-
Association of Maternal and Child Health Programs Conference
February 14, 2012
Healthy Babies Initiatives
David Lakey, M.D.CommissionerTexas Department of State Health
Services
-
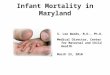
Infant Mortality 2008Preterm Births 2008*
-
Medicaid Costs>55% of all Texas births (225,000) paid by
Medicaid$2.2 billion per year in birth and delivery-related
services for moms and infants through first year ~70% of Medicaid
costs for hospitalized newborns tied to billing codes for
prematurityInfant care costs growing by ~10% per year50% are
attributable to extremely preterm infantsNewborn costs (1st
year)Extreme Preterm infant: $63,124Term infant: $404
**
-
Preconception Health Health Behaviors Perinatal CarePrenatal
Care High Risk Referral Obstetric CarePerinatal Management Neonatal
Care Pediatric SurgerySafe Sleep Breast Feeding Injury
PreventionPossible Points for Intervention**
-
Healthy Texas BabiesHealthy Texas Babies (HTB) is an initiative
to decrease infant mortality in Texas
Goals of Healthy Texas Babies Initiative:
Provide local partnerships and coalitions with major roles in
shaping programs in their communitiesUse evidence-based
interventionsDecrease preterm birth rate by 8% over 2 yearsSave ~
$7.2 million in Medicaid costs over 2 years
*
-
Healthy Texas Babies*
-
Legislature appropriated $4.1 million in General Revenue funds
to DSHS to fund the Healthy Texas Babies Initiative
Legislature passed three related perinatal health billsHB 1983
Develop quality initiatives and implement cost-cutting measures to
reduce elective inductions and c-sections before the 39th week in
Medicaid HB 824 Creates an outreach campaign to promote fathers'
involvement with their children before birthHB 2636 Creates a
council to study neonatal intensive care units to develop standards
and recommendations for Medicaid reimbursement2011 Texas
Legislative Actions*
-
ASTHO 2011 Presidential Challenge Improve birth outcomes by
reducing infant mortality and prematurity in the United States
Objectives:Focus on improving birth outcomes as SHOs and state
leadership teams work with state partners on health and community
system changesCreate a unified message that builds on the best
practices from around the nationDevelop clear measurements to
evaluate targeted outreach, progress, and return on investment
*S.M.A.R.T. Challenge:Reduce preterm births by 8% by 2014
-
One Roadmap to Reducing Prematurity by 8% by 2014Reduce
non-medically indicated elective inductions and cesarean sections
prior to 39 weeks gestation. Reduction of 25,000 PTBEnsure
universal access to 17P for eligible women. Reduction of 10,000
PTBEliminate the incidence of higher order multiples due to
assistive reproductive technologies, 97 percent of whom are born
pretermReduction of 2,300 PTBReduce rates of smoking among pregnant
women by 10 percent. Reduction of 1,300 PTB
*
-
HRSA Region IV &VI Summit onInfant MortalityJanuary 12-13,
20127 member State Teams State Health Officials, MCH Directors and
other MCH experts, State Medicaid Officials, March of Dimes,
Hospitals, Legislative and Governors Office senior staffFederal
partners HRSA, CMS, CDCRegional Goals and State Strategies
*
-
DRAFT STRATEGIES FOR A REGIONAL APPROACH TO REDUCING INFANT
MORTALITY AND PREMATURITY
Implement state policy change to eliminate elective inductions
and c sections prior to 39 weeks gestationHospital PoliciesPayment
Medicaid (Waivers)Individual, Provider EducationImprove access to
care for all women o reproductive age including 17-P as clinically
indicatedDevelop and implement a regional campaign to address the
following aspects of womens health:Life Course Health
preconception/pregnancy/inter-conceptionSmoking cessation,
especially for pregnant womenChronic conditions obesity and
diabetesInfluenza immunizations for pregnant womenSafe Sleep
*
-
Since the SummitState Teams are continuing their workMeeting
together to develop and implement next steps Alabama, Georgia,
Kentucky, Texas
State Summit In the Works Oklahoma
Sharing practical tools like economic impact calculation
formulas, hospital policies, legislative language
*
-
ASTHO Current Activities Current CommitteesSteering
CommitteeData and Best Practices/Policy CommitteesCommunication and
Marketing CommitteeStrong CollaborationHRSA, AMCHP, March of Dimes,
Leap Frog, National Association of Medicaid Directors, AHA,
Secretaries Advisory Committee on Infant Mortality, CDC, CMS
*
-
ASTHO WebsiteASTHO website with matrix of current emerging,
promising and best practices will be available soon Facilitating
use of a menu of strategies for varying levels of intervention
linked to concrete implementation steps and detailed resource
informationOther resources will include case studies and commentary
from state leaders Guide, create or strengthen state partnerships
and fine-tune current programs The ASTHO site will also link to
tool kits on best practices created by AMCHP and March of Dimes
*
-
ConclusionRates of prematurity and infant mortality are much
higher then they should beThe cost of prematurity is very high,
measured in both human and economic costsThere are proven methods
states can use to combat these public health issuesWe will not be
successful unless we work together
*
-
Thank You!*
*Source: National Center for Health Statistics, final mortality
data, 1990-1994 and period linked birth/infant death data,
1995-present.
