Embed Size (px)
Citation preview
Kindly supported by
by David Furness and Barney Gough
Reforming the NHS for an age of austerity
FROM FEAST TO FAMINE
The SMF Health Project Final Report
First puBlisheD By The Social Market Foundation, July 2009ISBN: 1-904899-68-4
11 Tufton Street, London SW1P 3QBCopyright © The Social Market Foundation, 2009The moral right of the authors has been asserted. All rights reserved. Without limiting the rights under copyright reserved above, no part of this publication may be reproduced, stored or introduced into a retrieval system, or transmitted, in any form or by any means (electronic, mechanical, photocopying, recording, or otherwise), without the prior written permission of both the copyright owner and the publisher of this book.
the social Market FounDationThe Foundation’s main activity is to commission and publish original papers by independent academic and other experts on key topics in the economic and social fields, with a view to stimulating public discussion on the performance of markets and the social framework within which they operate.
The Foundation is a registered charity and a company limited by guarantee. It is independent of any political party or group and is financed by the sale of publications and by voluntary donations from individuals, organisations and companies. The views expressed in publications are those of the authors and do not represent a corporate opinion of the Foundation.
chairManDavid Lipsey (Lord Lipsey of Tooting Bec)
MeMBers oF the BoarDViscount (Tom) ChandosGavyn DaviesDavid EdmondsDaniel FranklinMartin IvensGraham MatherBrian Pomeroy
DirectorIan Mulheirn
DesiGn anD proDuctionSoapBox
printeD ByWindsor Print Productions Limited
CONTENTS
contents
Acknowledgments 4
About the authors 5
Executive Summary 6
1 Introduction - A Social Market Approach
to Healthcare 31
part one
2 Equity in the Health System 42
3 Paying for Healthcare 72
4 National Standards and Governance 113
part two
5 Decentralisation 131
6 Commissioning Healthcare 152
7 Accountability in a Local System 209
8 Regulating a Local System 229
9 Conclusion 252
SOCIAL MARKET FOUNDATION
4
acknowleDGMents
This project would not have been possible without the generous
support of Bupa, Standard Life Healthcare, Pfizer and NHS
Connecting for Health.
The authors would like to thank the members of the SMF Health
Project Steering Group for their invaluable advice and guidance
throughout the duration of the project: Dr David Colin-Thomé,
Professor Angela Coulter, Dr Tim Crayford, Nigel Edwards, Chris
Exeter, Fergus Kee, Paul Lynes, Ben Page, Professor Peter Smith, Nick
Timmins and Richard Torbett.
Special thanks are also due to Mark Bassett, Helen Vaughan
Jones and Julian Ross.
The authors would also like to thank Jonathan Nicholls and
Chloe Smith at Ipsos MORI for their contribution to our work.
Additional thanks to all those who have contributed their time
and thoughts to shaping this report. Special thanks are due to those
experts and practitioners who gave up their time in interviews and
seminars, providing us with evidence, ideas and challenges – in
particular, David Stout and Don Redding.
Finally, we would like to thank colleagues at the Social
Market Foundation who have assisted us along the way. Thanks
are particularly due to Ian Mulheirn, Natalie Tarry, Jessica Griffith
Prendergrast and Dr Simon Griffiths.
While this publication has benefited enormously from the input
of many different people, any errors and omissions remain the sole
responsibility of the authors.
FROM FEAST TO FAMINE
5
aBout the authors
DaviD Furness
David joined the SMF as Health Project Leader in January 2007.
Since then his work has focused on the future of the NHS. David
has co-authored five background papers dealing with all aspects
of healthcare reform, as well as co-edited a special publication
bringing together leading voices to comment on the future of the
NHS at its 60th anniversary. His most recent publication was “Local
control and local variation in the NHS: what do the public think?”
He has also contributed to publications including Health Service
Journal and has spoken at various conferences and events. Prior to
joining the SMF he worked for Standard Life Healthcare, one of the
UK’s leading private health providers.
Barney GouGh
Barney joined the SMF as a researcher in March 2006. He co-
authored and edited a number of publications before working on
the SMF Health Project. Barney has co-authored five background
health papers and a publication examining public attitudes towards
the health service, and has co-edited an NHS 60th anniversary
collection. Barney took his BA in Social and Political Sciences at
Emmanuel College, Cambridge University.
SOCIAL MARKET FOUNDATION
6
executive suMMary
Britain is in the midst of a severe economic recession which
has ripped a deep hole in the public finances. A significant and
sustained public spending squeeze is inevitable and will hit the
NHS hard. Even if the NHS budget is maintained in real terms over
the next decade, rising workforce costs will mean that frontline
services will feel the pinch. Meanwhile, demographic changes
over the next ten years will see an ageing population stretch the
services the NHS provides as never before.
This presents a massive challenge to health policymakers and
begs the question that underpins this report: how best can a
quality health service be maintained over the next decade in the
context of a severe funding squeeze?
The task facing the health service in England is huge. Failure
to achieve greater efficiency and productivity may mean that the
entire post-war settlement of healthcare funding and provision will
be undone. To maintain support for the current system, the public
must be convinced that what is offered by state services is of a
high quality. And healthcare providers face a stiff task in achieving
continuing quality improvements at a time of rising government
debt, rising taxes and falling investment in public services.
Confronted with the dual dilemma of reduced funding and
increased demand, it may be tempting to look to the experience of
other countries and suggest that the NHS should be overhauled and
rebuilt as a system of social insurance, based on the perception that
such systems deliver better performance and increased efficiency.
But however appealing this may seem it is neither plausible nor
sensible. First, there is little evidence that social health insurance
performs much better than tax-funded systems. Indeed, many
European countries, including France and Germany, spend a greater
proportion of their GDP on healthcare than the UK does. Second,
FROM FEAST TO FAMINE
7
attempting such a transformation would be an enormous policy
gamble. While some systems have moved from an insurance-based
model to one that is predominantly tax-funded, there has never
been an example of a change in the opposite direction.1
Introducing a system of social insurance would require a total
structural overhaul, which must be avoided. Structural upheaval
has characterised healthcare reform in England over the last ten
years and more of the same is not the way to a stable, efficient
and quality service. Instead, the task of achieving good value
for money and equipping the health system to deal with the
substantial challenges it faces must be met without throwing out
the structures that already exist.
So, with large scale structural change ruled out, what options
remain to safeguard quality provision within the NHS in the next
decade? Two strategies will be key to success: improving efficiency
and introducing a mechanism to constrain the inexorable growth
in demand.
a local health service
If the necessary efficiency savings and cuts in services are to
be achieved then power must be devolved away from central
government to local commissioners. Difficult decisions about
healthcare services must be removed from the national level
if rational decisions are to be made and explained to service
users and understood and accepted by them. Without such
depoliticisation, populist demands risk skewing the priorities of the
NHS. Responsibility for decommissioning services must therefore
be placed in the hands of local commissioners, who will be able to
allocate resources with the best possible knowledge of local needs,
and make the case for change to people at a local level. But for this
1 D. G. Green et al., “For and Against: Social Insurance – The Right Way Forward for Health Care in the United
Kingdom?” British Medical Journal (International Edition) 325:7362 (2002).
SOCIAL MARKET FOUNDATION
8
to succeed, accountability structures in the health system will have
to change to reflect this shift in responsibility and power. Local
people must be able to hold commissioners to account if primary
care trusts (PCTs) are to have sufficient legitimacy to make tough
decisions that will be necessary over the next decade.
Granting autonomy to local commissioners will also improve
the efficiency and quality of services by stimulating innovation in
service delivery and allowing appropriate local services to develop.
Additionally, inappropriate utilisation of healthcare can be reduced
through high quality commissioning that can help to manage
referrals from primary care, thus reducing overall demand. Local
choice and local variation must become the guiding principles of
the health system, with central government playing a significantly
reduced role, primarily guaranteeing standards and patients’ rights.
allocating scarce resources
But empowering local commissioners to improve the use of existing
resources alone will not be enough to secure the future of the
NHS over the next ten years. One option is to introduce additional
charges in an attempt to raise extra revenue for the health service.
However, revenue raising charges soon run into serious ethical
problems, due to the fact that to raise money charges have to
either impact on the poor and the long-term ill, or have to be set at
a very high level; neither of which is a satisfactory situation.
It is clear, therefore, that charging to raise money is not a
plausible option. But what is also clear is that with the spending
tap closed, rationing of some sort is unavoidable. This fact must be
confronted head-on in a strategic manner otherwise rationing by
the backdoor will undermine the NHS. If nothing is done about the
need to ration healthcare in some way, then we will see a return to
the days of rationing by waiting list, crumbling infrastructure and
a poor quality service. Such a route cannot be countenanced as it
would ultimately destroy the NHS with higher income members of
FROM FEAST TO FAMINE
9
society opting to pay for private treatment instead of being treated
by the NHS. This would weaken support for a universal, tax funded
system, leaving behind a poor quality health service for those who
cannot afford to pay their way out.
The question, then, must be how to ration while safeguarding key
principles of equity and universalism, and maintaining a high quality
service. What is needed is a mechanism to encourage people to ration
themselves: a limited demand management tool that is consistent
with protecting the quality of the NHS and ensuring continued
middle-class buy in. Introducing limited charges for those who can
afford to pay, solely as a demand management tool, is the most likely
route to achieve this goal. Any form of charging is unpalatable, but if
designed correctly, with a fairly low charge and a total exemption for
those who cannot afford to pay, charges are the progressive option
which will help to safeguard the NHS for everyone.
To deal with the challenge described above, this report sets out
a number of recommendations that are detailed below.
recoMMenDations
equity (chapter 2)
Perhaps the most important criteria that healthcare systems
must fulfil is that they are fair. Equity in the NHS should be about
providing equal access for equal need in health services.
recommendation 1: central to the concept of equity in the
nhs should be a definition of equal access to equal need.
This will mean that health inequalities no longer form part
of the resource allocation formula applied by the NHS, with the
SOCIAL MARKET FOUNDATION
10
focus shifting instead to providing equal access to treatment for
equal need.
Health inequalities are so important that rather than being the
responsibility of the NHS, they should be overseen by the whole of
government. Government action to deal with health inequalities
should be joined up, with the NHS only one part of a wider agenda.
recommendation 2: a cabinet office minister for health
inequalities should be introduced with responsibility for
co-ordinating action across government to narrow the
gap in health within the population.
Equity is an essential principle for health services but there are
many different definitions of equity that support a range of different
types of health service. There is a need for a defined set of NHS
values that reflect a new understanding of the role and capacity of
health services. The NHS values must reflect a realistic assessment
of the need to maintain universal access in a time of scarcity, with
an open acknowledgement that wealthier people may need to pay
more for services if they can afford it. Furthermore, these values
should reflect the local priorities that will be necessary if the NHS is
to manage public expectations and maintain public support for a
tax-funded health system.
recommendation 3:
an nhs set of values should include:
• universal access: no-one is excluded from necessary
treatment because of their ability to pay, but some
people contribute if they can afford to.
FROM FEAST TO FAMINE
11
• a comprehensive range of services: the nhs will
provide a comprehensive range of services that offer
good value for money.
• equal access to treatment: the nhs will make
sure that everyone has equal access to treatment
regardless of age, gender, income or ethnic
background.
• local services for local need: the nhs will provide
a range of services appropriate for different local
areas. pcts will work with local people to decide
what is needed, and to justify the difference
between different areas.
FunDinG (chapter 3)
The cost of healthcare in the developed world has increased
tremendously in recent times, and questions about how best to
fund healthcare is an unending source of controversy. There is
almost no chance that the health system as it is currently designed
will be able to maintain or improve standards of care with the
severe resource constraints that will be in place for the foreseeable
future. However, it is crucial that any alterations to the system of
funding maintain the central principle of fairness.
It is clear that in our society there is a general willingness to
spend money on good health. Spending on alternative medicine
and general health and fitness products in the United Kingdom
is high and is increasing. This does not mean, however, that it is
possible to translate private spending on health into extra revenue
for the NHS. In fact, often patients choose to spend money
on alternative medicine precisely because it is not part of the
conventional health system.
SOCIAL MARKET FOUNDATION
12
Despite this there are some important lessons for the future
of the NHS. Many diverse groups choose complementary and
alternative medicine because it offers a ‘whole person’ service –
something not always found in conventional healthcare settings.
This insight offers PCTs the potential to raise satisfaction rates
with local healthcare services by encouraging a clinical approach
that recognises the importance of treating the whole person, not
simply managing an illness.
recommendation 4: the desire to access ‘holistic’
medical services indicates that pcts could improve
satisfaction rates by offering patients a greater array
of support services to help manage the whole of their
health, not just their illness.
recommendation 5: Gp led health centres should be
promoted as ‘wellness centres’ to engage individuals who
particularly value a holistic service, and counter concerns
that they will lead to a more impersonal form of medical
treatment.
Private spending on healthcare also shows that individuals
value their health and are willing to make a financial commitment
to maintaining it.
recommendation 6: Many individuals are willing to
prioritise their health in financial terms. local and
national decision-makers in healthcare must engage
people in a realistic discussion about adequate levels of
resources in health services.
FROM FEAST TO FAMINE
13
the future of “top-up” payments
The newly changed rules on the use of ‘top-ups’ in the NHS,
following a review by Professor Mike Richards, mean that patients
can now purchase privately drugs not available on the NHS and,
if they are administered privately, continue to receive publicly
funded treatment.
As such, it seems likely that the next decade will see a thriving
market in insurance based products that offer supplements to NHS
care. These will complement existing private medical insurance
products that offer an alternative to the NHS for some treatments.
The rise of such insurance products should not, however,
pave the way for the introduction of a social insurance system of
healthcare in this country. There is simply no evidence that a shift
to social insurance would be a desirable move.
recommendation 7: the nhs should continue to be
funded primarily from general taxation. a move to a
system of social insurance should not be considered by
policymakers over the next decade.
private payments
There are a range of private payment mechanisms that stop short
of social or private insurance models but which if introduced might
contain costs by affecting behaviour or raise revenue.
However, without a significant change in the system of
funding, that would shift the cost from the state to the individual,
it is difficult to see much scope for the NHS to raise money from
individual patients to cover potential NHS budget shortfalls.
SOCIAL MARKET FOUNDATION
14
recommendation 8: new private payments should not
be introduced in an attempt to raise revenue.
recommendation 9: scarce public resources mean that
abolishing existing charges (prescription, dental and
optical) should not be a priority for the nhs. instead,
charges should be reformed so that exemptions are
made on ability to pay, rather than somewhat arbitrary
categories such as retirement and pregnancy. this
should be achieved through the tax credit system.
Demand management
While new charges are not an appropriate method for raising revenue,
could they be used as a rationing mechanism? It is possible to see a
system of limited charges being introduced that safeguard the poor
and the sick while still reducing overall demand for healthcare.
recommendation 10: a limited range of charges,
capped at circa £100 per annum, for initial consultations
with Gps and other primary care practitioners should
be introduced. the charges would be designed to
incentivise wealthy individuals to avoid seeking
unnecessary initial consultations with clinicians. all those
individuals and families in receipt of tax credits would be
exempt from all nhs charges.
national stanDarDs anD Governance (chapter 4)
This report argues that the NHS should be designed around local
needs rather than national standards. This raises the question: if
FROM FEAST TO FAMINE
15
commissioners represent the heart of the NHS, what role is left for
national government?
While local health commissioners require greater autonomy in
order to improve health services there is still an important role for
national standards, management and political control in healthcare
in the years ahead.
recommendation 11:
the following roles should continue to be undertaken at
a central level:
1. setting the basic framework for health policy.
2. Making strategic decisions on the development of
health resources.
3. regulation concerning public safety.
4. Monitoring, assessment and analysis of the health of
the population and healthcare provision.
However, the number of centrally set national standards and targets
should be substantially reduced in order to free up commissioners to
innovate locally and design services that meet local need.
recommendation 12: the list of national standards and
targets should be substantially reduced to become a
minimum service guarantee.
recommendation 13: national government should
continue to have responsibility for revenue raising,
resource allocation, limited national standards and
defining nhs values.
SOCIAL MARKET FOUNDATION
16
Decentralisation (chapter 5)
Ultimately, any decision to devolve power in a health system is a
political choice that must take into account the country’s political
and historical context. In the case of the health service in England,
the NHS has been subject to a decade of centralised control which
has succeeded in raising activity levels, but which has failed to
improve productivity and has left staff disillusioned. In this context
decentralisation is the best option for improving the quality,
productivity and responsiveness of the health service in a time of
significant fiscal restraint.
However, a balance needs to be struck in which local level
decision-makers have responsibility for a wide range of service
related decisions, while the national level retains core strategic,
revenue raising and regulatory responsibilities.
recommendation 14: political and fiscal decentralisation
is not desirable, but administrative decentralisation
should be extended.
coMMissioninG (chapter 6)
At the heart of a social market approach to healthcare is the idea
that a pluralistic and diverse approach to the delivery of services
is the best way to stimulate innovation and to ensure that those
services suit the needs of local people, thus improving both quality
and efficiency.
Getting commissioning right will be key to squeezing out as
much performance in the health service as possible over the coming
years, in a context of what looks certain to be a much tighter funding
settlement post-2011, coupled with rising health costs.
FROM FEAST TO FAMINE
17
Some commentators have suggested that an integrated
system, such as Kaiser Permanente (KP) in the USA, which combines
commissioning and provision within the same organisation, would
be more successful than doggedly persisting with an internal
market in health. However, there is no indisputable evidence that
a KP-type model would provide better or cheaper care than is
currently achieved in the NHS2. Furthermore, introducing such a
system into England would require a rejection of the purchaser/
provider split and would entail significant structural change.
There is no appetite in the health sector for any more extensive
structural change, so it is essential to get the systems that are in
place working as well as possible.
recommendation 15: the purchaser/provider split should
be maintained and attention should be focused on
improving commissioning performance within existing
structures.
skills
If commissioning is to succeed in driving up quality in the NHS,
the capability, capacity and profile of individuals who work for
commissioning organisations, and the organisations themselves,
need to be strengthened. The world class commissioning
framework sets out 11 useful commissioning competencies.
However, a nationally dictated set of skills and competencies will
not meet all requirements; PCTs will need different skill sets to meet
different needs. As such commissioning skills should be developed
at a local, regional and national level.
2 A. Talbot-Smith et al., “Questioning the Claims From Kaiser”, British Journal of General Practice 415 (2004).
SOCIAL MARKET FOUNDATION
18
recommendation 16: pcts must continually assess the
skills and competencies that they require to successfully
commission at a local level, and then strive to develop
those capabilities.
investment in commissioning skills
Currently there is a cap on the number of personnel a PCT is allowed
to employ. Good local commissioning will only be achieved if PCTs
are enabled to develop their management skills and capacity.
recommendation 17: the cap on pct personnel numbers
should be removed, granting pcts responsibility for
determining their own staffing levels.
professional standards
Commissioners, both as individuals and organisations, would benefit
from the development of mechanisms for increasing their influence,
developing their skills and capabilities, and raising their profile.
However, formal recognition of commissioning as a professional
discipline may not be the best approach. Commissioning is an
organisational responsibility, not an individual task and defining a
standardised qualification or accreditation criteria would be hard
to achieve and could detract from the important task of addressing
specific local development needs.
recommendation 18: a formal set of individual
commissioning competencies should not be developed
for nhs commissioners.
FROM FEAST TO FAMINE
19
While a role is not envisaged for standardised commissioning
qualifications, the voice of commissioners should be strengthened
to enable them to stand up to provider organisations, recruit high
quality staff and stamp their authority on the health service.
recommendation 19: the current pct network should
develop to take on a role similar to a royal college, as a
way of strengthening commissioners in the nhs.
nice
NICE provides commissioners with crucial support and information.
Health minister Ara Darzi has set out an expanded role for NICE, which
is now expected to make more rapid appraisals of new drugs and set
national quality standards.3 This is to be welcomed, but it is important
that NICE appraisals do not end up focusing exclusively on new
pharmaceuticals at the expense of existing devices and procedures.
If commissioners are going to drive out ineffective practice they will
rely on NICE to assess old technologies, as well as new ones, so that
they can commission the most cost-effective treatment.
recommendation 20: the capacity of nice to appraise
existing procedures, as well as new ones, needs to be
strengthened.
The expansion of NICE’s role will require additional resources
which will be hard to find in a time of fiscal consolidation. NICE
has begun to offer consultancy services to foreign governments
and to offer scientific advice to companies seeking to tap into
3 Department of Health, High Quality Care for All: NHS Next Stage Review Final Report, by Ara Darzi (London:
HMSO, 2008).
SOCIAL MARKET FOUNDATION
20
NICE’s experience in health technology assessments.4 Both of these
ventures could provide significant revenue streams for NICE.
recommendation 21: the commercial capacity of nice
to offer consultancy to governments and private sector
companies should be expanded.
integration
The health system in England is far too focused on acute, hospital
based care and there is insufficient collaboration between
healthcare sectors. Integrated care can flourish under the current
system, but it is important that integrated services are allowed
to develop organically at a local level to meet local need, rather
than the Department of Health dictating how integration should
develop and what integrated care models should look like.
recommendation 22: pcts and local providers must
be given the freedom to develop integrated care
organisations at a local level to meet local need.
national contracts
The growth of integrated multidisciplinary organisations that
provide care across sectors will lead to the development of new
professional roles and the need for contracts to reflect new ways
of working. It seems sensible for PCTs to be able to set pay and
working conditions as part of contractual negotiations with
providers. This would lead to the emergence of innovative services
and new clinical roles that meet local need and emerging demand,
and could also lead to better value for money.
4 Richard Robinson, “New Look NICE”, http://www.fleishman-hillard.co.uk/uploads/documents/NewLook.pdf.
FROM FEAST TO FAMINE
21
recommendation 23: national contracts for Gps,
consultants and other medical staff should be abolished,
and renegotiated at a local level when they come up for
renewal.
Joint working
In the future localisation must become the watchword of the
health service, with devolved responsibilities a major driver of
improvement. However, PCTs are geographically too small and
lightly staffed to successfully carry out certain important tasks. As
such PCTs must be encouraged to work together in partnership to
undertake joint commissioning.
At the moment the world class commissioning framework
does not explicitly incentivise PCTs to work together. This must be
changed if joint working is to become a reality.
recommendation 24: competency two of the world
class commissioning assurance Framework should
be re-worded to require pcts to work collaboratively
with local and regional pcts and prevent needless
duplication.
Fesc
The government launched the Framework for procuring External
Support for Commissioners (FESC) to provide PCTs with easy access
to a set of private companies to support them in undertaking
their commissioning functions. However, FESC has transpired to
be a very slow and bureaucratic process. PCTs should be trusted
to purchase support from whichever private sector organisations
they think offer them the services that they need, rather than
SOCIAL MARKET FOUNDATION
22
solely those government approved organisations on the FESC. This
will stimulate the market to innovate and help reduce costs.
recommendation 25: Fesc should be abolished.
public engagement
Involving the public in the design and commissioning of health services
is an important element of ensuring effective local accountability.
To help achieve patient participation Local Involvement Networks
(LINks) have been established to offer a range of different ways for
local people to have a say, both through links with local voluntary
sector organisations and by using a range of techniques for engaging
the public, such as focus groups and surveys.
Currently a LINk has the power to refer an issue to their local council
health Overview and Scrutiny Committee (OSC) which can formally
question, scrutinise and influence the decisions of local NHS bodies.
However, the OSC has no duty to respond to the LINk. This should be
changed to ensure that users have more influence over services.
recommendation 26: oscs should be required to produce
a public response to any referral made by a link.
The world class commissioning framework stresses the
importance of patient and public involvement. The vision for world
class commissioning states that there should be “local ownership and
accountability” for decisions,5 but in reality no PCT is close to achieving
this vision. PCTs must go much further in engaging with local people.
5 Department of Health, “World Class Commissioning”, http://www.dh.gov.uk/en/managingyourorganisation/
commissioning/worldclasscommissioning/index.htm.
FROM FEAST TO FAMINE
23
recommendation 27:
to improve public engagement pcts must:
• Develop a statement of the aims and purposes of
patient and public involvement in their local area
and set out a two year programme to demonstrate
how these aims will be achieved.
• commission research to identify effective strategies
for engaging patients and local people.
• ensure senior managers take public engagement
seriously, providing it with adequate staffing and
resources.
• Dramatically improve their public profile, ensuring
that members of the public know that they exist and
understand what they do.
• change their names to indicate that they are the
nhs body for that area. For example, nhs hull rather
than hull pct.
• launch local information campaigns to clarify how
the health system works at the local level and how
individuals and groups can become involved.
• work hard to recognise when, where and how
members of the public want to be involved and
ensure that as wide a range of the public are
involved as possible.
• ensure that even when the public is happy to leave
decision-making up to the pct the public is still
kept informed about how and why decisions are
made and have a means to give feedback which is
responded to.
But this will not happen spontaneously: a national framework is
needed to kick start the process and ensure that PCTs take patient
and public involvement and engagement seriously.
SOCIAL MARKET FOUNDATION
24
recommendation 28: the Department of health
should develop a national framework to measure and
evaluate the effectiveness of pcts’ public engagement
programmes. the results of the evaluation would feed
into the world class commissioning assurance framework.
practice-based commissioning
Practice-based commissioning (PBC) was introduced in 2004 and
seeks to grant GPs more decision-making power over how NHS
resources are spent and enable them to deliver new services or
commission others to do so. However, PBC is currently not operating
effectively: progress has been slow and in some areas the policy
is grinding to a halt.6 Tens of millions of pounds have been spent
trying to encourage GPs to commission services, but on the whole
there is no great appetite amongst the profession for PBC.
Abandoning PBC would be a blow to those GPs who have
invested a lot of time, energy and resources into developing
organisational structures for PBC to work. So rather than the
Department of Health simply scrapping the policy, where PBC is
succeeding it should be allowed to continue, but the government
should stop spending on incentivising its adoption in practices that
have shown little interest thus far.
recommendation 29: the focus of policy should be on:
strengthening pct commissioners; ensuring clinicians
are closely involved in pct commissioning decisions; and
stimulating a thriving provider market. this will allow
current pBc consortia to evolve into integrated care
6 Natasha Curry et al., Practice-Based Commissioning: Reinvigorate, Replace or Abandon? (London: The King’s
Fund, 2008).
FROM FEAST TO FAMINE
25
organisations focused on providing joined up services,
rather than attempting to both commission and provide
services.
If local commissioners are to become the main drivers of
improvement in the health service the accountability structures
in the health system will have to change to reflect this shift in
responsibility and power. As PCTs gain more control over the
shape of the NHS in the future, it is going to become increasingly
important that they are effectively held to account at a local level.
accountaBility in a local systeM (chapter 7)
Currently accountability mechanisms face upwards. PCTs and
providers are accountable to the Secretary of State for Health,
Parliament and national regulators. However, with the ever increasing
complexity of the health service, and with local PCTs holding more
power and responsibility, it will be crucial for accountability to flow
down to local people, as well as up to central government.
Over the last few years there has been an attempt to strengthen
the tie between the NHS and local authorities. Overview and
Scrutiny Committees have been established, but their powers
should be significantly enhanced so that they can properly hold
PCTs to account.
recommendation 30 :
• oscs should have the power to report issues of
concern, relating to a pct, directly to the pct
regulator.
• the regulator should be required to make a public
response to the osc.
SOCIAL MARKET FOUNDATION
26
• if the regulator’s response does not successfully
address the issue of concern the osc should have
the power to trigger an external review of pct
performance.
• this review should have the power to remove the
pct board and put in place a turnaround team.
• after a maximum of 12 months from the
introduction of the turnaround team a new board
should be elected by the local population.
It is not just OSCs who need the power to trigger an external
review of an underperforming PCT. The general public should
also be able to make it clear when they are not happy with the
performance of their PCT, and to force action to be taken. This level
of accountability will be needed if PCTs are to have the necessary
legitimacy to make difficult decisions over the next decade.
recommendation 31:
• a public petition of an agreed proportion of the
local population should have the power to trigger
an external review of pct performance.
• this review should have the power to remove the
pct board and put in place a turnaround team.
• after a maximum of 12 months from the
introduction of the turnaround team, a new board
should be elected by the local population.
reGulation (chapter 8)
This report sets out a vision for a system in which local
commissioners increasingly have responsibility for the quality of
FROM FEAST TO FAMINE
27
NHS services. External review and inspection is the correct method
for ensuring safety but is not particularly suitable for securing
continuous quality improvement which is a long term, internal
process. Commissioner organisations, which are based at the
same local level as the provider and have a long term relationship
with them, are much better placed to stimulate and support this
internal improvement.
recommendation 32:
• the quality of provider organisations should be
assured and developed through pct contracts.
• the care quality commission should maintain
responsibility for setting minimum safety
and quality standards as part of the licensing
arrangement, and collecting comparative data on
providers across the health service.
However, a radically localised system does not mean a system
without national regulation. In fact, it is essential that a system in
which power is held at a local level is supported by centralised
standards and evaluation of performance.7 As such, the way in
which PCTs are regulated is of key importance.
Currently, PCTs report to four different bodies on different
aspects of their performance: the Department of Health; the Audit
Commission on financial performance; Strategic Health Authorities;
and the Care Quality Commission. There are two major problems
with this structure. First, it provides unnecessary work for hard-
pressed commissioners as they have to report to four different
bodies, each of which has different requirements and different
7 Karsten Vrangbaek, “Key Factors in Assessing Decentralization and Recentralization in Health Systems,” in
Decentralization in Health Care: Strategies and Outcomes, eds. Richard B. Saltman, Vaida Bankauskaite and
Karsten Vrangbaek (Berkshire: Open University Press, 2007). 72.
SOCIAL MARKET FOUNDATION
28
processes. Second, it is difficult for patients to access information
about PCT performance, as it is not held in a single repository.
It is imperative that patients and the public can easily access
high-quality information about how their local commissioner is
performing. There should be a consolidation of PCT regulation,
with a single body overseeing the performance of PCTs and
providing information for the public about the performance of
their local PCT.
recommendation 33: a single commissioning regulator
and inspectorate should be introduced – the nhs
commission – to sit alongside the care quality
commission.
As a corollary of the consolidation of PCT regulation the SHA is
left redundant, and should be abolished.
recommendation 34: the sha should be abolished.
conclusion
Whatever the political rhetoric, the NHS will not be immune
from a spending squeeze that will be worse than any previously
experienced by the vast majority of civil servants and public sector
workers. There is an urgent need to obtain better value for money
from health spending through greater efficiency and a proper
focus on demand management. If the NHS cannot do more for less,
then its future is in doubt. The long waiting lists and low quality
care of the past must not return if the health service is to maintain
public support in the years ahead.
FROM FEAST TO FAMINE
29
The recommendations set out in this report recognise the
need to take radical action but within politically realistic limits.
The NHS has suffered in recent years from the sheer number of
reorganisations it has undergone. There is no doubt that in some
cases reorganising the health service has not helped it to perform
better. The conclusions of the SMF Health Project acknowledge
that while a revolution in structures is undesirable, a revolution
in attitudes is essential. Policymakers in central government must
become genuinely committed to devolving power to frontline
commissioners. Those frontline commissioners must become
the driving force of NHS improvement, taking on vested provider
interests. And a dialogue with patients should be begun to help
users recognise the desirability of a diverse, varied system that
responds to the needs of local people, rather than aspiring to an
unrealistic and inefficient idea of national uniformity.
The move towards a system of local control and local variation
is essential if the NHS is to survive the crisis in public finances. The
limits of centrally driven performance management have been
reached. While there has been substantial improvement as a result
of the reform and investment of the past few years, the ability of
central government to make the savings that will be needed is
questionable. High quality local commissioning offers the best
chance to deliver value for money, not performance management
from the centre. It is time to try a new approach; one that harnesses
the creativity and energy of local professionals. Additionally, the
hard decisions that lie ahead can only be justified to local people
by local health organisations, backed by local accountability
mechanisms, not the Department of Health.
There will undoubtedly be political pain in the move from
a centralised service to one where local commissioners drive
improvement. However, public opinion research carried out as part
of the SMF Health Project shows that people are realistic about
the limits of NHS care, and open to the idea that resources should
SOCIAL MARKET FOUNDATION
30
be distributed according to the needs of different areas. Political
courage will be needed if a move away from the persistent idea that
the NHS is the same everywhere is to be achieved. But the benefits
of local choice must supersede concerns about postcode lotteries.
A diverse, varied service is one that fits with social market
principles. Markets in healthcare provision can provide a pluralist,
innovative and efficient system. Social goals of fairness and
universal access can still be achieved through accountable
commissioning organisations, and strong regulation. The benefits
of a market approach to healthcare could be considerable, and can
be achieved largely within existing NHS structures.
What does the future hold for the health system? It is a
rocky road ahead. The year on year rise in health spending as a
proportion of GDP cannot be continued indefinitely. It may be that
the recession will present an opportunity to radically transform
health services to save money in the long term. This transformation
will require policymakers to consider options that have hitherto
been politically unacceptable – including user charging.
In many different sectors of politics and society a new
consensus is emerging that public services must be substantially
reformed to deal with the challenges ahead. Old solutions that
look to management by central government to make savings and
improve outcomes for patients will not succeed in delivering value
for money. Instead, a radical redistribution of power must take
place. With strong commissioners, functioning provider markets
and better accountability through national regulation and local
accountability mechanisms, the NHS has every chance of a strong
future. Without these much needed reforms, the future is bleak.
FROM FEAST TO FAMINE
31
chapter one: introDuction – a social Market approach to healthcare
This report represents the final conclusions of the SMF Health
Project. Over the past two years the project team has examined
the challenges facing the health system in England. Some of
these challenges are well known and much discussed. A set of
background papers, published in July 2008, analysed the likely
impact of demographic change, new technologies and patient
expectations on healthcare.8 But since the publication of this
analysis a new challenge has emerged: perhaps the most serious
economic downturn for many decades. The impact of the
recession on public finances is severe, and will shape British politics
for many years to come. This presents a fresh challenge to health
policymakers, making more urgent the question of how to extract
best value for money from health services now that future funding
will be highly limited.
The research presented below shows how high-quality
healthcare can be maintained into the long-term future. The
methodology used has been to extrapolate current policy and
economic trends and determine their likely impact on the way care
is funded and provided. In ten years’ time the health system will look
very different from how it is today. What follows is an insight into
what changes we should expect and how they should be achieved.
This analysis is not based on wishful thinking, but on a realistic
assessment of what will be possible to achieve in both political and
policy terms. Many discussions of the future of the health system
begin with an assumption that the current system is undesirable
or unsustainable, and they look to offer an alternative. But it is clear
that perhaps the least desirable option for healthcare in the years to
come is a substantial structural overhaul. While there are undoubtedly
8 D. Furness et al., SMF Health Project Background Papers (London: Social Market Foundation, 2008).
SOCIAL MARKET FOUNDATION
32
lessons to learn from other health systems, some of which are
explored in subsequent chapters, it is clear that the NHS will remain a
central and recognisable part of the health system in this country. So
the recommendations that follow do not propose radical changes to
the structure of healthcare. Instead, ideas are explored that will both
deliver good value for money and equip the health system to deal
with the substantial challenges it faces, without having to rip up the
structures that already exist and start afresh.
The conclusions and recommendations featured in this report
are strongly influenced not only by the available evidence about
what works in health policy but also by a major piece of quantitative
and qualitative research into public attitudes about the future
of healthcare, carried out by the SMF Health Project team.9 If the
principles of a universal health system are to be maintained, public
support for change is crucial, and, therefore, an understanding of
how the public views the health service is essential. The findings
of this public opinion research have already been published, and
its implications are reflected throughout this report. In addition
to this, the project team has conducted a range of seminars and
interviews with health policy experts, practitioners and patients
which inform the conclusions presented below.
As well as being politically realistic and based firmly on the
need to maintain public support for universal access to healthcare,
this report also adopts a distinctively social market approach to
healthcare. The social market philosophy is the guiding principle
of the Social Market Foundation and offers a useful analytical
framework for making policy. Markets are uniquely capable of
delivering a prosperous society and improved public services.
But while market mechanisms are valuable, a wholly free market
approach cannot deliver the outcomes that a fair society demands.
9 D. Furness and B. Gough, Local Control and Local Variation in the NHS: What Do the Public Think? (London: Social
Market Foundation, 2009).
FOREWORD
33
As a result, markets must be limited and supplemented with
necessary, but careful, design and regulation. A social market
approach is therefore “pro-market”, but not “free-market”.
This principle guides the thinking throughout this report,
explaining why, for instance, the idea of private markets in
healthcare financing is rejected, while the improvements in care
that could be achieved with a better-functioning provider market
are welcomed. Above all, though, this research is informed by the
idea that healthcare is a valuable social good, and that universal
access to high-quality healthcare is central to a fair society and is
therefore a goal we must continue to aspire to reach.
Discussing the recession in The Times, Peter Riddell wrote:
The public debate avoids the real choices. The arguments
of the populist right and the public sector left have mirror
image flaws. The former claim the answer lies in wars on
waste and bloated bureaucracy, while the latter treats any
cuts as threatening the whole welfare state.10
A social market approach falls into neither of these categories.
Although there is scope for reducing bureaucracy to achieve
greater efficiency, this cannot be the whole solution; and adopting
pluralistic approaches can drive innovation and value for money.
At the same time, cuts and radical reinventions of welfare state
services, such as healthcare, cannot be rejected out of hand,
particularly where it can be shown that radical transformation can
be achieved without sacrificing important social values.
In 2009, there is one central challenge for policymakers in
healthcare: how to deal with the huge public spending squeeze
that will inevitably follow the current recession. This requires
10 P. Riddell, “Public to Brace for Pain to Get Economy Back on Track,” The Times (21 April 2009), 45.
SOCIAL MARKET FOUNDATION
34
policymakers to deal with the future finance of healthcare, and
also to examine radical ways of securing better value for money
through local decision-making.
FinancinG – challenGinG tiMes aheaD
Previous SMF Health Project research has shown that fears over
the likely impact on health services of an ageing population and
the advent of new medical technologies are largely overblown.11
However, since the publication of this analysis, the economic
climate has changed for the worse, and the impact of the recession
on public services has been significant. As the BBC political editor
Nick Robinson recently commented: “The whole of the public
sector is bracing itself for a squeeze the like of which few have
experienced before.”12 Forecasts made by the Chancellor of the
Exchequer in the 2009 budget have been criticised for being
overly optimistic,13 and, even under the scenarios he described,
public services face a tough time – annual increases of 0.7% from
2011.14 Furthermore, a report from the Institute for Fiscal Studies
has concluded that departmental expenditure limits (DELs) that
include NHS spending could be the worst hit – budgets might
have to be reduced by 2.3% per annum in 2011–14.15 For years,
healthcare discussions have raged about whether health systems
are sustainable, given the trend of increasing costs. Now, though,
instead of focusing on the cost implications of ageing, new
technologies, rising public expectations and an increase in chronic
disease and poor public health, the debate must instead turn to
the impact of a dramatic slowdown in health budgets.
11 D. Furness et al., SMF Health Project Background Paper 2: Demography and Technology: External Pressures for
Change (London: Social Market Foundation, 2008).
12 N. Robinson, “Age of Austerity”, http://www.bbc.co.uk/blogs/nickrobinson/2009/04/age_of_austerit.html.
13 L. Elliott, “City Pours Scorn on Treasury’s GDP Forecasts”, Guardian (23 April 2009).
14 HM Treasury, Budget 2009: Building Britain’s Future (London: HMSO, 2009).
15 G. Tetlow, Budget 2009: Public Spending (London: IFS, 2009).
FROM FEAST TO FAMINE
35
This report analyses current policy and economic trends in
healthcare and sets out a series of reforms that will help to achieve
a sustainable health system for the next decade and beyond. The
challenge facing the health service in England is not a small one,
and failure to achieve greater efficiency and productivity may
mean that the entire post-war settlement of healthcare funding
and provision will be undone. To maintain public support for the
current system, the public must be convinced that what is offered
by state services is of a high quality. And healthcare providers face
a stiff task in achieving continuing quality improvements at a time
of rising government debt, rising taxes and falling investment
in public services. While the recommendations set out below
offer the health system the best chance of achieving its goals, it
is possible that they will fail. If this occurs, it is difficult to see the
NHS continuing in its current form beyond 2020 – radical options
for restructuring and refinancing will become the only way to
guarantee ongoing universal access to healthcare into the future.
reDeFininG the nhs – national FraMeworks, local
stanDarDs
There is clearly a big challenge for future financing. Associated
with this is the urgent need to secure better value for money in
healthcare provision. To achieve massive efficiency savings, and to
drive through the cutbacks, reconfigurations and decommissioning
that will be required in the years ahead, it will be necessary to
redefine radically some of the principles of healthcare provision
that have seemed central since the inception of the NHS in 1948.
Chief among these is the idea of a national health service.
There is an ongoing tension between central control and the
drift of policy towards greater decentralisation to local primary
care trusts (PCTs). Fears have been expressed that this will lead to a
“postcode lottery” in healthcare. While unintended and unexplained
variation in care should not be tolerated, variation itself should
SOCIAL MARKET FOUNDATION
36
be enthusiastically embraced by policymakers as the best way to
ensure locally appropriate services that will save money overall.
There should be an open acceptance that variation between local
areas is desirable, leading to the efficient commissioning and use
of resources, innovation in service delivery and appropriate local
services. Local PCTs should be free to shape health services to meet
local needs, but this autonomy should be coupled with systems
that safeguard against unacceptable differences in quality, with
regulators playing a key role in providing comparative information
and setting minimum standards.
Local choice and local variation must become the guiding
principles of the health system, with a significantly reduced role
for central government. The state should remain as revenue raiser
and resource distributor, but the key driver of change in healthcare
should be local commissioners – PCTs. Commissioners must be
strengthened and given true autonomy to develop provider
markets that meet the needs and wants of local people, to which
they will be sensitive and responsive. Patients and the public
should be given an enhanced role in healthcare decision-making
with real power to hold commissioners to account.
The status of commissioners within the health system must
change, giving them greater power, to which providers are forced
to respond. And commissioners must be able to justify to the
people they serve the inevitability of an ever increasing degree of
local variation within the health system. Without radically shifting
power from the centre to the localities, and putting in place robust
mechanisms of local accountability, there is no prospect either of
significant efficiency gains and the development of innovative new
services, or of justifying to people the tough choices about what to
make available and what to cut in a publicly funded health system.
Along with the establishment of a truly local service, with
autonomous commissioners driving improvement, a new definition
FROM FEAST TO FAMINE
37
of NHS values is required. To ensure fair access into the future, the
values at the heart of the health system must be set out clearly
and should shape future policy. While fairness and universal access
should still be at the heart of the system, setting charges as a tool
of demand management must be considered. At the same time, the
whole area of NHS charges needs to be overhauled to ensure that
people on low incomes are offered genuinely free care. No longer
should pensioners automatically be exempt from charges while the
working poor pay for prescriptions. A radical redefinition of fairness
and NHS values can and should go hand in hand with the shift from
the centre to the frontline, from the national to the local.
DescriBinG the health systeM oF the Future
The sections above have shown how, in the context of the immense
financial challenge facing the health system, it is right to consider
the role of national financing and governance together with locally
driven healthcare options in order to secure good value for money.
The chapters that follow each examine a particular aspect of the
future of the health system. Recommendations are incorporated
that set out how the system should change so as to achieve greater
efficiency and quality and to transfer power from the centre to the
frontline. In large part, conclusions are developed from a discussion
of central principles of different aspects of health system design,
and/or an exploration of recent health system reform. In this way
the arguments presented in the following chapters are both a look
ahead at the next decade of healthcare and also an opportunity
to work from first principles. There is a great need to redefine the
state itself and, with it, welfare provision in the context of a crisis in
public finances. This report aims to contribute to an urgent political
debate on how this should be achieved.
The report is split into two parts. The first is a description
of what the future role of national frameworks and national
governance should be, including how resources should be raised
SOCIAL MARKET FOUNDATION
38
and distributed, and how NHS values should be defined. The
second analyses the way in which local health commissioners need
to change in order to drive service improvement.
Throughout this report relatively little attention is given to
the role of NHS providers as opposed to the commissioners of
healthcare. This is a deliberate choice: the report argues that in the
future the NHS will increasingly be responsible for commissioning
rather than with providing healthcare. So there is a greater focus
on how commissioners can develop strong provider markets than
on, for instance, the future of NHS hospitals. Questions about
who provides healthcare should become steadily less significant.
A genuinely diverse market of providers rather than an unhelpful
focus on NHS hospital care will be an important step in securing a
sustainable future for the health system.
part one
chapter 2: equity
Perhaps the most important criterion that healthcare systems
must fulfil is that they are fair. Chapter 2 explores why fairness in
healthcare is important, and how it can be defined. By comparing
different conceptions of equity, it posits a radical redefinition of
NHS values to ensure that universal access remains a priority, but, at
the same time, that limitations in care and variation between areas
are acknowledged. It is shown that the current definition of equity
to which policymakers aspire is unhelpfully narrow, and that a
broader idea of what is fair offers the best opportunity of securing
an equitable health system.
chapter 3: paying for healthcare
Chapter 3 focuses on emerging challenges to the current model
of healthcare funding. The cost of healthcare in the developed
world has increased tremendously in recent times, and questions
about how best to fund it is an unending source of controversy.
FROM FEAST TO FAMINE
39
While fears about the impact of ageing or new technologies are
overblown, there is a real challenge emerging as a result of the
dire state of public finances. There is almost no chance that the
health system as it is currently designed will be able to maintain
or improve standards of care given the severe resource constraints
that will be in place for the foreseeable future. However, it is crucial
that any alterations to the system of funding maintain the central
principle of fairness. This chapter marshals the evidence on sources
of healthcare funding, including user charges. The discussion is
framed in terms of a general public willingness to invest in health
and healthcare. The chapter weighs the evidence and makes some
radical proposals about how to maintain a universal health system
without compromising the core values of the NHS.
chapter 4: national governance
The framework set out in Part Two proposes a far more locally
autonomous health system, with a greatly reduced role for national
standards. In such a locally varied system what roles are left for
national government? The final chapter in Part One sketches the
process of recent NHS reform with an emphasis on the “target
culture” that was a product of strong central performance
management. Although this stifling approach should not be a
feature of the health system in the future, there are still certain key
tasks that central government must perform. Foremost among
these concerns raising funds and distributing resources, as well as
overseeing national regulators. It must also be the job of central
government to define a set of values for the health system that
provides a framework in which local commissioners will operate.
part two
chapter 5: Decentralisation
Chapter 4 examines decentralisation as a policy option and
suggests a model that the English health system should adopt.
Decentralisation has already become a feature of health policy
SOCIAL MARKET FOUNDATION
40
in the NHS with the introduction of PCTs and the establishment
of foundation trusts. But there are still great tensions between
national control and local priorities. This chapter explains how and
why a decentralised model of healthcare should operate in the
health system in this country.
chapter 6: commissioning
The era of central command and control in healthcare is over. Chapter
5 focuses on the ever more important role that commissioners will
have to play in the health system. In order to achieve the economies
that will be necessary to meet the challenge posed by recession,
the only real option for the NHS is significantly to strengthen
commissioning. Even this may not be enough – the evidence base
for the potential of better commissioning must be strengthened.
