Embed Size (px)
Citation preview
FOETUS IN FOETUAND THE RETROPERITONEAL TERATOMA
BY
R. H. LEWIS*From Llandough Hospital, United Cardiff Hospitals
(RECEIVED FOR PUBLICATION JUNE 17, 1960)
Foetus in foetu, a descriptive term attributed toMeckel (circa 1800), should be applied only to thoserare cases where a parasitic twin is found includedwithin the abdomen of its partner. Lord (1954;1956) reported two definite cases and reviewedother possible cases.
In contrast, the variety of teratoma which occursin the retroperitoneal space is much less defined.Since the description of the first recognizable case byDickinson (1871), an increasingly complex volumeof literature has accumulated. Palumbo, Cross,Smith and Baronas (1949) documented many of theearliest cases of retroperitoneal teratoma and theirwork drew together some of the facts concerning acondition which they rightly say is seldom discussedin the medical reference volumes. Charles (1953)traced 82 case reports in the literature and since thistime at least five further reports have appearedincluding some from Russia and Bulgaria. Manytheories of origin have been suggested, with someauthors contending that the teratoma represents aform of included twin. Although this is nowunacceptable, it has resulted in the description ofmany retroperitoneal teratomas in confusing terms.
Willis (1958) pointed out the separate nature of theretroperitoneal teratoma and foetus in foetu,emphasizing that the former is a true tumour whilethe latter is not. However, as both conditionsoccur in the upper part of the retroperitoneal space,it is not surprising that terms such as 'foetus infoetu', 'parasitic twin' and 'suppressed twin' havebeen misapplied to teratomas having a markeddegree of differentiation and some foetiform charac-teristic. Indeed, Willis concedes that final classi-fication may be difficult, though he does not admitthat the overlap of certain features implies that thetwo conditions are the same.The purpose of this report is (1) to describe a
further case where borderline pathological featuresare present; (2) to discuss and compare briefly the
* At present, Research Fellow in Surgery, Harvard Medical School,Boston, Mass., U.S.A.
pathology of foetus in foetu and retroperitonealteratoma and (3) to discuss their symptoms, physicalsigns, diagnosis and treatment.
Case ReportK.J., a 4-week-old female infant, was admitted to the
Department of Child Health, Llandough Hospital,Cardiff, on October 18, 1958. The provisional diagnosisby the referring practitioner was 'intussusception'. Themother stated that the infant, who hitherto had beenquite normal, had had vomiting after feeds, apparentabdominal pain, and green loose motions for 24 hours.
Birth weight was 7 lb. 5 oz. and gain had been normal.She was breast fed initially, but changed to artificial driedmilk after 10 days. Pregnancy and delivery ofthe motherhad been normal. The family was otherwise healthyand there was no history of previous twin pregnancies.On clinical examination, the infant appeared well
nourished and healthy. Weight was 8 lb. 6 oz. Therewere no signs of dehydration, anaemia or jaundice. A'strawberry' naevus was present on the lateral aspect ofthe right thigh. The abdomen appeared slightly dis-tended in the right upper quadrant, and in this region,extending across the midline, a firm, immobile, circum-scribed mass was palpable. The liver could be separatelypalpated a finger's breadth below the costal margin.Bowel sounds were increased. Rectal examination wasnegative.
In the early consideration of the diagnosis, a retro-peritoneal tumour was thought likely. A barium enemaexamination performed immediately was found to benormal. An excretory pyelogram showed normallysituated and functioning kidneys, with a bifid pelvison the right side. During these examinations abnormalcalcification was noted above the pole of the rightkidney. Further postero-anterior and lateral viewsdemonstrated a chain of solid calcification in this region.While exact interpretation was not possible at this time,the presence of this calcification appeared to favour thediagnosis of retroperitoneal teratoma.Blood group was A Rh+; Hb 80% (118 g.); white
blood cell count, 21,000/c.mm.; corrected erythrocytesedimentation rate, 39 mm./hour. A urine specimenwas found to contain pus cells and organisms identifiedas Esch. coli. A stool examination for pathogens wasnegative.
