Embed Size (px)
Citation preview

NURSE PRACTITIONER
HOSPITALIST PROGRAM
Charisse Oland, Chief Executive Officer Rusk County Memorial Hospital
Dr. Debra Frenn, Chief Patient Care Officer
TODAY’S OBJECTIVES To understand
APN hospitalist models in a rural setting
Cultural engagement by medical staff and others
Effect on quality, patient satisfaction and operations
Regulatory requirements for start up Please note that the views expressed by the conference speakers do not necessarily reflect the views of the American Hospital Association and Health Forum.
10 primary care MDs in 2010; 5 in 2015
1 Independent clinic and multiple specialists in 2010
Opened Provider Based Rural Health Clinic in 2014
2013-15 dynamic radical change
RUSK COUNTY MEMORIAL HOSPITAL
RUSK COUNTY MEMORIAL HOSPITAL
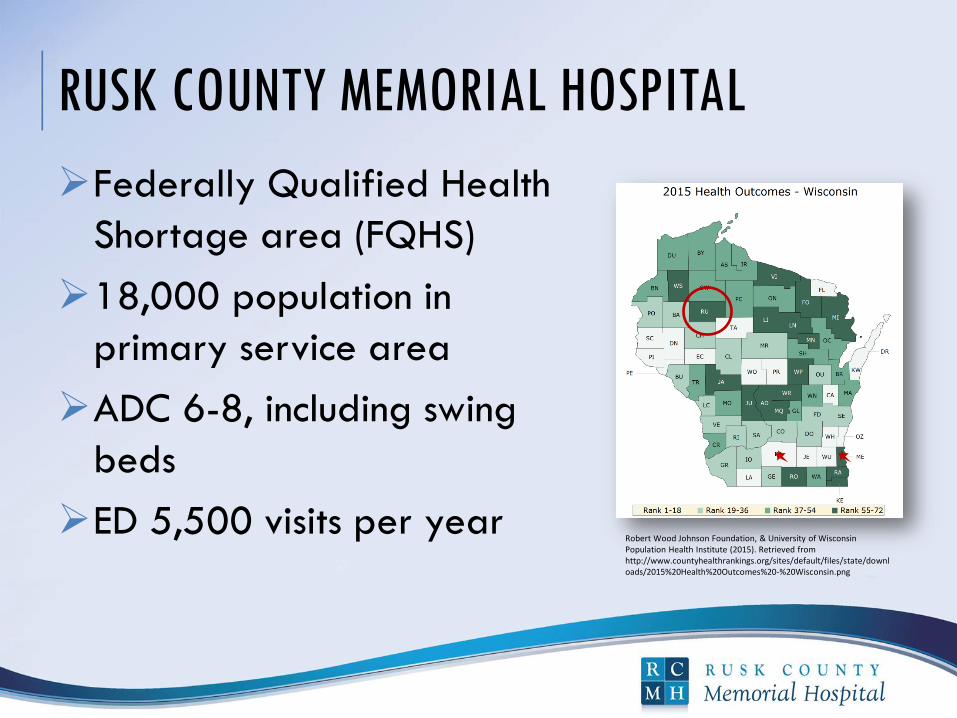
Federally Qualified Health
Shortage area (FQHS)
18,000 population in
primary service area
ADC 6-8, including swing
beds
ED 5,500 visits per year Robert Wood Johnson Foundation, & University of Wisconsin Population Health Institute (2015). Retrieved from http://www.countyhealthrankings.org/sites/default/files/state/downloads/2015%20Health%20Outcomes%20-%20Wisconsin.png
RWJF AND INSTITUTE OF MEDICINE – REPORT
ON THE FUTURE OF NURSING
Nurses should be full partners with physicians
Nurses should practice to the top of their license
Achieve higher levels of education and improve
the educational system for a seamless
educational progression
Effective workforce planning and policy making
Institute of Medicine. (2010). The future of nursing: Leading change, advancing health. Retrieved from http://books.nap.edu/openbook.php?record_id=12956&page=R1
WHY START A HOSPITALIST PROGRAM NOW?
Hospitalist: newer specialty term
First cited in a New England Journal of Medicine
article in 1996.
More than 50% of hospitals have a hospitalist
program
Many CAH use APNs due to primary care shortage
Primary focus is to improve the quality of care
through system change
Wachter, R. M. and Goldman, L. The Emerging Role of Hospitalist in the American Healthcare System; New England Journal of Medicine (1996) 335: 514-7.

IMPROVE RURAL PHYSICIAN RECRUITING
Of the 2,050 rural counties in the United
States, 77% have primary care shortages
One challenge in recruiting is the lower amount
of “time away from work” in a rural area i.e.,
On Call schedule
Doescher, M.P., Skillman, S.N. &Rosenblatt, R.A. (2009) The Crisis in Rural Primary Care (Policy Brief). WWAMI Rural Health Research Center.
WHY CHANGE NOW?
Loss of 6 primary care MDs in 2 years
Suspension of OB services
New replacement hospital 45 miles away
Independent physician group, also in radical change
Recruiting challenge: call burden
Decreased market share 2010: 43%, 2013: 21%
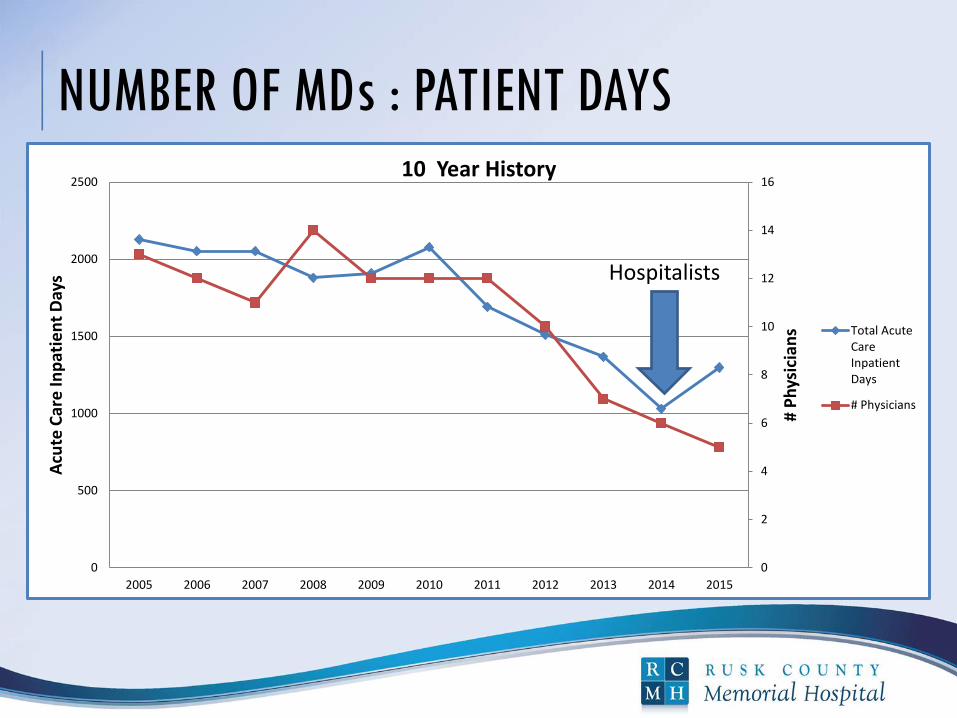
NUMBER OF MDs : PATIENT DAYS
0
2
4
6
8
10
12
14
16
0
500
1000
1500
2000
2500
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
# P
hys
icia
ns
Acu
te C
are
Inp
atie
nt
Day
s
10 Year History
Total AcuteCareInpatientDays
# Physicians
Hospitalists
DYNAMIC RADICAL CHANGE:
THE “QUADFECTA” 2014
Hospital opened own clinic (PBRHC)
APN Hospitalist Program launched
ED physician group replaced
Remodeled facilities “Fresh Eyes”
patient-centered care
Influence the continuum of care and outcomes

STRATEGIC GOAL – GROWTH PILLAR
We will be led by highly qualified providers
(physicians and extenders) with appropriate
number and compliment for the level of services
and programs expected to meet community
needs.

