Embed Size (px)
Citation preview
Increased incidence of EBV-related disease following paediatricstem cell transplantation with reduced-intensity conditioning
Epstein–Barr virus (EBV) is a c-herpes virus with B lympho-
cyte-specific tropism that causes significant clinical problems
in immunosuppressed patients of all ages. Following haema-
topoietic stem cell transplantation (HSCT), EBV reactivation
and related disease are a recognized complication, with an
incidence of 0Æ6–26%, which is higher in the context of
selective T-cell depletion (TCD; Antin et al, 1991; Lucas et al,
1998; Micallef et al, 1998; van Esser et al, 2001a).
EBV may be associated with a spectrum of clinical presen-
tations, from fever to lymphoproliferative disease (LPD),
which arise as a consequence of an outgrowth of B cells latently
infected with EBV in the setting of loss or suppression of
normal cytotoxic T-cell surveillance. LPD itself has a heterog-
enous clinico-pathological presentation, ranging from poly-
morphic hyperplasia to diffuse large B-cell lymphoma.
Established LPD post-HSCT is associated with a high mortality
and morbidity (Gross et al, 1999). With improved monitoring
and detection of EBV viraemia using polymerase chain
reaction (PCR)-based techniques, more accurate analysis of
the risk factors associated with EBV-related disease following
HSCT is now possible (Rooney et al, 1998; Milpied et al, 2000;
van Esser et al, 2002).
Several reports have attempted to define HSCT risk factors
that predispose to the development of EBV-LPD. A multicen-
tre retrospective analysis of over 18 000 transplants identified
the use of an unrelated donor, greater than single human
leucocyte antigen (HLA)-mismatch, TCD of the graft, use of
antithymocyte globulin (ATG) or anti-CD3 in vivo or the
presence of graft-versus-host disease (GvHD) as independent
risk factors (Curtis et al, 1999). In another single-centre
retrospective analysis of 2150 transplants, TCD, HLA-mis-
match, the use of ATG in vivo and primary immunodeficiency
(PID) as an underlying disease, were identified as independent
risk factors (Bhatia et al, 1996). Several other reports have
Jonathan Cohen, 1* Minal Gandhi, 1*
Paru Naik,1 David Cubitt,2 Kanchan
Rao,1 Urvashi Thaker,2 E. Graham
Davies,3 H. Bobby Gaspar, 3,4 Persis J.
Amrolia1,4 and Paul Veys1
Departments of 1Bone Marrow Transplantation,2Virology and 3Clinical Immunology, Great
Ormond Street Hospital NHS Trust, London, and4Molecular Immunology Unit, Institute of Child
Health, University College London, London, UK
Received 18 November 2004; accepted for
publication 26 January 2005
*These authors contributed equally to this study.
Correspondence: Dr Persis J. Amrolia,
Department of Bone Marrow Transplantation,
Great Ormond St Hospital, Great Ormond St,
London WC1N 3JH, UK.
E-mail: [email protected]
Summary
The incidence of Epstein–Barr virus (EBV) viraemia and lymphoproliferative
disease (LPD) was studied in a consecutive cohort of 128 paediatric patients
undergoing stem cell transplantation (SCT) with reduced-intensity
conditioning (RIC; n ¼ 65) or conventional-intensity conditioning (CIC;
n ¼ 68). Following CIC, six of 68 (8%) developed viraemia; all remained
asymptomatic. EBV viraemia (23 of 65 patients ¼ 35%, P < 0Æ001) and LPD
(10 of 65 ¼ 15%, P < 0Æ001) were significantly more frequent following RIC.
Of the 23 RIC patients who developed viraemia, eight remained
asymptomatic, five had symptomatic viraemia (fever ± rash), and 10
patients developed LPD, two of whom died. An absolute lymphocyte count
of <0Æ3 · 109/l at the time of onset of viraemia was strongly predictive of
development of LPD (P < 0Æ05) in this group. The incidence of viraemia was
significantly higher in patients receiving serotherapy with antithymocyte
globulin (ATG; 15 of 43, 35%) than Campath (12 of 73, 16Æ4%, P < 0Æ05).
Primary immunodeficiency and acute graft-versus-host disease were
associated with EBV viraemia in univariate analysis, but were not
independent risk factors. In conclusion, EBV viraemia and LPD appear to
be significantly more common in children following RIC SCT, particularly
with selective depletion of recipient T cells relative to B cells following the use
of ATG. This probably reflects the profound immunosuppression following
RIC SCT, together with the incomplete ablation of recipient-derived B cells.
Keywords: Epstein–Barr virus, lymphoproliferative disease, reduced-inten-
sity conditioning, stem cell transplant, viraemia.
research paper
ª 2005 Blackwell Publishing Ltd, British Journal of Haematology, 129, 229–239 doi:10.1111/j.1365-2141.2005.05439.x
confirmed that selective depletion of T cells, rather than both
T- and B-cell populations, from the graft and HLA-mismatch
increase the risk of EBV-LPD (Hale & Waldmann, 1998; Meijer
et al, 2002). In these reports, the majority of patients treated
were adults and only EBV-LPD rather than other EBV-
associated morbidity was documented. In all these studies
conventional myeloablative conditioning regimes (CIC) were
used for cytoreduction.
Increasing numbers of SCTs are now performed using non-
myeloablative or reduced-intensity conditioning (RIC)
regimes, which are designed to produce a state of profound
immunosuppression rather than myeloablation. RIC has been
used with good results for the treatment of both malignant and
non-malignant haematological conditions in adults and chil-
dren (Slavin et al, 1998; Gross et al, 1999; Amrolia et al, 2000).
To date, very little data has been reported regarding the
incidence of EBV-related disease following RIC, although
evidence suggests that LPD maybe problematic in this setting.
A single, fatal case LPD following RIC (Milpied et al, 1999) and
a series of 30 RIC transplants, one of which led to LPD, have
recently been described (Ho et al, 2002). Furthermore, the
delayed recovery of EBV-specific cytotoxic T-lymphocytes
following a RIC fludarabine/Campath 1H regime when com-
pared with conventional conditioning regimes, may predispose
to higher incidence of EBV disease (Chakrabarti et al, 2003).
Serial PCR-based monitoring for EBV in the blood of
patients following HSCT (Lucas et al, 1998; Hoshino et al,
2001) has enabled accurate determination of EBV viral load
and prediction of patients at risk of progression to overt EBV-
LPD. Pre-emptive antiviral or anti-B-cell therapies are there-
fore now regularly used and have been shown to be successful
in preventing LPD (van Esser et al, 2001b, 2002; Lankester
et al, 2002). As a result, it is increasingly difficult to use EBV-
LPD incidence as the outcome measure in studies looking at
risk factors for its development. However, demonstrating risk
factors that predispose to EBV viraemia following transplant
will be of great use in identifying patients at increased risk of
EBV-related disease.
This series is the largest reported to date, of EBV-related
disease following HSCT in paediatric patients. We compared the
incidence of EBV viraemia in a cohort of 128 patients undergoing
allogeneic SCT with CIC or RIC at our institution. In addition,
we examined the role of potential risk factors, including PID as
an underlying diagnosis, TCD and serotherapy and degree of
HLA-mismatch, in the development of EBV-related disease. We
demonstrated for the first time that EBV-related disease is
significantly higher following RIC compared with CIC.
Methods
Patients
From January 1999, all children undergoing allogeneic SCT at
Great Ormond Street Hospital, London, were screened for
EBV viraemia by DNA-PCR weekly until the circulating CD4
count was > 0Æ3 · 109/l, and were monitored for clinical
features attributable to EBV. A total of 133 allogeneic
transplants were performed on 128 patients between January
1999 and June 2002, with five patients undergoing two
transplants during this period. Their details are shown in
Table I. Ages ranged from 0 to 17Æ7 years (median: 4Æ1). About
42 patients (32Æ8%) were transplanted for haematological
Table I. Details of 133 allogeneic HSCT between January 1999 and
June 2002, by intensity of conditioning.
RIC CIC Total P-value
N 65 68 133
Female (%) 49Æ2 50 NS*
Age range,
years (median)
0Æ19–17Æ7(5Æ17)
0Æ23–13Æ4(3Æ58)
0Æ19–17Æ7(4Æ08)
0Æ149**
Disease
MH 5 37 42 <0Æ001*
NMH 15 14 29
PID 41 8 49
Other 4 9 13
Donor
Haplo 4 11 15 NS*
MMUD 14 11 25
MMFD 1 0 1
MMSD 1 0 1
MUD 25 20 45
MFD 7 7 14
MSD 13 19 32
Cells
BM 58 54 112 NS*
PBSC 6 13 19
BM + PBSC 1 0 1
Cord 0 1 1
TCD
Yes 4 29 33 <0Æ001*
No 61 39 100
Serotherapy
ATG 30 13 43 <0Æ001*
Campath 1G 0 15 15
Campath 1H 34 24 58
Neither 1 16 17
Mixed chimaeras (%)
At 6 weeks 37 14Æ5 24Æ8 <0Æ05*
At 12 weeks 37Æ3 28Æ3 33 <0Æ05*
CIC, conventional-intensity conditioning; RIC, reduced-intensity
conditioning; MH, malignant haematology; NMH, non-malignant
haematology; PID, primary immunodeficiency; MMUD, HLA-mis-
matched unrelated donor; MMFD, HLA-mismatched family donor;
MMSD, HLA-mismatched sibling donor; MUD, HLA-matched unre-
lated donor; MFD, HLA-matched family donor; MSD, HLA-matched
sibling donor; BM, bone marrow; PBSC, peripheral blood stem cells;
TCD, ex vivo T-cell depletion; ATG, antithymocyte globulin; NS, no
significant difference at 5% level; HSCT, haematopoietic stem cell
transplantation.