But there are many ways in which commissioning skills can be
developed, the capacity of commissioning organisations improved
and the status of commissioners within the health system raised.
The strength of commissioners can only be improved if government
relinquishes control of significant parts of healthcare decision-
making. And if commissioners are to succeed, they must be free
to develop new roles and provider markets. Indeed, the provision
of healthcare must become less important in the public mind
than the purchasing of it – over time the provider market should
move away from the monolith of NHS provision towards a genuine
market of competing providers from the public, private and third
sectors. These changes must lead to a locally varied service that
reflects the benefits of true local choice.
chapter 7: accountability
By changing the way healthcare is delivered, it will also be
necessary to introduce new systems of accountability. No longer
can accountability be centred on Parliament, with the Secretary
of State answerable for every dropped bedpan across the NHS. In
creating a localised health system, it is crucial, if legitimacy is to
be maintained, that new models of accountability are designed. In
FROM FEAST TO FAMINE
41
this there is a role for democratic processes. But local democracy
should not, as some have argued, play a central role in allocating
local resources. The results of SMF Health Project public opinion
research suggest that people do not want to be involved in this sort
of decision-making unless something goes wrong – the systems of
accountability set out in chapter 7 reflect this.
chapter 8: regulation
There has recently been substantial change to healthcare
regulation with the introduction of the Care Quality Commission
(CQC) representing a consolidation of previous regulators across
health and social care. But in the future it is commissioners, rather
than an arm’s length national regulator, who should be responsible
for securing the quality of local providers. The way in which
commissioners are regulated should also change so that their
crucial role in local health provision is recognised. Chapter 8 sets
out these arguments and establishes the right principles for the
future development of healthcare regulation.
SOCIAL MARKET FOUNDATION
42
Part One
chapter two: equity in the health systeM
It is rightly held that the values of the NHS are precious and should
be maintained. Chief among these is equity – the idea that health
services should be fair. This chapter is an examination of the way
in which different conceptions of equity in health and healthcare
play out in reality. It argues that while there is a good deal of
consensus about the desirability of equity in healthcare, there
are real problems in translating this into a reality that ordinary
people would regard as equitable. Because of this, problems are
encountered in the areas of resource allocation and the rules and
regulation of health systems that the available literature does not
help to solve. Equity is important in health policy because it sets
the overarching framework of what is considered acceptable,
particularly with regard to policy issues like charging. But without
an agreed definition of equity, approaches to policy challenges in
healthcare are without a secure foundation.
This chapter explores the idea of equity in healthcare. In
particular it considers the various different health systems and
structures that can be considered equitable and draws out
implications for the future of the NHS. It goes on to ask how far
various equity goals are fulfilled in the UK National Health Service
(NHS) and explores which different policies can be deemed
acceptable within a broadly equitable framework, with a particular
focus on charging and appropriate access targets.
The chapter is split into two sections. The first looks at the
theoretical literature on equity. Why is equity in healthcare
considered important? What different types of equity are there? Can
defining equity help us deal with policy challenges in healthcare?
This approach demonstrates the limitations of applying a theoretical
FROM FEAST TO FAMINE
43
approach to equity to practical problems in healthcare. Equity is a
much discussed term, and a common aspiration for health systems,
but it is clear from the arguments presented in this first section that
the lack of common agreement about how it should be defined is
a serious problem. The challenge of defining equity is ever more
urgent given the financial restrictions that the NHS faces in the
years to come. An equitable approach to healthcare will be crucial
if public support is to be maintained for a system that faces difficult
decisions about how best to allocate scarce resources.
The second part of the chapter is a brief survey of the extent to
which equity goals are achieved in the NHS. This section shows how
ideas about fairness have developed since the inception of the NHS in
1948. Interestingly, while equity is often referred to as a core principle
of the NHS, ideas about fairness have changed remarkably since the
Beveridge Report’s original proposal for a national health service. Not
only has the idea of equity as a policy goal changed over time, so too
have approaches to putting equity into practice. The discussion here
includes both the allocation of resources and access to healthcare
for different groups –the extent to which the NHS spends its money
equitably, and how different groups actually benefit from publicly
funded care. It is clear from an examination of the evidence that
serious challenges in providing equitable services remain, leading to an
argument for a new approach to target-setting for equity in the NHS.
The chapter finishes with a suggested definition of equity
in the NHS that builds on the set of values included in the NHS
Constitution. This definition of equity both safeguards important
principles of universal access to healthcare, while also providing
policymakers with room for manoeuvre in responding to a move
towards genuinely local health provision at a time of scarce public
resources – a move that this report encourages.
The intention of defining equity more clearly, and in a practical
sense, is both to inform policymakers and to engage public support
SOCIAL MARKET FOUNDATION
4 4
for the NHS as it seeks to deal with the ramifications of the crisis in
public finances. The suggested definition of equity also shows that
a health system can still be equitable even as it considers a range
of policy options that have hitherto been politically unacceptable.
The NHS is deeply embedded in British society, and there is
an undeniable sense that its values are important. However, while
debates about these values and the importance of fairness evoke
strong emotions, there is not necessarily any real agreement as to
how equity in the health system should be defined. Public opinion
research conducted as part of the SMF Health Project found that
attitudes to local variation in the NHS were based on a range of
different ideas about what is fair.16 That is why this debate is crucial
for the future of the health system. Public support for universal
healthcare must be maintained particularly during a period of
severe financial constraints, and defining equity is an important
political and policy goal towards achieving this aim.
what is equity anD why Does it Matter?
The first part of this chapter is an exploration of the different ways
in which equity has been defined in an academic sense. This is
an important debate, as it is through the academic literature that
policymakers are led towards principles that can be applied in practice.
However, while there is a wide acceptance that equity is desirable,
there are significant difficulties in applying theoretical lessons to the
real-world challenges that the health service faces in the years ahead.
Why is equity important in healthcare? It is accepted that
citizens have different levels of income, live in different houses, eat
different food and have different quality relationships. In general,
inequality is tolerated in most areas of day-to-day life. However, in
16 D. Furness and B. Gough, Local Control and Local Variation in the NHS (London: Social Market Foundation,
2009).
FROM FEAST TO FAMINE
45
developed countries there is general agreement that health should
not be considered a consumer good in the same way that watches,
cars or satellite television are. The most influential statement on the
idea that health and healthcare are goods that should not simply
be allocated according to capacity to pay was articulated by James
Tobin in 1970.17 He argued in favour of “specific egalitarianism” – a
view that health, among other goods, should be subject to special
consideration in civilised societies because it is so fundamental to
a good-quality life. This argument has been repeated many times,18
and is reflected in policy support for publicly funded health systems
that attempt to ensure that there is equitable access to healthcare
and an equal opportunity to be healthy, and that healthcare is of
equal quality for all citizens.
It is accepted that healthcare should not be subject to a free
market approach, and that equity in health systems is a desirable
aim. So, do markets have any part to play in healthcare? The social
market approach argues that they do. While it is socially desirable
for individuals to share their risk of catastrophic healthcare
expenditure, market mechanisms can certainly play a key role in
the provision of healthcare without undermining equity.
But what is equity? The first answer to this question is that
equity is not a concept that can easily be pinned down. There are
many ways in which fairness or equity can be defined – “equity,
like beauty, is in the eye of the beholder”.19 This is not a trivial
point. Different definitions of equity in healthcare can result in very
different relative outcomes for patients because of the different
priorities that policymakers attempt to reflect in resource allocation.
17 J. Tobin, “On Limiting the Domain of Inequality”, Journal of Law and Economics (1970).
18 For example, see S. Anand, “The Concern for Equity in Health”, Journal of Epidemiology and Community
Health (2002).
19 L. Cohen, “Health Care Equity Tackled From Many Angles at CHEPA Conference”, Canadian Medical
Association Journal 147:4 (1992).
SOCIAL MARKET FOUNDATION
46
For example, some aspirations towards equity in healthcare
can be so vague as to be almost meaningless. In 2003 came the
development of a new intergovernmental initiative called the
International Forum on Common Access to Health Services. This
brought together health ministers from a diverse range of countries
(Chile, Germany, Greece, New Zealand, Slovenia, Sweden and the
UK), “united by the value that health systems shall ensure all citizens
universal and equitable access to good health care”. For these
ministers, equitable access meant “good care on equal conditions
for all people, regardless of social circumstances or where in the
country you live”.20 Recognising diversity and responding to the
individual needs of the patients were, as far as they were concerned,
the key mechanisms to ensuring equity.
It is obvious that this alone is not an adequate framework for the
difficult decisions that have to be made in healthcare systems. One
wonders if, for example, on returning to Santiago the Chilean health
minister found this definition of equity much use as he pondered the
problems faced by his health system, which were perhaps very different
challenges from those facing his counterparts in other nations.
Confusion over equity can be compounded by the realisation
that, as Imre Loefler puts it: “Equity stands for fairness, yet what
is fair is not necessarily equal, and what is equal is not necessarily
fair.”21 An example of this tension is “orphan drugs” where
treatments for rare conditions can be extremely expensive. It might
not be equitable to allocate so much to an individual patient, but
it might seem unfair to deny care to someone unlucky enough to
suffer from a very rare disease. This example is considered in greater
depth below. Clearly, creating an equitable health system is not a
simple business.
20 “International Forum on Common Access to Health Care Service,” Euro Observer: Newsletter of the European
Observatory on Health Care Systems, 2003.
21 I. Loefler, “Let’s Be Fair About Equity and Equality,” British Medical Journal 332:7543 (2006); I. Loefler, Let’s Be
Fair About Equity and Equality (British Medical Association, 2006).
FROM FEAST TO FAMINE
47
Definitions of equity
Conceptions of equity in healthcare
The OECD argues: that “The concern for equity extends both to the
distribution of the payments for health care across the population
(fair financing) and to the distribution of access to health services
across the population (fair access).”22 This chapter is concerned less
with the financing of healthcare, a discussion of which can be found
in chapter 3, than with how health systems work in practice in terms
of access to treatment. However, it is important to remember that
financing systems profoundly influence equity in healthcare. The
best example of this is the USA, where many millions of people do
not have adequate health coverage, even though health spending
is some 15% of GDP – significantly above the OECD average (see
figure 2.1). This is because the USA operates a system of private
health insurance with limited state-funded provision for those on
lower incomes. The result is a fundamentally unfair system that
would certainly not be acceptable in this country.
The other common funding mechanisms for health systems
in OECD countries are general taxation or different forms of social
health insurance. Typically, both systems provide virtually universal
coverage, and take steps to ensure that access to healthcare
is based on need rather than ability to pay. These systems are
common in European countries. A survey of international health
financing systems found that tax funding systems are proportional
or mildly progressive, social insurance systems are regressive,
and private insurance systems are even more regressive.23 In this
instance, progressive systems are judged as those where ability
to pay impacts least on ability to access health services, and
wealthier individuals contribute at a higher level than people with
less money.
22 O. A. Arah et al., “A Conceptual Framework for the OECD Health Care Quality Indicators Project”, International
Journal for Quality in Health Care 18: Supplement 1 (2006).
23 E. Van Doorslaer et al., “Equity in the Delivery of Health Care: Some International Comparisons”, Journal of
Health Economics 11:4 (1992).
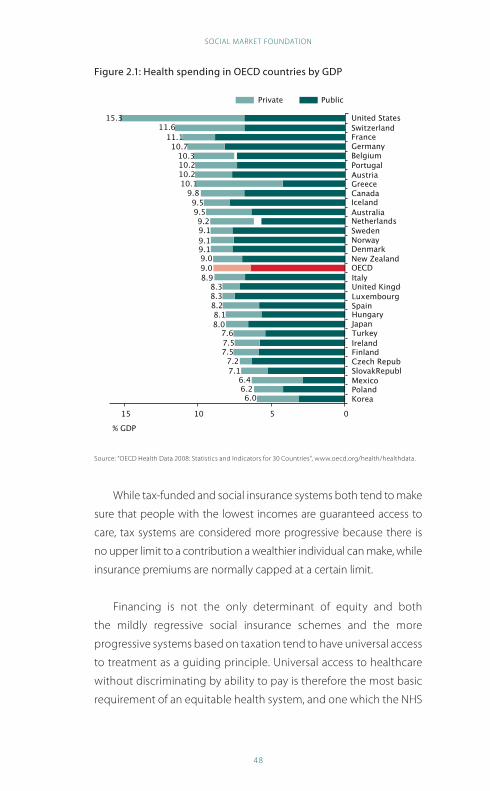
SOCIAL MARKET FOUNDATION
48
Figure 2.1: health spending in oecD countries by GDp
United States
Private Public
SwitzerlandFranceGermanyBelgiumPortugalAustriaGreeceCanadaIcelandAustraliaNetherlandsSwedenNorwayDenmarkNew ZealandOECDItalyUnited KingdomLuxembourgSpainHungaryJapanTurkeyIrelandFinlandCzech RepublicSlovakRepublicMexicoPolandKorea
051015
% GDP
15.311.6
11.110.7
10.310.210.210.1
9.89.59.59.29.19.19.19.09.08.9
8.38.38.28.18.0
7.67.57.5
7.27.1
6.46.26.0
Source: “OECD Health Data 2008: Statistics and Indicators for 30 Countries”, www.oecd.org/health/healthdata.
While tax-funded and social insurance systems both tend to make
sure that people with the lowest incomes are guaranteed access to
care, tax systems are considered more progressive because there is
no upper limit to a contribution a wealthier individual can make, while
insurance premiums are normally capped at a certain limit.
Financing is not the only determinant of equity and both
the mildly regressive social insurance schemes and the more
progressive systems based on taxation tend to have universal access
to treatment as a guiding principle. Universal access to healthcare
without discriminating by ability to pay is therefore the most basic
requirement of an equitable health system, and one which the NHS
FROM FEAST TO FAMINE
49
should continue to meet in the years ahead. But agreeing this basic
minimum leads to an important distinction in the analysis of equity
in healthcare – horizontal and vertical analyses.
Vertical and horizontal equity
Vertical equity is a reasonably straightforward condition to satisfy.
Vertical equity recognises that individuals do not all need to receive
the same benefits from the health system – people in greater need
should receive a greater proportion of the benefits. A health system
that did not fulfil the condition of vertical equity would be a bizarre
construction: healthy members of the public would be summoned
to hospital to receive unnecessary treatment while the sick and
the dying languish at home, receiving only the attention given
to every other member of the population. It is generally assumed
that developed health systems fulfil this basic consideration, so this
chapter is not predominantly concerned with vertical equity.
Much more important is horizontal equity. In this sense an
equitable service is defined as one that offers equal access to
healthcare for those in equal need.24 This is a much thornier
problem. There is concern that many health systems, including
the NHS, do not actually offer equal access for equal need.25 Older
patients, those from ethnic minorities, people with mental health
problems or people with low incomes may not have equal access
to treatment, for example.
The problem of defining need
There are problems of measurement here. First, there is a great
deal of debate about the nature of need and how it can be
measured. It cannot easily be defined and, once again, there is an
enormous literature discussing the problem.26 There is not space in
24 A. Dixon, Is the NHS Equitable? A Review of the Evidence (London: LSE Health and Social Care, 2003).
25 J. Gubb, “Why the NHS Is the Sick Man of Europe”, Civitas Rev 5:1 (2008).
26 M. Asadi-Lari, C. Packham and D. Gray, “Need for Redefining Needs”, Health and Quality of Life Outcomes
1:1 (2003).
SOCIAL MARKET FOUNDATION
50
this chapter to consider the multitude of definitions of need, but
it should be noted that different definitions have very different
implications for service design and resource allocation. For
instance, Culyer defines need as “capacity to benefit” and for him
this rests on the moral principle that good health is required for
individuals to “flourish” in their lifetime.27 This is very different from
the typology approved by the International Forum on Common
Access to Health Services, which use Bradshaw’s fourfold definition
of (i) normative need (defined by experts or professionals); (ii) felt
need (what the individual thinks they need); (iii) expressed need
(what the individual says they need); and (iv) comparative need
(where individuals in different locations are compared so that what
each needs can be established).
Clinicians who have discussed the various definitions of need
have concluded:
If needs analysis is intended to be meaningful rather than an
academic exercise or political propaganda, definitions must
reflect clinical reality. In this respect, current definitions fail
to recognise the needs that we have identified among our
own cardiac patients.28
This clearly presents a challenge to those who would analyse
horizontal equity in the NHS – if there is no agreement about what
needs exist, then how can it be shown whether they are met?
Despite this limitation, the issue is not hopeless. The later
discussion of equity within the NHS, in the second part of this chapter,
demonstrates that some firm conclusions can be made about equal
access to services based on need without having to thrash out an
unlikely consensus reconciling the myriad definitions of need.
27 A. J. Culyer, “Equity – Some Theory and Its Policy Implications”, British Medical Journal 27:4 (2001).
28 Asadi-Lari et al., “Need for Redefining Needs”.
FROM FEAST TO FAMINE
51
Defining equity in healthcare
The nature of fairness in healthcare is an issue that generates many
different intellectual approaches. What follows is a brief survey
of how equity can be defined. It illustrates how, far from being
complementary, there are some direct contradictions between
different approaches and, furthermore, it points out the limitations
of the debate in equipping us to deal with the practical challenges
faced by policymakers.
The World Health Organisation (WHO) definition is: “Equity is the
absence of avoidable or remediable differences among populations
or groups defined socially, economically, demographically, or
geographically.”29 Thus, equity becomes an outcome measure,
rather than a guiding set of principles for service design. The
WHO’s interpretation also demonstrates the extent to which some
definitions of equity are intrinsically linked with health inequalities.
Health inequalities are, of course, the product of many different
factors outside access to healthcare. Education, wealth, housing,
nutrition and access to exercise facilities all contribute to health
inequalities. Equity in access to healthcare should be considered
separately from the wider inequalities related to health that exist in
any society, though unequal access to care will certainly widen the
gap between the healthiest and the least healthy.
Equity is also a constituent part of the Ljubljana Charter on
Reforming Health Care which applies to members of the European
region of the WHO.30 The charter states: “Health care reforms must
be governed by principles of human dignity, equity, solidarity and
professional ethics.” Once again this demonstrates that institutional
conceptions of equity do not necessarily help us in making
practical decisions. What is equity? What is solidarity? Chinitz et al.
have drawn attention to how vague these concepts are. For them,
29 “WHO: Equity”, http://www.who.int/trade/glossary/story024/en/.
30 R. Saltman and J. Figueras, European Health Care Reforms. The Ljubljana Charter on Reforming Health Care
(Copenhagen: World Health Organisation, Regional Office for Europe, 1996).
SOCIAL MARKET FOUNDATION
52
universal, equitable coverage in European health systems equates
to “solidarity”. However, “During the past 50 years … the term
solidarity came to convey some vague notion about the welfare
state”31 rather than a consensus view about what equity means in
practical terms. Comparing their definition of solidarity with those
from other sources demonstrates that there is certainly confusion
about this term too.32
As well as the definitions offered by bodies like the WHO,
there is an extensive theoretical literature about equity. In an
influential article, Culyer and Wagstaff suggest four definitions:
utilisation, distribution according to need, equality of access and
equality of health.33 They argue that there are problems with each
of the definitions, and that they are mutually incompatible. For
example, equity based in principles of utilisation would contradict
vertical equity criteria that require different levels of utilisation
reflecting healthcare need. Some programmes that are popular
with the public, such as “Health MOTs”,34 might also be considered
inequitable on these grounds as they direct resources towards the
healthiest members of society. “It is self-evident that the principle
of equalizing expenditures will conflict with the principle of
distribution according to need, unless the persons in question are
deemed to be in equal need.”35
This is an important insight for policymakers, as this conclusion
conflicts with views expressed by members of the public. Research
conducted by the Social Market Foundation concluded that many
31 D. Chinitz, A. Preker and J. Wasem, “Balancing Competition and Solidarity in Health Care Financing”,
in R. Saltman, J. Figueras and C. Sakellarides (eds), Critical Challenges for Health Care Reform in Europe
(Buckingham: Open University Press, 1998).
32 According to the International Forum on Common Access to Health Services, solidarity means access to a
reasonable minimum range and standard of care
33 A. J. Culyer and A. Wagstaff, “Equity and Equality in Health and Health Care”, Journal of Health Economics
12:4 (1993).
34 Department of Health, Choosing Health: Making Healthy Choices Easier (London: HMSO, 2004).
35 Culyer and Wagstaff, “Equity and Equality in Health and Health Care”, 446.
FROM FEAST TO FAMINE
53
people believe that the NHS should offer the same services to
everyone, regardless of specific needs in particular areas: “When
the NHS came round it was the same treatment for everyone, and
I don’t think we should change that.”36 While the NHS does not
spend equally on different areas, it appears that people think it
does. This presents a political challenge, and suggests that a new
definition of equity is required in the NHS to reflect the actuality
of health policy rather than the different view of fairness held by
members of the public.
Culyer and Wagstaff go on to argue that policymakers tend to
understand equity in terms of equality of access – the opportunity
to access healthcare when it is required. To these authors, this is
the wrong approach. Instead, equality of health should be the
ultimate criterion for equitable health systems: “An equitable
distribution of health care is simply one which gives rise to an
equal distribution of health.”37 However, there is a difficulty in
judging health systems by their ability to distribute health equally
(i.e. reducing health inequalities): too many external factors are
influential in determining health to make it a fair test for healthcare
providers. A 2008 report for the Department of Health stated that it
is “ever clearer that the Department of Health and the NHS cannot
reduce health inequalities in isolation from other public services”.38
This is a serious problem when it comes to applying Culyer and
Wagstaff’s methodology to the evaluation of health systems. The
NHS needs a more straightforward definition of what is equitable
than “equal distribution of health”. This discussion is explored in
greater detail below.
What about those who actually try and apply principles of
equity? The National Institute for Health and Clinical Excellence
36 D. Furness and B.Gough, Local Control and Local Variation in the NHS: What Do the Public Think? (London:
Social Market Foundation, 2009).
37 Culyer and Wagstaff, “Equity and Equality in Health and Health Care”, 452.
38 Department of Health, Health Inequalities – Progress and Next Steps (London: HMSO, 2008), 10.
SOCIAL MARKET FOUNDATION
54
(NICE) is charged with evaluating technologies and reducing
variation in clinical standards across the whole of the NHS. Equity,
according to NICE, “refers to fairness in the ways in which the costs
and benefits of available care are distributed among all who use
the NHS”.39 This definition is not particularly remarkable, and it does
not represent a broad consensus on what equity should mean. This
is perhaps because, as NICE chairman Sir Michael Rawlins remarks,
“Much of the philosophical literature on equity is far from being
applicable in the real world.”40
More practical definitions of equity have been supplied by
writers like Whitehead. Referring specifically to the NHS, she lists
the features of the service that fall under her overarching concept
of equity, without focusing on an explicit philosophical framework.
Whitehead’s equity criteria are:
• service for everyone;
• free at the point of use;
• comprehensive range of services;
• geographic equality;
• high standards – levelling up not down;
• selection on need, not ability to pay;
• high ethical standards.41
This approach is much more useful in equipping policymakers to
deal with the challenges to equity that are discussed in more detail
below than the more abstract approaches to the design of services
and allocation of resources found in much of the literature.
conclusion
The preceding discussion has shown that equity in healthcare is
39 M. D. Rawlins and A. J. Culyer, “National Institute for Clinical Excellence and Its Value Judgments”, British
Medical Journal 329:7459 (2004).
40 Ibid.
41 M. Whitehead, “Who Cares About Equity in the NHS?”, British Medical Journal 308:6939 (1994).
FROM FEAST TO FAMINE
55
a nebulous concept, difficult to define precisely and the subject
of a great deal of academic debate. While many different health
systems have equity as a central aim, it is impossible to detect a
consistent approach. Even among the academic community there
is an acknowledgement that translating theoretical knowledge
about equity into practically applicable principles for service design
and resource allocation is a sticky problem. As one of the architects
of recent NHS reform, Julian Le Grand, writes: “The practical notions
of equity that should inform policy and the ways in which these
should be implemented are far from clear.”42
This lack of clarity about how equity should be defined
indicates that to apply principles of fairness consistently requires
a less abstract, more practical definition of what is considered
equitable. The second part of this chapter suggests how equity
should be defined in the context of a severe squeeze on healthcare
resources and in an increasingly localised system with ever more
variation of service between different localities.
equity anD the nhs
The first part of this chapter outlined the academic debate about
equity in health and healthcare. The discussion on different
conceptions of equity in health systems has demonstrated the
limits of a purely theoretical approach. The truly important
question is how equity is applied in practice – how to make
health services fair. This section looks specifically at how equity
has been approached in the NHS from its inception in 1948. It
then examines how equitable the service is now. Challenges
to conventional ideas about equity are then discussed before a
number of policy recommendations are suggested as a response
to changing circumstances.
42 F. Sassi, J. Le Grand and L. Archard, “Equity Versus Efficiency: A Dilemma for the NHS. If the NHS Is Serious
About Equity It Must Offer Guidance When Principles Conflict”, British Medical Journal 323:7316 (2001).
SOCIAL MARKET FOUNDATION
56
equity at the birth of the nhs
A brief look at the Beveridge Report
William Beveridge’s 1942 report, Social Insurance and Allied
Services (known as the Beveridge Report), served as the basis for
the post-war welfare state, including the National Health Service.
The report argued, notably, that social insurance is only one part
of a “comprehensive policy of social progress”, thus allowing for
the NHS to be paid for out of general taxation rather than via
national insurance.43
The report also set limits on the future NHS and welfare state,
arguing that the state “should not stifle incentive, opportunity,
responsibility; in establishing a national minimum, it should
leave room and encouragement for voluntary action by each
individual to provide more than that minimum for himself and
his family.” Beveridge argued that this system would provide
a minimum standard of living “below which no one should be
allowed to fall”.
The establishment of the NHS
The implementation of the report was carried out by Aneurin
(‘Nye’) Bevan, who was appointed Minister of Health in 1945.
The shape that the NHS took in its early years was to a large
degree dominated by the statist and centralist Fabian version of
socialism that dominated the Labour Party at that time. Under
the final settlement for the NHS, 2,688 voluntary and municipal
hospitals in England and Wales were nationalised and came under
Bevan’s supervisory control. Nothing in the Beveridge Report had
demanded this degree of central control.
The scope of Bevan’s NHS was also greater than Beveridge had
envisioned. Bevan established a service free at the point of delivery
for all, where “every person, regardless of wealth or position, would
43 W. H. B. Beveridge, Social Insurance and Allied Services (London: HMSO, 1942).
FROM FEAST TO FAMINE
57
have access to excellent health care”. This is a much more expansive
vision than Beveridge’s idea of minimum of treatment for those
who could not afford to pay for it.
Bevan’s vision was to “universalise the best”,44 which fits with
Whitehead’s “levelling up” criteria for equity. However, it is worth
noting that the words equity and equality were not mentioned
in early NHS documents.45 This is very likely to be because an
acknowledged definition of equity was not necessary when
the NHS was founded. The prospect of orphan drugs or top-up
payments for cancer care was not anticipated in 1948. This lack
of clarity about equity in the early NHS was demonstrated when
Bevan, appointed Minister of Labour in 1951, resigned in protest at
Hugh Gaitskell’s (then Chancellor of the Exchequer) introduction
of prescription charges for dental care and spectacles – created in
order to meet the financial demands imposed on the budget by the
Korean War. Implicit in this decision seems to be a maximalist view
of equity whereby any form of limitation to free care is considered
inequitable and, therefore, unacceptable. But it is clear that this
view is not sustainable, and has never been reflected in the realities
of the health service.
Developing the idea of equity in the nhs – allocating resources
The NHS (with some exceptions, such as dental and eye care) does
not deny care to people on the basis of their ability to pay. So the
challenge is largely one of distributive equity – making sure that
resources are directed to areas with the greatest need.
Since 1976 healthcare equity has been an explicit part of
resource allocation in the NHS. At that time it was decided that
healthcare should be geographically distributed to ensure equal
access for equal risk. The mechanism through which this was to be
44 T. Delamothe, “Founding Principles”, British Medical Journal 336:7655 (2008).
45 T. Delamothe, “Universality, Equity, and Quality of Care”, British Medical Journal 336:7656 (2008).
SOCIAL MARKET FOUNDATION
58
achieved was the Resource Allocation Working Party (RAWP), which
was appointed to oversee the process.46
As the methodology developed, the RAWP was replaced by the
Advisory Committee on Resource Allocation which, in 1999, added
a new requirement that resource allocation should contribute to
reducing health inequalities.47 This seems to embody a conception
of equity as an equal opportunity to be healthy, which is not the
same as equal access based on need (a definition discussed in the
preceding section).
The NHS model of resource allocation has continued to
develop, and since 2003–4 the AREA model has been in place.
Utilisation is used as a proxy for need in determining the level of
resource an area receives. So, areas where there are high levels
of healthcare utilisation are assumed to have high levels of need.
There are problems with this approach. Adopting utilisation as a
proxy assumes that need is fair; that people can and do access
healthcare only when they need it. This may have the inadvertent
effect of depressing the “need” of areas that have real health
problems, many of which may be connected with a failure to seek
timely medical care.
The Department of Health explains: “A weighted capitation formula
determines each PCT’s target share of available resources, to enable
them to commission similar levels of health services for populations
in similar need, and to reduce avoidable health inequalities.”48 This
formula is based on factors such as educational attainment, birth rate,
low income and morbidity in under 65-year-olds.
46 S. Asthana and A. Gibson, “Health Care Equity, Health Equity and Resource Allocation: Towards a Normative
Approach to Achieving the Core Principles of the NHS”, Radical Statistics 96 (2008).
47 Asthana and Gibson, “Health Care Equity, Health Equity and Resource Allocation”.
48 “About NHS Allocations: Department of Health – Managing Your Organisation”, http://www.dh.gov.uk/en/
Managingyourorganisation/Financeandplanning/Allocations/DH_076547.
FROM FEAST TO FAMINE
59
The methodology adopted to allocate resources is not just
a technical question, but one that reflects the central purpose
of the NHS, and its approach to equity. As the Department of
Health makes clear, the current formula is intended to narrow
health inequalities and, as such, it devotes a greater share
of resources to urban areas that tend to have higher levels of
deprivation. But this approach has been subject to criticism –
described as the “medicalisation of socioeconomic inequality”
by Sheena Asthana.49 More affluent areas tend to have a higher
proportion of older people, and may be relatively underfunded
compared to areas that meet more of the criteria set out by the
current formula, which places a higher emphasis on reducing
health inequalities than on treating actual ill health. In reality,
this might mean that rural areas are disadvantaged relative to
cities because they have an older population, but suffer less from
economic deprivation. Others have criticised the opacity of the
methodology. Nigel Hawkes sums up the mystery that surrounds
the resource allocation process: “Wizards uttering incantations
dance around a cooking pot stocked with tasty data, brewing
up heaven knows what. The light is dim, and understanding is
even dimmer.”50
The resource allocation formula was reviewed in late 2008,
but did not change in response to criticisms about possible bias
against rural areas. There was an acknowledgement, however,
that in defining a resource allocation formula it is impossible to
reconcile need and inequalities. One formula can define need,
while another is needed to define avoidable health inequalities.
It is a ministerial decision as to how much weight is given to the
inequalities formula relative to the need formula in allocating
resources. This was a recommendation of the advisory committee
on resource allocations, “as no technical way of assessing how
49 Quoted in S. Gainsbury, “NHS Inequalities Row Shrouded in Secrecy”, Health Care Analysis (11 September
2008).
50 “Resource Allocation – It’s a Jungle Out There”, British Medical Journal 338 (14 January 2009).
SOCIAL MARKET FOUNDATION
60
much weight should be given to the health inequalities formula
has been found”.51
This shows how far decisions about equity are political rather
than based on clear-cut academic formulae. It also reflects a
wider tension between two definitions of equity. One definition,
connected with health inequalities, sees the NHS as aiming to
offer equal opportunities to be healthy. The other definition,
reflected in the aim of the formula assessing need, sees “equal
opportunity to access health care for people at equal risk”52 as
central to equity.
It is clear that these two competing definitions lead to
significantly different approaches to resource allocation in
healthcare. But what is reflected in the NHS itself? How far does it
meet the equity goals that it sets itself? What follows demonstrates
why a more limited definition of equity, based on equal access
for equal need, is a more appropriate and sustainable goal for the
future of the health service.
equity in the nhs today
The NHS does not in fact provide a horizontally equitable service.
That is to say that people in need do not get the care they should.
Problems may be to do with access (e.g. geographic variations
in care) or institutionalised discrimination (perhaps against older
people). These inequalities are not necessarily connected with the
resource allocation debates described above, but they do reflect
different problems in the NHS.
A 2003 review conducted on behalf of the Number 10 Strategy
Unit concluded that, relative to their need, poorer people were
51 Department of Health, Report of the Advisory Committee on Resource Allocations (London: HMSO, 2008), 3.
52 Department of Health, Report of the Advisory Committee on Resource Allocations, 16.
FROM FEAST TO FAMINE
61
less likely to access healthcare than richer people.53 The authors
speculated that the impact of late presentation of symptoms might
be the main cause of inequity in chronic care, and also looked at
issues such as transport in preventing equal access to care.
Other authors have been much more explicit about the
institutional inequity of the NHS. Nigel Rice and Peter Smith have
raised the problem of geographical inequity:
[V]ery rural communities may suffer a lower level of services
than their urban counterparts, may have to travel further to
secure such services, or may receive healthcare in a different
manner (for example through greater use of telemedicine). The
issue of rurality exemplifies the trade-off that exists between
equity and efficiency in the allocation of health care resources.54
In other words, it is simply not efficient to try and even up
healthcare resources around the country given, for example, the
current distribution of hospitals, throughout England.
The inequitable distribution of healthcare in the UK is also
demonstrated in figure 2.2, which shows GP coverage per 100,000
weighted population. Clearly there is a great deal of variation across
the country.
Another challenge to equity is universal standards of care.
Recent research has pointed out that regardless of the quality of
its advice, NICE guidance is being ignored by many healthcare
professionals. The Healthcare Commission reported that failure
to implement NICE guidance is one of the most common self-
reported failures of compliance to the Healthcare Commission.55
53 Dixon, Is the NHS Equitable?
54 N. Rice and P. C. Smith, “Ethics and Geographical Equity in Health Care”, British Medical Journal 27:4 (2001).
55 Ibid.
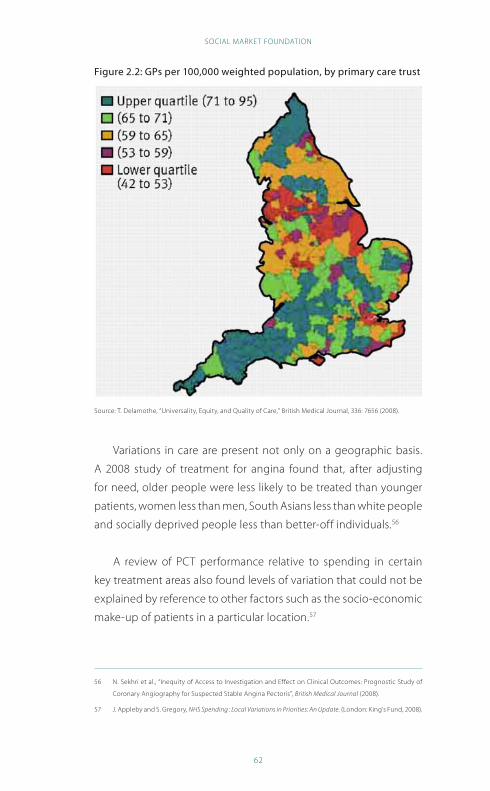
SOCIAL MARKET FOUNDATION
62
Figure 2.2: Gps per 100,000 weighted population, by primary care trust
Source: T. Delamothe, “Universality, Equity, and Quality of Care,” British Medical Journal, 336: 7656 (2008).
Variations in care are present not only on a geographic basis.
A 2008 study of treatment for angina found that, after adjusting
for need, older people were less likely to be treated than younger
patients, women less than men, South Asians less than white people
and socially deprived people less than better-off individuals.56
A review of PCT performance relative to spending in certain
key treatment areas also found levels of variation that could not be
explained by reference to other factors such as the socio-economic
make-up of patients in a particular location.57
56 N. Sekhri et al., “Inequity of Access to Investigation and Effect on Clinical Outcomes: Prognostic Study of
Coronary Angiography for Suspected Stable Angina Pectoris”, British Medical Journal (2008).
57 J. Appleby and S. Gregory, NHS Spending : Local Variations in Priorities: An Update. (London: King’s Fund, 2008).
FROM FEAST TO FAMINE
63
Equity, NHS targets and health inequalities
So there is some compelling evidence that the NHS does not always
meet high standards of horizontal equity and that access to care
can be determined by geography, age, gender, race and income
rather than medical need. This is despite attempts to distribute
resources equitably, and central targets aimed at reducing unequal
access to care.
The long-term future of the health system is local. If the NHS
is to deal with the challenge of a changing population, new
technologies and a funding squeeze related to what may be the
worst recession for many decades, it will have to make decisions
at a local level, and follow through on the policy trends embodied
in the world class commissioning programme. PCTs should be
properly equipped to work with local communities to design
services appropriate to them. This implies that the major aim of
the NHS should be to offer equal care for equal need for a defined
community. Health inequalities, after all, primarily reflect the
differences between rather than within different areas. In terms of
NHS targets, this would result in targets that, instead of focusing
on health inequalities overall, focus on inequalities of access.
What this would look like for the NHS is explored in a discussion of
appropriate NHS targets in chapter 4.
The argument that health services should be charged only
with securing equal access for equal need does not imply that the
importance of health inequalities should be downgraded. In fact,
health inequalities should move up the political agenda. There
has been substantial progress in improving health in the most
disadvantaged groups. Life expectancy for men in the Spearhead
groups (where most attention has been focused) has increased by
more than two and a half years in the period since 1995–7.58
58 Department of Health, Health Inequalities – Progress and Next Steps, 20.
SOCIAL MARKET FOUNDATION
64
However, there are still enormous problems – the gap in life
expectancy between the poorest and richest groups continues
to widen.59 And government policy already admits that a range of
stakeholders, not just the NHS, is needed to try and narrow inequalities.
“The role of central government is crucial – but limited. The most
important actors are local: including primary care trusts, primary care
practices, schools, houses, employers, Jobcentre Plus and community
midwife teams.”60 As the House of Commons Health Committee
concluded: “Measures to enable people to adopt healthier lifestyles
involve a range of government departments. These Departments
could do far more than they do at present.”61 These agencies should not
be coordinated by the NHS, but from a single point within government
with oversight across the whole range of government activity.
Equity in the NHS should be about providing equal access for
equal need in health services. This will mean that health inequalities
no longer form part of the resource allocation formula applied by
the NHS, with the focus shifting instead to providing equal access
to treatment for equal need.
Health inequalities are so important that rather than being
the responsibility of the NHS, they should be overseen by the
whole of government. Government action to deal with health
inequalities should be joined up, with the NHS only one part of a
wider agenda. This is a more appropriate and achievable goal for
health services because:
• the NHS does not currently provide equal access for equal
need;
• health inequalities will not be narrowed by health services
alone but by coordinated government action.
59 Ibid.
60 Ibid., 16.
61 House of Commons Health Committee, Health Inequalities: Third Report of Session 2008–09, Vol. 1 (London:
HMSO, 2009), 7.
FROM FEAST TO FAMINE
65
recommendation 1: central to the concept of equity in the
nhs should be a definition of equal access to equal need.
recommendation 2: a cabinet office minister for health
inequalities should be introduced with responsibility for
coordinating action across government to narrow the
gap in health within the population.
equity in other health systems
The discussion so far has focused on the limitations of a theoretical
approach to equity and traced the development of equity in the
NHS since its inception. A conclusion of this discussion has been
that central to the idea of equity should be equal access for equal
need. But while this might make a difference to how resources are
distributed, there are further implications of how equity is defined,
particularly with regard to patient charging.
The tax-funded NHS is considered broadly equitable. But so are
most other health systems that do not rely on private insurance or
out-of-pocket payments for the bulk of healthcare provision. In fact,
most systems that offer universal coverage are seen as equitable.
However, there is not a clear picture about what equity looks like in
practice. The case of the NHS shows that even with a progressive
system of funding and clear targets to improve horizontal equity,
inequalities remain both in health and access to healthcare. But the
example of other European countries shows that in order to remain
equitable, the NHS should consider implementing policy options
that have hitherto been deemed unacceptable.
the case of user charging
In the UK, user charges are seen as embodying all that is inequitable
about healthcare delivery. This sentiment was expressed by former
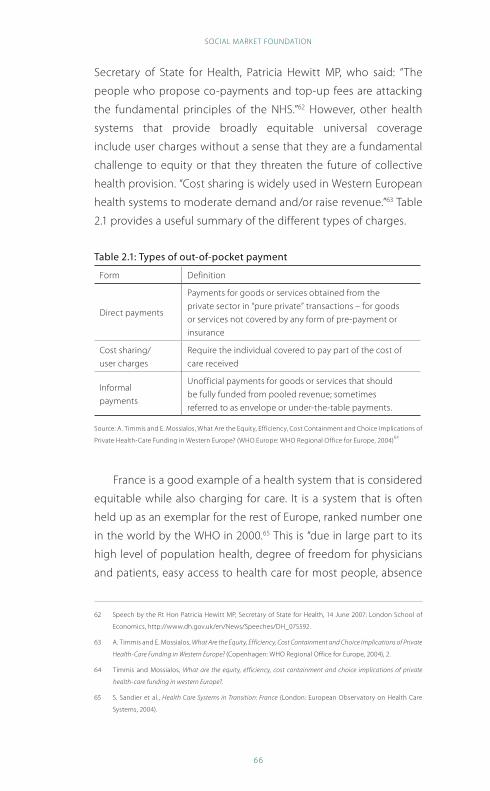
SOCIAL MARKET FOUNDATION
66
Secretary of State for Health, Patricia Hewitt MP, who said: “The
people who propose co-payments and top-up fees are attacking
the fundamental principles of the NHS.”62 However, other health
systems that provide broadly equitable universal coverage
include user charges without a sense that they are a fundamental
challenge to equity or that they threaten the future of collective
health provision. “Cost sharing is widely used in Western European
health systems to moderate demand and/or raise revenue.”63 Table
2.1 provides a useful summary of the different types of charges.
table 2.1: types of out-of-pocket payment
Form Definition
Direct payments
Payments for goods or services obtained from the
private sector in “pure private” transactions – for goods
or services not covered by any form of pre-payment or
insurance
Cost sharing/
user charges
Require the individual covered to pay part of the cost of
care received
Informal
payments
Unofficial payments for goods or services that should
be fully funded from pooled revenue; sometimes
referred to as envelope or under-the-table payments.
Source: A. Timmis and E. Mossialos, What Are the Equity, Efficiency, Cost Containment and Choice Implications of
Private Health-Care Funding in Western Europe? (WHO Europe: WHO Regional Office for Europe, 2004)64
France is a good example of a health system that is considered
equitable while also charging for care. It is a system that is often
held up as an exemplar for the rest of Europe, ranked number one
in the world by the WHO in 2000.65 This is “due in large part to its
high level of population health, degree of freedom for physicians
and patients, easy access to health care for most people, absence
62 Speech by the Rt Hon Patricia Hewitt MP, Secretary of State for Health, 14 June 2007: London School of
Economics, http://www.dh.gov.uk/en/News/Speeches/DH_075592.
63 A. Timmis and E. Mossialos, What Are the Equity, Efficiency, Cost Containment and Choice Implications of Private
Health-Care Funding in Western Europe? (Copenhagen: WHO Regional Office for Europe, 2004), 2.
64 Timmis and Mossialos, What are the equity, efficiency, cost containment and choice implications of private
health-care funding in western Europe?.
65 S. Sandier et al., Health Care Systems in Transition: France (London: European Observatory on Health Care
Systems, 2004).
FROM FEAST TO FAMINE
67
of waiting lists for treatment and universal coverage”.66 This ranking
was achieved with a funding system that would be politically
unacceptable in the UK.
The French system provides comprehensive coverage and is
mainly funded through statutory health insurance. Patients pay for
their treatment and are then reimbursed (with some exceptions
such as cosmetic treatments and those of unproven effectiveness).
However, reimbursement does not extend to the total cost of
treatment, with higher levels of charges for outpatient care and
pharmaceutical products and lower levels for hospital treatment. In
2000, these user charges raised 11.1% of total health expenditure.67
This is a far greater proportion than private spending in the UK. Figure
2.1 (above) showed the relatively minor role of private payments in
the UK relative to other OECD countries, including those that are (a)
also considered equitable and (b) higher performing.
It is clear that a broad conception of “equity” allows for great
variation in health system design, including the option to charge
users for healthcare. Chapter 3 contains a full discussion of potential
user charges in the UK, including a recommendation that some
limited charges be introduced for those who can afford to pay,
in order to reduce demand. But it is clear from the international
evidence that charges are not the affront to the fundamental
principles of the NHS that some have argued. The authors of an
OECD study rightly maintain that universal coverage is the basis of
an equitable health system, but demonstrate that many systems
can flourish within this broad definition:
In Switzerland, mandatory health insurance is the sole
source of cover for the entire population. Some countries’
public insurance rules, like Australia, Belgium, Finland,
66 Ibid.
67 Ibid.
SOCIAL MARKET FOUNDATION
68
France, Norway and Portugal, require their insured to pay co-
payments which vary depending on the type of services, while
in many other countries (like Denmark, Canada, Germany,
Spain, Portugal and the UK) visits to public sector doctors are
free at the point of delivery. In yet other countries, like Hungary
and Greece, care is officially free at the point of delivery but, in
practice, unofficial payments to doctors are widespread.68
The NHS should not be considered inequitable simply because it
charges those who can afford to pay for some services including
dental care and prescriptions. Health systems with varied sources
of funding can be considered equitable, and the example of user
charges shows that what is considered a fundamental principle in
one country is not considered so important in another. In fact, about
the only thing that “equitable” health systems have in common
is an idea of universal access: that patients should have access to
healthcare whatever their income. The defining characteristic of an
equitable health system is therefore universal access, not a limited
notion that services should be “free at the point of use”.
a definition of equity for the nhs
The European Observatory on Health Systems and Policies defines
equity thus: “The principle of being fair to all, with reference to a
defined and recognised set of values.”69 What is the NHS’s defined
and recognised set of values? An important product of Lord Darzi’s
Next Stage Review was the NHS Constitution, published early in
2009.70 It contains a list of NHS values, namely:
• respect and dignity;
• commitment to quality of care;
68 E. Van Doorslaer and C. Masseria, “Income-Related Inequality in the Use of Medical Care in 21 OECD
Countries”, in OECD, Towards High-Performing Health Systems (2004).
69 “European Observatory on Health Systems and Policies - Equity”, http://www.euro.who.int/observatory/
Glossary/TopPage?phrase=Equity.
