Embed Size (px)
Citation preview

A DESCRIPTION AND CLASSIFICATION OF THECOMMON DISORDERS OF SPEECH IN CHILDREN
BY
T. T. S. INGRAMFrom the Department of Child Life and Health, University of Edinburgh and the Royal Hospitalfor Sick Children,
Edinburgh
(RECEIVED FOR PUBLICATION MARCH 9, 1959)
The full assessment of children suffering fromspeech defects requires a team consisting of speechtherapist, paediatrician, psychologist and otologist.The additional services of a phonetician, neurologist,orthodontist, plastic surgeon, radiologist, socialworker or psychiatric social worker and childpsychiatrist are often helpful.
Unfortunately the majority of descriptions andclassifications of speech disorders in childhood areby speech therapists working without much medicalco-operation and advice. With honourable excep-tions, they tend to regard speech disorders as ratherisolated phenomena, dissociated from the otherbehavioural and psychological characteristics of thechild. In the present paper an attempt is made todescribe and classify the disorders of speech mostfrequently encountered in a hospital speech clinicfrom the point of view of the paediatrician of adiagnostic team.
Case Material and Methods of ExaminationThe descriptions of speech disorders are based
largely on experience in the Speech Clinic of theRoyal Hospital for Sick Children, Edinburgh, in thelast three years. During this time a total of 348patients were referred, though for various reasonsit was possible to investigate only 189 of them fully.The patients are not representative of an unselectedsample of children in the community as judged bythe figures for all live births given by the RegistrarGeneral for Scotland (1951). There is an excessof patients in Social Classes I and lI, possibly becauseof the greater attention paid to speech defects inthese classes (Table 1). The greater excess ofpatients in Social Classes I and 11 over the age of 5than under the age of 5 is probably the result of thefact that children in the lower social classes attendcorporation schools where there is a very compre-hensive speech therapy service. In private fee-payingschools, where more attention is usually paid to
speech defects, speech therapy is rarely provided.Children with speech defects attending these schoolswere frequently referred to the Speech Clinic in theHospital.
Detailed family, birth and developmental historieswere taken, with particular emphasis on the rate, andany abnormalities, of speech development. Thechildren were subjected to a detailed paediatric andneurological examination, and behaviour in playwas observed for as long as possible in each case.The child's speech was studied jointly by thepaediatrician and the speech therapist, and detailednotes were made of its intelligibility and of theparticular defects which were observed. In manycases tape recordings were made, though it is alwayseasier, in fact, to examine speech for defects ofarticulation in the presence of the patient. Speechwas studied from the points of view of level oflanguage ability and defects of articulation.
Attempts were made to assess the child's abilityto understand what was said to him by his parents
TABLE 1
DISTRIBUTION OF 189 PATIENTS WITH SPEECHDISORDERS BY AGE AND SOCIAL CLASS
Social ClassAge Total
II III IV V
Under 3 .. 1 153-5 .. 25 16 48 13 9 1115-10 12 I11 20 5 2 5010+ .. 3 3 3 2 2 13
All ages 41 31 81 22 14 189
Under 5 . 43 58 25 126Over5 29 23 11 63
All ages .. 72 81 36 189
Approx. % 39 42 19 100
RegistrarGeneralScotland1951 ..12-5 58 3 29-2 100
444
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from

CLASSIFICATION OF SPEECH DISORDERS IN CHILDRENand by other people. Any apparent tendency for thechild to rely unduly on gesture, or on watchingpeople talking to him, was noted. Rough tests ofhearing were used during the general examination ofthe patient, his responses to whistles of variouspitches, bells, the rustling of paper, vibration forks,whispering, talking and shouting being observed.Full audiometry was performed on all children assoon as they were co-operative enough for thisexamination to be performed. Handedness wastested rather unscientifically by noting the handwhich the child used in each of four performancetests carried out three times. Each patient was askedto turn a door handle, break a stick, throw and catcha ball. Patients not using a single hand for nineor more of the total of 12 tests were classified as beingambidextrous. Eyedness and footedness were alsotested (Ingram and Reid, 1956).A psychiatric social worker, seconded to the
Clinic, was asked to investigate the home situationof 41 patients in whom psychological stress appearedto be important. Thirty-one patients were furtherassessed in the Department of PsychologicalMedicine. The opinion of an otolaryngologist wasasked in 34 cases, of a plastic surgeon in five, and ofan orthodontist in eight. Eleven patients wereadmitted to hospital on account of physical condi-tions noted at the time of assessment. Theseincluded patients suffering from cretinism, epilepsy,enuresis, phenylketonuria, fibrocystic disease ofthe pancreas and Sj0gren's syndrome.
ClassificationThe classification is by clinical findings. Categories
are defined in the first place by the form of the majorspeech defect. Thus distinctions are made betweendisorders affecting the voice predominantly (dys-phonia), those whose main effect is to alter therhythm of speech (dysrhythmia) and those in whichabnormalities of articulation are the presentingfeature.
It must be admitted that classification on the basisof the major defect of speech is somewhat arbitraryand crude (as are most classifications), and it isnecessary to ignore a number of significant clinicalfindings in many cases for the purpose of givingthe speech condition a name. For example, manypatients suffering from a stammer will have minorabnormalities of articulation; some patients with'specific developmental speech disorders' will haveminor stammer (speech dysrhythmia). It is impos-sible to take account of these subsidiary defects inthe major categories.
Further classification is by associated clinicalfindings. When direct interference with the function
of the articulatory organs can be demonstrated thedisorder is considered to be 'dysarthric'. When theabnormalities of articulation are part of a moregeneral disorder and no direct interference with thefunction of the articulatory organs can be demon-strated they are considered to be 'secondary'. Whendisorders apparently confined only to the functionsof speech are present, unassociated with directinterference with the articulatory organs, they areclassified as 'specific developmental' or 'functionalspeech disorders' (Table 2).
