Embed Size (px)
DESCRIPTION
bgjhgvhjg
Citation preview

Nursing Case Study
Guillain- Barre Syndrome
A Case Study
Presented to the faculty of Nursing
University of St. La Salle
In partial fulfillment of the requirements
For NCM104
Presented by:
Keeshia Marie Magbanua
Rhea Marie V. Montes
Joe Vincent Montinola
Ariana C. Natiag
Ramadel C. Nervez
Kimberly Nimanand
Louella Marie Onday
Fe Padrino
Tess Marie Pagunsan
Rhealine Joy C. Poblete
BN3F-Group 3
1

March 18, 2011
Table of Contents
I. Introduction……………………………………………………………. 3
II. Objectives…………………………………………………………….....4
III. Anatomy and Physiology……………………………………………… 5
IV. Definition of Terms……………………………………………………..7
V. Baseline Data…………………………………………………………....8
VI. Nursing History (Gordon’s Functional Health Pattern)…….………..….9
VII. Health History………………………………………………………..... 11
VIII. Assessment………………………………………………………….…. 12
IX. Laboratory and Radiology……………………………………….……...15
X. Pathophysiology…………………………………………….................. 18
XI. Nursing Care Plan……………………………………………….…….. .29
XII. Drug Study……………………………………………………….……. .35
XIII. Health Teaching………………………………………………………. .42
XIV. Bibliography……………………………………………………………. 45
2

I. Introduction
Guillain-Barré syndrome is a disorder in which the body's immune system attacks part of
the peripheral nervous system. The first symptoms of this disorder include varying degrees of
weakness or tingling sensations in the legs. In many instances, the weakness and abnormal
sensations spread to the arms and upper body. In these cases, the disorder is life-threatening and
is considered a medical emergency. The patient is often put on a respirator to assist with
breathing.
Guillain-Barré syndrome is rare. Usually Guillain-Barré occurs a few days or weeks after
the patient has had symptoms of a respiratory or gastrointestinal viral infection. Occasionally,
surgery or vaccinations will trigger the syndrome. The disorder can develop over the course of
hours or days, or it may take up to 3 to 4 weeks. No one yet knows why Guillain-Barré strikes
some people and not others or what sets the disease in motion. What scientists do know is that
the body's immune system begins to attack the body itself, causing what is known as an
autoimmune disease. Guillain-Barré is called a syndrome rather than a disease because it is not
clear that a specific disease-causing agent is involved.
As Lasallian nurses, our main goal is to provide care for our patient. Help them cope with
their conditions and be the ones to lighten their minds with every medical procedure that they are
about to face.
The purpose of this case study is to understand the syndrome, its main cause and how to
treat it to help what our client is going into. The significance of this case study is to help others
in coping up with their health status and as well as to help us understand it well.
We hope that at the end of this study, the reader will be able to understand and to be
aware about this syndrome.
III. Anatomy and Physiology
Immune System
The immune system, which is made up of special cells, proteins, tissues, and organs, defends
people against germs and microorganisms every day. In most cases, the immune system does a
3

great job of keeping people healthy and preventing infections. But sometimes problems with the
immune system can lead to illness and infection.
The immune system is the body's defense against infectious organisms and other invaders.
Through a series of steps called the immune response, the immune system attacks organisms
and substances that invade our systems and cause disease. The immune system is made up of a
network of cells, tissues, and organs that work together to protect the body.
Peripheral Nerves
The peripheral nervous system consists of more than 100 billion nerve cells that run throughout
the body like strings, making connections with the brain, other parts of the body, and often with
each other. Peripheral nerves consist of bundles of nerve fibers. These fibers are wrapped with
many layers of tissue composed of a fatty substance called myelin. These layers form the myelin
sheath, which speeds the conduction of nerve impulses along the nerve fiber. Nerves conduct
impulses at different speeds depending on their diameter and on the amount of myelin around
them.
The peripheral nervous system has two parts: the somatic nervous system and the autonomic
nervous system.
Somatic Nervous System: This system consists of nerves that connect the brain and spinal cord
with muscles controlled by conscious effort (voluntary or skeletal muscles) and with sensory
receptors in the skin. (Sensory receptors are specialized endings of nerve fibers that detect
information in and around the body.)
Autonomic Nervous System: This system connects the brain stem and spinal cord with internal
organs and regulates internal body processes that require no conscious effort. Examples are the
rate of heart contractions, blood pressure, the rate of breathing, the amount of stomach acid
secreted, and the speed at which food passes through the digestive tract. The autonomic nervous
system has two divisions:
Sympathetic division: Its main function is to prepare the body for stressful or emergency
situations—for fight or flight.
Parasympathetic division: Its main function is to prepare the body for ordinary
situations.
4

These divisions work together, usually with one activating and the other inhibiting the actions of
internal organs. For example, the sympathetic division increases pulse, blood pressure, and
breathing rates, and the parasympathetic system decreases each of them.
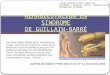
Cranial and Spinal Nerves: Nerves that connect the brain with the
eyes, ears, nose, and throat and with various parts of the head,
neck, and trunk are called cranial nerves. There are 12 pairs of
them. Nerves that connect the spinal cord with other parts of the
body are called spinal nerves. The brain communicates with most
of the body through the spinal nerves. There are 31 pairs of them,
located at intervals along the length of the spinal cord. Several
cranial nerves and most spinal nerves are involved in both the
somatic and autonomic parts of the peripheral nervous system.
Spinal nerves emerge from the spinal cord through spaces
between the vertebrae. Each nerve emerges as two short branches
(called spinal nerve roots): one at the front of the spinal cord and one at the back.
Motor (anterior) nerve root: The motor root emerges from the front of the spinal cord.
Motor nerve fibers carry commands from the brain and spinal cord to other parts of the
body, particularly to skeletal muscles.
Sensory (posterior) nerve root: The sensory root enters the back of the spinal cord.
Sensory nerve fibers carry sensory information (about body position, light, touch,
temperature, and pain) to the brain from other parts of the body. The sensory nerve fibers
from a specific sensory nerve root carry information from a specific area of the body,
called a dermatome.
After leaving the spinal cord, the corresponding motor and sensory nerve roots join to form a
single spinal nerve. Some of the spinal nerves form networks of interwoven nerves, called nerve
plexuses. In a plexus, nerve fibers from different spinal nerves are sorted and recombined so that
all fibers going to or coming from one area of a specific body part are put together into one nerve
(see Peripheral Nerve Disorders:Plexus Disorders ). There are two major nerve plexuses: the
brachial plexus, which sorts and recombines nerve fibers traveling to the arms and hands, and the
lumbosacral plexus, which sorts and recombines nerve fibers going to the legs and feet.
5