70 Department of Health, The NHS Constitution: The NHS Belongs to Us All (London: HMSO, 2009).
FROM FEAST TO FAMINE
69
• compassion;
• improving lives;
• working together for patients;
• everyone counts.
However, it did not address wider debates about NHS values,
including the discussion of equity outlined throughout this
chapter. In the context of scarce public resources, and a change to
the charging structure of the NHS, the health system must develop
a new definition of values reflecting the reality of healthcare in this
country. There are limitations to a purely theoretical approach, and
it is essential that a set of values is accessible and comprehensible
to people who use health services.
The SMF Health Project public opinion research revealed
that fairness remains a central priority when it comes to health
services, though the research showed that people have different
understandings of what this actually means in practice. Some
prefer the idea that health services are the same across the country,
while others think that services should be distributed according to
local need.71 For both groups, charging for some services was an
option discussed to safeguard the continuation of universal health
services overall. But their different understandings of fairness
suggests that there is a need for a defined set of NHS values that
would make clear what is actually the case in health services –
that services are different in different locations, and that people
contribute according to their means.
recommendation 3:
an nhs set of values should include:
• universal access: no one should be excluded from
necessary treatment because of an inability to pay,
but those who can afford it should contribute more;
71 Furness, Local Control and Local Variation in the NHS.
SOCIAL MARKET FOUNDATION
70
• a comprehensive range of services: the nhs should
provide a comprehensive range of services that
offers good value for money;
• equal access to treatment: the nhs should make sure
that everyone has equal access to treatment regardless
of age, gender, income or ethnic background;
• local services for local need: the nhs should
provide a range of services appropriate for different
local areas; pcts should work with local people to
decide what is needed and to justify the difference
between different areas.
These defined values reflect a new understanding of the role and
capacity of health services. They reflect a realistic assessment of the
need to maintain universal access in a time of scarcity, with an open
acknowledgement of limitations and the need for wealthier people
to pay more if they can afford it. Furthermore, these values reflect
the local priorities that will be necessary if the NHS is to manage
public expectation and maintain public support for a tax-funded
health system.
Equity is an essential principle for health services. But it is
clear that definitions of equity are many, and their application
is inconsistent and encompasses many potential systems of
healthcare delivery. By defining NHS values more carefully,
government can safeguard public support for a system of universal
access that, while it might not have satisfied Nye Bevan, is a realistic
assessment of the future of his creation.
conclusion
Equity will continue to play a central role in determining the future
design of the health system. However, equity should be clearly
FROM FEAST TO FAMINE
71
defined in a set of codified NHS values rather than being a vague
aspiration. As part of this move towards a clear definition of equity,
the NHS should no longer be primarily responsible for narrowing
health inequalities and should instead focus on ensuring that
individuals have equal access to treatment when they fall ill. Health
inequalities are a task for the whole of government, and should
be the responsibility of a minister in the Cabinet Office who can
coordinate the action of multiple agencies.
But equity should not be as narrowly defined as it is in the
current political debate about healthcare in England. Many other
health systems are considered equitable that have systems of
funding and charges that would not be politically acceptable here.
The crisis in public finances means that what is considered fair
now may not be desirable in the future. There is a great need for a
clearly defined set of values for the NHS that will provide a guide
for policymakers and also help to engage the public in the difficult
decisions that lie ahead.
SOCIAL MARKET FOUNDATION
72
chapter three: payinG For healthcare
The prognosis for the public finances is dire. The economy is in
recession, with a consequent fall in tax revenues and a massive
increase in expenditure, both reflected in unprecedented levels
of government borrowing. While public spending continues
apace in the short term to stave off depression, the outlook for
the coming decade is a sharp spending squeeze once the worst
of the recession is over. It is in this uncertain context that it is
vitally important to look again at the future financing of public
services. The NHS has been the beneficiary of record levels of
investment in recent years, but the days of largesse are over. The
research presented below analyses prospects for NHS spending
in an economic downturn. It also examines the potential for
increased private payments in the UK health system and includes
a number of policy proposals. It looks at the likely development of
private finance for healthcare over the long term, and examines
what can be learnt from the example of other international
health systems.
It is vitally important that the political debate about healthcare
develops to become an open and honest discussion concerning
the challenges facing the health system in the years ahead. This
discussion is necessary to ensure that the bold reforms that will
be necessary to guide the NHS through the downturn are put into
place. If this fails to happen it will be the least well-off members of
society who are most badly affected as it is they who rely most on
publicly funded health services.
public services and the downturn
Health services have been one of the main beneficiaries of the
extraordinary levels of public spending that we have seen in the
past few years. As Carl Emmerson of the Institute for Fiscal Studies
(IFS) put it, as public spending increased “the NHS was one of the
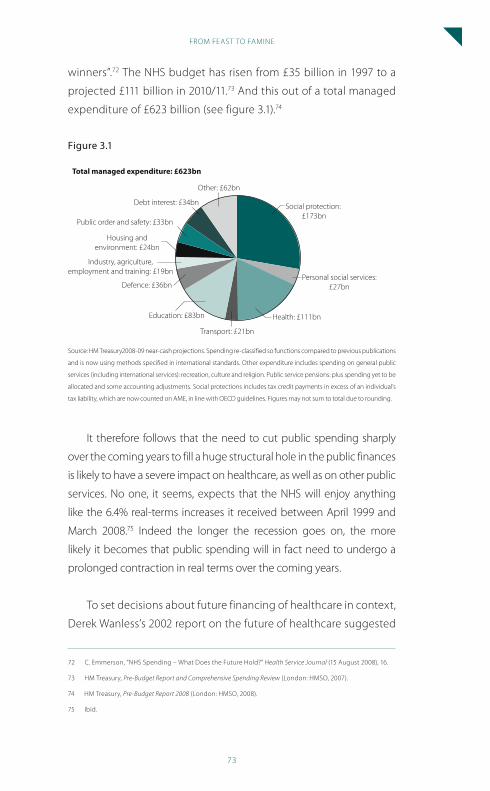
FROM FEAST TO FAMINE
73
winners”.72 The NHS budget has risen from £35 billion in 1997 to a
projected £111 billion in 2010/11.73 And this out of a total managed
expenditure of £623 billion (see figure 3.1).74
Figure 3.1
Social protection: £173bn
Personal social services:£27bn
Health: £111bn
Transport: £21bn
Education: £83bn
Defence: £36bn
Industry, agriculture,employment and training: £19bn
Housing andenvironment: £24bn
Public order and safety: £33bn
Debt interest: £34bn
Other: £62bn
Total managed expenditure: £623bn
Source: HM Treasury2008-09 near-cash projections. Spending re-classified so functions compared to previous publications
and is now using methods specified in international standards. Other expenditure includes spending on general public
services (including international services): recreation, culture and religion. Public service pensions: plus spending yet to be
allocated and some accounting adjustments. Social protections includes tax credit payments in excess of an individual’s
tax liability, which are now counted on AME, in line with OECD guidelines. Figures may not sum to total due to rounding.
It therefore follows that the need to cut public spending sharply
over the coming years to fill a huge structural hole in the public finances
is likely to have a severe impact on healthcare, as well as on other public
services. No one, it seems, expects that the NHS will enjoy anything
like the 6.4% real-terms increases it received between April 1999 and
March 2008.75 Indeed the longer the recession goes on, the more
likely it becomes that public spending will in fact need to undergo a
prolonged contraction in real terms over the coming years.
To set decisions about future financing of healthcare in context,
Derek Wanless’s 2002 report on the future of healthcare suggested
72 C. Emmerson, “NHS Spending – What Does the Future Hold?” Health Service Journal (15 August 2008), 16.
73 HM Treasury, Pre-Budget Report and Comprehensive Spending Review (London: HMSO, 2007).
74 HM Treasury, Pre-Budget Report 2008 (London: HMSO, 2008).
75 Ibid.
SOCIAL MARKET FOUNDATION
74
that even in the most optimistic of scenarios (in which the health
service becomes much more productive, and people take better
care of their health) health services would require average real-
terms increases in spending of 4.4% up to 2012/13 to achieve
continued improvement. His least optimistic scenario suggested
that spending would need to rise by 5.6% per annum.76
PricewaterhouseCoopers recently published an analysis suggesting
that the government faces a fiscal gap of around 3% of GDP by 2013/14
– equivalent to around £43 billion at today’s prices. The options for
meeting this gap are not palatable – an unprecedented freeze in
spending, or a slowing in spending increases that would still require
extra taxation of around £25 billion.77 The 2009 budget confirmed
much of this message, with the Chancellor announcing that public
services will see average real-terms rises of 0.7% from 2011 to 201478
– way below the level of increases that have previously been enjoyed
by the NHS and which have generally been seen as the minimum for
continued improvement in quality. An IFS analysis of the 2009 budget
concluded that the situation for departmental expenditure limits (DELs)
spending would be even worse. Departments, of which the NHS is the
largest, can expect annual spending decreases in real terms of 2.3%
between 2011 and 2014 (see figure 3.2).
In addition to a slowdown in funding, the public sector will be
required to find £9 billion of annual efficiency savings by 2013–14.79
Chief Executive of the King’s Fund, Niall Dickson, has said: “This is a wake
up call for the health service – no matter who is in power from 2011 the
NHS will have to manage with very low or no growth in its funding.”80
76 D. Wanless Securing Our Future Health – Taking a Long Term View (London: HMSO, 2002), 75.
77 J. Hawksworth and N. Jones, Dealing With Debt: Reforming Public Services and Narrowing the Fiscal Gap
(London: PricewaterhouseCoopers, 2009).
78 HM Treasury, Budget 2009: Building Britain’s Future (London: HMSO, 2009), ch. 6.
79 Ibid., 123.
80 “Budget a Wake-Up Call for the Health Service Ahead of 2011 Budget Squeeze”, http://www.kingsfund.org.
uk/what_we_do/press/budget_a_wakeup.html.
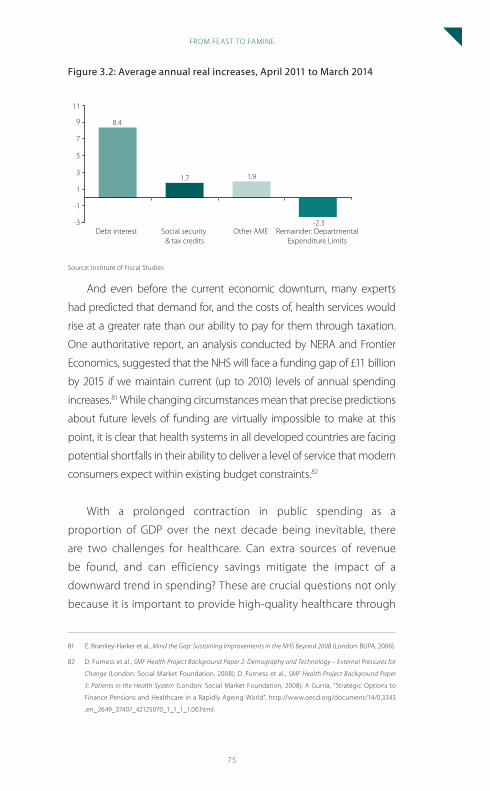
FROM FEAST TO FAMINE
75
Figure 3.2: average annual real increases, april 2011 to March 2014
-3
-1
1
3
5
7
9
11
8.4
Ave
rage
ann
ual r
eal i
ncre
ase
Debt interest Social security & tax credits
Other AME Remainder: DepartmentalExpenditure Limits
1.7 1.9
-2.3
Source: Institute of Fiscal Studies
And even before the current economic downturn, many experts
had predicted that demand for, and the costs of, health services would
rise at a greater rate than our ability to pay for them through taxation.
One authoritative report, an analysis conducted by NERA and Frontier
Economics, suggested that the NHS will face a funding gap of £11 billion
by 2015 if we maintain current (up to 2010) levels of annual spending
increases.81 While changing circumstances mean that precise predictions
about future levels of funding are virtually impossible to make at this
point, it is clear that health systems in all developed countries are facing
potential shortfalls in their ability to deliver a level of service that modern
consumers expect within existing budget constraints.82
With a prolonged contraction in public spending as a
proportion of GDP over the next decade being inevitable, there
are two challenges for healthcare. Can extra sources of revenue
be found, and can efficiency savings mitigate the impact of a
downward trend in spending? These are crucial questions not only
because it is important to provide high-quality healthcare through
81 E. Bramley-Harker et al., Mind the Gap: Sustaining Improvements in the NHS Beyond 2008 (London: BUPA, 2006).
82 D. Furness et al., SMF Health Project Background Paper 2: Demography and Technology – External Pressures for
Change (London: Social Market Foundation, 2008); D. Furness et al., SMF Health Project Background Paper
5: Patients in the Health System (London: Social Market Foundation, 2008); A Gurria, “Strategic Options to
Finance Pensions and Healthcare in a Rapidly Ageing World”, http://www.oecd.org/document/14/0,3343
,en_2649_37407_42125070_1_1_1_1,00.html.
SOCIAL MARKET FOUNDATION
76
the NHS, but also because it is questionable whether public support
for the health system can be maintained if the NHS fails to continue
its recent improvement. A failure to find more money and/or make
significant economies could be the end of the current political
settlement in healthcare that has existed for the past 60 years.
Part Two of this report presents a series of recommendations
for efficiency savings in the health system that can be achieved
through high-quality commissioning. As a means of achieving
improved commissioning, this report also recommends new
accountability mechanisms and a new responsibility for designing
locally varied services that will enable local health commissioners
to engage their local populations. But, as chapter 6 makes clear, it is
difficult to quantify the likely savings associated with improvements
in commissioning. It seems unlikely that efficiency savings will be
enough to deal with the severe squeeze in NHS budgets that is
now imminent. In this chapter we will therefore consider whether
changes to the way the health system raises revenue could be used
as a way either to increase resources or to manage demand.
This chapter explores the potential of increasing revenue for
the NHS from sources other than taxation, and also considers
options for limiting expenditure. Such issues raise a huge number
of questions that go to the heart of what the NHS was set up to
achieve. Would the introduction of private payments be desirable
for the NHS? What might their impact be on health finances,
service for patients and fairness in accessing healthcare? While
private payment for public services has, since the inception of the
NHS, largely been seen as undesirable, it is clear that people are
willing to pay for products they believe will help them to secure
good health. Complementary and alternative therapies thrive, as
do health, fitness and nutritional services. Can this willingness to
pay for good health be translated into a systematic willingness to
pay for good healthcare? The discussion in this chapter is informed
by a series of public opinion polling and discussion groups that
FROM FEAST TO FAMINE
77
explored how people would choose to make up shortfalls in
health budgets.83
puBlic willinGness to pay For healthcare
It is clear that in our society there is a general willingness to spend
money on good health. This raises a question about whether there are
ways to translate this willingness to pay for health and healthcare into
new sources of funding for the NHS. Anecdotally, the popularity of gym
memberships, vitamin supplements and “detox” programmes supports
the idea that the public is willing to make a financial commitment
to maintaining good health. It has been suggested that it might be
possible to harness this willingness to pay for good health and translate
it into an extra revenue stream for the NHS. This section of the report
looks at the evidence for general health spending and what motivates
it, before drawing some conclusions for the future of the NHS.
what does the public spend on good health?
This section considers health expenditure that does not fall under the
category of conventional healthcare. Taxation and National Insurance,
private medical insurance or self-payments for hospital treatment are not
relevant here. In general, the focus here is on complementary and alternative
medicines, physical exercise equipment and related subscriptions (gym
memberships), nutritional supplements and “health” foods. However, this
list is not exhaustive, as this sector is not coherently defined. Despite this,
there is convincing evidence that it is growing, perhaps indicating that
people are increasingly interested in securing improved health.
A meta-analysis of studies of the use of complementary and
alternative medicine (CAM) found that true prevalence is difficult
to measure. However, “the data suggest that complementary/
83 D. Furness and B. Gough, Local Control and Local Variation in the NHS (London: Social Market Foundation,
2009).
SOCIAL MARKET FOUNDATION
78
alternative medicine are used frequently and increasingly”.84
Thomas et al. conclude that around 10% of the population in
England use CAM in a given year, representing expenditure of about
£450 million.85 The House of Lords select committee investigation
concluded: “These rather limited data seem to support the idea
that Complementary and Alternative Medicine use in the United
Kingdom is high and is increasing.”86
The Stockholm Network has estimated the global health and
wellbeing industry at £1 trillion, with a total UK market of over £11
billion.87 It reports “exponential” growth in health spending, with a
58% increase in the sale of over-the-counter medicines between
1997 and 2007 and a 678% increase in sales of physical exercise
equipment from 1990 to 2000.88
The exact figures in this area are less important than the clear
scale of spending. Over recent years, the NHS has found itself
highly concerned with deficits and surpluses of around £1 billion.
Surely, then, it might be possible to translate some of the evident
spending on good health into extra revenue for a cash-strapped
health service? Unfortunately, the reality is not so simple.
why do people choose to spend money on health-related
products?
There are many different reasons why people choose to spend
money on health-related products. While some are straightforward
– people join gyms to benefit from easier access to physical exercise
84 E. Ernst, “Prevalence of Use of Complementary/Alternative Medicine: a Systematic Review,” Bulletin of the
World Health Organisation (2000): 78.
85 K. J. Thomas, J. P. Nicholl and P. Coleman, “Use and Expenditure on Complementary Medicine in England: a
Population Based Survey”, Complementary Therapies in Medicine 9:1 (2001).
86 House of Lords Science and Technology Committee, Complementary and Alternative Medicine (London:
HMSO, 2000).
87 D. Torstensson and G. Isyanova, A Healthy Market? The Health Quality Agenda (The Stockholm Network,
2008).
88 Ibid., 17.
FROM FEAST TO FAMINE
79
– others are less obvious. For example, Dr Ben Goldacre, author of the
well-known Bad Science blog, argues that the current popularity of
“detox” products that claim to cleanse the body of harmful elements
is in fact an updated version of ancient purification rituals, with most
products no more effective than a glass of water and a rest.89
Most of the literature in this area is concerned with why people
choose to use CAM, with relatively less attention paid to other
health-related products such as vitamin supplements. There is a
limited amount of CAM available through NHS referral and the vast
majority is privately funded. There are some important lessons
for the future of the NHS to be learned from understanding why
individuals choose to spend money outside the conventional
health system.
The data here is subject to some serious limitations. CAM users
are not distinct from users of health services in general, and much
usage is occasional, periodic and may not reflect a wider outlook
on health services. However, it is possible to make some broad
generalisations from examining studies both of disease-based
cohorts and CAM users in general.
Motivations for choosing CAM can generally be divided
into “push” and “pull” categories. “Push” factors might include a
dissatisfying experience with conventional medicine, while “pull”
factors include a worldview that correlates with that espoused by a
particular form of CAM.
Ong and Banks, writing for the Federation for Integrated Health,
offer an example of this push/pull or negative/positive typology for
those who choose complementary and alternative medicines:90
89 B. Goldacre, “Detox Debunked”, Sunday Times (18 January 2009), http://www.timesonline.co.uk/tol/
life_and_style/health/features/article5517912.ece.
90 C. K. Ong and B. Banks, Complementary and Alternative Medicine: The Consumer Perspective (London: Prince of
Wales’s Foundation for Integrated Health, 2003).
SOCIAL MARKET FOUNDATION
80
Negative
• poor outcomes from conventional treatment;
• adverse reaction to pharmaceuticals;
• negative doctor–patient relationship;
• anti-conventional view of health.
Positive
• good outcome from CAM;
• active participation in care;
• positive doctor–patient CAM relationship;
• view of their own health is in line with principles espoused
through CAM.
This description is fairly typical of the literature. It is significant to
note that different types of people in different countries all tend to
ascribe particular significance to the “holism” of CAM as compared
to conventional medicine. In this sense, CAM treats the “whole
person”, while conventional medicine is seen sometimes as treating
merely the illness. This holistic view ascribes more importance to an
individual’s values and perceptions. Italian mental health patients
and US army veterans were just two very different groups where
research found that this holistic approach was a key motivation for
choosing CAM.91
In the context of the increasing popularity of CAM it is possible
that this “pull” motivation of a holistic approach is becoming ever
more significant. Sirois compared data on CAM consumers in 1997–
8 and 2005 to investigate whether there was any change in why
people chose to access CAM. The study identified “[a] shift towards
91 K. Kroesen et al., US Military Veterans’ Perceptions of the Conventional Medical Care System and Their Use
of Complementary and Alternative Medicine (Oxford: Oxford University Press, 2002); N. Pellegrini and M.
Ruggeri, “The Diffusion and the Reason for the Use of Complementary and Alternative Medicine Among
Users of Mental Health Services: a Systematic Review of Literature,” Epidemiologia e Psichiatria Sociale 16:1.
FROM FEAST TO FAMINE
81
motivations focusing more on the positive aspects of CAM and less
on the negative aspects of conventional medicine … for the 2005
consumers”.92 So, the use of CAM is becoming more widespread,
and seems to be linked to a feeling that a holistic approach to
medicine is more desirable than the medicalised approach of
conventional health services.
Our research suggests that it would be very difficult to translate
the enormous private spending on health (as opposed to private
healthcare) into extra revenue for the NHS. The evidence suggests
that the variety of motivating factors behind choosing CAM
(though there is evidence that holism is particularly important) will
make it difficult for policymakers to direct this spending into the
collectively funded health system. It is not correct to see spending
on CAM and other health products as substitutes for conventional
healthcare. Indeed, it is clear that patients often choose to spend
money on alternative medicine precisely because it is not part of
the conventional health system. It is therefore difficult to see how
the large amounts of money spent each year on a whole range
of health and wellbeing products could be translated into extra
resources for the NHS. Despite this, there are some important
lessons for the future of the NHS. Most important, while it may not
be possible to move spending on wellbeing-related products into
the public health system, the market for health indicates a general
willingness to pay for healthcare. This has implications for the NHS,
particularly with regard to charging. This issue is explored in greater
detail later in this chapter.
iMplications For the health systeM
satisfaction rates and pcts
Measuring satisfaction rates for healthcare will become increasingly
92 F. M. Sirois, “Motivations for Consulting Complementary and Alternative Medicine Practitioners: A
Comparison of Consumers From 1997 and 2005”, BMC Complementary and Alternative Medicine 8:1 (2008).
SOCIAL MARKET FOUNDATION
82
important as PCTs become more responsive to the wants and needs
of their local populations. It is clear from the evidence that many
diverse groups choose CAM because it offers a “whole person”
service – something not always found in conventional healthcare
settings. This insight offers PCTs the potential to raise satisfaction
rates with local healthcare services by encouraging a clinical
approach that recognises the importance of treating the whole
person, not simply managing an illness. There is great potential for
GP-led health centres which hold within them a range of clinical
services to develop into local “wellness centres” that will engage
with individuals who particularly value a holistic service and
who may currently be investing money in ineffective alternative
medicine, possibly to the detriment of their overall health.
recommendation 4: the desire to access ‘holistic’
medical services indicates that pcts could improve
satisfaction rates by offering patients a greater array
of support services to help manage the whole of their
health, not just their illness.
recommendation 5: Gp led health centres should be
promoted as ‘wellness centres’ to engage individuals
who particularly value a holistic service, and counter
concerns that they will lead to a more impersonal form of
medical treatment.
spending on health and wellbeing and nhs charging
While the data is not perfect, there is certainly a substantial market
in the UK for health and wellbeing products in general, and CAM
in particular. This indicates a willingness by individuals to invest
financially in their own good health. A review of the evidence
FROM FEAST TO FAMINE
83
about CAM users found little correlation between high income and
use of CAM; a stronger association was found with higher levels of
education.93 So it is not just the very wealthy who choose to spend
money on health and wellbeing – it is true of all sorts of people.
And some aspects of health and wellbeing spending are certainly
high – gym membership rates can often exceed £50 per month.
In this context, it is appropriate to question why the political debate
over healthcare attaches such a high priority to the principle of “free”
healthcare for everyone – even those who are wealthy enough to
spend large amounts on CAM and gym memberships. This spending
indicates that many people are willing to monetise decisions about
their health and wellbeing. Our research with members of the public
also demonstrated that people are willing to countenance charging
if public resources are scarce. Government and NHS decision-makers
can use this insight to encourage an open and honest public debate
about the need to levy charges on some individuals in order to
safeguard the accessibility of healthcare for the poorest people and
those in ill health. How this might work is explored below.
recommendation 6: Many individuals are willing to
prioritise their health in financial terms. local and
national decision-makers in healthcare must engage
people in a realistic discussion about adequate levels of
resources in health services.
the Future oF “top-up” payMents
The discussion so far has been of the potential to integrate private
spending on health into the health system itself. This section
93 F. L. Bishop and G. T. Lewith, “Who Uses CAM? A Narrative Review of Demographic Characteristics and
Health Factors Associated With CAM Use”, Evidence-Based Complementary and Alternative Medicine (2008).
SOCIAL MARKET FOUNDATION
84
examines the possible future of top-up payments that have only
recently been introduced into the NHS. The newly changed rules,94
following a review by Professor Mike Richards, mean that patients
can now purchase privately drugs that are not available on the
NHS and, if they are administered privately, continue to receive
publicly funded treatment. Before this change, individuals who
purchased privately drugs that were not approved by NICE had
their NHS care withdrawn.
Central to this discussion is a consideration of the potential
for top-up payments to undermine public support for the NHS
model, which, until now, has generally been based on the idea
that care provided for all patients is of the same standard. While
“hotel” services such as bedside phone services have been paid
for by individual patients for some time, it is a new approach to
allow certain privately funded treatments to be delivered alongside
NHS care. Opponents of top-up payments have argued that this is
simply the beginning of a gradual process of defining an NHS core
package of minimum treatments and allowing wealthier individuals
to purchase an enhanced package of care. Despite this concern,
there is little evidence that the introduction of top-ups allows for
such a change. The range of treatment subject to top-up payments
is extremely limited – generally restricted to expensive cancer
drugs that have not been judged cost-effective by NICE. There are
few areas of medicine where there is so clear a line between what
is a “core” service and what is a “supplementary” service where
patients can top-up their NHS entitlement. In other words, without
radical action to exclude a large range of current treatments from
NHS funding, the prospect for the introduction of top-up payments
to lead inevitably to a core package is extremely limited. Instead, as
the following discussion demonstrates, it is more likely that top-ups
will remain on the margins of the health system.
94 Department of Health, Improving Access to Medicines for NHS Policy: A Report for the Secretary of State for
Health, by M Richards (London: HMSO, 2008).
FROM FEAST TO FAMINE
85
Following the change to NHS rules, it is still too early to tell
what effect the introduction of top-ups is having. There are clearly
equity challenges to overcome, as many poorer people will simply
never be able to afford the same access to medicines as those with
higher incomes. But it may be that the public mood on this issue
has shifted. A Populus poll conducted in late 2008 found that 71%
of people agree that “It is right to give people the chance to buy
treatments the NHS is unable to provide”. Of those polled, 77%
believed that the new system of top-ups was fairer, or no more
unfair, than the system it replaced.95 It would seem appropriate
to conclude that people would rather face the equity challenges
of this new system than to “level down” and deny all individuals
the chance to purchase potentially efficacious new drugs. This
reduces the possibility that top-ups will undermine overall support
for a universal public health system – people are realistic about
the limits of what can be provided, and where individuals should
bear more of the financial risk for expensive medicines that are not
necessarily cost-effective.
But what is the possible future for top-up payments? There are
several potential scenarios, detailed below:
• top-up payments remain on the margins of the health
system, affecting only a tiny minority of patients;
• mechanisms evolving from the collection of top-up
payments enable the NHS to introduce across-the-board
co-payments;
• a greater focus on eradicating ineffective treatments leads
to a much bigger market for top-ups, covering a whole
range of unfunded treatments.
The discussion below considers these scenarios and their
implications.
95 “NHS Top Ups Poll Summary”, http://www.populus.co.uk/uploads/NHS_top_ups.pdf.
SOCIAL MARKET FOUNDATION
86
The issue of access to drugs is prominent in the political
debate on health. PCTs are required by the NHS Constitution to
offer access to NICE-approved treatments, and the Richards review
makes provision for patients who wish to top up their NHS care
with non-approved medicines. At the moment this ruling affects
only a very small number of patients, and relatively few drugs have
been rejected by NICE on cost-effectiveness grounds. However,
despite the fact that the overall drugs bill is unlikely to destabilise
the financial state of the NHS, it seems probable that many more
expensive health technologies will become available in the next
decade.96 So, the likelihood is that top-ups will become ever more
significant, rather than simply remaining a marginal concern for
only a very few individuals. Furthermore, the pressure on public
finances over the years to come implies that NICE is likely to
maintain a hard line on treatments it does not consider can be
justified on the grounds of cost-effectiveness.
But what will be the impact of a more prominent role for top-
ups in NHS care? It is likely that insurers will play a bigger role in
insuring individuals against the possibility of requiring non-NICE-
approved treatment – the development of a genuine market in
top-up products is on the cards. There are already examples of this,
such as with WPA’s “My Cancer Drugs” policy, but more products of
this type should be expected. A spokesman for the Association of
British Insurers told the BBC: “Potentially the market is enormous.”97
The key issue here is where government draws the line at topping
up. At the moment, patients can top-up only for non-NICE-approved
drugs. But there are many areas of private treatment where patients
might choose to “mix and match” with NHS care – from private rooms
to post-operative rehabilitation. The years to come are likely to see
96 Furness et al., SMF Health Project Background Paper 2: Demography and Technology – External Pressures for
Change.
97 G. Satchell, “Insurers Eye NHS Top Ups Market”, http://news.bbc.co.uk/1/hi/health/7669230.stm, accessed
17 April 2009.
FROM FEAST TO FAMINE
87
many more patients demanding to top up different aspects of their
care where they want more than the NHS can provide. Now that the
principle has been established that “It is right to give people the chance
to buy treatments the NHS is unable to provide”, it will be hard, and
perhaps impossible, for government to deny people the opportunity
to buy what they want. The next decade will see a thriving market in
insurance-based products that offer supplements to NHS care. These
will complement existing private medical insurance products that
offer an alternative to the NHS for some treatments.
It is certainly possible that the NHS will develop payment
mechanisms that would enable the wholesale extension of co-
payments into other areas of provision. Patients will have to pay
somehow for the private drugs and staffing time that supplements
NHS standards if they choose to top up, and these amounts will not
be trivial. High-quality procedures will develop, most likely through
PCTs, to collect money from patients. This does not mean that co-
payments are likely to become widespread. The evidence set out
in this chapter indicates that while there is merit in the argument
to introduce a limited range of charges in an attempt to lessen
the free rider problem, there is no justification for systematic co-
payments in the NHS. Despite this, top-ups mean that the NHS is
further advanced in its ability to charge, perhaps offering options
to policymakers that have hitherto been impractical.
Most importantly, top-up payments make explicit the
rationing that has always been a largely unacknowledged feature
of healthcare in the UK. The debate over top-up payments has
at its heart an acceptance that there are certain things that the
NHS cannot or will not pay for. And research carried out by the
SMF shows that patients are willing to consider charging and
decommissioning of services to ensure the most efficient use of
NHS resources,98 especially in a severe economic downturn. Because
98 Furness and Gough, Local Control and Local Variation in the NHS.
SOCIAL MARKET FOUNDATION
88
of this, the most profound implication of top-up payments is likely
to be that they enable government and the NHS to engage in an
open debate about the limitations of care, and where cuts might be
made or charges imposed. In this discussion, the key player is the
PCT. PCTs are central to the sustainability of the NHS as they have
the responsibility of working with local people to design a range
of services appropriate to the needs of a particular area. So, PCT
accountability mechanisms become ever more important as the
implications of top-up payments become known. A full discussion
of commissioning and appropriate accountability mechanisms is
included in chapters 6 and 7 of this report.
private payMents
The preceding sections have established that there is a clear
willingness to pay for good health expressed in a thriving market
for health-related products. While this spending may not be easily
translated into systematic contributions to the NHS, it does add to
the sense that some form of private payment in healthcare may
be acceptable to the public. The recent change to allow top-ups
in NHS care are a further indication of changing public views, with
a majority of people in favour of this blurring of the lines between
public and private care. However, it does not seem desirable that
top-ups should develop in order that health spending can be
managed through the gradual establishment of a core package
of NHS treatments. The practical and political difficulties of this
approach, coupled with evidence suggesting that core packages
often do not achieve their goals, mean that this is the wrong route
for the NHS to take. There is far more potential to have an impact
on the financial sustainability of health services through private
payments. If the NHS is not to become a minimal system excluding
many forms of treatment, then the only possible option is to see
whether revenue can be raised and/or demand for health services
constrained through a limited range of private payments. This
section examines the evidence for the impact of private payments
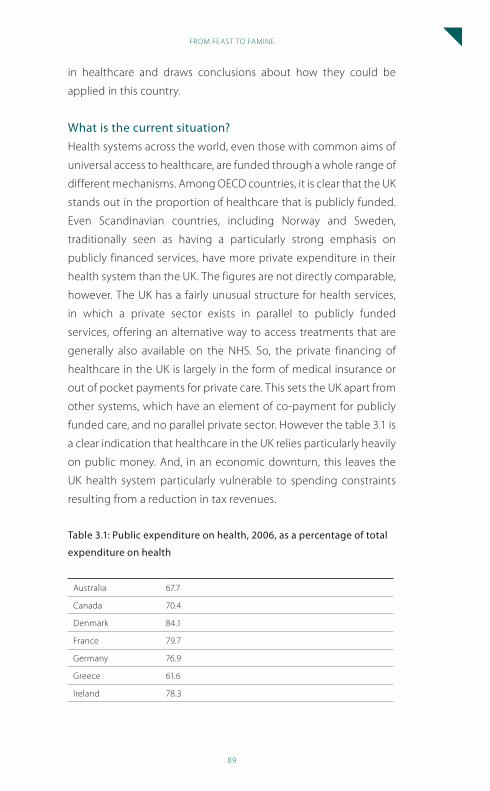
FROM FEAST TO FAMINE
89
in healthcare and draws conclusions about how they could be
applied in this country.
what is the current situation?
Health systems across the world, even those with common aims of
universal access to healthcare, are funded through a whole range of
different mechanisms. Among OECD countries, it is clear that the UK
stands out in the proportion of healthcare that is publicly funded.
Even Scandinavian countries, including Norway and Sweden,
traditionally seen as having a particularly strong emphasis on
publicly financed services, have more private expenditure in their
health system than the UK. The figures are not directly comparable,
however. The UK has a fairly unusual structure for health services,
in which a private sector exists in parallel to publicly funded
services, offering an alternative way to access treatments that are
generally also available on the NHS. So, the private financing of
healthcare in the UK is largely in the form of medical insurance or
out of pocket payments for private care. This sets the UK apart from
other systems, which have an element of co-payment for publicly
funded care, and no parallel private sector. However the table 3.1 is
a clear indication that healthcare in the UK relies particularly heavily
on public money. And, in an economic downturn, this leaves the
UK health system particularly vulnerable to spending constraints
resulting from a reduction in tax revenues.
table 3.1: public expenditure on health, 2006, as a percentage of total
expenditure on health
Australia 67.7
Canada 70.4
Denmark 84.1
France 79.7
Germany 76.9
Greece 61.6
Ireland 78.3
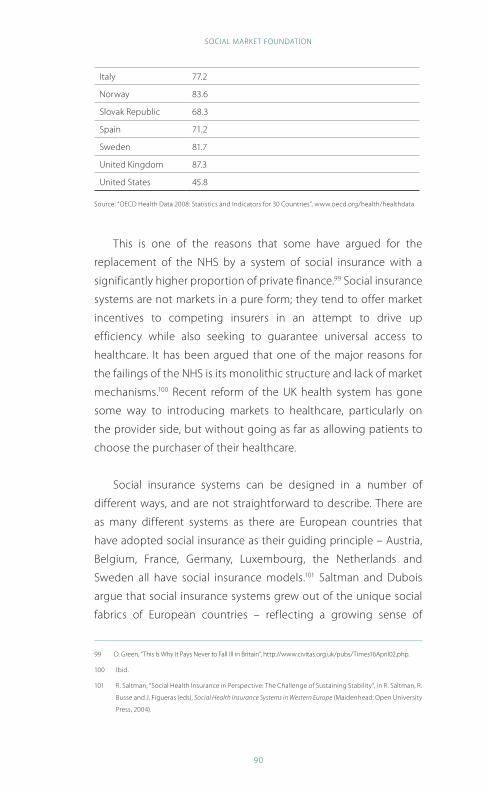
SOCIAL MARKET FOUNDATION
90
Italy 77.2
Norway 83.6
Slovak Republic 68.3
Spain 71.2
Sweden 81.7
United Kingdom 87.3
United States 45.8
Source: “OECD Health Data 2008: Statistics and Indicators for 30 Countries”, www.oecd.org/health/healthdata
This is one of the reasons that some have argued for the
replacement of the NHS by a system of social insurance with a
significantly higher proportion of private finance.99 Social insurance
systems are not markets in a pure form; they tend to offer market
incentives to competing insurers in an attempt to drive up
efficiency while also seeking to guarantee universal access to
healthcare. It has been argued that one of the major reasons for
the failings of the NHS is its monolithic structure and lack of market
mechanisms.100 Recent reform of the UK health system has gone
some way to introducing markets to healthcare, particularly on
the provider side, but without going as far as allowing patients to
choose the purchaser of their healthcare.
Social insurance systems can be designed in a number of
different ways, and are not straightforward to describe. There are
as many different systems as there are European countries that
have adopted social insurance as their guiding principle – Austria,
Belgium, France, Germany, Luxembourg, the Netherlands and
Sweden all have social insurance models.101 Saltman and Dubois
argue that social insurance systems grew out of the unique social
fabrics of European countries – reflecting a growing sense of
99 D. Green, “This Is Why It Pays Never to Fall Ill in Britain”, http://www.civitas.org.uk/pubs/Times16April02.php.
100 Ibid.
101 R. Saltman, “Social Health Insurance in Perspective: The Challenge of Sustaining Stability”, in R. Saltman, R.
Busse and J. Figueras (eds), Social Health Insurance Systems in Western Europe (Maidenhead: Open University
Press, 2004).

FROM FEAST TO FAMINE
91
solidarity in health services.102 Despite their differences and unique
characteristics, social insurance systems share two key features:103
• insured people pay a regular, defined (normally wage-
based) contribution;
• independent quasi-public bodies (normally called sickness
funds) manage the system and act as payers for healthcare.
Within this broad framework, different systems allow for
different rules. Membership of a sickness fund may be compulsory,
although there are systems in which individuals are allowed to opt
out. There may or may not be a degree of risk-pooling between
funds to equalise their liability to healthcare costs. There are
different degrees of competition between funds, with patients
sometimes allowed to switch between different purchasers of care.
In other systems patients are allocated to a particular fund based
on their occupation, geographical location or both, rather than
being allowed to choose.
There are strong arguments against the adoption of a social
insurance scheme in the UK, even in the context of a severe threat
to the NHS model. First, it would be an enormous policy gamble.
While some systems have moved from an insurance-based model
to one that is predominantly tax-funded, there has never been an
example of a change in the opposite direction.104 While it is always
difficult to make direct comparisons between health systems, it
would be very risky to embark on a massive structural reform in the
UK without any international evidence about how best to proceed.
102 R. Saltman and H. Dubois, “The Historical and Social Basis of Social Health Insurance Systems”, in R.
Saltman, R. Busse and J. Figueras (eds), Social Health Insurance Systems in Western Europe (Maidenhead:
Open University Press, 2004).
103 E. Mossialos, Funding Health Care: Options for Europe (Buckingham: Open University Press, 2002); C.
Normand and R. Busse, “Social Health Insurance Financing”, in E. Mossialos et al. (eds), Funding Health Care:
Options for Europe (Buckingham: Open University Press, 2002).
104 D. G. Green et al., “For and Against: Social Insurance – The Right Way Forward for Health Care in the United
Kingdom?” British Medical Journal (International Edition) 325:7362 (2002).
SOCIAL MARKET FOUNDATION
92
Additionally, there is little evidence that social health insurance
performs much better than tax-funded systems, and the same
challenge of scarce resources applies: “Because resources are
never sufficient to satisfy all demands, some form of rationing or
priority setting is inevitable. A shift from tax financing to social
health insurance does not change this.”105 Indeed, many European
countries, including France and Germany, spend a greater
proportion of their GDP on healthcare than the UK does. Social
insurance is not a “magic bullet” to reduce costs.
That said, there is some evidence that per capita spending
under social health insurance systems is lower than in tax-financed
systems – perhaps 3–4%. But this is more than outweighed by the
potential burden on employers. In many social insurance systems,
employers play a bigger role in financing healthcare than they
do in the UK, where NI contributions make up a relatively small
proportion of the overall health budget. An analysis conducted
by the World Bank found that social health insurance can have
an impact on overall levels of employment – reducing total
employment by up to 6% as employers choose not to take on staff
in order to avoid health costs.106 At a time of economic crisis it is not
right to take risks with the economy by placing additional costs on
employment.
While it is undoubtedly true that there are features of other
health systems that are better than the English NHS, there is simply
no evidence that a shift to social insurance would be a desirable
move. Reform of this kind could not be achieved without a
significant structural overhaul of the NHS. And, given the large-scale
organisational reform of recent years and the current economic
uncertainty, it would be extremely undesirable to make this a policy
priority. Our wide range of both formal and informal interviews with
105 Normand and Busse, “Social Health Insurance Financing”, 76.
106 A. Wagstaff, Social Health Insurance vs. Tax-Financed Health Systems – Evidence From the OECD (Washington,
DC: World Bank, 2009).
FROM FEAST TO FAMINE
93
stakeholders throughout the health system indicates little support
for a radical overhaul of the way the NHS is funded.
recommendation 7: the nhs should continue to be
funded primarily from general taxation. a move to a
system of social insurance should not be considered by
policymakers over the next decade.
However, there exists a range of private payment mechanisms
that stop short of social or private insurance models. Might any of
these prove appropriate for the NHS of the future?
containinG costs or raisinG revenue?
The sections above have outlined the severe threat to the health
system posed by the economic crisis. It is clear from the popularity
of a whole range of health and wellbeing products that individuals
value health and are prepared to pay for it. Neither defining a core
package nor replacing the NHS with a system of social insurance is
a desirable option for meeting the financial challenge of the years
ahead. What choices does that leave for closing this fiscal gap? The
major policy option left unexplored is user charging. There are two
possible reasons for introducing charges into health systems. One
is to contain costs by affecting behaviour – the behaviour of the
patient is affected by the introduction of a charge. The other reason
is to raise revenue – bringing more money into the system through
a system of charges. These approaches are considered below.
revenue raising
Is there potential for the NHS to raise additional money through the
introduction of a system of user charges? This argument rests on
the idea that there is a level beyond which the public is unwilling
to pay higher taxes, even for better services. This assumption is
SOCIAL MARKET FOUNDATION
94
partly borne out through our own opinion polling, in which higher
levels of taxation were not a popular option for meeting increased
demand for healthcare. Only 18% of people said that higher taxation
would be their preferred way of meeting potential shortfalls in
health budgets.107 Some participants in the SMF Health Project’s
specially commissioned discussion groups suggested that, to
preserve the ability of the NHS to deal with serious illnesses, people
should pay for the most common or most trivial conditions. This
was often coupled with the idea that people using NHS services
irresponsibly (by not turning up for appointments, for example)
should be penalised.108 A discussion of the potential for charges to
affect behaviour in seeking healthcare features later in this chapter.
Leaving aside questions of equity, one problem with this approach is
that it requires a huge level of charges to have any significant impact as
a proportion of a vast health budget. The OECD estimates that in 2006
the UK spent 8.4% of its GDP on health,109 and that by 2010–11 the NHS
budget will be around £110 billion. So, to make an impact on such a large
item of government spending would require substantial user charges.
One obvious example of an aspect of health services where
charges could be introduced is in primary care – GP and practice
nurse appointments. The NHS Information Centre estimates that in
2007 there were 283,480,000 consultations in GP practices.110 These
include consultations with GPs, practice nurses and other primary
care professionals. It is assumed that there would be no behavioural
response to charging on the part of the public – for example in the
number of appointments made. But in fact, this would not be the
case – a discussion that is explored in greater detail below.
107 Furness and Gough, Local Control and Local Variation in the NHS.
108 Ibid.
109 “OECD Health Data 2008: Statistics and Indicators for 30 Countries”, www.oecd.org/health/healthdata.
110 “Research Report on Consultation Rates in General Practice 1995–2008 “, http://www.ic.nhs.uk/statistics-
and-data-collections/primary-care/general-practice/qresearch-report-on-trends-in-consultation-rates-
in-general-practices-1995-2008.
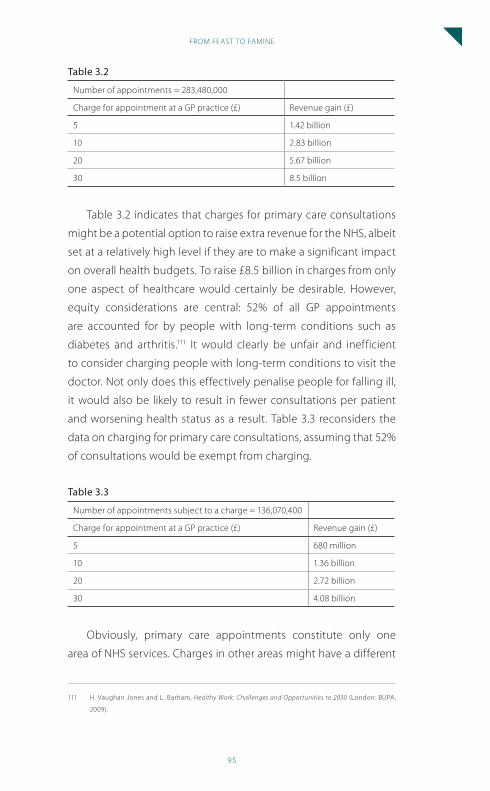
FROM FEAST TO FAMINE
95
table 3.2
Number of appointments = 283,480,000
Charge for appointment at a GP practice (£) Revenue gain (£)
5 1.42 billion
10 2.83 billion
20 5.67 billion
30 8.5 billion
Table 3.2 indicates that charges for primary care consultations
might be a potential option to raise extra revenue for the NHS, albeit
set at a relatively high level if they are to make a significant impact
on overall health budgets. To raise £8.5 billion in charges from only
one aspect of healthcare would certainly be desirable. However,
equity considerations are central: 52% of all GP appointments
are accounted for by people with long-term conditions such as
diabetes and arthritis.111 It would clearly be unfair and inefficient
to consider charging people with long-term conditions to visit the
doctor. Not only does this effectively penalise people for falling ill,
it would also be likely to result in fewer consultations per patient
and worsening health status as a result. Table 3.3 reconsiders the
data on charging for primary care consultations, assuming that 52%
of consultations would be exempt from charging.
table 3.3
Number of appointments subject to a charge = 136,070,400
Charge for appointment at a GP practice (£) Revenue gain (£)
5 680 million
10 1.36 billion
20 2.72 billion
30 4.08 billion
Obviously, primary care appointments constitute only one
area of NHS services. Charges in other areas might have a different
111 H. Vaughan Jones and L. Barham, Healthy Work: Challenges and Opportunities to 2030 (London: BUPA,
2009).
