Embed Size (px)
Citation preview
Arch. Dis. Childh., 1963, 38, 151.
EXPERIENCE AT HAMMERSMITH HOSPITALWITH CARDIOPULMONARY BY-PASS OPERATIONS
IN CHILDREN*BY
BLANCA SMITHtFrom the Cardio-Thoracic Unit of the Department of Surgery, Postgraduate Medical School ofLondon
During the five-year period July 1957 to June 1962,229 children with cardiac anomalies underwentsurgical correction aided by cardiopulmonary by-pass in the Cardio-Thoracic Unit of the Hammer-smith Hospital. This report includes only patientsup to 14 years of age, and outlines the diagnostic andpre-operative measures as well as the surgical andperfusion techniques used. Details of the post-operative management and the results are alsodiscussed.
DiagnosisChildren with suspected cardiac malformations
are in the first instance referred to the CardiologyDepartment and subsequently admitted for completeinvestigation. The following tests are conductedroutinely in addition to a thorough physical exami-nation: chest radiographs, electro- and phono-cardiograms, ear oximetry and right heart cathe-terization. The angiographic techniques are carriedout in conjunction with the Department ofDiagnosticRadiology.Great care is taken to assess the degree of pul-
monary vascular disease suggested by the physicalfindings. For confirmation the pulmonary arteryresistance is measured at catheterization taking intoaccount the response to acetylcholine vasodilatation.The pulmonary vessels are examined further byselective angiography and wedge arteriograms withinjection of contrast medium into a segmentalpulmonary vessel.
Selective right or left angiocardiography is carriedout in the majority of patients with intracardiacpathology, except those with an uncomplicatedatrial septal defect of the secundum type. Duringright heart catheterization, the left side of theheart is almost invariably entered should an atrial
* A paper read at a meeting of the British Association of PaediatricSurgeons in London, September 1962.
t Present address: Assistant Professor, Department of Surgery,Ohio State University and The Children's Hospital, Columbus,Ohio, U.S.A.
septal defect exist. For assessment of aortic andmitral incompetence, however, retrograde techniquesare preferred. An accompanying patent ductusarteriosus is always borne in mind, and if suspectedit is sought for on a retrograde aortogram. Trans-septal catheterizations are reserved for measurementof aortic gradients and left ventricular angiocardio-graphy. It is usually possible to perform thesediagnostic procedures under sedation and localanaesthesia only.When the investigations are completed the patient
with the pertinent diagnostic data is presented to theweekly Joint Cardiac Clinic of the Surgical andMedical Staff, and the future management is dis-cussed. The decision to defer surgery until a laterdate, to operate in the near future or not to operateat all is entered in the patient's records.
In those patients in whom operation is deferred,further dates for reassessment are booked. Amongstthese are, for example, symptomless children under6 years of age, with a small ventricular septal defect,normal pulmonary resistance and ratio of pul-monary to systemic circulation less than I 5 to 1.Surgery is also deferred in asymptomatic patientswith minimal pulmonary or aortic stenosis withoutevidence of hypertrophy of the respective ventricles.In these cases surgery will be advised if at futurerevisions symptoms are found to have developed,or clinical proof of progressive pathology becomesevident.The presence of a pulmonary vascular resistance
over five units would make surgery for an atrialseptal defect inadvisable. Fortunately this situationis uncommon in childhood. A ventricular septaldefect is placed among the inoperable group onlywhen the shunt has balanced or reversed and thehigh pulmonary resistance cannot be lowered byacetylcholine-induced vasodilatation. But whilesome degree of left-to-right shunting is still present,closure of the defect will be undertaken in spite ofthe pulmonary hypertension. The risks are there-fore proportionally higher. Complete correction of
151
on 16 June 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.198.151 on 1 April 1963. D
ownloaded from

ARCHIVES OF DISEASE IN CHILDHOOD
a Fallot's tetralogy is normally carried out in onestage. Marked hypoplasia of the pulmonary artery,however, contraindicates the one-stage repair.In these cases closure of the ventricular septal defectwould be preceded by a transventricular relief of thepulmonary outflow obstruction. An increase inthe calibre of the pulmonary artery is expected tofollow. Occasionally a proximal pulmonary atresiawith good calibre of the right pulmonary arterydistally, makes the candidate suitable for a Glenn(1958) type of anastomosis. Tricuspid atresia isanother indication for this right pulmonary arterysuperior vena cava shunt. In anomalies carryingan almost prohibitive surgical risk such as completeA-V canal, double outlet right ventricle and singleventricle, surgery is considered only if the severityof the symptoms justifies it.