II. Definition of Terms
Guillain Barre Syndrome- a serious disorder that occurs when the body’s defense
(immune) system mistakenly attacks part of the nervous system. This leads to nerve
inflammation that causes muscle weakness
Segmental demyelination- the destruction of myelin between the nodes of ranvier
Crawling skin- it is one specific form of a set of sensations known as paresthesia, which
also include the more common prickling, tingling sensation of pins and needles
Ophthalmoplegia- paralysis or weakness of the eye muscles
Areflexia- absence of reflexes
Ataxia- defective muscle coordination
Saltatory conduction- is the propagation of action potentials along myelinated axons from
one node of ranvier to the next node, increasing the conduction velocity of action
potentials without needing to increase the diameter of an axon
Tidal volume- is the lung volume representing the normal volume of air displaced
between normal inspiration and expiration when extra effort is not applied
Axon- a long, slender projection of a nerve cell, or neuron that conducts electrical
impulses away from the neuron’s cell body or soma
Nodes of Ranvier- are the gaps (approximately 1 micrometer in length) formed between
the myelin sheaths generated by different cells
6

V. Baseline Data
Name: MC
Address:
Age: 63
Birth Date:
Birth Place:
Gender: Male
Marital Status: Single
Religion: Roman Catholic
Educational Level: undergraduate
Nationality: Filipino
Occupation: student
Attending physician:
Chief Complaint: inability to move
Admitting Diagnosis: Community Acquired Pneumonia, to consider Guillain- Barre
Syndrome
Final Diagnosis: Guillaine- Barre Syndrome
7

VI. Nursing History
A. Health Maintenance- Perception Pattern
The patient is oriented to time, place, and person. He is knowledgeable as to his
condition and in acquiring such. He tries to regain himself by cooperating in the treatment
regimen and has a strong hope that he would recover as soon as possible.
A. Nutrition Pattern
Before admission, significant others stated that his diet is composed usually of
vegetables, pork, chicken and any other usual foods that we eat and he is funned of eating
junk foods and his meal is always composed of softdrinks. Before he experienced fever,
significant others stated that he ate chicken which does not taste good but still continued to
eat it. During the times that the patient is not feeling well, he doesn’t have time to eat lunch
because of busy schedule in school. His weight before admission is 50kg, but upon staying at
the hospital, it dropped down to 46kg and his mother stated that she thinks, it further
decreased due to his physical condition.
B. Elimination Pattern
Before admission, the client did not experience any problem when it comes to his
urination and defecation. He stated that he urinates to a yellow colored urine usually eight
times a day without any pain or discomfort. He further stated that he defecates daily with no
difficulty. Upon admission, significant others stated that he was attached to a foley catheter
but requested for it to removed due to discomfort and was replaced with diaper. The diaper is
usually fully soaked in about six hours. He experienced difficulty in defecating for about four
days and doctor requested to have suppositories. The client experienced diaphoresis three
weeks prior to admission at OLM and still manifests it upon assessment.
C. Activity and Exercise Pattern
Before admission, significant others stated that he likes to sew dress of Barbie dolls
and is not out going and stays only in the house. He is usually the one who does the
household chores such as washing the dishes, arranging the set in the house and a lot more.
Mother verbalized that his son does not engage in exercises.
D. Sleep and Rest Pattern
The patient usually sleeps 10 hours starting from 9 in the evening and he would wake
up at around 7 in the morning. He often has a good sleep due to tiredness because of the
activities in school. Patient doesn’t have siestas or afternoon naps during weekdays but does
during weekends. Two weeks before the admission, the patient only sleeps for about 5 hours
8

a day due to the activities in school. He would arrive home 1:00 in the morning and would
wake up 7:00am to go back to school again. Furthermore, during those days he has already
experiencing flu but tolerated it. During admission, he complained that he can’t sleep well
due to the environment and noise.
E. Cognitive- Perception Pattern
The client responds to non-verbal stimuli. When asked, he would show that he would
agree or disagree by nodding his head since he cannot speak due to endotracheal tube. He is
still in 4th year college taking up Hospitality Management.
F. Self Perception- Self Concept Pattern
His mother stated that he is comfortable of himself and has a strong self-esteem. He is
confident of whom he is and has trust but during admission, he thought of himself as
worthless because of his condition but he is trying his best to recover from his illness so that
he can continue to his normal way of living by submitting himself to necessary and important
treatment.
G. Role-Relationship Pattern
His family is composed of 8 members including his mother and father and he is the
2nd child among the 6. He has a good relationship with his family and they are supportive of
one another. Even in his times of illness, his family didn’t think that he is useless and they
are always there to show their love, care, and concern to him. Also, his extended family
members visit him in the hospital and didn’t neglect to support him financially.
H. Sexuality and Reproductive Pattern
He is single and didn’t experience any relationship with opposite sex. He doesn’t
engage in any sexual contact and not productive.
I. Coping- Stress Pattern
His mother stated that his hobby of sewing dresses of Barbie doll makes him relaxed
and entertained. He would go to sleep right after a long hour of school activities. If he has
problems, he would talk to his friends as well as with his family members.
J. Values and Beliefs Pattern
They are Roman Catholic and they only believe that there is only one God and they
have a strong faith on Him. He doesn’t have any other beliefs or rituals.
9

VII. Health History
1. History of Present Illness
Significant others stated that his son first experienced fever and he took it for
granted and still continued to go to school until such time that he can no longer tolerate
his condition.
Two weeks prior, patient was admitted and it was treated as typhoid, was
admitted for eight days in Silay Hospital.
One day prior, patient complaint of inability to move both upper and lower
extremities associated with vomiting, nausea, negative fever, difficulty of breathing and
seizure. There is persistence of signs and symptoms noted.
2. Past Health History
a. Childhood Illness
His mother stated that he has no any other serious illness since childhood.
He is well and healthy even though he didn’t completed his immunization
specifically Hepatitis B vaccine.
b. Past Hospitalization
The patient was hospitalized once during his younger days due to diarrhea
which lasted in three days.
c. Family/Social History
The patient’s family has no any other history of genetic diseases except in
his mother side which is hypertension.
10

