Embed Size (px)
Citation preview

1
Rheumatology for the Hospitalist
Amish J. Dave, MD, MPHVirginia Mason Franciscan Health

2
• Chief Complaint: 80-year-old male with long-standing rheumatoid arthritis on chronic immunosuppression with leflunomide and prednisone 10mg daily presenting with fevers for last 1 week and worsening diffuse joint most severe in the right knee. Right knee swelling and redness has worsened over the past 2 days. He was hospitalized for diverticulitis 3 weeks ago.
• Exam: Temp 100.6, P 100, BP 120/80, RR 18
• MSK: Synovitis in multiple joints, including the bilateral wrists, MCPs, and ankles. Swelling bilateral knees, with marked pain and erythema of the right knee
•• Labs: WBC 12 with normal hemoglobin and platelet count. CMR wnl. ESR 102, CRP 10
(normal <3). Blood cx: Gram positive cocci
• He is started on antibiotics and prednisone is increased to 20 mg. His joint pain improves, except for the right knee pain and swelling.
Case 1

3
Early Arthritis
Acute Arthritis: The sudden onset of inflammation of the joint, causing severe pain, swelling, and redness.
Synovitis: Inflammation of the synovial lining of the joint
Persistent synovitis can cause structural changes in the joint and erosions

4
Inflammatory vs.Non-Inflammatory Arthritis
Feature Inflammatory Non-inflammatoryPain (when?)SwellingErythemaWarmthAM stiffnessSystemic featuresî ESR, CRPSynovial fluid WBCExamples
Yes (AM)Soft tissue SometimesSometimesProminent SometimesFrequentWBC >2000Septic, RA, SLE, Gout
Yes (PM)BonyAbsentAbsentMinor (< 30 minutes)AbsentUncommonWBC < 2000OA, AVN

5
Acute Monoarthritis
Inflammation (swelling, tenderness, warmth) in one joint
Polyarticular diseases can present with monoarticular onset, including:
– Rheumatoid arthritis– JRA– Reactive and IBD-associated arthritis– Sarcoid arthritis– Viral arthritis– Psoriatic arthritis

6
Causes of Acute Monoarthritis
THE MOST CRITICAL DIAGNOSIS TO CONSIDER: INFECTION !

7
• Septic
• Crystal deposition (gout, pseudogout)
• Traumatic (fracture, internal derangement)
• Hemarthrosis
• Osteonecrosis/avascular necrosis
• Presentation of polyarticular disorders

8
Tailoring Questions to Elicit a Focused History
Sudden onset of pain: -within minutes: think fracture-over several hours or 1-2 days: think infection, crystalline disease, flare of inflammatory
arthritis
History of IV drug use or a recent infection: -rule out septic joint
Recurrent similar attacks?:-crystalline or inflammatory arthritis
Prolonged courses of steroids?:-rule out infection or osteonecrosis of the bone

9
Acute Monoarthritis

10
Indications for Arthrocentesis– You want to analyze the synovial fluid (diagnostic
arthrocentesis)
– You want to reduce pressure/pain within a joint (therapeutic arthrocentesis)
Arthrocentesis is the single most useful diagnostic study in initial evaluation of monoarthritis and is helpful when there is:
1. Suspicion of infection2. Suspicion of crystal-induced arthritis3. Suspicion of hemarthrosis4. Difficult differentiating inflammatory from non-inflammatory arthritis

11
Tests to Perform on Synovial Fluid
1. Gram stain
2. Bacterial culture
3. Cell count and differential– Inflammatory vs. non-inflammatory
4. Polarized microscopy to look for crystals
Chemistry (glucose, total protein, LDH) unlikely to yield helpful information beyond the previous tests.

