Embed Size (px)
Citation preview
134 Vas Dias, McKenzie
threatening for both the uptake and carryingthrough of treatment. The waiting area accom-modates adults and children for other clinics.Perhaps this allows the psychotherapist to beseen as part of a team and removes some of themystique and stigma often associated withreferral for treatment of emotional or be-havioural problems.A very reasonable criticism of psychotherapy
is that treatment is frequent and lengthy. Theexperience in the clinic suggests that there are anumber of children who may benefit from shortterm treatment, thus making it available tomore children. Psychotherapy does not lenditself easily to clinical trials. It would be difficultto compare this model with other approaches todiscover whether it is as effective in terms ofthroughput and outcome. The only outcomedescribed here is the resolution of referralsymptoms at the time of discharge and werecognise that this has not been evaluated
objectively. Nevertheless this parallel servicewould seem to address some of the problems ofreferring children with emotional and behaviour.problems for help.2 The experience has alsobeen of educational value, not only in thedevelopment of short term psychotherapeutictechniques,6 but also in the training of medicalstaff in the different ways to listen to howchildren and families communicate their con-cerns and the ways in which to work with them.
1 Garralda ME, Bailey D. Psychiatric disorders in generalpaediatric practice. Arch Dis Child 1989;64:1727-33.
2 Oke S, Moyer R. Referrals to child psychiatry-a survey ofstaff attitudes. Arch Dis Child 1991;66:862-5.
3 Josse JD, Challener J. Liaison psychotherapy in a hospitalpaediatric diabetic clinic. Arch Dis Child 1987;62:518-22.
4 Vas Dias S. Psychotherapy in special care baby units. NursingTimes 1987;83:50-2.
5 Black D, McFadyen A, Broster G. Development of apsychiatric liaison service. Arch Dis Child 1990;65:1373-5.
6 Vas Dias S. Paediatric psychotherapy: the development of atechique for a service in a general out-patient clinic. Journalof Child Psychotherapy 1990;16:7-20.
Coeliac disease and lymphangiectasia
Vojislav N Perisic, George Kokai
Mother and Child HealthInstitute of Serbia,Radoia Dakica 6-8,11070 Novi Beograd,YugoslaviaVojislav N PerisicGeorge KokaiCorrespondence to:Dr Perisic.Accepted 28 August 1991
(Arch Dis Child 1992;67:134-6)
AbstractTwo out of 74 children with coeliac diseasedemonstrated severe intestinal protein loss.In both children a serial small bowel biopsyspecimen showed intestinal lymphangiectasiato be also present. Intestinal lymphangiectasiais another disorder that may be associatedwith coeliac disease.
Several disorders have been found to occur inassociation with coeliac disease. Cystic fibrosis,ulcerative colitis, Crohn's disease, collagenouscolitis, giardiasis, and recurrent oral and smallintestinal ulceration have all been reported inchildren and adults with coeliac disease.' 2However, the coexistence of coeliac disease withintestinal lymphangiectasia has not so far beendescribed. Both diseases may present with sub-stantial enteric protein loss and steatorrhoea andpotentially mimic each other, although the dis-tinctive small intestinal mucosal changes willdiscriminate between the two.We describe for the first time coeliac disease
and intestinal lymphangiectasia occurringtogether in two children with severe entericprotein loss.
Patients and methodsBetween May 1981 and December 1985, 74children were diagnosed as having coeliac diseaseaccording to the criteria of the European Societyof Paediatric Gastroenterology and Nutrition.3In addition to chronic diarrhoea, failure tothrive, and steatorrhoea two of the children also
had clinical and laboratory evidence of severeintestinal protein loss (table).4 Case 1 alsodeveloped the clinical features of tuberoussclerosis: fibroangiomatous naevi, adenomasebaceum, and brain tubers on computed tomo-graphy at the age of 7-5 years.
