and B26 in
insulin-receptor interactions." J Biol
Chem 266(3): 1428-36 (1991).
13.Sanger, F. "Sequences, sequences, and sequences." Annu Rev
Biochem 57: 1-28(1988).
14.Schaffer, L. "A model for insulin binding to the insulin
receptor." Eur J Biochem221(3): 1127-32 (1994).
15.Steiner, D. F. and D. E. James. "Cellular and molecular
biology of the beta cell."Diabetologia 35 Suppl 2: S41-8
(1992).
16.Yip, C. C. and P. Ottensmeyer. "Three-dimensional structural
interactions of insulinand its receptor." J Biol Chem 278(30):
27329-32 (2003).
17.Rayner Rodriguez-Diaz, Robin Dando, Mcaroline Jacques-Silva,
Alberto Fachado,Judith Molina, Midhat H Abdulreda, Camilo Ricordi,
Stephen D Roper, Per-OlofBerggren and Alejandro Caicedo. Alpha
cells secrete acetylcholine as a non-neuronal
-
8/2/2019 Insulin Definitivo
27/27
paracrine signal priming beta cell function in humans. NATURE
MEDICINE, 17, 888-
892 (2011).
18. Tae Niwa, Yoshihisa Matsukawa, Takao Senda, Yuji Nimura,
Hiroyoshi Hidaka, andIchiro Niki. Intracellular movement of
secretory granules is a proximal stage in the
secretory cascade that ends in the release product from cells. D
i a b e t e s 47:1699
1706, 199819..
20.Sakurada M, Kanatsuka A, Saitoh T, Makino H, Yamamura K,
Miyazaki J, Kikuchi M,Yoshida S.Relation between glucose-stimulated
insulin secretion and intracellular
calcium accumulation studied with a superfusion system of a
glucose-responsive
pancreatic beta-cell line MIN6. Division of Endocrinology and
Metabolism, Institute
for Adult Diseases, Asahi Life Foundation, Tokyo, Japan.
Endocrinology. 1993
Jun;132(6):2659-65.
21.22.BD diabetes official web page: 23.Consenso en el
diagnstico y tratamiento de la diabetes tipo I del nio y del
adolescente:
24., ,
25.Laboratory investigation for diabetes mellitus: practical
concerns. The open diabetesJournal,2009, 3, 32-34.
26.Stem cells promising for Type 1 diabetes.27.Diabetes Research
Institute: Stem cells and diabetes.28. Gerald J.Taborsky Jr., Ph.D.
The physiology of glucagon. Journal of Diabetes Science
and technology. November 2010, Volume 4, Issue 6.29.Manuel
Serrano Ros, Jos A. Gutirrez Fuentes. Type 2 Diabetes Mellitus.
2010
Elsevier Espaa, S.L. ISBN: 978-84-8086-683-5.
30.Chunyan Xu, Beatrice Bailly-Maitre, and John C. Reed. J.
Clin.Endoplasmic reticulumstress: cell life and death decisions.
Invest. 115:26562664 (2005).
31.Claire Levy-Marchal et al. InsulinResistance in Children:
Consensus, Perspective, andFuture Directions.J Clin Endocrinol
Metab. 2010 December; 95(12): 51895198.
32.Amyloid in the islets of Langerhans: Thoughts and some
historical aspects. PerWestermark. Upsala Journal of Medical
Sciences. 2011; 116: 8189.
33.National Diabetes Information: Clearinghouse (NDIC).National
Institute of Diabetesand Digestive and Kidney Diseases (NIDDK),
National Institutes of Health (NIH).
34.MedlinePlus.service of the U.S. National Library of Medicine.
From the NationalInstitutes of Health National Institutes of
Health
35.DeFronzo RA, Tobin JD, Andres R. Glucose clamp technique: a
method for quantifyinginsulin secretion and resistance. Am J
Physiol. 1979 Sep;237(3):E214-23.
http://www.uptodate.com/contents/insulin-secretion-and-pancreatic-beta-cell-functionhttp://www.uptodate.com/contents/insulin-secretion-and-pancreatic-beta-cell-functionhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Sakurada%20M%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Sakurada%20M%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Kanatsuka%20A%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Saitoh%20T%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Makino%20H%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Yamamura%20K%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Miyazaki%20J%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Kikuchi%20M%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Yoshida%20S%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed/8504766?dopt=Abstracthttp://www.vivo.colostate.edu/hbooks/pathphys/endocrine/pancreas/%20insulin.htmlhttp://www.bd.com/http://www.scielo.cl/pdf/rcp/v78n5/art12.pdfhttp://en.wikipedia.org/wiki/Diabetic_ketoacidosishttp://en.wikipedia.org/%20wiki/Diabetes_mellitus_type_1http://en.wikipedia.org/%20wiki/Diabetes_mellitus_type_1http://en.wikipedia.org/wiki/%20Gestational_%20diabeteshttp://www.webmd.com/http://www.webmd.com/http://en.wikipedia.org/wiki/%20Gestational_%20diabeteshttp://en.wikipedia.org/%20wiki/Diabetes_mellitus_type_1http://en.wikipedia.org/%20wiki/Diabetes_mellitus_type_1http://en.wikipedia.org/wiki/Diabetic_ketoacidosishttp://www.scielo.cl/pdf/rcp/v78n5/art12.pdfhttp://www.bd.com/http://www.vivo.colostate.edu/hbooks/pathphys/endocrine/pancreas/%20insulin.htmlhttp://www.ncbi.nlm.nih.gov/pubmed/8504766?dopt=Abstracthttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Yoshida%20S%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Kikuchi%20M%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Miyazaki%20J%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Yamamura%20K%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Makino%20H%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Saitoh%20T%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Kanatsuka%20A%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Sakurada%20M%22%5BAuthor%5Dhttp://www.uptodate.com/contents/insulin-secretion-and-pancreatic-beta-cell-functionhttp://www.uptodate.com/contents/insulin-secretion-and-pancreatic-beta-cell-function