If the patient is accepted for surgery the relativeurgency of the operation is discussed, and a prioritycode number is assigned to each case on the waitinglist, guaranteeing that top priority cases are calledin for surgery as soon as possible.During this admission a search is made to rule
out the presence of sources of infection in tonsils,ears or urinary tract. The condition of the teethis determined and any necessary dental extractionsare done under antibiotic cover, either then, orseveral weeks at least before readmission for cardiacsurgery. Before discharge the Blood TransfusionDepartment performs routine blood grouping anddetailed screening for antibodies.
Pre-operative MeasuresThe child is readmitted as a surgical patient four
to five days before the scheduled date of operation.Chest radiograph, ear oximetry and electro- andphonocardiograms are repeated. The patient isvisited by the medical staff, and his case may bediscussed again at the Joint Cardiac Clinic if therehave been any important developments since hisoriginal evaluation.A full blood picture is obtained as well as deter-
mination of blood urea and electrolytes. Thefollowing screening tests to rule out any bleedingtendencies or coagulation defects are conductedin all patients, i.e. recalcification time, one-stageQuick's prothrombin time, platelet count andHick's modification of the thromboplastin genera-tion test. If any abnormalities are detected, addi-tional tests specific for the defect suspected arecarried out. In some of the severely cyanoticchildren with haematocrit levels over 70 %, attemptsare made to lower them by repeated exchange trans-fusions of plasma. Not more than 15 % of theblood volume is exchanged at any one time.
During the intervening days before operation adefinite effort is made to help the child to getacquainted with the routines, and the medical andnursing personnel. Practice sessions in respiratoryexercises are conducted twice daily in the ward bythe same physiotherapist who will take charge of thechild after operation. New patients and con-valescents frequently join in.- An old oxygen tentis available in the playroom for the children tobecome familiar with its appearance. As far aspossible the child's doubts about being anaesthe-tized are dispelled by a visit from the anaesthetistwho explains in simple language what the childshould expect. The Sister in charge of the RecoveryWard also visits so that her face will be familiarwhen the child wakes in the new surroundings ofthe Recovery Ward. Recent body weight, heightand surface area are among the essential data inthe case notes that accompany the patient to thetheatre. Details of the anaesthetic techniquesemployed at the present time are given by Beard(1963).
Surgical and Perfusion TechniquesBeing so closely related, they will be commented
upon in the approximate order in which they takeplace.The arterial pressure is monitored continuously
through a catheter in the radial artery, usually theleft. Catheters, passed via one of the externaljugular veins into the superior vena cava and viathe left saphenous vein into the inferior vena cava,are used to monitor the central venous pressure.Electrocardiogram and electro-encephalogram trac-ings are visible on the oscilloscopic screen and canbe recorded when required. Oesophageal andrectal temperatures are measured by electric ther-mometers.The skin from the' neck to mid thigh is covered