*Comparison between RIC and CIC groups made by chi-squared or
Fisher’s exact test, with P-value shown.
**P-value from unpaired t-test.
J. Cohen et al
230 ª 2005 Blackwell Publishing Ltd, British Journal of Haematology, 129, 229–239

malignancy, 27 (21Æ1%) for non-malignant haematological
disease, 47 (36Æ7%) for PID and 12 (9Æ4%) for metabolic and
other disorders.
Conditioning and matching of RIC/CIC groups
The conditioning regimes were categorized as myeloablative
CIC (n ¼ 68) or non-myeloablative RIC (n ¼ 65). Of the CIC
patients, 30 received conditioning incorporating total body
irradiation, whereas 38 received chemotherapy-alone regimens
(busulphan 16 mg/kg + cyclophosphamide 200 mg/kg,
n ¼ 22; busulphan 16 mg/kg + cyclophosphamide
120 mg/kg + melphalan 140 mg/m2, n ¼ 9; fludarabine
150 mg/m2 + busulphan 16 mg/kg + melphalan 140 mg/m2,
n ¼ 7). Fifty-nine of the 65 RIC transplants used fludarabine-
based regimens and the majority of these were with fludarabine
150 mg/m2 + melphalan 140 mg/m2. Only four of 65 RIC
transplants used an in vitro TCD graft, compared with 29 of
the 68 CIC transplants. The CIC and RIC groups were matched
for sex, donor type and cell source. There was a slight
difference in age between the two groups (median 5Æ17 years
for RIC, 3Æ58 years for CIC). The CIC group contained a larger
proportion of patients treated for malignant haematological
conditions than the RIC group (54Æ4% vs. 7Æ7%), whereas the
RIC group contained more patients with primary deficiency
than the CIC group (63Æ1% vs. 11Æ8%). Differences between
the groups with regard to in vitro TCD, in vivo serotherapy and
the presence of mixed chimaerism are discussed further below.
Grafts
Of the 133 allogeneic transplants, 91 involved a fully HLA-
matched donor: matched sibling donor (n ¼ 45); matched
family donor (n ¼ 14); matched unrelated donor (n ¼ 32).
Forty-two were HLA-mismatched: 1-antigen (Ag) mismatched
family donor (n ¼ 2); 1-Ag mismatched unrelated donor
(MUD; n ¼ 25); haplo-identical donor (n ¼ 15). Bone mar-
row was used as the stem cell source in 112 transplants and 19
patients received peripheral blood stem cells. One patient
received both bone marrow and peripheral blood stem cells.
One patient received cord blood. In vitro TCD was performed
in 33 grafts (Campath 1M + T-cell addback, n ¼ 18; Miltenyi,
n ¼ 15). Only four of 65 (6Æ2%) RIC transplants involved
in vitro TCD of the graft compared with 29 of 68 (46Æ2%) CIC
transplants.
Serotherapy
One hundred and sixteen patients of the 133 also received
serotherapy in vivo with conditioning to reduce rejection and
GvHD: 43 with ATG, 73 with Campath (Campath 1G, n ¼ 15;
Campath 1H, n ¼ 58). In 1999 and early 2000, MUD patients
received Campath 1G. Because of observed high incidence of
EBV in RIC patients, Campath 1H 0Æ2 mg/kg · 5 doses was
used as serotherapy in RIC patients from December 1999, and
from June 2000 onwards, all patients receiving in vivo
Campath, received Campath 1H. As a result of this, RIC
patients were more likely to have received ATG than CIC
patients (30 of 65, 46Æ2% vs. 13 of 68, 19Æ1%), less likely to
have received Campath 1G (zero of 65, 0% vs. 15 of 68, 22Æ1%)
and more likely to have received Campath 1H (34 of 65, 52Æ3%
vs. 24 of 68, 35Æ3%). Sixteen of 68 (23Æ5%) CIC patients
received no serotherapy compared with only one of 65 (1Æ5%)
RIC patients.
Chimaerism
Thirty-seven per cent RIC patients had mixed chimaerism at
both 6- and 12-weeks post-transplant, compared with 14Æ5 and
28Æ3% in CIC patients.
EBV detection
All patients had weekly DNA-PCR monitoring for EBV,
cytomegalovirus (CMV) and adenovirus. This was continued
until CD4+ cell counts were >0Æ3 · 109/l. Semi-quantitative
analysis for EBV viral load was also performed if weekly
monitoring proved persistently positive in both blood and
plasma. DNA was extracted from 200 ll of whole blood in
ethylenediaminetetraacetic acid (EDTA) or plasma using the
QIAamp DNA blood minikit (Qiagen Ltd, Crawley, UK)
according to the manufacturer’s instructions.
For EBV detection, a PCR using primers IR1a-5¢ and IR1a-
3¢, which amplify a specific region of 288 bp within the
internal repeat (IR), was performed as previously described
(Shroff et al, 2002). Negative and positive controls were
included in each run. If EBV-DNA was detected in whole
blood, a semi-quantitative assay to determine viral load was
performed the following day on plasma using log-dilution,
comparing with known dilutions of a plasmid containing the
IR region. The threshold of detection of the assay was found to
be approximately 100 DNA copies/ml when samples were run
in parallel with an external laboratory that uses a light cycler
for quantification and EBV-infected cells (10 genomic EBV-
DNA copies/cell). The presence of EBV-DNA was regarded as
significant if it was detected in plasma as well as whole blood,
indicating reactivation and probable lytic replication of latent
virus within B cells. This is referred to as EBV viraemia, below.
Disease classification and treatment
All patients were closely monitored for clinical features
attributable to EBV infection. Those with EBV viraemia were
categorized as either (i) asymptomatic, (ii) symptomatic
viraemia (culture-negative fever with or without rash) or
(iii) LPD. EBV-LPD was subclassified clinically as either
localized or disseminated and lymphadenopathic or lympho-
matous, according to the Pittsburgh classification (Nalesnik,
1998). Biopsy specimens were classified according to the
World Health Organization (WHO) classification (Harris et al,
EBV Disease after Reduced-intensity Transplantation
ª 2005 Blackwell Publishing Ltd, British Journal of Haematology, 129, 229–239 231
1999). The presence of EBV in biopsy samples was investigated
using in situ hybridization for EBV-encoded RNAs (EBERs).
Patients with viraemia or LPD were treated initially with
withdrawal of immunosuppression ± antivirals. If there was
no response, patients were treated with rituximab 375 mg/m2
weekly for one to four doses until resolution of viraemia and/
or complete resolution of LPD.
Statistical analysis
In the comparison of baseline characteristics of the RIC and
CIC groups, chi-squared or Fisher’s exact tests were used for
non-parametric variables. Student’s t-test was used for para-
metric variables.
Overall survival was analysed using a Cox proportional
hazards model. Survival in patients with EBV viraemia post-
transplant was compared to those without viraemia. A further
comparison was made between those who developed LPD and
those who had EBV viraemia without developing LPD.
A univariate analysis was performed looking at the odds of
developing EBV viraemia or LPD with respect to the following
factors: RIC versus CIC; presence or absence of PID; use of
Campath or ATG or neither (comparing ATG versus nothing,
Campath versus nothing and ATG versus Campath); HLA-
mismatched donor (yes/no); unrelated donor (yes/no); in vitro
TCD (yes/no); acute GvHD (aGvHD; yes/no); chronic GvHD
(cGvHD; yes/no); chimaerism at 6-weeks post-transplant
(mixed/full) and chimaerism at 12-week post-transplant
(mixed/full). Using chi-square or Fisher’s exact test, factors
that showed a statistically significant effect on the odds of EBV
infection or LPD at the 10% level, were considered for
inclusion in a bivariate logistic regression analysis that
included RIC versus CIC. Each factor was considered in turn
and the likelihood ratio test was used to determine if the factor
was statistically significant in the model. If it was statistically
significant at the 5% level, it was considered for inclusion in a
multivariate model.
Results
EBV viraemia and disease manifestations following HSCT
The incidence of EBV viraemia and EBV disease was greater
after RIC HSCT than CIC HSCT. Only six patients (8Æ8%) in
the CIC HSCT cohort developed viraemia. They all remained
asymptomatic and none progressed to EBV disease. Of the 65
patients receiving RIC HSCT, 23 (35%) had EBV viraemia at a
median time of 2 months following transplant (range: 4 d to
13 months). Their median age was 6Æ3 years (range: 0Æ46–17Æ7)
with a similar male/female ratio (11 male, 12 female). The
median time to neutrophil engraftment did not differ between
those who had EBV detected (10–31 d, median 14) and those
who did not (10–21 d, median 14).
