Embed Size (px)
Citation preview

P a g e 1 | 32
xxxx
Infant Mortality Research Partnership
Application Due Date: April 14, 2016, 5:00 PM (EDST)
Application Release Date: March 14, 2016
Request for Applications Primary Contact: Ohio Colleges of Medicine Government Resource Center Allison Lorenz, MPA Program Director Email: [email protected]
P a g e 2 | 32
Executive Summary On behalf of the Governor’s Office of Health Transformation (OHT), and the Ohio Departments of Medicaid (ODM), Health (ODH) and Higher Education (ODHE), the Ohio Colleges of Medicine Government Resource Center (GRC) is requesting applications from qualified investigators through the Infant Mortality (IM) Research Partnership to identify interventions and resources needed to improve health outcomes for underserved populations and address the complicated health issue of infant mortality from a systems perspective. The IM Research Partnership seeks to fund multiple research projects in areas including but not limited to: systems dynamics modeling of the impact of the following efforts on infant mortality: improved access to care, safe sleep, and impact of progesterone; predictive modeling for infant mortality; spatial GIS modeling for identifying high-risk communities; and evaluation of the impact of OIMRI home visiting programs. The IM Research Partnership seeks to provide up to $2,453,884 million dollars to fund multiple research projects. This opportunity will support, at minimum, 5 projects ranging from $250,000 to $627,000 over a 14-month period. Vendors must submit separate applications for each research project as identified in the Scope of Work, Tasks 1 through 5, as defined on pages 4 through 11 of this RFA. Technical Assistance Questions regarding this Request for Applications may be emailed to Allison Lorenz at: [email protected]. Questions will be accepted until March 28, 2016 at 12:00 PM Noon EDST A copy of this Request for Applications and all questions and answers posed by potential vendors will be posted at: http://grc.osu.edu/currentfunding/

P a g e 3 | 32
Table of Contents Page Number
I. METAPP Overview ………………………………………………………………………………………………….4
II. Infant Mortality Research Partnership Overview …………………………………………………...4
III. Scope of Work ………………………………………………………………………………………………………..4 - 11
IV. Deliverables ………………………………………………………………………………………………………….11 - 12
V. Roles and Responsibilities …………………………………………………………………………………….13
VI. Project Governance ………………………………………………………………………………………………13 - 14
VII. Project Budget ………………………………………………………………………………………………………14
VIII. Eligible Vendors …………………………………………………………………………………………………….15
IX. RFA Response Requirements …………………………………………………………………………………15
X. RFA Response Requirement Checklist ……………………………………………………………………15 - 21
XI. Application Review ……..…………………………………………………………………………………………21 - 22
XII. RFA Terms and Conditions …………………………………………………………………………………….22 - 23
XIII. Data Use and Management …………………………………………………………………………………..23 - 24
XIV. Presentation, Publications and Dissemination ……………………………………………………….24 - 25
XV. Appendices ……………………………………………………………………………………………………………26 - 32 a. MEDTAPP Project Progress Report ………………………………………………………………….26 b. Past Project Performance Report ……………………………………………………………………27 c. Gantt Chart of Activities and Timeline
i. Tasks 1 through 5 ……………………………………………………………………………….28 ii. Task 5 …………………………………………………………………………………………………29
d. Project Budget Form ……………………………………………………………………………………….30 e. The Ohio State University Standard Terms and Conditions ……………………………..31 f. Medicaid Data Use Agreement ……………………………….………………………………………32
P a g e 4 | 32
MEDTAPP Overview Section 1903(a) of the Social Security Act allows the federal government to participate financially in state Medicaid programs in such amounts "found necessary by the Secretary for the proper and efficient administration of the State (Medicaid) plan." The Medicaid Technical Assistance and Policy Program (MEDTAPP) is a Medicaid and university research partnership aimed at supporting the efficient and effective administration of the Medicaid program. GRC manages MEDTAPP for ODM, under which the IM Research Partnership Request for Applications (RFA) is sponsored. Infant Mortality Research Partnership Overview Ohio ranks 45th in the nation for infant mortality, with a rate of 7.33 deaths per 1,000 live births in 2013. While Ohio’s rate has declined by 10.3% since 2005, the decline has not kept pace with the decline for the nation (13.1%), and at least 20 states have experienced declines in excess of 15%. Infant mortality impacts Ohio families differently and is greatly influenced by race and location. Black babies are more likely to die within the first year of life even when social and economic factors are considered. Metropolitan and Appalachian counties also have higher rates of infant mortality compared to the state as a whole. Governor Kasich made reducing infant mortality a priority in his first State of the State, and launched numerous significant reforms. In June 2015, Governor Kasich signed the state’s two-year budget (HB 64), which included additional reforms that focus resources where the need is greatest. Specifically, the budget provided $1M per year to ODHE to advance collaborative research at institutions of higher education designed to: identify interventions and resources to improve health outcomes for underserved populations; and to address this complicated health issue from a systems perspective. To assist ODM with the efficient and effective administration of the Medicaid program, and at the request of OHT, ODM, ODH, and ODHE, the Ohio Colleges of Medicine Government Resource Center (GRC) will implement the Infant Mortality (IM) Research Partnership. Scope of Work MEDTAPP related Scope of Work The vendors procured through this RFA will undertake activities as defined and directed by ODM, ODH, and ODHE, and agreed to by GRC to support the efficient and effective administration of the Medicaid program. Vendors must submit separate applications for each scope of work task discussed below. Single applications that address multiple Scope of Work Tasks will be ineligible for consideration. Specifically, selected vendors will complete the activities for which they apply and are selected related to the MEDTAPP directed and supported IM Research Partnership project as described below. Note that the research and associated deliverables in this RFA must be actionable across the state health and human services enterprise (e.g. ODH, ODM, ODMHAS) to improve maternal and child health and reduce Ohio’s rate of infant mortality.
P a g e 5 | 32
Task 1: Examine and identify infant mortality solutions from a systems perspective in order to address the complexity and uniqueness of Ohio’s infant mortality problem. Develop a modeling approach, by sub-populations and regions, that evaluates and presents, in a logical and robust fashion, the contributions, potential consequences, and impact on Ohio’s rate of infant mortality for the following interventions:
1. Safe sleep (see existing quality improvement initiatives for hospitals, physicians and
Ohio AAP presentation). 2. Improved access to care (see some existing measures of access to care in WRA Data
Codebook). 3. Progesterone (see some existing measures of progesterone risk factors, access to care,
and access to Medicaid in WRA Data Codebook, and information on existing OPQC Progesterone Quality Improvement Project).
4. Any additional interventions identified by the project sponsors. The modeling process shall include key informant interviews, information gathering sessions, and consultation with policy, programmatic, and clinical subject matter experts on these topics to gain a comprehensive whole system perspective on the relationship between these interventions and infant mortality. Deliverables for Task 1 include:
1. A project plan that includes the following information: a. Approach to engaging subject matter experts to gain a comprehensive whole
system perspective on the relationship between interventions and infant mortality; b. Modeling approach proposed; c. Types of factors that the vendor intends to extract from given raw data for
modeling; d. New data sources and attributes that the vendor intends to use for modeling infant
mortality; and e. Challenges foreseen and how the team intends to overcome the challenges.
2. A data dictionary, including attributes, used in the data set. 3. A Modeling Report explaining the following:
a. Results of subject matter expert input to model description; b. Model description; c. Methodology and process undertaken to solve the objective; d. Validation and explanation of feature engineering/selection; e. Variable importance of all attributes used in prediction and indication of top
attributes/indicators that are key predictors along with an explanation of how the attributes may indicate a higher risk.
4. Fully commented Modeling Code along with a structured data set used as input for the model.
5. A final data set at the conclusion of Task 1.
P a g e 6 | 32
The following activities apply to selected vendors across Scope of Work Tasks 1 through 3 and should be reflected in the submitted application for Task 1:
1. Work with technical and subject matter experts at ODH, ODM and GRC to establish common data and variables definitions and to develop a comprehensive data dictionary for all infant mortality related work.
2. Incorporate existing and vendor recommended data on social, environmental and other determinants of health applicable to Medicaid and underserved populations.
3. Incorporate linked Vital Statistics birth and death data, and Medicaid claims data along with other applicable data sources as appropriate from the past 7 state fiscal years.