SOCIAL MARKET FOUNDATION
96
effect. But, as is clear from the basic calculation above, the idea
of raising significant revenue from user charges very quickly runs
into ethical problems. In secondary care an even greater majority of
NHS resources are devoted to those people who suffer from long-
term conditions: 65% of all outpatient appointments and 72% of all
inpatient hospital stays are accounted for by people with long-term
conditions. This means that charges for healthcare aimed at raising
revenue would have to be targeted at a relatively small number of
patients (assuming that people with long-term conditions remain
exempt), and thus set at a very high level. Without a significant
change in the system of funding that would shift the cost from
the state to the individual – across the board co-payments – it
is difficult to see much scope for the NHS to raise money from
individual patients to cover potential budget shortfalls. Even if a
system could be introduced that might reasonably expect to raise
£4.08 billion a year in charges, this represents only around 3.6% of
the NHS budget for 2010/11. A gain of this size would be wiped out
with perhaps only a year of standard funding increases. This finding
is consistent with the experience of other OECD countries. As Peter
Smith has commented: “Developed countries do not currently rely
to any great extent on charges as a significant source of finance.”112
The SMF Health Project does not believe that the NHS will, or
should, become an exception to this general rule.
recommendation 8: new private payments should not
be introduced in an attempt to raise revenue.
existing nhs charges
In this discussion about the desirability of the revenue-raising
potential of charging for NHS services it should not be forgotten
112 P. Smith, “The Future Role of User Charges in the National Health Service”, in House of Commons Health
Committee, NHS Charges: Volume III (London: HMSO, 2006), 155
FROM FEAST TO FAMINE
97
that some charges are already in place. Charges for dentistry, optical
services and prescriptions have been in place for several decades.
There is no clear rationale for why these things in particular
should be subject to charges, while other services are not. As
the House of Commons Health Committee pointed out, charges
have developed “piecemeal” and there are “no comprehensible
underlying principles”.113
While charges are levied for certain services, many people find
themselves exempt. For example, retired people, pregnant women
and the unemployed are all exempt from prescription charges.
Certain long-term conditions are exempt, while others are not.
Although 50% of people are subject to prescription charges, only
16% of prescriptions are actually paid for.114 But do NHS charges
actually raise much revenue? As of 2006, NHS charges raised
approximately £1 billion per annum,115 or around 1% of the NHS
budget. This is in line with the evidence explored above, where
it is clear that charges have only a very limited impact in raising
money for expensive health services. It could be argued, therefore,
that existing NHS charges should be scrapped or substantially
reformed, especially if they have an adverse impact on equity in
the health system.
The existing system of charges is inequitable. Those on low
incomes are disadvantaged and are discouraged from seeking the
healthcare they need. A 2001 survey by the Citizens Advice Bureau
found that 28% of people liable to pay prescription charges did not
have their medicines dispensed in full. Of these, 38% were single
parent households, and 37% had long-term conditions.116 This is not
necessarily an argument for the abolition of charges, but instead
compelling evidence that the current system should be reformed.
113 House of Commons Health Committee, NHS Charges: Volume III, 3.
114 Ibid, 15
115 Ibid, 15.
116 National Association of Citizens Advice Bureaux, Unhealthy Charges (London: NACAB, 2001).
SOCIAL MARKET FOUNDATION
98
The SMF Health Commission, examining the question of health
charges in 2004, concluded: “The fiscal case for new charges, increased
charges or extensions of existing charges is weak at a time when
the NHS is receiving increased levels of revenue, but might become
stronger during crisis periods when demand for services outstrips
investment levels.”117 The public services are no longer in a time of
plenty. The NHS is in no position to forgo revenue from existing
charges, however insignificant it might be in terms of the overall NHS
budget. Instead, the system of charges should be entirely overhauled
to reflect income rather than status in determining exemptions.
It is unclear why the wealthy pensioner should be exempt from
prescription charges while working people on low wages pay the full
charge. In a severe economic downturn that will undoubtedly have a
significant impact on the state’s ability to fund health services in the
years ahead, it is wrong to object on ideological grounds to charging.
Instead, those charges that are levied should be fair, and must not
deter people from accessing necessary healthcare. Importantly, while
prescription, optical and dental charges are not popular, they are
at least accepted by the public. It is far easier to adjust the existing
system than to introduce new charges. It should not be a priority
for the NHS to deny itself over £1 billion per annum by abolishing
patient charges that are generally accepted. Instead, the system of
prescription charges must be adjusted to make it fair.
recommendation 9: scarce public resources mean that
abolishing existing charges (prescription, dental and
optical) should not be a priority for the nhs. instead,
charges should be reformed so that exemptions are
made on ability to pay, rather than somewhat arbitrary
categories such as retirement and pregnancy. this
should be achieved through the tax credit system.
117 SMF Health Commission, User Charges for Healthcare: The Social Market Foundation Health Commission –
Report 2D (London: Social Market Foundation, 2004), 5.
FROM FEAST TO FAMINE
99
containing costs
It has been established that private payments for healthcare are
unlikely to prove a useful policy tool in providing extra revenue for
the NHS. A more fruitful line of enquiry is to ask whether, especially
with an ever-improving understanding of behavioural psychology
in public policy,118 private payments should be introduced to contain
demand for NHS services. This might help to maintain the health
system in the face of potentially overwhelming cost pressures.
The SMF Health Project has concluded that neither the
ageing population nor new technologies are unlikely seriously to
unbalance the NHS model.119 However, the upward trend in health
spending coupled with the downward trend in tax revenue means
that the issue of constraining demand for healthcare is of central
importance. Apart from the limited range of charges outlined in
the section above, the NHS is essentially free at the point of use.
In classical economics, that means there is a free-rider problem. If
healthcare goods are priced at zero, then there is no incentive not
to consume too much. Just as the shopper would load up their
trolley with unnecessary goods if everything on the shelves were
free, so the individual has no economic incentive either to avoid the
need to consume healthcare resources, or to use health services
responsibly. For example, the Adam Smith Institute has argued: “If
we had to fork out £30 to see our GP, we might opt for self-treatment
via our local chemist’s shop, and save the doctor’s skills for more
serious ailments.”120 This argument rests on the premise that there is
unnecessary consumption of healthcare resources because people
seek treatment either when they don’t need it, or in the wrong
setting. It is not easy to determine the extent to which the NHS
118 J. Prendergrast et al., Creatures of Habit? The Art of Behavioural Change (London: Social Market Foundation,
2008).
119 Furness et al., SMF Health Project Background Paper 2: Demography and Technology – External Pressures
for Change.
120 A. Singleton, “Time to Charge for GP Appointments”, http://www.adamsmith.org/think-piece/health/
time-to-charge-for-gp-appointments-2004082475/.
SOCIAL MARKET FOUNDATION
100
might be able to constrain demand for healthcare without adversely
affecting health – in an effort to reduce over-consumption on the
part of some, there is clearly a risk that necessary consumption by
others would be deterred. But there is some evidence that patients
do not always access healthcare appropriately.
One common criticism of the way some people use the NHS is
the number of patients who present at Accident and Emergency
departments with minor conditions. Since provision of this service
is very expensive, such cases threaten to deprive people with true
emergency problems from the quality of healthcare they need.
Norwich University Hospital claims that up to 70% of patients
attending A&E could have been treated in another setting, and
has launched a public information campaign under the slogan
“A&E – do you really need to go there?”121 to encourage people to
avoid using the service unnecessarily. But could charging people
for healthcare more generally really lead to a more responsible
attitude to using valuable services?
The evidence on unnecessary consumption of healthcare
rather than the inappropriate use of services, sometimes described
as “frivolous” demand, is less strong. There is a great deal of concern
expressed about the “worried well” and their impact on healthcare
resources, but little evidence to suggest that frivolous demand for
healthcare has a real impact on NHS budgets. However, there is
some international evidence, examined below, about the impact
of charging and reduced demand on health status – a reasonable
guide to action for the NHS.
The SMF has no ideological objection to patient charges.
A social market approach is not consistent with the idea that
charging for healthcare is wrong in principle, especially since
in the final analysis no healthcare is “free” – the costs are simply
121 “A&E – Do You Really Need to Go There?”, http://www.nnuh.nhs.uk/TrustDoc.asp?ID=126.
FROM FEAST TO FAMINE
101
shared through taxation and met in advance of treatment. Market
mechanisms reflecting the price of services can be appropriate
in healthcare, as they can in other public services, if they help to
achieve the desired social goals. However, in making the case for
extending private payments in an attempt to constrain costs, the
principle of universal access, rather than market efficiency alone,
must be the main consideration. In this, it is important to heed a
reminder from Carrin and Hanvoravongchai: “Society’s preferences,
and not just economics, have an important impact on choosing the
appropriate amount of care.”122
For any new system of charging to be acceptable for the future
of the NHS it ought to adhere to the following criteria:
• demand for healthcare is reduced, with a subsequent
reduction in costs;
• overall population health is not adversely affected by
charging;
• people on low incomes are not deterred from seeking
necessary care;
• people with ongoing health problems are not deterred
from seeking necessary care; and
• the costs and difficulty of implementing the system of charges
does not outweigh the benefits of reducing demand.
What follows examines the potential for each of these criteria to
be satisfied.
Key features of the evidence
One of the challenges in discussing the future of charging in
the NHS concerns the limitations of the evidence. Most of the
evidence on the impact of charging on healthcare consumption
122 G. Carrin and P. Hanvoravongchai, “Provider Payments and Patient Charges As Policy Tools for Cost-
Containment: How Successful Are They in High-Income Countries”, Human Resources for Health 1:1 (2003).
SOCIAL MARKET FOUNDATION
102
comes from Europe and the United States rather than the UK. The
radically different healthcare systems and political preferences of
these countries mean that it is not always straightforward to apply
lessons from the US to the UK. Also, as Dixon and Mossialos write:
“There are no randomised control trials of the effect of user charges
on utilisation in Europe; most studies trace the effects of a policy
change.”123 This means that to some extent policy on UK health
charges cannot be based on sound evidence. However, there are
clear principles that can be discerned from international evidence,
even if they are sometimes difficult to apply to this country.
Reducing demand for healthcare
There is clear evidence that introducing charges can reduce
demand for healthcare. The best example of this is the famous
RAND Health Insurance Experiment, which took place in the US.
This is one of the only examples of a randomised trial examining
the impact of charges on healthcare utilisation and health status.
In this experiment more than 7,700 individuals were randomly
assigned to a healthcare plan in which there were varying levels
of co-payments or charges. These ranged from completely free
access to 95% co-insurance up to an annual maximum of $1,000.124
Although this was a US experiment and was concluded in 1982,
it remains the best source of data for policymakers studying the
effects of charges.
The RAND experiment has proved highly controversial, but
one of its findings is clear. Charges can significantly lower demand
for healthcare. Table 3.4 includes data on hospital visits, admission
rates and overall spending for individuals on different types of
plan. This indicates that there is substantial potential for the NHS to
reduce demand for its services by levying charges across the board.
123 A. Dixon and E. Mossialos, “Funding Healthcare in Europe – Recent Experiences”, in J. Watson and P. Ovseiko
(eds), Health Care Systems: Major Themes in Health and Social Welfare (New York: Routledge, 2005), 61.
124 R. Brook et al., “The Health Insurance Experiment: A Classic RAND Study Speaks to the Current Health Care
Reform Debate”, 2006
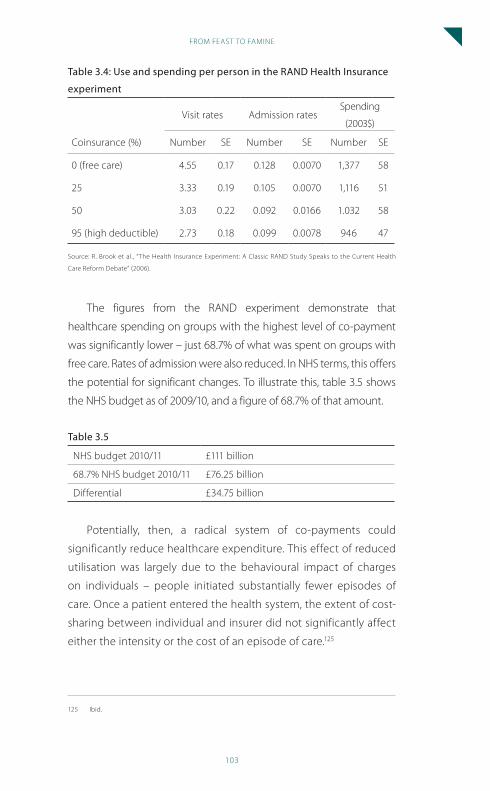
FROM FEAST TO FAMINE
103
table 3.4: use and spending per person in the ranD health insurance
experiment
Coinsurance (%)
Visit rates Admission ratesSpending
(2003$)
Number SE Number SE Number SE
0 (free care) 4.55 0.17 0.128 0.0070 1,377 58
25 3.33 0.19 0.105 0.0070 1,116 51
50 3.03 0.22 0.092 0.0166 1.032 58
95 (high deductible) 2.73 0.18 0.099 0.0078 946 47
Source: R. Brook et al., “The Health Insurance Experiment: A Classic RAND Study Speaks to the Current Health
Care Reform Debate” (2006).
The figures from the RAND experiment demonstrate that
healthcare spending on groups with the highest level of co-payment
was significantly lower – just 68.7% of what was spent on groups with
free care. Rates of admission were also reduced. In NHS terms, this offers
the potential for significant changes. To illustrate this, table 3.5 shows
the NHS budget as of 2009/10, and a figure of 68.7% of that amount.
table 3.5
NHS budget 2010/11 £111 billion
68.7% NHS budget 2010/11 £76.25 billion
Differential £34.75 billion
Potentially, then, a radical system of co-payments could
significantly reduce healthcare expenditure. This effect of reduced
utilisation was largely due to the behavioural impact of charges
on individuals – people initiated substantially fewer episodes of
care. Once a patient entered the health system, the extent of cost-
sharing between individual and insurer did not significantly affect
either the intensity or the cost of an episode of care.125
125 Ibid.
SOCIAL MARKET FOUNDATION
104
Where available, other evidence corroborates the findings of
the RAND experiment in this area. Peter Smith cites the example of
Belgium, where the introduction of charges reduced demand for
GP home visits.126
The RAND experiment has been subject to criticism for its
conclusion that health expenditure is reduced when users are
charged. Some have argued that it gives only a partial analysis of
the costs and benefits of charging: “[A]lthough the RAND results
showed that cost-sharing reduced third-party payer expenditure
on the services subject to these charges, providers could, over
time, expand activity on alternative services and thereby increase
overall expenditure.”127 Despite this, the substantial difference in
doctor visits between groups indicates that charging does indeed
have an impact on demand for healthcare. Additionally, the RAND
experiment took place over five years, in which time one might
reasonably expect provider behaviour to have changed in response
to the basket of goods covered by co-payments.
The evidence fits with the economic idea that patients over-
consume healthcare because it is priced at zero. It therefore
fulfils our first criteria for the potential introduction of charging
into the NHS – that it reduce overall demand for healthcare,
with a subsequent decline in costs. However the challenge is in
ensuring that people are not denied the healthcare they need on
the basis of ability to pay. After all, demand for healthcare could
easily be reduced with the introduction of prohibitively expensive
co-payments, but the real test of the policy would be in its
impact on health. It is here that the RAND experiment has proved
most controversial.
126 Smith, “The future role of user charges in the National Health Service”.
127 Mossialos, Funding Health Care: Options for Europe, 176.
FROM FEAST TO FAMINE
105
overall population health and charging, and the impact on
the poor and the sick
The RAND experiment measured not only healthcare utilisation
but also the overall health of the individuals involved. The study
concluded that “free care had at most a small impact on any of five
general health measures for the average enrolee”.128 In other words,
“cost sharing in general had no adverse effects on participant
health”.129 This would seem to be conclusive evidence that charging
is an appropriate policy tool for the NHS to help reduce demand
for healthcare.
However, data from the RAND experiment demonstrated that
when charges are levied for healthcare, it is those who are least
well-off who suffer the most significant adverse effects. As Ray
Robinson writes: “The RAND Health Insurance experiment showed
that cost-sharing tended to be associated with especially marked
reductions in the probability of medical use and outpatient visits
among lower income groups.”130 In some cases, this reduction in
healthcare utilisation had significant, even fatal, consequences
for poor patients. The poorest patients with hypertension in the
groups subject to charging had a 10% higher rate of mortality than
comparable patients with access to free care.131
This effect appears to be more than simply a question of system
design. Further evidence suggests that other types of charging can
deter the poor and the sick from seeking the care they need. Dixon
and Mossialos cite an analysis of user charging in Sweden, where
patients who reported their financial state as poor were ten times
more likely to forgo care than those who reported their financial state
128 R. H. Brook et al., The Effect of Coinsurance on the Health of Adults, (Santa Monica, CA: RAND Corporation,
1984), 4
129 Brook et al., “The Health Insurance Experiment”.
130 R. Robinson, “User Charges for Health Care”, in Mossialos, Funding Health Care: Options for Europe, 177
131 Brook et al., The Effect of Coinsurance on the Health of Adults.
SOCIAL MARKET FOUNDATION
106
as good.132 Other studies conclude that charges can affect those in
poor health. A review of charges for prescription medication found
that charges were associated with increased use of other healthcare
services for patients with congestive heart failure, diabetes and
schizophrenia.133 A WHO cross-country analysis found that cost-
sharing (or patient charges) led to a significant reduction in the use
of healthcare, with implications for equity.134
Tantalisingly though, the generally accepted conclusion of the
RAND experiment is that charging can lead to significant reductions
in healthcare demand, without compromising the health of the
average person. And research carried out by the SMF in conjunction
with Ipsos-MORI found that members of the public are willing to
countenance the idea of charging for certain minor conditions if
that safeguards the ability of the NHS to treat the most seriously
ill.135 Is there a way of safeguarding the poor and the sick while still
reducing overall demand for healthcare? For the NHS, the context
for this discussion is a likely level of funding increases that may not
otherwise be adequate to maintain the service at current levels.
For the NHS, it is clear that the following are true:
• there are few cost incentives to deter people from using
health services in the most efficient way;
• there are already charges in place that are broadly
accepted by the public;
• charging is an effective mechanism for reducing demand
and expenditure;
• a very small drop in demand among some groups would
132 A. Dixon and E. Mossialos, “Shifting Costs to Patients”, in Dixon and Mossialos, “Funding Healthcare in
Europe - Recent Experiences”, 61.
133 D. P. Goldman, G. F. Joyce and Y. Zheng, “Prescription Drug Cost Sharing” JAMA 298:1 (2007).
134 S. Thomson and E. Mossialos, What Are the Equity, Efficiency, Cost Containment and Choice Implications
of Private Health-Care Funding in Western Europe? (Copenhagen: WHO Regional Office for Europe, 2004).
135 Furness and Gough, Local Control and Local Variation in the NHS.
FROM FEAST TO FAMINE
107
help to manage expenditure in a time of scarce public
resources; and
• clinicians play the key role in determining whether referral
for diagnosis or secondary care is appropriate.
Given the above, the SMF Health Project recommends the
introduction of a very limited range of charges.
recommendation 10: a very limited range of charges
for initial consultations with Gps and other primary care
practitioners should be introduced.
The charges would be designed to incentivise wealthy individuals
to avoid seeking unnecessary initial consultations with clinicians.
Those who do not have the ability to pay would be totally exempt
from the charges. These charges would be so limited as to be virtually
symbolic, representing the introduction of weak price signals to
guide demand as well as a shared acceptance that lean times mean
that all health service users must do their utmost to use services
appropriately and when necessary. As a participant in an SMF Health
Project discussion group said: “If they start charging for the minor stuff
they can put the money towards the big stuff.” A system of charges
should be introduced as a way of affecting behaviour in an attempt
to “Save the NHS”. The public may well be receptive to this message
as the full impact of the recession on public services becomes clear.
Despite advocating limited charges, it is our conclusion that
patients who require diagnosis and/or treatment following initial
consultation should not be subject to further charging. This reflects
the reality that as clinicians play a key role in managing demand for
expensive health services, it is not appropriate to levy charges on
patients following referral from the GP. Indeed, the system proposed
is highly limited in the range of services for which charges would be
SOCIAL MARKET FOUNDATION
108
introduced, and the overall limit to charges. Charges are something
of a “blunt instrument” in affecting demand for healthcare, with the
potential for individuals to be deterred from seeking both necessary
and unnecessary healthcare. The system outlined below attempts to
minimise the likely negative impact of charging by applying charges
only to those who have the ability to pay. The discussion earlier in
this chapter about overall spending on health-related products
reinforces the idea that many individuals are already contributing
financially to their wellbeing. The charging system proposed here
therefore attempts to build on this willingness to pay for care. Key
features of this proposed system are outlined below:
What would patients be charged for?
Patients would be charged for initial appointments with GPs and
other primary care practitioners.
What would not be subject to charging?
No treatment resulting from referral from the GP would be subject
to charging. No community-based treatment resulting from GP
referral would be subject to charging.
Who would be exempt from charges?
Exemptions from charges would be linked to receipt of:
• Working Tax Credits
• Child Tax Credits
• Incapacity Benefit/Employment and Support Allowance
• Income Support
• Jobseeker’s Allowance
• Pension Credit
• Inaddition,everyoneaged18yearsoryoungerwouldbe
totally exempt from charges
We propose that any patient from a family in receipt of tax
credits be automatically exempted from charges. This would
FROM FEAST TO FAMINE
109
automatically exempt at least 3.9 million families with children from
charges136 – representing the poorest 52% of families in the UK
and 13.6 million adults and children in total. Exempting people in
receipt of Income Support, Jobseeker’s Allowance and Incapacity
Benefit, and retirees receiving Pension Credit would exclude a
further 7.5 million from charges. Individuals in receipt of these
qualifying benefits should also be exempted from prescription
charges as part of a wider overhaul of that system. Not only does
benefit and credit eligibility identify those on low incomes, it also
provides the most effective administrative mechanism to identify
those who should be exempt from charges. All in all, this approach
would exempt the lowest income one-third of people in the UK
from paying any charges at all.
What would be the level of charges?
The RAND experiment shows that charges set at a modest level
can still have an impact on demand for healthcare. The level of
charges should be as low as possible – perhaps £20 for an initial
appointment with a GP or primary care practitioner. It should be
noted that this is still below the actual cost of a GP consultation –
estimated at up to £36 by the PSSRU.137
What would be the limit of charges?
Total health charges (including existing prescription charges and
the new charges proposed above) should be limited at the same
level as current prescription charges – currently £102.50 per annum
(the cost of a 12-month prescription pre-payment certificate). This
low upper limit to charges indicates that our primary aim is to
reduce free-riding rather than introduce significant co-payments
into the NHS.
136 House of Commons Public Accounts Committee, HM Revenue and Customs: Tax Credits and Income Tax,
Fourteenth Report of Session 2008–09 (London: HMSO, 2009). 9
137 L. A. Curtis, Unit Costs of Health and Social Care 2008 (University of Kent: Personal Social Services Research
Unit, 2008), 109.
SOCIAL MARKET FOUNDATION
110
Who would be responsible for collecting charges?
The main responsibility for collection should rest with GP practices
which hold patient records and can monitor most easily the
number of consultations by any one individual.
What safeguards should be put in place?
A number of safeguards should be put in place to ensure that the
criteria outlined above are fulfilled through the small-scale charges
proposed. The Department of Health should monitor primary care
consultation rates in different groups, and report publicly on the
findings. There should be a particular focus on those with low
incomes, with extensive public information campaigns explaining
that no one receiving benefits or credits will be subject to NHS
charges for consultations, or for prescription charges for medication.
The Department of Health should also monitor rates of
attendance at A&E to analyse whether patients are avoiding
GP charges by accessing healthcare in other ways, potentially at
greater expense to the NHS.
What change in utilisation and spending could be expected
from the introduction of a £20 charge for initial consultations
in primary care?
Data is lacking on the income levels of patients consulting primary
care practitioners. There is also a lack of modelling applicable to the
UK that would indicate the likely drop in utilisation from charges
set at different levels. However, given that in the RAND experiment
there was up to a 30% difference in healthcare spending in groups
subject to charges relative to those who received free care, it is
reasonable to assume that any form of charging introduced into
the NHS would result in a drop in utilisation and spending among
some groups. Even a modest drop in demand for NHS services of
5% would effectively represent a year of decent funding increases
for the health service. In conjunction with the supply-side reforms
aimed at improving the commissioning function outlined elsewhere
FROM FEAST TO FAMINE
111
in this paper, some limited charges aimed at managing demand are
entirely appropriate to secure the future of universal healthcare in
an environment where resources are tightly squeezed.
Additionally, the system of charges should be annually reviewed
to ensure that it is impacting on demand without adversely
affecting health among groups subject to charges. It should be
comprehensively revised, or indeed abandoned, if it cannot be
shown that these criteria are being met.
conclusion
Radical change is inevitable in the next decade of the NHS. Some of
this will be clinically driven, while some will be the product of social
pressure or political choice. Most pressingly, the pressures of a severe
economic recession and the subsequent need for retrenchment in
public spending mean that the financial situation for the NHS in the
decade ahead is likely to be extremely tight. Elsewhere in this final
report, a number of policies are proposed aimed at creating better
value for money in the NHS, largely built around a radically local model
of accountability in which services can be designed to meet specific
needs. But as well as increasing value for money and efficiency on the
supply side, demand management will also be necessary if quality
improvements are to be secured in a tight fiscal environment.
Charging is a crude form of demand management, but
preferable to a decline in quality that would see, for instance, the
reappearance of unacceptably long waits for treatment which would
impact most heavily on the poor and the sick. Charging has limited
revenue-raising potential, but evidence from abroad indicates that
it can significantly reduce demand without affecting health status
for the average person. As a result of this, the system outlined above
totally exempts from charges those people on low incomes and a
huge proportion of working families with children. In fact, the
overall situation for these individuals would, under these proposals,
SOCIAL MARKET FOUNDATION
112
improve, since it is recommended that receipt of benefits or credits
should qualify for the exemption from prescription charges too.
The proposals outlined establish a system that slightly lessens
the free-rider problem in the NHS. However, it explicitly avoids the
possibility that patients will be subject to extensive charges by
excluding entirely secondary care from the charging regime, and
capping charges at a very low level. Thus, the challenge to equity
from charging is minimised, with the possibility of efficiency gains
significantly enhanced. The discussion of equity in health systems in
chapter 2 makes clear that charges for some better-off patients need
not challenge the principle of universal access to care. Indeed, the
NHS already charges for services, and does not always make sure that
people who cannot pay do not pay. The rationalisation of existing
prescription charges coupled with a new system of limited charges
for initial consultation provides the demand-side reform that the
health system requires to deal with the funding challenges it faces.
This will go hand in hand with SMF Health Project recommendations
set out below for greater efficiency savings through high-quality
commissioning, and an increased role for NICE in determining the
overall cost-effectiveness of NHS treatments.
Radical solutions to the need for increased resources do not
require a fundamental change in how the NHS is funded, with
taxation replaced by social health insurance. While people may
be willing to pay for other health-related goods, it will not be
possible in the next decade to translate that willingness directly
into extra NHS revenue. However, this adds weight to the argument
that robust processes must be developed that will enable local
populations to make tough decisions about the allocation of scarce
resources. Individuals make mature decisions about spending
on health – the popularity of products aimed at improving and
extending life are testament to this. It is this understanding that
good health is worth paying for that policymakers must look to
build on in the next decade.
FROM FEAST TO FAMINE
113
chapter Four: national stanDarDs anD Governance
This chapter examines the question of what future role national
government should play in an NHS that is designed around
local needs rather than national standards. Where does central
government fit into a system that is dominated by high-quality local
commissioners developing provider markets to deliver appropriate
local services? If commissioners represent the heart of the NHS,
what role is left for the centre? This chapter briefly outlines the
history of command and control through central targets in the NHS,
and draws conclusions about the future financial and governance
responsibilities of central government.
As discussed throughout this report (see chapter 2 on
equity), the NHS has always aspired to be a national service.
At its inception, Aneurin Bevan spelled out his intention to
“universalise the best” – spreading best practice across the
whole country. The national character of the health system
is reflected in finance and management. Almost the entirety
of the budget for the public health system is provided by
nationally collected taxation, and the Secretary of State for
Health remains the key figure in determining healthcare policy.
National standards and national control have long been a
notable feature of the management of the NHS. The most
memorable evocation of this principle is a much quoted line
of Bevan’s: “a dropped bedpan would resound through the
corridors of Whitehall”.
Clearly, performance in the NHS has been closely aligned, with
central control originating in central government. And what had
been a principle that arose with the post-war Labour government
was enthusiastically adopted by its New Labour successor post-
1997 – the NHS was driven from the centre. As Klein writes of
the first years of that government “The number of performance
SOCIAL MARKET FOUNDATION
114
indicators multiplied. So did the number of targets. … At the peak,
NHS managers reckoned they had to meet 300-plus targets.”138
And targets have worked. Few doubt that the dramatic
improvement in waiting times exhibited by the NHS in recent
years would have occurred without central performance
management and a real political focus on that issue. Waiting times
began to decline from the introduction of the 18-week target in
the 2000 NHS Plan, and have continued to fall. “From the patient’s
viewpoint, the new form of target represented a significant
improvement.”139 But over time, this emphasis on top-down
performance management as a mechanism for improvement has
receded. There are good reasons for this shift. Central targets can
lead to staff dissatisfaction, unintended outcomes and lack of
autonomy for local decision-making.
In Delivering the NHS Plan (2002), the government clearly set out
its desire to move away from “a top-down, centralised system that
inhibits local innovation”,140 stating that, instead, “power needs to
be devolved to locally run services with the freedom to innovate
and improve care for patients”.141 This policy shift was reflected in
the creation and consolidation of primary care trusts that are now
charged with designing a range of services appropriate to their
local communities.
Recent NHS reform has seen unprecedented devolution of
money and authority to PCTs at a local level. The vision set out in
the world class commissioning framework aims for a “new NHS –
locally driven”. It describes how commissioning will be “developed,
138 R. Klein, “The New Model NHS: Performance, Perceptions and Expectations,” British Medical Bulletin (2007), 3.
139 18 Week Waiting Times Target: an Update (London: King’s Fund, 2007).
140 Department of Health, Delivering the NHS Plan: next steps on investment, next steps on reform (London,
HMSO, 2002).
141 Department of Health, Delivering the NHS Plan: Next Steps on Investment, Next Steps on Reform (London:
HMSO, 2002), 28.
FROM FEAST TO FAMINE
115
articulated and owned by the local NHS, with a strong mandate
from local people and other partners”.142 In practice, this will mean
ever more variation between different areas.
But it is not at all clear how national standards and targets will
evolve in response to the increasing power of local commissioners
who have been told to “look outwards not upwards”143 – becoming
accountable not to central government but to local people. In fact,
it is not certain that local commissioning actually has as much
power as the Department of Health makes out. David Nicholson,
NHS Chief Executive, states that “the conditions are now absolutely
right for developing a framework within which PCTs, in conjunction
with their local communities, can set more of their own ambitions
rather than having them mainly set by Whitehall.”144 However, PCTs
are not exempt from central control. The NHS Operating Framework
2008–2009 shows that national targets still form an important
part of healthcare policy. It describes a set of “key non-negotiable
national NHS targets” for local PCTs.145 These include access targets
such as the 18-week maximum waiting time, as well as those
aimed at specific diseases, such as the extension of the NHS bowel
cancer screening programme. As David Stout, Director of the PCT
Network, points out, there are at least “60 instructions to PCTs,
and some of those are instructions which have other instructions
within them”. He declares that the Operating Framework “does not
sit well with a localised approach”.146 There is also a sense that the
pressure on NHS funds might lead to even more central control as
national government looks to secure efficiency savings and better
142 Department of Health, World Class Commissioning Framework: Vision (London: HMSO, 2007), http://www.
dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_080956,
accessed 6 April 2008.
143 Ibid.
144 Department of Health, NHS Operating Framework 2008-2009 (London: HMSO, 2008), 3.
145 Department of Health, NHS Operating Framework 2008-2009.
146 Quoted in S Gainsbury, “Operating Framework Reasserts DoH’s Central Control,” Health Service Journal,
December 19, 2007.
SOCIAL MARKET FOUNDATION
116
value for money.147 This tension between national standards and
increasing levels of local variation is crucial in discussing the future
of healthcare.
What should be the role of national government in the years
to come? How will national standards change to enable, and in
response to, the development of high-quality commissioning?
After a brief discussion of the role of central government in
financing and resource allocation, the bulk of this chapter is
devoted to an exploration of the future of national targets and
national governance.
national Governance, local variation
It is argued throughout this report that local health commissioners
require much greater autonomy in order to continue to improve
health services. Chapter 6 explores the potential for healthcare
commissioning to deliver better value throughout the health
system. Enabling this approach will require a new political
settlement in which central control recedes, allowing local
innovation to flourish. In later chapters the necessary changes
to regulation, accountability and resource allocation are defined,
within the broader context of the decentralisation of health
services. Earlier work undertaken by the SMF Health Project shows
how local people can be engaged in the process of designing a
range of truly local services.148 But there is still an important role for
national standards, management and political control in healthcare
in the years ahead. What follows is a description of what this role
should be in the future. This fits with the literature on the limits to
decentralisation: international evidence makes it clear that some
powers should be retained centrally (decentralisation is discussed
147 R. Evans R and S Gainsbury, “David Nicholson Warns NHS: “All Bets Are Off”,” Health Service Journal, June
4, 2009.
148 D. Furness and B. Gough, Local Control and Local Variation in the NHS: What Do the Public Think? (London:
Social Market Foundation, 2009).
FROM FEAST TO FAMINE
117
in more detail in chapter 5). For example, Hunter et al. argue not
only that there is a need for balance between national and local
control, but also that there are four key areas where decision-
making power should never be decentralised:
1. The basic framework for health policy. Health policy
involves value choices that affect other areas of social life.
Strategic decisions set out in the framework for a nation’s
health policy should therefore be made by the central
government that also sets the framework for other public
sector policy.
2. Strategic decisions on the development of health resources.
Resource-related decisions require a broad overview to
ensure an appropriate balance, as well as efficient use, of
scarce resources.
3. Regulations concerning public safety. Regulation should be a
matter for central control. Experience in some Central and
Eastern European and Commonwealth of Independent
States countries suggests that lower levels of authority
may be more susceptible to corruption than higher levels.
4. Monitoring, assessment and analysis of the health of the
population and healthcare provision. Assessment can be an
efficient tool for influencing the behaviour of decentralised
units. Since decentralisation involves central government
granting authority to lower-level bodies, it is important
that the centre remains able to monitor whether these
new bodies are performing adequately.149
This typology is reflected in the roles for national government set
out below.
149 D. J. Hunter, M. Vienonen and W. C. Wlodarczyk, “Optimal Balance of Centralized and Decentralized
Management”, in R. B. Saltman, J. Figueras and C. Sakellarides Critical Challenges for Health Care Reform in
Europe (Buckingham: Open University Press, 1998).
SOCIAL MARKET FOUNDATION
118
recommendation 11: the following roles should
continue to be undertaken at a central level:
1. setting the basic framework for health policy
2. Making strategic decisions on the development of
health resources
3. regulation concerning public safety
4. Monitoring, assessment and analysis of the health of
the population and healthcare provision
revenue raising
Chapter 3 includes a full discussion of future prospects for NHS
finances, and an analysis of the likely impact of future cost
pressures can be found in SMF Health Project Background Paper 2.150
This research concluded that the NHS will continue to be funded
predominantly from taxation. This argument is made in part on
equity grounds – taxation is the most progressive form of revenue
raising – and in part on practical grounds – over the next decade
it would not be desirable for the NHS to go through the kind of
structural overhaul that radical reform to the system of funding
would entail. So national government has, and will retain, the
central role in raising money for health services.
resource allocation
Chapter 2 contains a full discussion about the appropriate resource
allocation mechanisms that should be in place in an equitable
health system. What is clear from this is that, regardless of the
agreed formula for allocating resources, this is a task that must
be carried out by a central agency – the government. The task of
distributing resources from central taxation to individual localities
150 D. Furness et al., SMF Health Project Background Paper 2: Demography and Technology: External Pressures
for Change (London: Social Market Foundation, 2008).
FROM FEAST TO FAMINE
119
is central to the fair funding of healthcare and, as such, must be
carried out at a national level.
national targets
One of the most contentious aspects of national control of health
services is central target-setting. And while there has been a move
away from a target culture of command and control towards
an attempt to measure health outcomes, the current list of NHS
targets shows that there is still a long way to go before true
autonomy for PCTs can be achieved. The most up to date NHS
targets and priorities are set out in the NHS Operating Framework
2008–2009. David Nicholson emphasises in the foreword that the
government and the Department of Health are seeking to move
away from national targets, instead allowing PCTs, in conjunction
with their local communities, to “set more of their own ambitions
rather than having them mainly set by Whitehall”.151 However,
despite this rhetoric, there remains a great number of centrally set
demands. The framework outlines new national priorities which
cover cleanliness and healthcare-associated infections, improving
access, cancer, stroke, children, maternity, staff satisfaction and
engagement, public engagement and emergency preparedness.
In addition to these national priorities, the framework also
states that PCTs should set local improvement plans for areas of
concern. The document argues that this “marks a radical shift in
NHS planning and is designed to give more authority to local
NHS organisations and their communities”.152 However, despite
this sentiment, the framework then goes on to highlight “issues
requiring local attention”,153 in effect setting out priorities that
are determined centrally, but addressed locally. These include
equality, mixed-sex accommodation, learning disabilities, diabetic
151 Department of Health, NHS Operating Framework 2008-2009, 3.
152 Department of Health, NHS Operating Framework 2008-2009, 20.
153 Ibid.
SOCIAL MARKET FOUNDATION
120
retinopathy, crisis resolution, improving access to psychological
therapies, dementia, end-of-life care and disabled children.
On top of this, the framework makes it clear that PCTs are
also expected to determine and set their own local priorities and
targets. Finally, the document reveals that the 21 existing national
targets still apply.
national tarGets
Set out below are the key non-negotiable national NHS targets.
Cleanliness and healthcare associated infection
• maintain the annual number of bloodstream infections at
less than 50% of the number in 2003/04;
• from April 2009 all elective admissions must be screened
for MRSA in line with Department of Health guidance; and
• differential Strategic Health Authorities envelopes to
deliver nationally a 30% reduction in cases of MRSA by
2011 compared to 2007/08 baseline figures.
Improving access
Key targets for referral to treatment waiting times:
• 90% of pathways where patients are admitted to be
completed within 18 weeks; and
• 95% of pathways where patients are not admitted to be
completed within 18 weeks;
• PCTs to be expected to maintain the reductions in waits
for direct access audiology and hearing aid services that
they planned for delivery in 2008/09, and to support
benchmarking of active health partner (AHP) services;
referral to treatment data to become mandatory from
April 2010.
FROM FEAST TO FAMINE
121
Key targets for primary care access:
• 50% of practices to continue to offer extended opening
times as well as ongoing progress in improving GP
services, such as guaranteeing access to a GP within 48
hours and booking appointments further ahead;
• advance in securing and opening of GP-led health centres
that allow patients access to GP services 12 hours a day,
365 days a year;
• improved patient satisfaction as measured by the GP
Patient Survey; and
• continue to ensure year-on-year improvements in the
number of patients accessing NHS dental services,
including a review of dental commissioning strategies.
Improving health and reducing health inequalities
• no patients should wait more than 31 days for radiotherapy
by December 2010;
• all patients with breast cancer symptoms referred to a
specialist must be seen within two weeks of referral by
December 2009;
• NHS Breast Cancer Screening Programme will be extended
to all women aged 47–73 by 2012;
• NHS Bowel Cancer Screening Programme will be extended
from 2010 to invite men and women aged 70–75 to take part;
• cancer treatment (surgery and drug treatment) Patients
wait no more than 31 days from decision to treat to start of
treatment – all cancer treatments by 2010;
• all patients with suspected cancer, detected through
national screening programmes or by hospital specialists,
wait no more than 62 days for referral to treatment by
2009;
• all women should receive the results of their cervical
screening tests within two weeks by 2010.
SOCIAL MARKET FOUNDATION
122
Existing commitments to be maintained
• a four-hour maximum wait in A&E from arrival to admission,
transfer or discharge;
• guaranteed access to a primary care professional within 24
hours and to a primary care doctor within 48 hours;
• a maximum wait of 13 weeks for an outpatient
appointment;
• a maximum wait of 26 weeks for an inpatient appointment;
• a three-month maximum wait for revascularisation
• a maximum two-week wait standard for Rapid Access
Chest Pain Clinics;
• thrombolysis “call to needle” of at least 68% within
60 minutes, where thrombolysis is the preferred local
treatment for heart attack;
• guaranteed access to a genito-urinary medicine clinic
within 48 hours of contacting a service;
• all patients who have operations cancelled for non-clinical
reasons to be offered another binding date within 28 days,
or the patient’s treatment to be funded at the time and
hospital of the patient’s choice;
• delayed transfers of care to be maintained at a minimal
level;
• all ambulance trusts to respond to 75% of Category A calls
within eight minutes;
• all ambulance trusts to respond to 95% of Category A calls
within 19 minutes;
• all ambulance trusts to respond to 95% of Category B calls
within 19 minutes;
• a two-week maximum wait from urgent GP referral to first
outpatient appointment for all urgent suspected cancer
referrals;
• a maximum wait of one month from diagnosis to treatment
for all cancers;
• a maximum wait of two months from urgent referral to
FROM FEAST TO FAMINE
123
treatment of all cancers;
• 100% of people with diabetes to be offered screening for
the early detection (and treatment if needed) of diabetic
retinopathy;
• deliver 7,500 new cases of psychosis served by early
intervention teams per year;
• all patients who need them to have access to crisis
services, with delivery of 100,000 new crisis resolution
home treatment episodes each year;
• all patients who need it to have access to a comprehensive
child and adolescent mental health service, including 24-
hour cover and appropriate services for 16- and 17-year-
olds and appropriate services for children and young
people with learning disabilities;
• chlamydia screening programme to be rolled out
nationally.
There are a number of criticisms of this set of targets. The
most significant of these is the sheer scale of national targets
that commissioners and providers must meet. There are 35 key
performance measures outlined above. It is questionable whether,
after making all of these a priority, commissioners will have the
capacity to address other areas of need in their communities. PCT
staff interviewed by the SMF Health Project Team revealed that
there is still a large amount of central oversight that restricts their
ability to innovate locally.
The second criticism is that targets are not necessarily coherent.
Why, for example, is diabetes represented, but not arthritis? Why is
there a specific target for the speed of referral for suspected breast
cancer, but other cancers do not receive the same attention? Surely
a more effective way of meeting patient expectations would be
for local commissioners to determine the key priorities of people
in their area.
SOCIAL MARKET FOUNDATION
124
The third criticism is that there is a bias in the set of national
targets towards acute elective care, and access to it. The biggest
drain on NHS resources is care for patients with chronic conditions,
but there are no targets to reduce unnecessary admissions to
hospital for people with ongoing health needs. Do targets really
reflect the NHS in its entirety?
Chapter 8 describes a new approach to regulating the
performance of local health services, putting responsibility on
commissioners to ensure quality in their local area. This cannot
be reconciled with a set of national targets that deny local
commissioners the autonomy they need to be innovative, and
to determine local priorities. This was a sentiment repeatedly
expressed by commissioners and primary care professionals at SMF
Health Project research seminars.
Alan Milburn, architect of much of the Blairite reform of the
NHS, said:
Top-down Whitehall control has tended to stifle local
innovation. It has too often ignored the differing needs of
different local communities. It is not surprising, therefore,
that staff sometimes feel disempowered, local communities
are disengaged, and patients have traditionally had little say
and precious little choice. Our reform programme – indeed,
any reform programme – for the health service should be
about addressing these weaknesses so that we can build on
the NHS’s great strengths.154
Mark Britnell, when head of world class commissioning at the
Department of Health, commented on the benefits of local
autonomy: “Staff feel more accountable for solutions and you
154 “House of Common Hansard Debates for 8 Jan 2003”, http://www.publications.parliament.uk/pa/
cm200203/cmhansrd/vo030108/debtext/30108-08.htm.
FROM FEAST TO FAMINE
125
certainly cannot blame your performance on anybody else.”155
A good start in rejecting a model of top-down Whitehall control
would be to reduce the range and scale of national targets.
recommendation 12: the list of national standards and
targets should be substantially reduced to become a
minimum service guarantee.
reducing the number and scale of national targets
This would achieve two goals:
1. It would free up commissioners to innovate locally.
2. It would acknowledge the desirability of a service that
is tailored to local need rather than aspiring to a set of
national standards.
National targets should focus on core access measures where
it is reasonable to set national standards, but leave local priorities
for improvement to commissioners, who will have to justify them
to the regulator and, more importantly, to their local populations.
A set of future national targets and core standards to replace
the list above might include:
Guaranteeing access
• a four-hour maximum wait in A&E from arrival to admission,
transfer or discharge;
• guaranteed access to a primary care professional within 24
hours and to a primary care doctor within 48 hours;
155 Quoted in N. Hawkes, “Independence Day?,” British Medical Journal, 334: 7604 (2007).
SOCIAL MARKET FOUNDATION
126
• a maximum wait of 13 weeks for an outpatient
appointment;
• a maximum wait of 26 weeks for an inpatient appointment;
• by 2010 , all cancer patients (surgery and drug treatment)
to wait no more than 31 days from decision to treat to start
of treatment.
Guaranteeing satisfaction
• patient satisfaction rates with local services to improve
each year;
• quality of local healthcare provision as assessed by the
CQC and through Quality Accounts to improve each year.
On this account, patients would be guaranteed access to
healthcare, but targets for improvement would be based entirely at
a local level. It should be noted that this would not limit the ability
of central government to invest in things like screening programmes
that require a national approach to be successful. It simply means that
local health services would be encouraged to develop local priorities
– reflecting their role at the heart of the NHS and the new regulatory
and accountability structures recommended elsewhere in this report.
DeFininG nhs values
Chapter 2 looks at how equity will be defined in the future. SMF
polling work suggests that fairness is a key priority for the public,
but that it means different things to different people. For some,
fairness means that everyone should have access to exactly the
same services, while for others it means that services should be
strictly based on an analysis of local need156. The tough financial
environment in which health services will have to operate for
the foreseeable future indicates that some elements that have
156 Furness and Gough, Local Control and Local Variation in the NHS: What Do the Public Think?.
FROM FEAST TO FAMINE
127
previously been considered unfair are likely to be needed in the
health system of the next decade – notably user charges. To reflect
public views and to encourage a more open political debate about
options for healthcare, there is a need for a stronger definition of
NHS values, building on the existing NHS constitution. While local
commissioners should determine local health priorities, national
government should play the key role in determining and adjusting
a defined set of NHS values.