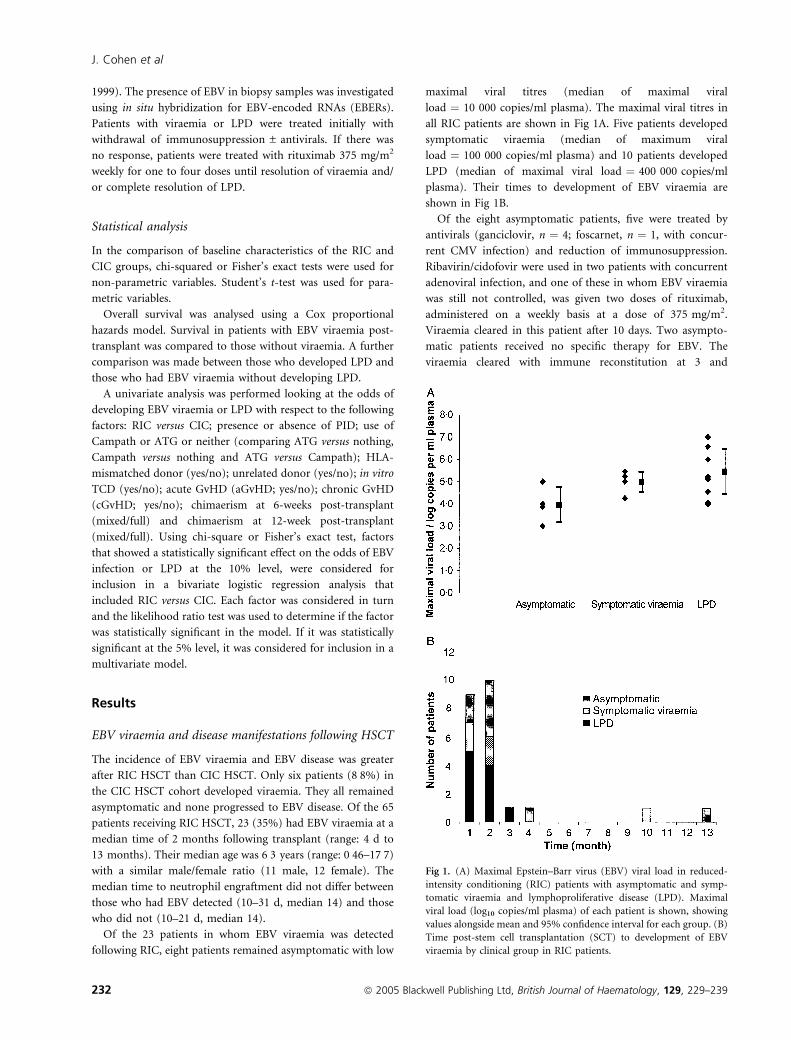
Of the 23 patients in whom EBV viraemia was detected
following RIC, eight patients remained asymptomatic with low
maximal viral titres (median of maximal viral
load ¼ 10 000 copies/ml plasma). The maximal viral titres in
all RIC patients are shown in Fig 1A. Five patients developed
symptomatic viraemia (median of maximum viral
load ¼ 100 000 copies/ml plasma) and 10 patients developed
LPD (median of maximal viral load ¼ 400 000 copies/ml
plasma). Their times to development of EBV viraemia are
shown in Fig 1B.
Of the eight asymptomatic patients, five were treated by
antivirals (ganciclovir, n ¼ 4; foscarnet, n ¼ 1, with concur-
rent CMV infection) and reduction of immunosuppression.
Ribavirin/cidofovir were used in two patients with concurrent
adenoviral infection, and one of these in whom EBV viraemia
was still not controlled, was given two doses of rituximab,
administered on a weekly basis at a dose of 375 mg/m2.
Viraemia cleared in this patient after 10 days. Two asympto-
matic patients received no specific therapy for EBV. The
viraemia cleared with immune reconstitution at 3 and
Fig 1. (A) Maximal Epstein–Barr virus (EBV) viral load in reduced-
intensity conditioning (RIC) patients with asymptomatic and symp-
tomatic viraemia and lymphoproliferative disease (LPD). Maximal
viral load (log10 copies/ml plasma) of each patient is shown, showing
values alongside mean and 95% confidence interval for each group. (B)
Time post-stem cell transplantation (SCT) to development of EBV
viraemia by clinical group in RIC patients.
J. Cohen et al
232 ª 2005 Blackwell Publishing Ltd, British Journal of Haematology, 129, 229–239

6 months respectively. The final patient, who had no symp-
toms of EBV disease, died of overwhelming pulmonary
aspergillosis with EBV-PCR detected in plasma prior to
specific therapy being instituted.
One patient with symptomatic viraemia responded to
treatment with ganciclovir and reduction of immunosuppres-
sion. The remaining four patients with symptomatic viraemia
did not respond to this, and were treated with rituximab as
described above (one dose, n ¼ 4; four doses, n ¼ 1), which
led to resolution of symptoms after a median of 13 d (range:
8–20) and clearance of viraemia after a median of 11 d (range:
4–29).
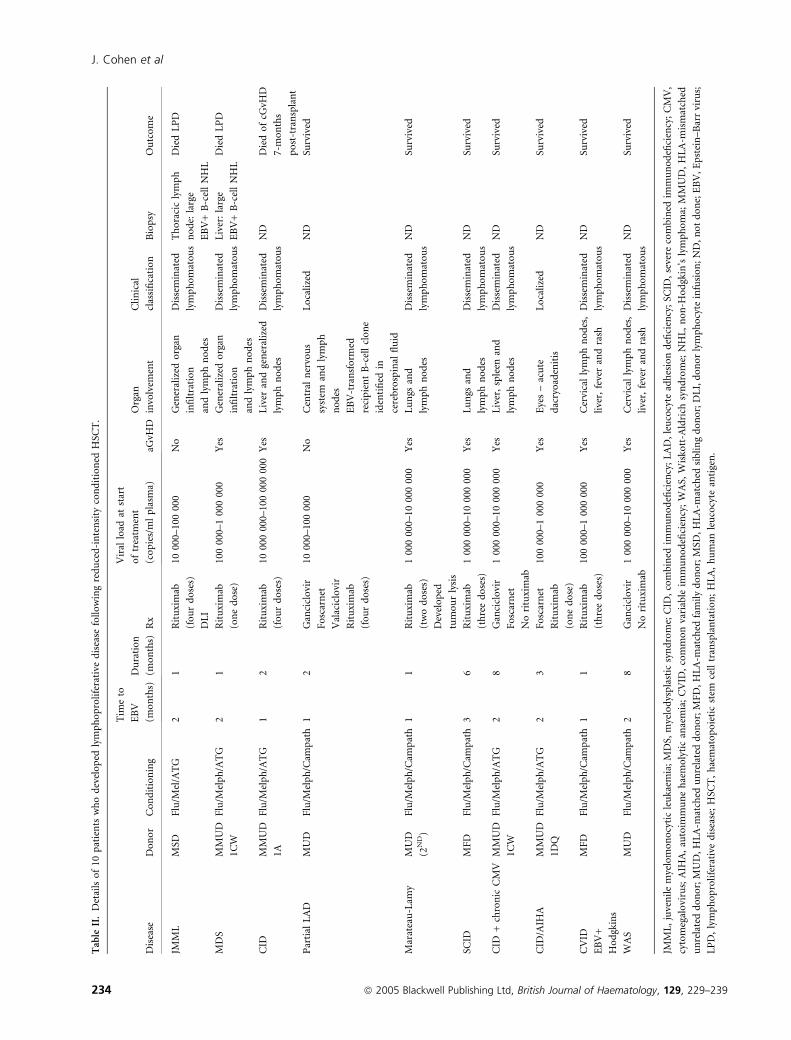
Ten patients developed LPD according to the Pittsburgh
criteria (Nalesnik, 1998). In two of the 10 patients, this was
limited to localized disease (central nervous system, n ¼ 1;
dacroadenitis, n ¼ 1). Both of these patients survived. The
remaining eight patients all had disseminated lymphomatous
disease. Viraemia commenced within 2 months of transplan-
tation in nine of the 10 patients and within 3 months for
patient 10. Two of the 10 patients responded to a reduction of
immunosuppression and treatment with antivirals (ganciclovir
alone in one patient; ganciclovir with foscarnet in one patient
with concurrent CMV viraemia). The other eight patients with
LPD were treated with rituximab. Six of the eight responded
with clinical resolution and reduction in viral load after 1–
4 weekly doses (median time to clinical complete response
23 d, range: 11–77), administered as described. There was
complete clearance of viraemia (<100 copies/ml plasma) in
these patients after a median time of 21 d (range: 9–36). One of
these patients, who was successfully treated with rituximab for
LPD, died of overwhelming GvHD 7 months after transplant.
The remaining two patients had progressive LPD that did not
respond to rituximab (one dose and three doses respectively) or
donor lymphocyte infusion (in one patient), with pulmonary/
airway involvement progressing to multiorgan failure and
death. They had both received RIC with fludarabine/melpha-
lan/ATG to treat myelodysplastic syndromes.
Rituximab was largely well tolerated, but noted to cause a
tumour lysis syndrome in one patient who had very high EBV
load (1 000 000 copies/ml) and bulky disease prior to therapy.
Eleven of 13 patients cleared viraemia, the patients who did
not died of progressive LPD. The median time to complete
clinical response was 20 d (range: 8–77) and to clearing
viraemia was 13 d (range: 4–36).
Two of the eight patients with disseminated lymphomatous
disease had a biopsy as part of their diagnostic work-up, one of
thoracic lymph node tissue, one a liver biopsy. Both demon-
strated monomorphic large B cell, EBV+, lymphomatous
disease according to the WHO criteria (Harris et al, 1999).
Both of these patients subsequently died. The source of the
proliferative B-cell clone was investigated in the two patients
with localized LPD by fluorescent in situ hybridization for sex
chromosomes (XY-FISH) and shown to be of recipient origin
in both cases. Further details of the 10 patients with LPD are
summarized in Table II.
In the 23 patients who developed viraemia following RIC, an
absolute lymphocyte count (ALC) of below 0Æ3 · 109/l at the
time of onset of viraemia was strongly predictive of develop-
ment of LPD [odds ratio (OR) ¼ 12Æ8; P < 0Æ05]. Further
details are shown in Table III.
There was a high incidence of co-infections at the time of
EBV viraemia. About 17 of the 23 patients had other viruses
detected in the same samples by PCR (EBV + CMV,
n ¼ 8; EBV + adenovirus, n ¼ 4; EBV + CMV + adenovirus,
n ¼ 5).