*Texas Medicaid covers 3 million Texans primarily low-income
families with children, pregnant women, the elderly and people with
disabilities. Pregnant women are covered up to 185 percent of the
federal poverty level. Non-citizens are not eligible for Medicaid
(except emergency Medicaid). More than 55 percent (225,000) of all
births in Texas are paid by Medicaid. Medicaid currently spends
over $2.2 billion per year in birth and delivery-related services
for moms and infants through their first year ($22 billion total
program services costs in 2010).Also in Texas, Medicaid costs
related to infant care are growing almost 10 percent per year.
Neonatal Intensive Care Unit utilization is growing faster than
expected. Over 50 percent of costs are attributable to extremely
preterm infants, who account for about 2 percent of births.
Extremely preterm infants are less than 28 weeks gestation or have
a birth weight under 1,000 grams. The average cost per claim for
extremely premature infants was $63,124, compared with $404 for a
normal newborn claim, based on Medicaid diagnosis-related group
billing codes.*Thank you for the opportunity to participate in our
Healthy Babies Presidential challenge at the upcoming Association
of State and Territorial Health Officials (ASTHO) meeting in
Portland. As promised, I am providing a formulation of how a
national goal of 8% reduction in rates of preterm birth (PTB) could
be achieved by 2014.
Many of the causes of PTB remain unknown, but evidence is
mounting that bold public health leadership can effect meaningful
changes in communities among clinicians and consumers, that
decrease the incidence of preterm birth and reduce its associated
harms and costs. Extensive analytic work prepared by MODs Perinatal
Data Center demonstrates that aggressive but reasonable activity in
four areas of intervention could yield the 8 percent reduction in
PTB rates that you envision. Models using national statistics,
peer-reviewed findings on evidence-based interventions, and
pre-published analyses by MOD on community-based interventions,
yield the following blueprint that we believe can guide individual
jurisdictions toward that 8 percent reduction. Considerations can,
of course, vary by locale.
1.Ensure universal access to 17P for eligible women. (Reduction
of 10,000 PTB)
Recently approved by the FDA for this purpose, 17 alpha
hydroxyprogesterone caproate ( 17P) has been demonstrated to reduce
subsequent PTB by 33% percent among women with PTB history who
received prenatal care during weeks 16-20 of pregnancy (Meis, et
al.,2003). Petrini and colleagues estimated that 10,000 of the
nations half million preterm births would be prevented annually if
all eligible women who sought prenatal care during the critical
gestational period received 17P. Even more preterm births could be
prevented if a higher proportion of women received early prenatal
care. This study predated FDA approval of the injection form of 17P
and the clinical trials of its vaginal gel form intended for women
with short cervix, which could result in even greater
reductions.
ASTHO leadership can increase the appropriate clinical use of
17P in two ways: first, by working with public and private payers
to eliminate access barriers to this important drug; and second, by
working through traditional means to get more pregnant women into
prenatal care during the critical gestational stage. We believe
that universal access to 17P, which may be within the reach of bold
and effective ASTHO leaders in their own jurisdictions, together
with higher rates of early prenatal care could yield 10,000 fewer
preterm births annually across the nation if applied
universally.
2.Eliminate the incidence of higher order multiples due to
assistive reproductive technologies (ART), 97 percent of whom are
born preterm. (Reduction of 2,300 PTB)
Nearly 35,000 preterm births annually are attributable to
assistive reproductive technologies (ART) and non-ART infertility
treatments that result in twins or higher order multiples. More
than 65% of twins and 97% of triplets and higher order multiples
that result from ART are delivered prematurely (CDC, 2009). While
it may be difficult during this next three years for ASTHO leaders
to effect sufficient change in the ART industry to reduce
substantially the incidence of twins, we believe that there is
sufficient political will to eliminate the triple (and higher)
embryo transfers that result in nearly 2,300 preterm births
annually. The state of the science has advanced in recent years to
yield reasonably high rates of implantation success from single
embryo transfer, and the evidence of harm from higher order
multiples is adequately documented to launch a successful statewide
campaign against the risky industry practice of triple embryo
transfer. ASTHO leadership and activism, therefore, has a realistic
probability of eliminating 2300 preterm births attributable higher
order multiples. If successful, this campaign may also reduce the
incidence of twins, who are also at higher risk for PTB.
3.Reduce rates of smoking among pregnant women by 10 percent.
(Reduction of 1,300 PTB)
The linkage between smoking and PTB is well established, as is
the benefit of smoking cessation for pregnant women. In its
landmark demonstration project Healthy Babies are Worth the Wait
(HBWW), conducted in Kentucky over the past four years, readily
available community-based smoking cessation initiatives executed
led by the Kentucky Department for Public Health, in partnership
with participating hospitals, and March of Dimes resulted in a 10
percent reduction in smoking among women delivering over the study
period. Based on estimates of the contribution of maternal smoking
to preterm delivery (Shah and Bracken, 2000), an estimated 12,700
babies nationwide are born premature as a direct result of smoking
during pregnancy. A 10 percent reduction in maternal smoking could
prevent nearly 1,300 preterm births annually nationwide. Many of
your ASTHO colleagues hold key positions in their jurisdictions to
launch these initiatives in partnership with local hospitals and
March of Dimes chapters. We learned from HBWW that such
partnerships can be effective.
4.Reduce non-medically indicated elective inductions and
cesarean sections prior to 39 weeks gestation. (Reduction of 25,000
PTB)
In 2010, the Joint Commission established a new perinatal care
core measure set that includes the number of elective deliveries
(both vaginal and cesarean) performed at >37 and