Embed Size (px)
Citation preview

14ournalofNeurology, Neurosurgery, and Psychiatry 1992;55:1014-1017
Impaired joint mobility in Guillain-Barresyndrome: a primary or a secondaryphenomenon?
I Soryal, E Sinclair, J Hornby, B Pentland
AbstractThree patients with Guillain-Barrk syn-drome had significant residual impair-ment of joint mobility. Pain in the limbsand axial skeleton was a prominent earlyfeature, as were autonomic disturbancesand bulbar involvement resulting in pro-longed mechanical ventilation. All threepatients developed marked joint stiffnessand contractures despite having physio-therapy from the outset. The skeletalproblems and complications becamemajor components of disability despiteimproving neurological status.
C( Neurol Neurosurg Psychiatry 1992;55:1014-1017)
Guillain-Barre syndrome is best regarded as aclinical syndrome rather than a specific diseaseentity. Classically the neurological featuresdevelop after episodes of viral or other infec-tions and the syndrome is infrequently asso-ciated with autoimmune, neoplastic and otherdiseases. The prognosis in idiopathic cases isgenerally good, with residual distal weakness asthe commonest cause of long term disability. Arecent review described persisting moderate orsevere motor deficit in 5-30% of cases. 'Although regular passive movements andsplinting to avoid contractures are often rec-ommended, reports of long term follow up donot describe contractures or other joint prob-lems as a persisting cause of disability. Wedescribe three patients with Guillain-Barresyndrome in whom reduction in the range ofjoint movement contributed significantly tothe disability.
RehabilitationMedicine Unit, AstleyAinslie Hospital,Edinburgh EH9 2HL,UKI SoryalE SinclairJ HornbyB PentlandCorrespondence to:Dr Soryal.Received 27 November 1991and in revised form 24February 1992.Accepted 10 March 1992
Patients and methodsAll the cases described fulfilled the criteria forthe Guillain-Barre syndrome defined by theNational Institute of Neurological and Com-municative Disorders and Stroke.2 Thus allpresented with predominantly progressivemotor weakness, which was relatively symmet-rical, loss of reflexes, mild sensory loss andfacial nerve palsy and autonomic dysfunction.The patients were referred from different acuteneurological units to a neuro-rehabilitationunit after prolonged periods of care. Improve-ments in fumctional ability were assessed usingthe Barthel Index,3 which is a measure of self-care and mobility scored on a range from 0(total dependence) to 20 (independent).
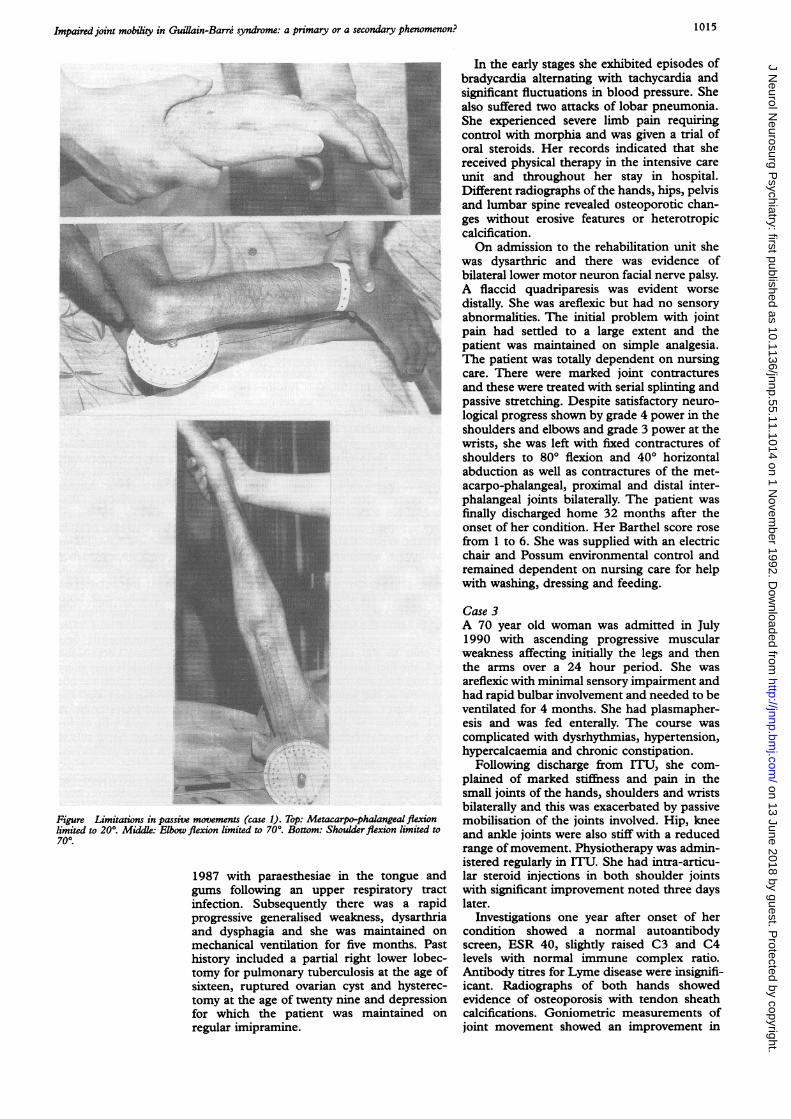
