Embed Size (px)
Citation preview

Bridges For Broken Hearts
HEART FAILURE Management
Tamara Chaker, MSN, CNS, ACNP-BC UCI Medical Center

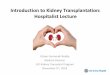
Hospitalization : Predominant Contributor to HF Costs
Transplants $270 million
Total= $38.1 billion 5.4% total HC costs
2010 American Heart Association

The heart is unable to produce cardiac output sufficient to meet metabolic requirements.
Heart Failure : Classic Definition
A syndrome caused by cardiac dysfunction : 1. Often resulting from myocardial muscle dysfunction or loss 2. Characterized by left ventricular dilatation or hypertrophy
3. Leading to neurohormonal and circulatory abnormalities and characteristic symptoms:
Fluid retention Shortness of breath Fatigue, especially on exertion
HFSA 2010 Practice Guidelines

Etiology of Heart Failure Common
Coronary artery disease (#1 cause in U.S.)/ischemic CMY Hypertension Valvular heart disease Idiopathic dilated
cardiomyopathy Drugs: alcohol, cocaine,
methamphetamine, medications (adriamycin)
Peri/Post Partum
Less Common
Congenital heart disease
Infiltrative cardiomyopathy : amyloid, sarcoid, restrictive
Hemachromotosis, Chagas
Thyroid disease/Hypo or Hyper-thyroid
Chronic renal disease
Viral and HIV cardiomyopathy

Heart Failure Pathophysiology
Myocardial injury Fall in LV performance
Neurohormonal Activation of RAAS, SNS, ET,
Vasopression, Cytokines, others
Myocardial toxicity Peripheral vasoconstriction Hemodynamic alterations
Remodeling and progressive
worsening of LV function
Heart failure symptoms Morbidity and mortality
ANP BNP, NO, PGE
-
-
Shah,M., et al. Rev Cardiovasc Med 2001: 2,(supplement2) 5:2.

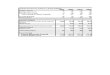
Left Ventricular Dilation and
Heart Failure Mortality
0 6 12 18 24
Months
0
20
40
60
80
100 Actuarial Survival %
LVEDDI < 44 m m /m
LVEDDI > 44 m m /m
2
2
P < 0.001
472 pts with Class III and IV Heart Failure
Independent mortality predictors: LVEDDI (p<0.001), Serum Na (p=0.02), Final PCW (p=0.01)
Ahmanson-UCLA Cardiomyopathy Center Lee AJC 1993;72:672-6.

Definition of Heart Failure
Systolic
Diastolic
However, still need to document for coding: • Acuity as Acute, Chronic, Acute on Chronic & • Type as Systolic, Diastolic, Combine

Common HF Symptoms
Physical Findings

New Approach to the
Classification of Heart Failure
Marked symptoms at rest despite
maximal medical therapy (eg, those
who are recurrently hospitalized or
cannot be safely discharged from the
hospital without specialized
interventions)
Refractory
end-stage HFD
Known structural heart disease
Shortness of breath and fatigue
Reduced exercise tolerance
Symptomatic HFC
Previous MI
LV systolic dysfunction
Asymptomatic valvular disease
Asymptomatic HFB
Hypertension
CAD
Diabetes mellitus
Family history of cardiomyopathy
High risk for
developing heart
failure (HF)
APatient DescriptionStage
Hunt SA et al. J Am Coll Cardiol. 2001;38:2101–2113.

New York Heart Association (NYHA) Functional Classification
Class I : No symptoms and no limitation in ordinary physical
activity, e.g. shortness of breath when walking, climbing stairs etc.
Class II : Mild symptoms (mild shortness of breath and/or angina)
and slight limitation during ordinary activity.
Class III : Marked limitation in activity due to symptoms, even
during less-than-ordinary activity, e.g. walking short distances (20-100 m). Comfortable only at rest.
Class IV : Severe limitations. Experiences symptoms even while
at rest. Mostly bed bound patients. Also, Pts with inotropes/VAD. ACC/AHA 2005 Guidelines Update for the Diagnosis and Management of Chronic Heart Failure in the Adult

Treatment Get With The Guidelines
Neurohumoral Antagonism is the Cornerstone of heart
failure management. Because of their beneficial effects on disease progression, functional status, hospitalizations,
and mortality risk, ACE-I, BB, and AA should be prescribed for all patients with left ventricular systolic dysfunction,
unless well defined contraindications exist.

