Embed Size (px)
DESCRIPTION
Presentation provided to Hospitalist leadership summit Dec 2 2010
Citation preview
Coordinating Care in Hospitalist Medicine
Hospitalist Executive Leadership Summit
December 2, 2010
Michael Wagner, MD FACPChief, Internal Medicine and Adult Primary Care
Michael Wagner MD FACP December 2010
Michael Wagner, MD FACP
Positions• Chief, Internal Medicine and Adult Primary Care, Tufts Medical Center 2008‐
present• Chief Executive Officer, EmCare Inpatient Services 2003‐8• Chief, General Internal Medicine, Tufts‐New England Medical Center 1999‐2003• Regional Medical Director, Cove Healthcare 1998‐1999• Internal Medicine Residency Program Director and Director of Medical Education,
St. Mary’s Hospital and University of Rochester 1992‐1997• Internist, New England Medical Center 1990‐1992• Chief Resident, Dartmouth‐Hitchcock Medical Center 1989‐1990• MD Georgetown University School of Medicine, 1986Current Roles• Associate Professor of Medicine, Tufts University School of Medicine• Vice Chair, institutional Review Board, Tufts Medical Center and Tufts University
Health Sciences • Physician Advisor, Information Technology Tufts Medical Center• Chair, Managed Care and Quality Committee, Tufts Medical Center Physician
Organization
Disclosures• None 2
Michael Wagner MD FACP December 2010
Collaboration – Goals of presentation
• Discuss broad concept of collaboration in hospitalist medicine
• Segment collaboration into functional assessment categories
• Discuss specific areas for collaboration and coordination• Discuss specific strategies to enhance and hardwire
collaboration and coordination of care into a hospitalist program
Michael Wagner MD FACP December 2010
Provisos
• Focus – Day/rounding hospitalist• Non-teaching environment
Michael Wagner MD FACP December 20105
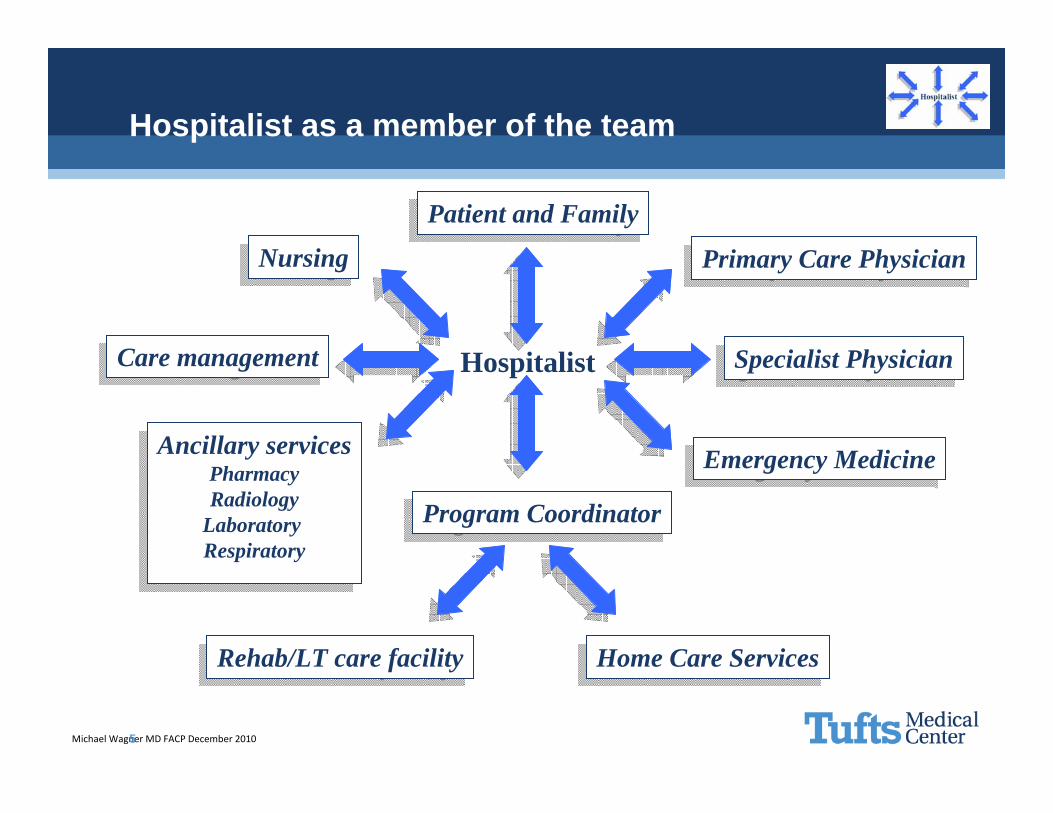