APN HOSPITALIST PROGRAM GOALS
↓ Call burden for MDs
↑ MD quality of life and recruiting potential
↑ Clinical quality outcomes with standardized
protocols and continuity of care
↑ Patient satisfaction
Retain community support
and market share
TRIPLE AIM
Improve experience of care
Decrease per capita cost
Improve population health
Haering, J. (2015, July 31). Why having a physician advisor is a good idea. (Web log content). Retrieved from http://blog.resonantadvisor.com/why_physician_advisor
Ministry–Eagle River Memorial Hospital, WI
2 APNs 12 hour shifts
DHS waiver telemedicine model
Wisconsin administrative code DHS 124.04(3)(a)
Nurse practitioner hospital pilot program
Aspirus-Medford, WI
24/7 with 3 ANPs
7 days on, 14 days off
Collaborating physician (FP) Rounding
EXPLORATION OF MODELS
VARIATION IN MODELS
APN:MD mixed model Job description: Excludes ED and/or clinic coverage
Difference: First responder vs. unit based vs. traditional
Telemedicine collaborating physician
Onsite collaborating physician
Scheduling Shift: 12 hour (day vs night) vs 24 hour
Pattern 7/14 vs 5/5/5 vs. ?
Backup coverage incorporated into plan
Salary/benefits; per diem locums

PHASE ONE PLANNING
Medical staff support
Board support/business
plan
Enabling medical staff
bylaws
Staff education
Community education

MEDICAL STAFF ENGAGEMENT
Meetings with independent
physician group clinic
management
Participation in site visits
Opinion polls
Attorney meetings
MEDICAL STAFF ENGAGEMENT
Bylaws revision team: Chief of Staff, ED
physician, CEO, Chief Patient Care Officer and
Quality Manager
Chief of Staff updates at monthly medical staff
meetings
Medical staff invited to participate in APN
interviews
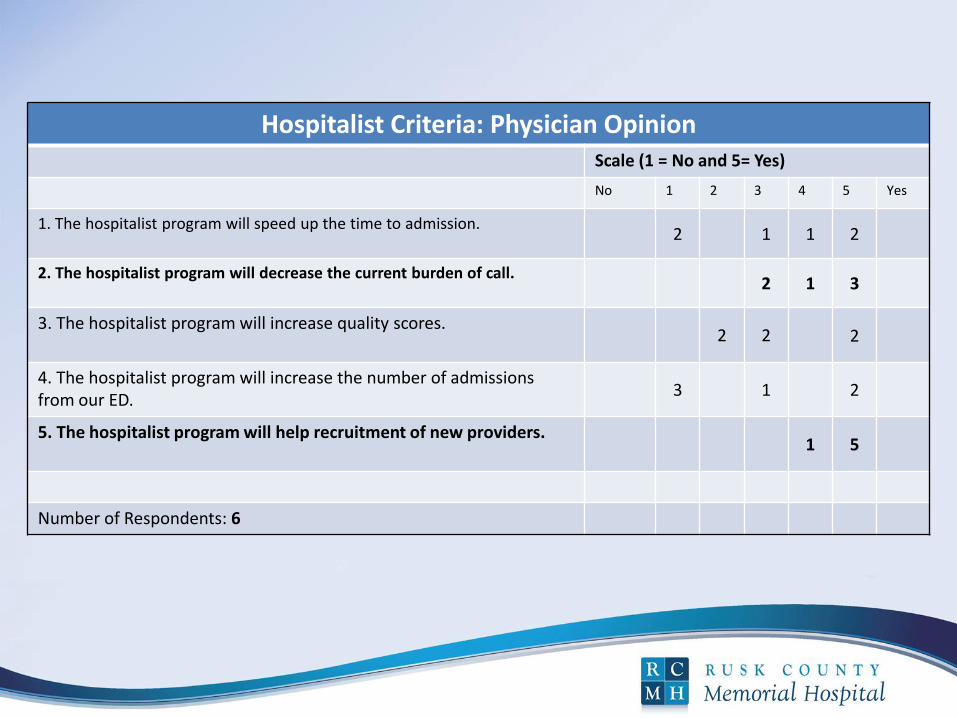
Hospitalist Criteria: Physician Opinion Scale (1 = No and 5= Yes)