ACE Inhibitors
• Interferes with the renin-angiotensin system
• Inhibits the enzyme responsible for converting
angiotensin I to angiotensin II
• Arterial and venous dilatation
• Decreases cardiac afterload
• Decreases preload
• Reverse cardiac remodeling

HFSA Practice Guideline
Prevention—ACEI and Beta Blockers
ACE inhibitors are recommended for prevention of HF in patients at high risk for this syndrome, including those with: Coronary artery disease Peripheral vascular disease Stroke Diabetes and another major risk factor
Strength of Evidence = A
ACE inhibitors and beta blockers are recommended for all patients with prior MI. Strength of Evidence = A

HFSA Practice Guideline
Pharmacologic Therapy: ACE Inhibitors
Recommended for symptomatic and asymptomatic patients with an LVEF ≤ 40%. Strength of Evidence = A
Titrate to doses used in clinical trials (as tolerated
during up titration of other medications, such as beta blockers).
Strength of Evidence = C


ACE Inhibitors Used in Clinical Trials
Trade Name Initial Daily
Dose
Target Dose Mean Dose in
Clinical Trials
Captopril Capoten 6.25 mg tid 50 mg tid 122.7 mg/day
Enalapril Vasotec 2.5 mg bid 10 mg bid 16.6 mg/day
Generic Name Monopril 5-10 mg qd 80 mg qd N/A
Lisinopril Zestril,
Prinivil
2.5-5 mg qd 20 mg qd 4.5 mg/day,
33.2 mg/day*
Quinapril Accupril 5 mg bid 80 mg qd N/A
Ramipril Altace 1.25-2.5 mg qd 10 mg qd N/A
Trandolapril Mavik 1 mg qd 4 mg qd N/A
*No mortality difference between high and low dose groups, but 12% lower risk of death or hospitalization in high dose group vs. low dose group.

ACEI : Therapeutics Contraindications:
Hx of angiodema, pregnancy, bilateral renal artery stenosis, “symptomatic” hypotension, shock, RI creat>3 , hyperkalemia>5.5
Complications:
Hyperkalemia, worsening renal function, cough, dysgeusia, angioedema
Practical Use:
Start lowest dose (you can even cut the lowest dose in ½)
Separate from beta blocker (if bp problem give mid-day)
Recheck CMP 1 week after each dose change > monitor K+, Creat

HFSA Practice Guideline
Pharmacologic Therapy:
Angiotensin Receptor Blockers (ARB)
Recommended for routine administration to symptomatic and asymptomatic patients with an LVEF ≤ 40% who are intolerant to ACE inhibitors for reasons other than hyperkalemia or renal insufficiency. (so if you get a big jump in K and a big jump in creat with an ACE, you will get the same with an ARB) (most commonly ordered due to ace induced cough).
Strength of Evidence = A

Angiotensin Receptor Blockers Used in Clinical Trials
Generic
Name
Trade Name Initial
Daily Dose
Target Dose Mean Dose in
Clinical Trials
Candesartan Atacand 4-8 mg qd 32 mg qd 24 mg/day
Losartan Cozaar 12.5-25 mg qd 150 mg qd 129 mg/day
Valsartan Diovan 40 mg bid 160 mg bid 254 mg/day

ARBs : Therapeutics
Contraindications: hyperkalemia >5.5, hx of angiodema, creatinine>3.0 (usually not used in men with a creat>2.5 and women with a creat >2.0)
Complications: angioedema, headache, dizziness, hyperkalemia, worsening renal function