VIII. Assessment
November 8, 2010
A. General Appearance 20 years old male adult Neat and clean physically With tidy hair With systemic jaundice noted
B. LOC awake, lying on bed in semi fowler’s position responsive and conscious to both verbal and non verbal stimuli and in painful
stimuli with GCS of 11 as evaluated
C. HEENT Pupils Equally Round and Reactive to Light and Accommodation with pale conjunctiva icteric sclerae with patent NGT for feeding inserted at right narynx with nasal flaring noted face symmetrical
D. Cardiovascular With ongoing IVF bottle#21 D5NM 1Lx60cc/hr infusing well at Right cephalic
vein with remaining solution of 280cc with strong palpable pulse at the rate of 90 bpm with BP = 100/80mmHg taken at Left arm in fowler’s position with good capillary refill of less than 2 seconds attached to pulse oximeter of 92 bpm
E. Respiratory With ET attached to mechanical vent with specific parameters of FIO2-40%,
back-up rate- 18, tidal vokume-300 on AC node With respiratory rate of 30 cpm with wheezing and crackles noted upon auscultation on both lung fields with symmetrical rise and fall of chest wall
F. Gastro-Intestinal Tract on OTF 225cc given q3H per NGT bowel sound auscultated at right lower with normoactive bowel sound auscultated at right lower quadrant with the rate of
8 cpm unable to defecate upon initial assessment
G. Genito-Urinary Tract With diaper not fully soaked upon initial assessment With an average of 2 diaper change per shift approximately 150 cc
H. Musculoskeletal Unable to move; assistance needed Able to move both upper and lower extremities minimally
I. Integumentary warm to touch with temperature of 36.9°C
11

with good skin turgor with pale mucous membrane as noted Hair well groomed, nail beds symmetrical and complete number of teeth as noted
November 9, 2010
A. General Appearance 20 years old male adult Neat and clean physically With tidy hair
B. LOC awake, lying on bed responsive and conscious to both verbal and non verbal stimuli with GCS of 11 as evaluated
C. HEENT Pupils Equally Round and Reactive to Light and Accommodation with pale conjunctiva icteric sclerae with patent NGT for feeding inserted at right narynx face symmetrical
D. Cardiovascular With ongoing IVF bottle#22 D5NM 1Lx60cc/hr infusing well at Right cephalic
vein with remaining solution of 350cc with strong palpable pulse at the rate of 90 bpm with BP = 100/80mmHg taken at Left arm in fowler’s position with good capillary refill of less than 2 seconds attached to pulse oximeter of 92 bpm
E. Respiratory With ET attached to mechanical vent with specific parameters of FIO2-40%,
back-up rate- 18, tidal vokume-300 on AC node With respiratory rate of 30 cpm with wheezing noted upon auscultation on both lung fields with symmetrical rise and fall of chest wall
F. Gastro-Intestinal Tract on OTF 225cc given q3H per NGT unable to defecate upon initial assessment
G. Genito-Urinary Tract With diaper not fully soaked upon initial assessment
H. Musculoskeletal Unable to move; assistance needed
I. Integumentary warm to touch with temperature of 36.8°C with good skin turgor with pale mucous membrane as noted
November 10, 2010
B. General Appearance
12

20 years old male adult Neat and clean physically With tidy hair
C. LOC awake, lying on bed in fowler’s position conscious and responsive to both verbal and non verbal stimuli with GCS of 11 as evaluated
D. HEENT Pupils Equally Round and Reactive to Light and Accommodation with pale conjunctiva icteric sclerae with patent NGT for feeding inserted at right narynx face symmetrical
E. Cardiovascular With ongoing IVF bottle#23 D5NM 1Lx60cc/hr infusing well at Right cephalic
vein with remaining solution of 250cc with strong palpable pulse at the rate of 88 bpm with BP = 90/70mmHg taken at Left arm in fowler’s position with good capillary refill of less than 2 seconds attached to pulse oximeter of 82 bpm
F. Respiratory With ET attached to mechanical vent with specific parameters of FIO2-40%,
back-up rate- 18, tidal vokume-300 on AC node With respiratory rate of 30 cpm with crackles noted upon auscultation on both lung fields with symmetrical rise and fall of chest wall
G. Gastro-Intestinal Tract on OTF 225cc given q3H per NGT with normoactive bowel sound of 6cpm auscultated at right abdomen unable to defecate upon initial assessment
H. Genito-Urinary Tract With diaper not fully soaked upon initial assessment
I. Musculoskeletal Able to move both upper and lower extremities
J. Integumentary cool to touch with temperature of 36.6°C with good skin turgor with pale mucous membrane as noted
IX. Laboratory and Radiology
Serum
October 21, 201013

Examination Result Normal Value Interpretation Implication
Creatinine 61.88 mmol/l 53.0 – 114.92mmol/
Normal Creatinine level is in normal
value
Potassium 4.30mmol/l 3.6 – 5.1mmol/l Normal Potassium level is in normal
value
Sodium 137.60mmol/l 137 – 146mmol/l Normal Sodium level is in normal value
Examination Result Normal Value Interpretation Implication
Creatinine 0.7 mg/dl 0.6 – 1.3 mg/dl Normal Creatinine level is in normal
value
Potassium 4.3 mg/dl 3.6 – 5.1 mg/dl Normal Potassium level is in normal
value
Sodium 137 mg/dl 137 – 145 mg/dl Normal Sodium level is in normal value
Significance: This test measures the kidney function
Complete Blood Count
October 21, 2010
Examination Result Normal Value Interpretation Implication
Hemoglobin 143 g/l 120 – 170 g/l Normal Hemoglobin count is in normal
value
Hematocrit 0.41 L/L 0.40 – 0.54 Normal Hematocrit count is in normal value
RBC 4.48 4.60 – 6.00x10-
12/LDecreased RBC is decreased,
may suggest anemia
WBC 8.6 5.00 – 10.00x10-
9/LNormal WBC count is in
normal value
Segmenters 0.63 0.50 – 0.70 Normal Segmenters is in normal value
14