No 1 2 3 4 5 Yes
1. The hospitalist program will speed up the time to admission. 2 1 1 2
2. The hospitalist program will decrease the current burden of call. 2 1 3
3. The hospitalist program will increase quality scores. 2 2
2
4. The hospitalist program will increase the number of admissions from our ED.
3 1 2
5. The hospitalist program will help recruitment of new providers. 1 5
Number of Respondents: 6
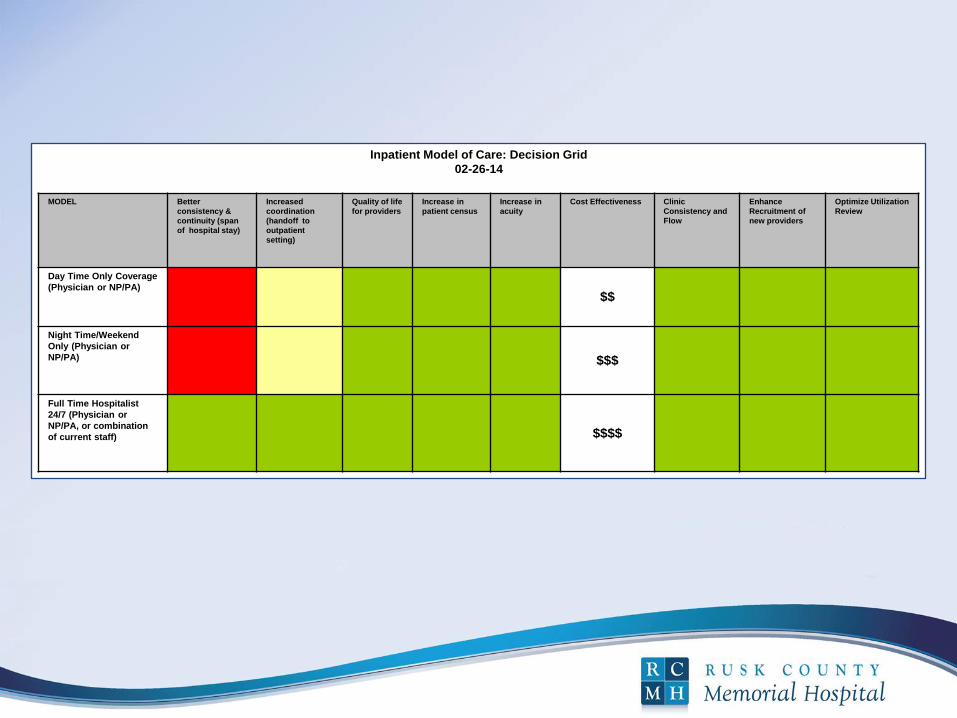
Inpatient Model of Care: Decision Grid
02-26-14
MODEL Better
consistency &
continuity (span
of hospital stay)
Increased
coordination
(handoff to
outpatient
setting)
Quality of life
for providers
Increase in
patient census
Increase in
acuity
Cost Effectiveness Clinic
Consistency and
Flow
Enhance
Recruitment of
new providers
Optimize Utilization
Review
Day Time Only Coverage
(Physician or NP/PA) $$
Night Time/Weekend
Only (Physician or
NP/PA) $$$
Full Time Hospitalist
24/7 (Physician or
NP/PA, or combination
of current staff) $$$$
REGULATORY/LEGAL
State laws: Wisconsin Administrative Code DHS
124.04(3)(a)
CMS rules and regulation
Swing bed provisions
Medical staff
bylaws
Wisconsin Hospital Association (2015). Retrieved from http://www.wha.org/pubArchive/special_reports/RH2015review.pdf
REGULATORY/LEGAL
State APNP Practice Act
Collaborating Physician Agreement-Contract
Primary Care Collaborator
Emergency Physician Contract
Authenticate admissions only
Wis. Stat. §35.93, Ch. N 8
COLLABORATING PHYSICIAN ROLE
Available by phone 24/7
Backup physician
Joint rounding
Monthly quality chart review
Sign off on H&P and discharge summary
ED physician sign off on authentication for
admission
MEDICAL STAFF BYLAWS KEY PROVISIONS
Active staff privileges/voting rights for APN
May not be an officer
Active staff privileges/voting rights for ED physicians
Collaborating agreement to authenticate admissions
Active staff privileges for no/low volume admitters who serve on committees
Option to admit and follow own patients
Peer review (OPPE/FPPE)
CRITERIA FOR APN CANDIDATE SELECTION
Acute care experience with practicums
Hospitalist experience preferred
ACLS certified
Excellent work history
and references
Cultural fit
Collaboration/communication
skills