220
copyright. on 8 June 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.36.186.220 on 1 A
pril 1961. Dow
nloaded from
FOETUS IN FOETU AND RETROPERITONEAL TERATOMAThe intercurrent urinary infection was treated with
nitrofurantoin for five days with satisfactory response.Twelve days after admission, laparotomy was per-
formed through a right paramedian incision (Mr.D. B. E. Foster). The exploration revealed a retro-peritoneal tumour approximately 2 in. (5 cm.) in diameterlying somewhat to the right of the midline, between thediaphragm and the third lumbar vertebra. The liverand its hilar structures, the duodenum and the pancreaswere displaced forwards by the mass. After mobiliza-tion of the duodenum and transverse colon medially anddownward, the capsule of the mass was opened with therelease of a little reddish brown fluid. The containedmass was easily removed, and after careful dissectionthe capsule was also excised. The abdomen was closedin layers without drainage.
Postoperative course was uneventful and normal feed-ing was rapidly re-established. When discharged fromhospital on the ninth postoperative day the infant weigh-ed 9 lb. 12 oz. The patient has shown normal progresswhen seen in the follow-up clinic.
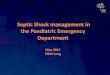
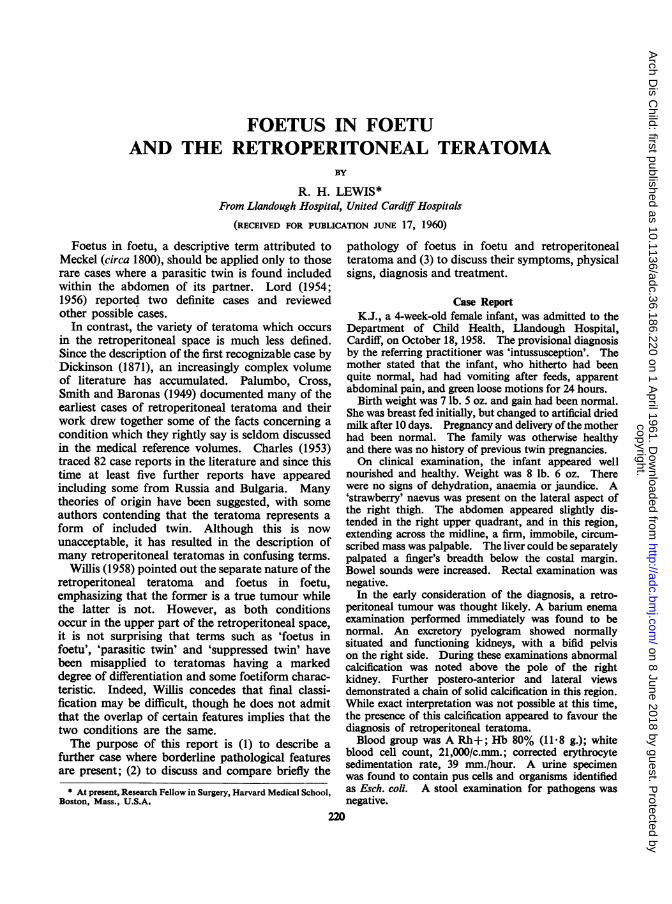
Pathological examination of the specimen was carriedout by Dr. F. K. Storing. 'Macroscopically: Thespecimen consisted of a parasitic foetus showing smallimperfectly developed extremities. A separate specimenlabelled capsule was also examined. Microscopically:Sections taken from the interior of the trunk part ofthe specimen showed heterogeneous arrangement of avariety of tissues and cells, including muscle fibres, fat,cartilage, intestinal mucosa, glands and nerve fibres.The appearances were typical of an adult teratoma. Thecapsule consisted of very vascular connective tissueembedded in which were ganglion cells, nerve fibres andscattered lymph follicles.'