The process of consulting and developing these values must
be managed by central government, helping to move the political
debate forward as new policy options for the health system
are considered.
GoverninG the nhs – no inDepenDent BoarD
Both the major political parties have raised the idea of an
independent board for the NHS in an attempt to depoliticise
decisions about the health system. As Chancellor of the Exchequer,
Gordon Brown investigated the possibility of replicating in the
NHS the model of the Bank of England and the BBC’s operational
independence. Under this kind of model, decisions about the
strategic direction of the health system would made by a panel of
experts.157 This has not become government policy, and meanwhile
the Conservatives are also in favour of such independence: “[B]
y establishing an independent board to run our NHS, we can
take politicians out of its day to day management.”158 The NHS
board that they envisage would have a statutory responsibility
to secure comprehensive health services, deliver improvements
in the physical and mental health of the population, and deliver
improvements in the diagnosis and treatment of illness.159
157 A. O’Dowd, “UK Chancellor Proposes Independent Board to Run NHS,” British Medical Journal, 333: 7570
(2006).
158 Renewal: Plan for a Better NHS (London: The Conservative Party, 2008).
159 Renewal: Plan for a Better NHS, 18.
SOCIAL MARKET FOUNDATION
128
Proposals for an independent board to govern the NHS are
in part a response to well-founded criticism of political micro-
management within the service. One study cited the following
examples of what they regard as unacceptable political interference:
• the fast-tracking of breast cancer drug Herceptin through
the NICE process;
• top-slicing of PCT budgets to compensate for over-spends
elsewhere in the system;
• the 2005 decision that PCTs should divest themselves
of provider services, which was subsequently partially
retracted.160
There has undoubtedly been unhelpful political intervention in
the management of the health system. But does this lead to the
conclusion that an independent board should oversee the running
of health services? While control by central government should
certainly be reduced, there are several reasons why an independent
board is not a desirable option.
accountability
The first objection is accountability. As stated above, central
government must retain a key role in raising resources. There are
strong arguments that an independent board made up of experts
would reduce overall accountability for a key part of government
spending. While the BBC might be operationally independent, for
example, it is able to sustain that independence through a Charter
that allows it the right to raise its own revenue via the license fee
and it operates in a competitive market. There is no precedent
or parallel for spending more than £110 billion a year of taxpayer
money through the direction of an independent board that the
general public would have no way of influencing or holding to
160 J. Glasby et al., Things Can Only Get Better? The Argument for NHS Independence (Birmingham: Health
Services Management Centre, School of Public Policy, 2007), 2.
FROM FEAST TO FAMINE
129
account. This makes it almost inconceivable that any such board
could or should possess or retain sufficient legitimacy to escape
the pressure of elected politicians.
what the public want
The second objection to the notion of an independent board is that
the public does not want one. As part of its work with members of
the public, the SMF Health Project explored the question of how
potential budget shortfalls in healthcare should be addressed. This
included a consideration of whether NHS or government should lead
prioritisation to save money. Many people were convinced that the
government has a key role to play in providing leadership in health
services – an implicit rejection of the idea of an NHS board. People
were concerned that decision-making left solely in the hands of the
NHS would be less accountable, and possibly less concerned with
overall levels of finance.161 Many people argued that government has a
key role in distributing resources to help achieve fairness. This is in line
with the recommendations set out throughout this report: national
government must retain a key role in raising money and allocating
resources, but with much more responsibility devolved to local health
services to design a range of services appropriate to local need. Thus,
central government should lose its day-to-day responsibility for
aspiring to the impossible (and undesirable) goal that the NHS should
be the same across the country, while maintaining its key function
of raising money and making sure it is distributed fairly. There is
currently, therefore, no strong case for an NHS board, nor is there
public support for the idea, particularly when political accountability
for public spending is set to become increasingly important.
conclusions
The future model for healthcare, if a high-quality universal system
is to be sustained, will be substantially different from today’s NHS.
161 Furness and Gough, Local Control and Local Variation in the NHS: What Do the Public Think?.
SOCIAL MARKET FOUNDATION
130
There are no further gains to be made from obsessive central
performance management designed to improve services across
the board. The future of the health system must see limited national
control, with as much authority and autonomy devolved to a local
level as possible. However, there are still certain key functions that
national government will undertake in the future.
recommendation 13: national government should
continue to have responsibility for revenue raising,
resource allocation, limited national standards and
defining nhs values.
These four key roles do not justify the introduction of a
supposedly independent NHS board: the need for accountability for
money spent and the views of the public support this conclusion.
It should not be forgotten that any act of public spending is, and
must remain, political, especially when it involves redistributing
resources from rich to poor and healthy to sick through the tax
system and the health system. While attempts should be made at
all levels to try to mitigate the impact of inappropriate interference
from central government, the politics of healthcare will not go
away, nor should they. Instead, they will be conducted at a local
level where the public can be involved in decisions about their care
and where local commissioners can be truly accountable for the
services they provide.
FROM FEAST TO FAMINE
131
Part twO
chapter Five: Decentralisation
It has been argued in chapter 1 of this report that, to enable
the cutbacks that will be necessary in health services over
the next decade, power should be moved from the centre to
the frontline and from the national to the local. This chapter
explores the advantages and problems with the various types
of decentralisation, before applying these lessons to the health
system in this country.
This chapter provides a context for the recommendations, set
out in detail in chapter 6, that power should be devolved to local
commissioners. It is argued that there is no single “right answer”
about the appropriate level of central and local control in health
systems. Ultimately, any decision to devolve power is a political
choice that must take into account the country’s political and
historical context. In the case of the health service in England, the
NHS has been subject to a decade of centralised control which
has succeeded in raising activity levels, but which has failed to
improve productivity and has left staff disillusioned. In this context
decentralisation appears to be the best option for improving the
quality, productivity and responsiveness of the health service, at a
time of significant fiscal restraint.
There has been much discussion over recent years, both
in government and amongst health policy experts, about the
importance of devolving more decision-making power to a local
level. David Nicholson, NHS Chief Executive, declared in the 2007/08
NHS Operating Framework that “the conditions are now absolutely
right for developing a framework within which PCTs, in conjunction
with their local communities, can set more of their own ambitions
SOCIAL MARKET FOUNDATION
132
rather than having them mainly set by Whitehall”.162 Compared
to the emphasis on top-down national targets that characterised
the early health reforms under New Labour, this emphasis on the
importance of local decision-making felt like a radical change of
direction. However, decentralisation within health policy is nothing
new; it has been an important issue in public policy right across
Europe for more than 60 years.163
what is Decentralisation?
Decentralisation can be defined in general terms as: “The transfer
of authority or dispersal of power in public planning, management
and decision-making, from the national level to sub national levels,
or more generally from higher to lower levels of government.”164
At its simplest, decentralisation is the diffusion of power and tasks
away from the centre towards more local levels of government or
to more local stakeholders.
Rondinelli, writing in the 1980s, set out the best-known
explanation of decentralisation. He identified four different types
of decentralisation: deconcentration; devolution; delegation and
privatisation.165
Deconcentration
Deconcentration refers to the transfer of decision-making away from
central government to lower-level government authorities who are
upwardly accountable to central government.166 Deconcentration
is the weakest form of decentralisation, as it redistributes decision-
162 Department of Health, The NHS in England: Operating Framework for 2007–08 (London: HMSO, 2006), 126.
163 R. B. Saltman and J. Figueras, Health Care Reform: Analysis of Current Strategies (Copenhagen: World Health
Organization, 1997), 45.
164 D. Rondinelli, “Government Decentralisation in Comparative Theory and Practice in Developing Countries”,
International Review of Administrative Sciences 47 (1981).
165 Ibid.
166 J. Ribot, Democratic Decentralization of Natural Resources: Institutionalizing Popular Participation
(Washington DC: World Resources Institute, 2002).
FROM FEAST TO FAMINE
133
making authority and financial and management responsibilities
among different levels of the national government.167
Deconcentration has been deployed in the past two decades in
a number of Eastern European states as a reaction against the central
control experienced under Soviet rule. In Poland, for example, major
reform of public administration was carried out in 1990 as a way
of breaking down the centralised model. The provincial authorities
acquired significant powers and were actively involved in making
decisions about the structure of health institutions.168
Delegation
Delegation is a more extensive form of decentralisation, which
involves the “delegation of decision-making and management
authority for specific functions to organisations that are not under
the direct control of central government ministries”.169 Decision-
making responsibility and administration of public functions is
transferred away from central government to semi-autonomous
organisations not wholly controlled by the central government, but
ultimately accountable to it. Governments delegate responsibilities
when they create non-departmental public bodies and quangos
(quasi-autonomous non-governmental organisations).170
Delegation takes institutions out of the direct control of
government regulation, allowing management to be more
flexible. The Italian health system underwent a process of
delegation in 1992 when the administrative structure of large
hospitals and “health units” was significantly reformed. The health
units and large hospitals were made into “public enterprises” and
167 Decentralization Thematic Team, “What Is Decentralization?”, http://www.ciesin.columbia.edu/
decentralization/English/General/Different_forms.html.
168 Saltman and Figueras, Health Care Reform: Analysis of Current Strategies. 45
169 D. Rondinelli, R. Nellis and S. Cheema, Decentralization in Developing Countries: A Review of Recent
Experience (Washington DC: World Bank Staff Working Papers No. 581, 1983).
170 Decentralization Thematic Team, “What Is Decentralization?”.
SOCIAL MARKET FOUNDATION
134
“public hospital agencies” respectively, with organisational and
administrational autonomy.171
In England, the same principle is behind the creation of
foundation trusts in the NHS. The control originally exerted
over these hospital trusts by the Secretary of State via Strategic
Health Authorities has been delegated to the chief executives of
foundation trusts, who enjoy a great deal of autonomy. In addition,
foundation trusts are not regulated by the Care Quality Commission
(which reports to the Secretary of State), but by the arms-length
regulator Monitor, which answers not to the Secretary of State but
to Parliament. This initiative is intended to delegate some control
over NHS institutions away from the iron grip of Whitehall, and
make health services more accountable and responsive to patients
and local communities.172
Devolution
Devolution refers to the process in which decision-making is
transferred not to a lower administrative level, but to a lower political
level. A process of devolution will require the strengthening or creation
of new lower levels of government that are, to a significant extent,
independent of central government.173 These levels of government
are typically regional or local, but in the case of devolution of power
from Westminster to Scotland, Wales and Northern Ireland, power was
devolved from the UK government to other national governments.
Devolution tends to result in a more radical restructuring of
health service organisations than deconcentration. This can be seen
by the way in which healthcare reform has evolved in the devolved
nations. Scotland, Wales and Northern Ireland now all have
significantly different healthcare policies from those of England.
171 Saltman and Figueras, Health Care Reform: Analysis of Current Strategies, 48.
172 E. Mayo and R. Lea, The Mutual Health Service (London: New Economics Foundation, 2002).
173 P. Clarke and J. Foweraker (eds), Encyclopaedia of Democratic Thought (London: Routledge, 2001), 126.
FROM FEAST TO FAMINE
135
privatisation
Rondinelli also includes privatisation in his typology of
decentralisation because power is shifted away from the centre
when tasks are transferred from public to private ownership.
criticisMs oF the Four part typoloGy
Although Rondinelli’s four-part typology of decentralisation is
the best-known attempt to define the process, it is by no means
undisputed. For example, it has long been argued by some
commentators that deconcentration is not actually a form of
decentralisation at all, as it does not lead to an increase in local
discretion in decision-making.174 Similarly, Rondinelli’s inclusion
of privatisation as a type of decentralisation is questioned by a
number of academics. It is argued that decentralisation involves the
transfer of authority and resources from the centre to the periphery
within a single system. Privatisation, on the other hand, involves
a transfer of power from the public sector to the private sector,
which requires the adoption of a different system of managing
activities. Hence, it is argued, decentralisation and privatisation are
two different processes.175
Because of the lack of clarity that surrounds the concept of
decentralisation, several health sector reforms have been lauded
as an example of the process even when it is far from clear whether
decentralisation did actually occur. For example, some policy
commentators highlight the shift of acute services from hospitals
to home care, which has occurred in many advanced health
systems over the past decade, as an example of decentralisation.176
174 J. W. Fesler, “Centralization and Decentralization”, in D L Sills (ed.), International Encyclopedia of the Social
Sciences (New York: The Macmillan Company and the Free Press, 1968).
175 C. Collins and A. Green, “Decentralization and Primary Health Care: Some Negative Implications in
Developing Countries”, International Journal of Health Services 24 (1994).
176 J. Wasem, “A Study on Decentralizing From Acute Care to Home Care Settings in Germany”, Health Policy
41 (2009).
SOCIAL MARKET FOUNDATION
136
However, such reforms do not entail a shift in the structure of power
or authority, so it is questionable whether they can be described as
decentralisation.
political, aDMinistrative anD Fiscal Decentralisation
The lack of clarity that surrounds the concept of decentralisation
in the world of health policy suggests that Rondinelli’s typology is
not entirely satisfactory. Saltman and Bankauskaite point out that
Rondinelli’s definition was designed for application in the public
sector in general and not for exploring the forms of decentralisation
that have developed specifically within the health sector. Saltman
and Bankauskaite therefore came up with their own definition of
decentralisation, which is directly applicable to the health sector.177
They split the process into three key functional dimensions:
political, administrative and fiscal decentralisation.
political decentralisation
Political decentralisation (like Rondinelli’s devolution) refers to
the shifting of policymaking responsibility from the centre to the
localities within a country. In England, there is little appetite for
political decentralisation of this type, which would see devolution
of health policy to local authorities. One of the main objections
to this is that PCT and local authority boundaries are not entirely
contiguous. For local authorities to take over health functions
would require yet another structural overhaul of the NHS.
Additionally, the existing organisational capacity of local authorities
does not include expertise on healthcare – the risk of this type
of political decentralisation would be great. However, there is a
need for greater cooperation between PCTs and local authorities,
particularly where individuals have needs that are addressed by
both health and social care.
177 R. B. Saltman and V. Bankauskaite, “Conceptualizing Decentralisation in European Health Systems: a
Functional Perspective”, Health Economics, Policy and Law 1 (2006).
FROM FEAST TO FAMINE
137
administrative decentralisation
Administrative decentralisation (like Rondinelli’s deconcentration)
refers to the transferral of decision-making to a lower administrative
level. The concept of administrative decentralisation emerged
within the field of public administration during the first half of the
twentieth century. It became an alternative to the Weberian notion
that bureaucracy imprisons individuals in an “iron cage”, limiting
individual human freedom and potential.
Instead, it was argued that public sector employees exercise
far more autonomy than Weber thought, as they constantly make
important organisational decisions. This recognition led to the
development of strategies designed to harness the informal power
of employees.178 In the health sector, this generated arrangements
to promote collective decision-making – for example, “consensus
management” in NHS hospitals in the UK.
Ultimately, administrative decentralisation led to the emergence
of the New Public Management (NPM) philosophy, which emphasises
the importance of choice, competition and the operation of markets
in the public sector. In the health sector, the idea of socially orientated
entrepreneurialism has been central to the concept of the “self-
governing trust” first proposed by the Conservatives in 1990, and
more recently reintroduced in Labour’s Foundation Hospital model.
There is scope to extend administrative decentralisation in the
health system in England. The increasing role of PCTs represents
an attempt to decentralise to local administrators. But, as chapter
6 makes clear, there is still a need for more power to be located
at PCT level and for central government to rein in its interfering
tendencies. At the same time much more must be done to
strengthen local commissioners to ensure that they can carry out
their responsibilities effectively.
178 Ibid.
SOCIAL MARKET FOUNDATION
138
Fiscal decentralisation
Fiscal decentralisation refers to the practice of fundraising and/
or expenditure activities being moved from the control of central
government to be performed instead by lower (regional or
municipal) levels of government.
The preceding chapters have shown that whatever system of
supplementary funding is introduced in response to the recession,
central government must remain responsible for raising money
and distributing resources. In part, this is a pragmatic decision – any
new form of financing would be difficult and costly to implement.
Centralised funding also enables a collective decision to be made
about the fair distribution of resource across the country. A regional
or local approach here would make it very much more difficult to
ensure equal access for equal need as poorer areas, particularly urban
centres, would find themselves at a particular financial disadvantage.
aDvantaGes oF Decentralisation
The discussion above has outlined the typologies of
decentralisation featured in the academic literature. But why might
decentralisation be desirable? A common criticism of centralised
administrations is that they are distant from service users and so
find it difficult to make appropriate and sensitive responses to local
preferences. On this critique, centralisation leads to poor-quality
public services and public disillusionment with what they see as
large, unresponsive, bureaucratic institutions. It is also argued that
central administrations are slow to change, slow to innovate and
are inefficient.
Proponents of decentralisation claim that these problems can
be overcome by transferring power, authority and responsibility
from the centre to lower and wider levels of government or
more local institutions. They argue that decentralisation will lead
to more flexible decision-making which will enable provision
FROM FEAST TO FAMINE
139
to respond more rapidly to changing circumstances and needs.
This freedom, it is argued, combined with pluralism, will also lead
to more innovation, as different localities develop interesting
and appropriate solutions to local problems and because large
monolithic structures are understandably risk-averse. Proponents
suggest that the effectiveness of policy decision-making will
improve because frontline workers have more information about
needs and are therefore better placed to identify problems
and devise effective remedies. Advocates of decentralisation
also suggest that it offers better opportunities for community
participation and greater accountability, as government officials
are more likely to be scrutinised by citizens who are engaged with
the process of policymaking and implementation.
Legitimacy in the eyes of the public is important if decision-
makers at any organisational level are going to be able to implement
reform.179 A system is more likely to be viewed as legitimate if
the public has some ability to provide input into the decision-
making process. A highly centralised health system that lacks clear
democratic processes may risk suffering diminishing support,
especially if potentially unpopular changes, such as reconfigurations
of services, need to be implemented. Decentralisation is seen as a
potential solution as it brings decision-making closer to the local
population and thus enhances satisfaction and acceptance in the
community.180
the DiFFiculties oF Decentralisation
Decentralisation has been embraced by policymakers as an
effective way of improving healthcare across Europe. However, the
outcomes of decentralisation have not always been evaluated fully
with proper consideration given to health gain, efficiency, quality
179 J. G. March and J. P. Olsen, Rediscovering Institutions (New York: The Free Press, 1989).
180 D. Stone, Policy Paradox: The Art of Political Decision-Making (New York: W. W. Norton, 1998).
SOCIAL MARKET FOUNDATION
140
of care and consumer choice. Decision-makers have on occasion
assumed that decentralisation will inevitably bring about positive
results, and so it has been trumpeted as an end in itself, rather than
as a way of achieving explicitly defined outcomes.181
Decentralisation should not be seen as a panacea: it must
be understood that decentralisation can throw up a number of
democratic, political and economic problems and difficulties.
The democratic argument against decentralisation emphasises
the degree of inequity that can accompany variation in service
provision; different standards of service are provided in different
localities with the result being that some citizens, often lower-
income or vulnerable groups, may receive poorer services. Evidence
from Finland, Norway and Denmark shows that local control over
health sector decision-making has led to increased disparities in
services provided, and it has been those individuals from lower
socio-economic groups who have been adversely affected.182
There is also concern that a localised system is more vulnerable
to political manipulation by particular stakeholders or interest
groups. This is why all increases in power for local commissioners
must be accompanied by strengthened local accountability
mechanisms to ensure that quality is upheld in every locality and
to prevent manipulation of the system from occurring. Further
thought is given to this issue in chapter 6.
Politically, there is a sense, especially in North European countries
with tax-funded health systems, that national politicians are blamed
when the health service fails to meet expectations (even if the
decision-making has been largely decentralised). Understandably,
181 K. Vrangbaek, “Key Factors in Assessing Decentralization and Recentralization in Health Systems”, in R. B.
Saltman, V. Bankauskaite and K. Vrangbaek (eds), Decentralization in Health Care: Strategies and Outcomes
(Buckinghamshire: Open University Press, 2007), 68.
182 R. B. Saltman, “Decentralisation, Re-Centralisation and the Future of European Health Policy”, European
Journal of Public Health 18:2 (2008).
FROM FEAST TO FAMINE
141
politicians tend to conclude that if they are going to be blamed for
what they cannot control, they may as well ensure that they have
the necessary controls so that they have some chance of correcting
any problems. It is also reported that deconcentration can lead to
confusion, with one level of government not knowing what the
other is doing.183 Currently in England, only a tiny minority of the
population actually knows what a local primary care trust is.184 If local
commissioners are to be given greater control over local services
and are going to be held to account by their local population, this
will need to change. In chapter 7 it is argued that much more effort
must be made by PCTs to publicise their existence, explain what
they do, and engage with their local population if local control and
accountability are to form a viable model.
The economic case against decentralisation focuses on the
inefficiency that results from a loss of economies of scale, and on
the likelihood of duplication, fragmentation and high transaction
costs of having multiple small providers. It is also argued that
small-scale units may have a limited capacity to handle complex
problems and that local finance bases are likely to be insufficient to
fund expensive future care needs.185
However, as set out in chapter 3, the SMF Health Project
does not recommend that NHS finances should be raised locally.
Furthermore, as discussed in chapter 6, strong local commissioning
can drive down costs and improve quality at the same time. Groups
of local commissioners, working together in partnership, can gain
the benefits of economies of scale, while also maintaining the
positive aspects of locally commissioned services held to account
183 D. J. Hunter, M. Vienonen and W. C. Wlodarczyk, “Optimal Balance of Centralized and Decentralized
Management”, in R. B. Saltman, J. Figueras and C. Sakellarides Critical Challenges for Health Care Reform in
Europe (Buckingham: Open University Press, 1998).
184 LGA Health Commission, “LGA Health Commission Opinion Polling – Results”, http://healthcommission.lga.
gov.uk/lga/core/page.do?pageId=579283.
185 M. De Vries, “The Rise and Fall of Decentralization: A Comparative Analysis of Arguments and Practices in
European Countries”, European Journal of Political Research 38:2 (2000).
SOCIAL MARKET FOUNDATION
142
by local people. And although there are certainly drawbacks to
a more localised system, there is no possibility that the NHS will
return to a centralised model of command and control – reform is
too far advanced for a rollback to be considered.
This chapter has thus far considered the theory behind
decentralisation. The next section turns to focus on the real world,
and evaluates the rise and fall of decentralisation in health policy
across Europe over the past 60 years.
rise oF Decentralisation
A central trend of European health policy over the past 60 years
has been the decentralisation of important aspects of decision-
making authority to increasingly lower levels of government, as
well as to private organisations. Decentralisation as a concept has
been accepted by many policymakers in Europe, although notably
not in the UK until very recently. However, in the second half of the
twentieth century, non-governmental control became part of the
“received wisdom” about what good health policy should include.186
For example, the tax-funded health systems in the European
Nordic countries have all experienced substantial health policy
decentralisation over the past few decades. In Sweden, Norway,
Finland and Denmark, most of the administrative and managerial
responsibilities, along with much of the policy and fiscal decision-
making control, has been decentralised within the public sector.187
The tax-funded health systems of Southern Europe have
also experienced this trend, with the majority of managerial and
political (but not key fiscal) responsibilities being devolved from
national to regional governments.
186 Saltman, “Decentralisation, Re-Centralisation and the Future of European Health Policy”.
187 Ibid.

FROM FEAST TO FAMINE
143
Countries with social health insurance systems in continental
Europe – such as Germany and the Netherlands – have not been
exempt from this decentralising pattern either. Most administrative
and managerial decisions, as well as many fiscal (but not key
political) decisions, have for a long time been delegated to private
not-for-profit bodies.
The state-based social insurance systems that have emerged since
1990 in many Central European countries have also decentralised
to a certain extent. Countries such as Hungary, Estonia and Poland,
reacting against the previously highly centralised model, have utilised
various forms of decentralisation. For example, ownership of hospitals
has moved from national to regional and local governments.188
recentralisation
For 50 years after the Second World War, decentralisation was
standard practice across European health policy. Over the past
decade, however, attitudes have been starting to change and
policymakers are reassessing the merits of decentralisation.
Since 2000, the role of the state in the health sector has begun
to strengthen measurably in many countries. State institutions
are beginning to change course and take back responsibility for
decision-making in many European healthcare systems. Countries,
especially those that have engaged in more radical decentralisation
of healthcare policy, are reclaiming control over key elements of the
system – typically, funding and setting professional standards.189
Norway is a prime example: responsibility for hospitals has swung
back and forth from central control, to local control and back. Initially,
political responsibility for hospitals in Norway was in the hands of the
national government. Then in 1969, control was decentralised from
188 Ibid.
189 Vrangbaek, “Key Factors in Assessing Decentralization and Recentralization in Health Systems”, 68.
SOCIAL MARKET FOUNDATION
14 4
state to regional level. However, the regional authorities failed to keep
hospital expenses within their agreed budget, which led to recurring
demands from regional governments for more state funds. Finally, in
January 2002, the Norwegian state recentralised both ownership and
policymaking for all Norwegian hospitals.190
A similar pattern of regional consolidation and a strengthening
of the state role has occurred in Denmark, the Netherlands and
Poland, and is under way in Sweden and Finland.191 So does this
mean that if the NHS embraces radical decentralisation it is
swimming against the tide of European policy? To a certain extent,
the answer is yes. But two points should be noted.
First, it is commonly agreed that the UK health system has
reached the limits of improvement through centralised control.192
To deal with the financial crisis in healthcare requires radical
thinking, and to move against the drift of policy in Europe may be
no bad thing. A significantly localised model of healthcare delivery
may prove to be the only possible future for public health services.
Localised services that meet local needs will be more efficient than
those imposed through central planning, just as a market economy
is more efficient than state planning.
Second, the English health system is much more centralised than
most of its European neighbours.193 As a result, if decentralisation
occurs in England while the rest of Europe recentralises health
policy, this can actually be seen as a convergence, rather than a
divergence, of policymaking.
190 J. R. Johnsen, Health Systems in Transition: Norway (Copenhagen: European Observatory on Health
Systems and Polices, 2006).
191 Saltman, “Decentralisation, Re-Centralisation and the Future of European Health Policy”.
192 See, e.g., Ara Darzi, High Quality Care for All: NHS Next Stage Review Final Report (London: HMSO, 2008);
The Conservative Party, Delivering Some of the Best Health in Europe: Outcomes Not Targets (London:
Conservative Party, 2008); The Liberal Democrats, Empowerment, Fairness and Quality in Healthcare:
Policies for an Effective NHS (London: Liberal Democrats, 2008).
193 Vrangbaek, “Key Factors in Assessing Decentralization and Recentralization in Health Systems”, 68.
FROM FEAST TO FAMINE
145
FinDinG the riGht Balance
So what can be taken from the European health policy experience
of decentralisation, followed more recently by recentralisation? The
first thing to note is that although it might appear that health policy
across Europe has lurched from one extreme to the other, in reality
this is not the case. The term “decentralised” and the categories
set out by Rondinelli as well as by Saltman and Bankauskaite are all
abstract concepts: they help us to understand what is going on, but
in reality no country has an entirely devolved, deconcentrated or
delegated health system. Just as there is no system that is completely
centralised with all decisions made at the highest possible level of
management, so too there is no country with a wholly decentralised
system where all decisions are taken at the lowest operational level.
In actuality, decentralisation in most European countries has
been focused on specific areas of decision-making. Policymaking
has become a shared exercise; local level decision-makers have
responsibility for a wide range of service-related decisions,
while the national level retains core strategic levers as well as
regulatory responsibilities. Successful decentralisation involves
balancing policymaking activities between national and regional
or municipal bodies.
Fiscal decision-making is often shared between national
and regional governments as opposed to being fully centralised
or decentralised. This is partly because control over finances is
politically important to national governments and so they are
reluctant to surrender it fully to lower-level bodies. For example,
county councils in Sweden raise 70% of their health sector revenue
from county-level taxes, while the remaining 30% comes largely
from state sources.194
194 Saltman and Bankauskaite, “Conceptualizing Decentralisation in European Health Systems: A Functional
Perspective”.
SOCIAL MARKET FOUNDATION
146
Concerns over equity also ensure that fiscal decentralisation
is balanced between national and regional levels. Countries tend
to have significant variations in wealth between regions, so most
fiscally decentralised systems include some sort of equalisation
payments to allocate extra resources to lower level governments
that are less well off.
Striking a balance between national and local accountability
structures is also important. Smaller units with decision-making
closer to the public are often seen as more transparent and easier
to hold accountable. The public find it easier to understand and
control processes at local levels rather than in large centralised
bureaucracies.195 However, on the other hand, there is a risk of
duplication of effort if quality assurance and data-collection
systems are based at the local level. It may also be more difficult
to compare performance across decentralised units, making
critical assessment harder to achieve. Therefore, a combination of
“decentralized decision units that are embedded in and supported
by centralised standards and evaluation of performance may be
the solution to this dilemma”.196 The issue of robust accountability
in a localised health system is given greater consideration in
chapter 7.
lesson For the nhs
There is no clear message for health policymakers in England; it
is possible to construct a strong intellectual argument both for
and against decentralisation. However, from the evidence that
is available, there seem to be some useful points that should be
borne in mind when considering whether to pursue a strategy of
decentralisation in the health sector.
195 Vrangbaek, “Key Factors in Assessing Decentralization and Recentralization in Health Systems”, 72.
196 Ibid.
FROM FEAST TO FAMINE
147
First, decentralisation should be regarded as a policy
mechanism to achieve a specific objective, not as an end in itself.
It must also be understood that decentralisation is not a panacea
to solve all structural and policy dilemmas. To be successful, a
health system needs a mix of decentralised and centralised areas,
so policymakers should concern themselves with the balance
between the two, a balance that will need to be continuously
adjusted to respond to competing pressures throughout the
system. There will always be trade-offs, for example between
“democracy”, “efficiency” and “participation”, which are ultimately
political considerations, rather than simply questions about
policy.197 A decentralisation strategy is based upon the “values,
objectives, and preferences of the decision-makers, which will
necessarily be context-dependent.”198
A country’s history, its bureaucratic infrastructure, its political
institutions, its civil society and the value base within that
society will all influence the appropriateness of various structural
choices in particular circumstances.199 In the case of the health
service in England, the NHS has been subject to a decade of
centralised control which has succeeded in raising activity levels,
but which has failed to improve productivity and has left staff
disillusioned. In this context, decentralisation is the best option
for improving the quality, productivity and responsiveness of the
health service.
Decentralisation is also the best way to drive change while
maintaining public support for the health service at a time of fiscal
constraint. As discussed above, legitimacy in the eyes of the public
is important if decision-makers are going to be able to implement
197 R. B. Saltman and K. Vrangbaek, “Drawing Lessons for Policy-Making”, in Saltman, Bankauskaite and
Vrangbaek (eds), Decentralization in Health Care: Strategies and Outcomes (Buckinghamshire: Open
University Press, 2007), 79.
198 Saltman and Vrangbaek, “Drawing Lessons for Policy-Making”, 80.
199 Vrangbaek, “Key Factors in Assessing Decentralization and Recentralization in Health Systems”, 69.
SOCIAL MARKET FOUNDATION
148
reform.200 A system is more likely to be viewed as legitimate if the
public has some ability to provide input into the decision-making
process. As such, decentralisation, which brings decision-making
closer to the local population, will help enhance satisfaction and
acceptance in the community, which will be crucial to the future
success of the health service at a time when difficult decisions
about resource allocation will need to be made.201
Finally, as set out above, a balance needs to be struck in which
decision-makers at the local level have responsibility for a wide
range of service-related decisions, while the national level retains
core strategic responsibilities as well as regulatory responsibilities.
Local commissioners must be granted the power and freedom to
innovate and take risks, but within a system that includes robust
national regulation.
what type oF Decentralisation?
As the preceding argument demonstrates, there is no pure form of
decentralisation. However, Saltman’s three functional dimensions
of decentralisation provide a framework to help determine where
decentralisation should and should not occur in the NHS.
recommendation 14: political and fiscal decentralisation
is not desirable, but administrative decentralisation
should be extended.
political decentralisation
The health system will not respond successfully to its crisis of
finance by delegating current national responsibilities to local
200 March and Olsen, Rediscovering Institutions.
201 Stone, Policy Paradox: The Art of Political Decision-Making.
FROM FEAST TO FAMINE
149
government. Not only does this fail to reduce the burden of
downwardly imposed targets and standards on local health
providers, but it would require a structural shift in the health
system to equip local government to take on responsibility for
healthcare. This is not a desirable option, and local government is
unlikely to play a substantially increased role in the management
of health services in the next decade.
Fiscal decentralisation
The preceding chapters have shown that whatever system of
supplementary funding might be introduced in response to the
recession, there is still a necessary role for central government in
raising money and distributing resources. In part, this is a pragmatic
decision – any new form of financing would be difficult and costly
to implement. Tax funding, while imperfect, has the advantage
of being cheap to collect and distribute. Centralised funding also
enables a collective decision about the fair distribution of resource
across the country. A regional or local approach here would make it
very much more difficult to ensure equal access for equal need as
poorer areas, particularly urban centres, would find themselves at a
particular financial disadvantage.
administrative decentralisation
As discussed above, administrative decentralisation ensures
that decision-makers are closer to, and in more frequent contact
with, the population. As a result, they should be more aware of
population needs and preferences and the public should have
more opportunities to participate in decision-making and to voice
their opinions.202
Administrative decentralisation also provides the opportunity
for decentralised units (in the case of the NHS local PCTs) to
offer differentiated services, thus allowing services to be tailored
202 Vrangbaek, “Key Factors in Assessing Decentralization and Recentralization in Health Systems”, 65.
SOCIAL MARKET FOUNDATION
150
to meet the needs of the specific population. Such differentiation
also allows local experimentation to take place which can
result in innovative solutions that are responsive and efficient at a
local level.203
Decision-making at a local level also promotes the use of
knowledge and experience accumulated by local staff and
strengthens feelings of responsibility among employees.204 It
is also argued that accountability and responsiveness may
increase by creating a shorter distance between users and
decision-makers.
As such, in place of top-down rules that tightly restrict the
day-to-day activities of lower level functionaries, commissioners
and providers should be subject to the lowest possible levels
of central control, with a radically reduced role for national
government that will largely be focused on raising money and
distributing it according to widely accepted definitions of what
is fair.
Local priorities should be reflected in a process of decision-
making that allows real variation. National guidance from
the Department of Health should be substantially reduced,
enabling local commissioners to work autonomously with local
populations to develop appropriate policy for their area. This
includes decisions about what services should be available, and
how money should be spent. Regulation will ensure that these
approaches are fair, and that they result in the delivery of high
quality services.
203 P. E. Mourtisen and J. Svara, Leadership at the Apex: Politicians and Administrators in Western Local
Governments (Pittsburgh: University of Pittsburgh Press, 2002).
204 O. E. Hughes, Public Management and Administration: An Introduction (New York: Palgrave, 2003).
FROM FEAST TO FAMINE
151
conclusion
In the light of these lessons about decentralisation, this report sets
out a vision for a health service that is based to a much greater
extent at a local level. Powerful, autonomous local commissioners,
free from central control, shape the local health system to suit
the needs and the wishes of the local population, who hold the
commissioners to account.
Such an approach will lead to care that suits local need and
will result in the development of a more efficient and innovative
service. But concurrently, the local thrust of the system will be
balanced by strong national regulation and a clearly defined role
for central government that will continue to raise money for the
NHS through central taxation, make resource allocation decisions,
set limited national standards and be responsible for defining
NHS values.
SOCIAL MARKET FOUNDATION
152
chapter six: coMMissioninG healthcare
The government sees commissioning as key to improving
quality and efficiency in the NHS. The Department of Health has
invested a lot of time and effort into developing the “world class
commissioning programme” in an attempt to raise the standards
of PCT commissioning as a route to improving services as a whole.
At the heart of a social market approach to healthcare is the idea
that a pluralistic and diverse approach to the delivery of services
is the best way to stimulate innovation and to ensure that those
services suit the needs of local people, thus improving both quality
and efficiency. However, it is clear that many PCTs are struggling to
manage the commissioning process.205 Past experience in the NHS,
as well as international attempts at commissioning, suggest that
excellent commissioning is very difficult to achieve. Some health
experts argue that the commissioning experiment will ultimately
prove to be fruitless.206
This chapter sets out a brief explanation of what commissioning
is and how the practice has evolved in the NHS, before considering
the lessons that can be taken from international attempts at
healthcare commissioning. The second half of the chapter focuses
on the world class commissioning programme before considering
what reforms should be introduced to improve healthcare
commissioning in England over the next 10–15 years.
Getting commissioning right will be key to squeezing out
as much performance in the health service as possible over the
coming years, in a context of what looks certain to be a much
tighter funding settlement post-2011, coupled with rising health
costs. There is no appetite in the health sector for any more
205 C. Ham, Health Care Commissioning in the International Context: Lessons From Experience and Evidence
(Birmingham: University of Birmingham, 2008).
206 J. Deffenbaugh and C. Ham, “Is World Class Commissioning the Answer?”, Health Service Journal (29 May
2008).
FROM FEAST TO FAMINE
153
extensive structural change, so it is essential to get the systems that
are in place working as well as possible.
Public sector spending will be significantly reined in after
the next general election. In the 2009 budget the Chancellor
announced £9 billion in new spending cuts on top of the
£5 billion identified in the pre-budget report in November,
adding up to a £14 billion annual reduction in public spending
from 2013. Financial commentators have suggested that the
Chancellor has not gone far enough and that cuts of around
£20 billion will be needed to reduce public sector borrowing
more rapidly.207 Most recently the NHS Confederation has gone
further still, warning that the NHS could face a shortfall in
funding of £15 billion over the next decade.208 Whatever the
exact figure, it is clear that there will be much less money to
play with over the next ten years. The NHS budget is protected
until 2011, but after that the service is going to have to prepare
for much more frugal times.
In this context, commissioners have a vital role to play in
shaping a health service that is high in quality and also efficient.
It is not certain that commissioners will be up to the task; it will
be extremely difficult for them to drive up quality, squeeze out
efficiency savings, improve productivity, prioritise treatments
and services, deal with continually changing health policy, and
keep the service afloat in a time of financial strain, coupled with
increasing demographic and technological demands placed upon
the service.
PCT commissioners are relatively new and inexperienced,
and are still quite weak in comparison to some hospital trusts.
Nevertheless, it is these local commissioning organisations that
207 K. Griffiths, “Public Sector Spending Slashed by £9bn in Budget 2009”, The Daily Telegraph (22 April 2009).
208 NHS Confederation, Dealing with the downturn (London: NHS Confederation, 2009).
SOCIAL MARKET FOUNDATION
154
are best placed to guide the NHS forward over the next decade –
precisely because they are local.
Local commissioners are best placed to:
• assess the needs of their local population and, with input
from patients and the public, determine what services to
provide;
• work with local providers to secure value for money for
the NHS;
• think innovatively and creatively about how to stimulate
the provision of cost-efficient and effective quality
services; and
• strike up a two-way conversation with their local
population about the shape of local services and about
prioritisation and decommissioning decisions.
It is intelligent healthcare commissioning that has the potential
to create more value for the users of the health service, the wider
public and the public purse.
After all, what are the alternatives? Central performance
management has driven up activity levels but at great expense
– both in terms of resources and in terms of the morale of staff.
Such tight control from Whitehall is no longer an option when
cuts are going to have to be made and justified at a local level,
and innovative answers are going to have to be developed to
meet pressing local need. The development of integrated care
organisations that both commission and provide services across
the healthcare environment has been suggested as an alternative
to PCT-level commissioning, but introducing such a system would
require a destabilising structural upheaval that the health service
cannot cope with at this point. As such it seems sensible to throw
our efforts into the difficult task of developing strong, intelligent,
strategic local commissioners.
FROM FEAST TO FAMINE
155
what is coMMissioninG?
The concept of NHS organisations purchasing health services is
not new. Since the introduction of the internal market in 1991, it
has been understood that, as well as providing services itself, the
NHS also negotiates agreements to purchase healthcare from other
provider organisations.
Commissioning, however, is a newer concept, which is less well
understood. Purchasing is an important part of the commissioning
process, but commissioning entails more than simply buying services.
At a minimum, commissioning is the technical or administrative
process of matching authorised service provision, as defined by the
Department of Health and the National Institute for Health and Clinical
Excellence (NICE), with the known health needs of a defined population.
This model “assumes a technocratic process of allocation that balances
a predetermined budget with politically and clinically defined
requirements”.209
However, commissioning is increasingly being viewed as
more than this, encompassing prioritisation decisions based
on the health needs of a defined population, while taking into
account mandated care and local and national health priorities.
This view of commissioning creates the opportunity for a process
of differentially valuing various forms of healthcare framed by
politically and clinically defined requirements.210
Although an accepted definition of commissioning in the NHS
remains elusive, it is the wider, more ambitious view of commissioning
that is being promoted under the latest NHS Operating Framework211
and the recent world class commissioning competencies.212 The SMF
209 J. Q. Tritter, Submission to the LGA Health Commission January 2008 ( 2008).
210 Ibid.
211 Department of Health, The NHS in England: The Operating Framework for 2009/10 (London: HMSO, 2008).
212 Department of Health, World Class Commissioning: Competencies (London: HMSO, 2007).
SOCIAL MARKET FOUNDATION
156
Health project held two expert health commissioning roundtables
and conducted an extensive interview process with healthcare
commissioners. This process revealed that, while different definitions
of commissioning are used, there is a growing agreement that the
commissioning process involves a number of central components:
• assessing health and social care needs of the target population;
• priority setting and allocation of resources to meet those
needs in line with local and national targets;
• contracting with providers or purchasing services to meet
those needs and targets;
• monitoring and evaluating outcomes;
• maximizing the use of data;
• assessing variations in clinical practice; and
• improving health outcomes and cost effectiveness.
With this ambitious definition in mind, what follows considers
the context in which healthcare commissioners in England will
have to operate over the next decade and asks whether there is
potential for better value for money to be delivered if they succeed
in achieving their goals.
coMMissioninG in context: value For Money as
puBlic sector spenDinG shrinks
Good-quality commissioning
Good-quality commissioning aims to save significant sums of
money and provide a better service for patients. And we know
that this is not just a theoretical concept, as good commissioning
is already making a significant difference: high-performing PCTs
are achieving much better results and saving a huge amount of
money, as compared to their lower-performing counterparts.
The NHS Institute for Innovation and Improvement has
published data that highlights the gulf between high- and low-
FROM FEAST TO FAMINE
157
performing PCTs for a number of different criteria. For example,
the way in which PCTs manage emergency admissions makes
a difference to the patient experience and to the amount of
resources spent. Many patients present at A&E with problems that
could have been avoided if they had been managed better in the
community. This is distressing for patients, and wastes A&E time
and NHS money.
NHS Institute data reveals that within West Midlands Strategic
Health Authority (SHA), for example, the top-performing PCT
achieved a rate of emergency admission in the third quarter of
2008 that was 13% below the expected level, while the lowest-
performing PCT’s emergency admissions rate was 53% above the
expected level. The data shows that if the lower-performing PCT was
to bring its performance up to achieve a population standardised
rate of admission in line with the top quartile performance, it would
save more than £6 million a year.213
Huge savings can also be achieved depending on the way in
which PCTs manage outpatient appointments. Many patients, for
example, could be treated effectively and more cheaply outside
hospital altogether, and follow-up of some patients could be
conducted over the telephone. The NHS Institute data reveals
that in the West Midlands SHA, the top-performing PCT could
have saved £53,000 a year if its referral rates had been in line with
the quartile of PCTs with the lowest standardised rate of referrals,
while the lowest-performing PCT in the SHA could have saved £1.3
million a year.214
Similarly, increasing low-cost prescribing by encouraging the
use of generic drugs, for instance, can save PCTs a huge amount of
213 NHS Institute for Innovation and Improvement, “Managing Variation in Emergency Admmissions”, http://
www.productivity.nhs.uk/Form_GetReport.aspx?period=2008-Q3&report=p22&orgCode=5PG.
214 NHS Institute for Innovation and Improvement, “Managing Variation in Outpatient Referrals”, http://www.
productivity.nhs.uk/Form_GetReport.aspx?period=2008-Q3&report=p24&orgCode=5PG.
SOCIAL MARKET FOUNDATION
158
money at no cost to the patient. The volume of statin prescribing
has increased significantly during recent years and there are large
cost differentials between the different statin drugs. By ensuring
that clinicians follow national clinical guidelines, PCTs can keep
prescribing costs down. A 28-day course of a branded statin is on
average about six times more costly than an appropriate generic
statin. If PCTs with below 78% use (achieved by the top quartile of
trusts) of lower-cost statins increased this to 78%, more than £64
million would be saved in a year.215
The NHS Institute data shows that in West Midlands SHA the
lowest-performing PCT could save more than £1 million a year if it
achieved a 78% rate of low-cost statin prescribing, while the highest-
performing PCT in the region was already achieving the 78% level.216
These are just three examples of the ways in which good-performing
PCTs in West Midlands SHA are saving millions of pounds a year, as compared
to their counterparts within the same SHA. This pattern is true in every SHA
across the country, which shows that although cost savings will be difficult
to achieve, they are not impossible. Commissioning organisations can be
strengthened by giving them more power and freedom to innovate
and focus on outcome-based commissioning, while commissioning
skills can be enhanced through education and training and through
spreading best practice and encouraging PCTs to work together to
build skills.
There is no guarantee that commissioning will ever become
“world class”, and it is clear that developing the strength and
skills of commissioners will be a difficult and slow process. But a
dramatic structural overhaul of the health service is unwelcome
and would be damaging. Instead, a concerted attempt to improve
commissioning appears to be the best hope for achieving a high-
215 NHS Institute for Innovation and Improvement, “Increasing Low Cost Prescibing for Lipid Modification”,
http://www.productivity.nhs.uk/Form_GetReport.aspx?period=2008-Q3&report=p43&orgCode=5PG.
216 Ibid.
FROM FEAST TO FAMINE
159
quality, effective, efficient health service which meets the needs
of local people and responds to their demands, in the context of
reductions in the growth of public sector funding that will have to
occur over the next decade.
If the NHS is to succeed in its aim of achieving world class
commissioning, it must look beyond its own shores to see how other
countries have approached the task of strategically commissioning
healthcare. Therefore, the chapter now turns to international attempts at
healthcare commissioning to consider what lessons the NHS can learn.
lesson FroM international experience
International attempts at healthcare commissioning offer some
useful lessons and insights for the English system.
information
In 1993, New Zealand separated commissioning and provider roles in
its health system, and this remained in place until 1999. A study of the
experience found that a lack of good information on costs, volumes
and quality hampered the commissioning process.217 However,
the study noted that the commissioning process encouraged an
increased focus on improving efficiency and quality of care.
size and skills
The USA, with a well-established market in healthcare, also provides
guidance for the more fledgling healthcare market in this country.
Donald W. Light summarised a number of lessons that the NHS should
learn from the American experience. He stressed that commissioning
organisations need to be large and strong and that commissioning
teams need to be intelligent, well trained and technically supported.218
217 T. Ashton, J. Cumming and J. McLean, “Contracting for Health Services in a Public Health System: The New
Zealand Experience”, Health Policy 69:1 (2004).