TABLE 2CLASSIFICATION OF SPEECH DISORDERS FOUND IN
189 CHILDREN
(1) Disorders of Voicing (Dysphonia) (4)a. With demonstrable disease of the larynx ....b. Without demonstrable disease of the larynx 3
(2) Disorders of Rhythm (Dysrhythmia) (29)a Clutter . ..3b. Stammer . .26
(3) Disorders of Articulation with Demonstrable Dysfunctionof Articulatory Apparatus (Dysarthria) (30)
a. Due to neurological abnormalities . ..7b. Due to local abnormalities.... .. ..23
(4) Disorders of Articulation without Demonstrable Dys-function of Articulatory Apparatus (Secondary SpeechDisorders) (41)
a. Secondary to hearing defect. ..... 8b. Secondary to mental retardation . ... 29c. Secondary to psychogenic disorders .. 3d. Secondary to aphasia due to brain damage . . 1
(5) Specific Developmental Speech Disorders (FunctionalSpeech Disorders) (80)
a. Involving language development and articulation 40b. Involving articulation only.... .. .. 40
(6) Mixed Cases (4) .. ... 4(7) Unclassified and Other (1) ......I
............189
In some cases there are contributory causal factorsin the speech disorder. For example, a child withbrain damage secondary to encephalitis or traumamay have a disorder of articulation which is partlysecondary to aphasia and partly the result ofinco-ordination of the organs of articulation. Suchpatients may conveniently be placed in the categoryof 'mixed cases'. They are relatively few.
CategoriesDisorders of Voicing. Disorders of voicing are
relatively uncommon in childhood, amounting to nomore than 4% in most large series of patients withspeech defects. In the present series there werefour patients with disorders of the voice (approxi-mately 2% of the series).The only disorder of voicing considered in the
present classification is chronic lack of voice, whichmakes the child sound as if he is hoarse. This issimilar in quality to the 'loss of voice" suffered byadults with laryngitis. It must be distinguished fromthe effects of excessive nasal escape (hyperrhino-phonia) or nasal obstruction (hyporhinophonia). In
445
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from

ARCHIVES OF DISEASE IN CHILDHOOD
these conditions difficulty of articulation is thestriking abnormality. They have therefore beenincluded under the heading of 'dysarthria'.Dysphonia affects girls rather more frequently
than boys, or at any rate is complained of morefrequently by the parents of girls. It may occur atany age and has been observed in a child of 6 months,but more commonly it begins between the ages of 2and 8 years. Its onset is commonly gradual. Oftenthere is a period of weeks or months during whichthe condition is intermittent, being present for a dayor two at a time and then recovering. Even whenfinally established, the severity of dysphonia variesfrom week to week, from day to day and even fromhour to hour. Frequently the child is able to shout,and sometimes to sing, but not to speak with normalvoice.A number of inflammatory, traumatic and neo-
plastic laryngeal conditions interfering with thefunction of the vocal cords may cause dysphonia inchildhood. I have seen it personally followingtraumatic laryngoscopy and inhalation of caustic,complicating chronic bronchitis and laryngitis,associated with nodules of the vocal cords andpapillomata of the larynx, and occurring in thecourse of Sjogren's syndrome (Birrell, 1954).
In many cases, however, no abnormalities of thelarynx can be found. The immediate assumption iscommonly made that the dysphonia is therefore of'psychological origin'. It seems to be equally likelythat there are abnormalities of the vocal cords inthese patients, which cannot be recognized by ourpresent crude methods of investigation.There are no well recognized methods of treating
dysphonia in childhood by 'speech therapy'. Restof the voice for a period of four to six weeks willoften result in a marked improvement in voicing.Unfortunately this is often transient, and relapseoccurs as soon as the child begins to shout again.A proportion of children with dysphonia, moreboys than girls, show improvement at the time ofadolescence, whether the larynx is obviously ab-normal or not. Such improvement is impossible topredict, however, and many patients continue tohave abnormalities of voicing into adult life.
Speech Dysrhythmias. Involuntary interferencewith the normal rhythm of speech is one of thecommonest disorders of speech in childhood. Twomain types may be recognized.
Clutter consists of a more or less sudden irregularacceleration of speech which results in a shift ofstress and syllable division in speech. The wordssound 'run into one another' and sometimes speechmay be so disturbed as to be incomprehensible.
Many children aged between 2 and 4 years mayshow clutter transiently for a period of weeks ormonths without any associated or subsequentabnormality of speech. When clutter occurs afterthe age of 5 it is more often associated with stammeror hesitation (Van Riper, 1947).
Involuntary temporary arrest of the flow of speechmay be manifest as hesitation, a transient inabilityto produce the next expected syllable resulting in aperiod of no speech. Stammer consists of theinvoluntary repetition of a sound as well as aninability to move beyond it. It is unrewarding todistinguish too cleverly between hesitation andstammer. They are often associated. Many patients'dysrhythmia first takes the form of hesitation, andmonths or years later they begin to stammer. Othersstammer first and then show hesitation.
Hesitation or stammer is found more often inchildren whose fathers are in Social Classes I and II(Registrar General) than in the lower social classes.There appears to be no difference in the observedand expected birth order of patients. Males aremore frequently affected than females, the ratio beingas high as four to one in some series (Wilson, 1954).In the family history a high proportion of relativesstammer, 44% according to Johnson, Brown,Curtis, Edney and Keaster (1948). There is a higherproportion of ambidexterity and left-handednessamongst relatives than expected (Travis, 1931). Ofthe present small series of 29 patients, 38% hadparents or siblings with speech defects. These weredysrhythmic in type except in one instance. Theparents and/or siblings of 27% were left-handed orambidextrous.The birth history and motor milestones of patients
tend to be within normal limits. Speech develop-ment is not significantly retarded. The majority ofchildren are of average intelligence or better, andshow no neurological defects.A relatively high proportion of patients will be
found to be left-handed or ambidextrous, the pro-portion depending largely on the methods of testingused (Orton, 1937; Morley, 1957). In the presentseries, 12 of the 29 patients were found to show littlelaterality of handedness, and one was sinistral.A high proportion of patients show abnormalities
of behaviour. These were present in 21 of the 29patients studied in this series. They includedtemper tantrums in four, excessive dependence infive, excessive excitability or tearfulness in five,night terrors in four, enuresis in three and habitspasms in three. Nine of the patients were disturbedenough to merit psychiatric treatment. The extentto which the speech dysrhythmia is an aetiologicalfactor in causing anxiety symptoms is probably over-
446
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from
CLASSIFICATION OF SPEECH DISORDERS IN CHILDREN
estimated. In many cases symptoms of abnormalbehaviour preceded the appearance of the speechdefect, and both could be related to the sameemotional stresses. Parents related the onset ofsymptoms to maternal separation before the age of4 years in five instances (the child being hospitalizedin three), to physical accidents in two, to severewhooping cough in two and to crippling accidentsto the father in two.The modes of onset and course of dysrhythmia in
childhood are relatively consistent. The majorityof cases of uncomplicated clutter recover normalspeech before they are 5 years of age. Hesitation orstammering appears in most persistent stammerersfor the first time between the ages of 2 and 4 years.In only five of 25 patients with stammer or hesitationin this series did symptoms appear after 5 years ofage. It is difficult to know how many childrenshowing definite persistent stammering at this periodrecover completely and how many later have dys-rhythmic speech symptoms. Ofchildren who presentwith persistent stammer, two-thirds (17 of 25 in thisseries) have never been really free of the symptomsfor more than four weeks at most from the time ofits onset.True remissions of stammer lasting for more than
six months are more frequent in those where firstsymptoms occur under the age of 5 years, but thestatement made in text-books that a stammeroccurring in a pre-school child is likely to be of littlesignificance. requires qualification. Of the eightremissions of stammer which occurred in this series,all but one of them occurred before the age of 5years. Only three of the remissions lasted longerthan three years. The remaining five patients beganto stammer again shortly after going to school. Itis too early to know if the other three remissions arepermanent or not.The subsequent course of stammer varied greatly
according to the reaction of the patient to hissymptom. Some children adjusted to quite a severedysrhythmia and were surprisingly undisturbed byits presence. Others began to avoid speaking andmaking social contact whenever possible. Theyattempted to avoid words on which they believedthey would stammer, and restricted their activitiesin an attempt to hide their speech defect. In timethe fear of stammering may become the most potentcause of stammer.
