Embed Size (px)
Citation preview

DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY CASE REPORT
Hemimegalencephaly: what happens when children get older?
NICKY WU1 | FELIPPE BORLOT1 | ANFAL ALI1 | TIMO KRINGS2 | DANIELLE M ANDRADE1
1 Division of Neurology, Epilepsy Genetics Program, Toronto Western Hospital, Krembil Neuroscience Centre, University of Toronto, Toronto, ON;2 Division of Neuroradiology, Department of Medical Imaging, Toronto Western Hospital, University of Toronto, Toronto, ON, Canada.
Correspondence to Danielle M Andrade, Toronto Western Hospital, 399 Bathurst Street, Toronto, ON M5T 2S8, Canada. E-mail: [email protected]
PUBLICATION DATA
Accepted for publication 16th December
2013.
Published online 5th February 2014.
ABBREVIATION
HME Hemimegalencephaly
AIMS Hemimegalencephaly (HME) is a rare congenital malformation of cortical development,
usually associated with developmental delay and severe epilepsy. This condition has rarely
been reported in adults. The aim of this study was to examine and compare neurological
findings in adult patients with HME.
METHOD We retrospectively examined adult patients with HME by evaluating the presence of
neurocutaneous disorders, current cognitive development, seizure control, and
documentation of therapies for seizure management and outcomes.
RESULTS Five patients were included in the study (three males, two females; mean age 23y
9mo [SD 6y 1mo], range 18–34y). Four patients had HME that was associated with
neurocutaneous syndromes and the remaining patient had isolated HME. Two patients
required surgical treatment for seizures in childhood. One patient had no intellectual
disability, while one had mild, and three severe intellectual disability. All patients presented
motor deficits ranging from mild hemiparesis in two patients to non-ambulation in one
patient. Patients in whom seizure onset occurred after the 7 years of age had better seizure
control and psychomotor development in adulthood than patients in whom seizure onset
occurred in the first year of life.
INTERPRETATION In our small sample of adults with HME, age at seizure onset, cognitive
disability, and seizure control were found to be associated.
Hemimegalencephaly (HME) is an uncommon congenitalmalformation of the brain characterized by the over-growth of one hemisphere. The enlarged hemisphereexhibits hamartomatous characteristics with dysplastic anddisorganized cell arrangements and atypical cell morpho-logy.1
The clinical picture varies depending on the severity ofthe malformation; however, HME patients typically exhibitrefractory epilepsy.2 Other clinical manifestations includemacrocephaly, colpocephaly, global developmental delay,intellectual disability, hemibody hypertrophy, and hemipa-resis.3 HME may present alone or in association with neu-rocutaneous syndromes, such as epidermal naevus and itssubtypes (i.e. linear naevus sebaceous syndrome and pro-teus syndrome), Klippel–Tr�enaunay–Weber syndrome,neurofibromatosis, or hypomelanosis of Ito.1–4
The pathogenesis of HME is probably related to errone-ous cell signalling during fetal development,1–3,5 possiblydue to genetic chimerism leading to discrepancy betweenthe affected and the unaffected hemispheres.6–8 Chimerismis a possible pathogeic model for isolated HME and neuro-cutaneous syndromes, given the similarities in clinical, neu-roradiological, and histopathological presentation of bothconditions. If two cell lineages arise from the neuralcrest progenitor cell line, one exhibiting normal cellular
physiology and the other abnormal cellular physiology,then different migration patterns could be observed. Thisexplains how skin lesions appear in neurocutaneoussyndromes and an enlarged hemisphere in patients withHME. Additionally, overgrowth of a hemisphere and epile-ptogenesis might be present if the affected cell line exhibitsmutations in the pathways regulating cell proliferation,such as the Wnt/b-catenin9 or phosphoinositide 3-kinase-AKT3-mTOR signalling pathway,8,10 or modified expres-sion of phospho-S67 ribosomal protein, interleukin 1b, andneuropeptide Y.10
While HME is well described clinically in infants andchildren, little has been reported on the long-term evolu-tion of this disorder into adulthood. The aim of this caseseries was to examine and compare neurological findings inadult patients with HME.