Hospitalist as a member of the team
Hospitalist
Program CoordinatorProgram Coordinator
Patient and FamilyPatient and Family
NursingNursing
Care managementCare management
Ancillary servicesPharmacyRadiology
Laboratory Respiratory
Ancillary servicesPharmacyRadiology
Laboratory Respiratory
Primary Care PhysicianPrimary Care Physician
Specialist PhysicianSpecialist Physician
Home Care ServicesHome Care ServicesRehab/LT care facilityRehab/LT care facility
Emergency MedicineEmergency Medicine
Michael Wagner MD FACP December 2010
Collaboration – Case
• Dr. Smith is a new graduate from a local residency program who recently joined your hospitalist service. He came with excellent references and interviewed very well when he was recruited.
• After 3 months into working, you (as the medical director of the program) perform a focused professional practice evaluation (FPPE). You perform a chart review and review the metrics that have been collected so far. He seems to be doing well and his documentation is complete and medically appropriate. Feedback from nursing is not negative.
• When you ask around most of the staff have met him but they say they don’t know him very well.
Michael Wagner MD FACP December 2010
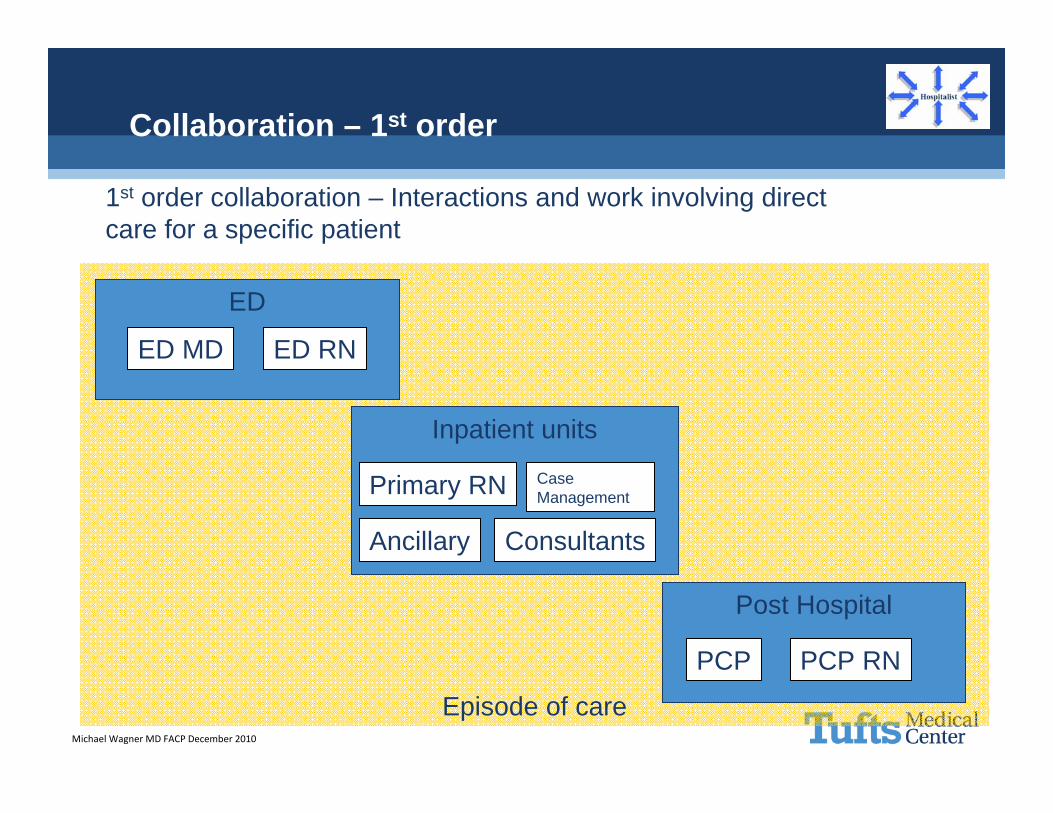
Episode of care
Collaboration – 1st order
1st order collaboration – Interactions and work involving direct care for a specific patient
ED
Inpatient units
Post Hospital
ED MD ED RN
Primary RN Case Management
PCP PCP RN
Ancillary Consultants
Michael Wagner MD FACP December 2010
Collaboration – Case continued
•When you begin your block of shifts you pick up Dr. Smith’s patients. In the process of finishing several discharges you find several inconsistencies in the medication lists between admission and the planned dc med list you have from his last note.•This prompts you to talk to the patient’s primary nurse.