Lymphocytes 0.37 0.20 – 0.40 Normal Lymphocytes is in normal value
Platelet count (CBC profile)
563 150.00 – 400.00x10-9/L
Increased Platelet count is increased, may
suggest myeloproliferative
disorder and thromboembolism
October 26, 2010
Examination Result Normal Value Interpretation Implication
Hemoglobin 141 g/L 120 – 170 g/L Normal Hemoglobin count is in
normal value
Hematocrit 0.40 L/L 0.40 – 0.54 Decreased Hematocrit is decreased, may suggest anemia
RBC 4.26 4.60 – 6.00x10-
12/LDecreased RBC is
decreased may suggest anemia
WBC 9.1 5.00 – 10.00x10-
9/LNormal WBC count is in
normal value
Segmenters 0.76 0.50 – 0.70 Increased Segmenters increased, may suggest viral
infection
Lymphocytes 0.24 0.20 – 0.40 Normal Lymphocyte is in normal value
Platelet count (CBC profile)
150 – 400.00x10-
9/L
October 27, 2010
Examination Result Normal Value Interpretation Implication
Hemoglobin 134 g/L 120 – 170 g/L Normal Hemoglobin count is in
15

normal value
Hematocrit 0.39 L/L 0.40 – 0.54 Decreased Hematocrit is decreased, may suggest anemia
RBC 4.09 4.60 – 6.00x10-
12/LDecreased RBC is
decreased may suggest anemia
WBC 8.9 5.00 – 10.00x10-
9/LNormal WBC count is in
normal value
Segmenters 0.74 0.50 – 0.70 Increased Segmenters increased, may suggest viral
infection
Lymphocytes 0.26 0.20 – 0.40 Normal Lymphocyte is in normal value
Platelet count (CBC profile)
150 – 400.00x10-
9/L
Significance: The complete blood count is the calculation of the cellular (formed elements) of blood. It may be a part of a routine check – up or screening, or as a follow up test to monitor certain treatments. It can also be done as a part of an evaluation based on a patient’s symptoms.
October 22, 2010
Examination Result Normal Value Interpretation Implication
ASO titer Positive <200 IU/mL Increased May suggest streptococcal infection
Chest PA
October 21, 2010
Chest PA sitting shows hazy infiltrates in the lower lung
Heart is not enlarged
No other remarkable findings to note
Remarks: Left lower lung pneumonia
Significance: A chest X-ray is a picture of the chest that shows your heart, lungs, airway, blood vessels, and lymph nodes. A chest X-ray also shows the bones of your spine and chest, including
16

your breastbone, ribs, collaboration, and the upper part of your spine. A chest X-ray is the most common imaging test or X-ray used to find problem inside the chest.
October 22, 2010
Examination Result Normal Value Interpretation Implication
ESR result 86 mm/hr 0.00 - 10.00mm/hr
Increased ESR increased, may suggest marker of infection or inflammation in the body.
Significance: The erythrocyte sedimentation rate (ESR) is an easy, inexpensive, nonspecific test that has been used for many years to help detect conditions associated with acute and chronic inflammation, including infections, cancers, and autoimmune.
ABG
October 22, 2010
Set-up: MV/Mode: AC FIO2 at 100% RR 20bpn Vt 350mL
Examination Result Normal Value Interpretation Implication
pH 7.41 7.35 – 7.45 Normal pH level is in normal value
pCO2 40 mmHg 35 – 45 mmHg Normal pCO2 level is in normal value
pO2 325 mmHg 80 – 100 mmHg Increased pO2is increased, may suggest Increased oxygen levels in the inhaled air and polycythemia
HCO3 25.1mEq/L 22 – 26 mEq/L Normal HCO3 level is in normal value
B.E. 0.6 mEq/L +/- 2 mEq/L Increased B.E is increased, may suggest Loss of buffer base, hemorrhage, diarrhea, ingestion of alkali
O2 Sat. 100% 97% Increased O2 sat. Is
17

increased, may suggest deep or rapid breathing occurs and inspired oxygen levels are increased, such as breathing from a 100% axygen source
Significance: An arterial blood gas (ABG) test measures the acidity (pH) and the levels of oxygen and carbon dioxide in the blood from an artery. This test is used to check how well your lungs are able to move oxygen into the blood and remove carbon dioxide from the blood.
Laboratory/Diagnostic test
Result Normal values Interpretation Implication
Urinalysis (10/22/10)
Physical
properties
Color: Straw Color: Straw Normal The urine is normal in color.
Transparency Transparency: Clear
Abnormal Hazy urine could mean that mucus, phosphates, bacteria, pus, or fats are spilling into your urine.
pH: 5.0 pH: 7.0 Decreased The urine had slight acidity.
Specific Gravity: 1.015
Specific Gravitiy:
1.003-1.030
Normal The urine’s concentration is normal.
Laboratory/Diagnostic test
Result Normal values Interpretation Implication
18

Urinalysis (10/22/10)
Physical
properties
Color: Dark yellow
Color: Straw Abnormal
Transparency: Slightly hazy
Transparency: Clear
Abnormal Hazy urine could mean that mucus, phosphates, bacteria, pus, or fats are spilling into your urine.
pH: 5.0 pH: 7.0 Decreased The urine had slight acidity.
Specific Gravity: 1.015
Specific Gravitiy:
1.003-1.030
Normal The urine’s concentration is normal.
Laboratory/Diagnostic test
Result Normal values Interpretation Implication
Urinalysis (10/22/10)
Chemical
Examination
Albumin:
-
- Normal Presence of Albumin is not
noted
Sugar:
-
- Normal Presence of sugar is not
noted
19

Laboratory/Diagnostic test
Result Normal values Interpretation Implication
Urinalysis (10/22/10)
Chemical
Examination
Albumin:
-
- Normal Presence of Albumin is not
noted
Sugar:
-
- Normal Presence of sugar is not
noted
Microscopic Examination
October 22, 2010
RBC: 3-5/hpf
Pus cells: 6-10/hpf
Epithelial cells: occasional
Mucus thread: many
Bacteria: few
Cast
Hyaline: 0-1/lpf
Crystal
Urates: occasional
October 22, 2010
RBC: 1-4/hpf
Pus cells: 0.2/hpf
Epithelial cells: occasional
Mucus thread: many
Bacteria: few
Cast
Hyaline: /lpf
Crystal
Urates: few
20

Significance: The urinalysis is used as a screening and/or diagnostic tool because it can help
detect substances or cellular material in the urine associated with different metabolic and kidney
disorders.
October 24, 2010
Examination Result Normal Value Interpretation Implication
Sodium 141.20mmol/L 137-146mmol/L Normal Sodium level is
in normal value
Examination Result Normal Value Interpretation Implication
Sodium 141.2mmol/L 137-145mmol/L Normal Sodium level is
in normal value
October 26, 2010
Examination Result Normal Value Interpretation Implication
Creatinine 79.56mmol/L 53.0-
114.92mmol/L
Normal Creatinine level
is in normal
value
Potassium 3.35mmol/L 3.6-5.1mmol/L Decreased Potassium level
is decreased, may
suggest
hypokalemia
Sodium 139.8mmol/L 137-146mmol/L Normal Sodium level is
in normal value
21