In both children small intestinal mucosalbiopsy specimens demonstrated either total orsubtotal villous atrophy with other microscopicfeatures commonly seen in coeliac disease: crypthyperplasia, increased number of intraepitheliallymphocytes, heavy lymphoplasmocytic in-filtration of the lamina propria, and appreciablelymphangiectasia (fig IA and 2A). Sweatchloride concentration, stool chromatographyfor sugars, duodenal juice and stool microscopyfor parasites, liver function tests, urinalysis,and chest radiography were all normal ornegative. Concentration of coagulation factorsII and VII were decreased and returned tonormal after parenteral administration ofvitamin K. Both children initially demonstrateda complete absence of serum IgA and IgM. Case1 had a low IgG concentration of 1-9 g/l (normalrange 7-62 (2 09) gl1). Case 2 also had adecreased IgG concentration of 1-6 g/l (normalrange 6-61 (2-19) g/l). Examination of peripheral
Details of the two patients with coeliac disease andlymphangiectasia
Case Sex Age Oedema Serum Faecal fat*No (months) albumin (gl100 g
(gil) stool)1 F 25 Generalised 10 68-42 M 12 Legs and eyelids 18 55-8
*Three day collection.4
on 6 May 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.67.1.134 on 1 January 1992. D
ownloaded from

Coeliac disease and lymphangiectasia
Figure I Case 1: (A) Initial biopsy specimen demonstratingsubtotal villous atrophy, crypt hyperplasia, and dilatedlymphatics in the lamina propria. (B) Specimen taken afterrestoration ofthe villous architecture to normal after glutenfree diet. Dilated lymphatics are also present. (C) Specimentaken after gluten challenge showing shortened and bluntedvilli and hyperplastic crypts. Lymphangiectasia persists. (Allhaematoxylin and eosin stainx 100.)
blood T lymphocytes from case 2 (E rosette test)showed decreased values of 30 5 (normal range
60-80%).A gluten free, low milk, low fat, high protein
diet with vitamin supplementation led to a
gradual improvement during the next eightmonths in both patients. Diarrhoea ceased andthey both reached an appropriate weight andheight. Serum albumin and immunoglobulinconcentrations returned to normal.
After two years on a gluten free diet bothchildren underwent gluten challenges after con-firmation of histological remission. Histologi-cally relapse occurred in each child after threemonths on gluten (fig 1B, IC and 2B, 2C).Small bowel biopsy specimens taken at followup demonstrated the persistence of lymph-angiectasia.
During a six year follow up, case 1 remainedon a strict gluten free diet, but on severaloccasions ate large amounts of fatty foods. Herstools became voluminous and pale and hereyelids and legs swollen. At the time of her firstrelapse, at the age of 3 5 years, her serumalbumin concentration decreased to 20 g/l, IgGto 2-6 g/l, and IgM to 0-17 g/l.During 2-5 years of follow up, case 3 has not
relapsed clinically, has remained strictly on therecommended diet, and thrived.
7>-AElF,;- t-- - W
Figure 2 Case 2: (A) Initial biopsy specimen demonstratingsubtotal villous atrophy and cystically dilated lymphatics.(B) Specimen taken after gluten free diet showing that villousarchitecture has returnedalmost to normal. Lymphangiectasiastill present. (C) Specimen taken after gluten challengeshowing evident total villous atrophy and lymphangiectasia.(Haematoxylin and eosin stain in (A) and (C) x 100, in(B) x50.)