Case 1A 57 year old salesman was admitted in July1989 with a history of pain in the extremities,peripheral sensory disturbances and progres-sive muscular weakness preceded by a week'shistory of pharyngitis, neck adenitis and con-junctivitis. He had flaccid quadriparesis, are-flexia and sensory loss in the extremities to midforearms and knees. His condition deterioratedrapidly with bulbar involvement and dysauto-nomia characterised by labile hypertension,urinary retention and faecal incontinence. Hewas ventilated for a period of 10 weeks. Hiscourse was complicated with recurrent chestinfections and deep vein thrombosis. Thepatient complained of persistent and severeaxial pain and marked symmetrical joint stiff-ness affecting most joints particularly the smalljoints in both hands (figure).On admission to the rehabilitation unit,
eleven months after the acute onset, he wastotally dependent on nursing care and was bedbound. He complained of backache and righthip pain as well as pain in both shoulders,elbows and wrists on passive exercises. Askeletal survey and a bone scan showed noevidence of active inflammation although thehip radiograph showed evidence of tendoncalcification. The haematological and bio-chemical screen including LFT and ESR werenormal. His autoantibody screen and serologyfor Lyme disease were negative. His neuro-logical state improved progressively withreturn of sensations and muscle bulk and theappearance of weak tendon reflexes. His pro-gress, however, was hampered by articulardisability. There was some improvement inproximal joint movement range over 12months: shoulder flexion increased from700-1200; abduction from 50°-80°, elbowflexion from 70°-1200; and hip and kneeflexion both from 80°-110°. Distal joints,however, showed minimal change, for exam-ple, wrist flexion from 45°-55°.
Functionally he regained continence insphincteric functions, was able to feed himselfwith adapted cutlery and mobilise independ-ently in an electric wheelchair with an adaptedmanual control knob, and was able to use acomputer and typewriter with a stick held inthe mouth. His ability to transfer improvedalthough he still required assistance with thisand with bathing and toileting, reflected in animprovement in Barthel score from 0-7.
Case 2A 54 year old woman was admitted in May
1014 on 13 June 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.55.11.1014 on 1 N
ovember 1992. D
ownloaded from
Impaired joint mobility in Guillain-Barre syndrome: a primary or a secondary phenomenon?
.....
Figure Limitations in passive movements (case 1). Top: Metacarpo-phalangealflexilimited to 200. Middl: Elbow flexion limited to 700. Bottom: Shoulder flexion limitea700.
