Embed Size (px)
DESCRIPTION
Seminar on Philippine Infant Mortality
Citation preview
SEMINAR ON PHILIPPINE INFANT MORTALITY
January ,2011
This entry gives the number of deaths of infants under one year old in a given year per 1,000 live births in the same year; included is the total death rate, and deaths by sex, male and female. This rate is often used as an indicator of the level of health in a country.
WHAT IS INFANT MORTALITY?
Perinatal mortality only includes deaths between the fetal viability (22 weeks gestation) and the end of the 7th day after delivery.
Neonatal mortality only includes deaths in the first 28 days of life.
Postneonatal mortality only includes deaths after 28 days of life but before one year.
Child mortality includes deaths within the first five years after birth
Related to INFANT MORTALITY
The infant mortality rate is also called the infant death rate (per 1,000 live births).
Historically, infant mortality claimed a considerable percentage of children born, but rates have significantly declined in the West in modern times. This has been mainly due to improvements in basic health care, though high-technology medical advances have also helped. Infant mortality rate is commonly included as a part ofstandard of living evaluations in economics.
The infant mortality rate correlates very strongly with, and is among the best predictors of, state failure.[4] IMR is therefore also a useful indicator of a country's level of health or development, and is a component of the physical quality of life index. However, the method of calculating IMR often varies widely between countries, and is based on how they define a live birth and how many premature infants are born in the country.
Comparing infant mortality rates
The World Health Organization (WHO) defines a live birth as any born human being who demonstrates independent signs of life, including breathing, voluntary muscle movement, or heartbeat. Many countries, however, including certain European states and Japan, only count as live births cases where an infant breathes at birth, which makes their reported IMR numbers somewhat lower and raises their rates of perinatal mortality
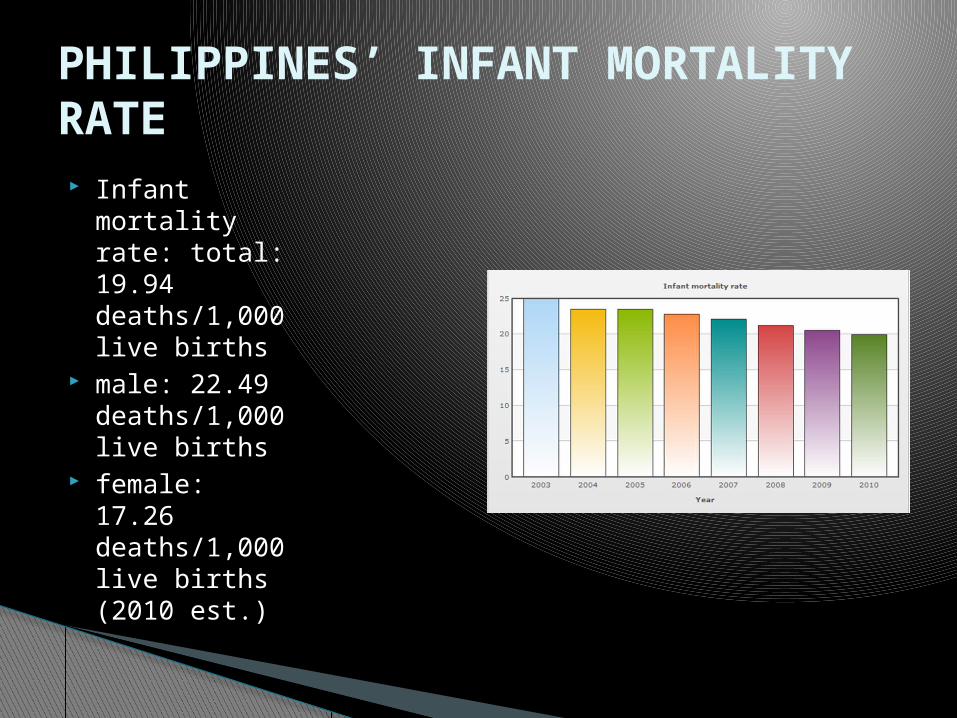
Infant mortality rate: total: 19.94 deaths/1,000 live births
male: 22.49 deaths/1,000 live births
female: 17.26 deaths/1,000 live births (2010 est.)