DiscussionSevere intestinal protein loss and steatorrhoeaare distinct features of a variety of gastro-intestinal disorders including coeliac diseaseand intestinal lymphangiectasia.S Clinically,both diseases may present with chronic diar-rhoea, failure to thrive, and oedema and therebymimic one another.6 Moreover, appreciablehypoproteinaemia, steatorrhoea, hypocalcaemia,and abnormal laboratory indices of intestinalprotein loss, for example raised faecal a1-anti-trypsin clearance, may occur in both coeliacdisease and intestinal lymphangiectasia. Thedistinctive small intestinal mucosal changes andthe presence of lymphopenia, hypoimmuno-globulinaemia, and T cell depletion are helpfulin differentiating intestinal lymphangiectasiafrom coeliac disease. Sometimes the normalvillous architecture of the jejunal villi may bedistorted appreciably by large dilated lacteals inintestinal lymphangiectasia, causing appearanceof villous atrophy.Our patients suggest an association between
intestinal lymphangiectasia and coeliac disease.The severe intestinal protein and fat losses, withassociated mineral and vitamin deficiencies,which characterise intestinal lymphangiectasiamay considerably exaggerate both the presenta-tion and the course of coeliac disease. If notrecognised promptly, intestinal lymphangiec-tasia may thereby cause treatment failure in
135
on 6 May 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.67.1.134 on 1 January 1992. D
ownloaded from
136 Perisic, Kokai
children with coeliac disease. Multiple smallintestinal biopsy specimens, perhaps takenendoscopically, may be helpful in establishingthe presence of intestinal lymphangiectasia inchildren with coeliac disease.3 6 As intestinallymphangiectasia may be an incidental finding,additional data, for example the presence ofhypoimmunoglobulinaemia andT cell depletion,may help in determining the clinical significanceof lymphangiectatic mucosal changes.' 6 Thesepatients with coeliac disease need lifelong dietmanagement.
The authors thank Dr Ian W Booth for his contribution to thismanuscript.
1 Cooke WT, Holmes GKT. Coeliac disease and associateddisorders. In: Cooke WT, Holmes GKT, eds. Coeliacdisease. Edinburgh: Churchill Livingstone, 1984:225-46.
2 Goodchild MC, Nelson R, Anderson CM. Cystic fibrosis andcoeliac disease: coexistence in two children. Arch Dis Child1973;48:684-91.
3 Meeuwisse GW. Diagnostic criteria in coeliac disease. ActaPaediatr Scand 1970;59:461-3.
4 King EJ. Microanalysis in medical biochemistry. London:Churchill, 1953;92-6.
5 Vardy PA, Lebenthal E, Shwachman H. Intestinallymphangiectasia: a reappraisal. Pediatrics 1975;55:842-51.
6 Walker-Smith JA. Protein losing enteropathies. In: Walker-Smith JA, ed. Diseases of the small intestine in childhood.London: Butterworth, 1988:420-5.
Positive end expiratory pressure via a portablesystem in thoracic dystrophy
S Edees, A Moulden, R J Winter
University Hospital,Nottingham NG7 2UH,Department ofChild HealthS EdeesA MouldenDepartment ofAnaesthesiaR J WinterCorrespondence to:Dr Winter.Accepted 3 September 1991
(Arch Dis Child 1992;67:136-7)
AbstractThe provision of positive end expiratorypressure, via a unique portable system, in thelong term management of a child with thoracicdystrophy is reported. The system uses lowgas flow enabling a reduction in equipmentand simplification of the circuit as comparedwith a standard continuous positive airwayspressure system.
For a child requiring long term continuouspositive airways pressure (CPAP), we devised asystem for providing positive end expiratorypressure (PEEP) using low flows of oxygen.The system, initially employed to provideCPAP, was a standard high flow Bennett systemnecessitating that the patient be restricted to hiscot on the infants' ward where there are pipedsupplies of oxygen and air. In order for him tobecome mobile around the hospital and ulti-mately at home, we devised a portable PEEPsystem.