October 27, 2010
Examination Result Normal Value Interpretation Implication
Creatinine 53.04mmol/L 53.0-
114.92mmol/L
Normal Creatinine level
is in normal
value
Potassium 2.75mmol/L 3.6-5.1mmol/L Decreased Potassium level
is decreased, may
suggest
hypokalemia
Sodium 141mmol/L 137-146mmol/L Normal Sodium level is
in normal value
Significance: This test measures the kidney functions.
Chemistry 1
October 25, 2010
Test CU (result) SI (result) CU (normal
value)
SI (normal
value)
Interpretation Implication
SGPT 215U/L 215 U/L 0.41U/L 0.41U/L Increased SGPT is
increased,
may
suggest
liver
damage
such as
hepatitis
22

October 30, 2010
Test CU (result) SI (result) CU (normal
value)
SI (normal
value)
Interpretation Implication
SGPT 364 U/L 364 U/L 0.41U/L 0.41U/L Increased SGPT is
increased,
may
suggest
liver
damage
such as
hepatitis
Significance: For confirming the suspected liver disease. For estimation of the liver damage and
as a guide for treating and knowing the prognosis of the liver disease.
Radiologic Report
Exam taken: Chest PA
Interpretation:
Chest PA SUPINE PORTABLE dated October 25, 2010 compared with the previous
examination dated October 21, 2010 shows interval development of fuzzy densities throughout
both lungs.
There is now haziness in the right lower lung, while the haziness in the left lower lung is
no longer seen.
Endotracheal tube is now seen with its tip above the carina.
Remarks:
Bilateral pulmonary congestion. Concomitant pneumonia in the right lung is not ruled
out.
Significance: A chest X-ray is a picture of the chest that shows your heart, lungs, airway, blood
vessels, and lymph nodes. A chest X-ray also shows the bones of your spine and chest, including
23

your breastbone, ribs, collarbone, and the upper part of the spine. A chest X-ray is the most
common imaging test or X-ray used to find problems inside the chest.
Clinical Chemistry
November 1, 2010
Examination Result Normal Value Interpretation Implication
A/G ratio:
Total Protein 77g/L 63-82g/L Normal Total protein is
in normal value
Albumin 34.90g/L 35-50g/L Decreased Albumin is
decreased, may
suggest liver
diseases
Globulin 42.10g/L 23-30g/L Increased Globulin is
increased, may
suggest infection
and hepatitis
A/G ratio 0.80 1.10-2.50 Decreased A/G ratio is
decreased, may
suggest liver or
kidney disorder
Examination Result Normal Value Interpretation Implication
A/G ratio:
Total Protein 7.70g/dL 6.30-8.20g/dL Normal Total protein is
in normal value
Albumin 3.49g/dL 3.50-5g/dL Decreased Albumin is
decreased, may
suggest liver
diseases
24

Globulin 4.21g/dL 2.30-3g/dL Increased Globulin is
increased, may
suggest infection
and hepatitis
A/G ratio 0.80 1.10-2.50 Decreased A/G ratio is
decreased, may
suggest liver or
kidney disorder
Significance: To detect any liver or kidney disease
BIlirubin Adult
Examination Result Normal Value Interpretation Implication
Total bilirubin 13.00 Umol/L 0.00-
19.00Umol/L
Normal Total bilirubin is
in normal value
Direct bilirubin 10.00 Umol/L 0.00-5.00Umol/L Increased Direct bilirubin
is increased, may
suggest hepatitis
Indirect
bilirubin
3.00Umol/L 0.00-
14.10Umol/L
Normal Indirect bilirubin
is in normal
value
Examination Result Normal Value Interpretation Implication
Total bilirubin 0.76mg/dL 0.00-1.11mg/dL Normal Total bilirubin is
in normal value
Direct bilirubin 0.58mg/dL 0.00-0.29mg/dl Increased Direct bilirubin
is increased, may
suggest hepatitis
Indirect
bilirubin
0.18mg/dL 0.00-0.82mg/dL Normal Indirect bilirubin
is in normal
value
25

Significance: A bilirubin test is a diagnostic blood test performed to measure levels of bile
pigment in an individual’s blood serum and to help evaluate liver function
Prothrombin Time
Examination Result Normal Value Interpretation Implication
Patient 13.7 9.15-11.28 secs Increased Patient is
increased
INR 1.15
% activity 63.2 More than 70% Decreased % activity is
decreased
NPM 10.22 sec Normal NPM is in
normal value
Significance: Prothrombin time (PT) is a blood test that measures how long it takes blood to
clot. A prothrombin time test can be used to check for bleeding problems. PT is also used to
check whether medicine to prevent blood clots is working.
November 1, 2010
Examination Result Normal Value Interpretation Implication
TSH 1.335UIU/ml 0.49-4.67UIU/ml Normal TSH is in normal
value
Significance: The TSH test is often the test of choice for evaluating thyroid function and/or
symptoms of hyper- or hypothyroidism
26

X. Pathophysiology
Precipitating Factors: Predisposing Factors:
Trauma Unknown Surgery Immunization 1 to 3 weeks before the onset Gastrointestinal Illness Acute Illness Viral infection and respiratory tract infection
27
Limited malfunction of the immune system
Immune system starts to destroy the myelin sheath that surrounds the axons (segmental demyelination)
Affects salutatory conduction (leaping of impulses from node to node)
Dispersion of Impulses Slow conduction velocities Conduction Block
Affects cranial, motor nerves, myelinated pain, touch, temperature, nerve fibers, and sensory functions
Brain, may receive inappropriate sensory signals
Milter Fisher VariantDescending GBS Ascending GBS
-Weakness of face or bulbar muscle of the jaw, sternocleidomastoid muscle, muscle of tongue, pharynx and larynx.
-Progress downward to involve limbs, breathlessness during speech, shallow respirations, decrease tidal volume.
-Opthalmoplegia, diplopia, functional blindness, numbness in hands, decrease or absent deep tendon reflexes
-Opthalmoplegia, areflexia, severe ataxia, inability to smile, frown whistle, drink from a straw, dysphagia, paralysis of larynx, inability to cough, gag or swallow, hypertensive or hypotensive episodes, orthostatic hypotension, bradycardia, heart block, asystole.
Entrance of pathogens (bacterial and viral) in the body
Pathogens invade the immune system
Note: All bold text are manifested by the patient