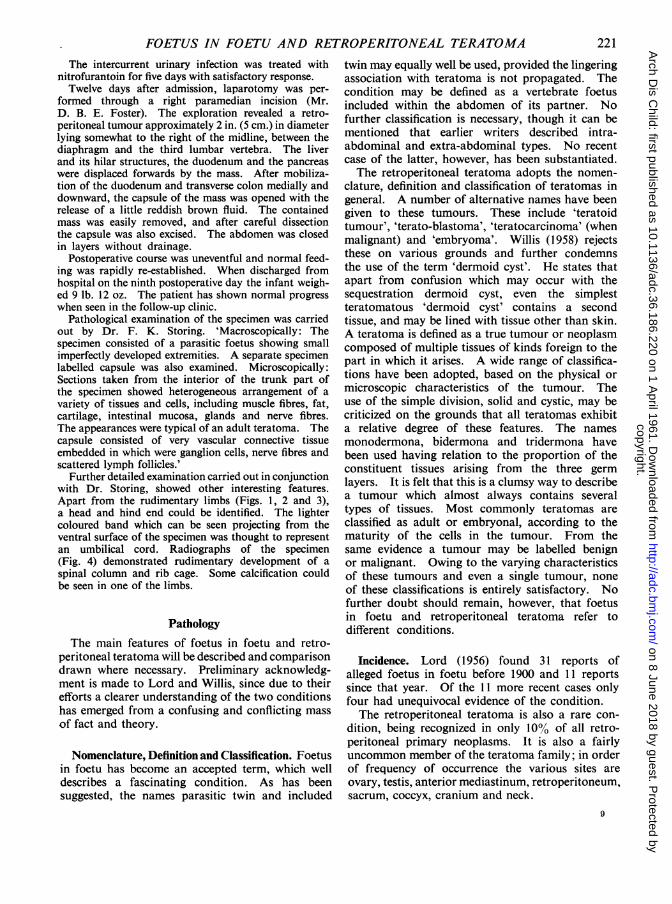
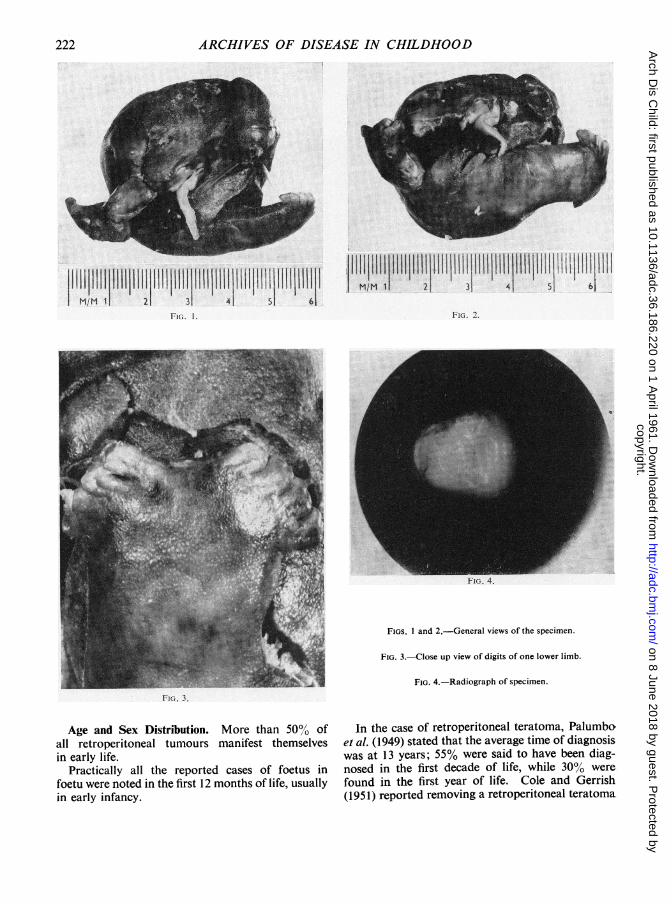
Further detailed examination carried out in conjunctionwith Dr. Storing, showed other interesting features.Apart from the rudimentary limbs (Figs. 1, 2 and 3),a head and hind end could be identified. The lightercoloured band which can be seen projecting from theventral surface of the specimen was thought to representan umbilical cord. Radiographs of the specimen(Fig. 4) demonstrated rudimentary development of aspinal column and rib cage. Some calcification couldbe seen in one of the limbs.