4. Recommend a range of possible interventions, including appropriate applied statistical certainties, that would improve outcomes for pregnant women and infants at highest risk of infant mortality among Medicaid and underserved populations.
5. Collaborate with GRC, other vendors and state sponsors across Tasks 1 through 4 to fully research infant mortality and incorporate findings from the respective models into the resulting data display system described in Task 4. GRC and the Task 4 vendor will facilitate the collaboration and project work will be conducted using applied practical methods on an iterative basis until the data display system is complete to the satisfaction of state sponsors.
6. Recommend software, analysis and data visualization techniques, in collaboration with GRC and the selected vendor for Task 4, to be incorporated into the state data display system. The resulting outputs from recommended software, analysis and data visualization techniques must be able to be incorporated into the data display system.
7. Provide technical assistance to ODM, ODH and other health and human services agencies’ staff for monitoring trends in infant mortality and related birth outcomes, risk factors (including social determinants of health), access to care, and service capacity in the identified infant mortality hotspots for the Medicaid health care delivery systems.
8. Produce a final report describing the research objective, methods, results (including maps), interpretation (technical and in lay language), limitations, and discussion of analyses that will become a chapter of the final report submitted to the state sponsors under Scope of Work Task 4. The Task 4 vendor will provide guidance on the format and structure of this report to ensure consistency across the Task 1-3 reports.
Task 2: Develop predictive models to identify pregnant women and babies, among Ohio Medicaid recipients and underserved populations, who are at a higher risk of infant death during the first year of life among Ohio Medicaid recipients and underserved populations.
1. Separate models predictive of neonatal death, post neonatal death, and pre-term birth related causes of death should be developed as data support.
2. Models should incorporate the ability to predict outcomes from time relative periods (multi-level factors + Individual Factors (1st- 3rd trimester, neonatal, etc.))
Deliverables for Task 2 include:
1. A project plan with the following information:
P a g e 7 | 32
a. Modeling approach proposed; b. Types of factors that the vendor intends to extract from given raw data for
modeling; c. New data sources and attributes that the vendor intends to use for modeling infant
mortality; and d. Challenges foreseen and how the team intends to overcome the challenges.
2. A data dictionary, including attributes, used in the data set. 3. A Modeling Report explaining the following:
a. Methodology and process undertaken to solve the objective; b. Validation and explanation of feature engineering/selection; c. Variable importance of all attributes used in prediction and indication of top
attributes/indicators that are key predictors along with an explanation of how the attributes may indicate a higher risk.
4. Fully commented Modeling Code along with a structured data set used as input for the model.
5. Provide a final data set at the conclusion of Task 2. The following activities apply to selected vendors across Scope of Work Tasks 1 through 3 and should incorporate the ability be reflected in the submitted application for Task 2:
1. Work with technical and subject matter experts at ODH, ODM and GRC to establish common data and variables definitions and to develop a comprehensive data dictionary for all infant mortality related work.
2. Incorporate existing and vendor recommended data on social, environmental and other determinants of health applicable to Medicaid and underserved populations.
3. Incorporate linked Vital Statistics birth and death data, and Medicaid claims data along with other applicable data sources as appropriate from the past 7 state fiscal years.
4. Recommend a range of possible interventions, including appropriate applied statistical certainties, that would improve outcomes from time relative periods (multi-level for pregnant women and infants at highest risk of infant mortality among Medicaid and underserved populations.
5. Collaborate with GRC, other vendors and state sponsors across Tasks 1 through 4 to fully research infant mortality and incorporate findings and the respective models into the resulting data display system described in Task 4. GRC and the Task 4 vendor will facilitate the collaboration and project work will be conducted using applied practical methods on an iterative basis until the data display system is complete to the satisfaction of state sponsors.
6. Recommend software, analysis and data visualization techniques, in collaboration with GRC and the selected vendor for Task 4, to be incorporated into the state data display system. The resulting outputs from recommended software, analysis and data visualization techniques must be able to be incorporated into the data display system.
7. Provide technical assistance to ODM, ODH and other health and human services agencies’ staff for monitoring trends in infant mortality and related birth outcomes, risk factors + Individual Factors (1st- 3rd trimester, neonatal, etc.) (including social determinants of
P a g e 8 | 32
health), access to care, and service capacity in the identified infant mortality hotspots for the Medicaid health care delivery systems.
8. Produce a final report describing the research objective, methods, results (including maps), interpretation (technical and in lay language), limitations, and discussion of analyses that will become a chapter of the final report submitted to the state sponsors under Scope of Work Task 4. The Task 4 vendor will provide guidance on the format and structure of this report to ensure consistency across the Task 1-3 reports.
Task 3: Develop and apply spatial method(s) to identify Ohio communities with the highest infant mortality experience among Medicaid and underserved populations that includes, but is not limited to, identification of social determinants of health, factors that impact birth outcomes, metrics of access to care, and healthcare service gaps and needs.
1. Recommend and apply spatial method(s) to be used across the state health and human services enterprise (e.g. ODH, ODM, ODMHAS) to identify Ohio communities with the highest infant mortality rates that includes, but is not limited to: social determinants of health; factors that impact birth outcomes; and access and service needs among Medicaid and underserved populations or regions. Apply spatial methods to identify patterns of maternal, infant and child health outcomes among these populations or regions in Ohio.
2. Under direction from GRC, ODM and ODH, establish cohorts of Medicaid and non-Medicaid sub-populations and geographic units for benchmarking and comparisons.
3. State-wide, identify by relevant geographic units those populations at risk of experiencing infant mortality.
4. Conduct a spatial analysis across the relevant geographic units to evaluate the prevalence of specific areas of risk, access, service gaps, and outcomes, inclusive of but not limited to:
a. Disparities; b. Preterm births; c. Low birth weight babies; d. Core HEDIS measures, including timeliness of prenatal care and postpartum visits; e. Poverty; f. Low or no educational attainment; g. Access to care, progesterone, long-acting reversible contraceptives (LARCs), and
other as determined by the research findings; h. Provider or health service capacity (by specialty, e.g., licensure); i. Social determinants including but not limited to housing, transportation, racism,
pollution, stress, education, etc.; and j. Birth outcomes to include infant mortality, prematurity, low birth weight, and
disparities. 5. Identify the best models to use for monitoring temporal trends in defined high-risk areas,
service gaps and needs. 6. Set up a system for monitoring indicators (of risk factors and of birth outcomes) by
geography over time. This system should be of use to multiple state agencies for timely evaluation and planning.
7. Provide technical assistance to ODM, ODH and other health and human services agencies’ staff for monitoring spatio-temporal trends in infant mortality and related birth outcomes,
P a g e 9 | 32
risk factor (including social determinants of health), access, and service capacity in the identified infant mortality hotspots for the Medicaid health care delivery systems.
The following activities apply to selected vendors across Scope of Work Tasks 1 through 3 and should incorporate the ability be reflected in the submitted application for Task 3:
1. Work with technical and subject matter experts at ODH, ODM and GRC to establish common data and variables definitions and to develop a comprehensive data dictionary for all infant mortality related work.
2. Incorporate existing and vendor recommended data on social, environmental and other determinants of health applicable to Medicaid and underserved populations.
3. Incorporate linked Vital Statistics birth and death data, and Medicaid claims data along with other applicable data sources as appropriate from the past 7 state fiscal years.
4. Recommend a range of possible interventions, including appropriate applied statistical certainties, that would improve outcomes from time relative periods (multi-level for pregnant women and infants at highest risk of infant mortality among Medicaid and underserved populations.
5. Collaborate with GRC, other vendors and state sponsors across Tasks 1 through 4 to fully research infant mortality and incorporate findings and the respective models into the resulting data display system described in Task 4. GRC and the Task 4 vendor will facilitate the collaboration and project work will be conducted using applied practical methods on an iterative basis until the data display system is complete to the satisfaction of state sponsors.
6. Recommend software, analysis and data visualization techniques, in collaboration with GRC and the selected vendor for Task 4, to be incorporated into the state data display system. The resulting outputs from recommended software, analysis and data visualization techniques must be able to be incorporated into the data display system.
7. Provide technical assistance to ODM, ODH and other health and human services agencies’ staff for monitoring trends in infant mortality and related birth outcomes, risk factors + Individual Factors (1st- 3rd trimester, neonatal, etc.) (including social determinants of health), access to care, and service capacity in the identified infant mortality hotspots for the Medicaid health care delivery systems.