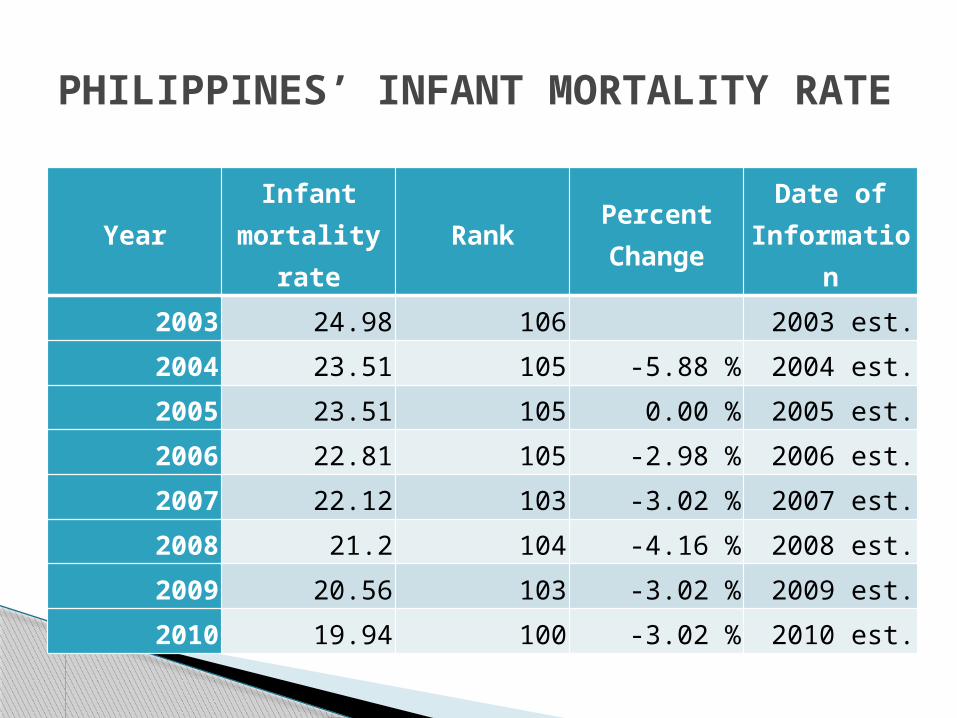
PHILIPPINES’ INFANT MORTALITY RATE
YearInfant
mortality rate
RankPercent Change
Date of Informatio
n
2003 24.98 106 2003 est.
2004 23.51 105 -5.88 % 2004 est.
2005 23.51 105 0.00 % 2005 est.
2006 22.81 105 -2.98 % 2006 est.
2007 22.12 103 -3.02 % 2007 est.
2008 21.2 104 -4.16 % 2008 est.
2009 20.56 103 -3.02 % 2009 est.
2010 19.94 100 -3.02 % 2010 est.
PHILIPPINES’ INFANT MORTALITY RATE
Since the NICHD was established, the nation's infant mortality rate has dropped by 70 percent-in part due to the contributions of Institute-sponsored research.[1] The newest advances of NICHD-funded researchers recently identified an exciting and relatively simple means to prevent preterm birth in some cases and uncovered additional threats to infant life and health, for which preventive steps can be taken.
Infant MortalityReducing Infant Deaths.
Preterm delivery (before 37 weeks of gestation) is the most important cause of infant mortality and morbidity in the United States. Furthermore, prematurity contributes substantially to racial/ethnic health disparities in infant mortality. It is also very costly. While preterm births account for 12 percent of births in the United States, new estimates show that hospital charges alone for premature/low-birthweight babies reached $13.6 billion in 2001, accounting for one-half of hospital charges for all newborns.[2][3] In addition, preterm babies are more likely to have long-term health problems.
Progesterone Injections Reduce Preterm Delivery.
Women whose first baby was preterm are at high risk for subsequent preterm delivery. Until recently, most previously tested strategies to prevent preterm birth in such high-risk women failed to produce effective, reliable results. Early research using progesterone showed promise, but these studies were too small, and the methods and populations were too diverse, to yield conclusive results. Working collaboratively in the NICHD's Maternal-Fetal Medicine Units Network, researchers administered either progesterone (17P) or a placebo to a large group of women who had delivered a previous preterm infant.
The 17P-treated women were 30 percent more likely than placebo-treated women to carry their babies to term, and their infants had lower rates of life-threatening complications. African American women benefited as much as white women from the experimental treatment. Furthermore, the researchers found no evidence that 17P caused birth defects or any other problem in the infants of treated mothers. Thus, 17P is a significant breakthrough that holds tremendous promise for reducing preterm birth and life-threatening medical complications in infants of high-risk women. This treatment may also help to reduce the entrenched disparity in birth outcomes for African American infants.