218 D. Light, Effective Commissioning (London: Office of Health Economics, 1998).
SOCIAL MARKET FOUNDATION
160
patient focus
A further study of commissioning in the US healthcare sector
during the period of managed care found that the health insurance
industry focused its strategies on understanding and influencing
physicians, with only secondary attention given to understanding
and influencing patients. The industry has subsequently had
to reposition itself as an agent of the patient rather than of the
employer and to focus its activities on informing and supporting
consumer healthcare choices.219 Although the health service
in England is different from the system of managed care in the
USA, what these findings highlight is the need for commissioners
in the NHS to keep the patients they are serving at the front of
their mind at all times. Commissioners must remember that it is
patients and the public that they serve, not doctors, clinicians
or provider organisations. Commissioners must engage with,
understand and inform the populations they serve, anticipate their
healthcare demands and work out how they can best be met,
while simultaneously working with providers to control costs and
improve performance.220
integration
The international experience makes it plain that healthcare
commissioning is difficult to do well. Chris Ham examined
healthcare systems across Europe, New Zealand and the US and
failed to find an example of “any working models of health care
systems where commissioning is working effectively across the
whole system”.221 Ham pointed to the complex nature of healthcare
and the need for commissioners to have a high level of technical
and managerial skills as the main reasons why it is so hard to
commission health services successfully.
219 J. C. Robinson, “Reinvention of Health Insurance in the Consumer Era”, JAMA 291 (2004).
220 Ham, Health Care Commissioning in the International Context, 5.
221 C. Ham, Commissioning in the English NHS: The Case for Integration (London: The Nuffield Trust, 2007), 8.
FROM FEAST TO FAMINE
161
Ham suggests that an integrated system which combines
commissioning and provision within the same organisation would be
more successful than doggedly persisting with an internal market in
health. He points to systems such as Kaiser Permanente (KP) in the
USA, which seem to perform well in comparison with other systems.222
KP is an integrated managed care organisation which operates
in nine US states with 8.7 million health plan members and 156,000
employees.223 It has received a lot of attention in England over the
past few years; the DH became impressed with some aspects of
the Kaiser operation, and there were suggestions that the NHS
should adopt some of its policies. It was argued that the KP model
delivers a cost-efficient and integrated healthcare service that lacks
the traditional distinction between primary and secondary care
and provides well-established pathways of care for many diseases.
It was suggested that the management costs of the system were
at least as efficient as the NHS and that it achieved fewer hospital
admissions per head of population.224
However, KP, unlike the NHS, does not deliver universal
coverage. It is not obliged to take all-comers and can cream off
the least risky patients who make low use of health services. This
practice is reinforced by healthier consumers self-selecting into the
lower-cost plans offered by managed care.225
As such, making direct comparisons between KP and the NHS
is difficult. There is no indisputable evidence that a KP-type model
would provide better or cheaper care than is currently achieved
in the NHS, and a number of commentators have actually argued
that the NHS is more efficient and provides higher-quality care.226
222 Ibid., 9.
223 “Fast Facts About Kaiser Permanente”, http://xnet.kp.org/newscenter/aboutkp/fastfacts.html.
224 C. M. Shapiro and A. McCall Smith, “Lessons for the NHS From Kaiser Permanente”, BMJ 327 (2003).
225 C. Donaldson and D. Ruta, “Should the NHS Follow the American Way?”, BMJ 331 (2005).
226 A. Talbot-Smith et al., “Questioning the Claims From Kaiser”, British Journal of General Practice 415 (2004).
SOCIAL MARKET FOUNDATION
162
In addition, the KP model combines commissioning and provision
within one organisation. Introducing this into the NHS would
require a rejection of the purchaser/provider split and would entail
significant structural change.
The Department of Health has invested heavily in a new
world class commissioning programme227 which would have to
be entirely overhauled if a KP model were to be introduced. The
potential benefits of such an overhaul are not certain enough to
justify the huge disruption, especially at a time when healthcare
professionals are desperate to avoid yet more structural upheaval
and the health service faces significantly tighter funding increases
over the next decade. Integrated care is discussed in more detail
later in this chapter.
Fundamentally restructuring the NHS once again,
particularly in a time of pressure on public finances, is not
the right approach to improving the quality and efficiency of
healthcare in England.
recommendation 15: the purchaser/provider split should
be maintained and attention should be focused on
improving commissioning performance within existing
structures.
The chapter now considers how commissioning came to
become central to the future of NHS, culminating, as it has done,
in the development of the world class commissioning programme.
227 Pockets of good commissioning exist, for example, Heywood, Middleton and Rochedale PCT, Sport
England and the Big Lottery Fund have joined together to regenerate local sports facilities.
FROM FEAST TO FAMINE
163
rise oF coMMissioninG in the nhs
Policymakers have been espousing the merits of purchasing within
the NHS for the past 20 years. The 1990 NHS and Community Care
Act introduced the “internal market” in an attempt to make the NHS
more efficient and less producer-dominated, by separating the roles
of the purchaser and the provider of healthcare (the “purchaser–
provider split”). At the same time, GP fundholding was established to
allow groups of GPs to take direct control over budgets for purchasing
hospital and other services. The “purchasers” (health authorities and
GP fundholders) used their budgets to buy health services (mostly
secondary care) from “providers” (such as acute hospitals, organisations
providing healthcare for the mentally ill, and ambulance services).
Health authorities and GP fundholders were granted the
freedom to alter established purchasing patterns in order better
to reflect the needs of their populations. However, they struggled
to influence powerful providers defending historical patterns of
service provision. Evidence suggests that despite the attempt to
beef-up the purchasing arm of the NHS, patterns of contracting
remained largely unchanged.228
The Labour government elected in 1997 immediately set
about reforming the internal market that had been set up by
the Conservatives, although the fundamental division between
purchasers – now termed “commissioners” – and providers
remained more or less intact. GP fundholding was abolished,
largely because of an aversion to markets in public services that
has since been overcome. Responsibility for purchasing healthcare
was taken away from health authorities and devolved to smaller,
newly created primary care groups (PCGs) made up of local GPs
and other clinicians.
228 M. Dusheiko et al., Trends in Health Care Commissioning in the English NHS: An Empirical Analysis (York:
University of York, 2006), 1–2.
SOCIAL MARKET FOUNDATION
164
Supply-side reform also occurred with the introduction of NHS
foundation trusts and independent sector treatment centres. At
the same time, the way in which NHS hospitals in England were
paid for the work they were doing was fundamentally changed. A
system termed “Payment by Results” (PbR) was introduced under
which hospitals are reimbursed for the activity they carry out using
a tariff of fixed prices that reflect national average costs: payments
to providers follow the patients they treat. This was meant to make it
easier for commissioners to switch providers or reconfigure services.
However, as was the case with the Conservative reforms of
the early 1990s, the small PCGs struggled to negotiate on equal
terms with the large providers. As a result, more recent policy has
attempted to strengthen primary care organisations in part by
merging PCGs to form larger, stronger entities. From the outset,
the 481 PCGs were supposed to evolve into 303 primary care trusts
(PCTs) after a probationary period in which they demonstrated
their ability to manage budgets and services. But in May 2006
the government announced plans to reduce the number of PCTs
to 152 to enable them to commission care more effectively and
economically. In addition, a variant of fundholding, known as
practice-based commissioning (PBC), was reintroduced, with GP
practices able to opt to hold budgets for secondary care.
Reintroducing commissioning capacity at GP level is at
odds with the government’s attempt to increase the size of
commissioning organisations. However, it was argued that different
services should be commissioned at different levels (local, regional
or national) and that PBC would in fact strengthen commissioning
by putting commissioning power in the hands of frontline clinicians.
This would lead to “high quality services for patients in local and
convenient settings” because “GPs, nurses and other primary care
professionals are in the prime position to translate patient needs
into redesigned services that best deliver what local people
FROM FEAST TO FAMINE
165
want”.229 Practice-based commissioning is discussed in more detail
later in this chapter.
This attempt by the Department of Health to strengthen the
commissioning arm of the NHS does not appear to have been much
more successful than the Conservative effort ten years earlier. A
study by Judith Smith et al. in 2004 found “little substantive research
evidence to demonstrate that any commissioning approach has
made a significant or strategic impact on secondary care services”.230
The study concluded that this was due in part to the fact that
commissioning organisations were not powerful or sophisticated
enough to exert their will on health providers because they lacked
the organisational stability enjoyed by many providers.
This conclusion is supported by research undertaken by the Centre
for Health Economics at York University, which found that in the period
between 1997/8 and 2002/3 the use of providers for elective care was
highly concentrated and became more so over time.231 The quality and
effectiveness of commissioning cannot be assessed solely in terms of
how concentrated the purchasing patterns are. Such concentration
may reflect the fact that PCTs were developing long-term relationships
with local providers, or that patients were reluctant to travel to more
distant providers. But whatever the cause, in this five-year period, at a
time when purchasers were actively encouraged by the Department of
Health to use a wider range of providers, the reverse occurred.232
More recently, PCTs have been subject to another wave of
reform, most notably with the introduction of the world class
commissioning programme.
229 Department of Health, “About Practice Based Commissioning”, http://www.dh.gov.uk/en/
Managingyourorganisation/Commissioning/Practice-basedcommissioning/DH_4138698.
230 J. Smith et al., A Review of the Effectiveness of Primary Care-Led Commissioning and Its Place in the NHS
(London: The Health Foundation, 2004), 2.
231 Dusheiko et al., Trends in Health Care Commissioning in the English NHS.
232 Ibid.
SOCIAL MARKET FOUNDATION
166
worlD class coMMissioninG
World class commissioning has been trumpeted by the Department
of Health as a key initiative to transform PCTs into commissioning
organisations that will drive up the quality of healthcare across the
NHS. Quality is the new maxim of NHS reform233 and the development
of world class commissioning is seen as a central lever to deliver it.
The world class commissioning programme, launched in
December 2007, aims to “transform the way health and care
services are commissioned”, delivering a “more strategic and long-
term approach to commissioning services, with a clear focus on
delivering improved health outcomes”.234
World class commissioning is a statement of intent made up of
four key elements:
• a vision for world class commissioning;
• a set of world class commissioning competencies;
• a support and development framework;
• an assurance system.
The vision, which outlines what world class commissioning means
(delivering better health and wellbeing, care and value), is backed up
by 11 core competencies set out by the Department of Health that
outline the knowledge, skills, behaviour and characteristics that a
world class commissioning organisation will need to develop.235
233 A. Darzi, High Quality Care For All: NHS Next Stage Review Final Report (London: HMSO, 2008).
234 Department of Health, “World Class Commissioning”, http://www.dh.gov.uk/en/managingyourorganisation/
commissioning/worldclasscommissioning/index.htm.
235 The 11 core competencies are: Locally lead the NHS; work with community partners; engage with public
and patients; collaborate with clinicians; manage knowledge and assess needs; prioritise investment;
stimulate the market; promote improvement and innovation; secure procurement skills; manage the local
system; make sound financial investment.
FROM FEAST TO FAMINE
167
SHAs have responsibility for supporting PCTs in achieving world
class commissioning by encouraging them to share services and good
practice, develop internal resources or buy in external expertise, for
example through the Framework for procuring External Support for
Commissioners (FESC). FESC enables PCTs to partner with independent
providers that can undertake aspects of the commissioning function
while remaining accountable to the PCT board throughout.
Most crucial of all to the success or failure of world class
commissioning is the new assurance framework which will hold
PCTs to account and reward performance and development. The
assurance framework is a nationally consistent system managed by
SHAs which will measure performance in three central areas: health
outcomes, competencies and governance. The three elements
will be assessed using a combination of self-assessment and
self-certification by PCTs, combined with the results of evidence
gathering and data analysis which will provide the input for a panel
day, which is the focal point in the commissioning assurance.236
The panel will make an assessment of the PCT across outcomes,
competencies and governance, and will provide developmental
advice to PCTs to support ongoing improvement.
For each PCT, a scorecard will be created to demonstrate their
performance relative to the national average for each outcome and
their rate of improvement relative to the national improvement
rate. PCTs will also be shown their performance adjusted for health
deprivation. For each of the 11 competencies, PCTs will be rated on
levels 1–4 (where level 4 is world class). The governance element of the
system focuses on whether the PCT board has a meaningful strategic
plan for commissioning, supported by a robust financial plan.
236 The panel will be made up of five individuals: the director from the local SHA; PEC chair or medical director
from another PCT; director of Adult Services or director of Children’s Services from another PCT; executive
director from an international organisation or another industry; PCT chief executive from another SHA
area.
SOCIAL MARKET FOUNDATION
168
Where an SHA has cause for concern about a PCT’s performance,
the PCT may be publicly designated as either “underperforming”, or
“seriously underperforming” or “challenged”. If a PCT is designated
as challenged, it would be subjected to an external review of
governance and board capability. Outputs from this would inform
the SHA of potential changes at board level. The SHA would sign
off a “turnaround plan” and, after a maximum of 12 months, the
SHA would submit a report to the NHS chief executive and make
recommendations either to remove the challenged designation
or to place the organisation “under direction”. Placing a PCT under
direction would involve action to take control of the board, and
could include replacing the board, outsourcing some or all of the
PCT functions or having another PCT take over.237
initial response to worlD class coMMissioninG
As mentioned above, this is not the first time that the Department
of Health has attempted to re-energise healthcare commissioning
and questions remain about whether this latest initiative will be
any more successful than previous reforms. However, there does
appear to be some optimism that the world class commissioning
programme could deliver this time. It is still very much in its
infancy, so at this stage it is difficult to determine its likely success.
Nevertheless, the initial response from PCT staff appears to be
reasonably positive. Commissioning is now seen as critical to
the NHS’s success in a way that was not previously the case, and
momentum seems to be building behind the programme.
The process to develop the world class commissioning strategy
involved stakeholders from across the health system, which means
that a lot of people are engaged with the process. The programme
has been praised for setting out a clear vision and aspirations
237 A. Laban, NHS Performance Regime (Yorkshire and Humber: NHS Yorkshire and Humber Strategic Health
Authority, 2008).
FROM FEAST TO FAMINE
169
for change. The core components of the assurance system
were designed and tested with the PCTs in the NHS North West
region and participating PCTs reported that the panel day was
“constructive, positively challenging and valuable”.238
assessing pcts
At the heart of the world class commissioning programme is the
assurance system for PCTs. This is intended to inform central government
and local stakeholders about commissioner performance, and make it
possible to compare results from different areas of the country.
Some concerns were expressed, before the publication of the
first round of results from the assurance framework, that almost no
PCTs would score levels three or four for any of their competencies,
meaning that there would be little gradation in scores and that
PCTs operating at different levels would end up with very similar
results. It was argued that, if this were the case, the rating system
would fail as an assessment of relative performance.239
However, the publication of the first round of results has taken place,
and although no PCT achieved level four for any of the 11 competencies,
level three was awarded 37 times, surpassing expectations that PCTs
would remain stuck at levels one and two. Mark Britnell, then Director
General of Commissioning at the DH, declared that the first round of
world class commissioning had gone “very well indeed”.240
Despite the general satisfaction with how the programme has
worked, some managers have warned that the scheme is at risk
of ‘gaming’ (this occurs when the rules of a system are used for
purposes outside what they were intended for). SHAs have stressed
the importance of PCTs achieving year-on-year improvements
238 A. Cowper, “World Class Commissioning: Quality Assurance”, HSJ (2008).
239 H. Crump, “Data Shortfalls Hinder World Class Commissioning Efforts”, HSJ (2008).
240 H. Crump, “PCTs Exceed Expectations in Year One”, HSJ (2009).
SOCIAL MARKET FOUNDATION
170
of their competency scores. As such, it has been suggested that
some PCTs deliberately attempted to score at a low level in the first
year so that improvements are easier to attain in coming years. A
senior PCT executive interviewed by the SMF Health Project team
indicated that such gaming of the assurance system was occurring
in his PCT. If such practices are widespread, it will devalue the
assurance framework’s grading system.
Another concern with the framework is that it rewards steady
PCTs that do not take risks. PCT Network director David Stout said:
“There’s an issue where if you’re ambitious but can’t articulate very
clearly how you’re going to achieve your ambition, the system will
mark you down.” It is important that the system does not create
overly cautious, risk-averse PCTs that focus on scoring well on world
class commissioning assurance tests rather than commissioning the
best healthcare for their population. Innovation may also be stifled
as PCTs focus solely on the 11 centrally determined competencies,
thus undermining a major benefit of the devolved approach.
There is also a possibility that the assurance process will uncover
more about the different approaches to the framework adopted
by the SHAs than the actual performance of PCT commissioners.
The NHS Alliance is concerned that the framework could become
a means for SHAs to exert undue influence and impose their own
agenda.241 Chair Michael Dixon questioned whether the process
will distinguish between those that commission well and those
that do not, “or will it be based on PCTs commissioning in the way
the SHA thinks they should?”242
John Appleby, Chief Economist at the King’s Fund, agrees,
pointing out that SHAs will be key decision-makers in awarding
scores and providing an assessment of PCT performance, and so will
241 H. Crump, “SHAs Urged Not to Abuse Their Power”, HSJ (2008).
242 Ibid.
FROM FEAST TO FAMINE
171
have the potential to manage the outcome to suit their preferred
approach to performance management.243 This could make
comparison of PCT performance across the country questionable,
as some SHAs may hold different interpretations of the scoring
criteria from others. It may also introduce a degree of subjectivity
into the system, which would weaken its credibility.
There are also question-marks about whether the new system
will actually lead to significant changes in commissioning patterns –
a goal that has so far remained out of reach. A survey by Health Service
Journal found that two out of three PCTs failed to decommission any
services in 2007.244 Decommissioning is not the only way to improve
services, and cancelling a contract is unlikely to be a commissioner’s
initial response to poor outcomes. Instead, commissioners would
be expected to work with providers to agree standards that will
improve quality and efficiency. However, world class commissioners
are supposed to stimulate the market, manage the local health
system and make sound investments, which will inevitably require
some services to be decommissioned, and currently PCTs are failing
to do this. This failure is underlined by the fact that PCTs performed
worst at competency seven: stimulating the market. While 17 PCTs
achieved level two, and no PCTs reached level three or four, 135 PCTs
only managed to reach level one, the lowest mark available.245
While the world class commissioning programme offers a useful
definition of commissioning, and is rightly considered a crucial
mechanism to improve the quality and value for money of the NHS,
there are clear issues with the way in which PCTs report on their
performance and how they are assessed by external agencies. As well as
this, there are problems of organisational underperformance that will be
present in any complex public service. The world class commissioning
243 Ibid.
244 H. Crump, “PCTs Failing to Decommission Services”, HSJ (2008).
245 Crump, “PCTs Exceed Expectations in Year One”.
SOCIAL MARKET FOUNDATION
172
programme must develop in the next few years to truly empower PCTs
to commission services effectively in their local area. This requires not
only a different approach to regulation, but also an in-depth focus on
the strategic performance of commissioning organisations.
A successful PCT assurance system must:
• provide detailed, comparable information about PCT
performance for public consumption;
• drive up PCT performance;
• support quality and ambition;
• encourage innovation;
• support decommissioning and encourage efficiency.
how to iMprove coMMissioninG in the Future
The SMF Health Project has identified many of the trends and
challenges that the health system in England will face over the
next 10–15 years, set out in detail in the project’s five background
papers.246 Commissioning is central to driving up performance
in the NHS and has the potential to create a health system that
reflects the needs of the local population in an innovative way.
However, for this goal to be achieved, some changes to the current
approach to commissioning are needed. The next section of this
chapter sets out a number of recommendations that aim to ensure
that commissioning is successful in the future.
skills
If commissioning is to succeed in driving up quality in the NHS,
the capability, capacity and profile of individuals who work for
246 SMF Health Project background papers: Paper1 – An Overview of Health Systems Reform and the NHS; Paper
2 – Demography and Technology: External pressures for Change ; Paper 3 – Commissioning Healthcare ;
Paper 4 - Providers of Healthcare; Paper 5 – Patients in the Health System. The background papers can be
downloaded from the SMF website: www.smf.co.uk
FROM FEAST TO FAMINE
173
commissioning organisations, and the organisations themselves,
need to be strengthened. The world class commissioning
framework sets out 11 useful commissioning competencies.
However, a nationally dictated set of skills and competencies
will not meet all requirements; PCTs will need different skill sets
to meet different needs. As such commissioning skills should be
developed at a local, regional and national level. This is happening
already to a certain extent; the Department of Health’s world class
commissioning team stresses that development may be self-
managed by PCTs, directed by SHAs or led by the department.247
West Kent PCT is an example of best practice in this respect. At
a national level, West Kent is involved in working collaboratively
with other PCTs on new development programmes, designed
to support boards in readiness for change. Regionally, West
Kent is in the process of reaching an agreement with Brighton
and Sussex University Medical School to run an MSc in health
commissioning. Locally, West Kent is creating a PCT-run
commissioning graduate development programme which will
be complementary to, but not part of, the national management
trainee scheme.248 This is intended to supply the PCT with the
skills it needs for the future, and is surely a more profitable use
of resources than striving to demonstrate adherence to a list of
centrally determined priorities.
recommendation 16: pcts must continually assess the
skills and competencies that they require to successfully
commission at a local level, and then strive to develop
those capabilities.
247 A. Cowper, “Supporting World Class Commissioning”, HSJ (2008).
248 Cowper, “Supporting World Class Commissioning”.
SOCIAL MARKET FOUNDATION
174
Commissioning skills are not just about managing data and
drawing up contracts; equally important is a cultural shift away from
a rigid focus on current systems to think instead about new ways of
achieving improvement through, for instance, engagement with all
the people who are effected by the system – managers, clinicians
and community members. A change in commissioning culture that
understands the power of people’s values and the motivational
force of engagement is just as important as system change.
investMent in skills
Significant investment in commissioning skills is required.
Commissioners need to be expert at a number of different skills –
risk analysis, health economics, procurement and data management.
Currently only around 1.4% of the NHS budget is devoted to the
mechanics of commissioning, whereas this figure is believed to be
about 5–6% in other health systems in the developed world.249 PCTs
don’t have huge management resources and, because of a political drive
to cut down NHS bureaucracy, a cap on numbers of personnel exists.
To function properly, PCTs must be allowed to develop themselves as
organisations rather than bowing to political pressure that demonises
bureaucrats. Health system performance will be improved with an
increased emphasis on management skills in commissioning. Better
management will also improve the capacity of PCTs to deal with
information flows in the health system that can be overwhelming.
Commissioners need to play a much more active role in promoting
quality in healthcare, and information about provider performance is
central to this. However, there are real fears that PCTs are simply not
very good at dealing with information in an effective way. Good local
commissioning will only be achieved if PCTs are enabled to develop
their management skills and capacity without top-down control of
the numbers of staff they are permitted to employ. This is not about
249 J. Appleby, “How to Get Commissioning Working Better: Skills, Data, Subsidiarity and Culture”, http://www.
commissioninghealth.com/index_files/v2n2Appleby.htm.
FROM FEAST TO FAMINE
175
creating large new bureaucracies, but about putting commissioners on
a level playing field with mature acute providers.
recommendation 17: the cap on pct personnel numbers
should be removed granting pcts responsibility for
determining their own staffing levels.
proFessional stanDarDs
As commissioning is becoming increasingly complex and central to
the way public sector services are delivered, there is a growing case
for a more formal recognition of commissioning as a professional
discipline. Commissioners, both as individuals and organisations,
would benefit from the development of mechanisms for increasing
their influence, developing their skills and capabilities, and raising
their profile. This could be achieved through a form of membership
organisation or professional body which could develop a set
of professional standards for commissioners. There are already
organisations, such as the Institute of Commissioning Professionals,
that aim to improve professional standards. Additionally, the
medical profession is well supported by a number of royal colleges
that both represent the collective interest of their members, and
also play a central role in training and professional standards.
However, for a number of reasons such a formalised approach
may not be the best option. First, in most cases commissioning
is an organisational responsibility, not an individual task. It is
not possible for an individual to possess all the competencies
required for effective commissioning, and there is concern
that the ability for an individual to become a professional
commissioner would undermine the notion of public sector
organisations as commissioners.
SOCIAL MARKET FOUNDATION
176
In a similar vein, because of the organisational nature of
PCT commissioning, there would be a question as to who
from the PCT should become accredited. Would it only be the
director of commissioning? Or would the chief executive have
to be accredited, or would all the senior mangers need to be
professional commissioners? And if it was only PCT managers who
became professional commissioners, it might create the idea that
commissioning is a “management” function that does not concern
other professionals. This would be at odds with the current DH
policy of practice-based commissioning, which encourages GPs to
view commissioning as a central part of their existing professional
role, not a new profession they need to enter.
Finally, the context-specific nature of commissioning competency
means that different individuals and organisations will need to develop
different skills in order to be competent. Defining a standardised
qualification or accreditation criteria that was applicable and stretching
for all would be hard to achieve, and could detract from the important
task of addressing specific local development needs.
recommendation 18: a formal set of individual commissioning
competencies should not be developed for nhs commissioners.
While a role is not envisaged for standardised commissioning
qualifications, the voice of commissioners should be strengthened to
enable them to stand up to provider organisations, recruit high quality
staff and stamp their authority on the health service. Currently, the
PCT Network, which was launched in December 2006, now has 95%
of the trusts as members and represents their interests. The Network
was established to improve the health system by raising the profile of
issues affecting PCTs and strengthen the influence of PCT members.
The Network aims to strengthen commissioning by putting in place
a support and development programme for PCTs around world class
FROM FEAST TO FAMINE
177
commissioning competencies. It also has a role influencing the regulatory
landscape positively for its members, enhancing the reputation of PCTs
and identifying examples of PCT successes.250 The Network puts on
seminars, conferences and forums to promote networking and learning
and publishes papers and information on primary care issues.
The PCT Network has made a strong start in its short existence.
According to Mark Britnell, it “is a highly effective membership
organisation that makes its point clearly and firmly”.251 However, a
number of changes could be made to give the organisation more clout
and make it a more effective vehicle for improving the quality and
strengthening the standing of healthcare commissioners in England.
First, it may be beneficial for the body representing
commissioners to be totally independent. At present, the PCT
Network is part of the NHS Confederation – a trade association
representing all types of NHS organisations with a number of
networks focusing on specific parts of the NHS. A commissioning
body would have more freedom if it was not part of a larger
organisation but stood alone with the sole responsibility of
furthering the interests of healthcare commissioners in England.
Second, the PCT Network is, in effect, a trade body for those
commissioners who work in PCTs. However, in the future it should
broaden out to include all healthcare commissioners in the health
system, moving from being a PCT Network to become a Healthcare
Commissioner Network. In a similar vein, at present the network
covers both commissioning and provider elements of PCTs’
roles, but PCTs are increasingly separating out these roles. In the
future, the Commissioner Network should focus exclusively on the
commissioner role, with provider interests supported elsewhere.
250 Primary Care Trust Network, “About the PCTN”, http://www.nhsconfed.org/Networks/PrimaryCareTrust/
AboutThePrimaryCareTrustNetwork/Pages/AboutPCTN.aspx.
251 Primary Care Trust Network, “Become a Member”, http://www.nhsconfed.org/Networks/PrimaryCareTrust/
Pages/BecomeAmemberPCTN.aspx.
SOCIAL MARKET FOUNDATION
178
Third, although a commissioning body would not develop a set
of professional commissioners skills, there is no reason why it could
not take on a number of roles that royal colleges currently carry
out for their members. This could certainly include an educational
element. A commissioning body could provide:
• distance learning;
• network accredited courses;
• study days;
• short courses;
• workshops; and
• assist commissioners in undertaking training courses or
other educational activities run by other establishments;
It could also:
• establish regional faculties to effectively support
commissioners across the country;
• actively encourage talented people to become healthcare
commissioners;
• publish work by members and others to improve
healthcare commissioning by spreading innovative ideas
and approaches and engendering discussion;
• diffuse information on all matters affecting healthcare
commissioning and establish, print, publish, issue and
circulate papers, journals, magazines, books, periodicals
and other publications;
• publish guidelines and best practice statements;
• undertake research to better understand the art of
healthcare commissioning, and encourage members and
others to do likewise;
• hold meetings, conferences, seminars and instructional courses;
• cooperate and form partnerships with other bodies to
further the aims of the Network;
• provide information to the general public, media and
external official bodies.
FROM FEAST TO FAMINE
179
recommendation 19: the current pct network should
develop to take on a role similar to a royal college, as a
way of strengthening commissioners in the nhs.
nice
NICE provides commissioners with crucial support and information.
The Institute produces web-based commissioning guides that
provide topic-specific information to help ensure that effective,
evidence-based care is commissioned.
Each commissioning guide offers practical advice on issues
such as local needs assessment and opportunities for clinical
service redesign. The guides set benchmarks to help commissioners
determine the level of service needed locally.
Within each guide, an interactive commissioning tool enables
commissioners to estimate the cost of local commissioning
decisions. The tool can help commissioners to:
• identify local service requirements;
• review current levels of commissioned activity;
• identify future change in capacity required using the
indicative benchmark provided;
• model future commissioning intentions and associated
costs over three years;
• calculate potential set-up and recurrent costs over three years.252
In addition, the NICE appraisal process provides essential
information about the clinical and cost-effectiveness of health
252 National Institute for Health and Clinical Excellence, “NICE Support for Commissioning”, http://www.nice.
org.uk/media/6BD/98/NICESupportForCommissioning2008.pdf.
SOCIAL MARKET FOUNDATION
180
technologies. This will become increasingly important as
commissioners attempt to squeeze out efficiency savings in the
years ahead.
Health minister Ara Darzi has set out an expanded role for
NICE, which is now expected to make more rapid appraisals
of new drugs and set national quality standards.253 This is to be
welcomed, but it is important that NICE appraisals do not end up
focusing exclusively on new pharmaceuticals at the expense of
existing devices and procedures. If commissioners are going to
drive out ineffective practice, they will rely on NICE to assess old
technologies, as well as new ones, so that they can commission
the most cost-effective treatment.
The expansion of NICE’s role will require additional resources
and, at a time of fiscal consolidation, finding extra money for a
quango will be difficult. NICE’s £30 million annual budget has already
come under attack in the media.254 However, investing in NICE is
money well spent, as it will lead to savings in later years. In addition,
the world-class reputation that NICE has required is starting to pay
dividends. NICE has begun to offer consultancy services to foreign
governments, such as in Ghana, Colombia, Jordan and Turkey,
which could bring in an important revenue. The Institute is also
beginning to offer scientific advice to companies seeking to tap
into NICE’s experience in health technology assessments.255 Again,
this could prove to be very lucrative.
recommendation 20: the capacity of nice to appraise
existing procedures, as well as new ones, needs to be
strengthened.
253 Darzi, High Quality Care for All.
254 R. Robinson, “New Look NICE”, http://www.fleishman-hillard.co.uk/uploads/documents/NewLook.pdf.
255 Robinson, “New Look NICE”.
FROM FEAST TO FAMINE
181
recommendation 21: the commercial capacity of nice
to offer consultancy to governments and private sector
companies should be expanded.
inteGration
Following the primary care strategy of the Darzi review, integrated
care organisation pilots are currently under way. Colleagues in primary,
secondary and tertiary care can come together to offer a joined-up set
of services provided under the umbrella of an integrated care contract.
Some commentators are calling for the establishment of
integrated care organisations along the lines of the American-
managed care provider Kaiser Permanente that combine
commissioning and provision and compete for patients. It is argued
that the introduction of such a system would lead to patient-centred,
joined-up care provided in the community rather than in hospitals,
which would be better for the patient and cheaper to provide.
There is no doubt that the current system in England is far too focused
on acute, hospital-based care and there is insufficient collaboration
between healthcare sectors. For too long, ministers and civil servants
have focused their attention on the acute sector, contributing to an
organisational culture where hospitals are given undue attention. In an
era of sophisticated speciality medicine, patients need to be diagnosed
and treated in multispeciality health centres where primary care teams
work in partnership with specialty nurses and doctors, laboratory and
imaging technicians and the pharmacy team.256
However, as discussed above, introducing integrated care
organisations along the lines of Kaiser Permanente would require
256 D. Light and M. Dixon, “Making the NHS More Like Kaiser Permanente”, BMJ 328 (2009).

SOCIAL MARKET FOUNDATION
182
significant structural change and the establishment of a different
funding mechanism for healthcare in England. The potential
benefits of such a transformation do not outweigh the massive
costs of upheaval that such a radical change would require.
Instead, the action plan originating from the Darzi review is
attempting to stimulate integrated care under the current system, which
is a worthwhile goal. However, it is important that integrated services
are allowed to develop organically at a local level to meet local need,
rather than the DH dictating how integration should develop and what
integrated care models should look like. The focus of the integrated care
pilots must be on the outcomes delivered rather than on the structure of
the organisation delivering the care. In some cases, clinicians from across
the health service will merge together into one organisation to offer
integrated services to a PCT; in other cases colleagues will look instead to
improve their information systems and governance structures to enable
them to work together more seamlessly.257
There are already pockets of very effective integrated care
across the NHS. In Bolton, for example, there is a locally managed
diabetes network that strives to provide patient-centred, integrated
care that is delivered in the appropriate place at the appropriate
time by the appropriately trained professional. The plan is that
Bolton will have a fully integrated service that irons out gaps or
duplication, and ensures a smooth referral from primary care to
specialist advice.258 This shows that where there is a shared long-
term vision, effective integration can be achieved.
recommendation 22: pcts and local providers must
be given the freedom to develop integrated care
organisations at a local level to meet local need.
257 “NHS Next Stage Review: The Whole Package”, HSJ (2008).
258 C. Ham, Integrating NHS Care: Lessons From the Front Line (London: The Nuffield Trust, 2008).
FROM FEAST TO FAMINE
183
aBolish national contracts
The growth of integrated multidisciplinary organisations that
provide care across sectors will lead to the development of new
professional roles and the need for contracts to reflect new
ways of working. Britnell recently suggested that the “the logical
conclusion of the success of integrated care organisations is
that they will lead to the abolition of the national [GP and
consultant] contracts”.259
It seems sensible for PCTs to be able to set pay and working
conditions as part of contractual negotiations with providers.
This would lead to the emergence of innovative services and new
clinical roles that meet local need and emerging demand, and
could also lead to better value for money.
In addition, a number of experts have suggested that the general
medical services contract prevents PCTs from dealing effectively with
poor-performing practices. Peter Reader, chair of the NHS Alliance
professional executive committee network and medical director at
Islington PCT, reveals that because of the nature of the GP contract,
practices in some areas are able to create a “smokescreen” of paperwork
behind which to hide poor performance.260 PCTs will instead draw up
local contracts with the freedom to define new roles to meet specific
local needs, set pay and conditions to attract the right staff, and use the
contract as a robust way to deal with poor performing practices.
recommendation 23: national contracts for Gps, consultants
and other medical staff should be abolished, and
renegotiated at a local level when they come up for renewal.
259 R. Finch, “Commissioning Chief Predicts End of Traditional Doctors’ Contracts”, BMJ 337 (2008).
260 C. Santry, “Care Quality Commission: a Chance to Peep Under the Primary Care Carpet”, HSJ (2008).
SOCIAL MARKET FOUNDATION
184
It has been argued that abolishing national contracts will lead to
big increases in GP and consultant pay as the DH’s bargaining power
will be lost and doctors will be able to drive up their salaries by playing
local organisations off against each other. However, this argument
loses its power in the wake of the latest national GP and consultant
contracts, both of which led to significant increases in pay. The recent
GP contract led to an average increase in GP earnings of 22.8% in its first
year taking an average annual GP salary up to £100,170. An investigation
by the National Audit Office published in early 2008 concluded that the
contract had cost substantially more than the DH had budgeted for
– nearly £1.8 billion in the first three years.261 Similarly, in the first three
years of the new consultant contract, consultants received an extra 27%
in pay, increasing their average annual pay from £87,000 to £110,000 by
2005–6. Over the same period the number of hours worked by full-time
consultants for the NHS decreased by an average of 1.4 hours per week
from 51.6 to 50.2 hours. This rise in pay was greater than the DH had
anticipated: by the end of March 2006, the department had spent £715
million on the new consultant contract, 27% more than the original
estimate of £565 million.262 The DH has failed to negotiate a good
deal for the tax-payer when it comes to GP and consultant contracts,
so local PCTs and provider organisations should be free to set wage
scales themselves.
Joint workinG
In the future localisation must become the watchword of the
health service, with devolved responsibilities a major driver of
improvement.
However, PCTs are geographically too small and lightly
staffed to be able successfully to carry out certain important
261 National Audit Office, NHS Pay Modernisation: New Contracts for General Practice Services in England
(London: National Audit Office, 2008), 6.
262 S. Williams and J. Buchan, Assessing the New NHS Consultant Contract: A Something for Something Deal?
(London: The King’s Fund, 2006).
FROM FEAST TO FAMINE
185
tasks. The answer to this problem is not a further round of
disruptive mergers that would dilute many of the positive aspects
of a localised service. Instead, the goal must be to increase the
capacity, expertise and influence of PCTs without undermining
the values of locality, or wasting public money on duplicated
functions where they are not needed.
An important factor in achieving this goal involves PCTs working
together in partnership. Individual PCTs are relatively small and do
not have enough commissioning clout when dealing with large
acute hospitals. This is particularly true in London; for example, it
takes six PCTs to account for just 60% of Imperial College Healthcare
NHS Trust’s NHS income. A PCT acting alone has little purchasing
power over such a large provider.
PCTs also currently struggle to fill gaps in crucial areas of
expertise such as health economics and predictive modelling.263
These skills would be expensive for a single PCT to recruit
or procure, so greater collaboration with neighbouring PCTs
is necessary.
Partnerships between PCTs are beginning to occur.
For example, Hammersmith and Fulham, Kensington and
Chelsea, and Westminster PCTs have joined together to
create a “commissioning alliance”. The three PCTs share similar
demographics, health priorities and investment strategies,
and commission the majority of hospital care from the same
two hospital trusts (Imperial College Healthcare NHS Trust and
Chelsea and Westminster Healthcare NHS Foundation Trust), so
close collaboration makes sense. The three PCTs understand
that they can bring the greatest improvements to the health of
residents across the three boroughs by creating a single team
263 S. Whiting, “Primary Care Trust Proposals for Strengthening Commissioning in Hammersmith and Fulham”,
http://www.lbhf.gov.uk/Images/HASCSCrevisedreport05112008_tcm21-108713.pdf. (3)
SOCIAL MARKET FOUNDATION
186
equipped with the skills and capacity to improve the quality of
commissioning decisions and reduce duplication of analytical,
contracting and quality assessment processes.264
The commissioning alliance is initially focusing on acute hospital
commissioning, along with contract and performance management
of pharmacists, dentists and opticians. However, it is hoped that
further joint commission will be developed in the future.265
This initiative has brought together three neighbouring PCTs,
but in some cases a wider basis will be needed to commission
certain services, such as trauma or paediatric surgery, across a
larger area. PCTs are beginning to put in place networks to achieve
these wider partnerships. Eight London PCTs across the north-west
of the capital, for example, have joined forces to create a project
team to lead the development of a sector-wide strategy. They
have established a joint committee with decision-making powers
to oversee consultation and the implementation of changes to
services on offer that affect them all.266
Finally, collaboration across an entire region is also important,
especially if SHAs are to be phased out. Currently, SHAs are
responsible for developing plans for improving health services in
their own area and making sure that local health services are of
a high quality and are performing well. SHAs provide a strategic
overview of the local population and have a regional level input
into how those services are configured. This role must be taken
on by PCTs working together across the region to set up strong
organisations to provide regional support, data, commissioning
and overview.
264 Ibid., 5.
265 Ibid.
266 Ibid.
FROM FEAST TO FAMINE
187
Some progress has been made forming region-wide PCT
networks. The 31 PCTs in London are in the process of developing
an expert support and shared services organisation (Hub) that will
help them to improve the quality of healthcare provision across
the region. And it is not just London PCTs that are starting to forge
strong working partnerships. In Manchester the Association of
Greater Manchester primary care trusts (AGMPCT) brings together
all its ten PCTs to work in partnership on issues of common
concern, while the Birmingham Primary Care Shared Services
Agency (BPCSSA) was established in April 2002 to provide core
non-clinical services to PCTs across Birmingham. The organisation
aims to encourage and promote:
• efficiency: by enabling increased economies of scale and
through avoiding duplication of services;
• expertise: reducing city-wide competition for scarce
resources and by building areas of expertise that the PCTs
can draw upon;
• partnership: by encouraging and enabling the Birmingham
PCTs to work together and share knowledge;
• focus: through the SSA concentrating solely on improving
non-clinical support services while the PCTs concentrate
solely on improving patient care.267
PCTs are tentatively starting to work together in partnership,
but much more needs to be done to develop local, regional and
national networks to stimulate joint commissioning, the pooling
of resources, the sharing of expertise, intelligence and information,
and the spread of best practice. At the moment, the world class
commissioning framework does not provide enough incentive
to persuade PCTs to work together. This must be changed if joint
working is to become a reality.
267 Birmingham Primary Care Shared Services Agency, “BPCSSA: Introduction”, http://www.bpcssa.nhs.uk/
AboutUs/index.htm.
SOCIAL MARKET FOUNDATION
188
recommendation 24: competency two of the world
class commissioning assurance Framework should be re-
worded to require pcts to work collaboratively with local
and regional pcts and prevent needless duplication.
Fesc
As the commissioning framework was being developed, the
Department of Health concluded that, on their own, many
PCTs did not have the capability at all levels to carry out the
entire commissioning role. Therefore, in 2005 the it published
Commissioning a Patient-led NHS, in which it was made clear that
PCT functions could be “provided by external agencies, partners
and consortia working on their behalf”. It was determined that the
private sector has commissioning skills that are lacking in the NHS
and that need to be tapped into.
As part of the process of encouraging PCTs to seek private
sector support rather than attempting to grow their own expertise,
the government launched the Framework for procuring External
Support for Commissioners (FESC) in October 2007. The framework
was designed to provide PCTs with easy access to a set of expert
suppliers to support them in undertaking their commissioning
functions. FESC provides a list of 14 “prequalified independent
sector organisations” that have been approved by the Department
of Health, from which PCTs can purchase a range of skills and
expertise in areas such as data analysis, contract management and
public engagement.268 The aim was that the framework would
assure the quality of private sector companies working with PCTs,
and would save time in undertaking procurement activities by
268 The 14 organisations are: Aetna Health Services; AXA PPP Healthcare Administration Services; BUPA
Membership Commissioning; CHKS, trading as Partners In Commissioning; Dr Foster Intelligence; Health
Dialog Services; Humana Europe; KPMG; McKesson Information Solutions; McKinsey & Company; Navigant
Consulting; Tribal Consulting; UnitedHealth Europe; WG Consulting Healthcare.
FROM FEAST TO FAMINE
189
providing PCTs with easy access to optimum value-for money
solutions, while reducing the legal and cost implications that can
be encountered when seeking to procure external support.
Launching FESC, the then Minister for Health, Ivan Lewis, stressed
that it would “allow PCTs to benefit from a bank of knowledge
already built up through the DH procurement process”. FESC would
mean that PCTs would be able to work with organisations that are
“already known and trusted” to free up PCTs to “concentrate their
efforts and expertise on providing patient care”.269 The Department
also made it clear that FESC is just one of the tools available to help
commissioners fill any gaps in expertise and that PCTs were not
obliged to use the framework.
The immediate response to FESC from PCT managers
was lukewarm. HSJ surveyed 93 chief executives, as well as
commissioning directors, finance directors and others from a total
of 74 PCTs about their views on FESC in November 2007. The survey
found that 80% of those questioned thought there were ways other
than FESC to help the commissioning process at PCT level, such as
developing internal capability through training and education and
more national information and support on best practice. Nearly
half thought that the framework would prove to be only “a little”
successful within their organisations.270
This pessimism has been vindicated: currently, only four PCTs have
used FESC to secure contracts with private sector organisations. The
main reason for the low uptake is the FESC has turned out to be a very
slow and bureaucratic process. It was intended to provide PCTs with a
fast-track route to procuring accredited providers; it was billed as a way
of receiving a quick injection of private sector expertise, but this has
not been the case. The average time for completing the framework has
269 BBC News, “Private Firms to Aid NHS Trusts”, http://news.bbc.co.uk/1/hi/health/7029809.stm.
270 H. Mooney, “HSJ Commissioning Supplement: an in-Depth Look at FESC”, HSJ (2007).
SOCIAL MARKET FOUNDATION
190
been a tedious 26 weeks, with the Department of Health being accused
of slowing the process down by requiring constant changes to FESC
bids. The DH has declared that it plans to shorten the FESC with the
possibility of devolving responsibility of overseeing the process to SHAs.
It is certainly true that the private sector has a lot to offer PCTs
in their difficult task of commissioning health services in a strategic
way for their local community. However, PCTs should be trusted to
purchase such support from whichever private sector organisations
they think offer them the services that they need. Why limit PCTs to
just 14 organisations, thus stifling choice and competition? Why put
in place a framework that takes 26 weeks to negotiate, thus slowing
down progress while driving up costs? Additionally, PCTs work with
many different private companies that are not part of the FESC
framework – for everything from office cleaning to health visiting. Why
should there be a centrally imposed set of companies pre-approved
to carry out a defined set of tasks? This is an unwarranted interference
in the development of a genuine market in commissioning support.
Part of the reason for the failure of FESC is that some PCTs are still
unwilling to engage with the private sector. There is some ingrained
conservatism in the NHS, and using the private sector remains an
anathema to some. However, FESC will not change this (if anything,
managers will simply resent being cajoled into using the DH’s
chosen private sector organisations) and PCTs should ultimately be
judged on their outcomes and held to account for their choices.
recommendation 25: Fesc should be abolished
puBlic enGaGeMent
Involving the public in the design and commissioning of
health services is an important element in ensuring effective
FROM FEAST TO FAMINE
191
local accountability. Accountability does not only mean formal
mechanisms such as democratic election, regulatory scrutiny
and audit, but must also ensure that the public and patients are
engaged with the authorities that run or commission services.
The system for patient and public involvement in the NHS, after
many years of stability, has undergone substantial change over
the past decade. Community Health Councils (CHCs), established
in 1974, were abolished by the Health and Social Care Act 2001
and were replaced by three bodies: the Patient Advice and Liaison
Service, designed to provide help and advice from within trusts; the
Independent Complaints Advisory Service, set up to pursue formal
complaints; and the Commission for Patient and Public Involvement
in Health, an arms-length body introduced to coordinate patient and
public involvement forums (PPIFs), to represent patients and citizens.
In 2004, PPIFs were abolished (less than six months after many had
begun to operate) to be replaced by patient local involvement networks
(LINks). These networks are no longer attached to individual NHS trusts,
as the forums were, but instead operate over a larger geographical area
which tends to be coterminous with a local authority or PCT boundary.