1987 with paraesthesiae in the tonguegums following an upper respiratory tinfection. Subsequently there was a r:progressive generalised weakness, dysartand dysphagia and she was maintainedmechanical ventilation for five months.history included a partial right lower loltomy for pulmonary tuberculosis at the agsixteen, ruptured ovarian cyst and hystetomy at the age of twenty nine and depresfor which the patient was maintainedregular imipramine.
In the early stages she exhibited episodes ofbradycardia alternating with tachycardia andsignificant fluctuations in blood pressure. Shealso suffered two attacks of lobar pneumonia.She experienced severe limb pain requiringcontrol with morphia and was given a trial oforal steroids. Her records indicated that shereceived physical therapy in the intensive careunit and throughout her stay in hospital.Different radiographs of the hands, hips, pelvisand lumbar spine revealed osteoporotic chan-ges without erosive features or heterotropiccalcification.On admission to the rehabilitation unit she
was dysarthric and there was evidence ofbilateral lower motor neuron facial nerve palsy.A flaccid quadriparesis was evident worsedistally. She was areflexic but had no sensoryabnormalities. The initial problem with jointpain had settled to a large extent and thepatient was maintained on simple analgesia.The patient was totally dependent on nursingcare. There were marked joint contracturesand these were treated with serial splinting andpassive stretching. Despite satisfactory neuro-logical progress shown by grade 4 power in theshoulders and elbows and grade 3 power at thewrists, she was left with fixed contractures ofshoulders to 800 flexion and 400 horizontalabduction as well as contractures of the met-acarpo-phalangeal, proximal and distal inter-phalangeal joints bilaterally. The patient wasfinally discharged home 32 months after theonset of her condition. Her Barthel score rosefrom 1 to 6. She was supplied with an electricchair and Possum environmental control andremained dependent on nursing care for helpwith washing, dressing and feeding.
Case 3A 70 year old woman was admitted in July1990 with ascending progressive muscularweakness affecting initially the legs and thenthe arms over a 24 hour period. She wasareflexic with minimal sensory impairment andhad rapid bulbar involvement and needed to beventilated for 4 months. She had plasmapher-esis and was fed enterally. The course wascomplicated with dysrhythmias, hypertension,hypercalcaemia and chronic constipation.
Following discharge from ITU, she com-plained of marked stiffness and pain in thesmall joints of the hands, shoulders and wristsbilaterally and this was exacerbated by passive
ion mobilisation of the joints involved. Hip, kneed to and ankle joints were also stiff with a reduced
range of movement. Physiotherapy was admin-istered regularly in ITU. She had intra-articu-
and lar steroid injections in both shoulder jointstract with significant improvement noted three daysapid later.hria Investigations one year after onset of heron condition showed a normal autoantibody
Past screen, ESR 40, slightly raised C3 and C4bec- levels with normal immune complex ratio.re of Antibody titres for Lyme disease were insignifi-rec- icant. Radiographs of both hands showed,sion evidence of osteoporosis with tendon sheathon calcifications. Goniometric measurements of
joint movement showed an improvement in
1015
.i.
'i,.kl. .4.3
I;k
!'O.- W -N, .'p.,.N..mm.. :;
i
:v
on 13 June 2018 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.55.11.1014 on 1 Novem
ber 1992. Dow
nloaded from

Soryal, Sinclair, Hornby, Pendand
shoulder abduction from 800 to 900 andextension 250 to 40°, wrist flexion 550 to 750,limited metacarpophalangeal flexion to 600and interphalangeal flexion to 200 during 6weeks of rehabilitation. There was also notice-able return of muscle bulk in the forearms andweak proximal stretch reflexes. Pain in thedifferent joints has settled to a minimum andsensations have recovered fully. The patient isstill dependent on nursing care for mostactivities of daily living but has made progressas an inpatient.