8. Produce a final report describing the research objective, methods, results (including maps), interpretation (technical and in lay language), limitations, and discussion of analyses that will become a chapter of the final report submitted to the state sponsors under Scope of Work Task 4. The Task 4 vendor will provide guidance on the format and structure of this report to ensure consistency across the Task 1-3 reports.
Task 4: Under the direction of GRC, the selected vendor will provide general coordination and facilitation for the IM Research Partnership to ensure that the work products from Tasks 1 through 3 are consolidated into a comprehensive product for the project sponsors. While the overall responsibility for this task lies with the IM Research Partnership Advisory Committee (as described in the Project Governance Section of this RFA), the successful applicant will be required to perform the following subtasks:
P a g e 10 | 32
Subtask 1: In consultation with GRC, create a Functional Specification of an interactive data display system that OHT, ODM and ODH will use to further advance IM Research Partnership goals. The Task 4 Selected Vendor will synthesize insights from Tasks 1, 2 and 3, feedback from the system’s anticipated users at OHT, ODM, ODH and subject matter expertise to describe in detail the externally-visible features and behavior of the system. This specification, which GRC will use as the detailed guide for implementing such a system, will include but is not limited to the following:
1. Detailed descriptions of the system’s features; 2. Detailed descriptions of the system’s user interfaces; 3. Detailed descriptions of the content and format of system outputs; 4. The system’s data requirements; 5. The system’s functional requirements; 6. Use cases indicating the system’s usefulness to the typical end-user; and 7. ‘User stories’ explaining how a typical user will interact and make use of the system.
The system to be described will, at minimum:
1. Be pre-parameterized with results from Tasks 1, 2 and 3; 2. Incorporate models contributed by Tasks 1, 2 and 3; 3. Allow users to manipulate parameters in the user interface in order to create and compare
alternate scenarios; 4. Allow users to use interfaces to view results and manipulate parameters at multiple levels
of analysis; 5. Generate outputs in a variety of formats, including but not limited to graphical, tabular and
geographical; 6. Allow incorporation of new data as it becomes available; and 7. Be extensible via an application programming interface (API).
Subtask 2: Chair the IM Research Partnership Advisory Committee efforts to:
1. Coordinate work between projects. 2. Prepare consolidated reports on progress of IM Research Partnership Scope of Work Tasks
including the following deliverables: a. Provide progress reports (in accordance with Deliverables, Section A as found on
page 11 of this RFA), with discussion as appropriate. b. Submit a draft summary report 5 weeks prior to the final report. c. Submit final report.
Subtask 3: Produce a comprehensive final report incorporating the reports from Tasks 1 through 3. This will include but will not be limited to, writing on overall introduction and discussion that synthesizes the findings from Tasks 1 through 3. Subtask 4: Assemble the final presentation in collaboration with and incorporating presentation materials from the vendors for Tasks 1 through 3.
P a g e 11 | 32
Additional detail to be developed after award of all Scope of Work Tasks may result in additional subtasks. Non-MEDTAPP Related Scope of Work A vendor procured through this RFA will undertake activities defined and directed by ODH and agreed to by GRC to evaluate the effectiveness of the Ohio Infant Mortality Reduction Initiative (OIMRI) home visiting program on birth outcomes. Task 5: The vendor will complete the following activities related to the OIMRI home visiting program:
• Conduct a retrospective process and outcome evaluation for OIMRI that addresses social determinants of health, outreach and engagement of high risk populations, access, utilization of health services (including specific referral sources), quality of care, health outcomes, and disparities.
• Produce a program logic model and evaluation questions. • Develop an analysis plan that uses OIMRI participant data linked to VS birth records; a non-
intervention cohort methodology is preferred, utilizing an existing VS/Medicaid claims linkage, and other data developed as a part of the Infant Mortality Research Partnership.
o Work with technical and subject matter experts at ODH, ODM and GRC to establish common data and variable definitions and to develop a comprehensive data dictionary for all infant mortality related work.
o Incorporate existing and vendor recommended data on social, environmental and other determinants of health applicable to Medicaid and underserved populations.
• Develop data collection and analysis plan for qualitative data as appropriate. • Develop an evaluation report and program recommendations. • Develop an ongoing reporting structure that includes timely performance feedback
mechanism(s). Deliverables
A. The selected vendors will submit reports (quarterly for Tasks 1 through 4 and monthly for
Task 5) to GRC detailing work activities with a focus on key accomplishments. GRC will review, reject or approve and compile approved reports and submit to ODM and/or ODH. The reports will provide detailed information on the status on each of the action items. The status of each item in the scope of work and each deliverable will be coded as P=Progress, NP= No Progress, and C= Completed in the report. A detailed description must accompany each code for each reported action item and deliverable. In the first report, the vendor will also identify a target date that the action item and/or deliverable being reported on will be completed. Once the action item and/or deliverable are completed, the subcontractor will report on the end date. If the target completion date is not met, the vendor will be required to submit an explanation in writing as an attachment to the report. This written explanation will include the following components: a) reason why the target

P a g e 12 | 32
completion date was not met, b) identified next steps for completing the action item and/or deliverable, and c) new target completion date. Please see Appendix A for an example of the format of the report.
B. The selected vendors will submit invoices to GRC according to the guidelines provided by the Ohio State University Office of Sponsored Programs (OSP). The invoices will be submitted in hard copy to OSP and in electronic format to the GRC Finance.
C. The selected vendors will submit a draft of the research design and implementation
process, including research questions, by June 30, 2016, and a final version of the research design and implementation process by September 1, 2016.
D. The selected vendors will submit a finalized list of variables required for each research
dataset at least 6-weeks in advance of requiring the dataset.
E. The selected vendors will complete an interim report of the progress of the awarded IM Research Partnership research task by December 31, 2016.
F. The selected vendors will participate in, at minimum, bi-weekly meetings via conference
call with GRC to discuss project development and progress.
G. As needed, the selected vendors will participate in meetings via conference call with ODM, ODH, GRC, and project sponsors as needed to discuss project development and progress.
H. The principal investigators of selected vendors will participate as members of the IM
Research Partnership Advisory Committee. The vendors will collaborate with each other and with other university experts by sharing best practices in research methods, spatial analytics, population and health care analytics. The vendors will collaborate with each other, GRC, and the state sponsors in creating common data and variable definitions and a data dictionary for all work.
I. The selected vendors will submit a final report prior to the close of State Fiscal Year 2017
(June 30, 2017). The report will summarize findings of the studies, with data presented in both tabular and graphical form. The report will be written for a general audience and include limited technical terminology. Technical information will be included in an appendix.
J. Selected vendors will be required to give in-person final presentation via webinar in
Columbus, to be scheduled in June 2017. The GRC will host the webinar in Columbus, and travel expenses for this one-day webinar event for the IM Research Partnership Project Presentation should be budgeted for in the application.
P a g e 13 | 32
Roles and Responsibilities GRC will be responsible for the overall performance of the contract. GRC will provide project management and data support for the IM Research Partnership including: monitoring the performance of all the vendors to ensure adherence with the scope of work and completion of the deliverables; serving as the data steward for the project and maintaining all datasets used in completing the research objectives; serving as the primary recipient for the project and subcontract with the selected vendors to provide payment for services; providing technical assistance to the selected vendors as needed to facilitate contracting processes; coordinating communication between ODM, ODH, and ODHE project sponsors and selected vendors; providing staffing support for the IM Research Partnership Advisory Committee; and providing written feedback on project deliverables. GRC researchers will be assigned to each project to participate in conceptual/logic modeling research design development, and provide assistance in development of datasets and measurements, data linkages, statistical models, and conversion of analytical products to end-user-facing software. GRC researchers should be considered as extensions of the vendors’ project teams and should be given attribution in outputs such as presentations and publications appropriate to their contributions to the project. The vendor will be responsible for executing the deliverables outlined in the scope of work above for the IM Research Partnership project. The vendor’s role is to ensure the adequate completion of the activities listed under the scope of work and the deliverables, provide detailed documentation and feedback to sponsors on work completed, and collaborate with GRC on all identified tasks listed under the scope of work and deliverables section for which the vendor is applying. Project Governance The Project will be governed using the following structure:
• Infant Mortality Advisory Committee o Will be comprised of members from the state agency sponsors (ODM, ODH,
ODHE), funded investigators, GRC investigators and other university subject matter experts.
o It is expected that the Advisory Committee will meet at least once a quarter.