It is extremely doubtful if speech therapy per seis helpful in speech dysrhythmia. A mother con-fessor or a child psychiatrist (either of which rolesspeech therapists may be found adopting) occasion-ally seems to benefit the patient's attitude to hisspeech defect. There appear to be no reliable
comparative figures on which to base conclusionsabout the proportion of patients with stammer whospontaneously improve at adolescence or in earlyadult life with the help of, in spite of, or withoutspeech therapy.My clinical impression is that patients in whom it
has taken very severe emotional stresses to pre-cipitate stammering tend to have a better prognosisthan those who stammered without much evidentemotional stress being necessary. This impression,like so many concerning speech disorders, requiresconfirmation.
Dysarthric Speech Disorders. In this category areincluded those disorders of articulation which arethe result of organic disease causing interferencewith or failure of the normal mechanical functionsof part or parts of the articulatory apparatus.Thirty-one of the 189 patients were in this category.The category is divided into two sub-categories.
Patients whose articulatory difficulties are due toneurological abnormalities are included in the first.In these there is rarely much deformity of thearticulatory organs themselves. In the second arethose disorders of articulation which are the resultof local abnormalities affecting the articulatoryapparatus. Deformity of the articulatory organsmay often be observed.
In general, speech defects in this category arecharacterized by their consistency. They varyrelatively little from day to day or from hour tohour, and the same sounds as are abnormal duringspontaneous speech are found on testing to bedefective. For example, the sounds requiring naso-pharyngeal closure will be consistently defective inpatients with cleft palate.
Apart from the six patients with cerebral palsy,motor milestones were within normal limits, andonly one of the other 24 patients had retardedlanguage development, though in many cases it wasa long time before people outside their immediatefamilies could understand what the children said.Three of the six patients with cerebral palsy failedto walk without support before 18 months, and allof them failed to say recognizable first words by18 months and phrases by 30 months (Table 3).Again with the exception of those patients withcerebral palsy, the children in this category appearedto be of average intelligence. A relatively highproportion, 14 of the 30 patients, suffered fromabnormalities of behaviour, however. In five casesthere was immaturity of behaviour, manifest asexcessive attachment to the mother, inability to playwith other children of similar age, inability to accepta school situation at the normal age or play
447
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from

ARCHIVES OF DISEASE IN CHILDHOODTABLE 3
WALKING AND SPEECH DEVELOPMENT OF 30 CHILDRENWITH DEMONSTRABLE DYSFUNCTION OF ARTICULA-
TORY APPARATUS (DYSARTHRIA)
Hypomandi-Walking and Speech Develop- Cerebral bulosis and Other Total
ment Palsy Malocclusion
Walking before 18 months .. 3 7 15 25Walking after 18 months . 3 11 5
Total .. .. 6 8 16 30
Words before 18 months andphrases before 30 months 0 68 14
Words before 18 months andphrases after 30 months 0 2 3 5Words after 18 months andphrases before 30 months
Words after 18 months andphrases after 30 months 60 1 7
Unknown .....0. 0 4 4
Total .. .. 6 8 16 30.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
characteristic of a younger age level. Enuresis was
present in six patients, thumb or hand sucking inthree. Three patients were excessively tearful, fearful,or unusually withdrawn. Three patients showed a
characteristic form of overactive behaviour oftenfound in children with cerebral damage, especiallywhen it affects the temporal lobe (Ingram, 1956).The extent to which these abnormalities of behaviourcould be regarded as other symptoms of the under-lying disturbance which was responsible for thespeech defect, and how much they were the resultdirectly and indirectly of the speech defect, isextremely difficult to assess.
The neurological lesions in this category are
conveniently divided into those affecting the brain,those affecting the brain stem and those affectingthe lower motor neurone (Table 4). Cerebral palsy
TABLE 4CLASSIFICATION INTO SUB-CATEGORIES OF 30PATIENTS SUFFERING FROM DISORDERS OF
ARTICULATION WITH DEMONSTRABLE DYSFUNCTIONOF ARTICULATORY APPARATUS (DYSARTHRIA)
a. Due to Neurological Abnormalities (7)Cerebral palsy ..........Suprabulbar palsy ......Lower motor neurone lesions ....
b. Due to Local Abnormalities (23)Jaws and Teeth Hypomandibulosis ..
Other malocclusion..Tongue Tie
Tongue thrustLips Cleft lip (only) ..
Other ..Palate Cleft (with or without cleft lip)
Other ..Pharynx Large pharynx (palatal dispropor-
tion) .. ..Acquired disease .. ..
Total .... .. .. .. ..
610
62
40
50
3
30
cerebral palsy. Though dysarthria is relativelyfrequently found in severe dip'egia, severe ataxia,dyskinesia and bilateral hemiplegia, it is uncommonin mild diplegia (especially paraplegia) and hemi-plegia. In the latter disorders defective speech ismore frequently part of a general retardation ofdevelopment, or is secondary to aphasia. In patientswith dyskinesia following kernikterus, abnormalitiesof articulation are commonly the result of a com-
bination of articulatory inco-ordination and hearingdefect.