XI. Nursing Care Plan 1
ASSESSMENT NURSING DIAGNOSIS RATIONALE DESIRED OUTCOME NURSING INTERVENTIONS
JUSTIFICATION EVALUATION
Actual Abnormal Findings:
RR= 30 PR= 90 Attached to
mechanical ventilator
Excessive sputum upon suctioning
Cold and clammy skin
Laboratory results
Chest PaOctober 21,2010Remarks: Left lower lung pneumonia
October 25, 2010Remarks: Bilateral pulmonary congestion
Risk Factors: Infection Retained
Ineffective Airway Clearance related to excessive, thickened mucus secretions and presence of disease as evidenced by having of rhonchi, alterations in laboratory results (Chest PA) and is attached to mechanical ventilator
Definition: Inability to clear secretions or obstructions from the respiratory tract to maintain a clear airway
Source: Doenges E., Moorhouse M., Geisller-Murr A., Nurse’s Pocket Guide 11th edition. p. 77
Precipitating Factor: Presence of disease
Guillain CAPBarre Syndrome Invasion Ofimmune bacteriasystem starts in theto destroy lungsthe myelin sheath that surrounds Chest Pathe axons showedof many haziness peripheral in bothnerves lung areas
nerves there iscannot accumulationtransmit of secretionssignals in the efficiently lungs
muscles begin to lose their ability to respond to
After 40 hours of nursing intervention, my client will be able to:
1. Maintain airway patency
2. Expectorate or clear secretions readily
3. Demonstrate behaviours to improve or maintain clear airway
Independent: Position head
in semi fowler’s position appropriate for age or condition
Suction tracheal/oral prn
Elevate head of bed/change position every 2 hours and prn
Assist with
To open or maintain open airway in at rest or compromised individual
To clear airway when excessive or viscous secretions are blocking airway
To take advantage of gravity decreasing pressure on the diaphragm and enhancing drainage of/ventilation to different lung segments
To maintain adequate airways, improve
After 40 hours of nursing intervention, the client was able to:
1. Goal met. Client able to breath properly, his tube was suctioned and cleaned from time to time and he undergone process of weaning.
2. Goal met. Client able to cough out secretions and participates when he is told during suctioning.
3. Goal met. Client made use of
28

secretions Presence of
artificial airway
Strength factor: Good family
support Good
participation in treatment regimen
Strong Faith in God
the brain's commands ronchi and cracklesWeakness heard or paralysis uponof spread auscultationto the in bothmuscles that lung fieldscontrol breathing
Ineffective Airway Clearance
Source:Brunner & Suddarth’s. Textbook of Medical-Surgical Nursing. 12th edition
use of respiratory devices and treatments
Position appropriately
Collaborative: Give
expectorants or bronchodilators as ordered
respiratory function and gas exchange
To help facilitate in the entry of air
To promote wellness
Source: Doenges E., Moorhouse M., Geisller-Murr A., Nurse’s Pocket Guide 11th edition. p. 77-81
gestures as means to communicate when he experiences difficulty in breathing.
29

Assessment Nursing Diagnosis Rationale Desired Outcomes Nursing Interventions
Justification Evaluation
Actual Abnormal Findings:
Subjective:
-“gulpi lang siya indi maka giho sang iya kamot kag tiil” as verbalized by client’s mother
Risk-Related Factors:
-Knowledge deficit
-Ecomomic difficulties
-Family patterns of healthcare
Strength/Wellness:
-Family support
-Religious beliefs and practices
Impaired physical mobility related to neuromuscular impairment as evidenced by limited range of motion; limited ability to perform gross/fine motor skills; difficulty turning.
Definition:
Limitation in independent, purposeful physical movement of the body or of one or two extremities.
Source: Doenges, Moorhouse, Murr. (2008). “Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales.” F.A.
Precipitating factor: Guillain-Barré syndrome
diffuse inflammation or
dymyelination (or both) of the ascending or descending
peripheral nerves
Damage to these nerves makes it hard for them to transmit
signals.
muscles have trouble responding
to your brain
After 40 hours of nursing interventions, the client will be able to:
1. Demonstrate techniques/behaviours that enable resumption of activities.
2. Demonstrate techniques/behaviours that enable safe repositioning.
3. Maintain position of function and skin integrity as evidenced by absence of contractures, footdrop, decubitus, and so forth.
Independent:
1. Assist client reposition self on a regular schedule
2. Assess nutritional status and client’s report of energy level.
3. Observe movement when client is unaware of observationto note any incongruencies with reports of abilities.
4. Provide regular skin care to include pressure area management.
Collaborative:
5. Consult with physician or occupational therapist,
1. To promote optimal level of function and prevent complication.
2. To identify causative/ contributing factor.
3. To assess functional ability.
4. To promote optimal level of function and prevent complication.
5. To develop individual exercise/mobility program and
After 40 hours of nursing interventions, the client will be able to:
1. Goal met. Client was able to demonstrate techniques/behavior that enable resumption of activities. He was able to do passive ROM
2. Goal met. Client was able to demonstrate techniques/ behavior that enable safe repositioning with the help of his mother and relatives
3. Goal met. Client was able to maintain position of function and skin integrity.
30

Davis Company: Philadelphia.11th ed. P. 457. Weakness or lack of
sensation in the legs, which spreads to the upper part of
the body
Impaired physical mobility
Source:
Black and Hawks. Medical-Surgical Nursing
as indicated. identify appropriate mobility devices.
Source: Doenges, Moorhouse, Murr. (2008). “Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales.” F.A. Davis Company: Philadelphia.11th ed. P. 459-460.
He did not have manifest any of contractures, footdrop, decubitus, pressure ulcers/bed sores. He was turned every 2 hours to prevent these conditions
31

Assessmet Nursing Diagnosis Rationale Desired Outcomes Nursing Interventions Justification Evaluation
Actual Abnormal Findings:
-difficulty of breathing
Risk-Related Factors:
-situation hindering elevation of the upper body
-reduced level of consciousness
-depressed cough/gag reflex
-impaired swallowing
Strength/Wellness:
-Family support
Risk for aspiration related to presence of endotracheal tube.
Definition:
At risk for entry of gastrointestinal secretions, oropharyngeal secretions, or solids or fluids into tracheobronchial passages.
Source: Doenges, Moorhouse, Murr. (2008). “Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales.” F.A. Davis Company: Philadelphia.11th ed.
Precipitating factor: presence of endotracheal tube
Nasogastric Tube feedings
Positioning (improper), depressed
gag/cough reflex
impaired swallowing
risk for aspiration
After 40 hours of nursing interventions, the client will be able to:
1. Experience no aspiration as evidenced by noiseless respirations; clear breath sounds, clear, odourless secretions.
2. Demonstrate techniques to prevent aspiration.
3. Identify causative or risk factor.
Independent:
1. Observe for neck and facial edema.
2. Suction as needed and avoid triggering gag mechanism when performing suction or mouth care.
3. Auscultate lungs sounds frequently.
4. Assist with postural drainage through changing of position (side lying)
Collaborative:
5. Refer to physician for medical intervention and exercise.
1. To assess causative or contributing factor. Client with tracheal or bronchial injury is at particular risk for airway obstruction and inability to handle secretion.
2. To clear secretion while reducing potential for aspiration of secretion.
3. To determine presence of secretions/ silent aspiration.
4. To mobilize
After 40 hours of nursing interventions, the client will be able to:
1. Goal partially met. Client did not experience aspiration but during suctioning, he voluntarily coughs out yellow to yellow green colored secretion and was not able to manifest noiseless respirations and clear breath sounds
2. Goal met. Client was able
32