• Data Stewardship o GRC will be responsible for implementing a technology platform to:
House all of the data used for the infant mortality research partnership. Link datasets using protected health information. Restrict access to protected health information for vendors so that they
receive only de-identified datasets. Distribute de-identified datasets to each of the vendors.
P a g e 14 | 32
Serve as the platform for the spatial analytics project which requires the use of protected health information.
Serve as a developmental analytical platform for use by state agencies for infant mortality predictive and spatial analytics. This may be replicated, after the conclusion of the project, with a separate production version procured and shared by state government agencies.
o The Center for Human Resource Research (CHRR) will serve in a similar role to GRC with respect to linking data using personal identifiers from OhioAnalytics.gov, including: House all of the data from OhioAnalytics.gov for the infant mortality
research partnership. Implement the linkage of datasets using personal identifiers. Restrict access to protected health information for researchers so that they
receive only de-identified datasets. Distribute de-identified datasets to each of the research projects.
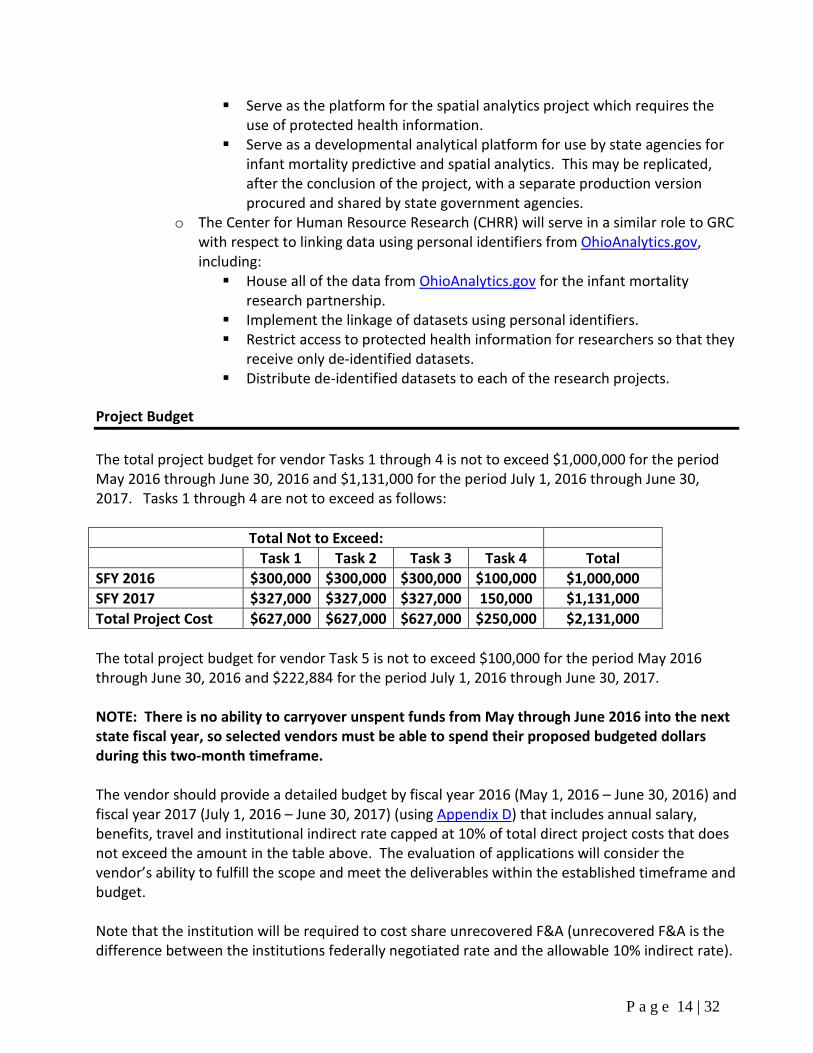
Project Budget The total project budget for vendor Tasks 1 through 4 is not to exceed $1,000,000 for the period May 2016 through June 30, 2016 and $1,131,000 for the period July 1, 2016 through June 30, 2017. Tasks 1 through 4 are not to exceed as follows:
Total Not to Exceed: Task 1 Task 2 Task 3 Task 4 Total
SFY 2016 $300,000 $300,000 $300,000 $100,000 $1,000,000 SFY 2017 $327,000 $327,000 $327,000 150,000 $1,131,000 Total Project Cost $627,000 $627,000 $627,000 $250,000 $2,131,000 The total project budget for vendor Task 5 is not to exceed $100,000 for the period May 2016 through June 30, 2016 and $222,884 for the period July 1, 2016 through June 30, 2017. NOTE: There is no ability to carryover unspent funds from May through June 2016 into the next state fiscal year, so selected vendors must be able to spend their proposed budgeted dollars during this two-month timeframe. The vendor should provide a detailed budget by fiscal year 2016 (May 1, 2016 – June 30, 2016) and fiscal year 2017 (July 1, 2016 – June 30, 2017) (using Appendix D) that includes annual salary, benefits, travel and institutional indirect rate capped at 10% of total direct project costs that does not exceed the amount in the table above. The evaluation of applications will consider the vendor’s ability to fulfill the scope and meet the deliverables within the established timeframe and budget. Note that the institution will be required to cost share unrecovered F&A (unrecovered F&A is the difference between the institutions federally negotiated rate and the allowable 10% indirect rate).
P a g e 15 | 32
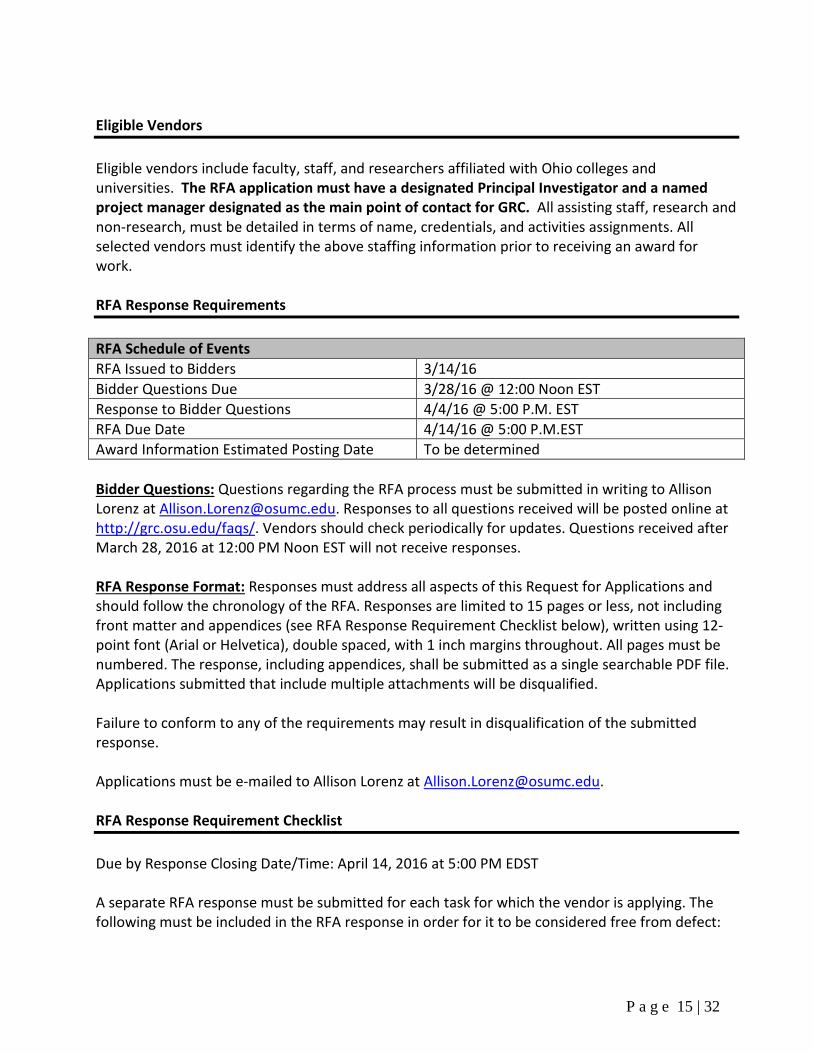
Eligible Vendors Eligible vendors include faculty, staff, and researchers affiliated with Ohio colleges and universities. The RFA application must have a designated Principal Investigator and a named project manager designated as the main point of contact for GRC. All assisting staff, research and non-research, must be detailed in terms of name, credentials, and activities assignments. All selected vendors must identify the above staffing information prior to receiving an award for work. RFA Response Requirements RFA Schedule of Events RFA Issued to Bidders 3/14/16 Bidder Questions Due 3/28/16 @ 12:00 Noon EST Response to Bidder Questions 4/4/16 @ 5:00 P.M. EST RFA Due Date 4/14/16 @ 5:00 P.M.EST Award Information Estimated Posting Date To be determined Bidder Questions: Questions regarding the RFA process must be submitted in writing to Allison Lorenz at [email protected]. Responses to all questions received will be posted online at http://grc.osu.edu/faqs/. Vendors should check periodically for updates. Questions received after March 28, 2016 at 12:00 PM Noon EST will not receive responses. RFA Response Format: Responses must address all aspects of this Request for Applications and should follow the chronology of the RFA. Responses are limited to 15 pages or less, not including front matter and appendices (see RFA Response Requirement Checklist below), written using 12-point font (Arial or Helvetica), double spaced, with 1 inch margins throughout. All pages must be numbered. The response, including appendices, shall be submitted as a single searchable PDF file. Applications submitted that include multiple attachments will be disqualified. Failure to conform to any of the requirements may result in disqualification of the submitted response. Applications must be e-mailed to Allison Lorenz at [email protected]. RFA Response Requirement Checklist Due by Response Closing Date/Time: April 14, 2016 at 5:00 PM EDST A separate RFA response must be submitted for each task for which the vendor is applying. The following must be included in the RFA response in order for it to be considered free from defect:

P a g e 16 | 32
NOTE: Only items D through J will be counted as part of the 15 page or less limit in the response. A. Cover Letter B. Application Face Page C. Table of Contents D. Project Summary E. Project Management and Scope of Work F. Methodology G. Data Requirements H. Organizational Capacity I. Staff Qualifications J. Resource Allocation & Time Commitment K. Appendices
• Gantt Chart of Activities and Timeline • Copies of staff resumes or NIH bio-sketch • Completed Past Project Performance Form • Signed DUA – must be included in application to be considered responsive. • Budgets and Budget Narrative
Further explanation related to each topic area is below. A. Cover Letter The cover letter must be in the form of a standard business letter, and must be signed by an individual authorized by the university to legally bind the vendor. The cover letter will provide an executive summary of the vendor’s request for funds, including whether planning and/or implementation funding is requested. The letter must also include:
1. A statement regarding the vendor’s university or college, Federal tax identification number, and address;
2. A list of the people who prepared the application, including titles; 3. The name, phone number, fax number, and email address of a contact person who has
authority to answer questions regarding the application; 4. The name, phone number, fax number, and email address of the Sponsored Programs
Officer responsible for the application; 5. The name, phone number, fax number, and email address of the individual(s) responsible
for certifying the non-federal matching funds required under this funding opportunity; 6. A list of all vendors, if any, that the vendor will use on the work if selected. If these vendors