PathologyThe main features of foetus in foetu and retro-
peritoneal teratoma will be described and comparisondrawn where necessary. Preliminary acknowledg-ment is made to Lord and Willis, since due to theirefforts a clearer understanding of the two conditionshas emerged from a confusing and conflicting massof fact and theory.
Nomenclature, Definition and Classification. Foetusin foetu has become an accepted term, which welldescribes a fascinating condition. As has beensuggested. the names parasitic twin and included
twin may equally well be used, provided the lingeringassociation with teratoma is not propagated. Thecondition may be defined as a vertebrate foetusincluded within the abdomen of its partner. Nofurther classification is necessary, though it can bementioned that earlier writers described intra-abdominal and extra-abdominal types. No recentcase of the latter, however, has been substantiated.The retroperitoneal teratoma adopts the nomen-
clature, definition and classification of teratomas ingeneral. A number of alternative names have beengiven to these tumours. These include 'teratoidtumour', 'terato-blastoma', 'teratocarcinoma' (whenmalignant) and 'embryoma'. Willis (1958) rejectsthese on various grounds and further condemnsthe use of the term 'dermoid cyst'. He states thatapart from confusion which may occur with thesequestration dermoid cyst, even the simplestteratomatous 'dermoid cyst' contains a secondtissue, and may be lined with tissue other than skin.A teratoma is defined as a true tumour or neoplasmcomposed of multiple tissues of kinds foreign to thepart in which it arises. A wide range of classifica-tions have been adopted, based on the physical ormicroscopic characteristics of the tumour. Theuse of the simple division, solid and cystic, may becriticized on the grounds that all teratomas exhibita relative degree of these features. The namesmonodermona, bidermona and tridermona havebeen used having relation to the proportion of theconstituent tissues arising from the three germlayers. It is felt that this is a clumsy way to describea tumour which almost always contains severaltypes of tissues. Most commonly teratomas areclassified as adult or embryonal, according to thematurity of the cells in the tumour. From thesame evidence a tumour may be labelled benignor malignant. Owing to the varying characteristicsof these tumours and even a single tumour, noneof these classifications is entirely satisfactory. Nofurther doubt should remain, however, that foetusin foetu and retroperitoneal teratoma refer todifferent conditions.
Incidence. Lord (1956) found 31 reports ofalleged foetus in foetu before 1900 and 11 reportssince that year. Of the 11 more recent cases onlyfour had unequivocal evidence of the condition.The retroperitoneal teratoma is also a rare con-
dition, being recognized in only 10% of all retro-peritoneal primary neoplasms. It is also a fairlyuncommon member of the teratoma family; in orderof frequency of occurrence the various sites areovary, testis, anterior mediastinum, retroperitoneum,sacrum, coccyx, cranium and neck.
221copyright.
on 8 June 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.36.186.220 on 1 April 1961. D
ownloaded from
ARCHIVES OF DISEASE IN CHILDHOOD
11llllllllllllllllllllllllllllllllllllllllllllllll 1lll lilllllll l llllllll1 1llll II I IIII!IIM/M 1 2 3 4 5 6
FIG. 1. FIG. 2.
FIGS. I and 2.-General views of the specimen.
FIG. 3.-Close up view of digits of one lower limb.
FIG. 4.-Radiograph of specimen.
Fi(;. 3.
Age and Sex Distribution. More than 50%0 ofall retroperitoneal tumours manifest themselvesin early life.
Practically all the reported cases of foetus infoetu were noted in the first 12 months of life, usuallyin early infancy.