12
Other Tests in Evaluation of Acute Arthritis
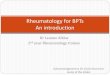
1. Almost always indicated: Radiographs – no erosions in rheumatoid arthritis until 1-2 years after
onset of synovitis; can see periarticular osteopenia within months of severe disease
CBC – cytopenias prior to disease onset can be helpful in diagnosis of SLE or rarely malignancy
ESR & CRP
2. Indicated in certain patients: Blood and urine cultures
3. Rarely indicated: Serologic: ANA, RF, anti-CCP, HLA-B27Serum uric acid level

13
Case 1, continued
Right knee aspiration performed by rheumatology
Cell count – 70,000 with neutrophil predominance
Gramm stain positive – Gram positive cocci on culture
Diagnosis: septic arthritis
The patient went for orthopedic joint wash-out, and had lengthy antibiotic course to treat septic arthritis

14
• Most articular infections – a single joint
• 15-20% cases polyarticular
• Most common sites: knee, hip, shoulder
• 20% patients afebrile
• Joint pain is moderate to severe
• Joints visibly swollen, warm, often red
• Comorbidities: RA, DM, SLE, malignancy, etc
Septic Joint

15
Septic Joints
• 80-90% monoarticular
• Most develop from hematogenous spread
• Most common:– Gram positive aerobes (80%)– Majority with Staph aureus (60%)– Gram negative 18%

16
Common Causes of Septic ArthritisGram Stain Patient Characteristic Organism of Concern
No Bacteria Young, healthy GC, Staph
No Bacteria History of RA Staph
No bacteria Immunosupression, IV drugs, Hx gm- infection
Staph, Strep, Pseudomonas, fungal
No Bacteria or Gm - Recent cat/dog bite Pasteurella multocida
Gm+ None Staph/Strep
Gm- diplococci None GC ( consider meningococcemia)
Gm - None Rx for possible pseudomonas
Gm - SLE or Sickle Cell Include coverage for Salmonella & Pseudomonas
No bacteria Hx prosthetic joint Staph epidermidis, Staph aureus
No bacteria HX fresh/salt H20 exposure + injury; chronic swelling
Mycobacterium marinum

17Am Fam Physician. 2011 Sep 15;84(6):653-60

18Am Fam Physician. 2011 Sep 15;84(6):653-60

19
Case 2
A 60-year-old woman is admitted to hospital with CHF exacerbation. She is treated with diuretics and does well with decreased dyspnea.
Three days into her hospitalization, she develops acute pain and swelling in the great toe and right hand. She denies having similar joint pain in the past.

21
Midfoot
Gout can occur in bursae, tendons,
and joints
Olecranon Bursa
Elbow
Wrist
KneeAnkle
Subtalar1st MTP
(eventually affected in ~90% of individuals with gout)
Fingers

22
Classic Gout vs Atypical Gout
Chronic form can be misdiagnosed as rheumatoid arthritis or osteoarthritis: acute flare-ups can be
misdiagnosed as cellulitis or infection
Can be misdiagnosed as cellulitis or infection
Chronic but can have acute flare-upsAcute
Tophi common at presentationTophi rare at presentation
Any joint, upper or lower extremity Usually in lower extremity
Symmetric or asymmetricAsymmetric
PolyarthritisMonoarthritis
Diagnosed in as many women as menPredominantly men
Observed in elderly patientsCan present at any age, including patients older than 60 years
Classic Gout Atypical Gout

23
Urate CrystalsNeedle-shaped
Strongly negative birefringent

24
Laboratory Testing in Gout• Synovial Fluid Analysis
WBC – 2000-100,000/ml MSU crystals- needle shaped, negatively birefringent
• Blood• Serum Uric acid level – important in monitoring treatment, but not
diagnostic– 40-49% will have normal uric acid levels
• Leukocytosis common• ESR and CRP are typically elevated• No indices of chronic inflammatory disease (albumin and
hemoglobin)• Measurable elevations in IL-6 and IL-1
• 24-hour uric acid collection • useful in young pts with gout + family history