have not yet been identified, this information must be submitted once selected; 7. For each proposed vendor, the vendor must attach a letter from the vendor, signed by
someone authorized to legally bind the vendor, including the following: a. The vendor’s legal status, tax identification number, and principal place of business
address; b. The name and phone number of someone who is authorized to legally bind the
vendor to contractual obligations; c. A description of the portions of the work the vendor will complete;
P a g e 17 | 32
d. A commitment to complete the work if the vendor is selected; e. A statement that the vendor has read and understood the RFA and will comply with
the requirements of the RFA. 8. A statement that the vendor’s application meets all the requirements of this RFA.
B. Application Face Page The application’s face page should identify the title of the funding opportunity, identified Task per the Scope of Work, vendor, contact person, and date of submission. C. Table of Contents The application’s Table of Contents should outline the application’s contents by page number. D. Project Summary For each application submitted, the summary must describe the background, rationale, objective, organization of the evaluation, and methodology. If the vendor is applying for Tasks 1, 2, 3, or 4, please also describe the benefit to the Medicaid program. E. Project Management and Scope of Work Project Management Plan: The vendor must fully describe its approach, methods, and specific work steps for completing the specific scope of work task applied for on this project and producing the deliverables. GRC encourages responses that demonstrate a thorough understanding of the nature of the project and steps the vendor will complete to ensure the completed product is of high quality. The vendor’s work plan should clearly and specifically identify personnel assignments and tasks. The work plan must identify a lead Principal Investigator and a project manager who will serve as the main point of contact for the vendor. After best and final negotiations and award, the project management plan will become the vendor’s management plan to fulfill the contract. The management plan must be as complete as possible at the time of submission. It must:
1. Describe the vendor’s organization and management structure responsible for fulfilling the evaluation requirements.
2. Describe the potential major challenges presented by this evaluation and how they would be addressed.
3. Describe any other potential problem areas, risks and recommended solutions to these problem areas and risks including any assumptions used in developing those solutions.
4. Describe how the vendor will ensure that the work will be completed on time, will be of high quality, and will meet contract specifications.
5. Describe how communication, status review, and reporting procedures will be conducted between all parties, including frequency and mode of communication (e.g. e-mail, telephone, personal meetings).
P a g e 18 | 32
6. Describe contingency plans if the primary plan is not able to meet the evaluation requirements, including an action plan if the vendor or GRC is dissatisfied with the individual performance of any key members of the project work team.
7. Include a detailed timeline in the form of a Gantt chart (see Appendix C for Tasks 1 – 4 and Appendix C for Task 5)).
F. Methodology The vendor should prepare a summary of the preliminary research methodology and design to complete the specified Scope of Work task. The summary should describe how the vendor proposes to measure upstream determinants of health, including social, environmental, clinical, geographic, etc. G. Data Requirements Vendors should describe the data and source(s) that are proposed to be used regarding the task for which they are applying, including the linking strategy with Women of Reproductive Age/Vital Statistics/Medicaid data. Vendors should identify whether project personnel or sub-contractors will need access to confidential Medicaid and Vital Statistics data, and/or the specified data they intend to use to perform their work. All RFA applications must include a signed Medicaid DUA to be considered responsive to the RFA. For projects that include data other than Medicaid data, the vendor will be responsible for securing the necessary signed data use agreements upon submission of the application. For applications in which data collection and use involves human subjects (e.g., qualitative structured focus group interviews), the vendor is expected to have an approved IRB application prior to the beginning of data collection. Qualitative approaches may be used to test the validity of quantitative analysis. Vendors should describe which aspect of their application requires IRB approval, and identify the IRB that will be used to approve the project. It is recommended that the vendor use their institution's IRB for human subjects' protection. The application must adhere to all HIPAA rules for personal health data as detailed by the Principle Investigator's university standards, including the storage of data and destruction of data after project completion. Vendors must also address data security, transport, and access protocols that will be included in the evaluation study to ensure compliance with pertinent federal/state law and regulations. H. Organizational Capacity Vendor Profile: Each application must include a profile of the vendor’s experience working on similar evaluations. The profile must also include the vendor’s university or college address, and telephone number, and any other background information that will help the evaluation committee gauge the ability of the vendor to fulfill the obligations of the contract. Past Project Performance: The vendor must complete the form in Appendix B including contact information for services the vendor has provided for up to three projects in the past five years that
P a g e 19 | 32
were similar in their nature, size, or scope to the work. The project and professional references information must include the organization for whom the work was done, and a project and professional reference person from that organization that includes the phone number, email and company or organization address. The completed past project performance form may be submitted as an appendix to the application. Equipment and Software Requirements: The vendor must provide an assurance they have the hardware, software, and technology staff support capacity capable of performing the tasks proposed in the application. The vendors for Tasks 1, 2, and 3 should identify the software that will be used for modeling, and describe the reasons for that selection. The criteria that should be described for this project include:
• Application to social, behavioral, and health sciences • Runs on Unix/Linux/web enabled Operating system • Web enabled user interface for state agency facing users.