Suprabulbar paresis (facial diplegia, Moebius'syndrome) is easily recognized when it is severe andespecially when it affects eye movements (Hender-son, 1939; Evans, 1955). Minor manifestations ofthe condition may be more difficult to recognize,however, and a number of patients have beenobserved in whom poor voluntary movements of thelips, tongue and soft palate were present withoutobvious voluntary paralysis of these organs. Thetrained phonetician can be of great help in theaccurate diagnosis of these disorders by his inter-pretations of the child's speech in terms of tongue,lip and palatal movements.Though no cases occurred in the present series,
lower motor neurone lesions affecting articulationhave been seen occasionally following poliomyelitisand diphtheria, but they are more commonly theresult of peripheral nerve damage during tonsil-lectomy. The history in patients who have suffereddamage to a palatal nerve is typical. Followingdischarge from hospital the speech is noted to beabnormal and fluids may come down the nose whenthe child tries to drink. Though the ability to drinkis recovered after a few weeks the child continuesto speak 'down the nose', and defects of the plosives,vowels and 's' 'E' and 'f ' sounds are noted.
Since a single local abnormality of the mouth or
pharynx may affect a number of the organs ofarticulation it is more convenient to classifydysarthric speech disorders by the nature of theabnormality rather than by the type of speechdefect which they cause. Thus whilst hypomandi-bulosis prevents correct dental occlusion and some-times apposition of the lips, involuntary protrusionof the tongue during speech, 'tongue thrust', is oftena more important cause of disordered articulation.
Other forms of malocclusion and dental abnor-malities cause abnormalities of articulation lessfrequently than hypomandibulosis. The com-
monest of them are the result of an undue promin-
ence of the lower jaw, associated with open bite,wide separation of the incisors, or missing teeth.These conditions are most frequently associatedwith 'lisping' due to the lateral or central protrusion
is by far the commonest cause of neurologicallesions, but it is worth emphasizing that dysarthriais not the commonest form of speech defect in
1-11
448
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from

CLASSIFICATION OF SPEECH DISORDERS IN CHILDRENof the tongue between the teeth when sibilants areproduced.
In a few children the wide separation or anteriorprotrusion of the upper incisors appears to beattributable to excessive finger or thumb sucking. Inothers there is associated 'tongue thrust', though theextent to which this can be regarded by itself as thecause of dental abnormalities must remain in doubt.Tongue tie is an uncommon cause of articulatory
difficulties, though it is often blamed for them. Acommoner abnormality of the function of the tonguewhich does cause articulatory difficulties is 'tonguethrust'. This condition may be associated withcerebral palsy or congenital abnormalities of themouth, as have been described. It is often found inassociation with chronic tonsillitis and adenoiditis.But it may be present as the only obvious abnor-mality in many cases. In children showing it thepattern of swallowing is often observed to beimmature in type and on stroking the lips gently amild sucking reflex associated with opening of themouth and some tongue protrusion is not infre-quently observed (Francis, 1958). Abnormalities ofthe lips alone are not a common cause of articulatorydifficulty, though one case occurred in the presentseries in which the upper lip was abnormally highand fixed.
Malformations of the palate are relatively frequentcauses of severe articulatory difficulties. Thecommonest malformation is an actual cleft in thesoft palate. Less commonly a midline defect in themuscular elements without a defect in the mucousmembrane (submucous cleft palate) may bediagnosed if the cleft palate is gently palpated. Thearticulatory defect is similar in type, though lesssevere than that found in a true cleft palate.The excessive nasal escape which results when the
palate is cleft impairs all vowel and consonantsounds, with the exception of 'm', 'n' and 'i' in whichconsiderable nasal outflow of air is usually required.Substitutions for particularly defective sounds arefrequent. For example glottal stops may replaceplosives. Associated abnormalities also contributeto the speech defect. Especially in children withbilateral clefts of the palate there is frequentlymarked deformity of the alveolar bony structure,especially after operation, and dental malocclusionresults. The upper lip is all too often ratherfunctionless (Morley, 1954).A relatively small number of patients present with
cleft palate speech' with nasal escape, in whom noabnormalities of palatal movement can be found.In the majority speech has been 'through the nose'from the earliest years, and in a few there is a historyof escape of fluids through the nose when drinking
in infancy. In others a change from normal speechhas been noted following adenoidectomy. Onexamination many of these patients show markedanterior prominence of the maxillary bones and thepharynx appears to be unusually deep, so that thelength of the palate is inadequate for its posteriormargin to reach the posterior nasopharyngeal wall.Radiological investigation will often confirm thatthe pharynx is, in fact, abnormally deep and thepalate inadequate in size, in spite of full movement,to close the nasopharynx. Many of these patientscan be helped by operations designed to reduce thesize of the pharyngeal aperture (Calnan, 1957;Gibb, 1958). In a few patients nasal escape appearsto be due to impaired palatal movement, the resultof inflammatory peri-tonsillar induration, or scarringfollowing tonsillectomy.
Tonsillitis and enlargement of the adenoids aremuch less common single causes of significantpersistent dysarthria in childhood than is oftenstated. In the present series only one patient wasincluded in the sub-category of dysarthria due to'acquired disease of the pharynx'.
Secondary Speech Disorders. These are disordersof articulation which are not due to direct inter-ference with the mechanics ofthe articulatory organs,but are secondary to other physical, mental orpsychiatric conditions. Often it may be demon-strated that these organs can be moved normally, andfrequently that sounds not used in spontaneousspeech can in fact be produced by the child. Themost important causes of articulatory disorders ofthis type are hearing defects and mental retardation.
Children with hearing defects have never heardor have ceased to hear speech sounds correctly, andtherefore cannot be expected to reproduce them inspeech. A study of the behaviour and articulatoryabnormalities shown by the child will often give aclue to the type of hearing defect. Children withsome loss of hearing for high tones only will com-monly show failure in articulating 'f' 'E', 'p', 't','J" and 's'. Children with more severe hearing lossfor all frequencies will often only produce soundsrequiring much lip movement, which they can seewhen they watch people talking to them. This isnot always the case, however, and a number ofpatients have been seen with retarded speechdevelopment and poor performance on intelligencetests whose hearing was found to be significantlydefective on audiometry, to the surprise of theexaminer. Once they have learnt how to use asuitable hearing aid the children have often improvedmarkedly in their performance on intelligence tests.This emphasizes the need for routine audiometry inall children with speech defects.