with a piece of thin plastic film (Vi-Drape) which ismade to adhere with a 'spray-cement' (Vi-Adherent).This gives a large sterile field, impermeable tomoisture for the duration of the procedure. Thesternum is split vertically, after exposure througha vertical skin incision in boys, and a low lyingtransverse incision in girls. Entry into eitherpleural cavity is avoided. Inspection of the heartto determine the size of the chambers and calibreof the great vessels follows. Atrial and ventricularpressures are measured and recorded as are PA oraortic pressures where relevant. Digital explorationof the right atrium may be carried out at this stage.The absence of a patent ductus or anomaly of thevenous drainage is also ascertained. Earlier in theseries unsuspected patent ductus arteriosus made
152
on 16 June 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.198.151 on 1 April 1963. D
ownloaded from
CARDIOPULMONARY BY-PASS OPERATIONS
perfusion impossible in three patients. If thepatient has tetralogy of Fallot with a previousshunt of the Blalock-Taussig type, access is gainedto the site of the anastomosis by dissecting over thearch of the aorta until the origin of the subclavianartery is reached. A ligature is placed around it,which is tied just before by-pass is begun.The Melrose NEP disc oxygenator has been used
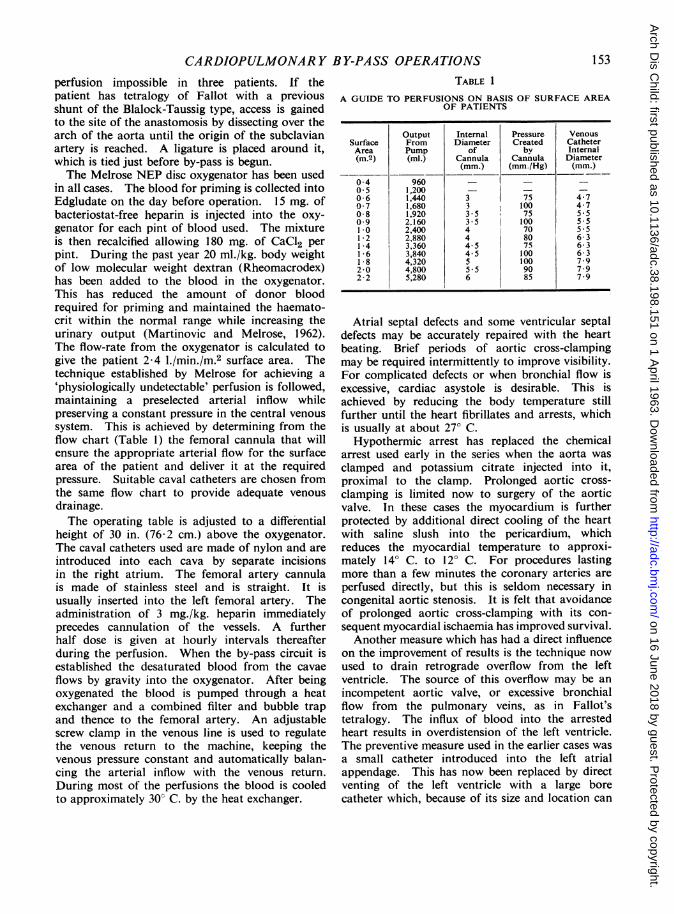
in all cases. The blood for priming is collected intoEdgludate on the day before operation. 15 mg. ofbacteriostat-free heparin is injected into the oxy-genator for each pint of blood used. The mixtureis then recalcified allowing 180 mg. of CaC12 perpint. During the past year 20 ml./kg. body weightof low molecular weight dextran (Rheomacrodex)has been added to the blood in the oxygenator.This has reduced the amount of donor bloodrequired for priming and maintained the haemato-crit within the normal range while increasing theurinary output (Martinovic and Melrose, 1962).The flow-rate from the oxygenator is calculated togive the patient 2-4 l./min./m.2 surface area. Thetechnique established by Melrose for achieving a'physiologically undetectable' perfusion is followed,maintaining a preselected arterial inflow whilepreserving a constant pressure in the central venoussystem. This is achieved by determining from theflow chart (Table 1) the femoral cannula that willensure the appropriate arterial flow for the surfacearea of the patient and deliver it at the requiredpressure. Suitable caval catheters are chosen fromthe same flow chart to provide adequate venousdrainage.The operating table is adjusted to a differential
height of 30 in. (76-2 cm.) above the oxygenator.The caval catheters used are made of nylon and areintroduced into each cava by separate incisionsin the right atrium. The femoral artery cannulais made of stainless steel and is straight. It isusually inserted into the left femoral artery. Theadministration of 3 mg./kg. heparin immediatelyprecedes cannulation of the vessels. A furtherhalf dose is given at hourly intervals thereafterduring the perfusion. When the by-pass circuit isestablished the desaturated blood from the cavaeflows by gravity into the oxygenator. After beingoxygenated the blood is pumped through a heatexchanger and a combined filter and bubble trapand thence to the femoral artery. An adjustablescrew clamp in the venous line is used to regulatethe venous return to the machine, keeping thevenous pressure constant and automatically balan-cing the arterial inflow with the venous return.During most of the perfusions the blood is cooledto approximately 30° C. by the heat exchanger.