Beta Blockers Interfere with sympathetic nervous system effects in HF by blocking norepinephrine
Inhibits cardiotoxicity of catecholamines
Slow heart rate for better diastolic ventricular filling
Decrease neurhormonal activation
Antiischemic
Antihypertensive
Antiarrhythmic
Reduce cardiac remodeling
The COMET trial demonstrated that carvedilol provided a 17% mortality reduction compared to metoprolol tartrate

Pharmacologic Therapy: Beta Blockers
Recommended for symptomatic and asymptomatic patients with an LVEF ≤ 40%.
IMPACT-HF demonstrated that in-hospital initiation is safe and improves treatment rates. Strongly consider initiation of carvedilol or another evidence based beta blocker prior to discharge, as this has been shown to improve patient compliance and treatment utilization. For patients who are tenuous or who have failed a prior attempt at initiation, ultra low doses may facilitate initiation. One suggested regimen is to start coreg 3.125 mg ½ tablet po Qhs, after 1 week the dose is given BID, after 3 weeks, the patient is advanced to 3.125 mg BID, then slowly titrated up at 4-8 week intervals Strength of Evidence = A

Effect of Beta Blockade on Outcome in Patients With HF and Post-MI LVD
Study Drug
HF
Severity
Target
Dose (mg)
Outcome
US Carvedilol1 carvedilol mild/
moderate
6.25-
25 BID
↓48% disease progression
(p= .007)
CIBIS-II2 bisoprolol moderate/
severe
10 QD ↓34% mortality (p <.0001)
MERIT-HF3 metoprolol
succinate
mild/
moderate
200 QD ↓34% mortality (p = .0062)
COPERNICUS4 carvedilol severe 25 BID ↓35% mortality (p = .0014)
CAPRICORN5 carvedilol post-MI
LVD
25 BID ↓23% mortality (p =.031)
1Colucci WS et al. Circulation 1196;94:2800-6. 2CIBIS II Investigators. Lancet 1999;353:9-13. 3MERIT-HF Study Group. Lancet 1999;353:2001-7. 4Packer M et al. N Engl J Med 2001;344 1651-8. 5The CAPRICORN Investigators. Lancet 2001;357:1385-90.

HFSA Practice Guideline
Pharmacologic Therapy: Beta Blockers
SYMPTOMATIC EXACERBATION Continuation of beta blocker therapy is recommended in most patients experiencing a symptomatic exacerbation of HF during chronic maintenance treatment, unless they develop cardiogenic shock, refractory volume overload, or symptomatic bradycardia. Strength of Evidence = C
Temporary dose reduction may be considered Avoid abrupt discontinuation Reinstate or gradually increase prior to discharge Titrate dose to previously tolerated dose as soon as
possible


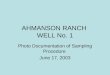
Effect of Carvedilol Dose on Mortality
in Patients with Heart Failure
15.5
6.1 5.6
1.1
Placebo 6.25 mg bid 12.5 mg bid 25 mg bid
Carvedilol Dose
0
5
10
15
20
% R
isk o
f M
ort
ality
Linear Trend p=0.0008
Carvedilol Dose-Response Trial (MOCHA)
p<0.001
p<0.05
Dose Response of Carvedilol in moderate heart failure patients on all cause mortality
Bristow Circulation 1996;94:2807

HFSA Practice Guideline
Pharmacologic Therapy: Aldosterone Antagonists
Recommended for patients on standard therapy, including diuretics, who have:
NYHA class II-IV HF AND reduced LVEF (≤ 35%)
Considered in patients post-MI with clinical HF or diabetes and an LVEF < 40% who are on standard therapy, including an ACE inhibitor (or ARB) and a beta blocker.
Strength of Evidence = A

