Embed Size (px)
Citation preview

Granulocyte TransfusionOleksandr Kravtsov, MD
PGY-I09/24/2015

ObjectivesHistory of granulocyte transfusion developmentIndications and clinical efficacyGranulocyte collection, processing and storageAdministration of the transfusion and determining
responseComplicationsRING study


Normal individuals produce approximately 6x1010 granulocytes/day.
Their half-life in the peripheral blood is only 6-7 hours.These cells cannot be stored for more than a few hours, as they
rapidly lose viability.Granulocytes need to be collected and transfused on a daily basis
ASAP (within 24 hours).Collection of adequate numbers of viable, functional granulocytes
was almost impossible before the invention of continuous flow apheresis blood collection devices in the late 1960s.

IndicationsMinimal criteria:●Absolute neutrophil count <500 cells/microL, except in the case of chronic granulomatous disease.●Evidence of bacterial or fungal infection (ie, clinical symptoms of infection, positive cultures, pathological diagnosis of infection from biopsies, radiographic evidence of pneumonia).●Unresponsiveness to antimicrobial treatment for at least 48 hours (except in extreme circumstances with life-threatening infection).●Anticipated future recovery of bone marrow function.

IndicationsNeutropenia from chemotherapy, hematopoietic cell
transplantation, aplastic anemia, when anticipated G-CSF response is poor
In patients with chronic granulomatous disease who continue to deteriorate under maximum antimicrobial therapy
Neonatal sepsis



First devices permitted the collection of only 1 x 1010 granulocytes during a 6-7 hour apheresis collection.
Corticosteroids were used to increase the donor's circulating granulocyte count.
Hydroxyethyl starch added to the donor's blood as it entered the centrifuge bowl.
With these improvements, collection of 2 to 3 x 1010 cells/unit was achieved.
A number of clinical trials were performed from 1972 to 1982, that yielded mixed results.
History

6 reports showed favorable responses to GTX, with 59-88% survival in patients receiving GTX, compared with 20-36% in control subjects.
In 1982, a randomized controlled clinical trial of therapeutic GTX was conducted in patients with gram-negative sepsis, which showed no benefits among treated patients.
The dosages of granulocytes used in the study were far too low, averaging one-half of the minimally acceptable dose of 1 x 1010 cells per transfusion.
As early as 1975, it had been reported that patients with good clinical responses received four times as many granulocytes as patients with poor responses.

Meta-analyses of clinical trials of GTX suggested that higher doses were provided in the studies showing clinical efficacy.
G-CSF causes a rapid increase in the granulocyte count that begins within two hours and peaks at approximately 12 hours after administration.

By stimulating donors with a combination of G-CSF and dexamethasone, collection of 5 to 10 x 1010 granulocytes at one sitting became possible.
Neutrophils collected after the administration of G-CSF appear to be of better quality.

RING studyThe Resolving Infection in people with Neutropenia with
Granulocytes (RING) trial was a randomized, controlled clinical trial designed to test the efficacy of transfusing G-CSF-stimulated granulocytes in patients with neutropenia and severe infection.
14 clinical sites participated (including Froedtert).Subjects eligible for the study were those with neutropenia
(ANC<500) and proven/probable/presumed bacterial or fungal infection.

Subjects were randomized to receive either:
1) standard antimicrobial therapy; 2) standard antimicrobial therapy plus daily granulocyte
transfusions from normal donors stimulated with G-CSF (450µg) and dexamethasone (8mg).
The primary endpoint was a composite one: survival plus a microbial response, both evaluated 42 days after randomization.

Response for bloodstream infections was defined as a negative blood culture.
For invasive bacterial or fungal infections, response was defined as resolution or improvement of clinical evidence of infection.
A stable infection was considered to be a failure.Subjects were excluded from the study if they were unlikely
to survive 5 days or if there was evidence that the patient was unlikely to be neutropenic for at least 5 days.

Secondary objectivesPrimary outcome within each infection subgroupThe frequency and nature of granulocyte transfusion
reactionsThe overall incidence of adverse effectsMortality through 3 months.

Statistical considerationsThe target sample size of 118 subjects per arm would provide
80% power to detect a treatment difference if the true success rate with antimicrobial therapy alone was 50%, and the true success rate with the granulocyte treatment arm was 70%.
Only 58 patients were recruited to the control arm and 56 - to the granulocyte transfusion arm.
The study was terminated short of the desired enrollment because of time limits on the funding of the TMH Clinical Trials Network.



Mild to moderate (grade 1-2) transfusion reactions were seen after one or more transfusions in 41% of subjects or 28% of the transfusions overall.
More severe (grade 3-4) reactions were seen after at least one transfusion in 20% of subjects (n=10, <5% of the overall transfusions).
These included hypoxia (n=7), tachycardia (n=1), hypotension (n=1), and an allergic reaction (n=1).
One subject experienced a grade 4 reaction (hypoxia) requiring temporary ventilatory support.
Out of 307 transfusions, transfusion reactions occurred in 32 of 116 (27.6%) low dose transfusions and 68 of 191 (35.6%) high dose transfusions.
Complications

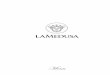
Primary Outcome Success Stratified by Infection

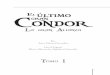
Day 42 Survival Status Stratified by Infection

Primary outcome success was 59%, 15%, and 37% for the high dose, low dose, and control groups, respectively.
Subjects who received the higher granulocyte dose fared substantially and statistically significantly better than those receiving the lower dose, both in terms of primary outcome and survival (p<0.01 and p=0.02, respectively).
Subjects in the control group did better than subjects in the low dose group, and worse than subjects in the high dose group, but these differences were not statistically significant.
Dose effect

Limitations of the studyClinically positive effect might been missed by chance
due to the low enrollment/lost subjects. The power of this study to detect a 20% difference in the overall success rates was reduced to approximately 40%.
Some clinicians/patients/relatives were convinced that granulocytes were efficacious and did not want to risk randomization to the control group.
Some were convinced that granulocytes were too dangerous and likely to be detrimental to the patient.

Limitations of the studyMore than a quarter of the subjects received a mean GCN
dose less than the goal of 0.6 x 109 cells/kg for a 70 kg subject, often substantially less.
Patients eligible for the study may not have been those for whom the clinician would normally consider granulocyte transfusions.

Key pointThis study failed to provide the definitive answer on the
efficacy of high dose granulocyte transfusion therapy, although secondary analyses do provide suggestive evidence that there may be efficacy if higher doses are actually delivered to the patient.