Embed Size (px)
DESCRIPTION
guillain barre syndrome
Citation preview
Jerlyn L. Yu
REFLECTING ON PRACTICE: CARE OF A CLIENT WITH IMMUNE-MEDIATED DISORDER - GUILLAIN BARRE SYNDROME
REFLECTING ON PRACTICE: CLIENT PROFILE AND CASE STUDYThis is a case of a 22 year old female born on November 6, 1991 via normal spontaneous delivery in Cebu City. In the course of this study, the patient was named as Leah to protect her identity. Leah and her parents are currently residing in Cebu City. Her parents are both Catholics and Filipino. Leah’s mother is a government employee while his father works in CAAP. Leah was admitted at Medical ward of Vicente Sotto Memorial Medical Center on August 15, 2013 with the diagnosis of Guillain Barre Syndrome.
Celebrating Practice:Patient was admitted to the hospital with weakness of the upper and lower extremities (2/5). After 3 days of nursing interventions, patient’s extremities remained weak (2/5).Effective/Efficient/Sensitive care
The nursing interventions are the following: Placing the patient in a comfortable and clean environment. Encourage to comply with steroids. Cytoxan or cyclophosphamide can also slow down
the progress of GBS. Anticoagulants are given as well in times of thrombophlebitis. Served a balanced diet must in order to prevent tissue and muscle breakdown. Observed for changes in respiratory pattern, shortness of breath, dyspnea, and suction
increased secretions. Checked for changes in cardiac rhythms, increased ectopy, and blood pressure. Assess
for chest pain or discomfort. Documented bowel movements. Repositioned every 2 hours to decrease risk of skin breakdown
Collaborative care: Arranged sessions for physical therapy for the patient to have optimal recovery.
Correcting Practice:Leah’s family decided to send her 1st to a “manghihilot” to relieve the weakness of her legs. The weakness of her legs which started from tingling of feet going up is a dangerous sign that her nerves are already being attacked. In our culture, we always choose the hospital as our last resort to alleviate what we feel. Anything unusual which is radiating or progressing needs to be immediately checked by a physician in order to rule out any dangerous conditions.
Understanding Self:Being a nurse, we yearn to provide quality health care to our patients. The primary role of a nurse is providing health education. It is very important that we are able to impart to everyone the importance of identifying cues that needs to be consulted immediately to a physician. In today’s dilemma of high priced health care, the number 1 solution in order to lessen incidences of diseases is to provide education to the community.
Understanding Others:It is important to explain to everyone that GBS is not contagious. Making people aware that they are not at risk of acquiring the same disease will allow them to openly interact with the patient. Interaction is very important to a patient as this will be the way for them to express what they feel.
Understanding Profession:Diagnostic examinations and other procedures are essential to evaluate the progress of recovery of a patient. In these times, a nurse is needed to monitor closely in order to identify whether the interventions that the patient receives needs to be modified.
Challenging Assumptions Supportive treatment
Approximately 25%-30% of patients with severe GBS have to be monitored or subjected to mechanical ventilation. The patients should be monitored in the ICU if they are dysautonomic, Hughes disability scale score ≥3 or <3 progressing. Intubation should be carried out if the patients are developing bulbar dysfunction and aspiration.
Nursing Consideration:1. Communication among care providers promotes optimal outcomes. For mechanically ventilated
patients, care providers may include primary care physicians, pulmonary specialists, hospitalists, respiratory therapists, and nurses.
2. When you enter the patient’s room, take vital signs, check oxygen saturation, listen to breath sounds, and note changes from previous findings. Also assess the patient’s pain and anxiety levels.
3. Read the patient’s order and obtain information about the ventilator. Compare current ventilator settings with the settings prescribed in the order. Familiarize yourself with ventilator alarms and the actions to take when an alarm sounds. Locate suction equipment and review its use. Look for a bag-valve mask, which should be available for every patient with an artificial airway; be sure you know how to hyperventilate and hyperoxygenate the patient.
4. Patients receiving positive-pressure mechanical ventilation have a tracheostomy, endotracheal, or nasotracheal tube. Most initially have an endotracheal tube; if they stay on the ventilator for many days or weeks, a tracheotomy may be done. Tracheotomy decisions depend on patient specifics.
5. Even though your patient can’t verbally express her needs, you’ll need to assess her pain level using a reliable scale. Keep in mind that a patient’s acknowledgment of pain means pain is present and must be treated. Two scales that help you evaluate your patient’s sedation level are the Richmond Agitation Sedation Scale and the Ramsay Sedation Scale.
6. Monitor the patient’s blood pressure every 2 to 4 hours, especially after ventilator settings are changed or adjusted. Mechanical ventilation causes thoracic-cavity pressure to rise on inspiration, which puts pressure on blood vessels and may reduce blood flow to the heart; as a result, blood pressure may drop. To maintain hemodynamic stability, you may need to increase I.V. fluids or administer a drug such as dopamine or norepinephrine, if ordered.
7. The cuff on the endotracheal or tracheostomy tube provides airway occlusion. Proper cuff inflation ensures the patient receives the proper ventilator parameters, such as TV and oxygenation. Following hospital policy, inflate the cuff and measure for proper inflation pressure using the minimal leak technique or minimal occlusive volume. These techniques help prevent tracheal irritation and damage caused by high cuff pressure; always practice them with an experienced nurse or respiratory therapist. Never add air to the cuff without using proper technique.
8. For optimal outcomes, ventilator patients must be well nourished and should begin taking nutrition early. But like any patient who can’t swallow normally, they need an alternative nutrition route. Preferably, they should have feeding tubes with liquid nutrition provided through the gut. If this isn’t possible, the healthcare team will consider parenteral nutrition.
9. As your patient’s indications for mechanical ventilation resolve and she’s able to take more breaths on her own, the healthcare team will consider removing her from the ventilator. Weaning methods may vary by facility and provider preference.
10. Seeing a loved one attached to a mechanical ventilator is frightening. To ease distress in the patient and family, teach them why mechanical ventilation is needed and emphasize the positive outcomes it can provide. Each time you enter the patient’s room, explain what you’re doing. Reinforce the need and reason for multiple assessments and procedures, such as laboratory tests and X-rays. Communicate desired outcomes and progression toward outcomes so the patient and family can actively participate in the plan of care.
Immunomodulating treatmentEffective immunomodulating treatment can lessen nerve damage, reduce progression, and shorten hospitalization. Plasmapheresis and IVIG are the mainstay of immunomodulatory treatment at present. Both treatments have proven to exhibit beneficial effects in various controlled trials by favorably altering the natural course of the disease. Their effectiveness is similar and both appear to be more effective than supportive treatment alone. Corticosteroids are still a doubtful topic in the treatment of GBS.
Nursing Consideration:The nurse is tasked with educating, instructing and supporting the patient at every stage of the disease and treatment. The nurse co-ordinates the care, chooses and advises the patient on the forms of help they can and should receive. Nurses should evaluate patient’s ability to perform activities of daily living (ADLs) and instrumental ADL (IADL) secondary activities related to independent living and safety issues at home, and employ interventions such as home health care services in patients. Nurses should use adult verbal or non-verbal pain scales for assessing neuropathic pain, and be guided by the world health organization (WHO) ladder of pain management.