HFSA Practice Guideline
Aldosterone Antagonists and Renal Function
Not recommended when: Creatinine > 2.5mg/dL (or clearance < 30 mL/min), >2 women Serum potassium> 5.0 mmol/L Therapy includes other potassium-sparing diuretics Strength of Evidence = A
Recommended that potassium be measured at baseline, then 1 week, 1 month, and every 3 months Strength of Evidence = A
Supplemental potassium is not recommended unless potassium is < 4.0 mmol/L Strength of Evidence = A

Lindenfeld J, et al. HFSA 2010 Comprehensive
Heart Failure Guideline. J Card Fail 2010;16:e1-e194.
HFSA Practice Guideline Aldosterone Antagonists
Generic Name Trade Name Initial Daily
Dose
Target Dose Mean Dose in
Clinical Trials
Spironolactone Aldactone 12.5-25 mg qd 25 mg qd 26 mg/day
Eplerenone Inspra 25 mg qd 50 mg qd 42.6 mg/day
Practical Use: Starting doses: Spironolactone 12.5 mg PO QD (or 6.25 mg in high
risk patient); Epleronone 25 mg QD. Get to target dose by 4 weeks if labs ok.
Decrease / discontinue supplemental K+, decrease loop diuretic
Check BMP 1 & 4 weeks with each dose change – monitor K, Creat
Contraindications: hyperkalemia, severe RI, metabolic acidosis

HFSA Practice Guideline
Pharmacologic Therapy: Hydralazine and Oral Nitrates
A combination of hydralazine and isosorbide dinitrate is recommended as part of standard therapy, in addition to beta-blockers and ACE-inhibitors, and an aldosterone antogonists for African Americans with HF and reduced LVEF
(Hydralazine 37.5-75mg tid, Isosorbide Dinitrate 20-40 mg tid)
A combination of hydralazine and isosorbide dinitrate may be considered in non-African American patients with HF and reduced LVEF who remain symptomatic despite optimized standard therapy

Device Therapy ICD / CRT

Cumulative Impact of Clinical Trial Evidence Based Heart Failure Therapies
Relative Risk 2 yr Mortality
None -- 35 %
ACE Inhibitor 23 % 27 %
Aldosterone Antagonist 30% 19 %
Beta Blocker 35% 13%
CRT-ICD EF < 35%, QRS>120 36 % 8%
Omega-3 FA 9 % 7 %
Cumulative risk reduction if all five therapies are used : 80%
Fonarow, GC. Lancet, 2008. 372(9645): p. 1195-6.

New Therapies for Heart Failure (Entresto) -(sacubitril/valsartan).
ENTRESTO is indicated to reduce the risk of cardiovascular death and hospitalization for heart failure in patients with chronic heart failure (NYHA Class II–IV) and reduced ejection fraction.
ENTRESTO is usually administered in conjunction with other heart failure therapies, in place of an ACE inhibitor or other ARB

.In heart failure with reduced ejection fraction, when compared with recommended doses of Enalapril…
Entresto was more effective than enalapril in . . .
Reducing the risk of CV death by 20% and HF hospitalization by 21% Reducing all-cause mortality by incremental 16% Incrementally improving symptoms and physical limitations Was better tolerated than enalapril . . . Less likely to cause cough, hyperkalemia, angioedema or renal impairment Less likely to be discontinued due to an adverse event More hypotension, but no increase in discontinuations.
PARADIGM-HF: Summary of Findings McMurray JJ et al. N Engl J Med. 2014 Sep 11;371(11):993-1004


Ivabradine Ivabradine was approved in the United States >3 years ago. It is indicated for the symptomatic treatment of chronic stable angina pectoris in patients with normal sinus rhythm who cannot take beta blockers. It is also indicated in combination with beta blockers in heart failure patients with LVEF lowers than 35 percent inadequately controlled by beta blockers alone and whose heart rate exceeds 70 beats per minute

Ivabradine..
Ivabradine is a specific inhibitor of the If current in the SA node and has no action in the heart or vascular system.
Unlike beta-blockers, ivabradine does not modify myocardial contractility and intracardiac conduction
Swedberg et al. Lancet 2010;376:875-885