Scientists agree that people who live in areas with polluted air tend to have more health problems. Scientists don't agree, however, as to whether air pollution actually causes the health problems and higher mortality. Areas with higher air pollution also tend to have high population densities, low income levels, and high crime rates, all of which could impact health unfavorably. Further, most previous air pollution research focused on adverse health effects in adults, with little attention paid to children due to the complexities of the issues involved. For instance, children may become ill from exposures that would not affect adults, and children may be more vulnerable to some environmental pollutants than are adults due to their size, growth, and behaviors.
More Babies Survive When Air is Clean.
An economic recession in 1981-82 provided scientists with a kind of natural laboratory to observe the effects of pollution. The economic slowdown reduced air pollution in selected geographic regions. NICHD-supported researchers were able to demonstrate a causal link between total suspended particulate air pollution and changes in infant death rates. The researchers estimated 100 fewer infant deaths per 100,000 live births occurred during this time of lower air pollution. Most of the decline was observed in very young infants between one day and one month of age. These findings strongly suggest that babies who live in clean air areas have a greater chance of living until their first birthday. The findings also have important implications when determining the cost-benefits of policies aimed at reducing certain types of air pollution and in developing federal, state, and local zoning and air pollution standards. Finally, the findings suggest that obstetrical and pediatric health care providers should more closely monitor their patients in high-risk environments.
. Despite substantial progress, wide racial disparities in infant mortality remain in the United States. The gap is particularly wide in Washington, D.C., where mortality rates for African American infants in 2000 were 16.1 infant deaths per 1,000 live births-more than double the national rate of 6.9 per 1,000, for all races.[5] A randomized, controlled trial, which was part of the NICHD-funded D.C. Initiative to Reduce Infant Mortality, tested a unique program of educational and supportive services for high-risk mothers and their infants. Nearly all of the mothers in the program were African American, had inadequate or no prenatal care, and had other risk factors including poverty and low educational levels. The program, Pride in Parenting (PIP), provided mothers with information about child health and development and health and social service resources available to them. This information, along with training and social support for the mothers, was provided in home visits, parent-child developmental play groups, and parent support groups.
Encouraging Well-Child Care as a Strategy against Infant Mortality
Unlike similar programs that used nurses for home visits, the PIP program achieved better acceptance by recruiting lay visitors from the mothers' own communities, and by training them extensively in child health and development before they began visiting the mothers. Another unique feature was that program staff neither arranged for nor accompanied mothers to health care and social service sites; instead, mothers were given information on available resources and coached in using services, but were solely responsible for ensuring that their children received the well-child care and immunizations. The program deliberately used lay home visitors to lessen the cultural barriers to health care that account, in part, for disparities in infant mortality and morbidity. Compared to mothers who used standard social services, mothers in the PIP program were more likely to 1) begin well-child care earlier, 2) make more frequent well-child care visits, and 3) complete the scheduled immunizations for their infants. If successfully replicated, this model program could enable minority mothers to seek and use health care for themselves and their children more effectively.
PROGRAM OF THE DOH
NEW BORN SCREENING
Newborn screening (NBS) is a simple procedure to find out if your baby has a congenital metabolic disorder that may lead to mental retardation and even death if left untreated.
What is newborn screening?
Most babies with metabolic disorders look normal at birth. One will never know that the baby has the disorder until the onset of signs and symptoms and more often ill effects are already irreversible.
Why is it important to have newborn screening?
Newborn screening is ideally done on the 48th hour or at least 24 hours from birth. Some disorders are not detected if the test is done earlier than 24 hours. The baby must be screened again after 2 weeks for more accurate results.
When is newborn screening done?
Newborn screening is a simple procedure. Using the heel prick method, a few drops of blood are taken from the baby's heel and blotted on a special absorbent filter card. The blood is dried for 4 hours and sent to the Newborn Screening Laboratory (NBS Lab).
How is newborn screening done?
P550. The DOH Advisory Committee on Newborn Screening has approved a maximum allowable fee of P50 for the collection of the sample.
How much is the fee for newborn screening?
Newborn screening results are available within seven working days to three weeks after the NBS Lab receives and tests the samples sent by the institutions. Results are released by NBS Lab to the institutions and are released to your attending birth attendants or physicians. Parents may seek the results from the institutions where samples are collected. A negative screen mean that the result of the test is normal and the baby is not suffering from any of the disorders being screened. In case of a positive screen, the NBS nurse coordinator will immediately inform the coordinator of the institution where the sample was collected for recall of patients for confirmatory testing.
When are newborn screening results available?