8
449
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from
ARCHIVES OF DISEASE IN CHILDHOODChildren with mental retardation present more
complex disturbances of articulation. Often thereappears to be a failure to perceive and discriminatespeech sounds accurately, possibly because of areduced span of attention. Even when 'parrotting'what has just been said to them, their articulationwill often be quite inaccurate. Speech developmentis usually considerably retarded, and the patientsshow errors of articulation commonly found inmuch younger normal children. In these patientsthe later acquired sounds are usually abnormal,especially 'r', 'E', 'J', 'tJ' and 'd3'.
Defects of articulation are often inconsistent andvary from sentence to sentence of spontaneousspeech. There may also be language disorder withthe omission of small words, especially prepositions,auxiliary verbs and conjunctions. There may be ageneral innaccuracy in the articulation of practicallyall speech sounds, which almost justifies the loosedescription of 'clumsy speech' which is often givenby the parents of these patients. There is often afailure to develop normal patterns of intonation andstress, so that speech is curiously monotonous.
Whilst in aphasia the defect of language is (bydefinition) the most important cause of interferencewith speech, the importance of articulatory abnor-malities has been rather under-estimated (Critchley,1952). Especially in children whose cerebral damagehas been sustained before speech development hasbeen completed, there is often gross disturbance ofthe ability to articulate words and their componentindividual syllables correctly. In many cases it isdifficult to draw a line between the languagedifficulties and difficulties in articulation; omissionof small words, conjunctions, prepositions, auxiliaryverbs and pronouns may be associated with theomission of syllables, especially the terminal partsof wotds; reversals and confusion of word ordermay be associated with reversals and the confusionof the order of syllables in individual words and inthe distortion and mispronunciation of syllableswhich are spoken. There may also be quite bizarrealterations of rhythm and stress, making the patientsound as if he were speaking a foreign languagerather well, as in a case of Monrad-Krohn(1947).As might be expected, the milestones of motor
and speech development were very retarded amongstpatients in the category of 'secondary speech dis-orders', largely due to the high proportion ofmentally retarded patients. Major and minorphysical abnormalities were relatively common.Epilepsy was present in six cases. Hyperteleorism,syndactyly, hypospadias, congenital heart diseaseand hemiplegia were each observed in two patients.
There was one untreated cretin amongst the mentallyretarded patients.
Behaviour abnormalities were also common,occurring in 31 of the 41 patients. Twenty-twochildren were described as being excessively depen-dent or immature by their parents. Three wereover-active and showed the typical behaviour shownby some brain-damaged children described byOunsted (1955) and Ingram (1956). In two casesbehaviour was classified as autistic by childpsychiatrists.
Specific Developmental Speech Disorders ('Func-tional Speech Disorders'). In this category are placedthose patients who show disorders of articulationfrom the time they first attempt formed speech, andin which the speech disorder is neither associatedwith obvious abnormalities of articulatory function,nor secondary to demonstrable disease. Eighty ofthe 189 patients who were fully examined wereplaced in this category.
Patients in this category are characterized by theunexpectedly slow development of intelligible speech,though their milestones of motor development areusually within normal limits and their intelligenceis within average limits, or not sufficiently impairedto account for the degree of retardation of speechdevelopment. This is shown in Table 5 in which itwill be observed that 49, or 61.25%, of the 80patients said their first recognizable words (exceptingMum, Mam, Mama, Da, Dad, Dada) after the age of18 months and first joined words together after theage of 30 months. Fifteen, or almost 19%, did notsay their first words until after 30 months and phrasesuntil 42 months or later. Yet, in spite of its slowdevelopment, speech is almost invariably perfectlyintelligible by the age of 7 or 8 years in these patients.Of the 80 patients in this category 58 were boys
and 22 were girls, giving a male to female sex ratiowhich is comparable to other hospital series ofchildren with specific developmental speech andrelated disorders (Hallgren, 1950). The high propor-tion of patients (46 25%) with fathers in SocialClasses I and II is striking, and probably reflects thegreater attention paid by parents in these classes toretarded speech development rather than any greaterprevalence of the disorders in the higher socialclasses. The prospects of their undergoing com-petitive entrance interviews in order to obtain aplace in private schools often exacerbated parents'anxieties about their children's speech.The majority of the children referred were under
the age of 5, as might be expected in view of thetendency for specific developmental disorders ofspeech to remit as the patient grows older. Only
450
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from

CLASSIFICATION OF SPEECH DISORDERS IN CHILDREN
15 of the 80 patients were over the age of 5, and inthe majority of these the speech disorder, though anuisance in school, had ceased to be a major causeof anxiety to the parents. The fact that only threeof the patients were over the age of 7 illustrates thatin the majority of patients speech is perfectlycomprehensible by this age.The distribution of children by their birth order
was not significantly different from the expectedrandom distribution. The fact that 43 of the 73patients were last-born is unremarkable in view oftheir youth. Their parents had not had time toproduce subsequent children, especially those staidmiddle-class Scots with planned families. Seven ofthe patients were illegitimate.A family history of retarded speech development
is often found in cases of specific developmentalspeech disorders. Thirty-seven of the 73 legitimatepatients (about half) had parents or siblings whosespeech development was known to have been slow.Since it was common on examination to find siblingswith speech disorders who had been stated by theparents to be 'rare talkers' or 'lovely speakers', thisis probably an under-estimate. Parents were knownto have retarded speech development in 19 cases, andone or more siblings in 21.
Fifteen patients were born after pregnancies,labours or deliveries which were in some wayabnormal, 11 of them being born prematurely byweight. No convincing evidence of birth injury wasfound in any of them, however, and neurologicalexamination failed to reveal any clinical signs ofcerebral injury.
Ambidexterity, as assessed by the tests which havebeen described, was noted in half of the 80 patients.Only one patient was strongly left-handed. Parentsreported left-handedness or ambidexterity in them-selves in 22 cases, and in the patients' siblings in16 cases. Thus 38, or approximately 52%, of 73legitimate patients had an immediate family historyof sinistrality or ambidexterity.