25
The inflammasomes are innate immune system receptors and sensors that regulate the activation of caspase-1 and induce inflammation in response to infectious microbes and molecules derived from host proteins.
The inflammasome is involved in the initiation or progression of diseases with a high impact on public health, such as metabolic disorders and neurodegenerative diseases.
Anakinra is an interleukin-1 receptor antagonist often used for patients with gout and active infection/sepsis
Nature Medicine volume 21, pages677–687 (2015)

26
Pseudogout

27
PseudogoutPseudogout can cause monoarthritis that is clinically indistinguishable from gout
Often precipitated by illness or surgery
Pseudogout is most common in the knee (50%) and wrist
Reported in any joint (including MTP and cervical spine)
Chondrocalcinosis commonly seen in asymptomatic elderly patients

28

29
Calcium Pyrophosphate Crystals
Rod or rhomboid-shaped
Weakly-positive birefringent crystals

30
Treatment of PseudogoutPrednisone!
Most clinicians undertreat pseudogout with too low of a dose of prednisone and for too short a period of time
Consider steroid taper such as:
Prednisone 60 mg QAM with food for 4 days then 40 mg QAM for 3-4 days then 20 mg QAM for 3-4 days then 10 mg QAM for 2-4 days then stop
Patients should be prescribed 20 mg omeprazole daily while on steroid taper

31
A 30-year-old preschool teacher is admitted to the hospital with 3 days of diffuse pain and swelling, mainly in small joints. The wrists, MCPs, ankles, and knees are painful and swollen. She is unable to walk without significant pain and notes morning stiffness for 4 hrs.
She has tried 6-8 tablets of ibuprofen per day with minimal response. Many kids at her school have been ill recently. Her exam is notable for synovitis in small joints of the hands and feet, wrists and ankles.
Vitals are normal. She has no rashes. CV exam normal.
Labs: She has mild anemia with otherwise normal CBC, BMP, and LFTs. RF, CCP, ANA are negative. C3 and C4 are normal.
Case 3

32
Polyarthritis
• Polyarthritis involves inflammation (swelling, tenderness, warmth) of > 5 joints
• A patient with 2-4 joints is said to have pauci-articular or oligoarticular arthritis

33
Infectious Causes of Acute Polyarthritis
Neisseria gonorrhea
Meningococcemia
Lyme disease; other tick-borne illnesses including erhlichiosisand anaplasmosis
Rheumatic fever
Bacterial endocarditis
Viral: rubella, mumps, parvovirus, hepatitis B, chikungunya, Dengue

34
Non-infectious inflammatory causes of acute polyarthritis
Rheumatoid arthritis Juvenile idiopathic arthritis Systemic lupus erythematosus Seronegative spondyloarthropathy
Reactive arthritisPsoriatic arthritisIBD-related arthritisAnkylosing spondylitis
Polyarticular gout Sarcoid arthritis

35
Temporal Patterns in Polyarthritis
Migratory pattern: – Rheumatic fever, gonococcal (disseminated
gonococcemia), early phase of Lyme disease
Additive pattern– RA, SLE, psoriasis
Intermittent: – Gout, reactive arthritis, palindromic rheumatism

36
Case 3
Diagnosis: Parvovirus B19
Given only partial response to NSAIDs (first line treatment), she can be treated with short course prednisone (i.e., 20 mg with taper over 2-3 weeks) with complete resolution of symptoms

37
Case 4
A 72-year-old woman arrives in the ER noting acute loss of vision in the left eye that felt like “a curtain was rolling down my eye.” Symptoms began 3 hours ago and she notes several weeks of sharp headaches over her occiput, lack of appetite, and fatigue. She notes stiffness in both shoulders and both thighs
Labs include CBC with white blood cell count 3.5, hemoglobin 9.6, platelet count 540,000, ESR 90, CRP 89, CMR with Na 134, K 3.5, creatinine 0.86 mg/dL, AST 50, ALT 42, AP 110
What is the diagnosis?