DiscussionPain is a well recognised accompaniment oftheacute phase of Guillain-Barre syndrome occur-ring in about half of the reported cases."6 Thisis most frequently back pain67 or buttock andother large muscle discomfort56 but can beprominent distally as in Landry's originaldescription.5 Explanations of the source of thispain include changes in the muscle of neuro-genic origin,5 poor posturing and joint stiff-ness, meningeal irritation8 and inflammationof the cutaneous nerves and distal roots stim-ulatory C fibres.8 It is also conceivable that insome cases pain may be a feature of aninflammatory process in the joints themselvesand/or the periarticular structures. As the painoften precedes the neurological deteriorationand therefore follows more quickly after theinfective episode, it is possible that a fleetingpost-infective arthritis occurs in some patients.If this was the case one might expect someinflammatory signs on examination which arenot usually present. Also in our cases noradiological signs of erosive arthropathy orinflammatory joint disease were evident eventhough these radiological exposures were car-ried out approximately one year after the acuteonset.Whatever the cause of pain in the early
stages of the cases described, the fact that thejoints were painful to move may have resultedin inadequate passive movement of the jointsresulting in stiffness and a degree of con-tractures. In her personal account of thecondition Bowes9 described nurses as beingreluctant to stretch her muscles and joints tothe point of resistance as this was painful. Inour cases the first patient's joints were "fixed"in a position which strongly suggested inade-quate passive movements resulting in con-tractures. The second patient had pains of suchintensity that they required narcotic analgesiaand this phenomenon has also been describedby others. Faced with such, degree of pain, thetherapist or the nurse may be understandablycautious about putting the joints through thefull range of movement.
Prolonged immobilisation is known to resultin poor muscular compliance with structuralhistopathological changes in muscle and con-nective tissue. Lack of stretch, when musclesare immobilised in the shortened state, andloss of contractility are the two main contribu-tory factors to such changes.0 This is followedby joint stiffness, muscular shortening andlargely irreversible contractures. It is clear
therefore that muscular stretch and/or elec-trical stimulation are two physical approachesto prevent contractures. Despite the lack ofreported cases of contractures due to inade-quate physiotherapy, a number of authors havestressed the need to perform regular repeatedpassive movements and the use of splints andpillows to maintain the position of func-tion. " "There is, however, perhaps a case fora more precise structured programme deter-mining the frequency and duration with whichrange of passive movements are done andlooking prospectively at the cause of thedisorder and subsequent disabilities in patientswith severe early joint pains.
In contrast to the supposition that jointimmobility results from inadequate physiother-apy, it is possible that inappropriate excessivepassive movement could result in capsulartears or other damage to joints. In the presenceof hypotonia and sensory impairment thepatient may be unable to detect excessive jointmovement by a therapist or nurse.Another hypothesis is that muscular paraly-
sis results in venous and lymphatic stasis withconsequent nutritional disturbances and accu-mulation of tissue fluid in tissue spaces. Thiswill result in a softening of capsule andligaments followed by adhesions and fibrosis. 3Vasomotor disturbances resulting from auto-nomic neuropathy may also be a furthercontributory factor to this mechanism. Per-haps another method of passive joint mobilisa-tion that is associated with a decrease in suchrisk, is the use of mechanical continuouspassive motion (CPM). There is some evidenceshowing that intensive CPM is effective inmaintaining joint range both in rabbits andhumans,'4 but this technique has not beenevaluated yet in the early management ofpatients with Guillain-Barre syndrome. Thepresence of severe pain, osteoporosis andsmooth skin in the fingers of case 3 bore somesimilarity to algodystrophy which is seen mostcommonly in the shoulder hand syndrome butthis patient had bilateral involvement of all themajor joints in the upper and lower limbs. Areflex neovascular dystrophy cannot be exclu-ded as a pathogenic mechanism but if this isthe case it must be a much more generalisedvariant than usual.