Pratt, S. (2015, March 18). 3 Steps to help you become the perfect candidate. (Web log content). Retrieved from http://www.socialtalent.co/blog/page/23
ORIENTATION PLAN
Hospitalist “Boot Camp” one week
Shadow APN at another CAH one week
Complete competency assessment
Collaborating physician mentoring time
General hospital orientation
TEAM CULTURE
APN available 24/7 to answer questions and concerns
Code response availability
No ED tuck-in orders
Multidisciplinary team rounding
Improved access for discussion of admissions
Increased nursing interaction and education
Increased patient and family interaction and education
APN EXPECTATIONS
Sleep space and work space
Communication expectations with primary care
provider re their patients (admission/daily
care/discharge process)
Orientation process (complete skills assessment,
attend hospitalist boot camp)
Involvement with design and testing of CPOE
order sets, P&P, optimizing workflows, etc.
MULTIDISCIPLINARY TEAM ROUNDING DAILY
MD collaborator during orientation, periodically thereafter
APN—generally done independently
Nursing leader
Occupational Therapy
Physical Therapy
Pharmacist
Case Manager
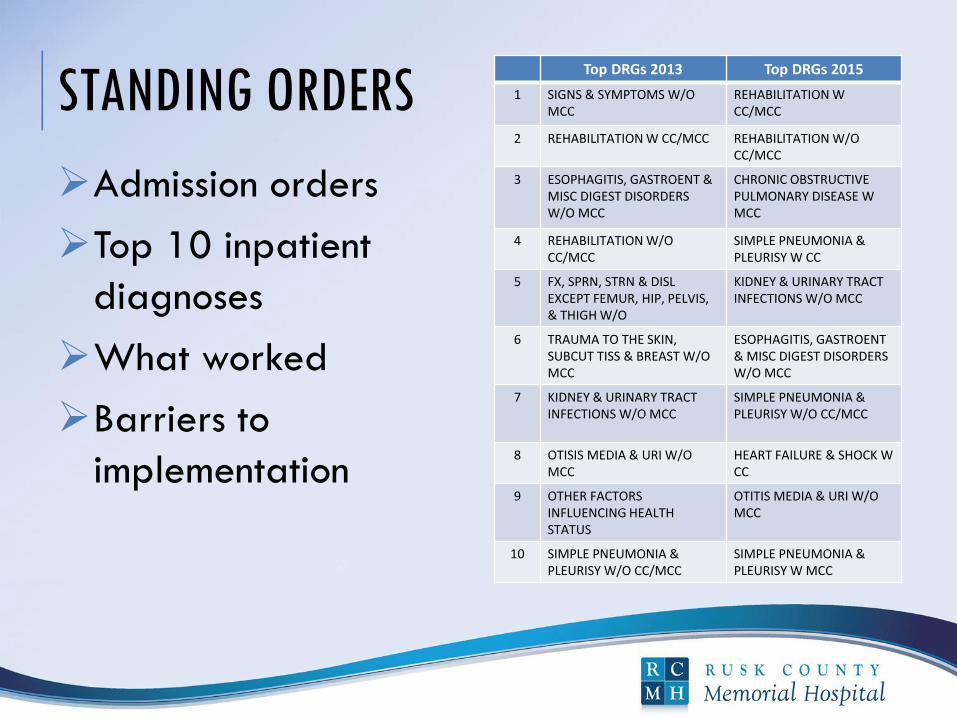
STANDING ORDERS
Admission orders
Top 10 inpatient
diagnoses
What worked
Barriers to
implementation
Top DRGs 2013 Top DRGs 2015
1 SIGNS & SYMPTOMS W/O MCC
REHABILITATION W CC/MCC
2 REHABILITATION W CC/MCC REHABILITATION W/O CC/MCC
3 ESOPHAGITIS, GASTROENT & MISC DIGEST DISORDERS W/O MCC
CHRONIC OBSTRUCTIVE PULMONARY DISEASE W MCC
4 REHABILITATION W/O CC/MCC
SIMPLE PNEUMONIA & PLEURISY W CC
5 FX, SPRN, STRN & DISL EXCEPT FEMUR, HIP, PELVIS, & THIGH W/O
KIDNEY & URINARY TRACT INFECTIONS W/O MCC
6 TRAUMA TO THE SKIN, SUBCUT TISS & BREAST W/O MCC
ESOPHAGITIS, GASTROENT & MISC DIGEST DISORDERS W/O MCC
7 KIDNEY & URINARY TRACT INFECTIONS W/O MCC
SIMPLE PNEUMONIA & PLEURISY W/O CC/MCC
8 OTISIS MEDIA & URI W/O MCC
HEART FAILURE & SHOCK W CC
9 OTHER FACTORS INFLUENCING HEALTH STATUS
OTITIS MEDIA & URI W/O MCC
10 SIMPLE PNEUMONIA & PLEURISY W/O CC/MCC
SIMPLE PNEUMONIA & PLEURISY W MCC
EARLY IMPLEMENTATION SUCCESSES &
CHALLENGES Successful recruiting
NP projected growth: 28% from 2012-2022
One of 3 had delay in obtaining WI license and DEA number