The nurse should begin with:1. establishing rapport2. identifying the patient's nursing problems adequately to the stage of the disease3. adjusting the nursing procedures to the patient's age4. assessing the patient and their family's knowledge regarding immunomodulatory therapies5. assessing the patient's disability (neurological disorders)6. providing the patient with information regarding the disease, diet, lifestyle and non-
pharmacological methods of alleviating the symptoms7. adjusting this information to the patient and their family's needs and expectations, as well as to
the current stage of the patient's disease8. denying untrue information9. eliminating anxiety10. organizing a support group (family, friends, other patients)11. The nurse informs the patient of the possibility of adverse effects occurring in the course of an
immunomodulatory therapy.
High-dose immunoglobulinThe empirical dose of IVIG generally used for the treatment of GBS is 0.4 g/kg per day for 5 days. There was a non-significant trend toward a better outcome noted in the group receiving longer treatment of 6 days, and this trend reached significance when only ventilated patients were considered, but the shorter course such as 3 days was proven to be significantly less effective.
Nursing Consideration:Whether the nurse is administering an intravenous infusion or teaching patients to administer their own subcutaneous infusion, safety should always be the first priority. The prescriber’s orders should be carefully followed and any problems with the orders should be addressed and resolved before the infusion
Before:1. Assess that the immunoglobulin product ordered is appropriate for the patient.2. Assess product integrity3. Assess product temperature4. Assess level of patient’s understanding of therapy5. Assess the patient’s general health and hydration status6. Assess for any weight loss or gain7. Assess heart rate and respiratory status8. Assess for fever prior to the start of infusion9. Assess the need for premedication10. Assess the need for localized anesthesia and obtain an order as necessary11. Emergency equipment should be readily available during the infusion12. Assess need for laboratory blood work prior to start of infusion
During:1. Assess the patient to ensure that the infusion is being tolerated
After:1. Assess for any problems occurring after the infusion which may be infusion related. These can
include headaches, myalgias, fever, arthralgias, rashes or a subjective feeling of general “unwellness.”
2. Assess the need for premedications for future infusions3. Assess the patient for his/her knowledge about the next infusion.
Plasma exchange (PE)PE is the first immunomodifying therapy proven to be effective in the treatment of GBS. Two exchanges are better than none for mild GBS, for moderate GBS as well as for severe cases. Four plasma exchange sessions are sufficient, further sessions are not helpful if there is no response to IVIG or if there is further deterioration during this treatment. The PE regimen involved exchange of approximately one plasma volume, 50 ml/kg. There are more adverse events with fresh frozen plasma as the replacement fluid than albumin. Five percent albumin solution is commonly used as the replacement solution unless there is an increased risk of bleeding, then fresh frozen plasma will be more appropriate.
Nursing Consideration:1. Educated and deemed competent in TPE. 2. Assess patient status prior to TPE. 3. Maximize patient comfort. 4. Educate patient about TPE
5. Plan and deliver safe effective treatment. 6. Documentation of treatment.
Before:1. Teach about the procedure and what to expect, including what the machine looks like, the need
for arterial and venous insertion sites, and the length of time of the procedure (2-5hours). Giving information, answering questions and addressing concerns decreases anxiety.
2. Check with physician about holding medications until after the procedure. Medications may be removed from the body as an incidental part of the plasmapheresis process.
3. Assess vital signs and weight. Baseline parameters are necessary to evaluate for fluid imbalances and response to therapy.
4. Assess CBC, platelet count and clotting studies. Clients undergoing plasmapheresis are at high risk of anemia and coagulation problems secondary to hemolysis of cells.
5. Check blood type and cross match for replacement blood products. Hypersensitivity reactions can occur and close monitoring is important.
During and After:1. Observe for dizziness or hypotension. Hypovolemia is a complication of plasma exchange,
especially during the procedure when up to 15% of the client’s blood volume is in the cell separator.
2. Apply pressure dressing to access site(s). Direct pressure helps decrease or prevents bleeding.3. Monitor infection and bruises at the intravenous port site. The site of vascular access is at risk
for complications and must be routinely and carefully assessed for signs of infection and for bleeding or hematoma formation.
4. Monitor electrolytes and signs of electrolyte loss. Report imbalances and replace electrolytes as ordered. Observe for circumoral tingling, Chvostek’s and Trosseau’s signs if calcium levels are low, and cardiac dysrhythmias and leg cramps if potassium are low. Hypocalcemia and hypokalemia may occur. Hypocalcemia occurs because the anticoagulant citrate dectrose binds with calcium.
5. Reevaluate preprocedure laboratory data, especially CBC, platelet count, and clotting times. The cell-separating process can damage cells; anticoagulation is part of the procedure.
CorticosteroidsCorticosteroids are widely used to treat many autoimmune disorders and once expected to be effective for GBS. However, the majority of trials showed no benefit from corticosteroids. A Dutch trial suggested the combination of intravenous methylprednisolone followed by IVIG hastens the recovery of GBS patients slightly more than IVIG alone. There is another report showing that corticosteroids may be effective against pain from GBS. Because of lack of more findings that support the efficacy of corticosteroids in GBS, corticosteroids are not recommended or at least should not be used alone in the treatment of GBS.
Nursing Consideration:Assessment:
1. Establish baseline and continuing data on BP, weight, fluid and electrolyte balance, and blood glucose.
2. Lab tests: Periodic serum electrolytes blood glucose, Hct and Hgb, platelet count, and WBC with differential.
3. Monitor for adverse effects. Older adults and patients with low serum albumin are especially susceptible to adverse effects.
4. Be alert to signs of hypocalcemia.
5. Ophthalmoscopic examinations are recommended every 2–3 months, especially if patient is receiving ophthalmic steroid therapy.
6. Monitor for persistent backache or chest pain; compression and spontaneous fractures of long bones and vertebrae present hazards.
7. Monitor for and report changes in mood and behavior, emotional instability, or psychomotor activity, especially with long-term therapy.
8. Be alert to possibility of masked infection and delayed healing (anti-inflammatory and immunosuppressive actions).
9. Dose adjustment may be required if patient is subjected to severe stress (serious infection, surgery, or injury).
10. Single doses of corticosteroids or use for a short period (<1 week) do not produce withdrawal symptoms when discontinued, even with moderately large doses.
Patient & Family Education1. Expect a slight weight gain with improved appetite. After dosage is stabilized, notify physician of
a sudden slow but steady weight increase [2 kg (5 lbs)/week].2. Avoid alcohol and caffeine; may contribute to steroid-ulcer development in long-term therapy.3. Do not ignore dyspepsia with hyperacidity. Report symptoms to physician and do NOT self-
medicate to find relief.4. Do NOT use aspirin or other OTC drugs unless prescribed specifically by the physician.5. A high protein, calcium, and vitamin D diet is advisable to reduce risk of corticosteroid-induced
osteoporosis.6. Notify physician of slow healing, any vague feeling of being sick, or return to pretreatment
symptoms.7. Do not abruptly discontinue drug; doses are gradually reduced to prevent withdrawal
symptoms.8. Report exacerbation of disease during drug withdrawal.9. Carry medical identification at all times. It needs to indicate medical diagnosis, drug therapy,
and name of physician.10. Apply topical preparations sparingly in small children. The hazard of systemic toxicity is higher
because of the greater ratio of skin surface area to body weight.11. Check shelf-life date on topical corticosterone during long-term use.12. Do not breast feed while taking/using this drug without consulting physician
Other treatmentsRehabilitation is necessary for the recovery of GBS patients. Treatment in the acute phase should include an individual program of gentle exercises involving isometric, isotonic, isokinetic, and manual resistive and progressive resistive exercises. Rehabilitation should be focused on proper limb positioning, posture, orthotics, and nutrition. Remission occurs in 70% of the patients though half of them remain mildly affected, being better in younger patients. Ten to twenty percent of the patients have a disability and mortality rate of 5% and 10% respectively. A few GBS patients could finally turn out to have CIDP.