Note that GRC currently uses Unix/Linux based R, SAS BI Enterprise Guide, and ArcGIS for analytics; SQL Server for database support; R-Shiny Pro, ArcGIS, and Tableau for web enabled user-facing applications. Other software can be used, but the cost of licensing, installation, and development using other software must be factored into the vendor’s application. Equipment over $5,000 must be identified in the application, or otherwise approved by GRC prior to purchase. I. Staff Qualifications One of the criteria on which GRC may base an award of contract is the quality of the Vendor’s Work Team. Within the project narrative, each vendor must identify the key members assigned to each area, including a named project manager who will serve as the point of contact for the vendor, and briefly describe their qualifications to execute the assigned responsibilities. In addition, each vendor must submit a four-page maximum resume or curriculum vitae for every key member as an appendix. Switching personnel after the award requires prior approval from GRC. The criteria and qualifications listed below will be used for evaluating personnel. Although the Preferred Desired Qualifications are not mandatory, vendors not meeting any of the Preferred Desired Qualifications must otherwise demonstrate their competence, capacity, and willingness to do the work to receive consideration. Vendors are encouraged to address the Preferred Desired Requirements and any additional education, training, experience, or expertise that is relevant to the work. NOTE: Key members of the work team may serve in multiple project roles if the vendor demonstrates that the proposed person meets all applicable qualifications and will devote sufficient time to the work to justify having multiple responsibilities.
P a g e 20 | 32
Researcher/Evaluator: The key member assigned to be the researcher or evaluator will have primary responsibility for the work, including planning and coordination of the work effort, assurance of timely completion of work, and assurance that work is of high quality and is completed using valid research methods in accordance to contract specifications. This key member will also be responsible for communication with GRC and addressing any issues or problems, including development of corrective action plans. Preferred Desired Qualifications:
• Researcher employed at a college or university in Ohio. • Minimum commitment of principal investigator of 10% or more. • Published research in peer reviewed journals, with at least three examples of publications
related to an evaluation. o At least two or the three examples should be directly related to the specific Scope
of Work task applied for. • At least two years’ experience and demonstrated competency in leading health services
research projects. • Demonstrated competency in planning, managing, and completing projects on schedule.
Preferred Qualifications:
• Experience working with publicly funded health programs such as Medicaid. • Key member of team is a recognized expert in Infant Mortality or related subject matter
expert. • Previous successful relevant work using Ohio data and populations.
J. Resource Allocation & Time Commitment The vendor must submit a table of organization graphic and narrative that clearly indicates the time commitment of the key members of the proposed work team to each deliverable of the project and to other projects during the term of the contract. K. Budgets and Budget Narratives Detailed Budget: In this section, the vendor must provide detailed budgets for the total scope of the application using the budget form provided in Appendix D and on the GRC website, (http://grc.osu.edu/currentfunding/). The vendor must also provide an accompanying budget narrative, detailing specific direct and indirect costs associated with the application. Please note that the sponsor limits facility and administrative cost (F&A or indirect rate, overhead) reimbursement to 10% of total project costs. This project spans the 2016 and 2017 State Fiscal Years (SFY) and may not exceed $ 2,453,884 for Tasks 1 through 4 and $322,884 for Task 5 in total project costs over this time period. The total project budget for Tasks 1 through 4 is limited to approximately $1,000,000 for the period May 2016 through June 30, 2016 and $1,131,000 for the period July 1, 2016 through June 30, 2017. The total project budget for vendor Task 5 is limited to approximately $100,000 for the period May 2016 through June 30, 2016 and $222,884 for the period July 1, 2016 through June 30, 2017. NOTE: There is no ability to carryover unspent funds from May through June 2016 into the next
P a g e 21 | 32
state fiscal year, so selected vendors must be able to spend the allotted dollars during this two-month timeframe. Award funding may be used for personnel expenses, software, travel and other direct costs. Funds may not be used for food, computer hardware or equipment over $5,000 (without extensive explanation and additional approval). The institution will be required to cost share unrecovered F&A (unrecovered F&A is the difference between the institutions federally negotiated rate and the allowable 10% indirect rate). In addition, applications must breakdown the amount of requested project funds required to meet the project deliverables per State Fiscal Year (SFY) within the project period identified in the Executive Summary (SFY 16 – May 1, 2016 – June 30, 2016 and SFY 17 – July 1, 2016 – June 30, 2017). Application Review Evaluation of Applications: The evaluation process may consist of up to five distinct phases:
1. The initial review of all applications for defects; 2. The evaluation committee’s evaluation of the applications; 3. Request for more information (interviews, presentations, and/or
demonstrations); 4. Negotiation with vendors on best and final offer if necessary; and 5. Selection of vendors and eventual contract award.
The RFA selection committee will be composed of representatives from the sponsor agencies. GRC will facilitate the review, but does not sit on the selection committee. Initial Review of Applications for Defects: All applications must meet the following criteria in order to be considered free from defects. A no answer for any of the following criteria will result in the application receiving no further consideration as it is not free from defects. Mandatory Criteria to be Free from Defect Application Meets
Mandatory Submission Guidelines
1 Application received by April 14, 2016 5:00 Noon EDST Yes No 2 Application submitted using required format Yes No 3 Application includes signed Medicaid DUA Yes No 4 Principal Investigator is affiliated with Ohio college or university Yes No 5 Named project manager identified as the main point of contact Yes No

P a g e 22 | 32
Application Evaluation Criteria: In the application evaluation phase, the committee will rate the applications free from defects submitted in response to this RFA based on the following criteria: Criteria Possible Points Weight Section 1: PROJECT MANAGEMENT PLAN 15 15 Section 2: METHDOLOGY AND DATA REQUIREMENTS 18 50 Section 3: ORGANIZATIONAL CAPACITY 6 10 Section 4: STAFF QUALIFICATIONS 9 20 Section 5: RESOURCE ALLOCATION AND BUDGETS 9 5 Vendors must receive a minimum of 60 out of the maximum 100 points to be considered for award. In the case of a tie, additional points will be awarded to applications that demonstrate collaboration across universities or colleges. RFA Terms and Conditions As the primary recipient of the Ohio Colleges of Medicine Government Resource Center, The Ohio State University (OSU) reserves the right to:
• Reject any or all applications received in response to this RFA; • Request clarification from any vendor on any or all aspects of its application; • Cancel and/or reissue this RFA at any time; • Retain all applications submitted in response to this RFA; and, • Invite some, all, or none of the vendors for interviews and further discussion; and • Negotiate with vendor(s) on best and final offer, including the need to submit a best and
final Application resulting from negotiations. If negotiations were limited and all changes were reduced to signed writings during negotiations, a best and final Application may not need to be submitted.
Provisions: If any provisions in a resultant agreement are held to be invalid, void, or unenforceable, the remaining provisions shall continue in full force and effect without being impaired or invalidated in any way. Funding will be adjusted to reflect any changes in the deliverables. The vendor will submit any changes in deliverables to GRC. Ethical Conduct: Apart from a contact required for any on-going business at OSU, vendors are specifically prohibited from contacting any individual at, or associated with OSU regarding this RFP. Vendor communication shall be limited to the contact named on the cover page of this document. A vendor’s failure to adhere to this prohibition may, at OSU’s sole discretion, disqualify the vendor’s application. Cancellation for Lack of Funding: A resultant agreement may be canceled without any further obligation on the part of The Ohio State University in the event that sufficient appropriated
P a g e 23 | 32
funding is unavailable to assure full performance of its terms. The vendor shall be notified in writing of such non-appropriation at the earliest opportunity. Quote: Vendor responses must be valid for 120 days. Contract Term: The contract term will commence on the date of award and continue through June 30, 2017. Pricing will remain firm for the entire period. Requirements for Advance Approval: Prior to out-of-state travel or conference attendance by the vendor, the vendor will consult with OSU concerning the nature and cost of each out-of-state travel plan and conference registration for an amount exceeding $2,500. Data Use and Management
A. The vendor will become familiar with and fully implement all requirements of HIPAA.
B. The vendor will be in compliance with Federal, HIPAA and State confidentiality law, for data use, and management including but not limited to access, storage, and transmission, shall be role-based, specific to this agreement.
C. The vendor shall enter separately into a Business Associate Agreement (BAA) with OSU-
GRC to receive data funded/authorized under this agreement, in accordance with the Business Associate Agreement between ODM and OSU-GRC.
D. The vendor shall submit a signed Data Use Agreement (DUA) as part of the submission of a
complete application to this RFA. Failure to submit the signed DUA will be considered an incomplete application and will receive no further consideration.
E. The vendor shall not use any information, systems, or records made available for any
purpose other than to fulfill the obligations specified herein.