Old EMR increased documentation time/challenge for implementing clinical pathways
Nursing staff not familiar with more acute patients
Wisconsin Hospital Association (2015) Wisconsin Health Care Workforce 2014 Report. Retrieved from http://www.wha.org/Data/Sites/1/pubarchive/reports/2014WorkforceReport.pdf
EARLY IMPLEMENTATION SUCCESSES &
CHALLENGES
Equipment Needs
Evaluate current equipment
Need for additional equipment for higher acuity
patients
May need more BiPap equipment
More telemetry for higher acuity patients
Ventilator
Respiratory equipment
EARLY IMPLEMENTATION SUCCESSES &
CHALLENGES
Educational needs
Assessment of higher acuity patients
Tertiary care nurse educator provided 2-day
educational sessions
Working with a chest tube patient
Care of the pediatric population
High volume back up plan
Difficulty finding part-time providers to fill in for
illness

YEAR ONE OUTCOMES
Patient satisfaction
Quality improvements
CMI : Heart Failure
Stabilize market share
Patient continuity for
the clinic start up
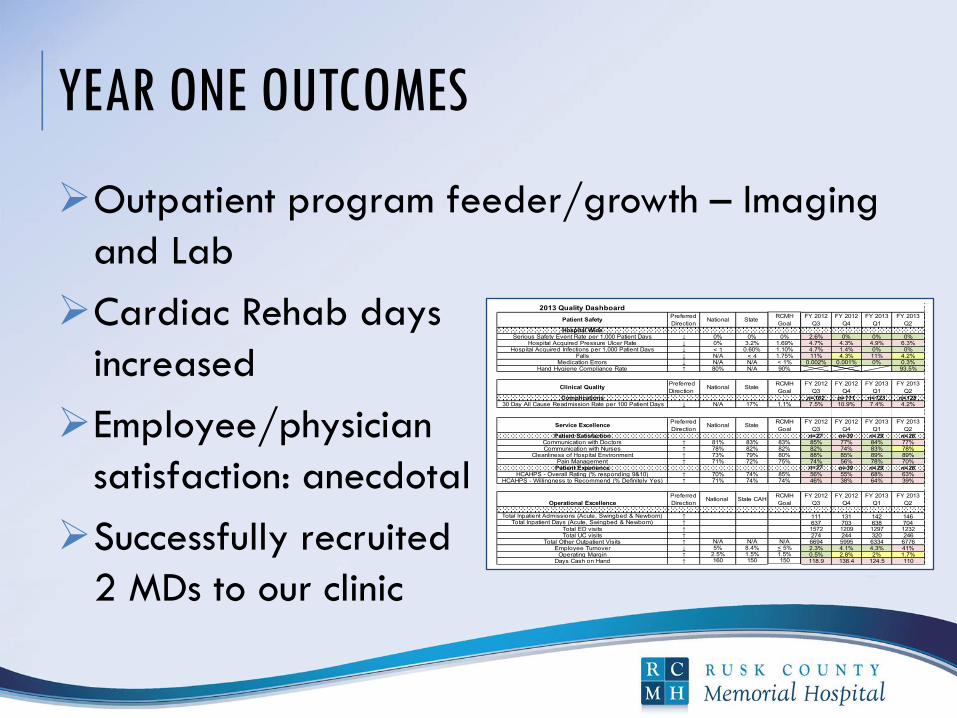
YEAR ONE OUTCOMES
Outpatient program feeder/growth – Imaging
and Lab
Cardiac Rehab days
increased
Employee/physician
satisfaction: anecdotal
Successfully recruited
2 MDs to our clinic
2013 Quality Dashboard
Hospital WideSerious Safety Event Rate per 1,000 Patient Days ↓ 0% 0% 0% 2.6% 0% 0% 0%
Hospital Acquired Pressure Ulcer Rate ↓ 0% 3.2% 1.69% 4.7% 4.3% 4.9% 6.3%Hospital Acquired Infections per 1,000 Patient Days ↓ < 1 0.60% 1.10% 4.7% 1.4% 0% 0%
Falls ↓ N/A < 4 1.75% 11% 4.3% 11% 4.2%Medication Errors ↓ N/A N/A < 1% 0.002% 0.001% 0% 0.3%
Hand Hygiene Compliance Rate ↑ 80% N/A 90% 93.5%
Complications n=102 n=111 n=123 n=128 30 Day All Cause Readmission Rate per 100 Patient Days ↓ N/A 17% 1.1% 7.5% 10.9% 7.4% 4.2%
Patient Satisfaction n=27 n=39 n=29 n=26Communication with Doctors ↑ 81% 83% 83% 85% 77% 84% 77%Communication with Nurses ↑ 78% 82% 82% 82% 74% 83% 78%
Cleanliness of Hospital Environment ↑ 73% 79% 80% 88% 85% 89% 89%Pain Management ↑ 71% 72% 75% 74% 56% 78% 70%
Patient Experience n=27 n=39 n=29 n=26HCAHPS - Overall Rating (% responding 9&10) ↑ 70% 74% 85% 56% 55% 68% 63%
HCAHPS - Willingness to Recommend (% Definitely Yes) ↑ 71% 74% 74% 46% 38% 64% 39%