Newborn screening can be done by a physician, a nurse, a midwife or medical technologist.
Who will collect the sample for newborn screening
Newborn screening is available in participating health institutions (hospitals, lying-ins, Rural Health Units and Health Centers). If babies are delivered at home, babies may be brought to the nearest institution offering newborn screening.
Where is newborn screening available?
1. Congenital Hypothyroidism (CH) CH results from lack or absence of thyroid
hormone, which is essential to growth of the brain and the body. If the disorder is not detected and hormone replacement is not initiated within (4) weeks, the baby's physical growth will be stunted and she/he may suffer from mental retardation.
What are the disorders included in the Newborn Screening Package?
2. Congenital Adrenal Hyperplasia (CAH) CAH is an endocrine disorder that causes severe salt lose, dehydration and abnormally high levels of male sex hormones in both boys and girls. If not detected and treated early, babies may die within 7-14 days.
3. Galactosemia (GAL)GAL is a condition in which the body is unable to process galactose, the sugar present in milk. Accumulation of excessive galactose in the body can cause many problems, including liver damage, brain damage and cataracts.
4. Phenylketonuria (PKU)PKU is a metabolic disorder in which the body cannot properly use one of the building blocks of protein called phenylalanine. Excessive accumulation of phenylalanine in the body causes brain damage.
5. Glucose-6-Phosphate Dehydrogenase Deficiency (G6PD Def)G6PD deficiency is a condition where the body lacks the enzyme called G6PD. Babies with this deficiency may have hemolytic anemia resulting from exposure to certain drugs, foods and chemicals.
Babies with positive results should be referred at once to the nearest hospital or specialist for confirmatory testing and further management. Should there be no specialist in the area, the NBS secretariat office will assist its attending physician.
What should be done when a baby is tested a positive NBS result?
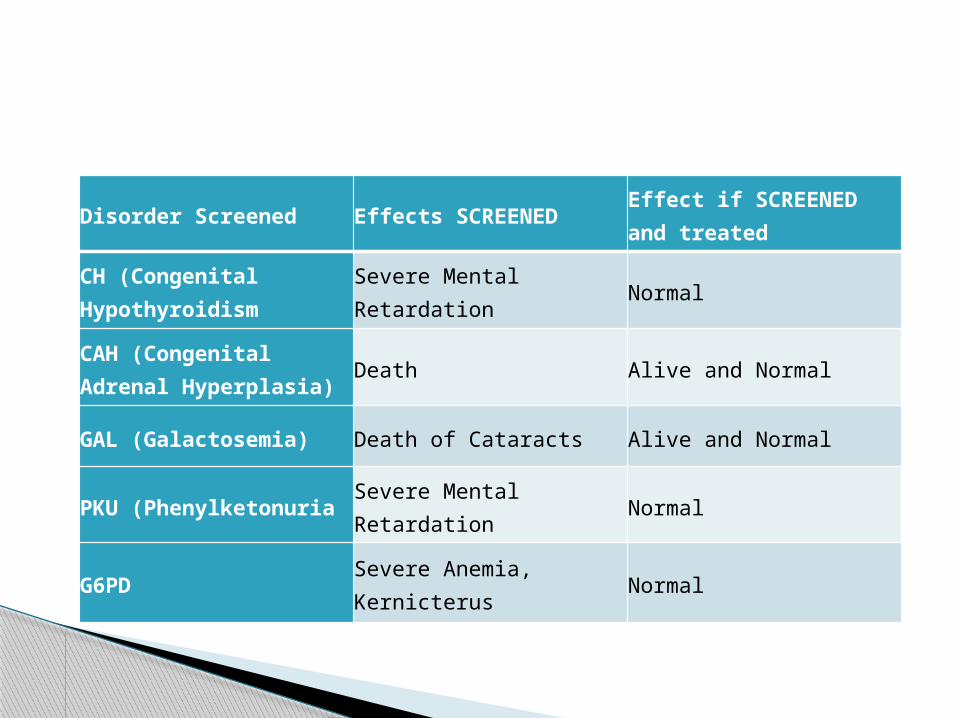
Disorder Screened Effects SCREENEDEffect if SCREENED and treated
CH (Congenital Hypothyroidism
Severe Mental Retardation
Normal
CAH (Congenital Adrenal Hyperplasia)
Death Alive and Normal
GAL (Galactosemia) Death of Cataracts Alive and Normal
PKU (PhenylketonuriaSevere Mental Retardation
Normal
G6PDSevere Anemia, Kernicterus
Normal