Seven children had intelligence quotients of morethan 120 on the Terman Merrill scale, and only twowere considered to be dull and backward. It wasinteresting to observe, however, that specificeducational difficulties (dysgraphia or dyslexia) werepresent in seven of the 15 patients over the age of 5.In these cases it seemed legitimate to conclude thatthe children were having specific difficulties with thewritten word which might be related to the troublesthey had previously had with the spoken word(Ingram and Reid, 1956; Drew, 1956).Two forms of retarded development may be
recognized in patients coming into this category.About half of the children are described by their
parents as having 'names' for objects within theirenvironment which are not intelligible to observingstrangers at quite an early age, though they may becomprehensible to the patient's siblings and parents.Their vocabulary is often considerable, but theirarticulation of the words they know is so defectivethat they cannot be understood. Frequently the endsof words are much less well articulated than theirbeginnings. When the children begin to join wordstogether the defects of articulation tend to becomemore prominent, and a frequent complaint frombaffled mothers is that 'he says plenty ar.d he'sanything but stupid, but I can understand only afew words of what he says'. In these patients themajor di:ability is imperfect articulation. Thedevelopment of language may not be much retarded,but what the child says is so imperfectly spoken thatmuch of it cannot be understood.The articulatory difficulties of children with
specific developmental speech disorders are com-plex, and at first hearing quite baffling when onetries to analyse them. The sounds most often poorlyarticulated are shown in Table 6. (It should bepointed out that this was the result of study by theauthor and by speech therapists, not that of properlytrained phoneticians.) In general the sounds whichare the last to be correctly articulated by normalchildren are the ones which cause most difficulty.They may be omitted, faultily pronounced, or sub-stituted by other sounds. The substitutions employedvary with the context of the sound which is defective.Sounds are more often omitted or faultily articulatedat the ends than at the beginnings or middle portionsof words, and more frequently at the beginnings thanthe middles. It is characteristic that words whichthe child has had in his vocabulary for a long timeare articulated with more faults than words morerecently acquired. Thus a child may say 'goggie'for 'doggie', 'wa-wa' for 'water' and 'ba' for 'bath',but be able to say 'Dalgleish', 'wetter' and 'with'quite well. That the articulatory difficulties appearto be so inconsistent often leads parents to accusetheir children of laziness. Their observation thatmany patients can produce sounds correctly onrequest, which are abnormal in spontaneous speech,further infuriates them.About half of the patients in the category have
language difficulties. They are slow in acquiringnew words and often the rate of vocabulary gain isso poor that they have to use gestures to indicatetheir simplest needs until the age of 3 years or older.When sentences are eventually formed, inversionof word order, omission of consonants, prepositions,auxiliary verbs and some personal pronouns arecommonly noted. Many of these children will use,
451
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from
ARCHIVES OF DISEASE IN CHILDHOOD
quite unwittingly, a completely inappropriate wordin a sentence in place of a similarly sounding one
which would have been appropriate. They sufferfrom classical 'developmental aphasia' (Orton, 1937).Of the 80 patients suffering from developmental
speech disorders in the present series, 40 had obviouslanguage (aphasic) difficulties of the type which hasbeen described, and in the other 40 the speech defectappeared to be predominantly of articulation and didnot affect the development of language so severely.
Difficulty in comprehending what was said to themwas frequently observed in children suffering fromspecific developmental speech disorders. In severe
cases the child's inability to understand what is saidis severe enough to make the parents suspect deaf-ness, though they will often give circumstantialaccounts of why they think this unlikely; forexample, 'he hears the whistle of the television setwhen it goes off, and looks up at aeroplanes'. In lesssevere cases parents were often irritated by thechild's tendency to demand repetition of everythingwhich was said to him by saying 'Eh', 'Beg pardon','What', or the child would look blank. Mothers andfathers would often complain of their partner'stendency to gesture to the child, though they are
unaware of their own tendency to do so. Onexamination a distinct lapse of time may be observedbefore the child comprehends what is said to him,though his reactions when he has understood are
often intelligent. The tendency of some patientsto look at faces and rely on gesture rather than on
speech is frequently evident.In the present series 30 patients appeared to have
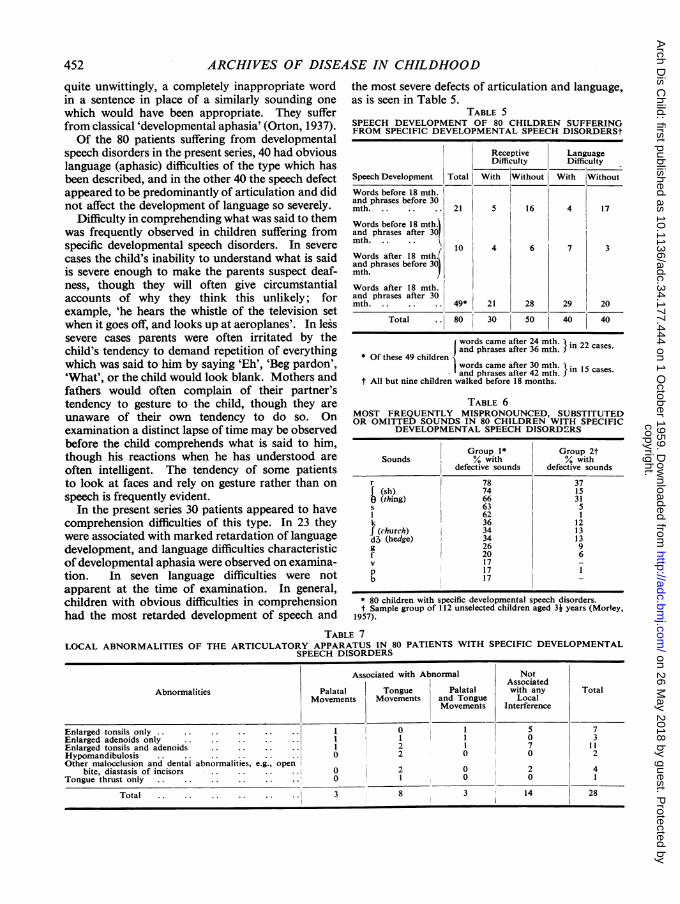
comprehension difficulties of this type. In 23 theywere associated with marked retardation of languagedevelopment, and language difficulties characteristicof developmental aphasia were observed on examina-tion. In seven language difficulties were notapparent at the time of examination. In general,children with obvious difficulties in comprehensionhad the most retarded development of speech and
the most severe defects of articulation and language,as is seen in Table 5.
TABLE 5SPEECH DEVELOPMENT OF 80 CHILDREN SUFFERINGFROM SPECIFIC DEVELOPMENTAL SPEECH DISORDERSt
Receptive LanguageDifficulty Difficulty
Speech Development Total With Without With Without
Words before 18 mth.and phrases before 30mth .. . .. 21 5 16 4 17
Words before 18 mth.land phrases after 301mth..
/10 4 6 7 3
Words after 18 mth.(and phrases before 30~mth.
Words after 18 mth.and phrases after 30mth 49* 21 28 29 20
Total 80 30 50 40 40
words came after 24 mth. n 22 cases.
and phrases after 36 mth. X* Of these 49 children
words came after 30 mth.and phrases after 42 mth. n 15 cases.
t All but nine children walked before 18 months.