“I was hoping to talk with one of you hospitalist about this patient’s med list. Dr. Smith wasn’t available and I never had the chance to talk with him the case. In fact sometimes I don’t even see him. I have to page him several times in the morning just to clarify orders he has written.”
Michael Wagner MD FACP December 2010
Collaboration - Engagement
Actively disengaged
Disengaged
Engagable
Actively Engaged
Michael Wagner MD FACP December 2010
Collaboration – 2nd order
• Floor nursing• Case management• Specialty physicians• ED physicians
2nd order collaboration – Interactions and relationships that are created and exist between the hospitalist and other care givers
Michael Wagner MD FACP December 2010
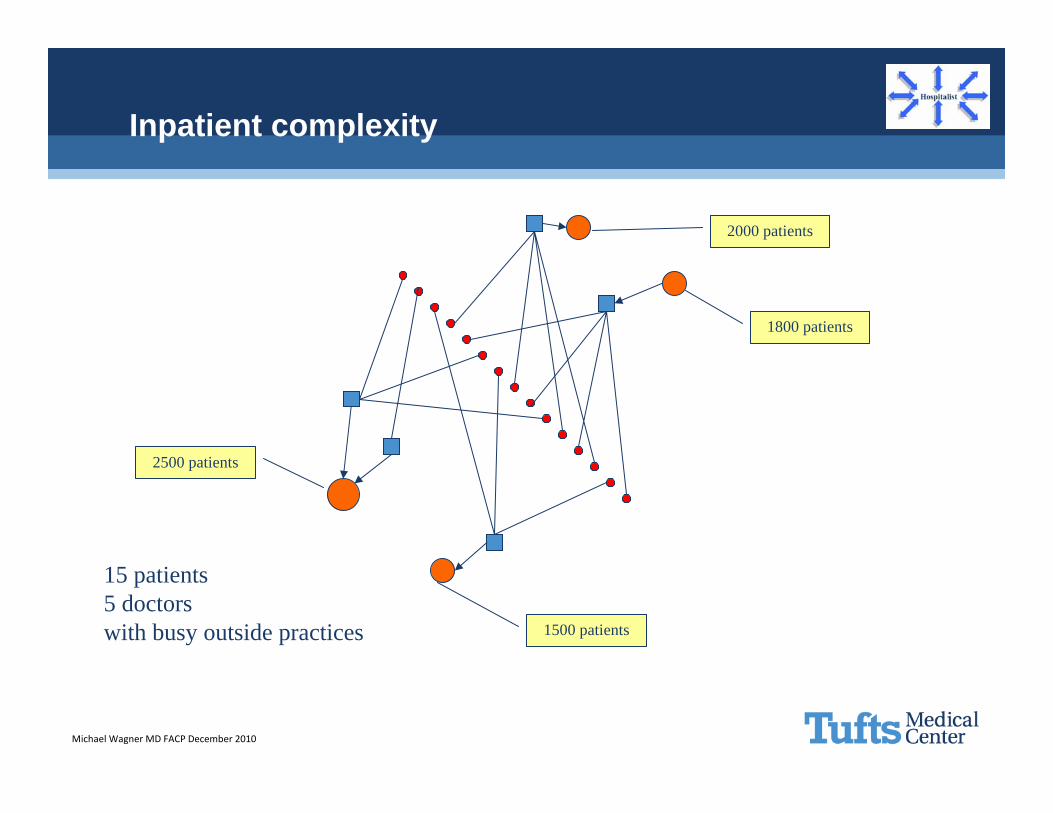
Inpatient complexity
1500 patients
15 patients5 doctorswith busy outside practices
2000 patients
2500 patients
1800 patients
Michael Wagner MD FACP December 2010
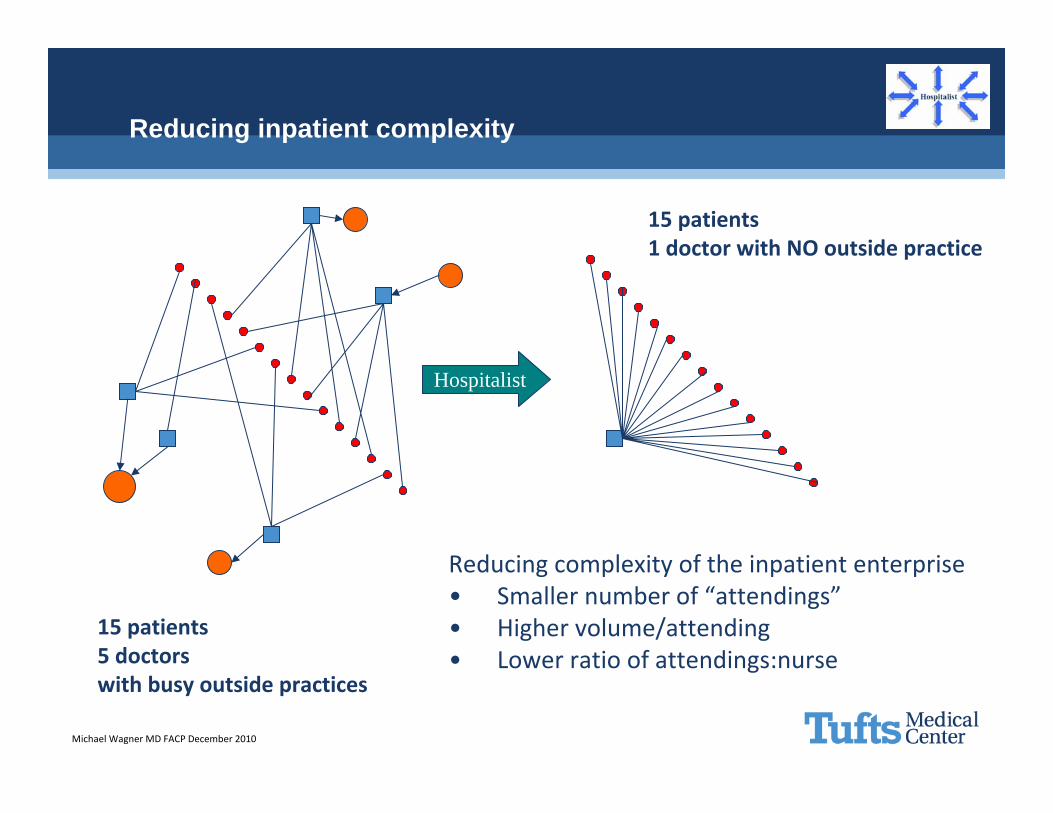
Reducing inpatient complexity
Hospitalist
Reducing complexity of the inpatient enterprise• Smaller number of “attendings”• Higher volume/attending• Lower ratio of attendings:nurse
15 patients5 doctorswith busy outside practices
15 patients1 doctor with NO outside practice
Michael Wagner MD FACP December 2010
Collaboration – Case continued
• You go and seek out Dr. Smith the next time he is on and ask him to recount his typical day:
“I usual start in the office and start my progress notes there. Igather the vital signs and labs that have returned so far. I then go to the floor and see my patients. You know there really isn’t a good place to think or write my notes so I go back to the office and finish my notes. You know it is really annoying that the nursing staff keep paging me, I think my orders are pretty clear. You know thenursing staff isn’t very good here.”
• You get the sense he is not very happy in his new role and you are not happy with his attitude.
Michael Wagner MD FACP December 2010
Collaboration – 3rd order
• Emergency Department• Nurse managers• Case management department• Primary care practices
3rd order collaboration – Interactions and relationships that are created and exist between the hospitalist program and the other clinical departments and outside referring physicians.