TABLE 1
A GUIDE TO PERFUSIONS ON BASIS OF SURFACE AREAOF PATIENTS
Output Internal Pressure VenousSurface From Diameter Created CatheterArea Pump of by Internal(m.2) (ml.) Cannula Cannula Diameter
(mm.) (mm./Hg) (mm.)
04 960 _ -0-5 1,200 - -
0-6 1,440 3 75 4-70 7 1,680 3 100 4-70-8 1,920 3-5 75 5 509 2.160 35 100 551.0 2,400 4 70 5-512 2,880 4 80 6-31*4 3,360 4 5 75 6-31-6 3,840 4-5 100 6-31*8 4,320 5 100 7*92-0 4,800 5-5 90 7 92-2 5,280 6 85 7-9
Atrial septal defects and some ventricular septaldefects may be accurately repaired with the heartbeating. Brief periods of aortic cross-clampingmay be required intermittently to improve visibility.For complicated defects or when bronchial flow isexcessive, cardiac asystole is desirable. This isachieved by reducing the body temperature stillfurther until the heart fibrillates and arrests, whichis usually at about 27° C.Hypothermic arrest has replaced the chemical
arrest used early in the series when the aorta wasclamped and potassium citrate injected into it,proximal to the clamp. Prolonged aortic cross-clamping is limited now to surgery of the aorticvalve. In these cases the myocardium is furtherprotected by additional direct cooling of the heartwith saline slush into the pericardium, whichreduces the myocardial temperature to approxi-mately 14° C. to 120 C. For procedures lastingmore than a few minutes the coronary arteries areperfused directly, but this is seldom necessary incongenital aortic stenosis. It is felt that avoidanceof prolonged aortic cross-clamping with its con-sequent myocardial ischaemia has improved survival.Another measure which has had a direct influence
on the improvement of results is the technique nowused to drain retrograde overflow from the leftventricle. The source of this overflow may be anincompetent aortic valve, or excessive bronchialflow from the pulmonary veins, as in Fallot'stetralogy. The influx of blood into the arrestedheart results in overdistension of the left ventricle.The preventive measure used in the earlier cases wasa small catheter introduced into the left atrialappendage. This has now been replaced by directventing of the left ventricle with a large borecatheter which, because of its size and location can
153
on 16 June 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.198.151 on 1 April 1963. D
ownloaded from
ARCHIVES OF DISEASE IN CHILDHOOD
more adequately fulfil the purpose (El Sayed,Bentall and Melrose, 1962).The left ventricular vent is inserted while the
patient is in partial perfusion and cooling is pro-
ceeding, before the heart is arrested. The correctivepart of the operation follows. Ventricular septaldefects and pulmonary infundibular stenosis are
corrected through a right ventriculotomy approach.The incision may be either vertical or transverse, as