Survival analysis
Of the 29 patients who developed viraemia (RIC, n ¼ 23; CIC,
n ¼ 6), five had died at the time of analysis (82Æ8% survival).
Of the 104 patients without viraemia (RIC, n ¼ 42; CIC,
n ¼ 62), 33 had died (68% survival). Of the 10 patients within
the viraemic group who developed LPD, three died. When
analysed using a Cox proportional hazards model, there was
no statistically significant difference in overall survival between
those who developed viraemia post-transplant and those who
did not. Similarly there was no significant difference between
those who developed LPD, those with viraemia who did not
develop LPD and those who did not develop viraemia. Results
of this analysis are shown in Fig 2.
Risk factors associated with EBV detection or LPD
Univariate analysis. The incidences of EBV viraemia and LPD
in various groups and the unadjusted ORs for risk factors are
presented with 95% confidence intervals and chi-squared
statistics in Tables IV and V respectively, and are discussed in
further detail below.
Conditioning: RIC versus CICThe RIC was the risk factor
most strongly associated with EBV viraemia. Twenty-three of
65 patients (35Æ4%) with RIC developed EBV viraemia versus
six of 68 (8Æ8%) of those conventionally conditioned, with an
OR of 5Æ66 (P < 0Æ001). All of the patients that developed LPD
had received RIC (10 of 65, 15Æ4%, vs. zero of 68, 0%;
P < 0Æ001).
In vitro TCD. In vitro TCD using Campath 1M or CD34-
selection was associated with a lower incidence of EBV
viraemia (two of 33, 6Æ1% for TCD versus 27 of 100, 27Æ0%
for others; OR 0Æ17; P < 0Æ012) and none of these patients
developed LPD. Two of 15 patients whose grafts were prepared
by CD34 selection using the Miltenyi system developed
viraemia. Of the 18 patients whose grafts were treated with
ex vivo Campath 1M and T-cell addback, none developed
viraemia.
Serotherapy: Campath versus ATG Use of serotherapy was
associated with a higher incidence of EBV viraemia than in
those patients in whom serotherapy was not given (27 of 116,
23Æ3% vs. two of 17, 11Æ8%; not significant, NS). Patients
whose grafts were not TCD in vitro and did not receive in vivo
serotherapy had a lower incidence of EBV viraemia than those
EBV Disease after Reduced-intensity Transplantation
ª 2005 Blackwell Publishing Ltd, British Journal of Haematology, 129, 229–239 233
Table
II.
Det
ails
of
10p
atie
nts
wh
od
evel
op
edly
mp
ho
pro
life
rati
ved
isea
sefo
llo
win
gre
du
ced
-in
ten
sity
con
dit
ion
edH
SCT
.
Dis
ease
Do
no
rC
on
dit
ion
ing
Tim
eto
EB
V
(mo
nth
s)
Du
rati
on
(mo
nth
s)R
x
Vir
allo
adat
star
t
of
trea
tmen
t
(co
pie
s/m
lp
lasm
a)aG
vHD
Org
an
invo
lvem
ent
Cli
nic
al
clas
sifi
cati
on
Bio
psy
Ou
tco
me
JMM
LM
SDF
lu/M
el/A
TG
21
Rit
uxi
mab
(fo
ur
do
ses)
DL
I
1000
0–10
000
0N
oG
ener
aliz
edo
rgan
infi
ltra
tio
n
and
lym
ph
no
des
Dis
sem
inat
ed
lym
ph
om
ato
us
Th
ora
cic
lym
ph
no
de:
larg
e
EB
V+
B-c
ell
NH
L
Die
dL
PD
MD
SM
MU
D
1CW
Flu
/Mel
ph
/AT
G2
1R
itu
xim
ab
(on
ed
ose
)
100
000–
100
000
0Y
esG
ener
aliz
edo
rgan
infi
ltra
tio
n
and
lym
ph
no
des
Dis
sem
inat
ed
lym
ph
om
ato
us
Liv
er:
larg
e
EB
V+
B-c
ell
NH
L
Die
dL
PD
CID
MM
UD
1A
Flu
/Mel
ph
/AT
G1
2R
itu
xim
ab
(fo
ur
do
ses)
1000
000
0–10
000
000
0Y
esL
iver
and
gen
eral
ized
lym
ph
no
des
Dis
sem
inat
ed
lym
ph
om
ato
us
ND
Die
do
fcG
vHD
7-m
on
ths
po
st-t
ran
spla
nt
Par
tial
LA
DM
UD
Flu
/Mel
ph
/Cam
pat
h1
2G
anci
clo
vir
Fo
scar
net
Val
acic
lovi
r
Rit
uxi
mab
(fo
ur
do
ses)
1000
0–10
000
0N
oC
entr
aln
ervo
us
syst
eman
dly
mp
h
no
des
EB
V-t
ran
sfo
rmed
reci
pie
nt
B-c
ell
clo
ne
iden
tifi
edin
cere
bro
spin
alfl
uid
Lo
cali
zed
ND
Surv
ived
Mar
atea
u-L
amy
MU
D
(2N
D)
Flu
/Mel
ph
/Cam
pat
h1
1R
itu
xim
ab
(tw
od
ose
s)
Dev
elo
ped
tum
ou
rly
sis
100
000
0–10
000
000
Yes
Lu
ngs
and
lym
ph
no
des
Dis
sem
inat
ed
lym
ph
om
ato
us
ND
Surv
ived
SCID
MF
DF
lu/M
elp
h/C
amp
ath
36
Rit
uxi
mab
(th
ree
do
ses)
100
000
0–10
000
000
Yes
Lu
ngs
and
lym
ph
no
des
Dis
sem
inat
ed
lym
ph
om
ato
us
ND
Surv
ived
CID
+ch
ron
icC
MV
MM
UD
1CW
Flu
/Mel
ph
/AT
G2
8G
anci
clo
vir
Fo
scar
net
No
ritu
xim
ab
100
000
0–10
000
000
Yes
Liv
er,
sple
enan
d
lym
ph
no
des
Dis
sem
inat
ed
lym
ph
om
ato
us
ND
Surv
ived
CID
/AIH
AM
MU
D
1DQ
Flu
/Mel
ph
/AT
G2
3F
osc
arn
et
Rit
uxi
mab
(on
ed
ose
)
100
000–
100
000
0Y
esE
yes
–ac
ute
dac
ryo
aden
itis
Lo
cali
zed
ND
Surv
ived
CV
ID
EB
V+
Ho
dgk
ins
MF
DF
lu/M
elp
h/C
amp
ath
11
Rit
uxi
mab
(th
ree
do
ses)
100
000–
100
000
0Y
esC
ervi
cal
lym
ph
no
des
,
live
r,fe
ver
and
rash
Dis
sem
inat
ed
lym
ph
om
ato
us
ND
Surv
ived
WA
SM
UD
Flu
/Mel
ph
/Cam
pat
h2
8G
anci
clo
vir
No
ritu
xim
ab
100
000
0–10
000
000
Yes
Cer
vica
lly
mp
hn
od
es,
live
r,fe
ver
and
rash
Dis
sem
inat
ed
lym
ph
om
ato
us
ND
Surv
ived
JMM
L,
juve
nil
em
yelo
mo
no
cyti
cle
uka
emia
;M
DS,
mye
lod
ysp
last
icsy
nd
rom
e;C
ID,
com
bin
edim
mu
no
defi
cien
cy;
LA
D,
leu
cocy
tead
hes
ion
defi
cien
cy;
SCID
,se
vere
com
bin
edim
mu
no
defi
cien
cy;
CM
V,
cyto
meg
alo
viru
s;A
IHA
,au
toim
mu
ne
hae
mo
lyti
can
aem
ia;
CV
ID,
com
mo
nva
riab
leim
mu
no
defi
cien
cy;
WA
S,W
isko
tt-A
ldri
chsy
nd
rom
e;N
HL
,n
on
-Ho
dgk
in’s
lym
ph
om
a;M
MU
D,
HL
A-m
ism
atch
ed
un
rela
ted
do
no
r;M
UD
,H
LA
-mat
ched
un
rela
ted
do
no
r;M
FD
,H
LA
-mat
ched
fam
ily
do
no
r;M
SD,
HL
A-m
atch
edsi
bli
ng
do
no
r;D
LI,
do
no
rly
mp
ho
cyte
infu
sio
n;
ND
,n
ot
do
ne;
EB
V,
Ep
stei
n–
Bar
rvi
rus;
LP
D,
lym
ph
op
roli
fera
tive
dis
ease
;H
SCT
,h
aem
ato
po
ieti
cst
emce
lltr
ansp
lan
tati
on
;H
LA
,h
um
anle
uco
cyte
anti
gen
.