METHODSParticipantsAll patients with HME were seen at the Adult TertiaryEpilepsy Centre at the Toronto Western Hospital, Univer-sity of Toronto. Participants were selected based on thefollowing inclusion criteria: (1) age over 18 years; and(2) HME diagnosis confirmed by magnetic resonance imag-ing (MRI) showing diffuse enlargement of one hemisphere.
© 2014 Mac Keith Press DOI: 10.1111/dmcn.12390 905

Patients were excluded if (1) they had not been assessed inthe last 12 months; or (2) there was no clear documenta-tion of seizure frequencies since onset, antiepileptic drugs,or neurosurgeries.
Data collectionWe conducted a retrospective chart review collectingdemographic data, associated conditions, current seizurefrequency, treatments, cognitive evolution, magnetic reso-nance reports and imaging, and neuropathology reports ofpatients who had undergone surgery. Cognitive evolutionwas determined by examining the patients’ history forattention deficits, learning disabilities, or cognitive delay(according to neuropsychologist reports), and if they werefollowing a modified academic curriculum, such as lifeskills or special education programmes. Positive cognitiveevolution was defined as the absence of neurobehaviouraldisorders during adulthood or transition into a regular aca-demic curriculum. This study was approved by theresearch ethics board of the University Health Network.
RESULTSOut of 1750 patients in the Epilepsy Clinic Database, fivequalified for the study (three males, two females, mean age23y 9mo [SD 6y 1mo], range 18–34y). All but one patientpresented global developmental delay in childhood. Threestarted having seizures within the first year of life, and twoafter 7 years of age. HME-associated conditions were hyp-omelanosis of Ito in three patients and linear naevus seba-ceous syndrome in one patient. The diagnosis of HMEwas made after epilepsy onset through neuroimaging (com-puted tomography, MRI, and angiography), confirming thepresence of an enlarged hemisphere with associated dilatedventricles to varying degrees. Other imaging findingsincluded loss of grey matter–white matter differentiation,heterotopias, and cortical enlargement (Fig. 1). Neuro-pathological examination of resected sections from patients3 and 4 revealed gross disorganization or loss of corticallamination with immature balloon cells and disorganizeddendrites (Table I).
Treatment with antiepileptic drugs did not result incomplete seizure control, except in patient 2, who experi-enced a seizure-free period of 14 years before her seizuresresumed at 22 years of age. At present, all patients are onantiepileptic drugs (mean number of drugs 2.2). Patientswith syndromic HME required polytherapy to managetheir seizures. Patients 3 and 4, with childhood seizure fre-quencies in excess of 15 seizures daily, underwent hemi-spherectomy at 9 and 2 years of age respectively. Althoughthese patients continue to experience seizures, seizure con-trol has significantly improved since surgical intervention.
Cognitive impairment in adulthood ranged from lowernormal cognition to severe impairments (Table I). Patient1 has completed high school, albeit following a modifiedcurriculum and is currently a volunteer; patient 2 was ableto complete secondary school on a regular curriculum andis currently attending college. Patients 3, 4, and 5 require
constant supervision for daily living activities; they under-stand only a few simple commands, and use few words tocommunicate.
Our sample of adult patients demonstrated that theremight be an association between age at seizure onset,seizure control, and cognitive disability. Patients with lessextensive brain abnormalities and seizure onset after7 years of age (patients 1 and 2) had better cognitive devel-opment and seizure control during adulthood than patientswith a seizure onset within the first year of life and exten-sive brain abnormalities (patients 3 and 4).
Patients 1 and 2 are able to perform simple work orvolunteer duties, while those with early-onset epilepsy aretotally dependent for activities of daily living. In addition,the patient who presented isolated HME (patient 2) exhib-ited the best prognosis in our sample, being the only oneto experience a long seizure-free period.
On examination, all patients exhibited some form ofmotor defect. Patients 1, 2, 4, and 5 exhibited hemiparesis.Patient 3 was the only non-ambulatory patient in ourcohort. This patient had a fractured left femur at 4 yearsof age, and subsequently experienced several orthopaediccomplications, which may have contributed to his non-ambulatory state.