P. 98.
Source: Suddarth’s Medical surgical manual
thickened secretions that may interfere with swallowing.
Collaborative:
5. To strengthen muscles and learn techniques to enhance swallowing/reduce potential aspiration.
Source: Doenges, Moorhouse, Murr. (2008). “Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales.” F.A. Davis Company: Philadelphia.11th ed. P. 98-101.
to demonstrate techniques to prevent aspiration such as coughing out of secretions and cooperates during suction
3. Goal met. Client was able to identify causative or risk factor such as accumulation of secretions in airway passages
33

XII. Drug Study
NAME OF DRUG
DOSAGE, FREQUENCY,
ROUTE
MECHANISM OF ACTION
INDICATION CONTRAINDICATION ADVERSE EFFECT NURSING RESPONSIBILITIES
Generic Name:Metropolol
Brand Name:AstraZeneca
Classification: Antihypertensive; Beta1-selective adrenergic blocker
Dosage: 50mg/tabRoute: NGT Frequency: BID
Competitively blocks beta-adrenergic receptors in the heart and juxtaglomerular apparatus, decreasing the influence of the sympathetic nervous system on these tissues and the excitability of the heart, decreasing cardiac output and the release of rennin, and lowering BP; acts in CNS to reduce
Hypertension, alone or with other drugs, especially diuretic.
Immediate-release tablets and injection: Prevention of reinfarction in MI patients who are hemodynamically stable or within 3-10 days of acute MI.
Long-term treatment of angina pectoris.
Tropol-XL only; treatment of stable, symptomatic heart failure of ischemic,
Contraindicated with sinus bradycardia (HR less than 45 bpm); second or third degree heart block (PR interval more than 0.24 sec), cardiogenic shock, heart failure
Use cautiously with asthma or COPD
Allergic: pharyngitis, erythematous rash, fever, sore throat, laryngospasm
CNS: dizziness, vertigo, tinnitus, fatigue, emotional depression, paresthesias, sleep disturbances, hallucinations, disorientation, memory loss, slurred speech
CV: heart failure, cardiac arrhythmias, peripheral vascular insufficiency, claudication, CVA, pulmonary edema,
1. Do not discontinue drug abruptly after long-term therapy.
2. Give drug with food to facilitate absorption.
3. Provide continual cardiac monitoring for patients receiving the drug.
34

sympathetic outflow and vasoconstrictor tone.
hypertensive, or cardiomyopathic origin.
hypotension Dermatologic:
rash, pruritis, sweating, dry skin
EENT: eye irritation, dry eyes, conjunctivitis, blurred vision
GI: gastric pain, flatulence, constipation, diarrhea, nausea, vomiting, anorexia, ischemic colitis, renal and mesenteric arterial thrombosis, retroperitoneal thrombosis, retroperitoneal fibrosis, hepatomegaly, acute pancreatitis
GU: impotence, decreased libido, dysuria, Peyronie’s disease, nocturia, frequent urinitaion
MS: joint pain, arthralgia, muscle
35

cramp Respiratory:
bronchospasm, dyspnea, cough, bronchial obstruction, nasal stuffiness, rhinitis, pharyngitis
Other: decreased exercise tolerance, development of ANA, hyperglycemia or hypoglycaemia, elevated serum transaminase, alkaline phosphate
36

NAME OF DRUG
DOSAGE, FREQUENCY,
ROUTE
MECHANISM OF ACTION
INDICATION CONTRAINDICATION ADVERSE EFFECT NURSING RESPONSIBILITIES
Generic Name:Levofloxacin
Brand Name:Levocin
Classification: Antibiotic; Fluoroquinolone
Dosage: 500mg/tabRoute: NGT Frequency: OD
Bactericidal: interferes with DNA by inhibiting DNA gyrase replication in susceptible gram-negative and gram-positive bacteria, preventing cell reproduction.
Treatment of adults with Community Acquired pneumonia, bacterial sinusitis caused by susceptible bacteria including multidrug resistant strains
Treatment of acute exacerbation of chronic bronchitis caused by susceptible bacteria
Treatment of nosocomial pneumonia due to methicillin-sensitive Staphylococcus aureus,
Contraindicated with allergy to fluoroquinolones
Use cautiously with renal impairment, seizures
CNS: headache, dizziness, insomnia, fatigue, somnolence, blurred vision
GI: nausea, vomiting, dry mouth, constipation, flatulence, abnormal liver function
GU: abnormal renal function, acute renal failure, UTI, urine retention
Hematologic: elevated BUN, serum creatinine and alkaline phosphatise, neutropenia, anemia
Other: fever, rash, photosensitivity, muscle and joint
1. Arrange for culture and sensitivity tests before beginning therapy
2. Continue therapy as indicated for condition being treated
3. Ensure that patient is well hydrated during course of therapy.
4. Discontinue drug at any sign of hypersensitivity or at complaint of tendon pain, inflammation, or rupture
5. Monitor clinical response; if no improvement is seen or a relapse
37

Pseudomonas strains, Serratia E.coli, Klebsiella, Haemophilus influenza, Streptococcus pneumoniae
tenderness, increase serum glucose
occurs, repeat culture and sensitivity test
38

NAME OF DRUG
DOSAGE, FREQUENCY,
ROUTE
MECHANISM OF ACTION
INDICATION CONTRAINDICATION ADVERSE EFFECT NURSING RESPONSIBILITIES
Generic Name:Fluimucil
Brand Name:Acetylcysteine
Classification: Therapeutic category:Mucolytic agent
Dosage: 600mg/tab +50cc water
Route: NGT Frequency: OD
Exerts mucolytic
action through its
free sulfhydryl
group which opensup the disulfide bonds in the mucoproteins thus lowering mucous viscosity. The exact mechanism of action in acetaminophen toxicity is unknown. It is thought to act by providing substrate for conjugation with the toxic metabolite.
Treatment of respiratory affections characterized by thick and viscous hypersecretions: acute bronchitis, chronic bronchitis and its exacerbations; pulmonary emphysema, mucoviscidosis and bronchiectasis.
Severe hypertension;
severe. Coronary artery
disease, hypersensitivity to
pseudoedephrine,
acrivastine or any
component; renal
impairment
Rarely, urticaria,
bronchospasm, nausea,
vomiting. Aerosol
treatment: Rhinitis,
stomatitis.
1. Monitor effectiveness of therapy and advent of adverse/allergic effects.
2. Instruct
patient in appropriate
use and adverse effects
to report
39