TABLE 6MOST FREQUENTLY MISPRONOUNCED, SUBSTITUTEDOR OMITTED SOUNDS IN 80 CHILDREN WITH SPECIFIC
DEVELOPMENTAL SPEECH DISORDERS
Group 1* Group 2tSounds % with % with
defective sounds defective sounds
r 78 37(sh) 74 15(thing) 66 31
s 63 51 62 1k 36 12f (church) 34 13d3 (hedge) 34 13g 26 9f 20 6v 17 _p 17 1b 17 _
* 80 children with specific developmental speech disorders.t Sample group of 112 unselected children aged 3k years (Morley,
1957).
TABLE 7LOCAL ABNORMALITIES OF THE ARTICULATORY APPARATUS IN 80 PATIENTS WITH SPECIFIC DEVELOPMENTAL
SPEECH DISORDERS
Associated with Abnormal NotAssociated
Abnormalities Palatal Tongue Palatal with any TotalMovements Movements and Tongue Local
Movements Interference
Enlarged tonsils only .........1 0 1 5 7Enlarged adenoids only . . .. .. .. . 0 3Enlarged tonsils and adenoids .1 2 1 7 11Hypomandibulosis . .0 2 0 0 2Other malocclusion and dental abnormalities, e.g., open
bite, diastasis of incisors .0 2 0 2 4Tongue thrust only .......0 1 0 0 1
Total.3 8 3 14 28* ~ ~~~__ __
452
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from
CLASSIFICATION OF SPEECH DISORDERS IN CHILDREN
Frequently minor abnormalities of the articula-tory apparatus are observed in patients with specificdevelopmental speech disorders. Those found in thepresent series are shown in Table 7. In many
patients (14 of the 28 with local abnormalities) nointerference with the function of the articulatoryorgans could be demonstrated. In the remainderit required only a rudimentary knowledge ofphonetics to realize that the local abnormalitiescould not be held responsible for the complex speechdisturbance, often affecting language as well asarticulation of a wide variety of sounds.
Abnormalities of behaviour are frequent inpatients with specific developmental speech dis-orders. In the majority of cases they appear to besecondary to the speech defect. Obviously thesituation in which an intelligent child with a speechdefect often finds himself is stressful. He is deprivedof the means to communicate his ideas, frequently insocial circumstances where much attention is paidto language and articulation. Later on specificeducational difficulties may also be present.
His reactions to this situation may be by with-drawal. Solitariness, inability to play with otherchildren, day-dreaming, excessive dependence onthe mother, and fearfulness were complained of in18 of the patients. Four others seemed unusuallytense, excitable and tearful. Four reacted tofrustration by severe temper tantrums. Three (overthe age of 4 years) were enuretic.
Mixed Cases and Unclassified Cases. In aclassification whose categories are defined in termsof the single major speech disability it is inevitablethat a small number of patients with multiple defectscould fall into more than one of the major categories.Provision is made for them by having a category for'mixed cases'. There were only four such patientsin the present series. They included one child withsevere hypomandibulosis, cerebral diplegia causingimpaired voluntary movement of the articulatoryorgans and mental defect. Another had a cleft palateand suffered from nerve deafness following tuber-culous meningitis.A few patients resist classification even after full
investigation and they are provided for in thecategory of 'other and unclassified cases'. Thiscategory may be compared to a basket of corres-pondence marked 'pending', from which cases willbe taken and placed in other categories when moreaccurately diagnosed.
DiscussionThat there is a need for an adequate description
of speech disorders in childhood cannot be doubted
by anyone who has to deal with children sufferingfrom speech defects, or by anyone acquainted withthe currently accepted literature on the subject(Seth and Guthrie, 1935; Van Riper, 1947). Un-fortunately the amount of clinical investigationdevoted to disorders of children's speech has beenrelatively small. Much of it has been the result ofspeech therapists, phoneticians, linguists, otologists,neurologists or psychologists working in isolation.Yet the problems of accurate diagnosis cannot besolved by a lone worker from one of these disciplines,however expert he may be. Classification based onthe clinical findings which seem to be important toa worker in any one of these sciences is bound to beinadequate for other workers with differing pointsof view.The benefits of a team approach to speech
problems in childhood have not been sufficientlyrealized, though the work of Miss Muriel Morleyand her colleagues shows that it may be rewarding(Morley, Court and Miller, 1950; Morley, Courtand Miller, 1954; Morley, Court, Miller and Gar-side, 1955; Morley, 1957). Their pioneer descrip-tions and classification of speech defects in childhoodmark a significant advance on previous work anddeserve close study and criticism (Table 8).
TABLE 8CLASSIFICATION OF SPEECH DEFECTS IN CHILDHOOD
BY MORLEY (1957)
Delayed Development of Speech:Due to psychogenic retardationDue to mental retardationDue to hearing defectsDue to developmental aphasia
Defective Articulation:Developmental dysarthriaDevelopmental articulatory apraxiaDyslaliaDue to partial hearing lossDue to structural (local) abnormalities
Stammering
It will be seen that an attempt is made to dis-tinguish between 'delayed development of speech'and 'defective articulation' as major categories.Unfortunately this ignores the fact that a high pro-portion of patients with 'delayed development ofspeech' have defective articulation, and a significantnumber with 'defective articulation' have retardedspeech development.The definition of a number of the sub-categories
is unsatisfactory, and sometimes misleading. Thus72 of her 74 patients considered to suffer from'developmental aphasia' are regarded as sufferingfrom 'executive aphasia' because they showed nodifficulty in comprehending speech at the time ofexamination, though their speech development wasretarded. The term 'executive aphasia' has a very
453
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from
ARCHIVES OF DISEASE IN CHILDHOOD
specific meaning in adult neurology. It is misusedwhen it is applied to children with retardation oflanguage development merely because they have noobvious difficulties of comprehension. If speechwere merely the issuing through the mouth ofsequences of sounds which had been poured into thechild's ear, as if through a pipeline, there might besome justification for using the term in this way.But the processes involved in the perception, com-prehension and utterance of speech are incrediblycomplicated and still poorly understood. To assumethat a child suffers from 'executive' or even 'expres-sive aphasia' because the end result of this processis defective, though the child appears to comprehendspeech, is an unjustified simplification of anextremely complicated problem.The term 'developmental articulatory apraxia' is
open to severe criticism. It implies that appreciationof the movements made by the articulatory organsduring speech is so defective that accurate articula-tion is impossible. Yet it is usually impossible todemonstrate any abnormality of movement onexamination, as the author admits. The assumptionshe makes that apraxia is troublesome only withfine movements required by speech is more ingeniousthan convincing. The use of the term 'apraxia', adescriptive neurological term, is probably bestavoided until means of testing for apraxia of tongue,lips and palate during speech are available.The fact that five of 12 children with 'develop-
mental articulatory apraxia' who were closely studiedby Morley and her colleagues had 'some delay inthe first use of words; and phrases were notattempted before 4 years', suggested similarities tohistories of patients she classifies as suffering from'developmental aphasia'. Nine of the 15 childrenwith 'developmental aphasia' had 'defective articu-lation'. There seems to be a good case for groupingtogether patients with these two conditions into asingle major category of 'specific developmentalspeech disorders', in which retardation of thedevelopment of language and articulation are themajor characteristics. This suggestion is followedin the present classification.