DISCUSSIONHME is a malformation of cortical development with path-ological findings strongly suggestive of errors affecting allthree phases of neuronal development: cell differentiation/proliferation, neuronal migration, and organization. Theaffected hemisphere usually demonstrates cytomegalic/bal-loon cells, disoriented axons and dendrites, heterotopicneurons, and indistinct/absent cortical lamination.1,11,12
Interestingly, the contralateral, supposedly ‘normal’, hemi-sphere may also be atypical, and this fact may explainthe lack of complete seizure control in our two patientswho underwent hemispherectomy (Patient 3: Engelclass IVA; Patient 4: Engel class IIIA). For instance,non-affected hemispheres were found to present cerebralhypoperfusion and hypometabolism, indicating that theymight also have developed abnormalities in early develop-ment.13 Structurally, the supposedly ‘normal’ hemispherecan demonstrate atypical columnar cortical arrangement,3
possibly contributing to the persistence of seizures afterhemispherectomy.
Long-term outcome in hemimegalencephalyEarly seizure activity may be indicative of the severity ofthe brain overgrowth/dysplastic nature. In turn, the sever-ity of the structural abnormalities could explain the poorer
What this paper adds• This is the first study of the progression of hemimegalencephaly into adult-
hood.
• Patients with late-onset epilepsy may exhibit better seizure control duringadulthood.
• Non-syndromic and/or less extensive hemimegalencephaly is associated withbetter outcomes.
906 Developmental Medicine & Child Neurology 2014, 56: 905–909

outcome (regarding cognition and seizure control) ofpatients in whom seizure onset occurred in the first year oflife, compared with those with seizure onset after 7 yearsof age, in our series. Undoubtedly, neuronal developmentdefects are strongly associated with poor cognition andrefractory epilepsy, as seen in patients with polymicrogyriaand lissencephaly.11,14 Thus, maintaining proper neuronalmigration and cortical lamination to some degree may bebeneficial in facilitating cognitive development and attenu-ating seizure frequency. The effects of continuous seizureson a developing brain, however, may also contribute tocognitive problems in adulthood.
For instance, it has been found that, among childrenwith temporal lobe epilepsy, neuropsychological function is
poorer in those in whom onset occurred early than inthose in whom onset was later, a finding attributed to pro-longed exposure to seizures.15 Moreover, prolonged expo-sure to pharmacoresistant epilepsy can impair cognition. Ina cohort study of 198 children, pharmacoresistant epilepsywas associated with lower performance on cognitive tests.16
Review of the literature demonstrates that in the major-ity of patients with HME, seizure onset occurred betweenthe first days of life and 2 years 6 months.2,5,10,17–20 In rareinstances, however, individuals with HME have experi-enced seizure onset during adulthood. In such cases, sei-zures are usually mild and intelligence is normal.21,22
Indeed, one of our patients was able to complete highschool on a regular curriculum, obtain a college-level
a b c
d e f
g h i
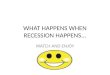
Figure 1: Patient 1 – MRI with (a and b) axial T1-weighted scans and (c) coronal fluid attenuated inversion recovery (FLAIR)-weighted image. The greymatter–white matter transition within the right posterior lobe is ill defined on the FLAIR-weighted sequences. This is confirmed on the T1-weightedsequences where the grey matter–white matter interface is less defined and the white matter is more hypointense compared with the left side overthe entire right occipital lobe extending toward the parietal operculum. Patient 2 – MRI with (d, e, f) axial FLAIR-weighted scans. There is evidence foran ill-defined grey matter–white matter junction, slight hyperintensity of the white matter of the right parietal, frontal, and temporal lobes with sparingof the occipital lobe. Patient 4 – MRI with (g, h, i) T1-weighted scans showing prominent sulcus in the left parietal lobe extending to the periventricularregion; prominent sylvian fissure with coarsening of gyral pattern and mild dilation of the left lateral ventricle.