In the case of retroperitoneal teratoma, Palumboet al. (1949) stated that the average time of diagnosiswas at 13 years; 55% were said to have been diag-nosed in the first decade of life, while 30% werefound in the first year of life. Cole and Gerrish(1951) reported removing a retroperitoneal teratoma
222copyright.
on 8 June 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.36.186.220 on 1 April 1961. D
ownloaded from
FOETUS IN FOETU AND RETROPERITONEAL TERATOMA
15 hours after birth, while at the other extreme asimilar tumour has been removed from a patientaged 53 years.There is no indication of any particular sex
incidence in either condition. Gross and Clat-worthy (1951) made the observation that whilethe sex incidence in retroperitoneal teratoma isnearly equal, in sacrococcygeal teratomas there isa four to one preponderance toward occurrencein females.
Site of Occurrence. The upper part of the retro-peritoneal space is the only site of occurrence offoetus in foetu. No case has been reported in thepelvis or in any abdominal organ. Previouswriters have described the occurrence of foetalstructures within the brain, abdominal wall and theuterus. A particular case is that of Kimmel,Moyer, Peale, Winborne and Gotwals (1950). Inthis instance, there was a cerebral tumour allegedlycontaining five human foetuses. However, doubtexists whether these fully meet the requirements toclassify as included quintuplets, and discussionstill continues.The foetus in foetu is usually suspended by a
peduncle within a capsule containing a little fluid.The wall of the capsule is often thickened at thepoint of attachment of the peduncle with an asso-ciated plexus of vessels. The thickened part maybe orientated toward the base of the mesenteryand the origin of the superior mesenteric artery.No direct connexion of peduncular vessels withthose of the host has been shown, in the cases wherethis examination has been possible.The retroperitoneal teratoma also more commonly
occurs in the upper part of the retroperitoneal space.Arbitrarily dividing the space into left and rightcompartments, with the spinal column forming themedian boundaries, this type of teratoma is saidto occur twice as frequently on the left side. Mostare located in an immediate paramedian pre-axialposition.The retroperitoneal teratoma is typically without
a capsule or pedicle, and attachment to the posteriorabdominal wall is broad and intimate. The area ofattachment may be in close relation to the upperpole of the kidney, the pancreas or the coeliacaxis of vessels. Growth of the tumour maydisplace any related organ with resulting distortionof the anatomical situation.
Macroscopic and Microscopic Appearance. Theoutward appearance of the foetus in foetu may varyfrom an anencephalic globular or reniform mass,with rudimentary limb buds, through all stages of
development to the well-formed foetus. More thanone part of a foetus should always be recognizableand the suspending cord or peduncle should also beidentifiable.
Internally, a vertebral column at some stage ofdevelopment will be found, together with otherbones. A complete foetal skeleton may exist. Ofthe soft tissue structures, the intestinal tract is usuallybest represented. Various other organs may berecognizable including brain, spinal cord, lungs,gonads and adrenals. A rudimentary cardiovascularsystem may be present, but this is not functionaland the foetus is acardiac, deriving its blood supplyfrom its host. The enclosing capsule usually con-sists of connective tissue with a lining endotheliumwhich may be stratified squamous in type. Notrophoblastic or placental tissue has yet beendescribed in the capsule.The gross and histological features of the tera-
toma are well known. The tumour may reach avery large size and one weighing 26 lb. has beenreported. This is in contrast to the foetus in foetuwhich remains quite small. Occasionally a well-formed foetal part may be found within the teratoma,such as a single digit. An instance of this wasdescribed by Krug (1956). The formation of avertebral column and the occurrence of segmentationis unknown.
Microscopically, multiple different mature andimmature tissues will be observed, with no evidenceof organ-like arrangement. It is interesting, how-ever, that some tissue correlation does occur. Forexample, teeth may be set in bony sockets and mayeven erupt into cystic cavities, alimentary mucosamay be related to smooth muscle, and respiratorytissue to cartilage. In explanation, Willis (1958)suggests that contiguous tissues may exert an induc-tive effect on one another. In malignant teratomasabundant immature embryonic cells will be seen,having marked proliferative and invasive properties.