Michael Wagner MD FACP December 2010
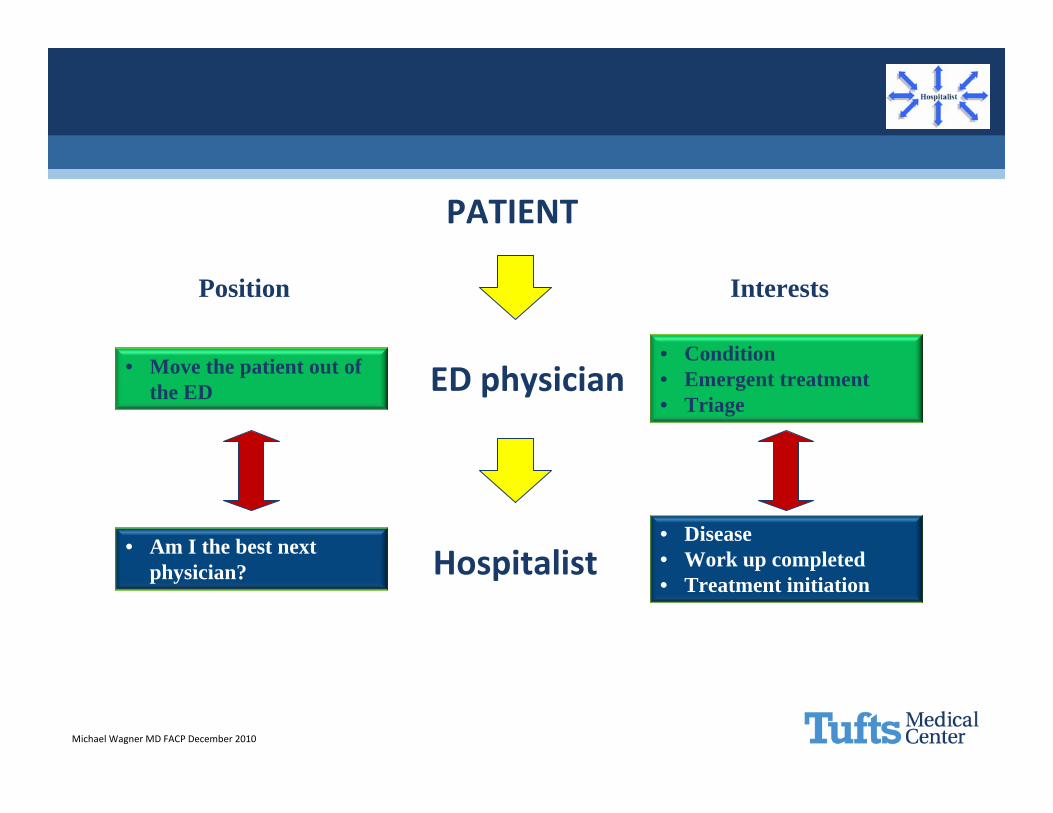
ED physician
PATIENT
Hospitalist
• Condition• Emergent treatment• Triage
• Disease• Work up completed• Treatment initiation
InterestsPosition
• Move the patient out of the ED
• Am I the best next physician?
Michael Wagner MD FACP December 2010
Collaboration – Case continued
• The hospital administrator calls you to complain about the delays in transfers from the ED to the floors. He has gotten feedback from the ED that the hospitalists are taking forever to call back and get down to the ED for new admissions. He also states at the last FLOW committee the assigned hospitalist did not show up.