Ultrafiltration? CARESS-HF trial. Aggressive diuretics vs
Ultrafiltration. In the trial, adding metolazone to the loop diuretic vs Ultrafiltration.
Both had same amount of weight loss
Ultrafiltration group had more adverse events

Discharge Criteria
Near optimal volume status achieved, goal is euvolemia.
Patient should be without any heart failure complaints. Able to
lay in bed flat and sleep well through the night, walk around
the nurses station without shortness of breath
Near optimal oral therapy achieved. On EBT BB, ACE/ARB,
MRA- at least low dosages as long as no contraindications
Transition from IV to oral medications. On po lasix/bumex for
preferably 24 hrs with good diuresis prior to discharge
Appointment within 7 days
Have received bedside education from nurse or resident
Ability to purchase meds or pharmacy to give 30 day supply

Discharge Criteria-per MOA
1. Resolution of clinical signs of volume overload
2. Decrease of at least one NYHA Classification for heart failure (order changed)
3. Discharge BNP with a minimum reduction of 30% and an optimally reduction of 50%, less than admit BNP. High BNP at discharge= high mortality
4. Sodium >130. Hyponatremia strongly linked to poor outcomes
5. No creatinine rise (>0.5 from baseline or for elderly >0.3 from baseline). Poor renal function has higher mortality.
6. Comorbid condition controlled & treated, and pain
7. Patient verbalizes understanding of discharge instructions and follow up care with physician/health care providers

Cardiovascular Center-Pav4 Daily heart failure clinic
Ability to give IV BUMEX or IV LASIX
Ability to see patients multiple times a week (if insurance allows)
Unable to see HMO patients
HF Palliative clinic- Palliative MD, and a social worker staff along with HF attending or NP Available

Observation Unit- HF OBS Protocol Low risk HF patients are placed in the OBS unit
HF NP comes to consult and help the OBS NP with diuresis and transitioning the patient out of the hospital
Patient will, if insurance allows, get an appt with HF NP within 1-3 days if needed for continued IV diuresis as an outpatient
Patient will be followed closely in clinic as needed and HF medications up-titrated to target dosages.

HOSPITAL
READMISSION
noncompliance
Not
weighing daily
Inadequate
discharge planningLack of fluid
restriction
Dietary indiscretion
Failed
social support
NSAIDS rxPoor follow-up
failure to seek careSuboptimal medical
therapy
Lack of
patient education

What Next ? Refractory Heart Failure Despite Maximum Medical Therapy …
Options ? : Referral to a HF Center Heart Transplantation Ventricular Assist Device Palliative Care

_ _
_Ventricular Assist Devices

LVAD on Chest X Ray

Biventricular support

PA Pressure monitoring (CardioMEMs)
http://www.ucirvinehealth.org/news/2015/02/first-to-use-remote-heart-failure-monitoring

CARDIOMEMS HF SYSTEM

Palliative Care It is an obvious strategy to address the needs of heart failure patients. The term palliative care does not connote care of the dying; rather, it is a holistic set of interventions designed to address the quality of life for patients and their families affected by life-limiting illnesses, whether needed for months or even years. Although palliative care appears to be the evident approach for heart failure patients; less than 10% of persons with heart failure receive palliative care services.

Summary
The burden of heart failure continues to grow and heart
failure is one of the single most deadly and expensive health
care problems
Medical therapies and nonpharmacologic measures for heart
failure that can impact patients' need for re-hospitalization,
costs of care, and survival are underutilized in conventional
practice settings
Every effort should be made to implement evidence-based,
guideline-directed therapies
Further research into promising therapies for HF is needed

Summary Initial goal of therapy is focused on symptom management followed by interventions that delay disease progression, reduce readmission, and prolong survival.
Palliative care referrals should be part of the HF management continuum to relieve symptoms, address the psychological and spiritual aspects of pt care and support the family/caregivers during illness into bereavement. It offers a support system to help pts live as actively as possible until they pass away.