F. The vendor’s possession of information provided may be considered confidential or proprietary under the laws of the State of Ohio or under federal law, and that vendor agrees to promptly notify OSU and ODM of the receipt of any public records requests for information related to this Agreement in order to seek to have any confidential or proprietary information withheld from the document prior to its release.
G. All data provided to the vendor may only be used for the specific associated agreement
and for no other use in projects not associated with the agreement, and that any vendor’s data release, sharing, or transfer beyond its initial approved scope and specifications will be considered as unauthorized.
P a g e 24 | 32
H. The selected vendors for Tasks 1 and 2 will receive de-identified data from GRC. If these projects have additional data sources that need to be linked to the de-identified data, they will have to be submitted to GRC for the linkage process, and the results will be provided to the project. Data will be shared through a secure FTP server.
I. Task 3 will require the use of protected health information (consumer’s addresses, longitude, latitude). All work with identifiable data must be done on GRC’s Infant Mortality Analytic Server (IMAS). Project staff will receive security tokens, must pass a background check, and receive an OSU guest e-mail account as needed. IMAS software will include ArcGIS, SAS/BI Enterprise Guide, R and Shiny Server (Pro), and Tableau.
J. Data sets available to selected vendors includes the following:
• Linked Medicaid/VS data
• Clinical measures, access to care, birth outcomes, housing instability, family income, demographics
• Other state agency data (confirmed) • OIMRI (ODH) Home visiting program • SACWIS (ODJFS – Child Welfare) – Family stability • PRAMS/VS Survey (ODH)
• Other state agency data (not confirmed) • SNAP (ODJFS) – Food insecurity • TANF (ODJFS) – Employment Stability • WIC (ODH) – Nutrition and Breast Feeding
• Other data thru CHRR (not confirmed) – OhioAnalytics.gov • Housing Quality • Employment Stability • Education
• Other possible statewide or local data resources • PantryTrak – Food Insecurity • Funded Project specific data – to be determined.
Presentation, Publications and Dissemination
A. The vendor shall obtain GRC and either ODM, ODH, or ODHE, as applicable, prior approval for release of any results including preliminary and/or final results related to funded projects or funded data under this Agreement. GRC and either ODM ODH or ODHE, as applicable, will review, approve or reject publications, presentations or disseminations resulting from activities of this Agreement.
B. GRC and either ODM, ODH, or ODHE, as applicable, will review and comment within 30 days
upon submission of a draft to ODM, ODH, or ODHE, as applicable, proof peer-reviewed
P a g e 25 | 32
academic journal articles. Notwithstanding the proceeding, if the parties disagree concerning whether certain information should be deleted or modified, the parties agree to meet for the purpose of making good faith efforts to discuss and resolve any issues or disagreements.
C. Time Sensitivity – Any data or publication release may be pending or delayed due to
ODM policy/program change.
D. The vendor shall obtain GRC and either ODM, ODH, or ODHE, as applicable, prior review and permission to release any products resulting from activities, funded data or projects under this Agreement.
E. When issuing press releases, requests for applications, bid solicitations, and other
documents or statements describing projects or programs funded in whole or in part with Federal money, all grantees receiving Federal funds, including but not limited to State and local governments shall clearly state:
1. The percentage of total costs of the program or project which will be financed
with Federal money;
2. The dollar amount of Federal funds for the program or project; and
3. The percentage and dollar amount of the total costs or the program or project that will be financed by nongovernment sources.
P a g e 26 | 32
Appendix A
MEDTAPP Project Progress Report
Project Title: Project #
Project Information
Submission Date:
Description of Accomplishments:
Emerging/Pending Issues (that could impact schedule, scope or resources):
Action Steps for Scope of Work/ Deliverables
Status and Description (C= completed, P = progress, NP = no progress)
Target Date
Completion Date
Documents Attached (describe):
Recommended Changes to Project Plan:
Schedule Deliverables Resource Allocation
Other Description: Approved by: Date:

P a g e 27 | 32
Appendix B
PAST PROJECT PERFORMANCE
REFERENCE/CONTACT
The Vendor must list up to three organizations that have received services of similar size, nature or scope to the work from the Vendor in the past five years. Include the company or organization, contact name, address, current phone number and beginning and ending dates of work on the project for each.
Company/Organization: Contact:
Address: Phone Number:
Project Name: Beginning Date of Project Month/Year:
Ending Date of Project Month/Year:
Company/Organization: Contact:
Address: Phone Number:
Project Name: Beginning Date of project Month/Year:
Ending Date of Project Month/Year:
Company/Organization: Contact:
Address: Phone Number:
Project Name: Beginning Date of Project Month/Year:
Ending Date of Project Month/Year:
Vendor’s Name:
P a g e 28 | 32
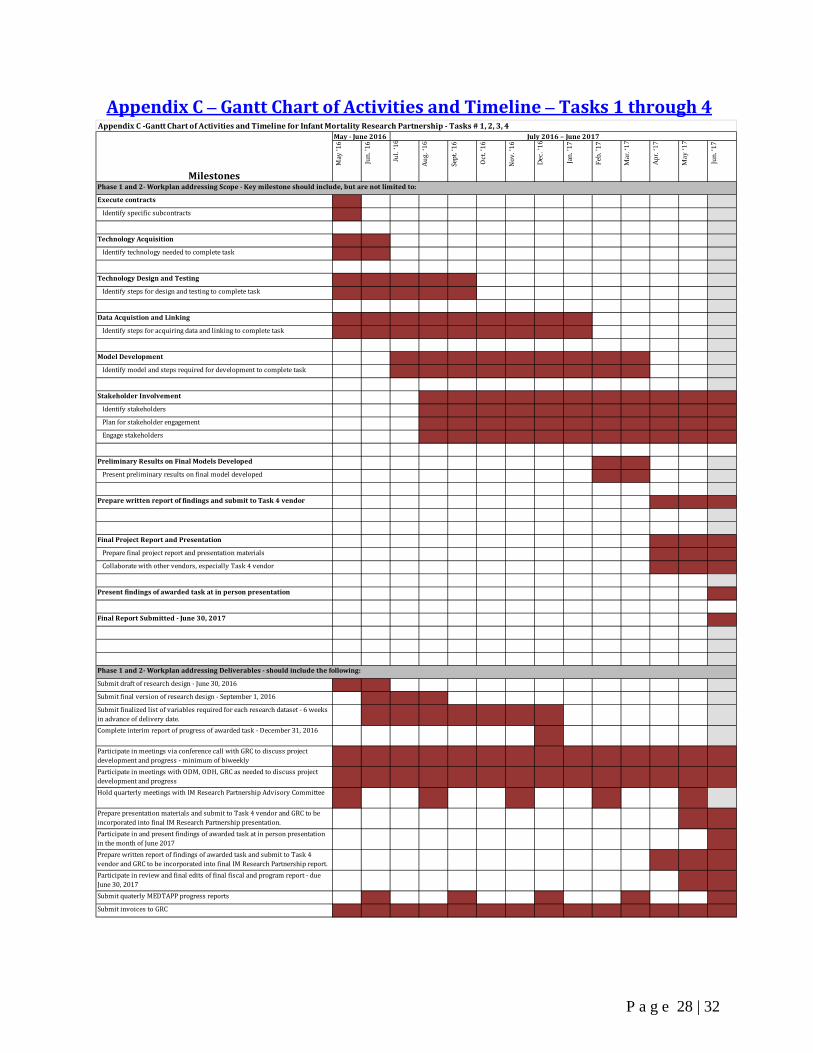
Appendix C – Gantt Chart of Activities and Timeline – Tasks 1 through 4
May
‘16
Jun.
'16
Jul.
‘16
Aug
. ‘16
Sept
. ‘16
Oct
. ‘16
Nov
. ‘16
Dec
. ’16
Jan.
’17
Feb.
’17
Mar
. ‘17
Apr
. ‘17
May
‘17
Jun.