J. Cohen et al
234 ª 2005 Blackwell Publishing Ltd, British Journal of Haematology, 129, 229–239
who received grafts without in vitro TCD but with in vivo
serotherapy (two of 17, 11Æ8% vs. 25 of 83, 30Æ1%; NS). In
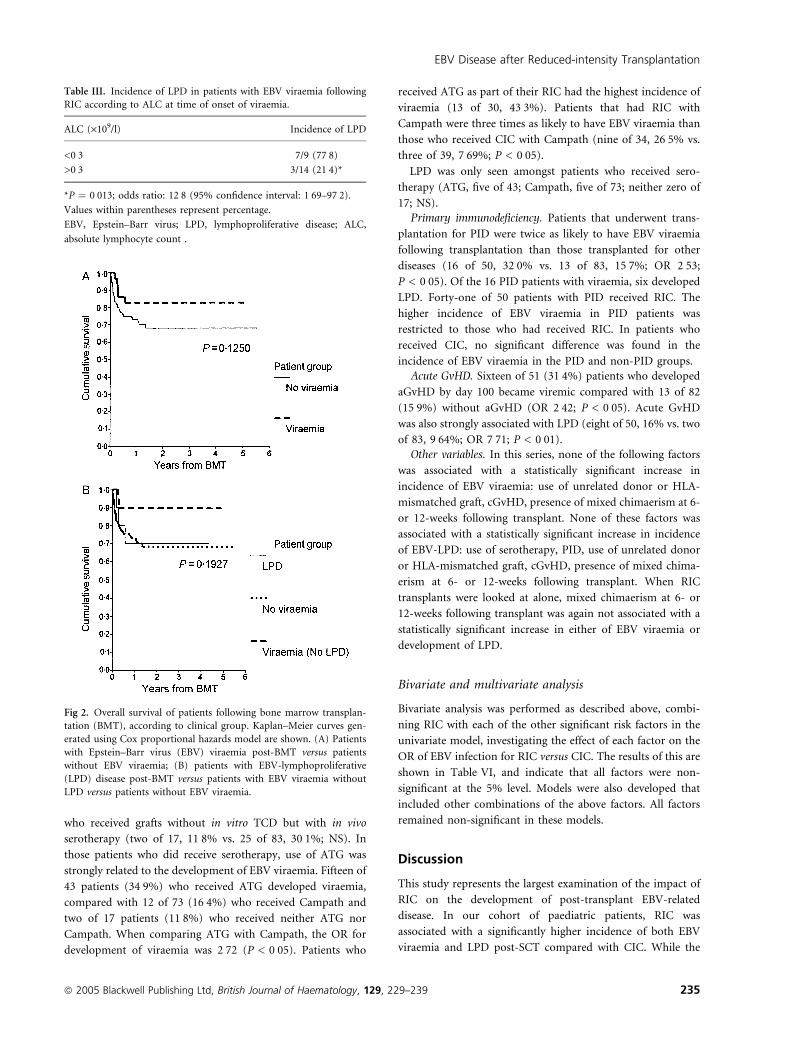
those patients who did receive serotherapy, use of ATG was
strongly related to the development of EBV viraemia. Fifteen of
43 patients (34Æ9%) who received ATG developed viraemia,
compared with 12 of 73 (16Æ4%) who received Campath and
two of 17 patients (11Æ8%) who received neither ATG nor
Campath. When comparing ATG with Campath, the OR for
development of viraemia was 2Æ72 (P < 0Æ05). Patients who
received ATG as part of their RIC had the highest incidence of
viraemia (13 of 30, 43Æ3%). Patients that had RIC with
Campath were three times as likely to have EBV viraemia than
those who received CIC with Campath (nine of 34, 26Æ5% vs.
three of 39, 7Æ69%; P < 0Æ05).
LPD was only seen amongst patients who received sero-
therapy (ATG, five of 43; Campath, five of 73; neither zero of
17; NS).
Primary immunodeficiency. Patients that underwent trans-
plantation for PID were twice as likely to have EBV viraemia
following transplantation than those transplanted for other
diseases (16 of 50, 32Æ0% vs. 13 of 83, 15Æ7%; OR 2Æ53;
P < 0Æ05). Of the 16 PID patients with viraemia, six developed
LPD. Forty-one of 50 patients with PID received RIC. The
higher incidence of EBV viraemia in PID patients was
restricted to those who had received RIC. In patients who
received CIC, no significant difference was found in the
incidence of EBV viraemia in the PID and non-PID groups.
Acute GvHD. Sixteen of 51 (31Æ4%) patients who developed
aGvHD by day 100 became viremic compared with 13 of 82
(15Æ9%) without aGvHD (OR 2Æ42; P < 0Æ05). Acute GvHD
was also strongly associated with LPD (eight of 50, 16% vs. two
of 83, 9Æ64%; OR 7Æ71; P < 0Æ01).
Other variables. In this series, none of the following factors
was associated with a statistically significant increase in
incidence of EBV viraemia: use of unrelated donor or HLA-
mismatched graft, cGvHD, presence of mixed chimaerism at 6-
or 12-weeks following transplant. None of these factors was
associated with a statistically significant increase in incidence
of EBV-LPD: use of serotherapy, PID, use of unrelated donor
or HLA-mismatched graft, cGvHD, presence of mixed chima-
erism at 6- or 12-weeks following transplant. When RIC
transplants were looked at alone, mixed chimaerism at 6- or
12-weeks following transplant was again not associated with a
statistically significant increase in either of EBV viraemia or
development of LPD.
Bivariate and multivariate analysis
Bivariate analysis was performed as described above, combi-
ning RIC with each of the other significant risk factors in the
univariate model, investigating the effect of each factor on the
OR of EBV infection for RIC versus CIC. The results of this are
shown in Table VI, and indicate that all factors were non-
significant at the 5% level. Models were also developed that
included other combinations of the above factors. All factors
remained non-significant in these models.
Discussion
This study represents the largest examination of the impact of
RIC on the development of post-transplant EBV-related
disease. In our cohort of paediatric patients, RIC was
associated with a significantly higher incidence of both EBV
viraemia and LPD post-SCT compared with CIC. While the
Fig 2. Overall survival of patients following bone marrow transplan-
tation (BMT), according to clinical group. Kaplan–Meier curves gen-
erated using Cox proportional hazards model are shown. (A) Patients
with Epstein–Barr virus (EBV) viraemia post-BMT versus patients
without EBV viraemia; (B) patients with EBV-lymphoproliferative
(LPD) disease post-BMT versus patients with EBV viraemia without
LPD versus patients without EBV viraemia.
Table III. Incidence of LPD in patients with EBV viraemia following
RIC according to ALC at time of onset of viraemia.
ALC (·109/l) Incidence of LPD
<0Æ3 7/9 (77Æ8)
>0Æ3 3/14 (21Æ4)*
*P ¼ 0Æ013; odds ratio: 12Æ8 (95% confidence interval: 1Æ69–97Æ2).
Values within parentheses represent percentage.
EBV, Epstein–Barr virus; LPD, lymphoproliferative disease; ALC,
absolute lymphocyte count .
EBV Disease after Reduced-intensity Transplantation
ª 2005 Blackwell Publishing Ltd, British Journal of Haematology, 129, 229–239 235
higher incidence of PID and ATG usage, both of which are
established risk factors for LPD, may partially explain this, our
univariate analysis suggests that RIC was the risk factor most
strongly associated with EBV viraemia and LPD and bivariate
analysis suggests an effect of RIC independent of these factors.
The use of in vivo ATG as part of RIC significantly increased
the likelihood of EBV viraemia, with an incidence in this
subgroup of 43%. Both patients who died of LPD had received
RIC incorporating ATG. Whilst EBV viraemia and LPD were
frequent following the use of Campath in the RIC setting,
viraemia was significantly less common than when ATG was
used. Acute GvHD was associated with EBV viraemia and LPD
in univariate analysis, but was not a risk factor independent of
RIC.
In vitro TCD of the graft has been previously shown to
significantly increase the risk of LPD (Antin et al, 1991;
Micallef et al, 1998). In this study, in vitro TCD was associated
with less EBV viraemia than in those cases where the graft was
not TCD in vitro. This is likely to reflect the fact that, in the
majority of the latter group, patients received in vivo
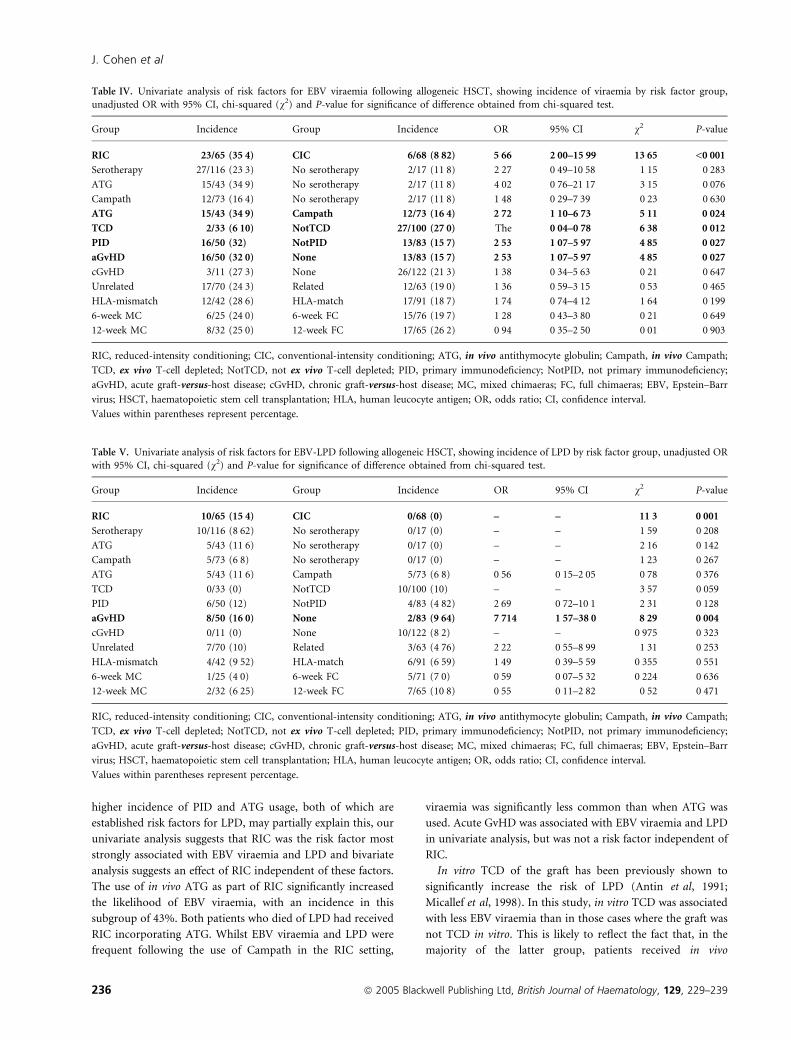
Table IV. Univariate analysis of risk factors for EBV viraemia following allogeneic HSCT, showing incidence of viraemia by risk factor group,
unadjusted OR with 95% CI, chi-squared (v2) and P-value for significance of difference obtained from chi-squared test.