Growth and Malignancy. The foetus in foetu,commencing existence as a true twin, grows initiallyin parallel with its fellow. Soon, however, becauseof its anatomical confinement and perhaps someother factor which determined its parasitic role, itlags behind its host. From the latter it becomesdependent for its blood supply, and does notdevelop a functioning heart and circulation of itsown. Although the limbs of the included foetusmay appear to be well developed, their ratio totrunk is behind that of a similar age normal foetus.After attaining a variable size, further growth ceases,and actual retrogression can occur as the hosttwin progresses. Willis (1958) describes in detail
223
copyright. on 8 June 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.36.186.220 on 1 A
pril 1961. Dow
nloaded from
ARCHIVES OF DISEASE IN CHILDHOOD
how reduction of a parasitic twin may be broughtabout, with loss of head, limbs and internal organs.It is not, however, certain whether the factor in-volved is the vascular dominance of the host twin,or some inherent defect in its parasitic partnerwhich causes these changes. It thus becomesevident that the extensively reduced foetus may bedistinguishable only with difficulty from a teratoma.There is no evidence, however, to suggest that thefoetus in foetu can become anything but a quiescentmalformation, and therefore has no neoplastic ormalignant propensities.
Quite oppositely, the retroperitoneal teratoma ischaracterized by progressive growth. It probablyarises at an early stage in prenatal development andwill have been present for a long period beforediscovery in infancy, childhood or later life.Maturation of tissues in the tumour may continueapace with those of the host. In fact maturationmay become complete and the tumour becomequiescent. The presence, therefore, of relativelyimmature tissues in the tumour of a small infantmay not be a sign of malignancy. The observationof such cells or tissues in the teratoma of an adult,however, would have serious implications.Immediate recognition of malignancy may be
difficult. It is probable that more than the accepted10% of retroperitoneal teratomas are malignantat time of operation. Metastases are frequentand may occur in the lungs, liver and vertebrae.If the parent tumour is actively proliferating, forexample in a young patient, then the metastaseswill be composed of mixed cells and tissues. If,however, in an adult type tumour one elementbecomes malignant, then the metastases will be ofthis tissue.
Pathogenesis. The foetus in foetu is a monozygotictwin. Developing from a single ovum, it would,but for the limitations in growth which occur later,be of the same sex and closely resemble its host.It is not proposed to discuss the phenomenon oftwinning, apart from recalling the strong hereditarytendency, and noting that the membranes may beshared to a varying degree by the developingfoetuses. Early cleavage of the dividing cell massmay so occur that each may have its own chorion,or that this may be shared. It is then likely thateach foetus will have its own amniotic cavity.Occasionally the twin embryos appear at a laterstage and a common amniotic cavity is utilized.Willis (1958) states that most if not all conjoinedtwins and double monsters are in this group. Whileit would be possible to theorize that even latercleavage into twins might result in the inclusion
of the second embryo within the body layers of itspartner, there is no supporting evidence for this, andfor that matter no other reason for foetal inclusionhas been suggested.
In contrast to the foetus in foetu, very muchhas been written about the pathogenesis of the retro-peritoneal teratoma and teratomas in general. Manytheories have been put forward, both complex andconflicting. Most attempt to relate the develop-ment of a teratoma to some form or gradation oftwin development, or the parthogenetic stimulationof sex or dislocated germ cells. These views shouldnow be discarded. Teratomas should not beconsidered as incomplete or distorted foetuseswithin a host, nor the result of fertilization of anovum within a foetus or infant.Spemann (1938) first postulated that a 'primary
organizer' determined the orderly development andgrowth of embryonic tissues into the normal struc-ture of the human body. Askanazy (1908) hadalready indicated that teratomas must arise fromabnormal tissue primordia in early embryonic life,while Budde (1926) first suggested the theory thatteratomas result from disturbances in the primitivestreak. Needham (1936; 1942), Nicholson (1935)and especially Willis (1935; 1937; 1953) endorsed,expanded and nurtured the theory that teratomaswere derived from cells related to the invaginatingprimitive streak, which escaped organizer influence.