Nursing Consideration:During the acute and recovery phases, show the patient and family how to perform range-of-motion exercises and establish an exercise program that places the patient’s joints through their full range of motion every 8 hours. Proper positioning is vital to maintaining optimal joint function. The ideal joint position is neutral.
Splints, orthotic devices and adjunctive aids may be indicated to prevent or correct joint contractures. Isometric and isotonic exercises of uninvolved or partially involved muscle groups should accompany
range-of-motion exercises. Patients must avoid too frequent or vigorous exercise because it may contribute to demyelination. Exercise goals-set mutually with the patient and family-should be celebrated with positive reinforcement when achieved.
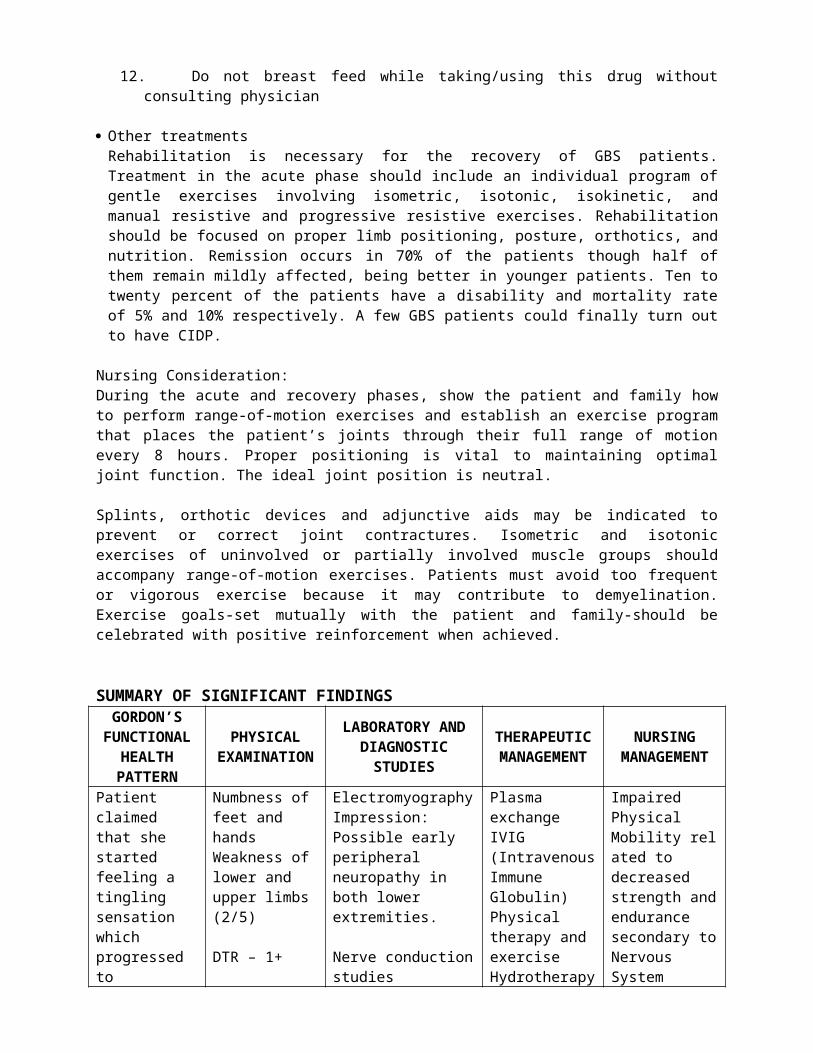
SUMMARY OF SIGNIFICANT FINDINGSGORDON’S
FUNCTIONAL HEALTH
PATTERN
PHYSICAL EXAMINATION
LABORATORY AND DIAGNOSTIC STUDIES
THERAPEUTIC MANAGEMENT
NURSING MANAGEMENT
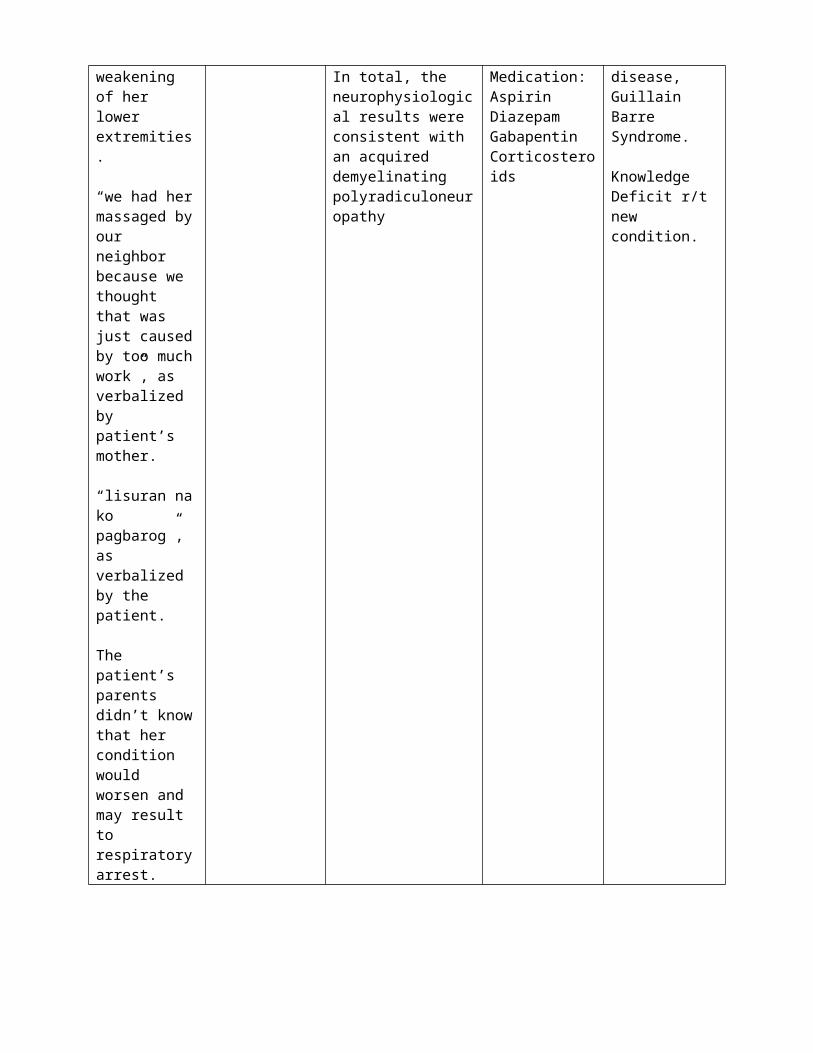
Patient claimed that she started feeling a tingling sensation which progressed to weakening of her lower extremities.