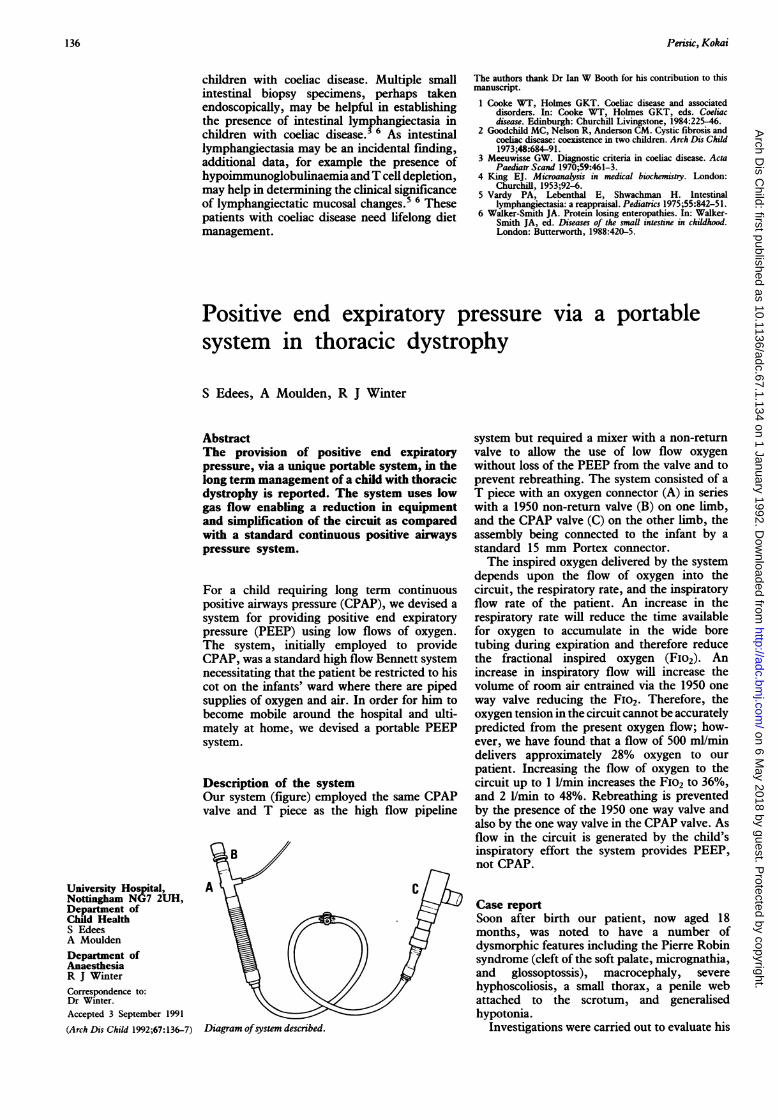
Description of the systemOur system (figure) employed the same CPAPvalve and T piece as the high flow pipeline
B
AC
Diagram ofsystem described.
system but required a mixer with a non-returnvalve to allow the use of low flow oxygenwithout loss of the PEEP from the valve and toprevent rebreathing. The system consisted of aT piece with an oxygen connector (A) in serieswith a 1950 non-return valve (B) on one limb,and the CPAP valve (C) on the other limb, theassembly being connected to the infant by astandard 15 mm Portex connector.The inspired oxygen delivered by the system
depends upon the flow of oxygen into thecircuit, the respiratory rate, and the inspiratoryflow rate of the patient. An increase in therespiratory rate will reduce the time availablefor oxygen to accumulate in the wide boretubing during expiration and therefore reducethe fractional inspired oxygen (FIo2). Anincrease in inspiratory flow will increase thevolume of room air entrained via the 1950 oneway valve reducing the FiO2. Therefore, theoxygen tension in the circuit cannot be accuratelypredicted from the present oxygen flow; how-ever, we have found that a flow of 500 ml/mindelivers approximately 28% oxygen to ourpatient. Increasing the flow of oxygen to thecircuit up to 1 I/min increases the FIO2 to 36%,and 2 I/min to 48%. Rebreathing is preventedby the presence of the 1950 one way valve andalso by the one way valve in the CPAP valve. Asflow in the circuit is generated by the child'sinspiratory effort the system provides PEEP,not CPAP.
Case reportSoon after birth our patient, now aged 18months, was noted to have a number ofdysmorphic features including the Pierre Robinsyndrome (cleft of the soft palate, micrognathia,and glossoptossis), macrocephaly, severehyphoscoliosis, a small thorax, a penile webattached to 'the scrotum, and generalisedhypotonia.
Investigations were carried out to evaluate his
on 6 May 2018 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.67.1.134 on 1 January 1992. D
ownloaded from





