Group Incidence Group Incidence OR 95% CI v2 P-value
RIC 23/65 (35Æ4) CIC 6/68 (8Æ82) 5Æ66 2Æ00–15Æ99 13Æ65 <0Æ001Serotherapy 27/116 (23Æ3) No serotherapy 2/17 (11Æ8) 2Æ27 0Æ49–10Æ58 1Æ15 0Æ283
ATG 15/43 (34Æ9) No serotherapy 2/17 (11Æ8) 4Æ02 0Æ76–21Æ17 3Æ15 0Æ076
Campath 12/73 (16Æ4) No serotherapy 2/17 (11Æ8) 1Æ48 0Æ29–7Æ39 0Æ23 0Æ630
ATG 15/43 (34Æ9) Campath 12/73 (16Æ4) 2Æ72 1Æ10–6Æ73 5Æ11 0Æ024TCD 2/33 (6Æ10) NotTCD 27/100 (27Æ0) The 0Æ04–0Æ78 6Æ38 0Æ012PID 16/50 (32) NotPID 13/83 (15Æ7) 2Æ53 1Æ07–5Æ97 4Æ85 0Æ027aGvHD 16/50 (32Æ0) None 13/83 (15Æ7) 2Æ53 1Æ07–5Æ97 4Æ85 0Æ027cGvHD 3/11 (27Æ3) None 26/122 (21Æ3) 1Æ38 0Æ34–5Æ63 0Æ21 0Æ647
Unrelated 17/70 (24Æ3) Related 12/63 (19Æ0) 1Æ36 0Æ59–3Æ15 0Æ53 0Æ465
HLA-mismatch 12/42 (28Æ6) HLA-match 17/91 (18Æ7) 1Æ74 0Æ74–4Æ12 1Æ64 0Æ199
6-week MC 6/25 (24Æ0) 6-week FC 15/76 (19Æ7) 1Æ28 0Æ43–3Æ80 0Æ21 0Æ649
12-week MC 8/32 (25Æ0) 12-week FC 17/65 (26Æ2) 0Æ94 0Æ35–2Æ50 0Æ01 0Æ903
RIC, reduced-intensity conditioning; CIC, conventional-intensity conditioning; ATG, in vivo antithymocyte globulin; Campath, in vivo Campath;
TCD, ex vivo T-cell depleted; NotTCD, not ex vivo T-cell depleted; PID, primary immunodeficiency; NotPID, not primary immunodeficiency;
aGvHD, acute graft-versus-host disease; cGvHD, chronic graft-versus-host disease; MC, mixed chimaeras; FC, full chimaeras; EBV, Epstein–Barr
virus; HSCT, haematopoietic stem cell transplantation; HLA, human leucocyte antigen; OR, odds ratio; CI, confidence interval.
Values within parentheses represent percentage.
Table V. Univariate analysis of risk factors for EBV-LPD following allogeneic HSCT, showing incidence of LPD by risk factor group, unadjusted OR
with 95% CI, chi-squared (v2) and P-value for significance of difference obtained from chi-squared test.
Group Incidence Group Incidence OR 95% CI v2 P-value
RIC 10/65 (15Æ4) CIC 0/68 (0) – – 11Æ3 0Æ001Serotherapy 10/116 (8Æ62) No serotherapy 0/17 (0) – – 1Æ59 0Æ208
ATG 5/43 (11Æ6) No serotherapy 0/17 (0) – – 2Æ16 0Æ142
Campath 5/73 (6Æ8) No serotherapy 0/17 (0) – – 1Æ23 0Æ267
ATG 5/43 (11Æ6) Campath 5/73 (6Æ8) 0Æ56 0Æ15–2Æ05 0Æ78 0Æ376
TCD 0/33 (0) NotTCD 10/100 (10) – – 3Æ57 0Æ059
PID 6/50 (12) NotPID 4/83 (4Æ82) 2Æ69 0Æ72–10Æ1 2Æ31 0Æ128
aGvHD 8/50 (16Æ0) None 2/83 (9Æ64) 7Æ714 1Æ57–38Æ0 8Æ29 0Æ004cGvHD 0/11 (0) None 10/122 (8Æ2) – – 0Æ975 0Æ323
Unrelated 7/70 (10) Related 3/63 (4Æ76) 2Æ22 0Æ55–8Æ99 1Æ31 0Æ253
HLA-mismatch 4/42 (9Æ52) HLA-match 6/91 (6Æ59) 1Æ49 0Æ39–5Æ59 0Æ355 0Æ551
6-week MC 1/25 (4Æ0) 6-week FC 5/71 (7Æ0) 0Æ59 0Æ07–5Æ32 0Æ224 0Æ636
12-week MC 2/32 (6Æ25) 12-week FC 7/65 (10Æ8) 0Æ55 0Æ11–2Æ82 0Æ52 0Æ471
RIC, reduced-intensity conditioning; CIC, conventional-intensity conditioning; ATG, in vivo antithymocyte globulin; Campath, in vivo Campath;
TCD, ex vivo T-cell depleted; NotTCD, not ex vivo T-cell depleted; PID, primary immunodeficiency; NotPID, not primary immunodeficiency;
aGvHD, acute graft-versus-host disease; cGvHD, chronic graft-versus-host disease; MC, mixed chimaeras; FC, full chimaeras; EBV, Epstein–Barr
virus; HSCT, haematopoietic stem cell transplantation; HLA, human leucocyte antigen; OR, odds ratio; CI, confidence interval.
Values within parentheses represent percentage.
J. Cohen et al
236 ª 2005 Blackwell Publishing Ltd, British Journal of Haematology, 129, 229–239

serotherapy (83 of 101 patients), because of the high
proportion of patients receiving grafts from unrelated donors.
Additionally, in our cohort, the methods of in vitro TCD were
not T-cell specific and would deplete B cells as well. The
selective depletion of T cells without depletion of B cells
appears critical for the pathogenesis of PTLD. In the CIC
setting, depletion of both T and B cells from the graft has been
associated with a very low incidence of LPD (Hale &
Waldmann, 1998). Our data supports this finding: only two
of 15 patients transplanted with grafts that were CD34-selected
using the Miltenyi system developed EBV viraemia. Similarly,
where TCD was performed with Campath 1M with subsequent
T-cell addback, again no patient developed EBV viraemia. The
use of ATG in vivo was significantly associated with higher EBV
viraemia than with Campath 1H.
The incidence of LPD in our RIC patients who received
Campath 1H in vivo was higher than that seen in previous
cohorts of patients conditioned with CIC regimes incorporat-
ing this antibody (Hale & Waldmann, 1998). Peggs et al (2003)
reported four cases of LPD in a cohort of 100 adult patients
allografted using a RIC protocol similar to ours, two of which
were associated with the use of ATG for treatment of GvHD.
The incidence of EBV viraemia was not studied, but the lower
incidence of LPD observed in this study compared with our
cohort may reflect the higher proportion of transplants from
alternative donors in our study, an increased recognition of
atypical clinical presentations of LPD with prospective mon-
itoring of viraemia or differences between paediatric and adult
populations. Whether our finding of increased EBV viraemia
and LPD after RIC transplantation is specific to non-myelo-
ablative protocols utilizing serotherapy is unclear and this
needs to be addressed in further studies. The increased
incidence of EBV-associated disease in the RIC setting
observed in our study may relate to the persistence of EBV
in residual recipient B cells after non-myeloablative condi-
tioning. Indeed, in the two patients who were investigated for
the origin of the proliferative B-cell clones, both were
identified by FISH as recipient-derived. This suggests that it
is the relative preservation of recipient B cells in a profoundly
immunosuppressed setting which increases the chances of
post-transplant EBV proliferation.
Reduced Intensity Conditioning produces a state of profound
functional immunosuppression for at least 6–9 months follow-
ing transplant (Amrolia et al, 2000; Chakrabarti et al, 2002).
While recent work has demonstrated that, following an
unrelated donor transplant for PID, T- and B-cell reconstitution
occurs with similar kinetics in the RIC and CIC settings (Rao
et al, 2005), the number of circulating CD4+ and CD8+ T cells at
the time of the majority of EBV reactivations (2–3 months post-
SCT) with either conditioning regimen was profoundly
depressed. We have demonstrated that an ALC < 0Æ3 · 109/l
at the time of onset of viraemia was strongly predictive of
development of LPD, highlighting the need to take into account
immune reconstitution as well as viral load in estimating the risk
of development of LPD. We have previously observed a higher
incidence of viral reactivations (EBV, CMV and adenovirus) in
PID patients after RIC than CIC (Rao et al, 2005) and the
coincident appearance of other viruses around the same time as
EBV observed in this study is highly suggestive of a reduction in
early viral-specific immunity with RIC. Reduced numbers of
EBV-specific cytotoxic T-lymphocytes have been shown to be
associated with the development of EBV post-SCT (Meij et al,
2003). Indeed, in vitro studies of EBV-specific immune
responses using enzyme-linked immunospot assays have shown
markedly delayed recovery of EBV-specific immunity with a
fludarabine/melphalan/Campath regime similar to ours, when
compared with a CIC regime (Chakrabarti et al, 2003). We are
now prospectively studying EBV-specific T-cell immune recon-
stitution, comparing RIC and CIC in a paediatric setting.