“we had her massaged by our neighbor because we thought that was just caused by too much work”, as verbalized by patient’s mother.
“lisuran na ko pagbarog”, as verbalized by the patient.
The patient’s parents didn’t know that her condition would worsen and may result to respiratory arrest.
Numbness of feet and handsWeakness of lower and upper limbs (2/5)
DTR – 1+
ElectromyographyImpression: Possible early peripheral neuropathy in both lower extremities.
Nerve conduction studiesIn total, the neurophysiological results were consistent with an acquired demyelinatingpolyradiculoneuropathy
Plasma exchangeIVIG (Intravenous Immune Globulin)Physical therapy and exerciseHydrotherapyMedication:AspirinDiazepamGabapentinCorticosteroids
Impaired Physical Mobility related to decreased strength and endurance secondary to Nervous System disease, Guillain Barre Syndrome.
Knowledge Deficit r/t new condition.
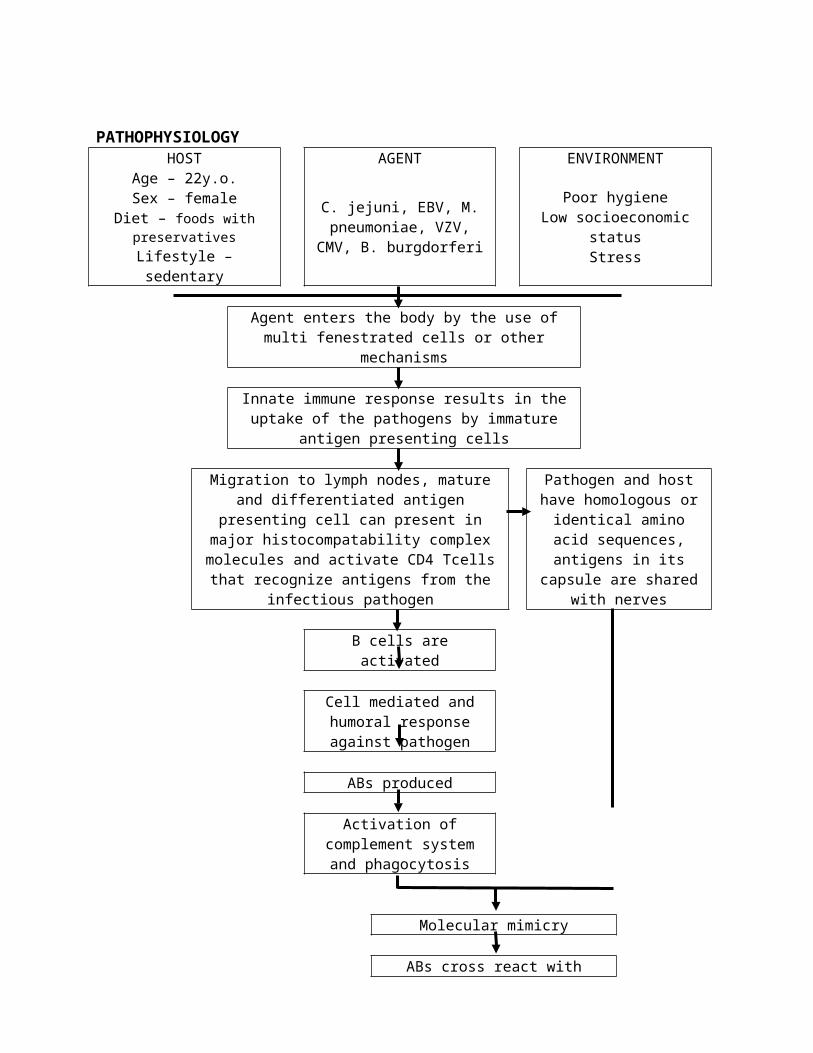
PATHOPHYSIOLOGYHOST AGENT ENVIRONMENT
Age – 22y.o.Sex – female
Diet – foods with preservativesLifestyle – sedentary
C. jejuni, EBV, M. pneumoniae, VZV, CMV, B.
burgdorferi
Poor hygieneLow socioeconomic status
Stress
Agent enters the body by the use of multi fenestrated cells or other mechanisms
Innate immune response results in the uptake of the pathogens by immature antigen presenting cells
Migration to lymph nodes, mature and differentiated antigen presenting cell can present in major histocompatability complex molecules and activate CD4 Tcells that recognize antigens
from the infectious pathogen
Pathogen and host have homologous or identical amino acid sequences,
antigens in its capsule are shared with nerves
B cells are activated
Cell mediated and humoral response against pathogen
ABs produced
Activation of complement system and phagocytosis
Molecular mimicry
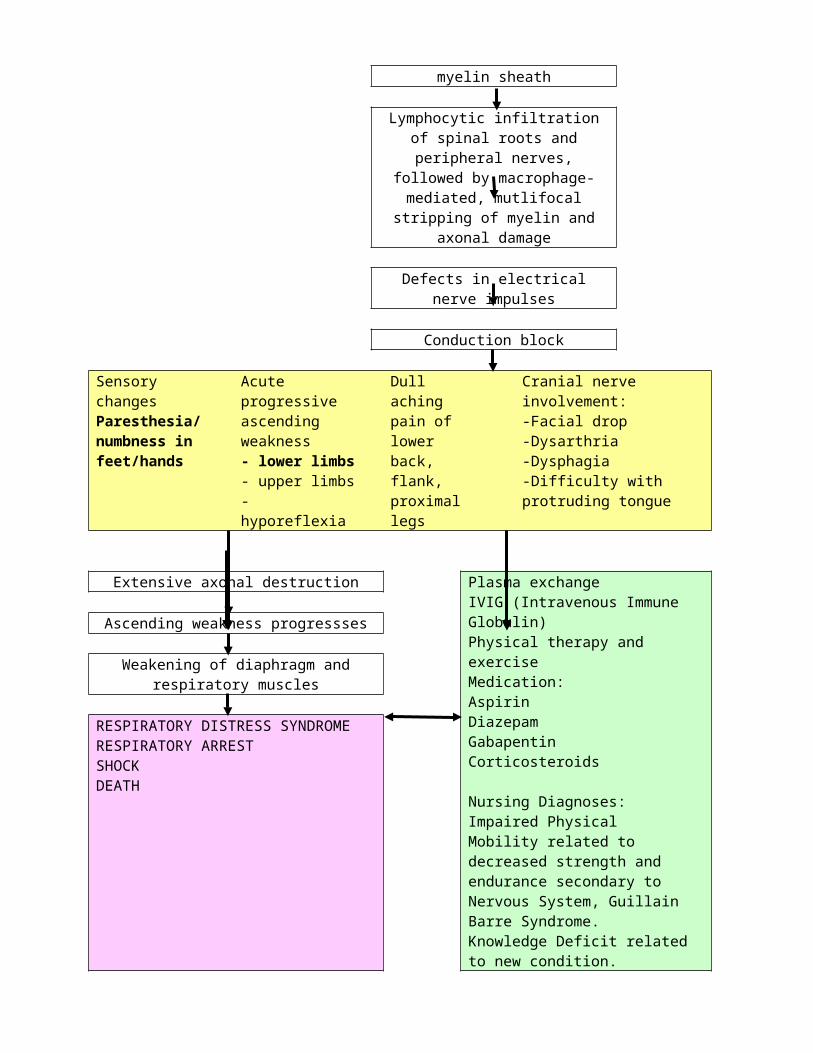
ABs cross react with myelin sheath
Lymphocytic infiltration of spinal roots and peripheral nerves, followed by macrophage-mediated, mutlifocal
stripping of myelin and axonal damage
Defects in electrical nerve impulses
Conduction block
Sensory changesParesthesia/ numbness in feet/hands
Acute progressive ascending weakness- lower limbs- upper limbs- hyporeflexia
Dull aching pain of lower back, flank, proximal legs
Cranial nerve involvement:-Facial drop-Dysarthria-Dysphagia-Difficulty with protruding tongue
Extensive axonal destruction Plasma exchangeIVIG (Intravenous Immune Globulin)Physical therapy and exerciseMedication:AspirinDiazepamGabapentinCorticosteroids
Nursing Diagnoses:Impaired Physical Mobility related to decreased strength and endurance secondary to Nervous System, Guillain Barre Syndrome.Knowledge Deficit related to new condition.