the anatomy of the coronary branches indicates.Septal defects are closed directly by sutures wherepossible or by a patch. In the early cases thematerial used for the patch was compressed'ivalon' sponge. This has been replaced by 'teflon'felt. Pulmonary infundibular stenosis is now
corrected by extensive infundibulectomy and releaseof tight trabeculae carnea, inserting outflow tractpatches only when essential. The material usedfor the patch may be 'teflon' felt or pericardium, andextension across the pulmonary valve is avoidedas much as possible. Pulmonary and aorticvalvotomies are done under direct vision afterexposing the valve through the incised vessel wall.When a patch is used for repair of an atrial septal
defect with associated cleft mitral valve (AV canal),the left atrial side of the patch is covered with a
piece of pericardium. This prophylactic manoeuvrehas been in use since two adult patients developedhaemolytic anaemia following repair of an atrio-ventricular canal (Sayed, Dacie, Handley, Lewis andCleland, 1961). It was thought that the patchwas being exposed to a regurgitant jet of blood fromresidual mitral regurgitation, the trauma con-
tributing to the haemolysis. The left atrial sideof the patch was covered with pericardium at a
second operation effecting dramatic cure of thehaemolysis.When the corrective part of the operation is near
completion, rewarming of the patient is begun.Meanwhile, the cardiotomy or arteriotomy is closed.When hypothermic arrest has been used, spon-
taneous defibrillation usually occurs on rewarming.If it does not, defibrillation is generally achievedwith a single shock of approximately 200 volts.The voltage is chosen according to the size of thechild. With a regular rhythm restored, the hearttakes over and perfusion is gradually slowed downand stopped. Diagnostic pressures are repeatedand if they are satisfactory the cannulae are removed.If there is atrial ventricular dissociation, pacemakerwires are inserted into the myocardium.The heparin is neutralized with protamine sulphate
(6 mg./kg. body weight). This drug is preferredas no appreciable decrease in post-operative bleedingwas noted in the 50 cases who received hexadi-
methrine bromide. The parallel between bleedingand abnormalities in clotting tests detected in 400perfusions at Hammersmith Hospital will be thesubject of a separate report. Careful attention ispaid to haemostasis, and the chest is closed onlyafter the surgeon is completely satisfied that theblood loss is under control. This attitude hasgreatly reduced the incidence of continued bleeding,necessitating re-exploration. The pericardium isonly loosely approximated. Several large borecatheters connected to suction are used to drainthe mediastinum, the pericardium, and the pleuraif it has been opened. In patients with high pul-monary vascular resistance, elective tracheostomymay be performed at the conclusion of the operation.The patient is no longer weighed before and afterperfusion as, using the described technique forperfusion management, the patient's blood volumeis expected to be the same at the end of by-pass asit was at the beginning. All blood loss occurringduring the chest closure is replaced before leavingthe theatre and the chest tubes are clamped whilethe patient is taken to the recovery ward.