‘17
Execute contracts
Identify specific subcontracts
Technology Acquisition
Identify technology needed to complete task
Technology Design and Testing
Identify steps for design and testing to complete task
Data Acquistion and Linking
Identify steps for acquiring data and linking to complete task
Model Development
Identify model and steps required for development to complete task
Stakeholder Involvement
Identify stakeholders
Plan for stakeholder engagement
Engage stakeholders
Preliminary Results on Final Models Developed
Present preliminary results on final model developed
Prepare written report of findings and submit to Task 4 vendor
Final Project Report and Presentation
Prepare final project report and presentation materials
Collaborate with other vendors, especially Task 4 vendor
Present findings of awarded task at in person presentation
Final Report Submitted - June 30, 2017
Submit draft of research design - June 30, 2016
Submit final version of research design - September 1, 2016
Submit finalized list of variables required for each research dataset - 6 weeks in advance of delivery date.Complete interim report of progress of awarded task - December 31, 2016
Participate in meetings via conference call with GRC to discuss project development and progress - minimum of biweeklyParticipate in meetings with ODM, ODH, GRC as needed to discuss project development and progressHold quarterly meetings with IM Research Partnership Advisory Committee
Prepare presentation materials and submit to Task 4 vendor and GRC to be incorporated into final IM Research Partnership presentation.Participate in and present findings of awarded task at in person presentation in the month of June 2017Prepare written report of findings of awarded task and submit to Task 4 vendor and GRC to be incorporated into final IM Research Partnership report.Participate in review and final edits of final fiscal and program report - due June 30, 2017Submit quaterly MEDTAPP progress reports
Submit invoices to GRC
Phase 1 and 2- Workplan addressing Deliverables - should include the following:
Appendix C -Gantt Chart of Activities and Timeline for Infant Mortality Research Partnership - Tasks # 1, 2, 3, 4
Milestones
May - June 2016 July 2016 – June 2017
Phase 1 and 2- Workplan addressing Scope - Key milestone should include, but are not limited to:

P a g e 29 | 32
Appendix C – Gantt Chart of Activities and Timeline – Task 5
May
‘16
Jun.
'16
Jul.
‘16
Aug
. ‘16
Sept
. ‘16
Oct
. ‘16
Nov
. ‘16
Dec
. ’16
Jan.
’17
Feb.
’17
Mar
. ‘17
Apr
. ‘17
May
‘17
Jun.
‘17
Execute contracts
Identify specific subcontracts
Technology Acquisition
Identify technology needed to complete task
Technology Design and Testing
Identify steps for design and testing to complete task
Data Acquistion and Linking
Identify steps for acquiring data and linking to complete task
Model Development
Identify model and steps required for development to complete task
Stakeholder Involvement
Identify stakeholders
Plan for stakeholder engagement
Engage stakeholders
Preliminary Results on Final Model Developed
Present preliminary results on final model developed
Final Project Report and Presentation
Prepare final project report and presentation materials
Present findings of awarded task at in person presentation
Final Report Submitted - June 30, 2017
Submit draft of research design - June 30, 2016
Submit final version of research design - September 1, 2016
Submit finalized list of variables required for each research dataset - 6 weeks in advance of delivery date.Complete interim report of progress of awarded task - December 31, 2016
Participate in meetings via conference call with GRC to discuss project development and progress - minimum of biweeklyParticipate in meetings with ODH and GRC as needed to discuss project development and progressHold quarterly meetings with IM Research Partnership Advisory Committee
Prepare presentation materials and submit to GRC for final IM Research Partnership presentation.Participate in and present findings of awarded task at in person presentation in the month of June 2017Prepare written report of findings and submit to GRC
Participate in review and final edits of final fiscal and program report - due June 30, 2017Submit quaterly progress reports
Submit invoices to GRC
Phase 1 and 2- Workplan addressing Deliverables - should include the following:
Appendix C - Gantt Chart of Activities and Timeline for Infant Mortality Research Partnership - Task # 5
Milestones
May - June 2016 July 2016 – June 2017
Phase 1 and 2- Workplan addressing Scope - Key milestone should include, but are not limited to:
P a g e 30 | 32
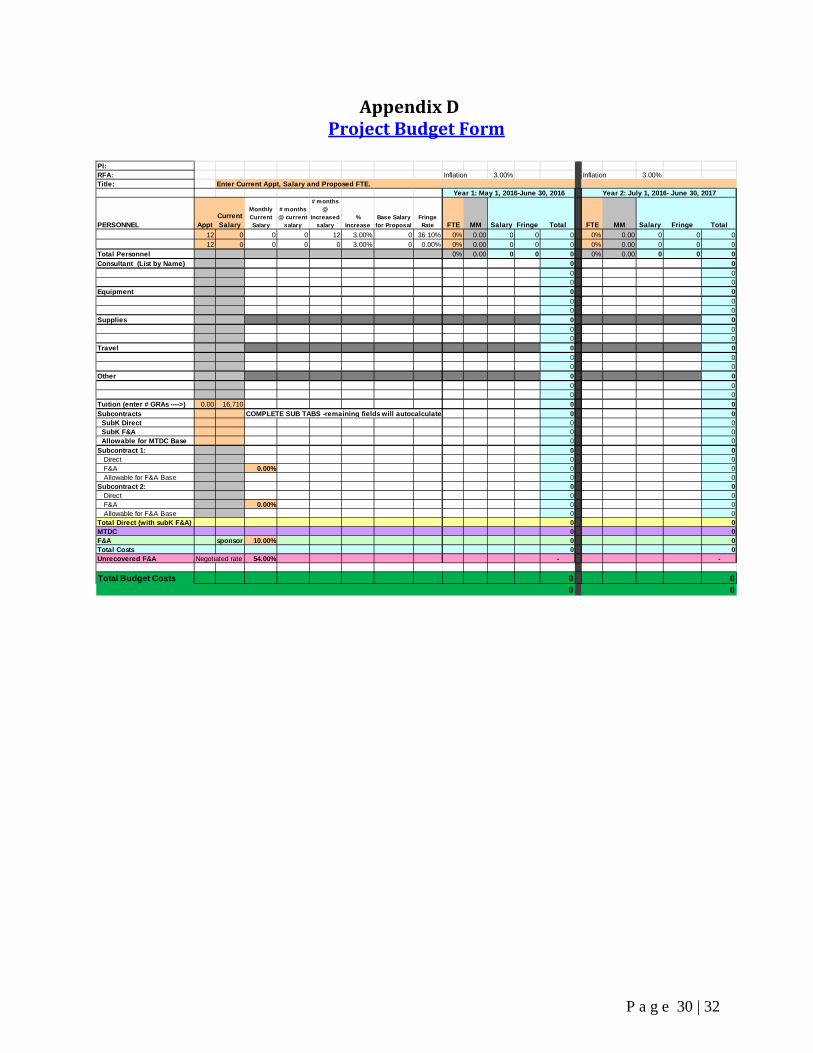
Appendix D Project Budget Form
PI: RFA: Inflation 3.00% Inflation 3.00%Title:
PERSONNEL ApptCurrent Salary
Monthly Current Salary
# months @ current
salary
# months @
increased salary
% Increase
Base Salary for Proposal
Fringe Rate FTE MM Salary Fringe Total FTE MM Salary Fringe Total
12 0 0 0 12 3.00% 0 36.10% 0% 0.00 0 0 0 0% 0.00 0 0 012 0 0 0 0 3.00% 0 0.00% 0% 0.00 0 0 0 0% 0.00 0 0 0
Total Personnel 0% 0.00 0 0 0 0% 0.00 0 0 0Consultant (List by Name) 0 0
0 00 0
Equipment 0 0 0 0 0 0Supplies 0 0
0 00 0
Travel 0 0 0 0
0 0Other 0 0
0 00 0
Tuition (enter # GRAs ---->) 0.00 16,710 0 0Subcontracts 0 0 SubK Direct 0 0 SubK F&A 0 0 Allowable for MTDC Base 0 0Subcontract 1: 0 0 Direct 0 0 F&A 0.00% 0 0 Allowable for F&A Base 0 0Subcontract 2: 0 0 Direct 0 0 F&A 0.00% 0 0 Allowable for F&A Base 0 0Total Direct (with subK F&A) 0 0MTDC 0 0F&A sponsor 10.00% 0 0Total Costs 0 0Unrecovered F&A Negotiated rate 54.00% - -
Total Budget Costs 0 00 0
Enter Current Appt, Salary and Proposed FTE. Year 1: May 1, 2016-June 30, 2016
COMPLETE SUB TABS -remaining fields will autocalculate
Year 2: July 1, 2016- June 30, 2017

P a g e 31 | 32
Appendix E
The Ohio State University Office of Sponsored Programs Standard Terms and Conditions

P a g e 32 | 32
Appendix F
Medicaid Data Use Agreement
Please include the applicable Attachment A form that applies to the task applied for:
Attachment A – Tasks 1 through 4
Attachment A – Task 5