Ascending weakness progressses
Weakening of diaphragm and respiratory muscles
RESPIRATORY DISTRESS SYNDROMERESPIRATORY ARRESTSHOCKDEATH
CARE MAP
Part I. Nursing Diagnostic Reasoning: Analysis of Data
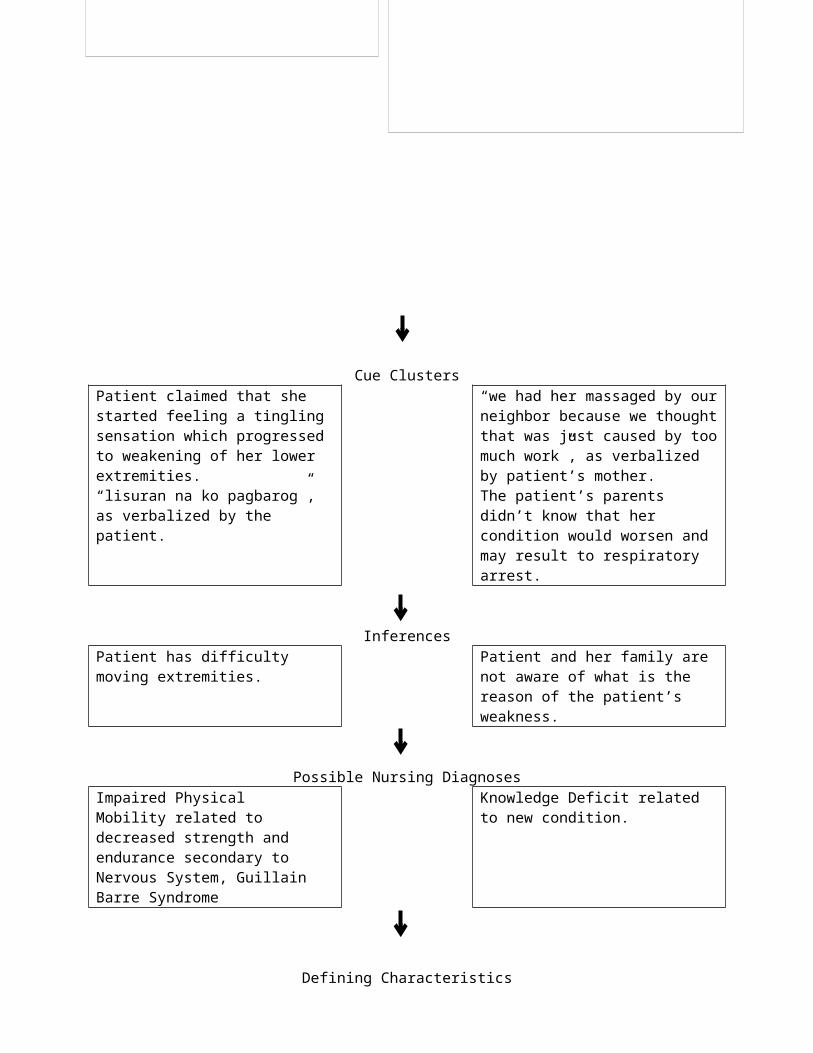
Cue ClustersPatient claimed that she started feeling a tingling sensation which progressed to weakening of her lower extremities.“lisuran na ko pagbarog”, as verbalized by the patient.
“we had her massaged by our neighbor because we thought that was just caused by too much work”, as verbalized by patient’s mother.The patient’s parents didn’t know that her condition would worsen and may result to respiratory arrest.
InferencesPatient has difficulty moving extremities.
Patient and her family are not aware of what is the reason of the patient’s weakness.
Possible Nursing DiagnosesImpaired Physical Mobility related to decreased strength and endurance secondary to Nervous System, Guillain Barre Syndrome
Knowledge Deficit related to new condition.
Subjective DataPatient claimed that she started feeling a tingling sensation which progressed to weakening of her lower extremities.
“we had her massaged by our neighbor because we thought that was just caused by too much work”, as verbalized by patient’s mother.
“lisuran na ko pagbarog”, as verbalized by the patient.
The patient’s parents didn’t know that her condition would worsen and may result to respiratory arrest.
Objective DataNumbness of feet and handsDTR – 1+Weakness of lower and upper limbs (2/5)
ElectromyographyImpression: Possible early peripheral neuropathy in both lower extremities.
Nerve conduction studiesIn total, the neurophysiological results were consistent with an acquired demyelinating polyradiculoneuropathy
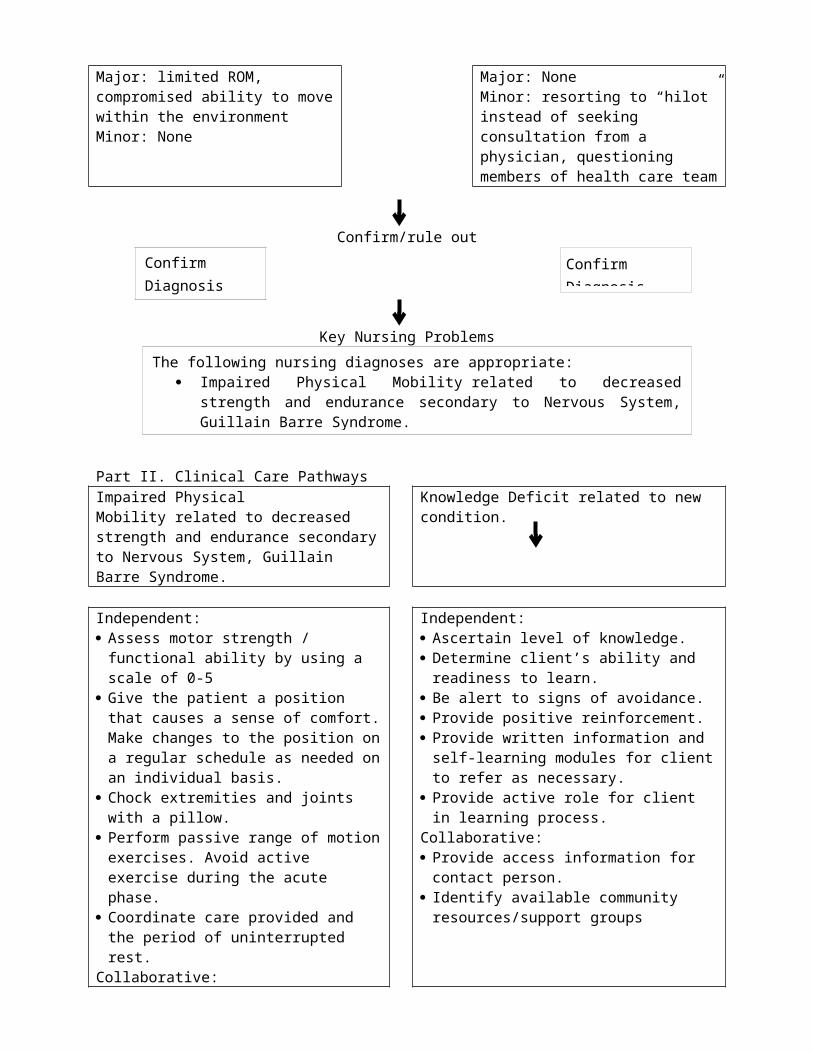
Defining CharacteristicsMajor: limited ROM, compromised ability to move within the environmentMinor: None
Major: NoneMinor: resorting to “hilot” instead of seeking consultation from a physician, questioning members of health care team
Confirm/rule out
Key Nursing Problems
Part II. Clinical Care PathwaysImpaired Physical Mobility related to decreased strength and endurance secondary to Nervous System, Guillain Barre Syndrome.