Total Inpatient Admissions (Acute, Swingbed & Newborn) ↑ 111 131 142 146Total Inpatient Days (Acute, Swingbed & Newborn) ↑ 637 703 638 704
Total ED visits ↑ 1572 1209 1297 1232Total UC visits ↑ 274 244 320 246
Total Other Outpatient Visits ↑ N/A N/A N/A 6694 5995 6334 6776Employee Turnover ↓ 5% 8.4% < 5% 2.3% 4.1% 4.3% 41%
Operating Margin ↑ 2.5% 1.5% 1.5% 0.5% 2.8% 2% 1.7%Days Cash on Hand ↑ 160 150 150 118.9 138.4 124.5 110
Patient SafetyPreferred
DirectionNational
FY 2012
Q3
FY 2012
Q4
Clinical QualityPreferred
DirectionNational State
RCMH
Goal
Operational Excellence
Preferred
DirectionNational State CAH
RCMH
Goal
Service ExcellencePreferred
DirectionNational State
RCMH
Goal
FY 2013
Q1
FY 2013
Q2
FY 2012
Q4
State RCMH
Goal
FY 2013
Q2
FY 2012
Q3
FY 2012
Q4
FY 2013
Q1
FY 2012
Q3
FY 2012
Q4
FY 2013
Q1
FY 2013
Q2
FY 2013
Q1
FY 2013
Q2
FY 2012
Q3
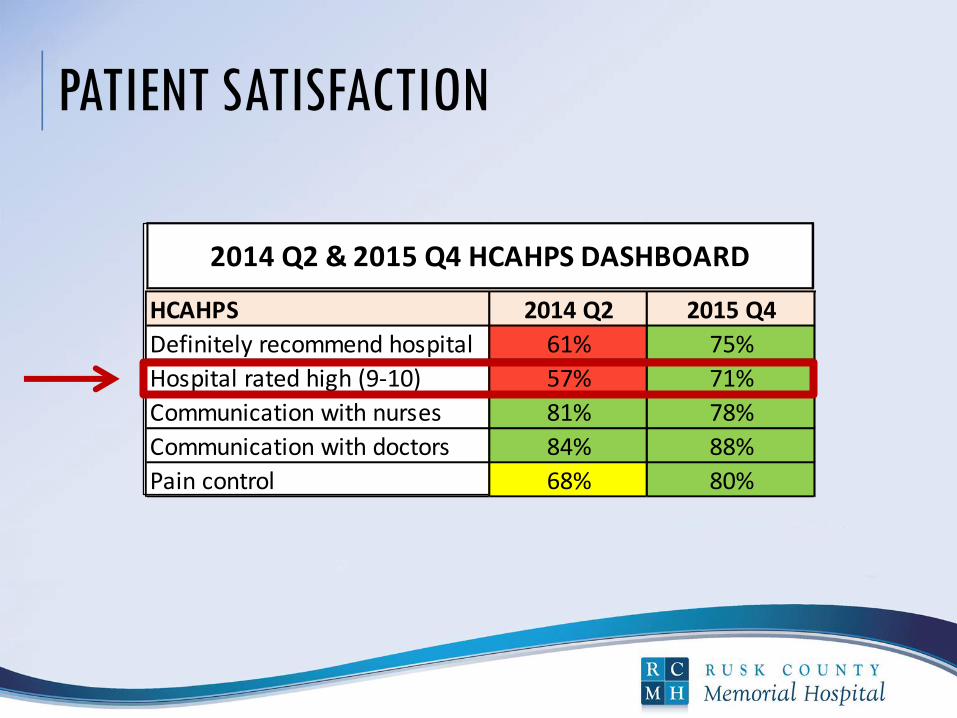
PATIENT SATISFACTION
HCAHPS 2014 Q2 2015 Q4
Definitely recommend hospital 61% 75%
Hospital rated high (9-10) 57% 71%
Communication with nurses 81% 78%
Communication with doctors 84% 88%
Pain control 68% 80%
2014 Q2 & 2015 Q4 HCAHPS DASHBOARD
QUALITY IMPROVEMENTS:CORE MEASURES
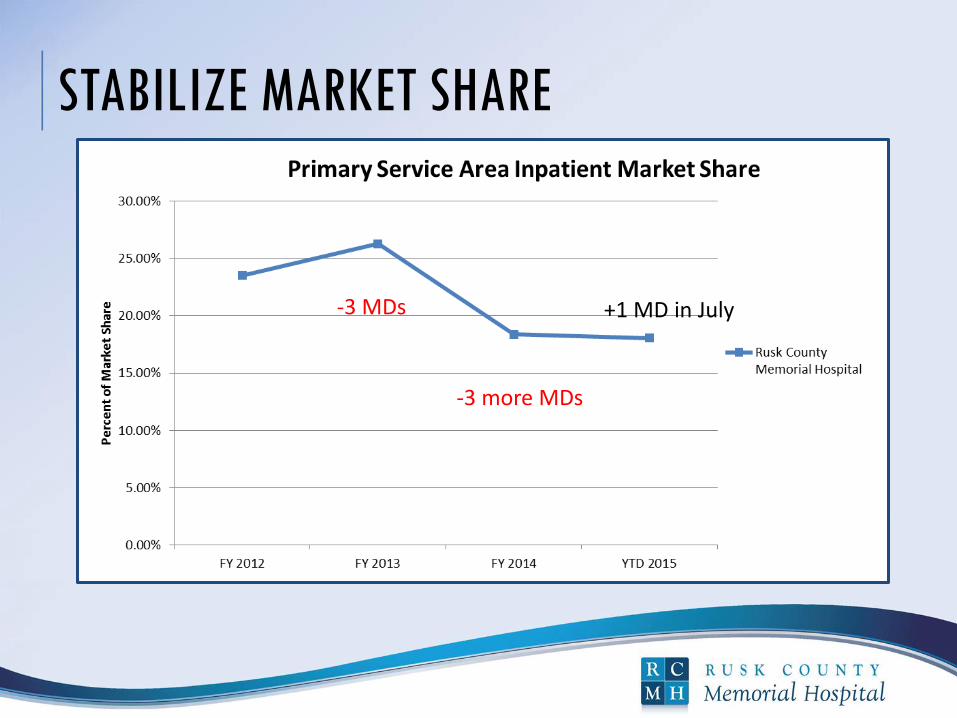
STABILIZE MARKET SHARE
-3 MDs
-3 more MDs
+1 MD in July
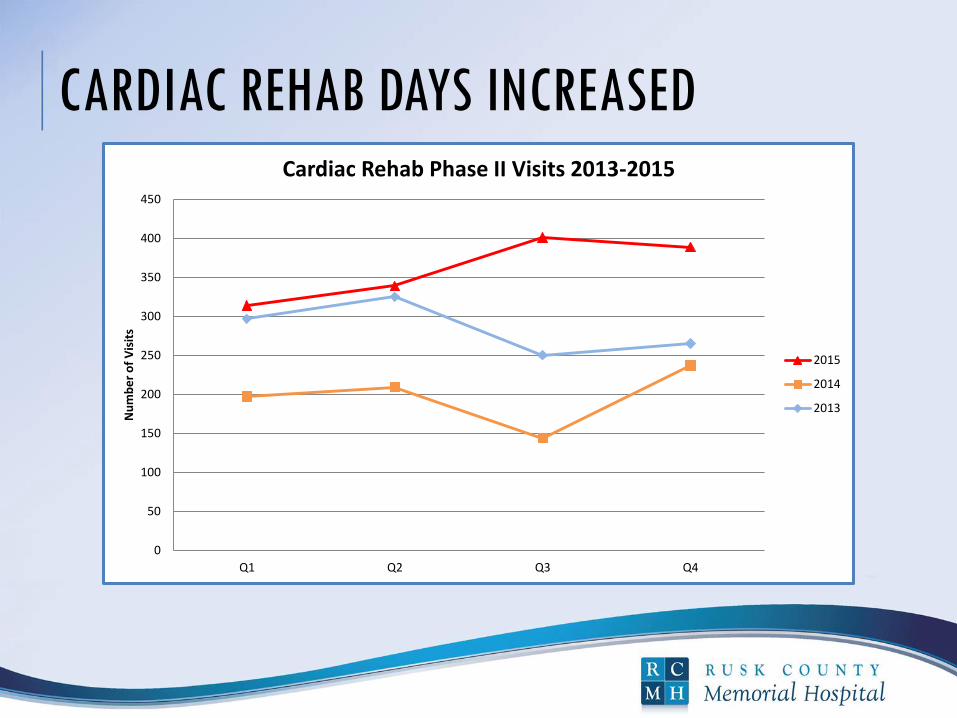
CARDIAC REHAB DAYS INCREASED
0
50
100
150
200
250
300
350
400
450
Q1 Q2 Q3 Q4
Nu
mb
er
of
Vis
its
Cardiac Rehab Phase II Visits 2013-2015
2015
2014
2013
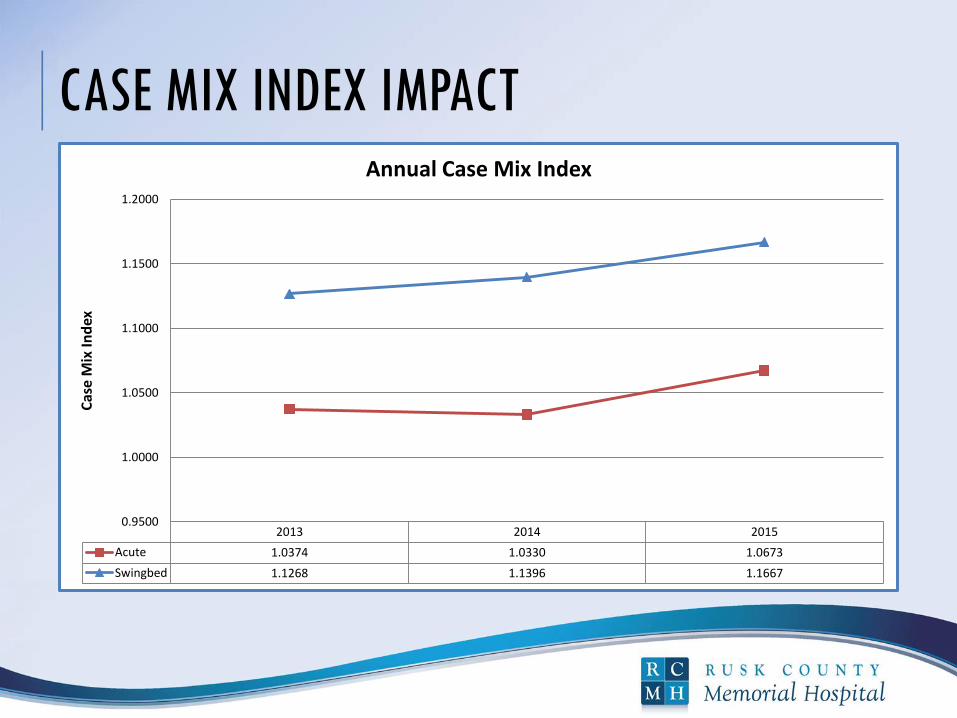
CASE MIX INDEX IMPACT
2013 2014 2015
Acute 1.0374 1.0330 1.0673
Swingbed 1.1268 1.1396 1.1667
0.9500
1.0000
1.0500
1.1000
1.1500
1.2000
Cas
e M
ix I
nd
ex
Annual Case Mix Index
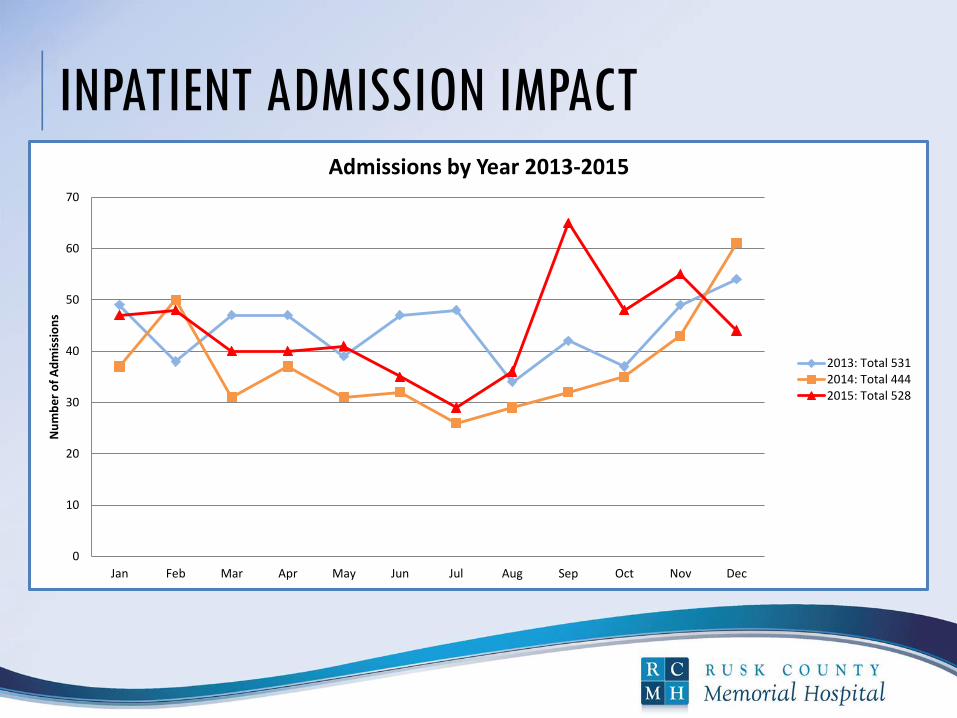
INPATIENT ADMISSION IMPACT
0
10
20
30
40
50
60
70
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Nu
mb
er
of
Ad
mis
sio
ns
Admissions by Year 2013-2015
2013: Total 5312014: Total 4442015: Total 528
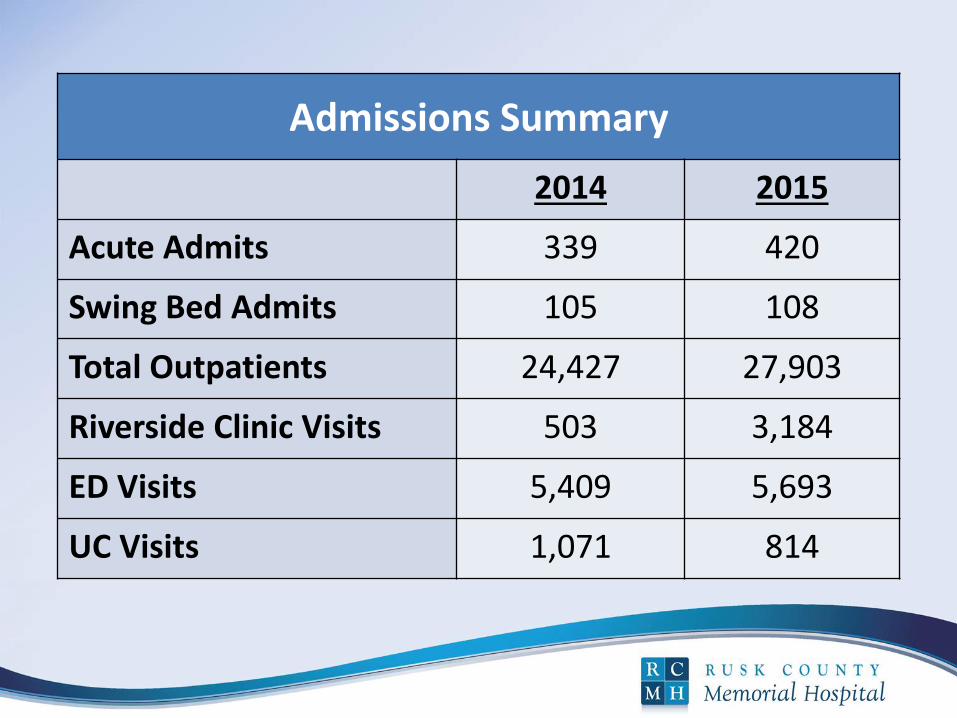
Admissions Summary
2014 2015
Acute Admits 339 420
Swing Bed Admits 105 108
Total Outpatients 24,427 27,903
Riverside Clinic Visits 503 3,184
ED Visits 5,409 5,693
UC Visits 1,071 814
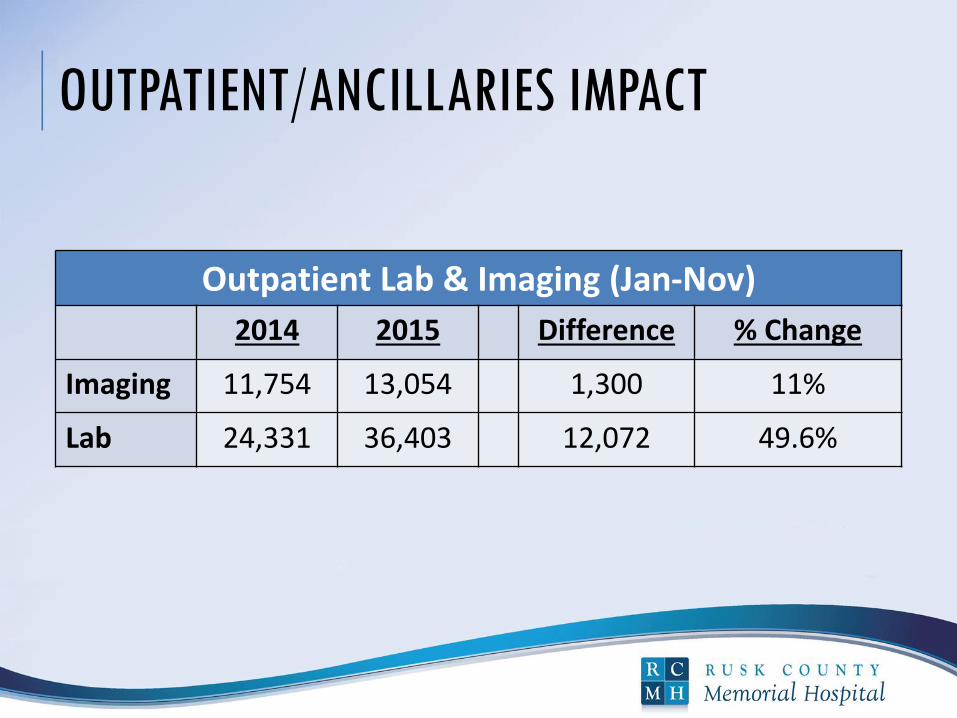
OUTPATIENT/ANCILLARIES IMPACT