In summary, it may be concluded that the retro-peritoneal teratoma (or any teratoma) is congenital,and arises in a median or paramedian location fromembryonic pleuripotential cells associated with theprimitive streak. These cells, uninfluenced by theprimary organizer, form a true neoplasm, whichmay later exhibit benign or malignant character-istics.
Symptoms, Signs, Diagnosis and TreatmentFoetus in foetu and retroperitoneal teratoma may
present in essentially the same fashion. Certainvariations do occur and these will be indicated. Ina similar way diagnosis and treatment may beconsidered concurrently.
Symptoms and Signs. These are due to thepressure effects of the tumour, and while initiallyvague, become increasingly persistent as the tumourenlarges. This is especially so in the case of retro-peritoneal teratoma where pressure effects tend to bemore severe.The infant may present with feeding difficulties,
vomiting, constipation, weight loss, dyspnoea andpain. Alternatively, abdominal distension with anaccompanying abdominal mass may be noticed first.
224
copyright. on 8 June 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.36.186.220 on 1 A
pril 1961. Dow
nloaded from
FOETUS IN FOETU AND RETROPERITONEAL TERATOMA 225
This is more likely to be the case in older patientshaving a retroperitoneal teratoma. The mass isusually circumscribed, sometimes mobile and mayfeel lobulated or cystic. Dilated veins may be seenbeneath the skin of the abdominal wall and theextremities may exhibit secondary oedema. Sepsisin, or avascular necrosis of, a foetus in foetu maycause rapid increase in size of the tumour, withpyrexia and possibly signs of peritoneal irritation.
Diagnosis. By a process of elimination thepresence of a retroperitoneal tumour may bededuced and indeed it may be possible to specifyfoetus in foetu, or teratoma.
In infants, other conditions will require urgentexclusion. These include intussusception, Wilms'tumour and neuroblastoma. In older patientsextensive investigation may be required to excludegastrointestinal tract, pancreatic and renal tractlesions. Secondary abdominal lymph node depositsfrom a malignant testicular tumour may give rise toan abdominal mass, 'the epigastric tumour ofOsler'. An associated pyrexia may influence thediagnosis toward a malignant tumour, primaryretroperitoneal or otherwise, except in the circum-stances already mentioned.
Plain radiographs of the abdomen may provideconclusive evidence. Apart from the position ofthe soft tissue mass on postero-anterior films andlateral films, and indentation or displacement ofgas shadows, irregular calcification or actual bonesmay be seen. The presence of a formed foetalskeleton, or bones with vertebrate organizationis strongly in favour of a foetus in foetu. It must beremembered, however, that calcification may occurin other degenerating tumours. Barium studies ofthe upper and lower intestinal tract may be necessaryif the diagnosis is in doubt. An excretory pyelo-gram will serve to exclude a renal lesion. Normallyfunctioning kidneys may be outlined, but the closeproximity of a retroperitoneal tumour may causeone or the other kidney to be displaced forwardand laterally.
Treatment. Surgical removal of the tumourshould be carried out without undue delay. Coleand Gerrish (1951) commented that nothing was tobe gained in small infants by procrastination, andreiterated that as time goes on the newborn infantbecomes a poorer surgical risk.
If the diagnosis is reasonably certain, however,the removal of a foetus in foetu does not normallycall for such urgency. In the absence of infectivecomplications, which might induce peritonitis ora local adhesive reaction, a reasonable time for
investigation and preparation may be taken.Depending on the age and condition of the patientand the anatomical relations of the tumour, it maybe considered advisable to remove the foetus only,from within its sac.On the other hand, the potentially malignant
nature of a teratoma, and of other similarly situatedtumours when the diagnosis is doubtful, calls forearly operation. The patient and surgeon shouldbe prepared for a lengthy and difficult procedure.Complete removal of all the abnormal tissue mustbe aimed at; otherwise local recurrence with possiblesubsequent malignant degeneration can occur.Preoperative preparation should include a chestradiograph and skeletal films, since distant meta-stases may have occurred already. Lord (1954)in her review of previous cases of foetus in foetu,observed that the prognosis was far better in thiscondition, than in teratoma, with or withoutsurgical intervention.