NAME OF DRUG
DOSAGE, FREQUENCY,
ROUTE
MECHANISM OF ACTION
INDICATION CONTRAINDICATION ADVERSE EFFECT NURSING RESPONSIBILITIES
Generic name: Multiple vitamins
Brand Name:KREBB C
Classification: Multivitamin
Dosage: 1 cap
Route: NGT Frequency: OD
Dietary supplement for the treatment and prevention of vitamin deficiencies. These vitamins are necessary for normal growth and development. Many act as coenzymes or catalysts in numerous metabolic processes.
Multivitamins are used to provide vitamins that are not taken in through the diet. Multivitamins are also used to treat vitamin deficiencies (lack of vitamins) caused by illness, pregnancy, poor nutrition, digestive disorders, and many other conditions.
Contraindicated to patients with alcohol intolerance, hypersensitivity to preservatives, colorants or additives including tartrazine, saccharine, and aspartame.
GU: urine discoloration
Others: allergic reactions to preservatives, additives or colorants
1. Instruct patient to report adverse effects of the drug.
40

XIII. Health Teaching Plan
Medication Exercises Treatment Hygiene Outpatient Diet
Levofloxacin (Levocin) Fluoroquinolone/anti -
infective Inhibits the enzyme DNA
gyrase in susceptible gram-negative and gram-positive aerobic and anaerobic bacteria, interfering with bacterial DNA synthesis
Dosage: 1cap 500mg, Route: PO, Frequency: OD
Tell patient to stop taking drug and contact prescriber if he experiences signs or symptoms of hypersensitivity reaction (rash, hives, or other skin reactions) or severe diarrhea (which may indicate pseudomembranous colitis).
Check vital signs, especially blood pressure. Too-rapid infusion can cause hypotension.
Closely monitor patients with renal insufficiency.
Monitor blood glucose level
1. Teach client breathing exercises
to deepen breathing and for better lung expansion
How?
Place hands on the border of rib cage
Inhale through nose and exhale trough mouth
Do this at least 10 times every time patient is awake
2. Ambulate from time to time
To improve circulation
Tracheostomy
to bypass an airway
that has become
obstructed
to remove fluid that
has built up in the
upper airway,
particularly in the
throat and trachea
(windpipe)
to assist with
breathing by
delivering oxygen to
the lungs
Fluid/IVF
therapy – for
hydration and to
replace loss
fluids and
electrolytes
1. Oral Hygiene- Tooth
brushing- Mouth
washing
2. Personal Hygienea. Skin care- apply
lotion to moisturize the skin
b. Bathing- removes dirt and dead epithelial cells from the surface of skin, reducing the chance of infection
c. Hair care- brushing and combing the hair stimulates circulation of blood in the scalp
d. Eye care- soften dried secretions
1. Have adequate rest and should maintain healthy diet to promote recovery.
2. Continue medications prescribed by the doctor.
3. Instruct family to return to attending physician for a scheduled check-up.
4. Continue mild exercise regimen for faster recovery. Avoid strenuous exercises.
5. Advise to report to the physician if
Osteorized Feeding on strict aspiration precaution- give feeding via nasogastric tube
41

closely in diabetic patients.
Metropolol (AstraZeneca) Antihypertensive; Beta1-
selective adrenergic blocker Competitively blocks beta-
adrenergic receptors in the heart and juxtaglomerular apparatus, decreasing the influence of the sympathetic nervous system on these tissues and the excitability of the heart, decreasing cardiac output and the release of rennin, and lowering BP; acts in CNS to reduce sympathetic outflow and vasoconstrictor tone.
Dosage: 50mg/tab; Route: NGT; Frequency: BID
Provide continual cardiac monitoring for patients receiving the drug.
Do not discontinue drug abruptly after long-term therapy.
Give drug with food to facilitate absorption.
Fluimucil (Acetylcysteine) Therapeutic category:
Mucolytic agent
3. Do passive ROM
Also to improve circulation
4. Have Enough rest
to provide relief to the pain felt
- D5NM
Medications
- Anti infective
- Antihypertensive
- Mucolytic Agents
- Multivitamins
using tap clean water, wipe from inner to outer canthus
e. Ear care- clean the pinna with moist wash cloth
f. Nose care- clean nasal secretions by blowing the nose gently with soft tissue
g. Hand washingh. Regular change
of clothingi. Environmental
Sanitation
any sign of complications occur
42

Exerts mucolytic action through its free sulfhydryl group which opens up the disulfide bonds in the mucoproteins thus lowering mucous viscosity. The exact mechanism of action in acetaminophen toxicity is unknown. It is thought to act by providing substrate for conjugation with the toxic metabolite.
Dosage: 600mg/tab +50cc water; Route: NGT; Frequency: OD
Monitor effectiveness of therapy and advent of adverse/allergic effects.
Instructpatient in appropriate use and adverse effects to report
Multiple vitamins (KREBB C) Multivitamin Dietary supplement for the
treatment and prevention of vitamin deficiencies. These vitamins are necessary for normal growth and development. Many act as coenzymes or catalysts in numerous metabolic
43

processes. Dosage: 1 cap; Route: NGT;
Frequency: OD Instruct patient to report
adverse effects of the drug.
44

Bibliography
Brunner and Suddarth’s. “Medical Surgical Nursing. Lippincott Williams and
Wilkins”. 12th Edition. Volume II. Pp.1966 – 1970
Hinchliff, Montague and Watson (1996). “Physiology for Nursing Practice”. Harcourt
Brace and Company. 2nd Editoin. p281
Doenges, et.al (2006). “Nurses Pocket Guide: Diagnoses, Interventions and
Rationales”. F.A. Davis Company: Philadelphia. 11th Edition.pp98-101, 70-73, 77-81
http://www.ninds.nih.gov/disorders/gbs/gbs.htm
http://www.mayoclinic.com/health/guillain-barre-syndrome/DS00413
http://www.scribd.com/doc/22044205/guillain-barre-syndrome-pathophysiology
45