Post-operative ManagementThis is carried out in a recovery ward suitably
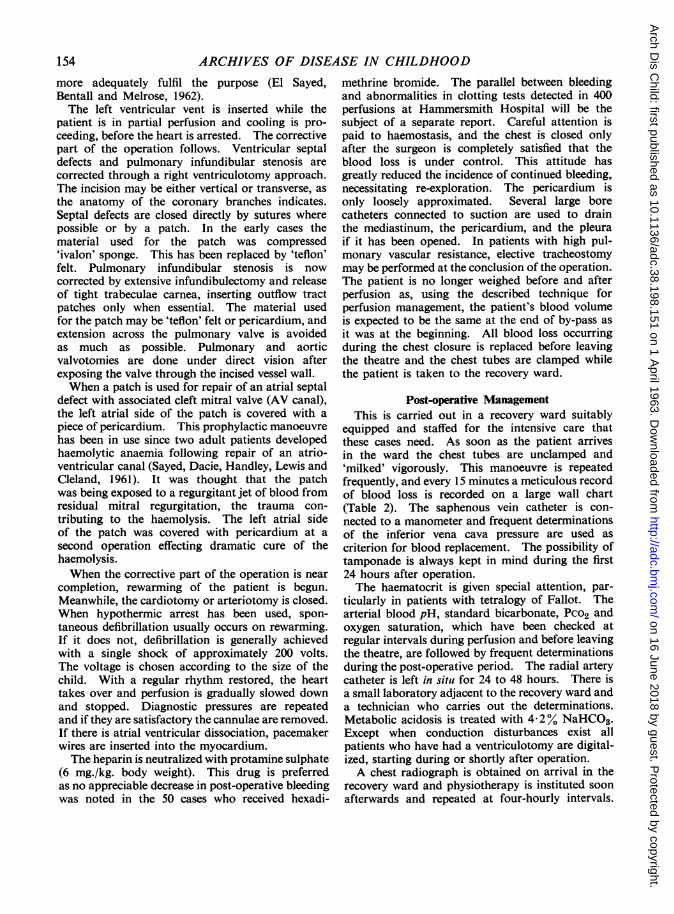
equipped and staffed for the intensive care thatthese cases need. As soon as the patient arrivesin the ward the chest tubes are unclamped and'milked' vigorously. This manoeuvre is repeatedfrequently, and every 15 minutes a meticulous recordof blood loss is recorded on a large wall chart(Table 2). The saphenous vein catheter is con-nected to a manometer and frequent determinationsof the inferior vena cava pressure are used ascriterion for blood replacement. The possibility oftamponade is always kept in mind during the first24 hours after operation.The haematocrit is given special attention, par-
ticularly in patients with tetralogy of Fallot. Thearterial blood pH, standard bicarbonate, Pco2 andoxygen saturation, which have been checked atregular intervals during perfusion and before leavingthe theatre, are followed by frequent determinationsduring the post-operative period. The radial arterycatheter is left in situ for 24 to 48 hours. There isa small laboratory adjacent to the recovery ward anda technician who carries out the determinations.Metabolic acidosis is treated with 4-2y% NaHCO3.Except when conduction disturbances exist allpatients who have had a ventriculotomy are digital-ized, starting during or shortly after operation.A chest radiograph is obtained on arrival in the
recovery ward and physiotherapy is instituted soonafterwards and repeated at four-hourly intervals.
154
on 16 June 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.198.151 on 1 April 1963. D
ownloaded from
CARDIOPULMONARY BY-PASS
I~~~~~~~~~~~ I0;I"C) 0s c
* C "
l l | A " | 5I lU
oIo
I 7HolI | t |
3=o"
I
:0
I<i X
.-
3so
XIGo
Ur000
r
z0m
rc-C
r30-z
m
AAC3c
r
4m
-I
r
m
Im
m
5a-IIm
-Im
.3
0
(A
m
3
a.
2!cr
oq
_..13 o
I0
3
s
11 >
? mOHlI pC
I
A
I0
z
I)
I C
0 =
_.0
3a
n :iO :r" 03.0
0w.0CI.-
3ff
U
00
m
-4n
zm
-I
0r0a
ac
2
OPERATIONS
V o'~z* ZV
* 3_3
3
It
so
0;;. oU
CsI
Ca-
0x
oe04
o>"Eq
t
n <SOEqq*
.3m
In
c
0IIz0t
n-. 0~~., 0
0 -1 0~-1
I I I_
!I 11 1 ! I0.Ic00
B. "2 I
a.02
a
(A
Im
0
0
-1L
w
a
(0Cx
m
5
0(A)
cma
m
z
m
(A
I-
axac
ImIm0
I-
0
I-
0z0
0
0
(A
m
I50-g
155
C)
'o>
IU,
00rn
I ;
CA0
tI
Om
zo
zH
U)
0
rn0
z0nmx
rirn
III
I--- 11 11
- -11' 11 .-
11
..~~
CA
a,
on 16 June 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.198.151 on 1 April 1963. D
ownloaded from
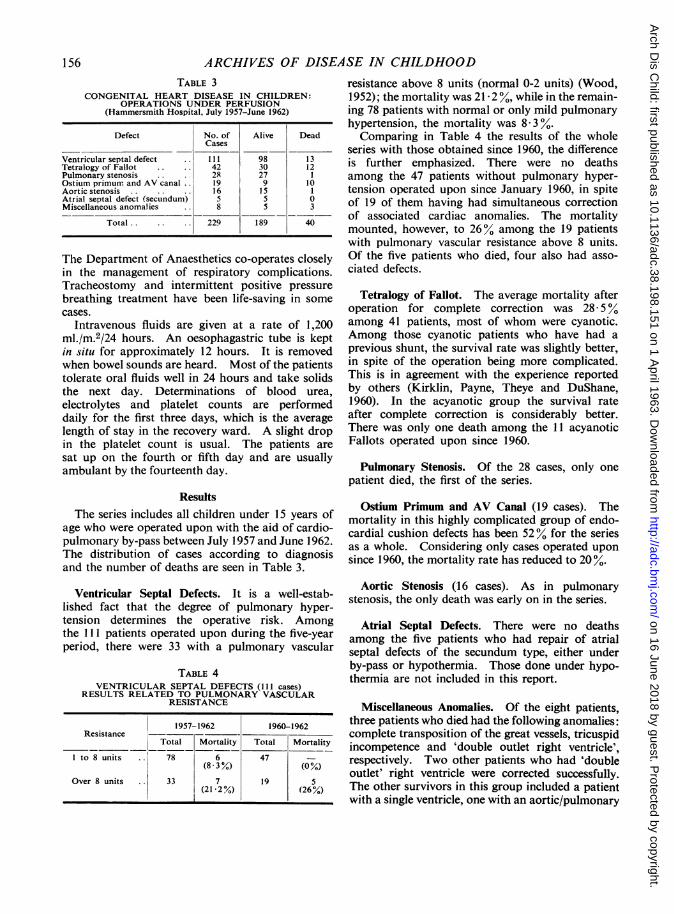
ARCHIVES OF DISEASE IN CHILDHOODTABLE 3
CONGENITAL HEART DISEASE IN CHILDREN:OPERATIONS UNDER PERFUSION
(Hammersmith Hospital, July 1957-June 1962)
Defect No. of Alive DeadCases
