Embed Size (px)
Citation preview
Facility Revenue Workshop
EDDA 2 2019Michael A. Granovsky MD CPC FACEP
President, LogixHealth
▪ Regulatory Update for Off Campus EDs▪ Accurate Charge Capture▪ Picking a charge capture algorithm▪ Implementation of revenue capture best
practices
Taking It To The Next Level
June 2017 Report to Congress by the Medicare Payment Advisory Commission (MedPAC)
“In recent years, there has been significant growth in the number of health care facilities located apart from
hospitals that are devoted primarily to emergency department services. This includes both off-campus
provider-based emergency departments that are eligible for payment under the OPPS and independent
freestanding emergency departments not affiliated with a hospital that are not eligible for payment under the
OPPS.”
2019 Off Campus Provider Based Emergency Departments
- Page 586/1182 2019 OPPS Final Rule
“Med Pac and others have expressed concerns that services may be shifting to the higher cost emergency departments due to higher payment rates for services performed in off campus provider based emergency departments…..due to the exemption for services provided in an emergency department included under section 603 of the Bipartisan Budget Act of 2015 (Pub. L. 114-25), whereby all items and services (emergency and nonemergency) furnished in an emergency department are excepted from the payment implications of section 603.”
2019 Off Campus Provider Based Emergency Departments
- Page 587/1182 2019 OPPS Final Rule
“We agree with MedPAC’s recommendation and believe we need to develop data to assess the extent to which OPPS services are shifting to off-campus provider-based emergency departments. Therefore, we announced in the CY 2019 OPPS/ASC proposed rule (83 FR 37138) that we are implementing through the subregulatoryHCPCS modifier process a new modifier for this purpose, effective beginning January 1, 2019.”
“We stated in the proposed rule that we will create a HCPCS modifier “ER”—Items and services furnished by a provider-based off-campus emergency department) that is to be reported with every claim line for outpatient hospital services furnished in an off-campus provider-based emergency department. We specified in the proposed rule that the modifier would be reported on the UB–04 form for hospital outpatient services. We stated that critical access hospitals (CAHs) would not be required to report this modifier.”
2019 OPPS Provider Based Emergency Departments Reporting Detail