Outpatient Lab & Imaging (Jan-Nov)
2014 2015 Difference % Change
Imaging 11,754 13,054 1,300 11%
Lab 24,331 36,403 12,072 49.6%
PHASE TWO: NEEDS OF A GROWING PROGRAM
Respiratory Therapy added
Patient Navigator added (RN)
Daily operations handoff 0730 with Hospitalist,
ED, collaborator and nursing
PHASE TWO: NEEDS OF A GROWING PROGRAM
Role delineation between hospitalists and
nurses/skills assessment
Rehiring APN for cultural fit
Increasing part time staff for back up support
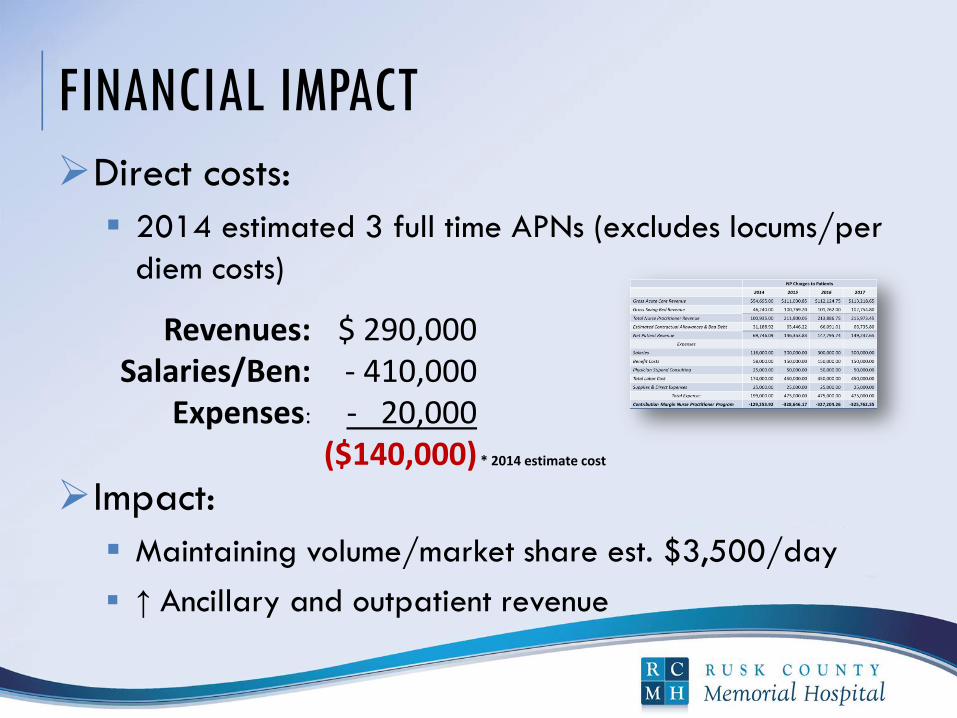
FINANCIAL IMPACT
Direct costs:
2014 estimated 3 full time APNs (excludes locums/per
diem costs)
Impact:
Maintaining volume/market share est. $3,500/day
↑ Ancillary and outpatient revenue
$ 290,000 - 410,000 - 20,000
($140,000)
Revenues: Salaries/Ben:
Expenses:
* 2014 estimate cost
WHAT WOULD WE DO DIFFERENTLY?
Clinical pathways completed
and in place
Anticipate increased acuity
Anticipate new equipment
needs
Back up staffing plan for
illness/unanticipated gaps
CMO on the leadership team
Ridgley, S. K. (2015, March 12) Presentation preparation—The second P. (Web log content). Retrieved from http://www.ihatepresentations.com/presentation-preparation-second-p/
OUR CONSIDERATIONS
Did we capture appropriate admissions?
Do our physicians support the program?
Has the call burden decreased?
Were we able to recruit MDs with a Hospitalist
Program?
Did we establish the clinic?

LESSONS LEARNED
KEY factors in program design:
Medical staff support and transition plan
Staffing model
Physician champion
Collaborating physicians/APN relationship
APN experience vs credential
Medical/legal risk tolerance
State laws

LESSONS LEARNED
Disengagement of other primary care providers
Backup support plan for illness, high census,
burnout
Cultural fit and teamwork among hospitalist
group and others
Keeping pace with growing demand
Sharing with others creates new knowledge
SUMMARY: OBJECTIVES MET APN hospitalist models in a rural setting
Multiple models to fit organization/MD expectations
Cultural engagement by medical staff and others Positive when collaborating toward agreed upon
model
Effect on quality, patient satisfaction and operations Quality & satisfaction exceeded with positive $$
impact