Ventricular septal defect 111 98 13Tetralogy of Fallot 42 30 12Pulmonary stenosis 2R 27Ostium primum and AV canal 19 9 10Aortic stenosis. 16 1 5 1Atrial septal defect (secundum) 5 5 0Miscellaneous anomalies 8 5 3
Total . . 229 189 40
The Department of Anaesthetics co-operates closelyin the management of respiratory complications.Tracheostomy and intermittent positive pressurebreathing treatment have been life-saving in somecases.
Intravenous fluids are given at a rate of 1,200ml./m.2/24 hours. An oesophagastric tube is keptin situ for approximately 12 hours. It is removedwhen bowel sounds are heard. Most of the patientstolerate oral fluids well in 24 hours and take solidsthe next day. Determinations of blood urea,electrolytes and platelet counts are performeddaily for the first three days, which is the averagelength of stay in the recovery ward. A slight dropin the platelet count is usual. The patients aresat up on the fourth or fifth day and are usuallyambulant by the fourteenth day.
ResultsThe series includes all children under 15 years of
age who were operated upon with the aid of cardio-pulmonary by-pass between July 1957 and June 1962.The distribution of cases according to diagnosisand the number of deaths are seen in Table 3.
Ventricular Septal Defects. It is a well-estab-lished fact that the degree of pulmonary hyper-tension determines the operative risk. Amongthe Ill patients operated upon during the five-yearperiod, there were 33 with a pulmonary vascular
TABLE 4VENTRICULAR SEPTAL DEFECTS (111 cases)
RESULTS RELATED TO PULMONARY VASCULARRESISTANCE
1957-1962 1960-1962Resistance
Total Mortality Total Mortality
I to 8 units .. 78 6 47 -(833%) (0%)
Over 8 units 33 7 19 5(21-2%) (26%)
resistance above 8 units (normal 0-2 units) (Wood,1952); the mortality was 21- 2 , while in the remain-ing 78 patients with normal or only mild pulmonaryhypertension, the mortality was 8-3%.Comparing in Table 4 the results of the whole
series with those obtained since 1960, the differenceis further emphasized. There were no deathsamong the 47 patients without pulmonary hyper-tension operated upon since January 1960, in spiteof 19 of them having had simultaneous correctionof associated cardiac anomalies. The mortalitymounted, however, to 260% among the 19 patientswith pulmonary vascular resistance above 8 units.Of the five patients who died, four also had asso-ciated defects.
Tetralogy of Fallot. The average mortality afteroperation for complete correction was 28-500among 41 patients, most of whom were cyanotic.Among those cyanotic patients who have had aprevious shunt, the survival rate was slightly better,in spite of the operation being more complicated.This is in agreement with the experience reportedby others (Kirklin, Payne, Theye and DuShane,1960). In the acyanotic group the survival rateafter complete correction is considerably better.There was only one death among the 11 acyanoticFallots operated upon since 1960.