The significance of EBV viraemia post-SCT should be
interpreted in the context of both the type of transplant and
the extent of immune reconstitution. A number of groups
have demonstrated that high viral loads may be predictive of
development of LPD following TCD myeloablative trans-
plants (Rooney et al, 1995; van Esser et al, 2001a; Sirvent-
von Bueltzingsloewen et al, 2002; Wagner et al, 2004), but in
recipients of unmanipulated grafts this is less predictive.
Even in the former group of patients, while EBV viraemia
has a high negative predictive value (NPV), the positive
predictive value (PPV) for developing LPD is generally only
25–40%. Given the efficacy of pre-emptive rituximab in
preventing LPD in patients with viral loads (van Esser et al,
2002), it is now ethically difficult to perform similar studies
to determine the true predictive value of high EBV loads in
patients undergoing transplant with RIC. In our study, the
majority of patients with asymptomatic or symptomatic
viraemia were treated with modulation of immunosuppres-
sion ± pre-emptive rituximab. It is likely that without such
interventions our incidence of LPD may have been even
higher. Nonetheless, the fact that 10 of 23 viraemic patients
in our RIC cohort went on to develop LPD (PPV: 43%),
demonstrates that EBV viraemia is frequently clinically
significant after RIC.
Table VI. Bivariate analysis of risk factors for EBV viraemia following
allogeneic HSCT, showing adjusted OR for risk factor with 95% CI,
chi-squared (v2) and P-value for significance of difference obtained
from chi-squared test, after accounting for the use of RIC.
Factor adjusted for Adjusted OR 95% CI v2 P-value
PID (versus NotPID) 1Æ19 0Æ45–3Æ12 0Æ12 0Æ730
ATG (versus Campath) 2Æ09 0Æ83–5Æ29 2Æ49 0Æ288
TCD (versus NotTCD) 0Æ40 0Æ08–2Æ01 1Æ42 0Æ234
aGvHD (versus none) 2Æ20 2Æ12–15Æ08 3Æ07 0Æ080
PID, primary immunodeficiency; NotPID, not primary immunodefi-
ciency; ATG, in vivo antithymocyte globulin; TCD, ex vivo T-cell
depleted; NotTCD, not ex vivo T-cell depleted; aGvHD, acute graft-
versus-host disease; EBV, Epstein–Barr virus; HSCT, haematopoietic
stem cell transplantation; RIC, reduced-intensity conditioning; OR,
odds ratio, CI, confidence interval.
EBV Disease after Reduced-intensity Transplantation
ª 2005 Blackwell Publishing Ltd, British Journal of Haematology, 129, 229–239 237

Surveillance studies published subsequent to the start of this
study have suggested cut-off values for EBV viral loads, above
which anti-EBV therapeutic manoeuvres are suggested to pre-
empt and thereby prevent the progression to LPD (van Esser
et al, 2001b, 2002; Hoshino et al, 2001) Such studies used
differing laboratory methodologies to quantify the viral load
on differing patient samples, and hence suggested different
thresholds, but the available evidence suggests this approach
may be effective in preventing LPD (Lankester et al, 2002).
Because of the semi-quantitative methodology used and the
fact that the threshold for initiation of anti-EBV therapies
varied between the patients reported in this study, we are
unable to state whether or not such threshold values are
supported by our data. In eight of the 10 patients who
developed LPD in this study, viral load exceeded 105 copies/ml
at the start of treatment. Additionally, even without an
absolute threshold value for initiation of therapy, the rate of
rise in viral load may be significant. There is clearly a need for
large, prospective studies to determine appropriate thresholds
for, and the efficacy of, pre-emptive reduction in immuno-
suppression/rituximab in patients undergoing TCD SCT who
develop high-level EBV viraemia. Such studies should incor-
porate standardized thresholds and utilize accurate quantifi-
cation of viral load with real-time PCR.
The risk of progression to LPD appears to depend on the
balance between EBV reactivation and recovery of EBV-
specific immunity: indeed, combining tetramer assays of
recovery of circulating EBV-specific CD8+ T cells with high-
level viraemia increases the PPV markedly (Meij et al, 2003).
However, such assays are not widely available and what is
needed is a simple method for identifying those viraemic
patients at high risk of LPD. In our patient cohort, EBV
viraemia in patients with a lymphocyte count of <0Æ3 · 109/l
was strongly predictive of LPD.
The majority (six of eight) of patients with established LPD
went into durable complete response after rituximab, demon-
strating that this is an effective therapy in the SCT setting,
avoiding the need to use myelosuppressive chemotherapy.
Indeed, in our cohort, survival in patients with either viraemia
or LPD was equivalent to survival in those with no viraemia
[the statistically non-significant increased survival in patients
with viraemia may reflect the lower treatment-related mortal-
ity in the RIC group (Rao et al, 2005)]. The response rate to
rituximab is similar to that previously reported (Faye et al,
2001) and this is sufficient therapy in the majority of cases.
However, our experience suggests that in some patients with
extremely aggressive LPD, particularly those with airway/
pulmonary involvement, chemotherapy may be indicated for
more rapid disease control.
In conclusion, in our cohort of paediatric patients, RIC
appears to be a significant risk factor for developing EBV-LPD
post-transplant, particularly when ATG is incorporated into
conditioning. Further studies are needed to determine if this is
also true for other patient groups, such as adults with
haematological malignancies. This group of patients needs
careful observation to detect early EBV viraemia through PCR
monitoring of the peripheral blood, together with a high
clinical index of suspicion. The recent introduction of real-
time PCR for monitoring viraemia (Jabs et al, 2001; Wagner
et al, 2004), combined with studies of reconstitution of EBV-
specific immunity and pre-emptive treatment with rituximab,
should lead to the development of more rational strategies to
prevent and treat LPD post-SCT.
References
Amrolia, P., Gaspar, H.B., Hassan, A., Webb, D., Jones, A., Sturt, N.,
Mieli-Vergani, G., Pagliuca, A., Mufti, G., Hadzic, N., Davies, G. &
Veys, P. (2000) Nonmyeloablative stem cell transplantation for
congenital immunodeficiencies. Blood, 96, 1239–1246.
Antin, J.H., Bierer, B.E., Smith, B.R., Ferrara, J., Guinan, E.C., Sieff, C.,
Golan, D.E., Macklis, R.M., Tarbell, N.J. & Lynch, E. (1991) Selective
depletion of bone marrow T lymphocytes with anti-CD5 mono-
clonal antibodies: effective prophylaxis for graft-versus-host disease
in patients with hematologic malignancies. Blood, 78, 2139–2149.
Bhatia, S., Ramsay, N.K., Steinbuch, M., Dusenbery, K.E., Shapiro,
R.S., Weisdorf, D.J., Robison, L.L., Miller, J.S. & Neglia, J.P. (1996)
Malignant neoplasms following bone marrow transplantation.
Blood, 87, 3633–3639.
Chakrabarti, S., Mackinnon, S., Chopra, R., Kottaridis, P.D., Peggs, K.,
O’Gorman, P., Chakraverty, R., Marshall, T., Osman, H., Mahendra,
P., Craddock, C., Waldmann, H., Hale, G., Fegan, C.D., Yong, K.,
Goldstone, A.H., Linch, D.C. & Milligan, D.W. (2002) High
incidence of cytomegalovirus infection after nonmyeloablative stem
cell transplantation: potential role of Campath-1H in delaying im-
mune reconstitution. Blood, 99, 4357–4363.
Chakrabarti, S., Milligan, D.W., Pillay, D., Mackinnon, S., Holder, K.,
Kaur, N., McDonald, D., Fegan, C.D., Waldmann, H., Hale, G.,
Rickinson, A. & Steven, N. (2003) Reconstitution of the Epstein-
Barr virus-specific cytotoxic T-lymphocyte response following T-
cell-depleted myeloablative and nonmyeloablative allogeneic stem
cell transplantation. Blood, 102, 839–842.
Curtis, R.E., Travis, L.B., Rowlings, P.A., Socie, G., Kingma, D.W.,
Banks, P.M., Jaffe, E.S., Sale, G.E., Horowitz, M.M., Witherspoon,
R.P., Shriner, D.A., Weisdorf, D.J., Kolb, H.J., Sullivan, K.M.,
Sobocinski, K.A., Gale, R.P., Hoover, R.N., Fraumeni, J.F. Jr & Deeg,
H.J. (1999) Risk of lymphoproliferative disorders after bone marrow
transplantation: a multi-institutional study. Blood, 94, 2208–2216.
van Esser, J.W., van der Holtm, B., Meijer, E., Niesters, H.G.,
Trenschel, R., Thijsen, S.F., van Loon, A.M., Frassoni, F., Baciga-
lupo, A., Schaefer, U.W., Osterhaus, A.D., Gratama, J.W.,
Lowenberg, B., Verdonck, L.F. & Cornelissen, J.J. (2001a) Epstein-
Barr virus (EBV) reactivation is a frequent event after allogeneic
stem cell transplantation (SCT) and quantitatively predicts EBV-
lymphoproliferative disease following T-cell-depleted SCT. Blood,
98, 972–978.
van Esser, J.W., Niesters, H.G., Thijsen, S.F., Meijer, E., Osterhaus,
A.D., Wolthers, K.C., Boucher, C.A., Gratama, J.W., Budel, L.M.,
van der Holt, B., van Loon, A.M., Lowenberg, B., Verdonck, L.F. &
Cornelissen, J.J. (2001b) Molecular quantification of viral load in
plasma allows for fast and accurate prediction of response to therapy
of Epstein-Barr virus-associated lymphoproliferative disease after
allogeneic stem cell transplantation. British Journal of Haematology,
113, 814–821.