Case Report 907

TableI:
Dem
ographic
statistics,clinical
data,a
ndmag
netic
resona
nceimagingan
dne
uropatho
logy
repo
rtsin
aserie
sof
adultpa
tientswith
hemimeg
alencephaly
Patients
12
34
5
Age(y)/se
x23/m
ale
24/female
34/female
18/m
ale
20/m
ale
Ageatse
izure
onse
t7y
8y
2d
3mo
11mo
Psy
chomotor
development
Mildlanguagedelayed
Mildgloballydelayed
Severe
globallydelayed
Severe
globallydelayed
Severe
globallydelayed
Hemisphere
affected
Right
Right
Right
Left
Right
Associatedco
nditions
HypomelanosisofIto,
righthemibody
hypertrophy
None
HypomelanosisofIto,
severe
scoliosis
HypomelanosisofIto
Linearnaevusse
bace
ous
syndrome
Intellectualdisabilitya
Mild
None
Severe
Severe
Severe
Currentmedications
Carbamazepine,
topiramate,lamotrigine
Carbamazepine
Carbamazepine,so
dium
divalproex
Clonazepam,phenytoin
Sodium
divalproex,lamotrigine,
nitrazepam
Currentse
izure
status;
typesofse
izures
Threese
izurespermonth;
foca
lonse
tse
izures+foca
lonse
tse
izureswithse
condary
generalization
Seizure
free;previous
foca
lonse
tse
izures+foca
lonse
tse
izureswithse
condary
generalization
40–5
0se
izurespermonth;
foca
lonse
tse
izures
+foca
lonse
tse
izures
withse
condary
generalization
30–6
0se
izurespermonth;foca
lonse
tse
izures
Clusters
ofthreeorfourse
izures
every
6mo;foca
lonse
tse
izures+foca
lonse
tse
izures
withse
condary
generalization
Motorneurological
deficits
Left
mildhemiparesiswith
norm
altoneanddeep
tendonreflexes
Leftmildhemiparesiswith
norm
altoneanddeep
tendonreflexes
Non-ambulatory,bilateral
pyramidalsigns,
global
hyperreflexia,andankle
clonus
Righthemiparesiswith
pyramidalsigns
Left
hemiparesiswithpyramidal
signs.
Left-handdystonic
posture
Neurosu
rgical
interventionsperform
ed
None
None
Rightfunctional
hemispherectomy;
ventricle
peritonealsh
unt
Left
functionalhemispherectomy
andsu
bduralperitonealsh
unt
inch
ildhood;rece
ntly,
anatomicalleft
hemispherectomyand
calloso
tomy
None
Neuroim
agingand/or
neuropathologyreports
MRI:mildpach
ygyria
overrightparietaland
occipitalco
rtexandill-
definedgreymatter–
whitematterjunction
overtherighttemporal,
parietal,andoccipital
lobesb
MRI:theright-sidesh
ows
ill-definedgreymatter–
whitematterjunctionin
theparietal,frontal,and
temporallobes.
The
threedescribedlobes
exhibitedhyperintensity
ofthewhitematter
signalb
Neuropathologyreport:
rese
ctedse
ctions
showedhistological
findingsco
nsistentwith
hemim
egalence
phaly;
cerebralco
rtex
containinglargenumber
ofabnorm
allylarge
neurons;
chaotica
lly
neuronalorganization
withdendritespointing
invariousdirectionsand
noco
rticallaminationc
MRI:left-sided
hemim
egalence
phaly
with
extensiveinvolvementofleft
hemisphere
andrelativesp
aring
oftheoccipitallobe.