Pulmonary Stenosis. Of the 28 cases, only onepatient died, the first of the series.
Ostium Primum and AV Canal (19 cases). Themortality in this highly complicated group of endo-cardial cushion defects has been 52% for the seriesas a whole. Considering only cases operated uponsince 1960, the mortality rate has reduced to 20 %.
Aortic Stenosis (16 cases). As in pulmonarystenosis, the only death was early on in the series.
Atrial Septal Defects. There were no deathsamong the five patients who had repair of atrialseptal defects of the secundum type, either underby-pass or hypothermia. Those done under hypo-thermia are not included in this report.
Miscellaneous Anomalies. Of the eight patients,three patients who died had the following anomalies:complete transposition of the great vessels, tricuspidincompetence and 'double outlet right ventricle',respectively. Two other patients who had 'doubleoutlet' right ventricle were corrected successfully.The other survivors in this group included a patientwith a single ventricle, one with an aortic/pulmonary
156
on 16 June 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.198.151 on 1 April 1963. D
ownloaded from

CARDIOPULMONARY BY-PASS OPERATIONS 157window and a child with absent aortic arch in whoma 'teflon' graft was inserted under left heart by-pass.
Summary
The diagnostic, surgical and perfusion techniquesused at present in Hammersmith Hospital have beendiscussed. The report is confined to children under15 years of age, who were operated upon with theaid of cardiopulmonary by-pass between July 1957and June 1962.The changes that have been introduced since the
techniques previously reported from this Unit(Cleland, Beard, Bentall, Bishop, Baimbridge,Bromley, Goodwin, Hollman, Kerr, Lloyd-Jones,Melrose and Telivuo, 1958) have been stressed.The results obtained during the past two years
are compared with those in the earlier part of theseries.
Grateful acknowledgement is given to Dr. J. F.Goodwin, Dr. A. Hollman, and the Department ofMedicine; to Professor R. E. Steiner and the Department
of Diagnostic Radiology; to Dr. A. J. W. Beard, Dr.E. B. Lloyd-Jones, Dr. M. K. Sykes and the Departmentof Anaesthetics and to the Department of Surgery,particularly to Mr. W. P. Cleland, Mr. H. H. Bentalland Dr. D. G. Melrose, whose patients are the subjectof this report.
REFFRENCESBeard, A. J. W. (1963). In Thoracic Anaesthesia, ed. W. Mushin.
Blackwell, Oxford.Cleland, W. P., Beard, A. J. W., Bentall, H. H., Bishop, M. B.,
Baimbridge, M. V., Bromley, L. L., Goodwin, J. F., Holiman, A.,Kerr, W. F., Lloyd-Jones, E. B., Melrose, D. G. and Telivuo,L. J. (1958). The treatment of ventricular septal defect. Brit.med. J., 2, 1369.
El Sayed, H., Bentall, H. and Melrose, D. (1962). The tetralogy ofFallot. A new approach to complete correction. Lancer,1, 549.
Glenn, W. W. L. (1958). Circulatory bypass of the right side of theheart. IV. Shunt between superior vena cava and distal rightpulmonary artery. Report of clinical application. New Engl.J. Med., 259, 117.
Kirklin. J. W., Payne, W. Spencer, Theye, R. A. and DuShane,J. W. (1960). Factors affecting survival after open operationfor tetralogy of Fallot. Ann. Surg., 152, 485.
Martinovic, N. and Melrose, D. G. (1962). The use of low molecularweight dextran in extracorporeal circulation. Reported at theEuropean Cardiovascular Congress, Stockholm.
Sayed, H. M., Dacie, J. V., Handley, D. A., Lewis, S. M. and Cleland,W. P. (1961). Haemolytic anaemia of mechanical origin afteropen heart surgery. Thorax, 16, 356.
Wood, P. (1952). Pulmonary hypertension. Brit. med. Bull.,8, 348.
on 16 June 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.198.151 on 1 April 1963. D
ownloaded from





