Regulatory requirements for start up Vary by state rules and Med staff bylaws

GOOD THINGS TAKE TIME
REFERENCES
Doescher, M.P., Skillman, S.N. &Rosenblatt, R.A. (2009) The Crisis in Rural Primary Care (Policy
Brief). WWAMI Rural Health Research Center.
Haering, J. (2015, July 31). Why having a physician advisor is a good idea. (Web log content).
Retrieved from http://blog.resonantadvisor.com/why_physician_advisor
Institute of Medicine. (2010). The future of nursing: Leading change, advancing health.
Retrieved from http://books.nap.edu/openbook.php?record_id=12956&page=R1
Pratt, S. (2015, March 18). 3 Steps to help you become the perfect candidate. (Web log content).
Retrieved from http://www.socialtalent.co/blog/page/23
Ridgley, S. K. (2015, March 12) Presentation preparation—The second P. (Web log content).
Retrieved from http://www.ihatepresentations.com/presentation-preparation-second-p/

REFERENCES (CONT.)
Robert Wood Johnson Foundation, & University of Wisconsin Population Health Institute (2015).
Retrieved from http://www.countyhealthrankings.org/sites/default/files/state/downloads/
2015%20Health%20Outcomes%20-%20Wisconsin.png
Society of Hospital Medicine. Nurse practitioners and physician assistants: The role of nurse
practitioners and physician assistants in hospital medicine (2015). Retrieved from
http://www.hospitalmedicine.org/Web/Membership/Nurse_Practitioners_and_Physician_Assi
stants/Web/Membership/non_physician/NP_PA/role_of_nurse_practitioners_and_physician_
assistants.aspx

REFERENCES (CONT.)
Stiefel M, Nolan K. (2012). A Guide to Measuring the Triple Aim: Population Health, Experience of Care,
and Per Capita Cost. IHI Innovation Series white paper. Cambridge, Massachusetts: Institute for
Healthcare Improvement
Wachter, R. M. and Goldman, L. The Emerging Role of Hospitalist in the American Healthcare System;
New England Journal of Medicine (1996) 335: 514-7.
Wisconsin Hospital Association (2015). Retrieved from http://www.wha.org/pubArchive/
special_reports/RH2015review.pdf
Wisconsin Hospital Association (2015) Wisconsin Health Care Workforce 2014 Report. Retrieved from
http://www.wha.org/Data/Sites/1/pubarchive/reports/2014WorkforceReport.pdf
Wis. Stat. §35.93, Ch. N 8