Knowledge Deficit related to new condition.
Independent: Assess motor strength / functional ability by
using a scale of 0-5 Give the patient a position that causes a
sense of comfort. Make changes to the position on a regular schedule as needed on an individual basis.
Chock extremities and joints with a pillow. Perform passive range of motion exercises.
Avoid active exercise during the acute phase. Coordinate care provided and the period of
uninterrupted rest.Collaborative: Confirm with / refer gets physical therapy /
occupational therapy Administer medications as prescribed.
Independent: Ascertain level of knowledge. Determine client’s ability and readiness to
learn. Be alert to signs of avoidance. Provide positive reinforcement. Provide written information and self-learning
modules for client to refer as necessary. Provide active role for client in learning process.Collaborative: Provide access information for contact person. Identify available community resources/support
groups
After the holistic nursing intervention Client will be able to:Verbalize understanding of situation and individual treatment regimen and safety measures.Demonstrate techniques/behaviors that enables resumption of activities.Participate in ADLs and desired activities.Maintain position of function and skin integrity.
After the holistic nursing intervention Client will be able to:Participate in learning process.Identify interferences to learning and specific action to deal with them.Exhibit increased interest/assume responsibility for own learning by beginning to look for information and ask question.Verbalize understanding of condition/disease
Confirm Diagnosis Confirm Diagnosis
The following nursing diagnoses are appropriate: Impaired Physical Mobility related to decreased strength and endurance
secondary to Nervous System, Guillain Barre Syndrome. Knowledge Deficit related to new condition.
Maintain or increase strength and function of affected and/or compensatory body part.
process and treatment.Identify relationship of signs/symptoms to the disease process and correlate symptoms with causative factors.Perform necessary procedures correctly and explain reasons for the actions.Initiate necessary lifestyle changes and participate in treatment regimen.

Dennis L. Zacarias
REFLECTING ON PRACTICE: CARE OF A CLIENT WITH IMMUNE-MEDIATED DISORDER - IDIOPATHIC THROMBOCYTOPENIC PURPURA
REFLECTING ON PRACTICE: CLIENT PROFILE AND CASE STUDYThis is a case of a 2-month old baby boy born on September 23, 2009 via normal spontaneous delivery with assisted midwife at their home in Talisay City. In the course of this study, the patient was named as Noynoy to protect his identity. Noynoy and his parents are currently residing at Talisay City. His father is a born-again Christian while his mother is a Seventh-day Adventist believer. Both of his parents are a Filipino citizen and finished secondary education. Noynoy’s mother is a plain housewife while his father is a habal-habal driver. In this study the informants are his parents.
Noynoy was admitted at Pediatric unit of Vicente Sotto Memorial Medical Center on November 27, 2009 with an initial diagnosis of Idiopathic Thrombocytopenic Purpura vs Evans Syndrome. He was discharged on December 10, 2009 with the final diagnosis of Idiopathic Thrombocytopenic Purpura.
Celebrating Practice:Patient was admitted to the hospital with increased body temperature of 39.3C orally. After 30 minutes of nursing interventions, patient’s temperature was decreased to 37.5.
Effective/Efficient/Sensitive careThe nursing interventions are the following:
Monitor patient temperature every hour. Provided tepid sponge bath. Limit excess clothing. Encourage mother to have the baby drink plenty of fluids.
Collaborative care: Informed dietary department to include fruit juice on his diet due to his high fever. Administer antipyretics as ordered.
Correcting Practice:The health condition of the patient depends on how his family would react with it. Noynoy’s parents have accepted his diagnosis and are eager to help him recover. They are very open to all options that are possible for Noynoy’s recovery. The need for guidance is needed since the family is at risk of accepting false ideas on how to cure their son.
Understanding Self:Being a nurse, having a child close to me with the same diagnosis helped me understand how I should care for Noynoy. I would be open to any hearsay on how to help that child. This made me understand how important health education is.
Understanding Others:His family’s acceptance of the diagnosis is a good start in order to provide effective caring for the patient. They will not be hesitant and will be cooperative in every procedure. However, proper communication is needed in order for them to understand what is happening.
Understanding Profession:The role of a nurse is important in such a way that we manage the health care done to patients. We are the ones who collaborate with other health care providers such as physicians, dieticians, medical
technologists, etc. Thorough analysis is needed in order to arrive at a correct nursing diagnosis and provide effective and efficient nursing care.
Challenging AssumptionAnother new option for patients with ITP is eltrombopag, a nonpeptide TPO receptor agonist that can be given once daily orally on an empty stomach. Eltrombopag inhibits the organic anion transporting polypeptide OATP1B1, which can increase the levels of drugs that are substrates for this enzyme. Eltrombopag is distributed through a restricted distribution program similar to that for romiplostim. The prescribing information carries a black-box warning for hepatotoxicity, and unlike the package insert for romiplostim, the literature for eltrombopag warns of cataracts.
Nursing Consideration:1. Modify the dosage regimen of concomitant idiopathic thrombocytopenic purpura medication to
avoid excessive increases in platelet counts during therapy with eltrombopag.2. Do not administer more than one dose in any 24 hr period.3. Reduce the initial dose to 25 mg once daily in clients with moderate to severe hepatic
impairment.4. Discontinue if platelet count does not increase to a level sufficient to avoid clinically important
bleeding after 4 weeks of therapy.5. Store tablets from 15-30C.