Neuropathologyreport:
rese
ctedse
ctionssh
owed
histologicalfindingsco
nsistent
withhemim
egalence
phaly;
disorderedco
rticallamination
andneuronalorientation,
balloonce
lls,
giantneurons,
abnorm
alitiesofneuronal
shapeandNissl
patterns,
poor
greymatter–whitematter
junction,gliosis,
andneuronal
heterotopia
inthewhitematter
MRI:prominentsu
lcusin
the
rightparietallobeextending
deeply
totheperiventricular
region,co
arseningofthegyral
pattern,andaprominent
primitivesy
lvianfissure;mild
dilatationoftherightlateral
ventricle
withheterotopic
grey
matteraroundtheanterior
horn;asy
mmetricaldeepwhite
matterin
rightce
rebral
hemisphere,greymatter–white
matterdifferentiationis
well
maintainedb
aCognitiveevolutionwasdeterm
inedbyexaminingthepatients’history
forevidence
oflearningdisabilitiesorco
gnitivedelay(accordingto
neuropsy
chologistreports),and/ormodified
aca
demic
curriculum,su
chaslife
skills
orsp
ecialeduca
tionprogrammes.
Mildintellectualdisability:patients
havetheabilityto
profiteduca
tionallywithin
aregularclass
withtheaid
of
considerable
curriculum
modifica
tionandsu
pportivese
rvices.
Moderate
intellectualdisability:patients
needco
nsiderable
support
inschool,athome,andin
theco
mmunityin
orderto
participate
fully.Theyca
nlearn
simple
healthandsa
fety
skills,andtheymaywork
inash
elteredworksh
op.Severe
intellectualdisability:patients
needmore
intensivesu
pport
andsu
pervi-
sionthroughouttheir
entire
life.Theymaylearn
someactivitiesofdailylivingandtheirIQ
isbelow
35.bNopathologyreportsare
available
since
these
patients
havenotundergoneany
rese
ctivesu
rgery.cNopre-surgicalMRIavailable.
908 Developmental Medicine & Child Neurology 2014, 56: 905–909

degree, and achieve seizure control for 14 years withmonotherapy. We believe her late seizure onset, isolatedHME presentation, and less extensive brain abnormalityresulted in her experiencing a better clinical outcome thanour other patients.
Isolated versus syndromic hemimegalencephalyHME may result from genetic chimerism tying neurocuta-neous syndrome into the clinical picture of HME.6–8 How-ever, while chimerism and mutations regulating cellproliferation would explain the association between HMEand neurocutaneous syndromes,8–10 the differences in theclinical severity of isolated HME compared with syndro-mic HME have not been widely addressed. Flores-Sarnat1,3
found the same clinical neurological, neuroimaging, andneuropathological features in isolated and syndromicHME.
In our sample of adult patients, of the two patients withlate-onset epilepsy, the one with isolated HME exhibited
a better clinical outcome. Obviously, larger cohorts ofadult patients must be studied to make any statistical asso-ciation.
CONCLUSIONHME progression into adulthood has rarely beendescribed. In our evaluation of five adult patients, a lessfavourable outcome was seen in those in whom seizureonset was earlier, probably reflecting the severity of thestructural malformations. Of the two patients with late-onset epilepsy, the one with isolated HME exhibited abetter clinical outcome than the patient with syndromicHME. In addition, despite a reduction in seizure fre-quency, hemispherectomy did not provide complete seizurecontrol. This may be related to abnormalities on the sup-posedly ‘normal’ contralateral hemisphere. We recognizethat our sample of patients is small, and further studies onadults with HME are necessary to better characterize thelong-term evolution of this condition.
REFERENCES
1. Flores-Sarnat L. Hemimegalencephaly syndrome. Handb
Clin Neurol 2008; 87: 153–76.
2. Di Rocco C, Battaglia D, Pietrini D, Piastra M, Mas-
simi L. Hemimegalencephaly: clinical implications and
surgical treatment. Childs Nerv Syst 2006; 22: 852–66.
3. Flores-Sarnat L. Hemimegalencephaly: part 1. Genetic,
clinical, and imaging aspects. J Child Neurol 2002; 17:
373–84; discussion 84.
4. Menascu S, Donner EJ. Linear naevus sebaceous syn-
drome: case reports and review of the literature. Pediatr
Neurol 2008; 38: 207–10.
5. Tinkle BT, Schorry EK, Franz DN, Crone KR, Saal
HM. Epidemiology of hemimegalencephaly: a case ser-
ies and review. Am J Med Genet A 2005; 139: 204–11.