38
Clinical Signs of Giant Cell Arteritis• New headaches or worsening of prior headaches in a patient over age 50• Scalp tenderness• New vision changes, including monocular vision loss of any duration of time• Jaw claudication – pain and/or stiffness with chewing or opening the mouth• Fever of unknown origin• Anemia of chronic disease• High ESR and/or CRP• Prior history of PMR or concomitant PMR symptoms• Chest pain or palpitations – rare signs of aortitis• Carotid bruits• Claudication of upper extremities – arterial stenosis of subclavian or carotid arteries

39
Epidemiology of Giant Cell Arteritis (GCA)As with PMR, northern Europeans/Scandinavians are most at risk and women develop GCA more often than men.
GCA almost never occurs in adults under age 50 and also peaks between ages 70-80.
GCA can involve any of the branches of the aorta, including the temporal arteries but also the aorta itself.
Image from Cleveland Clinic. http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/rheumat
ology/polymyalgia-rheumatica-and-giant-cell-arteritis/

40
Association of PMR with Giant Cell Arteritis (GCA)
• PMR is 2-3 times more common than giant cell arteritis (aka, temporal arteritis)
• That is, most patients with PMR will never develop giant cell arteritis
• But, 50% of patients with giant cell arteritis will have polymyalgia rheumatica
• Recurrence of PMR symptoms in a patient with known history of giant cell arteritis might be a sign of giant cell arteritis flare.
• PMR is not technically a “myositis.” Rather, is involves inflammatory in the proximal joints, bursae and tendons. Ultrasound, MRI, and PET imaging showed subacromial bursitis, subdeltoid bursitis, trochanteric bursitis, iliopsoas bursitis, and synovitis of the hips.

41
Initial Presentation of PMR• PMR involves abrupt (NOT subclinical) onset of symmetric aching and stiffness (not always pain) in the shoulders, hips, neck, and thighs
• The patient is over 50 years of age and cannot remember an antecedent illness or injury
• There is prominent morning stiffness and gelling (lack of activity makes stiffness worse)
• The stiffness can last into the afternoon or evening and affects activities of daily living (“I can’t comb my hair” and “I can’t get out of a car seat or out of a chair”)
• Systemic symptoms are common, including low-grade fever, fatigue, anergia, depression, and weight loss
Image from Mayo Foundation for Medical Education and Research.

42
Physical Exam in PMR• Given proximal articular inflammation, evaluating for bilateral shoulder and hip girdle limited range of motion is key.
• Pain may not always be present; patients might have more stiffness symptoms.
• Rarely, wrists, elbows, and hand joints might have swelling but this swelling is rarely overt synovitis as in rheumatoid arthritis. The feet and ankles are rarely involved.
•Remember, PMR does not actually involve the muscles themselves (not a true myositis) so signs of loss of sensation or loss of motor function might suggest a neurological deficit.
Image from Nature Reviews Rheumatology (2012);8:509-21. https://www.nature.com/articles/nrrheum.2012.97

43
• ESR and CRP• CBC with differential +/- smear• Liver function tests• BUN/creatinine• ANCA (MPO/PR3) panel• Vitamin D-25OH• Appropriate infectious work-up• SPEP• CPK/aldolase, RF and CCP if PMR symptoms
Lab Testing

44
Initial Treatment for ER Patient
Begin high dose methylprednisolone 1 gram daily for 3-5 days
Call Ophthalmology and Rheumatology consults to evaluate the patient and to guide the plan
Vision loss may be reversible with prompt initiation of high dose steroids
If high clinical suspicion for GCA but no vision loss or stroke, begin prednisone 1 mg/kg daily (40-60 mg).
Always begin daily PPI for GI ppx and calcium carbonate-vitamin D 600 mg-400 units 1 tab BID
Do NOT wait for temporal artery biopsy.
Use caution in patients with diabetes, severe hypertension, depression/suicidal tendencies, or prior poor steroid tolerance.