SUMMARY OF SIGNIFICANT FINDINGSGORDON’S
FUNCTIONAL HEALTH PATTERN
PHYSICAL EXAMINATION
LABORATORY AND DIAGNOSTIC
STUDIES
THERAPEUTIC MANAGEMENT
NURSING MANAGEMENT
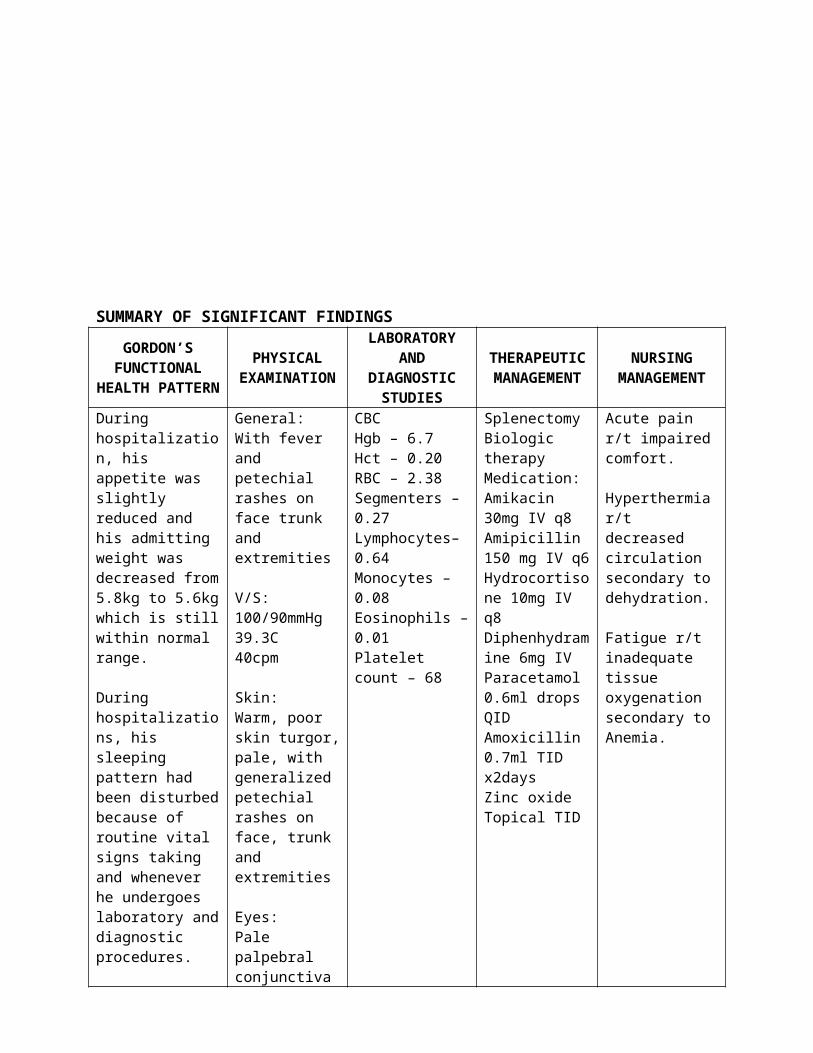
During hospitalization, his appetite was slightly reduced and his admitting weight was decreased from 5.8kg to 5.6kg which is still within normal range.
During hospitalizations, his sleeping pattern had been disturbed because of routine vital signs taking and whenever he undergoes laboratory and diagnostic procedures.
When the fever had gradually decreased but the rashes all over his body remained, they got worried and brought him to the nearest hospital.
The mother noticed that Noynoy is not playful every time they play with him.
As per patient’s mother, Noynoy always cry and seems to be in pain.
General:With fever and petechial rashes on face trunk and extremities
V/S:100/90mmHg39.3C40cpm
Skin:Warm, poor skin turgor, pale, with generalized petechial rashes on face, trunk and extremities
Eyes:Pale palpebral conjunctivaConjunctival hemorrhage
Mouth:Petechial rashes on buccal mucosa, dry oral mucosa
Hematologic:Easy bruising or bleeding
CBCHgb – 6.7Hct – 0.20RBC – 2.38Segmenters – 0.27Lymphocytes–0.64Monocytes – 0.08Eosinophils – 0.01Platelet count – 68
SplenectomyBiologic therapyMedication:Amikacin 30mg IV q8Amipicillin 150 mg IV q6Hydrocortisone 10mg IV q8Diphenhydramine 6mg IVParacetamol 0.6ml drops QIDAmoxicillin 0.7ml TID x2daysZinc oxide Topical TID
Acute pain r/t impaired comfort.
Hyperthermia r/t decreased circulation secondary to dehydration.
Fatigue r/t inadequate tissue oxygenation secondary to Anemia.
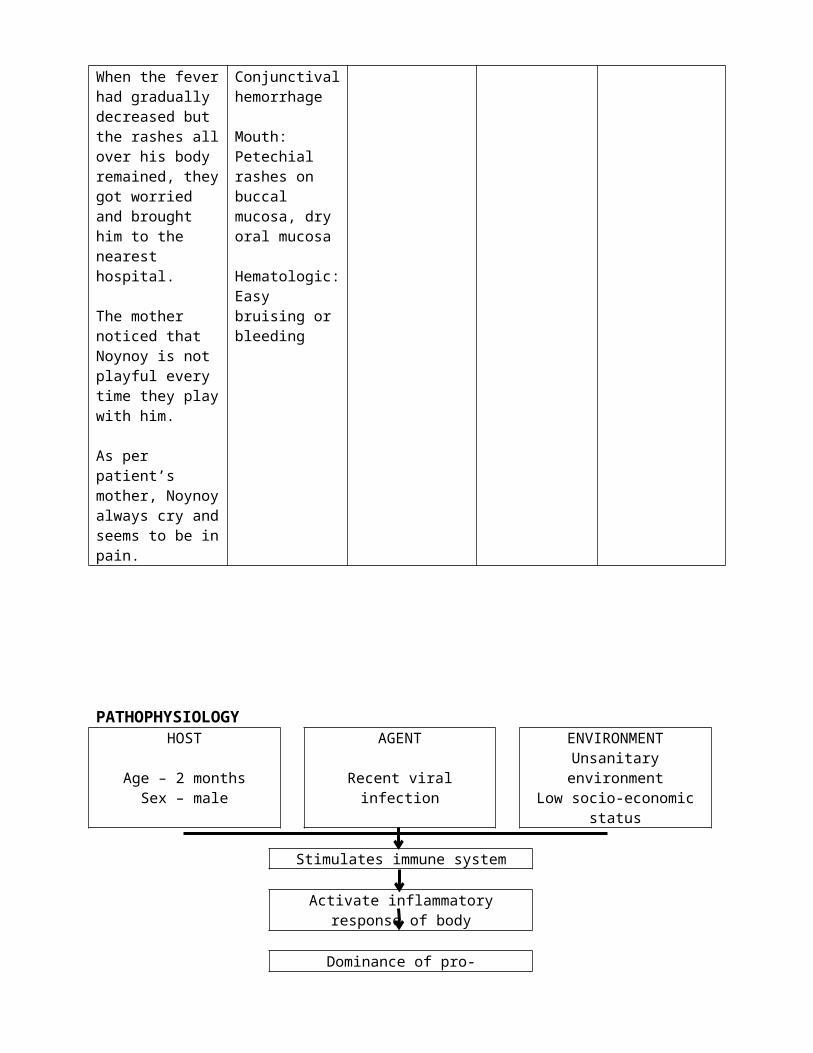
PATHOPHYSIOLOGYHOST AGENT ENVIRONMENT
Age – 2 monthsSex – male
Recent viral infection Unsanitary environmentLow socio-economic status
Stimulates immune system
Activate inflammatory response of body
Dominance of pro-inflammatory cytokines Tcell repertoire
Abnormal autoimmune reaction
Production of ABs
ABs bind with viral/bacterial AG React with platelet membrane
Platelet become antigenic
Increases production of ABs against glycoprotein
Increase number of cytotoxic cells
Phagocytosed by splenic macrophages
IgG coats the platelets Increase demand in # of platelets
Destruction of platelets Increase workload of megakaryotes
Damaged megakaryotes
Decrease platelet count Decrease platelet lifespan
Altered clotting
Local hemorrhage
Decrease blood volume Dehydration Narrow pulse pressureDecrease Hgb and RBC Pallor Decrease O2 supplyWeakness Fever PainLow Hgb Low RBC count Low Hct
HEMORRHAGIC SHOCKINTRACRANIAL HEMORRHAGEPERMANENT DAMAGE & LOSS OF BRAIN FUNCTIONDEATH
CT ScanBone Marrow Aspiration (BMA)Blood transfusionSplenectomyBiologic therapyMedication:Amikacin 30mg IV q8Amipicillin 150 mg IV q6Hydrocortisone 10mg IV q8Diphenhydramine 6mg IVParacetamol 0.6ml drops QIDAmoxicillin 0.7ml TID x2daysZinc oxide Topical TID
Nursing Diagnosis:Acute pain r/t impaired comfort.