J. Cohen et al
238 ª 2005 Blackwell Publishing Ltd, British Journal of Haematology, 129, 229–239
van Esser, J.W.J., Niesters, H.G.M., van der Holt, B., Meijer, E., Os-
terhaus, A.D.M.E., Gratama, J.W., Verdonck, L.F., Lowenberg, B. &
Cornelissen, J.J. (2002) Prevention of Epstein-Barr virus-lympho-
proliferative disease by molecular monitoring and preemptive ri-
tuximab in high-risk patients after allogeneic stem cell
transplantation. Blood, 99, 4364–4369.
Faye, A., Quartier, P., Reguerre, Y., Lutz, P., Carret, A.S., Dehee, A.,
Rohrlich, P., Peuchmaur, M., Matthieu-Boue, A., Fischer, A. &
Vilmer, E. (2001) Chimaeric anti-CD20 monoclonal antibody (ri-
tuximab) in post-transplant B-lymphoproliferative disorder follow-
ing stem cell transplantation in children. British Journal of
Haematology, 115, 112–118.
Gross, T.G., Steinbuch, M., DeFor, T., Shapiro, R.S., McGlave, P.,
Ramsay, N.K., Wagner, J.E. & Filipovich, A.H. (1999) B cell lym-
phoproliferative disorders following hematopoietic stem cell trans-
plantation: risk factors, treatment and outcome. Bone Marrow
Transplantation, 23, 251–258.
Hale, G. & Waldmann, H. (1998) Risks of developing Epstein-Barr
virus-related lymphoproliferative disorders after T-cell-depleted
marrow transplants. CAMPATH users. Blood, 91, 3079–3083.
Harris, N.L., Jaffe, E.S., Diebold, J., Flandrin, G., Muller-Hermelink,
H.K., Vardiman, J., Lister, T.A. & Bloomfield, C.D. (1999) World
Health Organization classification of neoplastic diseases of the he-
matopoietic and lymphoid tissues: Report of the Clinical Advisory
Committee Meeting – Airlie House, Virginia, November 1997.
Journal of Clinical Oncology, 17, 3835–3849.
Ho, A.Y., Adams, S., Shaikh, H., Pagliuca, A., Devereux, S. & Mufti,
G.J. (2002) Fatal donor-derived Epstein-Barr virus-associated post-
transplant lymphoproliferative disorder following reduced intensity
volunteer-unrelated bone marrow transplant for myelodysplastic
syndrome. Bone Marrow Transplantation, 29, 867–869.
Hoshino, Y., Kimura, H., Tanaka, N., Tsuge, I., Kudo, K., Horibe, K.,
Kato, K., Matsuyama, T., Kikuta, A., Kojima, S. & Morishima, T.
(2001) Prospective monitoring of the Epstein-Barr virus DNA by a
real-time quantitative polymerase chain reaction after allogenic stem
cell transplantation. British Journal of Haematology, 115, 105–111.
Jabs, W.J., Hennig, H., Kittel, M., Pethig, K., Smets, F., Bucsky, P.,
Kirchner, H. & Wagner, H.J. (2001) Normalized quantification by
real-time PCR of Epstein-Barr virus load in patients at risk for
posttransplant lymphoproliferative disorders. Journal of Clinical
Microbiology, 39, 564–569.
Lankester, A.C., van Tol, M.J., Vossen, J.M., Kroes, A.C. & Claas, E.
(2002) Epstein-Barr virus (EBV)-DNA quantification in paediatric
allogenic stem cell recipients: prediction of EBV-associated lym-
phoproliferative disease. Blood, 99, 2630–2631.
Lucas, K.G., Burton, R.L., Zimmerman, S.E., Wang, J.H., Cornetta, K.G.,
Robertson, K.A., Lee, C.H. & Emanuel, D.J. (1998) Semiquantitative
Epstein-Barr virus (EBV) polymerase chain reaction for the
determination of patients at risk for EBV-induced lymphoprolifera-
tive disease after stem cell transplantation. Blood, 91, 3654–3661.
Meij, P., van Esser, J.W., Niesters, H.G., van Baarle, D., Miedema, F.,
Blake, N., Rickinson, A.B., Leiner, I., Pamer, E., Lowenberg, B.,
Cornelissen, J.J. & Gratama, J.W. (2003) Impaired recovery of Ep-
stein-Barr virus (EBV)-specific CD8+ T lymphocytes after partially
T-depleted allogeneic stem cell transplantation may identify patients
at very high risk for progressive EBV reactivation and lymphopro-
liferative disease. Blood, 101, 4290–4297.
Meijer, E., Slaper-Cortenbach, I.C., Thijsen, S.F., Dekker, A.W. &
Verdonck, L.F. (2002) Increased incidence of EBV-associated
lymphoproliferative disorders after allogeneic stem cell transplan-
tation from matched unrelated donors due to a change of T cell
depletion technique. Bone Marrow Transplantation, 29, 335–339.
Micallef, I.N.M., Chhanabhai, M., Gascoyne, R.D., Shepherd, J.D.,
Fung, H.C., Nantel, S.H., Toze, C.L., Klingemann, H.G., Sutherland,
H.J., Hogge, D.E., Nevill, T.J., Le, A. & Barnett, M.J. (1998) Lym-
phoproliferative disorders following allogeneic bone marrow trans-
plantation: the Vancouver experience. Bone Marrow
Transplantation, 22, 981–987.
Milpied, N., Coste-Burel, M., Accard, F., Moreau, A., Moreau, P., Ga-
rand, R. & Harousseau, J.L. (1999) Epstein-Barr virus-associated B cell
lymphoproliferative disease after non-myeloablative allogeneic stem
cell transplantation. Bone Marrow Transplantation, 23, 629–630.
Milpied, N., Vasseur, B., Parquet, N., Garnier, J.L., Antoine, C.,
Quartier, P., Carret, A.S., Bouscary, D., Faye, A., Bourbigot, B.,
Reguerre, Y., Stoppa, A.M., Bourquard, P., de Ligny, B.H., Dubief,
F., Mathieu-Boue, A. & Leblond, V. (2000) Humanized anti-CD20
monoclonal antibody (Rituximab) in post transplant B-lympho-
proliferative disorder: a retrospective analysis on 32 patients. Annals
of Oncology, 11, 113–116.
Nalesnik, M.A. (1998) Clinical and pathological features of post-
transplant lymphoproliferative disorders (PTLD). Springer Seminars
in Immunopathology, 20, 325–342.
Peggs, K.S., Banerjee, L., Thomson, K. & Mackinnon, S. (2003) Post
transplant lymphoproliferative disorders following reduced intensity
conditioning with in vivo T cell depletion. Bone Marrow Trans-
plantation, 31, 725–726.
Rao, K., Amrolia, P.J., Jones, A., Cale, C.M., Naik, P., King, D., Davies,
G.E., Gaspar, H.B. & Veys, P.A. (2005) Improved survival after
unrelated donor bone marrow transplant in children with primary
immunodeficiency using a reduced intensity conditioning regimen.
Blood, 105, 879–885.
Rooney, C.M., Loftin, S.K., Holladay, M.S., Brenner, M.K., Krance,
R.A. & Heslop, H.E. (1995) Early identification of Epstein-Barr
virus-associated post-transplantation lymphoproliferative disease.
British Journal of Haematology, 89, 98–103.
Rooney, C.M., Smith, C.A., Ng, C.Y.C., Loftin, S.K., Sixbey, J.W., Gan,
Y.J., Srivastava, D.K., Bowman, L.C., Krance, R.A., Brenner, M.K. &
Heslop, H.E. (1998) Infusion of cytotoxic T cells for the prevention
and treatment of Epstein-Barr virus-induced lymphoma in allo-
geneic transplant recipients. Blood, 92, 1549–1555.
Shroff, R., Trompeter, R., Cubitt, D., Thaker, U. & Rees, L. (2002)
Epstein-Barr virus monitoring in paediatric renal transplant
recipients. Paediatric Nephrology, 17, 770–775.
Sirvent-von Bueltzingsloewen, A., Morand, P., Buisson, M., Souillet,
G., Chambost, H., Bosson, J.L. & Bordigoni, P. (2002) A prospective
study of Epstein-Barr virus load in 85 hematopoietic stem cell
transplants. Bone Marrow Transplantation, 29, 21–28.
Slavin, S., Nagler, A., Naparstek, E., Kapelushnik, Y., Aker, M., Civi-
dalli, G., Varadi, G., Kirschbaum, M., Ackerstein, A., Samuel, S.,
Amar, A., Brautbar, C., Ben Tal, O., Eldor, A. & Or, R. (1998)
Nonmyeloablative stem cell transplantation and cell therapy as an
alternative to conventional bone marrow transplantation with lethal
cytoreduction for the treatment of malignant and nonmalignant
hematologic diseases. Blood, 91, 756–763.
Wagner, H.J., Cheng, Y.C., Huls, M.H., Gee, A.P., Kuehnle, I., Krance,
R.A., Brenner, M.K., Rooney, C.M. & Heslop, H.E. (2004) Prompt
versus preemptive intervention for EBV lymphoproliferative disease.
Blood, 103, 3979–3981.
EBV Disease after Reduced-intensity Transplantation
ª 2005 Blackwell Publishing Ltd, British Journal of Haematology, 129, 229–239 239