The rationale behind LINks is that they will provide trusts with a
means to access the views of a much more representative sample of
the local population than the PPIFs did.271 In theory, LINks will offer a
range of different ways for local people to have a say, both through
links with local voluntary sector organisations, and by using a range of
techniques for engaging the public, such as focus groups and surveys.
Evaluation of LINks pilots by the NHS National Centre for
Involvement found that it was too early to report significant
change in public involvement or in the response of the NHS
271 R. Thorlby, R. Lewis and J. Dixon, Should Primary Care Trusts Be Made More Locally Accountable? (London:
The King’s Fund, 2008), 33.
SOCIAL MARKET FOUNDATION
192
organisations.272 Time will tell whether LINks become an important
mechanism in helping NHS organisations to access a wide variety
of patient and public views, and whether they manage successfully
to communicate bottom-up views on health from patients and
the local public. However, to aid the process, the relationship
between LINks and overview and scrutiny committees should be
strengthened to ensure that the public is involved in the scrutiny
process. Currently, a LINk has the power to refer an issue to its local
OSC but the OSC has no duty to respond. This should be changed
to ensure that users have more influence over services.
recommendation 26: oscs should be required to
produce a public response to any referral made by a
link.
Benefits of patient and public involvement
The success of LINks is still uncertain, but what is clear is that patients
are keen to be engaged.273 They value being involved in decisions,
having their preferences respected and being presented with clear,
comprehensible information.274 Involvement increases patients’
satisfaction and confidence, and reduces their anxiety. It can also
lead to improved trust and better relationships between patients
and healthcare professionals.275 Involving patients in shared decision-
making about their care and treatment and in how to manage their
own condition can improve the appropriateness of care, improve
health outcomes, reduce risk factors and prevent ill-health.276
272 NHS National Centre for Involvement, “Learning From the Early Adopter Programme: Interim Report”,
http://www.nhscentreforinvolvement.nhs.uk/docs/EAPS%20interim%20report%20Final.pdf.
273 D. Furness and B. Gough, Local Control and Local Variation in the NHS: What Do the Public Think? (London:
Social Market Foundation, 2009).
274 Picker Institute, “Why Patients Should Share in Decision-Making”, http://www.pickereurope.org/Filestore/
Policy/position_papers/Picker_Policy_3_Why_patients_should_be_involved.pdf.
275 C. Farrell, Patient and Public Involvement: The Evidence for Policy Implementation (London: HMSO, 2004).
276 Picker Institute, “Why Patients Should Share in Decision-Making”.
FROM FEAST TO FAMINE
193
Evidence also shows that patient involvement can lead to more
cost-effective outcomes, moderate demand, improve safety and
reduce complaints and litigation.277 This was emphasised in the
Wanless review of the future of the NHS, which stated that the
health service would be most sustainable where patients and the
public were “fully engaged”.278
If patients feel engaged with the health service, they are also more
likely to trust healthcare professionals and support the NHS. This will
be particularly important in the coming years as the NHS experiences
a tightening of its budget. Difficult decisions are going to have to
be made about which services to fund and how services should be
delivered. People will accept those decisions more readily if they feel
that they have been involved in the decision-making process. Finally,
most health professionals tend to view patient involvement positively,
seeing it as a rewarding process for both parties.279
legal obligation
As well as being valuable, patient and public involvement is also
a legal obligation. Since 2003 healthcare professionals have had
a statuary duty to consult the public regarding any major service
change, and, more recently, legislation has required PCTs to work
with local government in assessing population service needs.
The world class commissioning programme also stresses the
importance of involving the public. The vision for world class
commissioning sees PCTs as “visible leaders of their local NHS. … They
act as an advocate for the people within their community, and their
objectives and priorities resonate with the local population. … There
is local ownership and accountability for these decisions, which are
made with a strong mandate from their local population and other
277 Ibid.
278 D. Wanless, Securing Good Health for the Whole Population: Final Report (London: HMSO, 2004).
279 Farrell, Patient and Public Involvement.
SOCIAL MARKET FOUNDATION
194
partners.”280 In reality, no PCT is close to achieving this vision. SMF
Health Project interviews with PCT staff revealed that PCTs are aware
of the importance of public engagement but are struggling either to
implement systematic programmes of engagement or to carry out
sophisticated market research in order to understand the views of their
local population. The Picker Institute supports these findings, stressing
that most PCTs are using a limited range of techniques, and that they
are more focused on consulting about service redesign decisions
that they have already decided are desirable. The Institute found that
“few PCTs are using more intensive, deliberative techniques; involving
the public in early priority setting; or involving people in monitoring
and reviewing the performance of service providers”.281 Most senior
managers are still not taking public engagement seriously enough
and are failing adequately to resource it.282
The NHS’s continuing failure to give patients enough say on
local health services was further underlined in a recent report by the
Healthcare Commission. The study of 130 healthcare organisations and
170 user groups in England revealed that patients do not feel they have
enough input into what services are provided or how they are delivered.
The Commisson’s report states: “Few trusts could demonstrate that
people’s views routinely influence their decision-making.”283 The report
found that some PCTs are undertaking “excellent practice” in certain
areas, particularly in consulting the public on large reorganisations of
services. However, it revealed that PCTs are still not routinely considering
patients’ opinions about GP practices or requiring hospitals or surgeries
to take account of the public as part of their contracts.284 As such, it
should come as no surprise that in the first round of the world class
280 Department of Health, “World Class Commissioning”.
281 Picker Institute, Accountability – Public Views and What to Do About Them (Oxford: Picker Institute Europe,
2008), 6.
282 Ibid.
283 The National Centre for Involvement, “Watchdog Calls On Healthcare Services To Do More To Act
On The Views Of Patients And The Public”, http://www.nhscentreforinvolvement.nhs.uk/index.
cfm?action=PRE&PressID=300.
284 Ibid.
FROM FEAST TO FAMINE
195
commissioning assurance tests not a single PCT scored level three or
four on competency three (engaging with public and patients) and 51
PCTs did not manage to score higher than level one.
In an opinion poll for the Local Government Association Health
Commission carried out in 2008, more than half the respondents
did not know what a PCT was or what they did. Almost three-
quarters of those questioned could not name their local PCT, and
fewer than 10% had been involved in any patient group or forum
concerned with local NHS services.285 PCTs cannot be held to
account by the public if the public does not know they exist. These
results highlight the inadequacy of most PCTs’ public engagement
strategies and the gulf that exists between the rhetoric of the
world class commissioning vision and reality.
Having said this, it is also important to remain realistic when
considering the scope of public engagement in healthcare
commissioning. While a large majority of people think that the
public should be consulted on decisions that shape the NHS, most
people do not want to become full-time health service planners.
Ipsos MORI carried out a set of polling and discussion groups for the
SMF Health Project. The polling showed that 74% of respondents
thought that the public should either be consulted on decisions
shaping the NHS, or should be much more actively involved, while
only 20% thought that such decisions should be made solely by
qualified health professionals and not the general public. However,
when this theme was explored more deeply in the discussion
groups, it turned out that although most of the participants
thought the general public should be involved in decision-making,
the individual participants did not themselves want to be involved
in decision-making. As one participant put it when asked if they
would personally get involved: “Oh God no, it’s too much work.”286
285 LGA Health Commission, Who’s Accountable for Health? LGA Health Commission Final Report (London: Local
Government Association, 2008), 28.
286 Ipsos MORI, discussion group, for the SMF Health Project, 2009.
SOCIAL MARKET FOUNDATION
196
A number of research studies have found that this pattern is
reflected across the public sector: around 75% of respondents say the
public should be more involved in the planning or delivery of local
services; however, only about 25% say that they personally would get
involved, and in reality only about 1 or 2% actually do get involved.287
A study by the Audit Commission on public trust in local
services concluded that there was “no great unmet desire on the
part of the public to involve themselves in the planning or delivery
of key public services. Only around one in five would like to get
involved in helping their council or NHS hospital to plan and deliver
services (17 per cent and 22 per cent respectively).”288
However, although the public might not want to be involved
in every decision about their local health service, they do want to
feel that they are being listened to and consulted about how the
services they use are run. The Local Government Association (LGA)
Health Commission argues that people want to be able to have
their say and make an input when strategic plans are being made.
They found, for example, that patients have strong views about
how, where and when GP services are provided.289
This finding was echoed in the SMF Health Project patient
discussion groups: all four groups thought that the public should
be involved in decisions about how their local GP practice decided
on funding priorities. They came to the general conclusion that the
public need to be consulted or involved when:
• a decision affects a lot of people a lot of the time;
• there is a feeling that the NHS is currently getting the
decision wrong;
287 Author interview with Jonathan Nicholls, Ipsos-MORI.
288 Audit Commission, Corporate Governance: Improvement and Trust in Local Public Services (London: Audit
Commission, 2003), 37
289 LGA Health Commission, Who’s Accountable for Health?, 4
FROM FEAST TO FAMINE
197
• the public has genuine knowledge about what services
are needed, for example the range of services that should
be provided at their GP practice;
• the solution needs public buy-in, for example combating
child obesity.
Conversely, the discussion groups concluded that they would
be happy not to be involved in decision-making if:
• they felt the NHS was currently getting the decision right;
• the decisions should be objective and clinical.
The participants were also concerned that public involvement
could lead to subjective, rather than objective, decision-making,
and could fall victim to interest groups. Hence, unless well managed,
the participants were concerned that public involvement could
jeopardise fairness.
In addition, the participants stressed that while they do not
want to be involved in every decision about how the health service
is run, they do demand transparency about how decisions are made.
Information, clarity and transparency can counteract cynicism around
decision-making. As one participant put it: “If you don’t feel involved in
something, it’s like somebody’s making every decision on your behalf. It
feels like a military state.”290 All the participants found it easier to accept
tough decisions if they were privy to the rationale behind them.
The Picker Institute also found in their own discussion groups
that the public are keen to be involved in decisions about local
health services if certain conditions are met. They found that
people are willing to see consultation as a route to involvement
and potentially a key part of accountability. However, participants
stressed that consultations must be meaningful:
290 Ipsos MORI, discussion group, for the SMF Health Project, 2009.
SOCIAL MARKET FOUNDATION
198
• the decision should not already have been made;
• the public must be able to influence the decision;
• the results of the consultation and the action taken (or not
taken) must be communicated back to them.291
The Picker Institute argued that people feel that these three
conditions are rarely fulfilled, which leads to a cynicism about the
validity of consultation. The Institute suggested that this cynicism
may be one of the factors that creates a gap between expressions
of willingness to be involved, and actual participation.292
PCTs should be free to develop public engagement strategies
that best suit their local circumstances. Having said that, it is crucial
that they take the practice of public engagement seriously. This
is particularly important as patients cannot “exit” their PCT by
choosing another PCT to commission services on their behalf. PCTs
therefore have a duty to listen and respond to their local population
and to involve them in planning or delivery of local services where
there is an appetite for such involvement.
The Department of Health’s latest guidance for PCTs on
local decision-making about medicines states that they should
take “reasonable steps to provide an explanation to the public
on the need for PCT prioritisation”.293 This guidance should be
substantially strengthened. Although PCTs should be free to
develop their own engagement programmes, they must also
be held to account for implementing those programmes and be
able to show the impact that the programme has on the way
the PCT operates. It is not acceptable for PCTs simply to take
“reasonable” steps to provide an explanation of their actions
to the public – such information must be seen as an essential
291 Picker Institute, Accountability – Public Views and What to Do About Them, 5.
292 Ibid.
293 Department of Health, Defining Guiding Principles for Processes Supporting Local Decision Making About
Medicines, National Prescribing Centre (London: HMSO, 2009).
FROM FEAST TO FAMINE
199
minimum, and any PCT failing to provide such information
should be held accountable for such a failure.
recommendation 27:
to improve public engagement pcts must:
• Develop a statement of the aims and purposes of
patient and public involvement in their local area
and set out a two-year programme to demonstrate
how these aims will be achieved.
• commission research to identify effective strategies
for engaging patients and local people.
• ensure senior managers take public engagement
seriously, providing it with adequate staffing and
resources.
• Dramatically improve their public profile, ensuring
that members of the public know that they exist and
understand what they do.
• change their names to indicate that they are the
nhs body for that area. For example, nhs hull rather
than hull pct.
• launch local information campaigns to clarify how
the health system works at the local level and how
individuals and groups can become involved. the
campaigns should inform the local population about
how different parts of the health service interact
and about the different accountability mechanisms.
• work hard to recognise when, where and how
members of the public want to be involved and ensure
that as wide a range of them are involved as possible.
• ensure that even when the public is happy to leave
decision-making up to the pct, the public is still kept
informed about how and why decisions are made and
have a means to give feedback, which is responded to.
SOCIAL MARKET FOUNDATION
200
But this will not happen spontaneously: a national framework is
needed to kick start the process and ensure that PCTs take patient
and public involvement and engagement seriously.
recommendation 28: the Department of health
should develop a national framework to measure and
evaluate the effectiveness of pcts’ public engagement
programmes. the results of the evaluation would
feed into the world class commissioning assurance
framework.
practice-BaseD coMMissioninG
Practice-based commissioning (PBC) seeks to grant GPs more
decision-making power over how NHS resources are spent and
enable them to deliver new services, or commission others to do
so. The thinking behind this policy is that putting commissioning
power in the hands of frontline clinicians will lead to “high quality
services for patients in local and convenient settings” because “GPs,
nurses and other primary care professionals are in the prime position
to translate patient needs into redesigned services that best deliver
what local people want”.294
The Department of Health has set out that the aims of practice-
based commissioning are to:
• encourage clinical engagement in service redesign and
development;
• bring about better, more convenient, services for patients;
• enable better use of resources.295
294 Department of Health, “About Practice Based Commissioning”.
295 Ibid.
FROM FEAST TO FAMINE
201
Under PBC, GP practices are given virtual budgets (known as
indicative budgets) with which to purchase health services for their
patients.296 The indicative status of the budget means that the local
PCT remains legally responsible for the money and is accountable
for any overspends. The GP practice is able to submit business
cases to the PCT, proposing changes to commissioning or the
establishment of new services.
history
Giving GPs more power over resources and allowing them
to commission services is not a new idea. In the 1990s, the
Conservatives introduced similar policies in the form of GP
fundholding. Fundholding was abolished by the Labour
government in 1997, because of initial trepidation about using
competition to drive change in the NHS. There was also concern
that fundholding created extra bureaucracy and benefited some
areas more than others, thus exacerbating inequality in access to
care for patients.297
Nevertheless, despite the hostility towards fundholding,
the 1997 White Paper, The New NHS: Modern, Dependable, did
acknowledge that the experience of GP fundholding had delivered
some benefits to patients, for instance by broadening the range of
services available in GP surgeries. In fact the White Paper went as far
as to predict that over time “indicative budgets [will be devolved]
to individual practices” for a full range of services. Six years later, by
which time any doubts about choice and competition as drivers
of change had been swept aside, the policy re-emerged when the
government announcement in December 2004 that all practices
would be involved in practice-based commissioning by 2008.298
296 Practice-based commissioning budgets are separate from the funds that GP practices receive under their
existing contracts for their core work (General Medical Services and Personal Medical Services).
297 Department of Health, The New NHS: Modern, Dependable (London: HMSO, 1997).
298 Department of Health, Practice Based Commissioning: Promoting Clinical Engagement (London: HMSO,
2004).
SOCIAL MARKET FOUNDATION
202
impact of practice-based commissioning
The Department of Health has published examples of the sorts of
change that can be made to services under PBC.299 These include
examples of reducing avoidable emergency admissions through better
management of people with chronic conditions, referral management
centres run by PBC groups in order to control the number of elective
referrals, and GPs performing minor surgery in their offices.
This suggests that PBC does have the potential to lead to
effective service redesign. However, for this to occur, GPs have to
engage in the process. A number of financial incentives have been
made available to encourage GPs to sign up to the scheme. From
2005 to the end of the financial year 2007/08, a centrally funded
incentive scheme was available which paid GPs directly for their
involvement in PBC. A similarly structured local financial incentive
is now offered by some PCTs to encourage GPs to fulfil or invest in
a particular commissioning activity.300 GPs are also entitled to retain
up to 70% of the indicative budget that has been saved at the end
of the financial year to invest back into the GP practice.301
However, despite these incentives, take-up has been poor. In
2007 the Department of Health published a survey of 1,200 GP
practices across England, which revealed that although nearly two-
thirds of practices said they were “supportive” of PBC as a policy,
60% said they had not commissioned any new services as a result
of the policy.302 The survey also found that 37% of respondents
believed that it was “too early to tell” whether PBC had improved
patient care, 31% “disagreed” that PBC had made improvements
and only 13% felt that it had.
299 Department of Health, Practice Based Commissioning (PBC): Implementation Progress Report (London:
HMSO, 2007).
300 N. Curry and R. Thorlby, Practice-Based Commissioning: King’s Fund Briefing November 2007 (London: The
King’s Fund, 2007).
301 Department of Health, Practice Based Commissioning: Achieving Universal Coverage. (London: HMSO,
2006).
302 Department of Health, Practice Based Commissioning: GP Practice Survey (London: HMSO, 2007).
FROM FEAST TO FAMINE
203
A 2007 Audit Commission report examined the results of PBC.
It highlighted some positive examples of service redesign and
stressed that general practices had a better understanding of the
financial consequences of their decisions and engaged more in
managing their patients’ use of secondary care. However, these
achievements had been secured at a cost of at least £98 million
in 2006/07. The report concluded that GPs tended to be more
interested in directly providing services on a small scale and in a
few clinical areas than getting involved in commissioning.303
A more recent report by the King’s Fund found that GPs have
still failed to engage fully with PBC. The report reveals that the
majority of GPs, while supportive of the principles of the PBC,
prefer to observe passively and let others lead.304 The Department
of Health has been forced to accept that, so far, the policy is not
working satisfactorily. The NHS Next Stage Review acknowledged
that “there is a widespread view that, with some exceptions, [PBC]
has not yet lived up to its potential”.305
why has practice-based commissioning stalled?
Evidence shows that a minority of entrepreneurial and innovative
GP practices across England have used the policy of PBC to improve
services considerably.306 This suggests that the policy has the potential
to be successful, but so far it is failing. There appear to be a number
of reasons why this is so. The first is simply that there may be a limited
number of entrepreneurial and managerially talented GPs who want
to get involved in commissioning services. This assumption is backed
up by the Audit Commission report and also by the past experience of
303 Audit Commission, Putting Commissioning Into Practice: Implementing Practice Based Commissioning
Through Good Financial Management (London: Audit Commission, 2007).
304 N. Curry et al., Practice-Based Commissioning: Reinvigorate, Replace or Abandon? (London: The King’s
Fund, 2008), viii.
305 Department of Health, NHS Next Stage Review: Our Vision for Primary and Community Care (London: HMSO,
2008), 51.
306 Curry et al., Practice-Based Commissioning: Reinvigorate, Replace or Abandon?, 13.
SOCIAL MARKET FOUNDATION
204
GP fundholding.307 The government has attempted to overcome this
by using incentive payments to encourage GPs to support PBC. But so
far it seems that the incentives have not been strong enough to deliver
more than token involvement. This may in part be due to the fact
that the incentives to undertake PBC are undermined by the stronger
incentives contained within the GPs’ General Medical Services contract.
The King’s Fund highlights a number of other reasons why PBC
has failed to take off. These include disagreements between GPs
and PCTs over their roles and responsibilities in commissioning;
a lack of commissioning skills amongst GPs; a lack of reliable,
timely data; and concern amongst PCT senior managers that the
levers are not available to allow them adequately to hold GPs to
account. In addition, poor-quality relations between GPs and the
government have discouraged GPs from fully engaging with PBC,
while a perceived deterioration in the level of priority given to PBC
by the Department of Health has resulted in some GPs and PCT
staff spending less time and energy on the policy.308
One way of strengthening the financial incentives for GPs
to fully engage in PBC and the budgetary accountability would
be for practice-based commissioners to receive real devolved
budgets rather than the current indicative budget. However, this
would throw up some problems, not least the question of conflict
of interest. PBC creates an implicit incentive for GPs to invest in
and commission local services that they themselves provide. This
creates a direct conflict of interest, which would become even more
acute if PBCs held real budgets. New governance arrangements
would need to be established to ensure that patient choice and
the quality of GP referrals were not compromised.
307 Audit Commission, Putting Commissioning Into Practice ; N. Goodwin, “GP Fundholding”, in J. Le Grand, N.
Mays and J. A. Mulligan (eds), Learning From the NHS Internal Market: A Review of the Evidence (London:
The King’s Fund, 1998).
308 Curry et al., Practice-Based Commissioning: Reinvigorate, Replace or Abandon?, x.
FROM FEAST TO FAMINE
205
Evidence also shows that that practice based commissioners
have tended to commission services based in primary and
community care settings and, according to the King’s Fund, have
failed to address fully “the more strategic commissioning activities
related to whole patient pathways”.309 As a result, the scope of
what could be purchased by budget-holding practice-based
commissioners would need to be defined at the PCT level, which
to some degree negates the point of PBC, as it takes the purchasing
decisions away from the GP and places it back with the PCT.
the future of pBc
PBC is currently not operating effectively: progress has been slow and in
some areas the policy is grinding to a halt.310 Tens of millions of pounds
have been spent trying to encourage GPs to commission services, but
on the whole there is not a great appetite amongst the profession for
PBC. More money could be invested in an attempt to re-energise the
policy, but one has to ask whether it would be money well spent trying
to incentivise GPs to get involved in an activity that many are either not
interested in doing or do not have the skills to do well.
Even if GPs’ disregard for the policy could be overcome,
fundamental issues around conflicts of interest and governance
suggest that significant redesign of the policy would be needed. It
also seems perverse that while the government is encouraging PCTs
to give up their provider functions to establish a clear separation
between commissioners and providers, the policy of PBC seeks to
establish that GPs are providers and commissioners of services.
There is no doubt that clinicians need to be closely involved
in the commissioning process: clinicians have a crucial part to play
in helping commissioners draw up strategic plans and design and
commission services that build on the current clinical evidence
309 Ibid., 53.
310 Ibid., x
SOCIAL MARKET FOUNDATION
206
base, maximise local care pathways, and use resources effectively.
But PBC is not the only way to achieve this. Instead of focusing
on PBC, more effort could be made to ensure that GPs and other
clinicians play a central role in providing clinical input into PCT
commissioning decisions. Structures must be put in place to widen
clinician involvement in PCT commissioning so that not only GPs
but also hospital clinicians and other healthcare professionals are
included.311 Collaboration between commissioners and providers
must also be encouraged during contractual negotiations.312
There is concern that the traditional GP practice can be inward-
looking, replicating what has been delivered in the past and failing
to adapt as lifestyles and patterns of ill-health evolve. Practice-
based commissioning is seen as a way of changing this, delivering
interrelated, high-quality and responsive care, and releasing
resources from traditional hospital services. However, apart from in
a minority of cases, PBC has not led to a change in service delivery.
As discussed, PBC incentivises practices to commission services
from their own practice and has led PBC consortiums to commission
traditional services based in primary and community care settings
rather than to think more strategically and commission activities
related to whole patient pathways.
The best way to stimulate an outward-looking, joined-up, integrated
service would be for PCTs to have the freedom to commission services
from a range of providers, either working together or competing with
each other. As opposed to PBC, which actually hampers choice and
competition, commissioners should have the freedom to purchase
care from the providers offering the best package. A thriving provider
market would stimulate GPs and other health professionals across the
sector to join together into integrated care organisations, to offer PCTs
the chance to commission joined-up services. It is competition that
311 A. Liddel and N. Timmins, Making It Happen: Next Steps in NHS Reform (London: The King’s Fund, 2008).
312 J. Smith and N. Goodwin, Towards Managed Primary Care: The Role and Experience of Primary Care
Organisations (Aldershot: Ashgate, 2006).
FROM FEAST TO FAMINE
207
will encourage providers to improve patient journeys and pathways,
making them faster, safer, of higher quality and more resilient.
should pBc be abandoned?
To date, NHS managers have tended to be unwilling to comment on
PBC, but it seems that some managers’ patience with the policy is
starting to crack. Alison Tonge, director of health system development
at NHS North West, has suggested that practice-based commissioning
could be split in two, with PCT commissioners given a duty to engage
clinicians as part of a care pathway and system design team. Hull PCT
chief executive, Chris Long, has suggested that GPs, local authorities
and the public should be brought together under a “locality director”
who would report to the PCT chief executive.313 Could these public
statements of discontent mark the beginning of the end for PBC?
Abandoning PBC would be a blow to those GPs who have
invested a lot of time, energy and resources into developing
organisational structures for the system to work. So rather than the
Department of Health simply scrapping the policy, where PBC is
succeeding it should be allowed to continue, but the government
should stop spending on incentivising its adoption in practices that
have shown little interest thus far.
recommendation 29: the focus of policy should be on
strengthening pct commissioners, ensuring clinicians
are closely involved in pct commissioning decisions, and
stimulating a thriving provider market. this will allow current
pBc consortia to evolve into integrated care organisations
focused on providing joined-up services, rather than
attempting to both commission and provide services.
313 Helen Crump, “Managers Call for GP Commissioning Reforms”, HSJ (2009).
SOCIAL MARKET FOUNDATION
208
conclusion
This chapter has demonstrated that commissioning is the key
driver of quality in the health system. It is, in fact, the best hope
of maintaining high-quality universal healthcare in a financial
crisis. There are massive potential efficiencies to be gleaned from
commissioning, but equally it is very difficult to extrapolate this out
to model the potential cost savings should commissioning function
at a high level. Nevertheless, the recommendations set out above
are testament to the potential that exists, and the many different
approaches to improvement that can be adopted by policymakers.
The overarching theme of this chapter has been that
commissioners need to be strengthened by the removal of central
control, and by taking on new responsibilities that will offer them
the opportunity to influence providers and generate a real market
for care. Only this offers the chance of savings that will maintain
public health services in a universal form.
FROM FEAST TO FAMINE
209
chapter seven: accountaBility in a local systeM
Chapter 6, above, set out the case for a health system at the
heart of which sit local commissioners, driving improvements by
means of strong relationships with providers, and shaping health
services to suit the needs of local people through engagement
with the public. Although central government should remain as
the revenue-raiser and resource-distributor, the bodies tasked
with driving change and improving the efficiency and quality of
healthcare will be local PCTs.
The accountability structures in the health system will have to
change to reflect this shift in responsibility and power. Currently,
accountability mechanisms face upwards. PCTs and providers are
ultimately accountable to the Secretary of State for Health, Parliament
and national regulators. However, with the ever-increasing complexity
of the health service, and with local PCTs holding more power and
responsibility, it will be crucial for accountability to flow down to local
people as well as up to central government.
This chapter considers how the accountability structures in
the health service have evolved since the inception of the NHS
in 1948 and highlights the changing nature of accountability in
the NHS over the past 60 years. It focuses on what accountability
means in the health system and on the different types of
accountability in the NHS, underlining the multiple forms that
accountability mechanisms can take. The chapter concludes by
considering how powerful local commissioners should be held
to account at a local level.
evolution oF accountaBility MechanisMs
The accountability structures and institutions of today’s NHS have
their roots, to some extent at least, in the negotiations that preceded
the formation of the NHS in 1948. The Labour MP and Cabinet Minster
SOCIAL MARKET FOUNDATION
210
Herbert Morrison supported local government control, but he was
overruled by Nye Bevan’s preference for a single national hospital service.
Bevan argued for national rather than local accountability, but
not for national control over service delivery. Partly in order to
secure the participation of doctors in the NHS, Bevan promised to
provide them with “all the facilities, resources, apparatus and help
I can, and then leave you alone as professional men and women to
use your skills and judgement without hindrance”.314
As a result, right up until the 1980s, accountability in the NHS
consisted largely of a system of professional self-regulation. It was not
until 1982 that annual accountability mechanisms were introduced.
But even with this development, the Griffiths Report criticised the
accountability structures of the NHS in 1983, arguing that it was
impossible to tell who was in charge of any given NHS hospital. The
recommendations set out in the Griffiths Report were implemented
from 1985 with the aim of improving the general management
of the health system. Nevertheless, the confusion over who was
accountable for what continued, resulting in a Department of Health
White Paper, published in 1989, which declared that for the first time
“a clear and effective chain of management command running from
districts … to the Secretary of State” was to be introduced.315
In the past 20 years there have been further attempts to
reshape the accountability structures of the NHS, first through
internal markets, then through a reinforced hierarchy centred on
national targets, and finally through the reintroduction of market
mechanisms based on a mixed economy of supply.316
314 Quoted in C. Webster, The National Health Service: A Political History (Oxford: Oxford University Press,
2008).
315 Department of Health, Working for Patients (London: HMSO, 1989).
316 LGA Health Commission, Accountability for Health: A Scoping Paper for the LGA Health Commission (London:
Local Government Association, 2008).
FROM FEAST TO FAMINE
211
Over the past decade, accountability has been focused upwards
with the emphasis placed on meeting centrally set targets.317 However,
over the last few years a growing reaction against this central control
has been building, with calls to end political interference and create an
independent NHS and to strengthen local accountability mechanisms.318
what is accountaBility in the health systeM?
Put simply, accountability in the public sector aims to ensure that
those who deliver public services are answerable to those who
either finance them or use them.319 The OECD defines accountability
as “the obligation of those entrusted with particular responsibilities
to present an account of, and answer for, their execution”.320
Ashworth and Skelcher identify four components of
accountability:
• taking into account – through consultation with citizens
and stakeholders;
• giving an account – explaining actions that have been taken;
• holding to account – citizens hold the government to
account at the ballot box, for example;
• redress – the right for compensation of some kind, or to
remedy or set right the situation, when services have not
been delivered to an appropriate standard.321
317 R. Thorlby, R. Lewis and J. Dixon, Should Primary Care Trusts Be Made More Locally Accountable? (London:
The King’s Fund, 2008).
318 See, for example, The Conservative Party, NHS Autonomy and Accountability: Proposals for Legislation (London:
The Conservative Party, 2007); B. Edwards, An Independent NHS: A Review of the Options (London: Nuffield
Trust, 2007); A. Dixon and A. Alvarez-Rosete, Governing the NHS: Alternative to an Independent Board (London:
The King’s Fund, 2007); BMA, An NHS Constitution for England (London: British Medical Association, 2008).
319 P. Day and R. Klein, Accountabilities (London: Tavistock, 1987).
320 OECD, Modernising Government: The Way Forward (Paris: Organisation for Economic Cooperation and
Development, 2005).
321 R. Ashworth and C. Skelcher (The Office of the Deputy Prime Minister), Meta-Evaluation of the Local
Government Modernisation Agenda: Progress Report on Accountability in Local Government (London: HMSO,
2005).
SOCIAL MARKET FOUNDATION
212
So in some respects accountability is about ensuring that
institutions are transparent and made to justify their actions. But
accountability also goes further than this: it must include the power
to dismiss decision-makers or challenge decisions. There is no point
in simply being accountable either upwards to government or
downwards to people unless a change is implied – accountability
mechanisms must have the power to change behaviour.
types oF accountaBility in the nhs
The Local Government Association (LGA) Health Commission
distinguishes five types of accountability in the NHS:
1. Professional accountability – based on a professional body
setting the standards of practice that service users can
expect, with professionals answerable to their peers for
their performance against these standards.
2. Audit – performance assessment carried out to ascertain
the validity and reliability of information and to provide an
assessment of a system’s internal control for the purpose
of accountability.
3. Democratic control – in the UK, this has conventionally
meant elected representatives holding professional officers
to account and having the power to enforce decisions.
4. Stakeholding – the building of partnership to ensure
accountability, with one institution providing a check on
its partner organisation or branch of government.
5. Market mechanisms – politically managed markets,
designed to ensure equity and social justice, are a means
of delivering individual-level accountability.322
Accountability can be achieved in different ways, via different
mechanisms to meet different goals. How much weight is given to
322 LGA Health Commission, Accountability for Health: A Scoping Paper for the LGA Health Commission.
FROM FEAST TO FAMINE
213
any one of these types of accountability will depend on the type of
health service that is being designed and the type of accountability
that is desired. In a decentralised health system there is a key role
for a national audit – making sure that local commissioners are
putting out high-quality information into the public domain. There
may also be a role for democratic control of some kind, particularly
to justify local variation of services.
at what level is accountability currently located?
Accountability can be located at either a central or a local level: it
can be directed upwards to a higher authority (which must itself
be held to account by the public through national democratic
structures) and downwards to local people or service users
(achieved through local government or another form of local
governance arrangement).
central accountability
On the whole, accountability in the NHS is located centrally with
government and national regulators. This is in a large part because
of the funding arrangements of the NHS: centrally raised taxes
have always resulted in national government responsibility for, and
control over, the expenditure of these funds.323
Professional accountability, carried out by the professional
bodies such as the General Medical Council, has been the main way
in which the health service in England has been held to account
for the past 60 years. However, a number of high-profile cases of
substandard care and abusive behaviour by doctors have led to
calls for a more robust system of accountability.324
As a result, the role of audit has become increasingly important.
Since 2000, the performance of NHS institutions has been assessed
323 Thorlby et al., Should Primary Care Trusts Be Made More Locally Accountable?, 13.
324 For example, the behaviour of Harold Shipman, Clifford Ayling, Rodney Ledward and the problems at the
Bristol Royal Infirmary.
SOCIAL MARKET FOUNDATION
214
against publicly available standards and targets, first by the
Commission for Health Improvement (CHI), then by the Healthcare
Commission, and since April 2009 by the Care Quality Commission
(CQC). The CQC is the new independent regulator of health and
social care in England which replaced the Healthcare Commission,
the Commission for Social Care Inspection and the Mental Health
Act Commission. Financial scrutiny is carried out by the Audit
Commission.325
National accountability has also been strengthened by the
introduction of National Service Frameworks, NICE and clinical
governance processes. All these developments aim to reduce variations
in practice across the NHS, making local NHS bodies accountable for
meeting national standards and guidelines. The role of regulation in the
health system is discussed in more detail in chapter 8.
local accountability
The system of audit, carried out by national regulators, has ensured
managerial accountability upwards but it has been less effective
in ensuring accountability downwards to the local population.326
There appears to be a growing consensus, both in some parts of
government (to a certain extent) and within the health community,
that it is time to move on from the process of upward accountability
characterised by top-down national targets towards systems of
local accountability.327
What is meant by local accountability?
Local accountability is a somewhat unclear term; it is possible
to confuse local accountability with public involvement.
325 The regulation of the health service in England is dealt with in more detail in chapter 8.
326 Thorlby et al., Should Primary Care Trusts Be Made More Locally Accountable?.
327 See, for example, A. Darzi, High Quality Care for All: NHS Next Stage Review Final Report (London: HMSO,
2008); The Conservative Party, Delivering Some of the Best Health in Europe: Outcomes Not Targets (London:
The Conservative Party, 2008); The Liberal Democrats, Empowerment, Fairness and Quality in Healthcare:
Policies for an Effective NHS (London: The Liberal Democrats, 2008).
FROM FEAST TO FAMINE
215
Public involvement can strengthen accountability, but simply
introducing some form of public involvement into health services
via a mechanism such as a citizen’s jury does not automatically
ensure accountability. There needs to be a synthesis of public
involvement and accountability exercised at a local level for true
local accountability to be achieved.328
Democratic accountability
One way to achieve this synthesis is through the ballot box. General
elections act as a form of direct, democratic accountability in the
NHS. However, the belief that national elected representatives
hold all public servants to account, including those at a local level,
has become less convincing over time as the NHS has become
more complicated and as more responsibility has been devolved
outwards to national, unelected arm’s-length bodies. Also, general
elections occur infrequently, are rather remote and are not focused
solely on the government’s handling of the health service, but on
their running of the country as a whole.
It is possible to argue that democratic influences are not
entirely absent at a sub-national level as a significant part of an
MP’s constituency business is taken up with health service matters.
However, in reality MPs lack any real means of enforcement.329
Consequently, a number of suggestions have been made about
how the NHS can be made more democratically accountable. The
next section considers how commissioners can be held to account
at a local level, and examines a number of democratic options.
pct accountability
As PCTs gain more control over the shape of the NHS in the future, it
is going to become increasingly important that they are effectively
held to account at a local level. Currently, PCTs are formally held
328 Thorlby et al., Should Primary Care Trusts Be Made More Locally Accountable?.
329 C. Johnson, Scrutinising for Health: Health Scrutiny Evaluative Research Project (London: Centre for Public
Scrutiny, 2007).
SOCIAL MARKET FOUNDATION
216
to account through the world class commissioning assurance
framework (discussed in detail in chapter 6), which is managed by
Strategic Health Authorities, which are themselves accountable to
the Secretary of State for Health. PCT performance is also assessed
by the Care Quality Commission, which monitors the quality
and safety of PCTs’ service delivery as well as their activity levels,
and by the Audit Commission, which measures value for money
and probity (both of these bodies are themselves accountable
to Parliament).
This form of accountability is essentially “upwards” to central
government and Parliament rather than “downwards” to the
public that they serve. There is a growing consensus that more
accountability should be devolved locally and that clinicians, local
NHS staff and the public need to be more involved in decision-
making. Lord Darzi’s review of the health service, Our NHS, Our
Future, emphasises the importance of direct engagement with
patients, the public and their representatives while the 2008/09
NHS Operating Framework has promised “a decisive move towards
greater local autonomy”.330
PCTs now receive 80% of the NHS budget and are starting
to gain more freedom to commission local services. The current
arrangements, however, which rely for the most part on centralised
mechanisms of oversight, do not adequately ensure that local
decision-makers are held to account.331
In the current system, characterised by national standards and
targets, there are significant local variations in the quality and the
nature of services provided by different PCTs that are not fully
330 D. Nicholson (Department of Health and NHS Finance Performance and Operations), The NHS in England:
The Operating Framework for 2008/09 (London: HSMO, 2007).
331 LGA Health Commission, Who’s Accountable for Health? LGA Health Commission Final Report (London: Local
Government Association, 2008), 4
FROM FEAST TO FAMINE
217
explained by differences in the patient population.332 This is hardly
surprising as even in a highly centralised system decisions are
continually being made at a local level.
In the future, as local commissioners are granted greater
discretion, the local variability that already exists will increase
further. For this scenario to be accepted by the public, any
variation in services must be seen to be legitimate, transparent and
accountable at a local level.333 In short, the more local autonomy
PCTs receive, the more important it is that clear and robust
“downward” accountability mechanisms are in place.
Currently, the local accountability mechanisms are not sufficient
to enable PCTs successfully to carry out all the responsibilities that
commissioning entails with the support of their local population.
For example, PCTs are currently failing to decommission services,
partly because they do not hold a clear mandate for major service
changes. Public protests are the norm when changes to local
services are proposed334 and PCTs do not have the democratic
legitimacy to withstand such popular pressure.
It is becoming increasingly clear that an “accountability gap”
exists which needs to be filled. This lack of accountability needs
to be addressed both because of the intrinsic value of public
accountability in maintaining the integrity of the system, and also
for the pragmatic reason that public buy-in and ownership is crucial,
especially in a constrained fiscal environment with increasingly
high public expectations.
The lack of local public accountability of PCTs has been made
even more apparent since the creation of NHS foundation trusts which
332 J. Appleby and S. Gregory, NHS Spending – Local Variations in Priorities: An Update (London: The King’s
Fund, 2008).
333 LGA Health Commission, Who’s Accountable for Health? LGA Health Commission Final Report, 21
334 BBC News, “Actress Backs Hospital Campaign”, http://news.bbc.co.uk/1/hi/england/6378189.stm.
SOCIAL MARKET FOUNDATION
218
are “owned” by their members who are drawn from the public, staff,
patients and carers. Members elect governors who, together with
a number of appointed governors, have a distinct role to play in the
overall governance of the trust. This local public accountability on
the provider side has emphasised the “democratic deficit” of PCTs.
Essentially, policymakers have directed their efforts at the wrong side
of the purchaser/provider split: it is more important that commissioners
are held accountable by local people, rather than hospital trusts.
The government, in an effort to remedy the local accountability
deficit, has put in place a range of mechanisms to improve local
decision-making and support local accountability and public
involvement. These include directors of public health who are jointly
appointed by the NHS and local government, local council health
overview and scrutiny committees (OSCs), local strategic partnerships
and local area agreements, comprehensive area assessments, and
local involvement networks (LINks). Various arrangements have
also been made by the NHS and local government to support joint
commissioning of services. Finally, there is now a strengthened duty
on PCTs to involve and consult the public.
overview anD scrutiny coMMittees
Over the last few years there has been an attempt to strengthen
the tie between the NHS and local authorities. OSCs have been
established which give local councillors the opportunity to
formally question, scrutinise and influence the decisions of local
NHS bodies. OSCs have powers to summon NHS staff and request
information.335 The Department of Health states that OSCs “bring
democratic accountability into healthcare decisions and make
the NHS more publicly accountable and responsive to local
communities”.336
335 R. Thorlby and R. Lewis, How to Score Public Accountability Points (London: The King’s Fund, 2008).
336 The Department of Health, “Local Authority Overview and Scrutiny Commmittees (OSCs)”, http://www.
dh.gov.uk/en/Managingyourorganisation/PatientAndPublicinvolvement/DH_4093409.
FROM FEAST TO FAMINE
219
Although the development of OSCs represents a step towards
greater local accountability, questions remain about their degree
of influence and effectiveness. Department of Health guidance
states that PCT executives and key stakeholders are “encouraged to
implement” OSC recommendations,337 but PCTs are not obligated
to do so. The most recent evaluation of OSCs found that they have
only made a small impact in terms of changes to PCT services
and plans.338 It is also the case that the legitimacy of OSCs rests
on the democratic mandate of local government, which could be
undermined by continued low turnout at local elections.
Despite these shortfalls, there is a feeling that OSCs represent
a fruitful platform on which to build. The King’s Fund states that
the role of OSCs could be enhanced and the responsibility of ward
councillors extended.339 The Conservative Party agrees, arguing
that OSCs should be given greater powers and scope to investigate
and report on NHS services.340
Current proposals for OSCs do not go far enough. The SMF
Health Project recommends that they be given significantly
enhanced powers to hold PCTs to account.
recommendation 30:
• oscs should have the power to report issues of
concern, relating to a pct, directly to the pct
regulator.
• the regulator should be required to make a public
response to the osc.
• if the regulator’s response does not successfully
337 The Department of Health, “Local Authority Overview and Scrutiny Commmittees (OSCs)”.
338 Johnson, Scrutinising for Health: Health Scrutiny Evaluative Research Project.
339 Thorlby et al., Should Primary Care Trusts Be Made More Locally Accountable?.
340 The Conservative Party, Delivering Some of the Best Health in Europe: Outcomes Not Targets.
SOCIAL MARKET FOUNDATION
220
address the issue of concern the osc should have
the power to trigger an external review of pct
performance.
• this review should have the power to remove the
pct board and put in place a turnaround team.
• after a maximum of 12 months from the
introduction of the turnaround team a new board
should be elected by the local population.
other partnerships Between the nhs anD local
authorities
A number of other partnership arrangements exist to enable the NHS
to work with local government. NHS bodies and local authorities can
now pool budgets and integrate staff from different organisations
to work under a single management structure. Local authorities,
meanwhile, have a duty to set up local strategic partnerships to draw
together a range of bodies, including the NHS, to create strategies to
improve the wellbeing of the local area. There are also requirements
for PCTs and local authorities to cooperate through “joint strategic
needs assessment”, and to assess needs and commission services
together through local area agreements (LAAs).
However, the aim of many of these partnerships is not primarily
to improve local accountability but to meet local needs and drive
up service standards. Because of the democratically elected
status of local government, the NHS may be seen as more locally
accountable if it were to work closely with local authorities, but this
is very much local accountability by proxy and does not provide
the necessary legitimacy to allow PCTs to make tough decisions.
The system is moving in the right direction, but the reforms
have evolved in a piecemeal way resulting in a confusing set of
FROM FEAST TO FAMINE
221
arrangements that healthcare professionals, let alone the general
public, find difficult to understand.341 It remains unclear where
decisions are made, how decisions can be influenced and who is
responsible for what. An opinion poll for the LGA Health Commission
revealed a widespread lack of understanding and a high level of
confusion among the public about the structure and organisation
of the NHS, including the role of PCTs. It also found that only half
of those surveyed felt that their local PCT was currently answerable
for the quality of its services.342
The new accountability mechanisms, such as OSCs, are
essentially “external” mechanisms of local public accountability.343
New structures to deliver “internal” and participative local public
accountability are needed.
strenGtheninG local accountaBility: the options
Before leaping to suggest new systems of accountability it is first
worth considering the wisdom in allowing the current system,
which has only recently been developed, to bed in. Many healthcare
professionals argue that the mechanisms now in place will provide
satisfactory local accountability if they are given time to get up and
running and for local people to understand how they work. An NHS
Confederation online consultation with its members found that
80% of respondents were in favour of “retaining the existing system
to enable it to at least be fully implemented before considering
more change”.344 Another reorganisation of PCT structures so soon
after establishing the new system in 2006 would be disruptive and
should be avoided.
341 LGA Health Commission, Who’s Accountable for Health? LGA Health Commission Final Report, 5
342 Ibid.
343 J. Smith, R. Lewis and T. Harrison, Making Commissioning Effective in the Reformed NHS in England (London:
Health Policy Forum, 2006), 35.
344 The NHS Confederation, Principles for Accountability: Putting the Public at the Heart of the NHS (London: The
NHS Confederation, 2008), 3.
SOCIAL MARKET FOUNDATION
222
Nevertheless, while major structural reorganisation must be
avoided, it is essential for the credibility of the service that PCTs are
properly held to account by the local public in a way that cannot be
achieved under current arrangements.
Foundation pcts
One option that would give the public more of a say would be
to develop the concept of the foundation PCT, in which high-
flying PCTs would be granted the same governance structure as
foundation trusts.
Although this option seems appealing, as it would neatly
replicate the foundation status available to NHS trusts, there
are a number of problems. PCTs might well struggle to attract
members, especially as most people are not clear what a PCT is.
It is also unlikely that PCT membership would be representative
of the community as a whole, while the experience of foundation
trusts suggests that a large variation in the knowledge and skills
base of governors elected by members can be expected. Also, a
foundation PCT model would lead to a loss of direct control by the
Department of Health over commissioning to go alongside the
increasing loss of direct control of provision. Unsurprisingly, the
government has not shown enthusiasm for the idea. Furthermore,
identifying foundation PCTs would surely exacerbate variations in
performance between the best and worst commissioners rather
than drive service improvement across the board.
elected pcts
Alternatively, local public accountability of PCTs could be
strengthened alongside current upward accountability to central
government. For example, some or all of the PCT board could be
elected by the local public. This would provide local democratic
input but would not necessarily mean that PCTs have to sever ties
to the Department of Health (the DH could set policy and manage
locally elected boards). This is the system that was adopted in New
FROM FEAST TO FAMINE
223
Zealand,345 and has been considered by the Scottish Executive.346
However, PCT elections would be expensive and would probably
be undermined to some extent by low turnout, which would
prevent the PCT from being representative of all sections of the
community. There is also a danger of single issue politics and short-
termism controlling a politicised local health system.