- Page 588/1182 2019 OPPS Final Rule
ED Facility Charge Capture
▪ ED Facility E/M leveling– Key Area for financial performance– Need accurate charge capture– Frequently undervalued services
ED Facility Revenue Cycle:Major Components
“CMS has instructed hospitals to report facility resources for clinic and emergency department visits using CPT E/M codes and to develop internal hospital guidelines to determine what level of visit to report for each patient.”
OPPS Final Rule
ED Facility Level Assignment
“In the CY 2019 OPPS proposed rule, we proposed to continue with our current emergency department hospital outpatient visits payment policies. We sought public comments on any changes to these codes. We did not receive any public comments on our proposals to continue our current ED hospital outpatient visits payment policies Therefore, we are adopting these proposals as final without modification.”-2019 OPPS Final Rule page 520/1182
2019 ED Facility Guidelines Update
MedPAC Report to Congress to relook at national guidelines 2022

▪ Facilities must develop their own guidelines▪ Must relate to resource use and be consistently
appliedOptions
– Home grown versions– Point systems– ACEP Guidelines– EMR—not able to put it over the finish line
• Nurses use free text areas so automated suggested coding can be unreliable
• Infusions/injections
Facility Level Guidelines
▪ Uses common ED interventions determine Level – Procedures– Monitoring– Transportation– Tests– Complexity Of Discharge Instructions
▪ Developed by: The American College of Emergency Physicians CNAC – Interventions– Examples
▪ Established nationally applied guidelines
ACEP Model
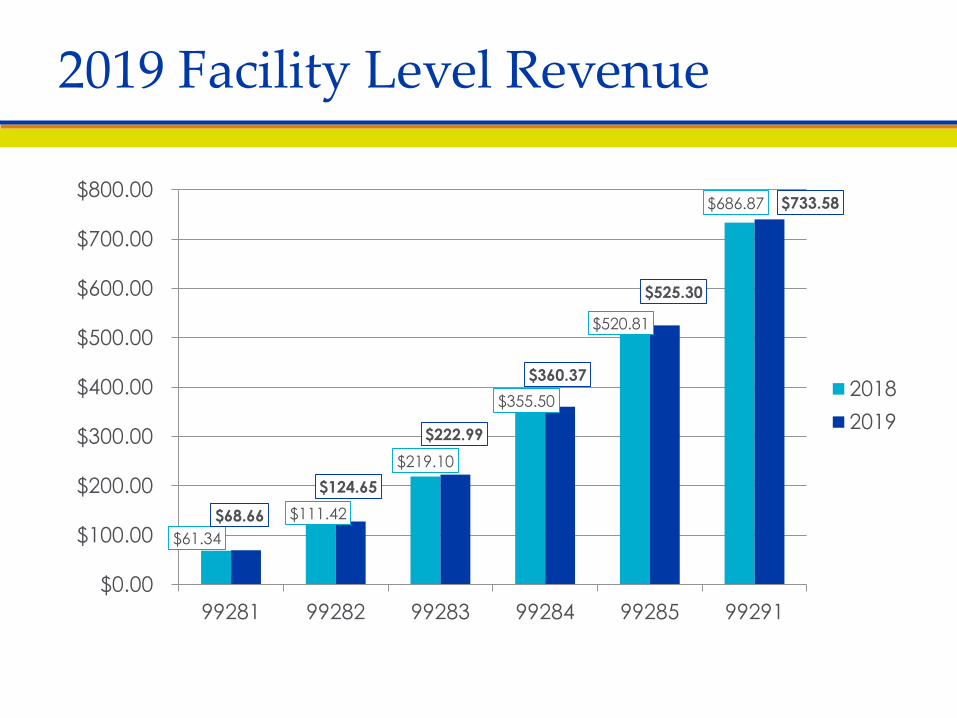
$61.34 $111.42
$219.10
$355.50
$520.81
$686.87
$68.66
$124.65
$222.99
$360.37
$525.30
$733.58
$0.00
$100.00
$200.00
$300.00
$400.00
$500.00
$600.00
$700.00
$800.00
99281 99282 99283 99284 99285 99291
20182019
2019 Facility Level Revenue
▪ Increased packaging of services in to the E/M level
▪ OPPS becoming even more of a prospective payment
▪ Less like a fee schedule
Putting the “Prospective” in OPPS
▪ ED services Status Indicator (S.I.) V
▪ Bundling and Q Status Indicators
2019 ED Packaging Increases
V Emergency Department Paid under OPPS; separate APC payment.
Q1 STV-Packaged Codes Q2 T-Packaged Codes Q3 Codes that may be paid through a Composite APCQ4 Conditionally packaged laboratory tests
▪ ED Services as S.I. V will package many services▪ Q1 continues to expand
– Packaged with S, T, or V– Many laceration repairs