Several recent reports have described theresidual disability after Guillain-Barre syn-drome in populations of patients1 615 andresidual weakness is reported to be the majorproblem with no reference made to loss of orreduced joint mobility. Some reports describ-ing joint problems requiring surgery in chil-dren with the condition are available'6 17 butthese are mainly concerned with scoliosis andfoot drop correcting procedures. Our patientsmay represent the chance occurrence of atyp-ical cases but all three had profound disabilityand social handicap over one to three yearsafter acute neurological presentation primarilyas a result of reduced joint mobility rather thanneurogenic weakness.One could therefore argue the case for
intensive monitoring and periodic measure-ments of joint range ofmovement as a standard
1016 on 13 June 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.55.11.1014 on 1 N
ovember 1992. D
ownloaded from

Impaired joint mobility in Guillain-Barre syndrome: a primary or a secondary phenomenon?
part ofmanagement from the outset to identifypatients at risk of developing articular compli-cations. Perhaps it is also time to review thedifferent aspects of nursing care and physicaltherapy with specific recommendationstowards integrated standardised methods formobilisation and care of joint structures.
We thank colleagues for allowing us to study their patients andare particularly grateful to Dr RWill and Dr J Hunter for helpfulcomments. We are also grateful to Mr M Devlin, MedicalPhotography Department and to MrsY Jones for her secretarialassistance.
1 de Jager AEJ, Minderhoud JM. Residual signs in severeGuillain-Barre syndrome: analysis of 57 patients. NeurolSci 1991;104:151-6.
2 Asbury AK. Diagnostic considerations in Guillain-Barresyndrome. Ann Neurol 1981 ;9(Suppl): 1-5.
3 Mahoney JR, Barthel DW. Functional assessment: TheBarthel Index. Maryland state Med 1965;14:61-65.
4 McFarland HR, Heller GL. Guillain-Barre disease com-
plex. Arch Neurol 1966;14:196-201.5 Ropper AH, Shahani BT. Pain in Guillain-Barre syndrome.
Arch Neurol 1984;41:511-4.6 Winer JB, Hughes RAC, Osmond C. A prospective study of
acute idiopathic neuropathy I. Clinical features and theirprognostic value. Neurol Neurosurg Psychiatry 1988;51:605-12.
7 Clague JE, Macmillan RR. Backache and the Guillain-Barresyndrome: a diagnostic problem. BMJ 1986;293:325-6.
8 de Jager AEJ, Sluiter HJ. Clinical signs in severe Guillain-Barre syndrome: analysis of 63 patients. Jf Neurol Sci1991;104: 143-50.
9 Bowes D. The doctor as a patient: an encounter withGuillain-Barre syndrome. Can Med Assoc J 1984;131:1343-8.
10 Williams PE, Catanese T, Lucey EG, Goldspink G. Theimportance of stretch and contractile activity in theprevention of connective tissue accumulation in muscle. JAnat 1988;158:109-114.
11 Parry CW Disorders of peripheral nerves. In: Nichols PRJ,ed. Rehabilitation medicine, 2nd ed. London: Butter-worths, 1980:144-58.
12 Lee JM. Polyneuropathy. In: Downie PA, ed. Cash's textbookof neurologyfor physiotherapists, 3rd ed. London: Faber andFaber, 1982:328-47.
13 Sunderland S, ed. Changes in bones, joints and peri-articular structures, due to denervation. Nerves and nerveinjuries, 2nd ed. London: Churchill Livingstone, 1978:219-28.
14 Salter R. Clinical application of basic research on con-tinuous passive motion for disorders and injuries ofsynovial joints: a preliminary study. J Orth Res 1984;1:325.
15 Winer JB, Hughes RAC, Greenwood RJ, Perkin GD, HealyMJR. Prognosis in Guillain-Barre syndrome. Lancet1985;1: 1202-3.
16 Berman AT, Tom L. The Guillain-Barre syndrome inchildren. Clin Orthop 1976;116:61-5.
17 Gordon SL, MorrisWT, Stoner MA, Greer RB. Residua ofGuillain-Barre polyneuritis in children. J Bone Jt Surg1977;59-A:193-7.
1017 on 13 June 2018 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.55.11.1014 on 1 N
ovember 1992. D
ownloaded from