ConclusionAn attempt has been made to separate the charac-
teristics of two interesting conditions, often con-fused in the past. A further illustrative case hasbeen described, which in the author's opinion wasprobably a foetus in foetu. Certain contradictionsin the pathological description are evident. Theinternal histology of the specimen was manifestlyteratomatous. Yet could this represent all thatremained of the interior of a markedly reducedfoetus? It is suggested that it may still be difficultto identify correctly borderline instances of theseconditions, unless very minute and painstakingexamination of the fresh specimen is carried out.
The author wishes to thank Professor A. G. Watkins,Department of Child Health, Cardiff, and Mr. D. B. E.Foster for permission to publish details of the casehistory; and Dr. F. K. Storing, Llandough Hospital,Cardiff, for his assistance.
REFERENCES
Askanazy, M. (1908). Die Teratome nach ihrem Bau, ihrem Verlauf,ihrer Genese und im Vergleich zum experimentellen Teratoid.Verh. dtsch. path. Ges., (1907), 11, 39.
Budde, M. (1926). UJber die Genese der Fetalinklusionen. Beitr.path. Anat., 75, 357.
Charles, D. (1953). Retroperitoneal teratoma in infancy. Arch.Dis. Childh., 28, 147.
Cole, J. W. and Gerrish, E. W. (1951). Removal of a primarylateral retroperitoneal teratoma with survival in a fifteen-hour-oldinfant. Surgery, 30, 371.
Dickinson, W. H. (1871). Mesenteric tumour. Trans. path. Soc.Lond., 22, 296.
Gross, R. E. and Clatworthy, H. W., Jr. (1951). Twin fetuses infetu. J. Pediat., 38, 502.
Kimmel, D. L., Moyer, E. K., Peale, A. R., Winborne, L. W., andGotwals, J. E. (1950). A cerebral tumor containing fivehuman fetuses; a case of fetus in fetu. Anat. Rec., 106, 141.
Krug, G. (1956). Ein Beitrag zu den Teratomen des Retroperitoneal-raumes. Zbl. Chir., 81, 2454.
copyright. on 8 June 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.36.186.220 on 1 A
pril 1961. Dow
nloaded from

226 ARCHIVES OF DISEASE IN CHILDHOODLord, J. M. (1954). Intra-abdominal foetus in foetu-2 cases.
Proc. roy. Soc. Med., 47, 684.- (1956). Intra-abdominal foetus in foetu. J. Path. Bact.,
72, 627.Needham, J. (1936). New advances in the chemistry and biology of
organized growth. Proc. roy. Soc. Med., 29, 1577.-(1942). Biochemistry and Morphogenesis. Cambridge Univer-
sity Press, London.Nicholson, G. W. (1935). Studies on tumour formation-An
abdominal foetiform teratoma. Guy's Hosp. Rep., 85, 379.
Palumbo, L. T., Cross, K. R., Smith. A. N. and Baronas, A. A. (1949).Primary teratomas of the lateral retroperitoneal spaces. Surgery,26, 149.
Spemann, H. (1938). Embryonic Development and Induction.Oxford University Press, London.
Willis, R. A. (1935). The structure of teratoma. J. Path. Bact.,40, 1.
- (1937). A further study of the structure of teratomata. Ibid.,45, 49.(1953). Pathology of Tumours, 2nd ed. Butterworth, London.(1958). The Borderland of Embryology and Pathology. Butter-worth, London.
copyright. on 8 June 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.36.186.220 on 1 A
pril 1961. Dow
nloaded from