A variation of this approach would be to incorporate existing local
democratic mechanisms into PCT governance. The most extreme
example of this system would be to pass all NHS commissioning
responsibilities on to local authorities which would then be held
accountable to their electorates, as is the case in countries such as
Denmark and Sweden.347 This option establishes a link between local
elected members and the local health system without requiring
additional local elections. There would be a democratic influence
on the local health system but without the single issue politics that
could emerge from a directly elected board.
However, such a system would not deliver specific accountability
for health services, as local government elections would be fought
on a number of different local issues, not just health. Also, as
local authorities and PCTs do not share the same boundaries, this
approach would result in further disruptive reorganisation, would
swamp local councils’ other work and could result in local party
politics interfering in the running of the NHS.
Some critics also argue that it is inappropriate for local
government to spend money that has been raised at a national
level; health is a centrally funded public service and so, it is argued, it
345 T. Ashton, N. Mays and N. Devlin, “Continuity Through Change: The Rhetoric and Reality of Health Reform
in New Zealand”, Social Sciences and Medicine 61 (2005).
346 The Scottish Parliament, Health Board Elections (Scotland) Bill (Edinburgh: HMSO, 2006).
347 S. Thorton, “Democratic Control Is Essential”, BMJ 333 (2006); J. Glasby, J. A. Smith and H. Dickinson,
Creating NHS Local: A New Relationship Between PCTs and Local Government (Birmingham: Health Services
Management Centre, 2006).
SOCIAL MARKET FOUNDATION
224
should not be the domain of local councillors. One response to this
objection would be to allow local areas to raise revenue to spend
on healthcare in their locality. However, this is not an option that the
SMF Health Project endorses. There is little appetite for local funding
of the health service from the public or from national politicians and
setting up such a system would cause further major disruption to
the health service. There would also be significant equity concerns
under such a funding system. with more affluent areas potentially
able to raise more funds than less well-off localities.348
The most powerful argument against simply incorporating
existing local democratic mechanisms into PCT governance as the
way to strengthen local accountability is that such an approach
would not necessarily satisfy the public. Public perceptions of local
government are generally not positive: work undertaken by the
Department for Communities and Local Government revealed that
most people do not know the identity of their local councillors,
are cynical of their reasons for being in local politics and do not
trust councils to deliver cost-effective services or honour the
promises they make in the run-up to elections.349 Similar views
were uncovered by the Audit Commission, which found that
councils are perceived by the public to have poor-quality leaders
and managers,350 while a Home Office study of police authorities,
where councillors sit on the board, found public scepticism about
whether this makes them more effective and accountable.351
Finally, polling for the NHS Confederation revealed that only 6% of
the public believe that decisions about medicines or treatments
funded by the local NHS should be made by local councillors.352
348 For more on funding issues, see chapter 3.
349 LGA Health Commission, Who’s Accountable for Health? LGA Health Commission Final Report.
350 2003 MORI survey for the Audit Commission, cited in Picker Institute, Accountability – Public Views and What
to Do About Them (Oxford: Picker Institute Europe, 2008), 10.
351 The Home Office, “Public Perceptions of Police Accountability and Decision-Making”, http://www.
homeoffice.gov.uk/rds/onlinepubs1.html.
352 The NHS Confederation, Principles for Accountability: Putting the Public at the Heart of the NHS.
FROM FEAST TO FAMINE
225
These findings suggest that involving local councillors in the
running of PCTs would not solve the public perception that PCTs
have a local accountability gap.
The public appear to believe that there is a democratic deficit at
a local level in the health service and so want services to be more
democratically run,353 but at the same time they have little trust in
national or local politicians. They also want local accountability to be
strengthened, but only want to be involved in decision-making when
they can influence the process and when something is not working.
In summary, the SMF Health Project argues that:
• the lack of local PCT accountability will become
increasingly unacceptable to the public as more power is
devolved to PCTs and their commissioning duties become
more widely understood;
• the ever greater variation in local services that is a desirable
consequence of greater PCT autonomy and improved
commissioning performance means that it will become
essential to strengthen local PCT accountability in order
to lend legitimacy to the decisions made by local health
officials;
• further involvement of elected local councillors is not an
adequate solution as the public do not have sufficient
confidence in local government;
• introducing directly elected PCT boards would solve the
“democratic deficit”, but could lead to single issue politics
and short-termism controlling the local health system and
would probably be undermined by low turnout.
None of these proposed ways to strengthen local PCT
accountability are entirely satisfactory.
353 A. Chisholm et al., Patient and Public Involvement in PCT Commissioning (Oxford: Picker Institute Europe, 2007).
SOCIAL MARKET FOUNDATION
226
a new MoDel For pct accountaBility
Currently, PCTs are held to account by SHAs through the world class
commissioning assurance framework. It is still unclear exactly what
will happen to failing PCTs, but Mark Britnell stated that they will
be subjected to “directed development” from their strategic health
authorities for “a year or two”, with the possibility of the private
sector being brought in to “accelerate their improvement”.354 The
SMF Health Project argues that it is at this point that greater public
involvement needs to be introduced in order to strengthen local
accountability. Ipsos MORI carried out polling and discussion
groups for the SMF Health Project with members of the public. The
results revealed that it is precisely when NHS functions are failing
that the public are most keen to be involved in decision-making on
the future of the failing service.
The current top-down intervention in which SHAs make the
decision about when to step in and intervene in the running of a
PCT needs to be accompanied by some manner of citizen trigger if
accountability is to be meaningful. The public need a way of being
able to make it clear when they are not happy with the performance
of their PCT, and to force action to be taken.
The SMF Health project recommends that this should take the
form of a citizens’ initiative to trigger a review of PCT competence.
The White Paper Our health, Our Care, Our Say granted new
powers to local communities to stimulate a “public petition” to
initiate action by PCTs where the public believe that some or all
local services are deficient.355 However, the White Paper simply
states that PCTs will have to “respond” to these public petitions,
but goes no further than this. This concept should be given teeth
in the same way that Recommendation 30, above, gives more
354 H. Crump, “PCTs Exceed Expectations in Year One”, HSJ (2009).
355 Department of Health, Our Health, Our Care, Our Say: A New Direction for Community Services (Lonson:
HMSO, 2006), 160.
FROM FEAST TO FAMINE
227
power to OSCs. The general public should be able to make it clear
when they are not happy with the performance of their PCT, and
to force action to be taken. This level of control and accountability
will be necessary if PCTs are to have the necessary legitimacy to
make difficult decisions over the next decade.
recommendation 31:
• a public petition of an agreed proportion of
the local population should have the power to
trigger an external review of pct performance.
• this review should have the power to remove the
pct board and put in place a turnaround team.
• after a maximum of 12 months from the
introduction of the turnaround team, a new
board should be elected by the local population.
conclusion
The model of accountability described in this chapter would fill
an important gap in the health system. Currently, accountability
is focused upwards towards the SHA and the Secretary of State.
But in a system where more autonomy is granted to local
commissioners, it becomes ever more important to make sure that
PCTs are accountable to local people. The proposals put forward
in this chapter would give real power to OSCs and the public in
general to bring regulatory attention to problems in the local
health system. It is hoped that not only would this encourage
greater legitimacy in commissioning decisions, but would also
support the role of the regulator in avoiding catastrophic failures
in the health system.
While it is certain that local people should have more power
over their commissioners, it is not so clear that local democracy
SOCIAL MARKET FOUNDATION
228
is the answer to questions of accountability. SMF Health Project
public opinion research found that people want to be involved in
health service decision-making when things go wrong. Therefore,
the project has concluded that there should be elections for
new PCT boards only when there has been a clear failure of the
incumbents. This offers the best chance of stability in management
for the PCT as well as allowing local people to get involved when
there are real problems to address in a particular area. In this way,
commissioners can be accountable for the decisions they make as
the health service moves away from a centralised top-down system
of governance.
FROM FEAST TO FAMINE
229
chapter eiGht: reGulatinG a local systeM
Throughout this report arguments in favour of a radically localised
health system have been championed. The report has set out a
vision for a system in which local commissioners, in combination
with clinicians and with involvement from patients and the public,
shape local health services that are innovative, high quality, efficient
and meet the needs of local people.
However, as discussed in chapter 5, a radically localised
system does not mean a system without national regulation. In
fact, it is essential that a system in which power is held at a local
level is “embedded in and supported by centralised standards
and evaluation of performance”.356 Effective national regulation
is crucial to ensuring that safety standards across the system are
upheld and that the public has confidence in both providers and
commissioners. National regulators also play an invaluable role in
the collection and publication of detailed, comparable data on the
performance of commissioners and providers.
In healthcare, as in other areas, “regulation” often has a negative
connotation, viewed as centrally imposed interference that restricts
innovation and stifles enterprise. At the same time, however, the
public expect direct and extensive oversight to ensure that quality
and safety are maintained. The regulatory framework of the health
system in England has to balance these two desires and attempt
to provide a robust system that protects patient safety without
becoming too burdensome. This chapter provides a review of the
current regulatory system and examines how it has evolved over
the past decade. It highlights the regulatory principles that should
guide policy in this area to support a shift from central to local
control of the health service.
356 K. Vrangbaek, “Key Factors in Assessing Decentralization and Recentralization in Health Systems,” in R. B.
Saltman, V. Bankauskaite and K. Vrangbaek (eds), Decentralization in Health Care: Strategies and Outcomes
(Buckinghamshire: Open University Press, 2007), 72.
SOCIAL MARKET FOUNDATION
230
The chapter sets out a brief theoretical explanation of regulation
before considering in detail principles that should inform the
regulation of healthcare provider organisations and commissioners.
what is reGulation?
Regulation involves the establishment of mechanisms that allow
governments, directly or indirectly, to oversee and shape the
behaviour of providers or funders of goods and services to ensure
that governmental objectives, such as efficiency, safety and quality,
are achieved.357
Regulation tends to be viewed principally as a remedy for
market failure,358 but it is also used to achieve wider social goals,
such as ensuring equity, diversity or social solidarity, and to hold
corporate, professional and social interests to account.359
quality regulation and economic regulation
A regulatory system has two main tasks: to provide quality regulation
and to provide economic regulation. Quality regulation aims to
protect consumers by ensuring that services and goods are safe and
of high quality. It should also ensure fair access to services and manage
the externalities and by-products of service provision. In healthcare
this would include public health and overall public safety.360
Economic regulation generally has three key objectives: first, to
develop a reliable delivery of services through regulating market
entry and exit and ensuring that competent and efficient providers
receive sustainable returns; second, to promote efficiency and
accountability by monitoring the financial performance of
357 R. Lewis, A. Alvarez-Rosete and N. Mays, How to Regulate Health Care in England? An International Perspective
(London: The King’s Fund, 2006), 2.
358 A. Ogus, Regulation: Legal Form and Economic Theory (Oxford: Hart Publishing, 2004).
359 K. Walshe, “The Rise of Regulation in the NHS,” BMJ 324 (2002).
360 Monitor, Developing an Effective Market Regulatory Framework in Healthcare (London: Monitor, 2005).
FROM FEAST TO FAMINE
231
suppliers and by intervening if necessary; and, finally, to foster a
fair operating environment by enforcing the rules of the game and
preventing anti-competitive behaviour.361
It is most common for both quality and economic regulation
to be carried out either by two separate bodies or by multiple
bodies across economic regulation and quality inspection
for different industry segments. However, another option is for
one body, a super regulator, to perform both economic and
quality regulation.
types of regulation
Regulation can be ex ante: anticipatory intervention that seeks
to prevent adverse behaviour or outcomes from occurring – for
example, the licensing of service providers before they enter the
market. Alternatively regulation is ex post: action is taken after an
offence has been detected to redress proven misconduct through
a range of options, including fines, injunctions and bans.
Regulatory agencies can also adopt different styles of
regulation; on the whole, they opt for one of two regulatory
models: deterrence or compliance. The deterrence model works
from the assumption that the organisation being regulated is an
“amoral calculator”362 that will act to maximise its own best interests
in whatever environment it is in. As such, the organisation must
be forced to behave responsibly by strict regulation enforcement.
The compliance model takes the opposite view, assuming that
the organisation being regulated is well meaning and will behave
dutifully where possible. Regulators who take this line provide
support and advice, and are more lenient in respect of mistakes
that occur.363
361 Ibid.
362 R. A. Kagan, “The ‘Criminology of the Corporation’ and Regulatory Enforcement Strategies”, in K. Hawkins
and J. M. Thomas (eds), Enforcing Regulation (Boston: Klunwer-Nijhoff Publishing, 1984), 67–96.
363 Walshe, “The Rise of Regulation in the NHS”.
SOCIAL MARKET FOUNDATION
232
Of course, in reality organisations aren’t “good” or “bad” but
have a wide variety of motivations and react in different ways to
different circumstances. Some regulators attempt to take account of
such variations by applying a range of different approaches, but are
often forced by legislative or political pressures to use a particular
regulatory style, regardless of its appropriateness.364 Traditionally,
regulators in the NHS have adhered to the compliance model of
regulation.365 However, more recently regulation of the public
sector has become increasingly orientated towards deterrence,
with this change in emphasis being favoured by politicians, the
media and the public.366
effective regulation
Effective regulation relies on a number of guiding principles.
First, it is important for regulators to be responsive. If regulation
is to be effective, then the agency carrying out the regulation
must appreciate the diversity of organisations it regulates and
be able to adapt to the way different organisations behave. A
“one-size-fits-all” policy should be rejected in favour of a more
flexible approach.
Walshe, writing in the British Medical Journal, argues that if
this responsive approach is to work, the regulators need to have
a range of graduated incentives and sanctions at their disposal:
incentives and informal interventions on the first rung, formal
supervision and inspection on the next rung, and closure of an
organisation or removal of their license at the top, for the most
serious cases. Regulators should be able to move freely up and
down the hierarchy of methods to ensure the most effective
regulation.367
364 Ibid.
365 P. Day and R. Klein, “The Regulation of Nursing Homes: A Comparative Perspective”, Milbank Q 65 (1987).
366 Walshe, “The Rise of Regulation in the NHS”.
367 Ibid.
FROM FEAST TO FAMINE
233
A further feature of effective regulation is the ability of
regulators to work with other stakeholders in the organisations
they regulate, as opposed to viewing the relationship between
them and the organisation as bilateral. This approach, known as
tripartism, requires groups such as patients and staff to be involved
in the process of carrying out regulation. Regulators tend to have
very limited resources and can only ever oversee a small proportion
of regulated activities. Tripartism enables them to extend their
oversight by using stakeholders to inform the regulatory process,
and sometimes, in the case of self-regulation, for example, to take
on regulatory responsibilities themselves.
Involving patients in the regulatory process also guards
against other stakeholders becoming dominant at the expense
of patients. A regulator’s relationship with different stakeholders
needs to be managed carefully, as there will always be
asymmetries in the extent to which different stakeholders can
mobilise resources to influence the regulatory process. There is
potential for ‘capture’ if the regulator fails to maintain an arm’s-
length independent relationship, becoming too closely identified
either with the interests of the organisations it regulates
(firm capture) or, alternatively, with those of the government
(government capture). It is important to make sure that industry,
professional or governmental interests are balanced by patient
interests.
Finally, to be effective and respected, regulators must strive to
balance independence and accountability. Regulatory agencies
need to be independent to ensure their credibility and their
impartiality, and to give them the freedom to take actions that
could be unpopular with some stakeholders. But, at the same
time, regulators must be held accountable for their actions and the
effects of their regulation.368
368 Ibid.
SOCIAL MARKET FOUNDATION
234
reGulation in the nhs
the rise of regulation
When the NHS was founded in 1948, the responsibility of providing a
good-quality service was left to the healthcare professionals. In order
to win the support of doctors for the new National Health Service,
the government struck a deal with the professions whereby the
government set the overall budget for the NHS and the professionals
were free to spend it how they saw fit.369 By the 1980s, variations in
care and concerns about equity across the health service, along with
the prevalence of inefficient and ineffective practices, meant that this
pact was in need of reform. In an effort to improve the performance of
the NHS, the government decided to take an increasingly direct role.
Through the use of primary and secondary legislation, directives from
the centre and performance management at a local, regional and
national level, it was hoped that the quality of healthcare provision
could be standardised and improved.370
The shift in emphasis towards greater performance
management of the NHS is part of a wider growth of the “regulatory
state”371 in the private and public sectors that has occurred in
Britain over the past 20 years. The Conservative government, while
publicly committed to deregulation, in fact introduced a host of
new regulatory agencies between 1979 and 1997. Many of these
regulators were created to oversee newly privatised industries, but
the government also increasingly used regulation to manage the
performance of public sector organisations.
The growth in regulation was in part the result of changes in the
way public sector organisations were managed and structured. The
Conservative government embraced the new public management
369 R. Klein, The New Politics of the NHS (London: Prentice Hall, 2000).
370 J. Dixon, Regulating Health Care: The Way Forward (London: The King’s Fund, 2005), 8.
371 G. Majone, “The Rise of the Regulatory State in Europe”, West European Politics 14: 3 (1994).
FROM FEAST TO FAMINE
235
philosophy, which extols the virtues of providing greater autonomy
for public sector organisations, placing them at arm’s length from
the government, separating purchasing and providing functions
and increasing competition. This approach did lead to greater
autonomy for public sector organisations, but was accompanied by
increased regulation.372
The development of regulatory agencies has also been spurred
on by a shift in the way society holds public services to account.
Previously, it was felt that accountability was satisfactorily achieved
through elected central and local government. But over the past
20 years, with the rise of the consumer society, it has increasingly
been felt that this is no longer adequate. There is now a desire across
society for more direct and extensive oversight.373
clinical performance of nhs hospitals
The drive to strengthen the regulation of healthcare was taken up by
the Labour government that came to power in 1997. At this time, public
confidence in the healthcare system – and especially in the healthcare
professions – had been seriously undermined by several high-profile
quality failures.374 In the period around and following the Bristol Royal
Infirmary inquiry – a detailed investigation into the deaths of 29 babies
undergoing heart surgery at an NHS hospital in Bristol – the media and
public began to call for a more robust system for quality assurance and
improvement, questioning whether the professions, left to regulate
themselves, could assure a high quality of care.375 This pressure resulted
in substantial reform of the regulatory system.
In 1999, the Commission for Health Improvement (CHI) was
established to inspect the clinical activity of NHS trusts. It was the first
372 Lewis et al., How to Regulate Health Care in England?, 2.
373 Ibid.
374 For example, the cases of Harold Shipman, Clifford Ayling and Rodney Ledward.
375 BBC News, “The Bristol Inquiry”, http://news.bbc.co.uk/1/hi/health/background_briefings/the_bristol_
heart_babies/297370.stm.
SOCIAL MARKET FOUNDATION
236
organisation ever to assess the clinical performance of NHS hospitals in
England. Although other statutory and non-statutory forms of external
review had been used in parts of the NHS in the past (such as the
Audit Commission and the National Audit Office), this was the first time
that an agency with a broad remit for quality improvement had been
created to review the activity of NHS trusts. The CHI reported directly
to the Secretary of State for Health and was tasked with providing an
“independent guarantee that local systems to monitor, assure, and
improve clinical quality are in place”.376 The CHI had wide powers to
monitor how clinical governance was implemented and to carry out
investigations into the management, provision or quality of healthcare
provided by trusts. It was planned that every trust would be reviewed
and reported on by the CHI within four years of its establishment.
However, despite the powers that the CHI enjoyed, its authority
was not as complete as some had hoped it would be. It did not possess
the power to impose sanctions or incentives to force or encourage
healthcare organisations to take account of its views, apart from the
publication of its reports, and it could only advise the Secretary of
State if it thought action was needed.377 In addition, the powers the
CHI did hold were limited to NHS organisations and property, and
excluded healthcare providers in the private sector and most general
practice premises, as they tend to be owned by the GPs themselves,
not the NHS. The government emphasised the independence of the
Commission, but in fact the Secretary of State had complete power to
direct the way in which it exercised any of its functions.
Subsequently, in April 2004, following completion of the
Kennedy Review into the Bristol Royal Infirmary cardiac deaths,
the CHI was replaced by the Commission for Healthcare Audit and
Inspection, which became know as the Healthcare Commission.378
376 K. Walshe, “Improvement Through Inspection? The Development of the New Commission for Health
Improvement in England and Wales”, Quality in Health Care 8 (1999).
377 Ibid.
378 J. R. Haslam, “What Is the Healthcare Commission Trying to Achieve?”, Soc Med 100 (2007).
FROM FEAST TO FAMINE
237
the healthcare commission
The Healthcare Commission had more power than its predecessor.
It could replace managerial staff in poorly performing NHS
organisations and even force the merger or break-up of trusts as
a last resort. It provided guidance to the NHS, reviewed formal
complaints against the NHS, carried out patient satisfaction surveys
and presented an annual “state of healthcare” report to Parliament.
It was also responsible for inspecting and regulating private
sector providers against national requirements, a task that the CHI
did not undertake. However, its approach to regulating private
sector providers was somewhat different from its approach to NHS
providers. The Commission was required to inspect all independent
providers once a year against the national minimum standards for
independent healthcare. These standards were similar to the core
standards that applied to the NHS, but were more detailed and
difficult to achieve. If independent providers failed to comply with
the requirements, the Commission could intervene and ultimately
prosecute or de-register the provider.379
The establishment of the Healthcare Commission was initially
viewed as an important development in the drive to improve
quality across the NHS, but it soon began to receive mixed reviews.
It was criticised for placing too heavy a bureaucratic burden on the
organisations that it inspected, and for taking a reactive approach
to quality improvement.380 These problems were highlighted
in a Healthcare Commission survey of 220 NHS trusts in 2006–7,
which uncovered frustration amongst trusts about a perceived
duplication of Healthcare Commission roles with other regulators,
as well as concerns about follow-up inspections and questions
about the comparability of scores across trusts. However, despite
379 The Department of Health, The Future Regulation of Health and Adult Social Care in England (London:
HMSO, 2006), 31.
380 S. Leatherman and K. Sutherland, The Quest for Quality: Refining the NHS Reforms (London: The Nuffield
Trust, 2008), 35.
SOCIAL MARKET FOUNDATION
238
these qualms, the survey revealed that 93% of trusts found that the
annual health check did have a positive impact on patient care.381
It is difficult objectively to assess the impact of the Healthcare
Commission compared to other interventions to improve quality.
Improvement in overall ratings was mainly achieved in the better-
performing trusts, with a significant increase in the number of trusts
rated “excellent” for both quality of services and use of resources,
while the number of trusts rated “weak” remained static. High-
performing trusts were mainly foundation trusts, so it is hard to know
whether their improvements were due to the regulatory impact of
the Healthcare Commission or to other organisational changes, such
as greater autonomy enjoyed by foundation trusts.382
Foundation trusts
The Healthcare Commission did not directly regulate foundation
trusts; instead, this task was carried out by Monitor, an independent
regulator established in January 2004. Monitor is responsible for
licensing new foundation trusts, for monitoring their performance
and for intervening in their management if the trust significantly
breaches the terms of its authorisation.
Performance of foundation trusts was assessed against
healthcare standards by the Healthcare Commission, which then
sent reports to Monitor which had the power to intervene in the
running of a foundation trust in the event of failing performance.
Monitor’s statutory powers of intervention included imposing
changes on the composition of the trust board and requiring that
it complied with an imposed action plan.383
381 Ibid.
382 Ibid., 35–6.
383 Monitor, Monitor’s Rules of Procedure (London: Monitor, 2006).
FROM FEAST TO FAMINE
239
Further reForM oF healthcare reGulation
Despite the establishment of the Healthcare Commission and
Monitor, there continued to be calls for further changes to
the system. One concern was the burden that the regulatory
system placed on providers.384 The demands of the Healthcare
Commission, coupled with continuing financial reviews by the
Audit Commission and requests for information about trust activity
from numerous other organisations, led to what some described as
“inspectorial overload”.385
Another concern with the regulatory framework was that it
had become fragmented over time.386 As mentioned above, there
were different regulatory procedures, standards and enforcement
measures for NHS and independent sector providers, and the
system also retained the barriers between health and social care.
As more decisions were being devolved to the local level and
more choice given to patients and the public, it was felt that the
distinctions would become more and more archaic.387
In response to these concerns, the Department of Health,
in 2005, began a review of regulation in health and social care
that resulted in the Health and Social Care Act 2008, receiving
Royal assent on 22 July 2008. 388 The Act contained significant
measures to modernise the regulation of health and social care.
Most crucially, it set out the establishment of the Care Quality
384 R. C. Heron, “Better Coordination of the Inspection, Review and Audit of Healthcare Organisations”, http://
www.concordat.org.uk/_db/_documents/Better_coordination_of_the_inspection,_review_and_audit_
of_healthcare_organisations.pdf.
385 Walshe, “The Rise of Regulation in the NHS”.
386 C. Hughes, “Evidence Submitted by The Hearing Aid Council (Audio 42)”, http://www.publications.
parliament.uk/pa/cm200607/cmselect/cmhealth/392/392we26.htm.
387 The King’s Fund, “Response to the Department of Health Consultation on the Future of Regulation of
Health and Adult Social Care in England”, http://www.kingsfund.org.uk/applications/site_search/?term=
consultation+response+regulation&searchreferer_id=2. 2
388 Department of Health, The Future Regulation of Health and Adult Social Care in England: A Consultation on the
Framework for the Registration of Health and Adult Social Care Providers (London: HMSO, 2008).
SOCIAL MARKET FOUNDATION
240
Commission, a new integrated regulator for health and adult
social care.
care quality commission
On 1 April 2009 the Care Quality Commission (CQC) took over from the
Healthcare Commission, the Commission for Social Care Inspection
and the Mental Health Act Commission. The new Commission, for the
first time, provides regulation across both health and adult social care,
reflecting the growing integration of those services.
The CQC is responsible for:389
Safety and quality assurance
• registering providers of health and adult social care;
• monitoring and assessing providers against a set of
registration requirements;
• escalating serious service failures, using discretionary
sanctions that ultimately lead to enforced closure of
a service or of the provider through de-registration, if
patients or users of services are seriously at risk;
• conducting further inspections or investigations where
there are significant risks to the required levels of safety
and quality;
• publishing information and reports using information
gathered through carrying out its functions.
Commissioner assurance and performance assessment of
providers
• ensuring good-quality information is available to support
patient and service user choice;
389 Health and Social Care Act 2008 (London: HMSO, 2008).
FROM FEAST TO FAMINE
241
• publishing an independent assessment of both providers
and commissioners for the purpose of public accountability;
• providing an annual report to Parliament on the state
of health and adult social care and the operation of the
Mental Health Act;
• carrying out general service reviews, studies and research
on issues that arise from carrying out its functions.
Minimising the burden of regulation and inspection
• adhering to the principles of good regulation and carrying
out its functions in a way that minimises the burden of
regulation and is proportionate, targeted, accountable,
consistent and transparent.
The introduction of the CQC is a clear signal of the trend towards
consolidation of regulatory functions as a mechanism to achieve
quality. Innovations in the CQC model are considered below, and
later in this chapter consideration is given to whether an external
regulator such as the CQC is best placed to improve quality.
reGistration
From April 2010, all providers of health and adult social care
regulated activities, including NHS, local authority, private and third
sector providers, will have to be registered with the CQC.390 Before
the introduction of the CQC, any non-NHS provider of health and
social care had to register with either the Healthcare Commission
or the Commission for Social Care Inspection in order to provide
services legally. However, there was no registration system for NHS
bodies, which were instead assessed against the Standards for
Better Health by the Healthcare Commission.
390 Care Quality Commission, “Summary of Guidance About Compliance”, http://www.cqc.org.uk/_db/_
documents/LP_consultation.rtf.
SOCIAL MARKET FOUNDATION
242
The new initiative is an attempt to develop a coherent system
of registration across health and adult social care based on one
set of generic “registration requirements”, which all providers have
to meet. Providers have to demonstrate that they can meet the
essential levels of safety and quality required for registration and
will need to continue to meet them to maintain their registration.
registration requirements
The robustness of the system of registration will depend on the
registration requirements. A single set of registration requirements
is proposed for all providers which will concentrate on essential
levels of safety and quality.391 They will be separate from the
revised set of improvement standards to be developed for the
NHS to benchmark good practice. Baroness Young, chair of the
CQC, has declared that registration “will involve meeting a wider
range of standards”392 than under the old regulation regime, and
the Department of Health has set out 18 broad standards that will
apply to health and social care services. These will replace the
current core standards for better health, which apply to NHS trusts,
and the national minimum standards and regulations, which apply
to social care and independent sector health providers.393
391 Director of Adult Social Services, “Report to Cabinet Members for Health, Social Care and Partnerships”,
http://www.solihull.gov.uk/akssolihull/images/att15145.doc.
392 Care Quality Commission, “New Regulator for Health, Mental Health and Adult Social Care”, http://
www.cqc.org.uk/newsandevents/pressreleases.cfm?cit_id=34816&FAArea1=customWidgets.content_
view_1&usecache=false.
393 Proposed topics for registration requirements: making sure people get the care and treatment that
meet their needs safely and effectively; safeguarding people when they are vulnerable; managing
cleanliness, hygiene and infection control; managing medicines safely; making sure people get the
nourishment they need; making sure people get care and treatment in safe, suitable places which
support their independence, privacy and personal dignity; using equipment that is safe and suitable for
people’s care and treatment and supports their independence, privacy and personal dignity; involving
people in making informed decisions about their care and treatment; getting people’s ongoing
agreement to care and treatment; responding to people’s comments and complaints; supporting
people to be independent; respecting people and their families and carers; having arrangements for
risk management, quality assurance and clinical governance; keeping records of the provision of care
and treatment; checking that workers are safe and competent to give people the care and treatment
they need; having enough competent staff to give people the care and treatment they need; supporting
workers to give people the care and treatment they need; and working effectively with other services.
FROM FEAST TO FAMINE
243
The registration requirements aim to ensure that care provided
is safe, effective, fair and personalised. The requirements are
generic, but the criteria used to assess compliance, which will
be developed by the CQC, will be tailored to the type of service
being registered, taking into account the differences between, for
example, a hospital and a care home.394
primary care
Initially it was unclear whether primary care providers would have
to register with the CQC. Primary care professionals are already
individually registered by their professional governing bodies and
are subject to the Quality and Outcomes Framework (QOF) and PCT
contracting arrangements. It was thought that CQC registration
may be unnecessary.
However, although the QOF does gather data on some aspects
of the quality of general practice, it is far from exhaustive and
does not cover all areas of primary care.395 The QOF is also failing
adequately to detect the considerable variation in the quality of GP
services that is recognised both in the profession and among PCT
managers.396 Commissioners are expected to commission for best
practice but are hampered by a lack of adequate information that
benchmarks different practices nationally.
In addition, the current primary care regulatory arrangements
focus mainly on the competence of the individual professional, as
opposed to the practice. Given the increasing range of services
offered in primary care, including minor operations and other
services traditionally provided in hospitals, it was argued that
primary care organisations should be subject to the same standards
as secondary care providers.
394 Director of Adult Social Services, “Report to Cabinet Members for Health, Social Care and Partnerships”.
395 The Department of Health, “Quality and Outcomes Framework (QOF)”, http://www.dh.gov.uk/en/
Healthcare/Primarycare/Primarycarecontracting/QOF/DH_099079.
396 H. Mooney, “GP Quality: the Final Frontier for Inspectors”, HSJ (2009).
SOCIAL MARKET FOUNDATION
24 4
As such, the Department of Health decided, after additional
consultation, that NHS primary medical and dental services must
register with the CQC by 2010/11 (a year later than other NHS
providers). This development means that, for the first time, around
8,500 GP practices and 9,000 dental practices will be required to
register with the mainstream regulator.397
The Department of Health has stated that the new system
will “strengthen PCTs’ core responsibility for managing primary
care contracts, provide broader information about primary care
services to the public, and tackle unacceptably poor or unsafe
performance”.398 The CQC will have the authority to fine or shut
down substandard GP practices.
reGulation anD quality
The nature of the relationship between quality and regulation is
a key question. Regulators have a central role in ensuring safety,
but there is a general lack of clarity about the role of regulators as
a driver of improved quality relative to the local commissioner or
the provider itself. Some commentators, such as NHS Alliance chair
Michael Dixon, have suggested that the registration of primary care
services would ensure a minimum level of quality and safety, but
would be less effective at generating continuing improvements.399
Similar sentiments have been expressed, for example, by the King’s
Fund, about the new regulatory system’s ability to ensure quality
across the whole service.400
This argument is linked to a wider question about whether
inspection is the best way of ensuring quality. The CQC does
not want to be thought of as a traditional inspectorate. Baroness
397 C. Santy, “Care Quality Commission to Regulate Primary Care”, HSJ (2009).
398 Department of Health, cited in ibid.
399 C. Santry, “Care Quality Commission: A Chance to Peep Under the Primary Care Carpet”, HSJ (2008).
400 The King’s Fund, “Response to the Department of Health Consultation on the Future of Regulation of
Health and Adult Social Care in England”, 8.
FROM FEAST TO FAMINE
245
Young is adamant that the CQC will be a modern, proportionate
and responsive regulator, which will work with the providers
and commissioners of services to encourage improvement. But
nevertheless, the CQC will carry out inspection. Baroness Young
has stressed that the CQC will not be an easy touch: the regulator
will inspect and monitor health and social care providers and is
equipped with a range of tough new enforcement powers which
they “won’t be afraid to use … when it is appropriate”.401
Inspection tells organisations what problems exist, but does not
necessarily help them to solve those problems. There is a danger
that problems are identified but then little changes as a result.
External review and inspection is the correct method for ensuring
safety, but may not be particularly suitable for securing continuous
quality improvement. Quality improvement is an organisational
challenge internal to the healthcare provider, so although an
external perspective on performance and quality can be valuable,
alone it cannot change anything. To bring about improvements,
the organisation has to take on board the need for change and
have the skills and resources itself to make change happen.
External inspection processes can also seem threatening and lead
to defensiveness and self-justification, which makes improvement
more difficult to achieve.402
Other mechanisms will therefore have to be relied upon to
ensure quality improvement. Financial incentives may play a part
– for example, payment for outcomes rather than activity could be
introduced. Competition for patients might lead to improvements
in quality, while routine reporting of comparative performance
data on performance indicators will also be important.403 However,
401 Care Quality Commission, “Care Quality Commission Launches”, http://www.cqc.org.uk/newsandevents/
newsstories.cfm?cit_id=34817&FAArea1=customWidgets.content_view_1&usecache=false.
402 Walshe, “Improvement Through Inspection?”.
403 The King’s Fund, “Response to the Department of Health Consultation on the Future of Regulation of
Health and Adult Social Care in England”, 7.
SOCIAL MARKET FOUNDATION
246
relying solely on choice, competition and the availability of
performance information to drive up quality has not been
particularly successful to date. There is no substantive evidence,
even in a highly competitive market system like that in the US, that
patient choice will significantly drive quality improvement,404 while
some international evidence suggests that patients are unlikely to
use quality information when making their choices.405
The other mechanism that is being relied upon to drive up
quality is commissioning.
local commissioners responsible for the quality of provider
organisations
Commissioners increasingly have responsibility for the quality of
NHS services. Although the new regulator, the CQC, does have a
statuary responsibility for the quality and safety of NHS services,
the Department of Health has emphasised that “key ‘regulatory’
functions … will be picked up elsewhere”, most noticeably “by
commissioners”.406 The department states that although the CQC
will have an important role in ensuring that all providers meet
national standards, it is “excellent commissioning” that will drive up
the quality of services and ensure that a range of local providers is
available to offer choice of services to patients.
The CQC has a vitally important role to play in approving new
providers, making sure that minimum standards are adhered to,
guaranteeing safety and compiling nationally comparable data on
provider performance. But it is PCTs that should be responsible for
using this data to commission effectively and ensure the quality
of the services that they commission. Commissioners are much
404 P. Shekelle et al., Does Public Release of Performance Results Improve Quality of Care? A Systematic Review
(London: The Health Foundation, 2008).
405 E. C. Schneider and T. Lieberman, “Publicly Disclosed Information About the Quality of Health Care:
Response of the US Public”, Quality in Health Care 10:2 (2001).
406 The Department of Health, The Future Regulation of Health and Adult Social Care in England, 6
FROM FEAST TO FAMINE
247
better placed to drive up quality, as they are embedded in local
areas and can see from day to day what works well and where
there are problems.
External review and inspection is the correct method for
ensuring safety but is not particularly suitable for ensuring
continuous quality improvement, which is a long term, internal
process. Commissioner organisations, which are based at the
same local level as the provider and have a long-term, continuous
relationship with the provider, are much better placed to help
encourage, stimulate and support this internal improvement.
They also have more flexible responses to failure. Commissioners
can tweak contracts in multiple ways to stimulate improvement,
which an external regulator cannot. Indeed, since the PCT “holds
the purse strings”, it is the most effective organisation to demand
improvement from the providers it works with.
recommendation 32:
• the quality of provider organisations should be
assured and developed through pct contracts.
• the care quality commission should maintain
responsibility for setting minimum safety
and quality standards as part of the licensing
arrangement, and collecting comparative data
on providers across the health service.
the reGulation oF coMMissioners
The preceding section has established a need to involve PCTs in the
regulation of local providers, alongside an assurance of safety and
basic standards from the CQC. But how should PCTs themselves be
regulated?
SOCIAL MARKET FOUNDATION
248
Currently, PCTs report to four different bodies on different
aspects of their performance
• the Department of Health;
• the Audit Commission on financial performance;
• Strategic Health Authorities; and
• the Care Quality Commission.
There are two major problems with the structure as it stands.
First, it provides unnecessary work for hard-pressed commissioners.
They report to four different bodies, each of which has different
requirements and different processes. SMF Health Project
interviews with commissioners and seminar discussions identified
frustration at the unnecessary work this generates.
The second problem is one of accountability. For patients, it
is difficult to access information about PCT performance, as it is
not held in a single repository. This situation must change as
commissioners develop, and as we move away from a centralised
system driven by national standards. It is imperative that patients
and the public can easily access high-quality information about
how their local commissioner is performing.
There should be a consolidation of PCT regulation, with a single
body overseeing the performance of PCTs against minimal national
targets, and providing information for the public with a particular
focus on Patient Reported Outcome Measures (PROMS).
recommendation 33: a single commissioning regulator
and inspectorate should be introduced – the nhs
commission – to sit alongside the care quality
commission.
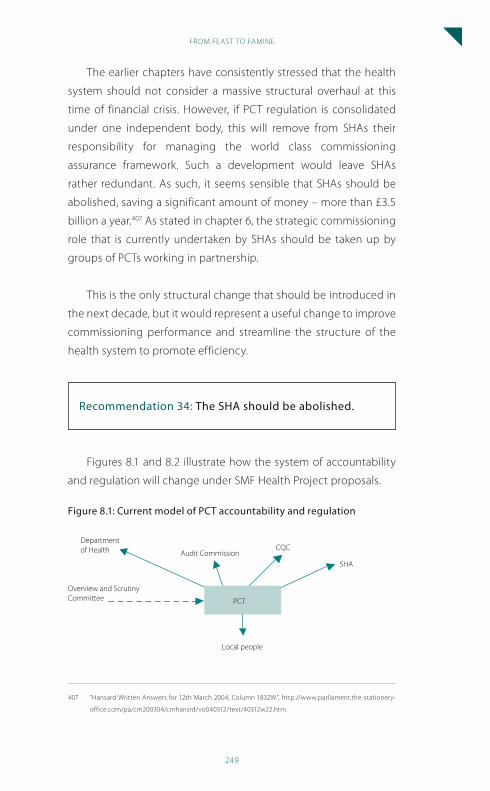
FROM FEAST TO FAMINE
249
The earlier chapters have consistently stressed that the health
system should not consider a massive structural overhaul at this
time of financial crisis. However, if PCT regulation is consolidated
under one independent body, this will remove from SHAs their
responsibility for managing the world class commissioning
assurance framework. Such a development would leave SHAs
rather redundant. As such, it seems sensible that SHAs should be
abolished, saving a significant amount of money – more than £3.5
billion a year.407 As stated in chapter 6, the strategic commissioning
role that is currently undertaken by SHAs should be taken up by
groups of PCTs working in partnership.
This is the only structural change that should be introduced in
the next decade, but it would represent a useful change to improve
commissioning performance and streamline the structure of the
health system to promote efficiency.
recommendation 34: the sha should be abolished.
Figures 8.1 and 8.2 illustrate how the system of accountability
and regulation will change under SMF Health Project proposals.
Figure 8.1:
Department of Health
Overview and Scrutiny Committee
Audit CommissionCQC
SHA
Local people
PCT
current model of pct accountability and regulation
407 “Hansard Written Answers for 12th March 2004, Column 1832W”, http://www.parliament.the-stationery-
office.com/pa/cm200304/cmhansrd/vo040312/text/40312w22.htm.
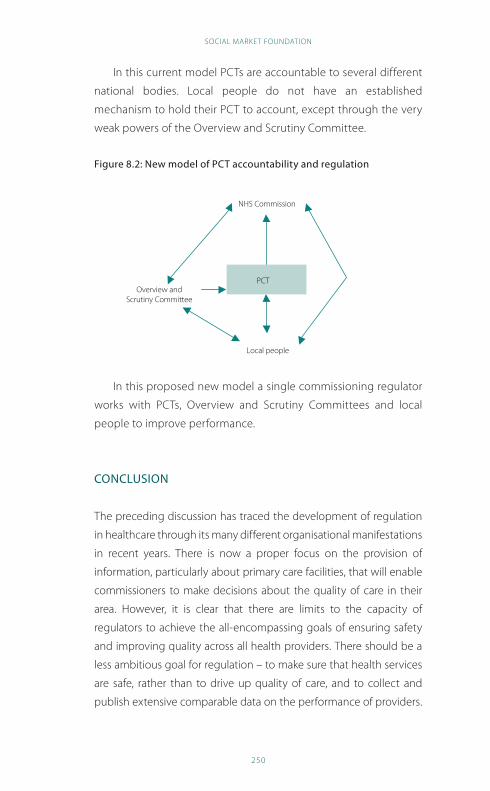
SOCIAL MARKET FOUNDATION
250
In this current model PCTs are accountable to several different
national bodies. Local people do not have an established
mechanism to hold their PCT to account, except through the very
weak powers of the Overview and Scrutiny Committee.
Figure 8.2: new model of pct accountability and regulation
Overview and Scrutiny Committee
NHS Commission
Local people
PCT
In this proposed new model a single commissioning regulator
works with PCTs, Overview and Scrutiny Committees and local
people to improve performance.
conclusion
The preceding discussion has traced the development of regulation
in healthcare through its many different organisational manifestations
in recent years. There is now a proper focus on the provision of
information, particularly about primary care facilities, that will enable
commissioners to make decisions about the quality of care in their
area. However, it is clear that there are limits to the capacity of
regulators to achieve the all-encompassing goals of ensuring safety
and improving quality across all health providers. There should be a
less ambitious goal for regulation – to make sure that health services
are safe, rather than to drive up quality of care, and to collect and
publish extensive comparable data on the performance of providers.
FROM FEAST TO FAMINE
251
Through a more sophisticated use of information and their local
purchasing power, it is commissioners who must play a bigger role in
driving up quality, and weeding out poor providers of care.
SOCIAL MARKET FOUNDATION
252
chapter 9: conclusion
This report has set out a process of reform to help the health service
in England deal with the catastrophic impact of the recession on
the public finances. Whatever the political rhetoric, the NHS will
not be immune from a spending squeeze that will be worse than
any previously experienced by the vast majority of civil servants
and public sector workers. There is an urgent need to obtain better
value for money from health spending through greater efficiency
and a proper focus on demand management. If the NHS cannot do
more for less, then its future is in doubt. The long waiting lists and
low quality care of the past must not return if the health service is
to maintain public support in the years ahead.
The recommendations set out above recognise the need
to take radical action but within politically realistic limits. The
NHS has suffered in recent years from the sheer number of
reorganisations it has undergone. There is no doubt that in some
cases reorganising the health service has not helped it to perform
better. The conclusions of the SMF Health Project acknowledge
that while a revolution in structures is undesirable, a revolution
in attitudes is essential. Policymakers in central government must
become genuinely committed to devolving power to frontline
commissioners. Those frontline commissioners must become
the driving force of NHS improvement, taking on vested provider
interests. And a dialogue with patients should be begun to help
users recognise the desirability of a diverse, varied system that
responds to the needs of local people, rather than aspiring to an
unrealistic and inefficient idea of national uniformity.
The move towards a system of local control and local variation
is essential if the NHS is to survive the crisis in public finances. The
limits of centrally driven performance management have been
reached. While there has been substantial improvement as a result
of the reform and investment of the past few years, the ability of
FROM FEAST TO FAMINE
253
central government to make the savings that will be needed is
questionable. High quality local commissioning offers the best
chance to deliver value for money, not performance management
from the centre. It is time to try a new approach; one that harnesses
the creativity and energy of local professionals. Additionally, the
hard decisions that lie ahead can only be justified to local people
by local health organisations, backed by local accountability
mechanisms, not the Department of Health.
There will undoubtedly be political pain in the move from
a centralised service to one where local commissioners drive
improvement. However, public opinion research carried out as
part of the SMF Health Project shows that people are realistic
about the limits of NHS care, and open to the idea that resources
should be distributed according to the needs of different
areas. Political courage will be needed if a move away from
the persistent idea that the NHS is the same everywhere is to
be achieved. But the benefits of local choice must supersede
concerns about postcode lotteries.
A diverse, varied service is one that fits with social market
principles. Markets in healthcare provision can provide a pluralist,
innovative and efficient system. Social goals of fairness and
universal access can still be achieved through accountable
commissioning organisations, and strong regulation. The benefits
of a market approach to healthcare could be considerable, and can
be achieved largely within existing NHS structures.
What does the future hold for the health system? It is a
rocky road ahead. The year on year rise in health spending as a
proportion of GDP cannot be continued indefinitely. It may be that
the recession will present an opportunity to radically transform
health services to save money in the long term. This transformation
will require policymakers to consider options that have hitherto
been politically unacceptable – including user charging.
SOCIAL MARKET FOUNDATION
254
In many different sectors of politics and society a new
consensus is emerging that public services must be substantially
reformed to deal with the challenges ahead. Old solutions that
look to management by central government to make savings and
improve outcomes for patients will not succeed in delivering value
for money. Instead, a radical redistribution of power must take
place. With strong commissioners, functioning provider markets
and better accountability through national regulation and local
accountability mechanisms, the NHS has every chance of a strong
future. Without these much needed reforms, the future is bleak.
FROM FEAST TO FAMINE
255
copyright © the social Market Foundation, 2009










![Feast and Famine: Regulation of Black Hole Growth in Low ... · arXiv:0812.1224v2 [astro-ph] 27 Apr 2009 Feast and Famine: Regulation of Black Hole Growth in Low Redshift Galaxies](https://img.pdfslide.us/doc/110x75/601364db31b59e2c4238a88c/feast-and-famine-regulation-of-black-hole-growth-in-low-arxiv08121224v2-astro-ph.jpg)