Hyperthermia r/t decreased circulation secondary to dehydration.
Fatigue r/t inadequate tissue oxygenation secondary to Anemia.
CARE MAPPart I. Nursing Diagnostic Reasoning: Analysis of Data
Cue Clusters
Subjective DataDuring hospitalization, his appetite was slightly reduced and his admitting weight was decreased from 5.8kg to 5.6kg which is still within normal range.During hospitalizations, his sleeping pattern had been disturbed because of routine vital signs taking and whenever he undergoes laboratory and diagnostic procedures.When the fever had gradually decreased but the rashes all over his body remained, they got worried and brought him to the nearest hospital.The mother noticed that Noynoy is not playful every time they play with him.As per patient’s mother, Noynoy always cry and seems to be in pain.
Objective DataGeneral: With fever and petechial rashes on face trunk and extremitiesV/S: 100/90mmHg, 39.3C, 40cpmSkin: Warm, poor skin turgor, pale, with generalized petechial rashes on face, trunk and extremitiesEyes: Pale palpebral conjunctivaConjunctival hemorrhageMouth: Petechial rashes on buccal mucosa, dry oral mucosaHematologic: Easy bruising or bleedingCBC: Hgb – 6.7, Hct – 0.20, RBC – 2.38, Segmenters – 0.27, Lymphocytes–0.64, Monocytes – 0.08, Eosinophils – 0.01, Platelet count – 68
Platelet count – 68Conjunctival hemorrhagePetechial rashes on buccal mucosa, paleEasy bruising or bleedinggeneralized petechial rashes on face, trunk and extremitiesAs per patient’s mother, Noynoy always cry and seems to be in pain.V/S: 100/90mmHg; 39.3C; 40cpm
The mother noticed that Noynoy is not playful every time they play with him.Pale palpebral conjunctivaHgb – 6.7; Hct – 0.20; RBC – 2.38
With fever Warm skinT - 39.3CLymphocytes–0.64Monocytes – 0.08; Eosinophils – 0.01Increase respiratory rate – 40cpmPoor skin turgorDry oral mucosa, As per patient’s mother, Noynoy always cry and seems to be in pain.
Inferences
Possible Nursing Diagnoses
Defining Characteristics
Confirm/rule out
Key Nursing Problems
Client is in pain. Client is possibly tired to counter act with his environment.
Client is hyperthermic.
Hyperthermia r/t decreased circulation
secondary to dehydration.
Acute pain r/t impaired comfort.
Fatigue r/t inadequate tissue oxygenation
secondary to Anemia.
Major: cryingMinor: increased respiratory rate – 40cpm, crying
Major: pale palpebral conjunctiva, Hgb – 6.7, Hct – 0.20, RBC – 2.38Minor: not playful
Major: T – 39.3C, Lymphocytes – 0.64, Monocytes – 0.08, Eosinophils – 0.01Minor: none
Confirm Diagnosis Confirm Diagnosis Confirm Diagnosis
The following nursing diagnoses are appropriate: Acute pain r/t impaired comfort. Hyperthermia r/t decreased circulation secondary to dehydration. Fatigue r/t inadequate tissue oxygenation secondary to Anemia.
Major: crying, inability to maintain usual routinesMinor: none
Major: T – 39.3C, Minor: warm skin, increased respiratory rate 40cpm, Dehydration, in pain, weakness
Part II. Clinical Care Pathways
Independent: Assessed and monitored
vital signs. Assessed for any signs of
bleeding. Monitored platelet count. Avoided IV/SC injections and
rectal procedures as necessary.
Placed sign over patient’s bed as reminder of bleeding precautions.
Maintained safe environment for patient.
Collaborative: Transfused platelet
concentrate as prescribed. Administered orally
Hydrocortisone as ordered.MOA: Hydrocortisone inhibits the delayed hypersensitivity reaction and cellular cytotoxic activity.
Independent: Assessed functional
ability/extent of impairment initially and on a regular basis.
Evaluated action of irritability and fatigue of the patient from parents.
Provided quiet environment and uninterrupted rest periods.
Encouraged parents to have rest periods for the child before feeding.
Instructed parents and assisted in changing positions every 2 hours.
Set goals with parents for play or activities of the baby.
Recommended breast feeding for the baby.
Monitored CBC results.
Collaborative: Transfused PRBC and
platelet concentrate as prescribed.
Provided supplemental fluids such as IVF#5 (D5IMB 500cc x 24cc/hr)
Independent: Monitored client
temperature. Moqnitored environmental
temperature Provided tepid sponge bath,
avoided use of alcohol. Provided blankets.
Collaborative: Administered orally Calpol as
indicated.MOA: Acetaminophen belongs to a class of drugs called analgesics (pain relievers) and antipyretics (fever reducers). It may reduce the production of prostaglandins in the brain. Prostaglandins are chemicals that cause inflammation and swelling. Acetaminophen relieves pain by elevating the pain threshold, that is, by requiring a greater amount of pain to develop before a person feels it. It reduces fever through its action on the heat-regulating center of the brain. Specifically, it tells the center to lower the body's temperature when the temperature is elevated.
Acute pain r/t impaired comfort
Fatigue r/t inadequate tissue oxygenation secondary to Anemia
Hyperthermia r/t decreased circulation secondary to dehydration
Goals partially met. After 8 hours shift, patient still at risk for bleeding but eventually reduced as evidenced by vital signs within normal range, absence of narrowed pulse pressure and diminished signs of bleeding.V/S:90/60mmHg, 36.2C, 122bpm, 34 cpm
After 3 days of nursing interventions, patient maintained reduced risk for bleeding as evidenced by dimished signs of bleeding.Platelet – 10Hgb – 0.28Hct – 0.96
Goal partially met. Patient was able to demonstrate measurable increase in activity through being responsive to others but still maintained low levels of CBC results making the patient less energetic.
After 3 days of nursing interventions, patient was able to participate in play activity as evidenced by smiling and energetic movements whenever parents and nurses made cooing sounds or provide colorful objects.
Goal met. After 2 hours of nursing intervention, patient’s body temperature decreased as evidenced by normal body temperature of 37.5C and absence of any complications.
After 2-3 days of nursing interventions, patient’s body temperature remained stable.