Michael Wagner MD FACP December 2010
Collaboration – Best practices
• Recruit relaters• Primary nurse face to face communication• Organized daily multi-disciplinary rounds• Deal with the ED conflict issue• Virtually integrate with your referring PCPs• Develop care expectations• Leadership
Michael Wagner MD FACP December 2010
Develop care expectations
• Traditional– Pneumonia– CHF– Chest pain
• Service standards– Time to see patients– Communication
• Special populations– Frail elderly– Warfarin– Poly-pharmacy– Frequent re-admissions
Michael Wagner MD FACP December 2010
Collaboration – Hospital based physicians
• 1st order– Verbal communication about why you want the consult or
procedure done– Make a point to touch base if you see consultant and discuss case
face to face
• 2nd order– Introduce yourself– Interact in MD lounge – Eat lunch with someone new
• 3rd order– Participate in medical staff committees– Go to medical staff meetings– Discuss sources of frustrations with medical director
Michael Wagner MD FACP December 2010
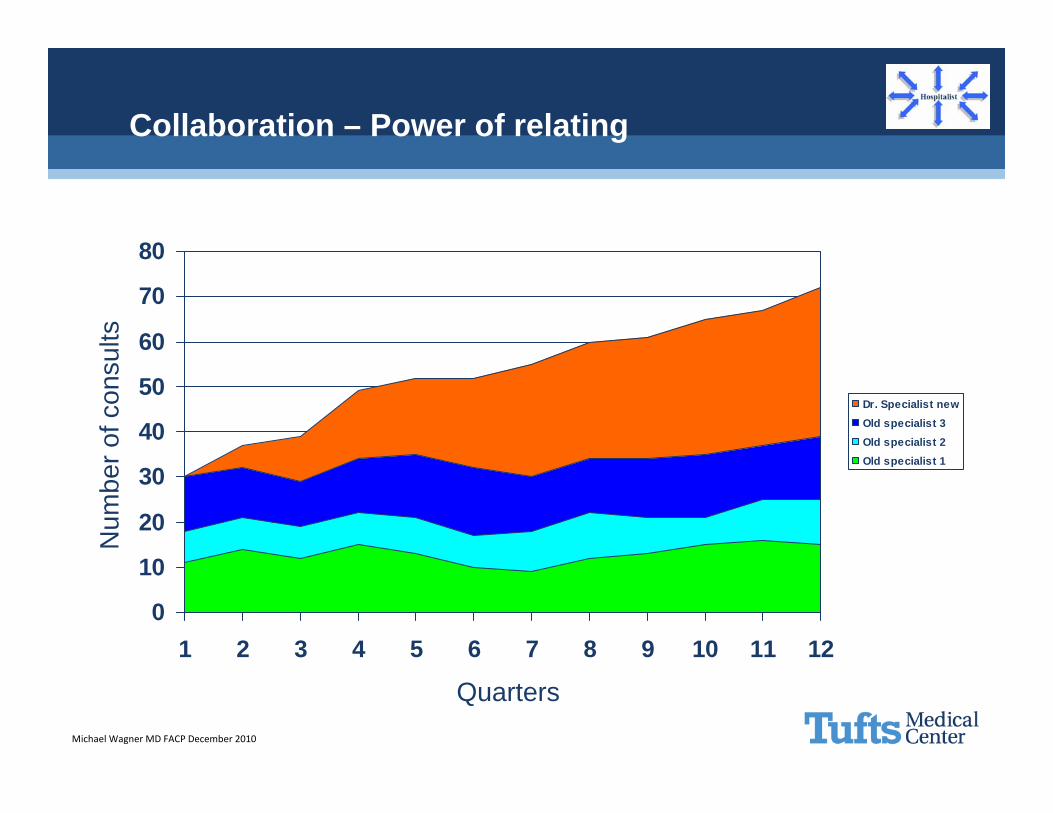
Collaboration – Power of relating
0
10
20
30
40
50
60
70
80
1 2 3 4 5 6 7 8 9 10 11 12
Dr. Specialist newOld specialist 3Old specialist 2Old specialist 1
Quarters
Num
ber o
f con
sults
Michael Wagner MD FACP December 2010
Collaboration – PCPs
• 1st order– Make an attempt to call and discuss case with PCP on admission– Call PCP at time of DC– Write a concise and accurate discharge summary
• 2nd order – Go to mixers for PCP staff
• 3rd order– Get involved in IDN/ACO committees – there will be PCPs driving
this process and discussion
Michael Wagner MD FACP December 2010
Collaboration – Case conclusion
• Dr. Smith is very appreciative of your feedback and specific suggestions on rounding with the primary nurse. The number of pages has decreased and he is feeling more comfortable. He agrees to participate in the Flow committee as well.
Michael Wagner MD FACP December 2010
The hospitalist’s dilemma
“Bummer of a birthmark, Dr. Hal.”