6. Malherbe V, Pariente D, Tardieu M, et al. Central ner-
vous system lesions in hypomelanosis of Ito: an MRI
and pathological study. J Neurol 1993; 240: 302–4.
7. Tagawa T, Futagi Y, Arai H, Mushiake S, Nakayama
M. Hypomelanosis of Ito associated with hemimegalen-
cephaly: a clinicopathological study. Pediatr Neurol 1997;
17: 180–4.
8. Lee JH, Huynh M, Silhavy JL, et al. De novo somatic
mutations in components of the PI3K-AKT3-mTOR
pathway cause hemimegalencephaly. Nat Genet 2012;
44: 941–5.
9. Yu J, Baybis M, Lee A, et al. Targeted gene expression
analysis in hemimegalencephaly: activation of beta-cate-
nin signalling. Brain Pathol 2005; 15: 179–86.
10. Boer K, Troost D, Spliet WG, Redeker S, Crino PB,
Aronica E. A neuropathological study of two autopsy
cases of syndromic hemimegalencephaly. Neuropathol
Appl Neurobiol 2007; 33: 455–70.
11. Guerreiro MM. Malformations of cortical development.
Arq Neuropsiquiatr 2009; 67: 570–4.
12. Cepeda C, Andr�e VM, Vinters HV, Levine MS, Math-
ern GW. Are cytomegalic neurons and balloon cells
generators of epileptic activity in paediatric cortical dys-
plasia? Epilepsia 2005; 46: 82–8.
13. Uematsu M, Haginoya K, Togashi N, et al. Unique dis-
crepancy between cerebral blood flow and glucose
metabolism in hemimegalencephaly. Epilepsy Res 2010;
92: 201–8.
14. Desai J. Epilepsy and cognition. J Paediatr Neurosci
2008; 3: 16–29.
15. Hermann BP, Seidenberg M, Bell B. The neurodevelop-
mental impact of childhood onset temporal lobe epilepsy
on brain structure and function and the risk of progres-
sive cognitive effects. Prog Brain Res 2002; 135: 429–38.
16. Berg AT, Zelko FA, Levy SR, Testa FM. Age at onset
of epilepsy, pharmacoresistance, and cognitive
outcomes: a prospective cohort study. Neurology 2012;
79: 1384–91.
17. Woo CL, Chuang SH, Becker LE, et al. Radiologic-
pathologic correlation in focal cortical dysplasia and
hemimegalencephaly in 18 children. Pediatr Neurol 2001;
25: 295–303.
18. Di Rocco C, Iannelli A. Hemimegalencephaly and
intractable epilepsy: complications of hemispherectomy
and their correlations with the surgical technique. A
report on 15 cases. Pediatr Neurosurg 2000; 33: 198–207.
19. Sugimoto T, Otsubo H, Hwang PA, Hoffman HJ, Jay
V, Snead OC. Outcome of epilepsy surgery in the first
three years of life. Epilepsia 1999; 40: 560–5.
20. Mathis JM, Barr JD, Albright AL, Horton JA. Hemim-
egalencephaly and intractable epilepsy treated with
embolic hemispherectomy. AJNR Am J Neuroradiol
1995; 16: 1076–9.
21. Beaulieu-Boire I, Lortie A, Bissonnette J, Prevost S,
Bergeron D, Bocti C. Hemimegalencephaly in an adult
with normal intellectual function and mild epilepsy. Dev
Med Child Neurol 2012; 54: 284–6.
22. Civardi C, Vicentini R, Collini A, Boccagni C, Cantello
R, Monaco F. Motor cortical organization in an adult
with hemimegalencephaly and late onset epilepsy. Neuro-
sci Lett 2009; 460: 126–9.
Case Report 909







![Our ermatology Online Letter to the Editor Inflammatory ... · intracerebral calcification and hemimegalencephaly, mental retardation is the most common one as in our case [1,6,8,9]](https://img.pdfslide.us/doc/110x75/5f895f1804e0b01fa00d76d0/our-ermatology-online-letter-to-the-editor-inflammatory-intracerebral-calcification.jpg)