It will be noted that the classification dispenseswith the category of 'dyslalia' which occurs in MissMorley's classification. The term dyslalia is usedvery indiscriminately by clinicians to refer to a widevariety of speech disorders in childhood. EvenMorley (1957) does not provide a satisfactorydefinition though most of the patients she includesin the category appear to suffer from transient,usually mild, disorders of articulation not associatedwith obvious abnormalities of the movements of thearticulatory organs or with retardation of speech
development. She suggests that 'dyslalia' may beassociated with mental defect, 'environmental andpsychogenic factors', and imitation or persistence offaulty patterns of articulation. Many of the casesin this category could obviously be placed in otherof her categories. In view of this and the widemisuse of the term dyslalia, it has been thought bestto discard it.The term 'developmental dysarthria' is misleading.
The adjective 'developmental' implies that thedisorder will disappear or be very much amelioratedwith maturation. Yet many of the patients in thecategory of 'developmental dysarthria' suffer fromcerebral palsy and other neurological abnormalities.In them the improvement in speech tends to beextremely disappointing, especially after the age of5 or 6 years. In this sense their speech disorderscannot be regarded as being 'developmental'.The aim in the present classification has been to
define the categories of children's speech disordersin terms of the major abnormality of speech whichis present, and by the child's associated clinical andpsychological abnormalities. Clearly such a classi-fication requires that patients shall be fully studiedfrom a number of different points of view. Thisrequires a team approach in modern conditions,similar to that used in cerebral palsy and childguidance clinics. If such a team approach cannotbe adopted, accuracy of diagnosis of speech defectssuffers, and the classification accordingly becomesless useful.
SummaryDescriptions of the commoner defects of speech
encountered in a hospital speech clinic largelydevoted to the treatment of pre-school children havebeen presented.A new classification of speech disorders in child-
hood based on the major defect of speech and onassociated clinical and psychological findings isgiven. It is emphasized that accurate diagnosis andclassification of speech defects requires a teamconsisting of speech therapist, psychologist, paedi-atrician and otologist. The help of a social worker,neurologist, phonetician, child psychiatrist and otherhospital staff may be required in both diagnosis andtreatment.
Criticisms are made of the classification of speechdefects proposed by Morley (1957) on the groundsof the imprecise use of a few neurological terms andthe lack of clear definition of some of the categoriesproposed, in terms of clinical findings.
I have to thank Miss Morrison, Speech Therapist tothe Royal Hospital for Sick Children, Edinburgh, andher assistants for their co-operation and interest during
454
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from

CLASSIFICATION OF SPEECH DISORDERS IN CHILDREN 455the investigation. I am indebted to Miss Mason, latelyof the Psychology Department, University of Edinburgh,and Miss Mary Waller for the psychological examina-tions, Miss Sylvia Massey of the Department of Psycho-logical Medicine for her psychiatric soCial reports, andDr. Margaret Methven of the same Department for herconsistent co-operation and help. Dr. Werner Schuttexamined many of the patients from the paediatric pointof view. I must thank Professor R. W. B. Ellis for hisstimulus and encouragement of this work, and thephysicians and surgeons of the Royal Hospital for SickChildren for their interest and co-operation during it.I am grateful to Mr. Ian Catford, Director of the Schoolof Applied Linguistics, University of Edinburgh, who wasgood enough to criticize this paper.
REFERENCESBirrell, J. F. (1954). Speech, 18, 40.Calnan, J. (1957). Ibid., 21, 59.Critchley, M. (1952). J. Laryng., 66, 1.Drew, A. L. (1956). Brain, 79, 440.Evans. P. R. (1955). Archives of Disease in Childhood, 30, 237.Francis, T. R. (1958). Speech Path. and Therapy, 1, 70.
Gibb, A. G. (1958). J. Laryng., 72, 433.Hallgren, B. (1950). Acta psychiat. scand., Suppl. 65.Henderson, J. L. (1939). Brain, 62, 381.Ingram, T. T. S. (1956). J. ment. Sci., 102, 550.
and Reid, J. F. (1956). Archives of Disease in Childhood, 31,161.
Johnson, W., Brown, S. F., Curtis, J. F. Edney, C. W. and Keaster, J.(1948). Speech Handicapped School Children. Harper, NewYork.
Monrad-Krohn, G. H. (1947). Acta psychiat. scand., Suppl. 46, 204.Morley, M. E. (1954). Cleft Palate and Speech, 3rd ed. Livingstone,
Edinburgh.(1957). The Development and Disorders of Speech in Childhood.Livingstone, Edinburgh.Court, D. and Miller, H. (1950). Brit. med. J., 1, 574.
(1954). Ibid., 1, 8.T- and Garside, R. F. (1955). Ibid., 2, 463.
Orton, S. T. (1937). Reading, Writing and Speech Problems inChildren Chapman and Hall, London.
Ounsted, C. (1955). Lancet, 2, 303.Registrar General for Scotland (1951). Ninety-seventh Annual
Report. H.M.S.O.Seth, G. and Guthrie, D. (1935). Speech in Childhood: Its Develop-
ment and Disorders. Oxford University Press, London.Travis, L. E. (1931). Speech Pathology. Appleton, New York.Van Riper, C. (1947) Speech Correction-Principles and Methods,
2nd ed. Prentice-Hall, New York.Wilson, S. A. Kinnier (1954). Neurology, 2nd ed. Edited by A. N
Bruce. Butterworth, London.
copyright. on 26 M
ay 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.34.177.444 on 1 October 1959. D
ownloaded from





