45
Try to obtain temporal artery biopsy (1-2 cm) through discussion with ENT, Neurosurgery, Vascular Surgery, or General Surgery within first 2 weeks for best chance of positive biopsy.
One-third of biopsies may be false-negative after >2 weeks of prednisone.
Obtain temporal artery biopsy on side with more headaches. If no headaches or scalp tenderness, go for bilateral temporal artery biopsy.
If unilateral temporal artery biopsy without signs of giant cells or fibrinoid necrosis, consider contralateral biopsy or treating empirically for GCA.
Temporal Artery Biopsy

46
Classic Pathological Findings• Evaluate for a panarteritis with inflammation of vessel walls with CD4+ lymphocytes and macrophages. Giant cells are not necessary to make the diagnosis.
Image from Nature Reviews Rheumatology (2012);8:509-21. https://www.nature.com/articles/nrrheum.2012.97
Image from Cleveland Clinic. http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/rheumat
ology/polymyalgia-rheumatica-and-giant-cell-arteritis/

47
• In patients with negative temporal artery biopsy, consider CT-A, MR-A, or PET-CT for evaluate of aorta and upper extremity vasculature.
• Findings might include mural thickening of the aorta, stenoses and dilatations of the carotid arteries, subclavian arteries, and brachial arteries.
• GCA rarely ever involves the coronary arteries, mesenteric blood vessels (PAN) or renal arteries
Image from Nature Reviews Rheumatology (2012);8:509-21. https://www.nature.com/articles/nrrheum.2012.97
Large Vessel Involvement in GCA

48
Initial Treatment of Giant Cell Arteritis
Image from Johns Hopkins Vasculitis Center. https://www.hopkinsvasculitis.org/types-vasculitis/giant-cell-arteritis/
Image from American Academy of Ophthalmologyhttps://www.aao.org/eyenet/article/giant-cell-arteritis-a-review
• For patients with positive temporal artery biopsy and/or imaging showing large vessel vasculitis, we typically treat with 1 mg/kg oral prednisone x 1 month (40-60 mg).
• After 1 month, taper by 5-10 mg every 2 weeks until 10 mg prednisone daily.
• Then taper by 1 mg every 2-4 weeks until off prednisone.
• For patients without eye disease at presentation, risk of futureeye disease is very rare if on prednisone 1 mg/kg daily for 2 weeks.
• ESR, CRP, CBC, and CMR are trended with prednisone taper.

49
Long-term Considerations with Steroid Therapy
•High risk of osteoporosis with GCA dosing of prednisone and steroid taper. Begin calcium, vitamin D (goal 30-60), alendronate or Reclast infusion for bone ppx.
• Begin PPI for GI ppx while on prednisone.
• Close ophthalmology follow-up for glaucoma or cataracts.
• Close PCP follow-up for hypertension, glycemic control, and lipid management.
• Monitor closely for adrenal insufficiency once on prednisone <10 mg/daily.

50

51
Differential Diagnosis of Giant Cell Arteritis
• Takayasu arteritis (women <40; renal artery stenosis)
• Primary CNS angiitis (multiple strokes)
• ANCA vasculitis (involves small blood vessels)
• Polyarteritis nodosa (involves medium-sized blood vessels)
• Infection
• Malignancy
• Crowned dens syndrome/CPPD
• Adult-onset Still’s disease

© 2014 Virginia Mason Medical Center
Summary• Septic arthritis is a medical emergency and requires arthrocentesis and synovial fluid culture/analysis for diagnosis and prompt initiation of antibiotic therapy
•Polyarticular gout is commonly seen in patients with heart failure on diuretics; anakinra is an option for patients with gout and infection
•Pseudogout is a not uncommon cause of fever of unknown origin and lengthy steroid taper is often effective treatment strategy
• GCA (or temporal arteritis) is a large vessel vasculitis involving any branch of the aorta. Classic symptoms include new or changing headaches, jaw or upper extremity claudication, scalp tenderness, vision changes, fevers, chills, night sweats, or fatigue.
• While steroids are first-line therapy for both PMR and GCA, anti-IL-6 therapy with tocilizumab has been FDA-approved for treatment of giant cell arteritis.
52

53
Thank you!