▪ Packaging continues to increase– Most plain films and most labs (Q4), Some US– Minor procedures (e.g. lacerations Q1)– Foley, TC of EKG (Q1)
2019 ED Packaging
2019 OPPS Final Rule:“The OPPS packages payments for multiple interrelated items and services into a single payment to create incentives for hospitals to furnish services most efficiently and to manage their resources with maximum flexibility. Our packaging policies support our strategic goal of using larger payment bundles in the OPPS to maximize hospitals’ incentives to provide care in the most efficient manner.”
-2019 OPPS Final Rule page 111/1182
Increased ED Packaging: Why?
▪ CMS is telegraphing the vision of increased bundling
▪ Packaging of services rewards those hospitals which are resource conscious
▪ There is cost for labs/US/plain films but no additional payment
▪ Proposal to bundle medication services
Are you measuring ancillary utilization?
Impact of Increased Packaging
Putting The Guidelines To Use
▪ Initial Assessment▪ No medication or treatments▪ Rx refill only, asymptomatic▪ Note for Work or School▪ Wound recheck▪ Booster or follow up immunization, no acute injury▪ Dressing changes (uncomplicated)▪ Suture removal (uncomplicated)▪ Discussion of Discharge
99281
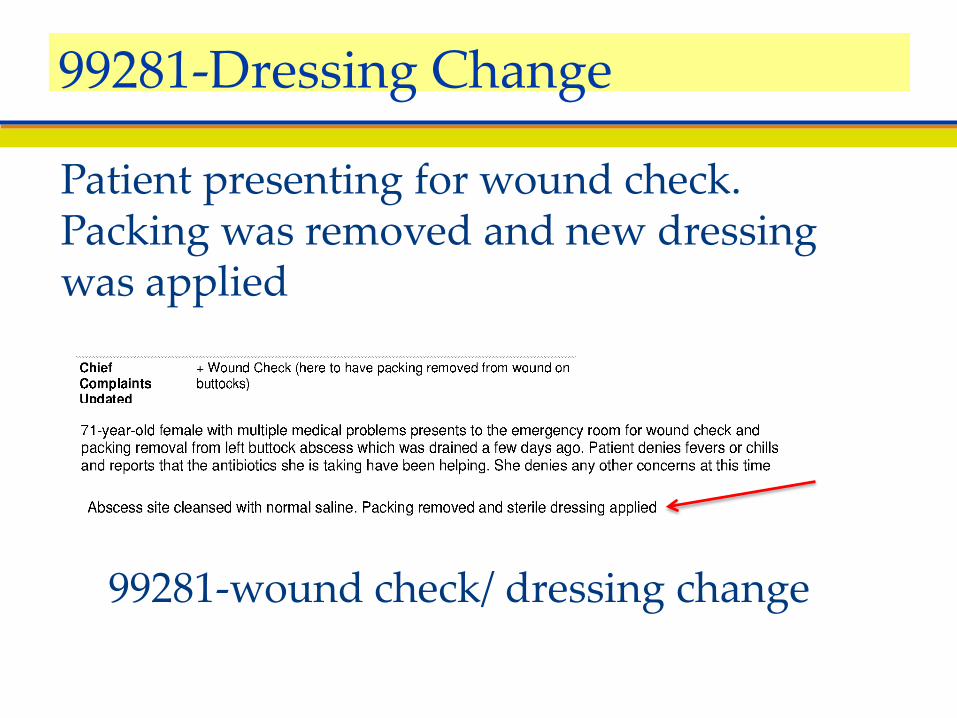
Patient presenting for wound check. Packing was removed and new dressing was applied
99281-wound check/ dressing change
99281-Dressing Change
▪ Tests by ED staff: – Urine dip– Accucheck
▪ Visual acuity ▪ Simple DC instructions▪ Simple procedures
– Minor laceration– Simple abscess
99282
▪ Localized skin rash, lesion, sunburn▪ Minor viral infection▪ Eye discharge- painless▪ Ear Pain▪ Urinary frequency without fever▪ Simple trauma (with no X-rays)
99282 Clinical Presentations
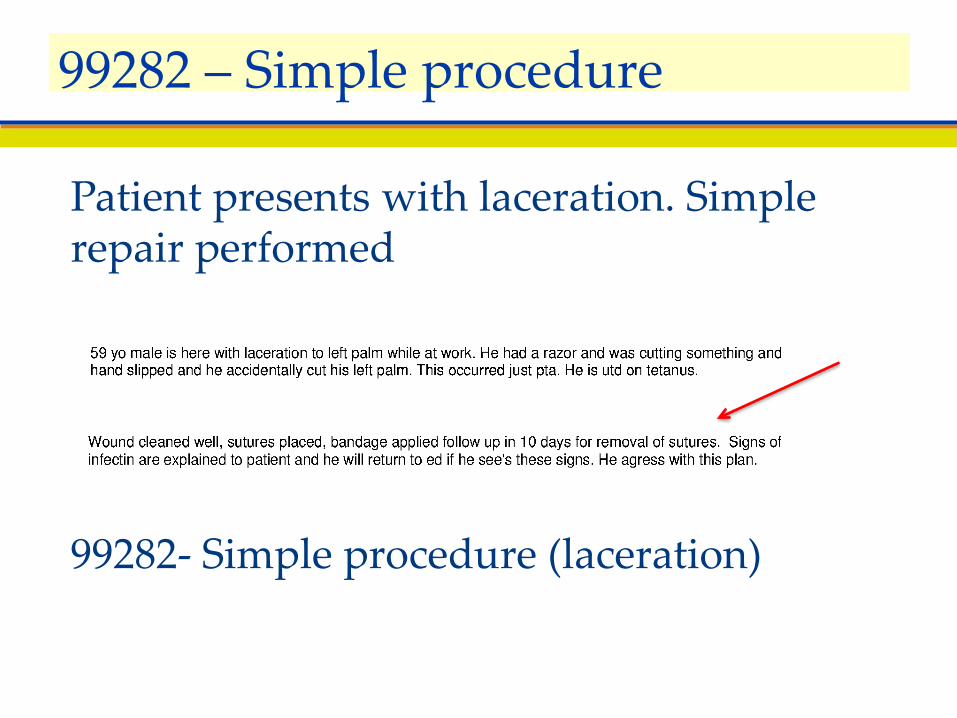
Patient presents with laceration. Simple repair performed
99282- Simple procedure (laceration)
99282 – Simple procedure
▪ Receipt of EMS patient▪ Heparin/saline lock▪ 1 Nebulizer treatment▪ Blood draws (8000 series)▪ EKG▪ Plain X-rays 1 area▪ PO Presc. Medications▪ Foley & I/O cath.▪ Procedures: joint
aspiration, simple fracture care etc.
▪ Routine psych medical clearance
▪ Limited social worker intervention
▪ Post mortem care▪ Direct Admit via ED
99283
▪ Minor trauma▪ Prescription drug management▪ Fever which responds to antipyretics ▪ Headache - Hx of, no serial exam▪ Head injury- without neurologic symptoms▪ Eye pain ▪ Mild dyspnea -not requiring oxygen
99283 Clinical Presentations
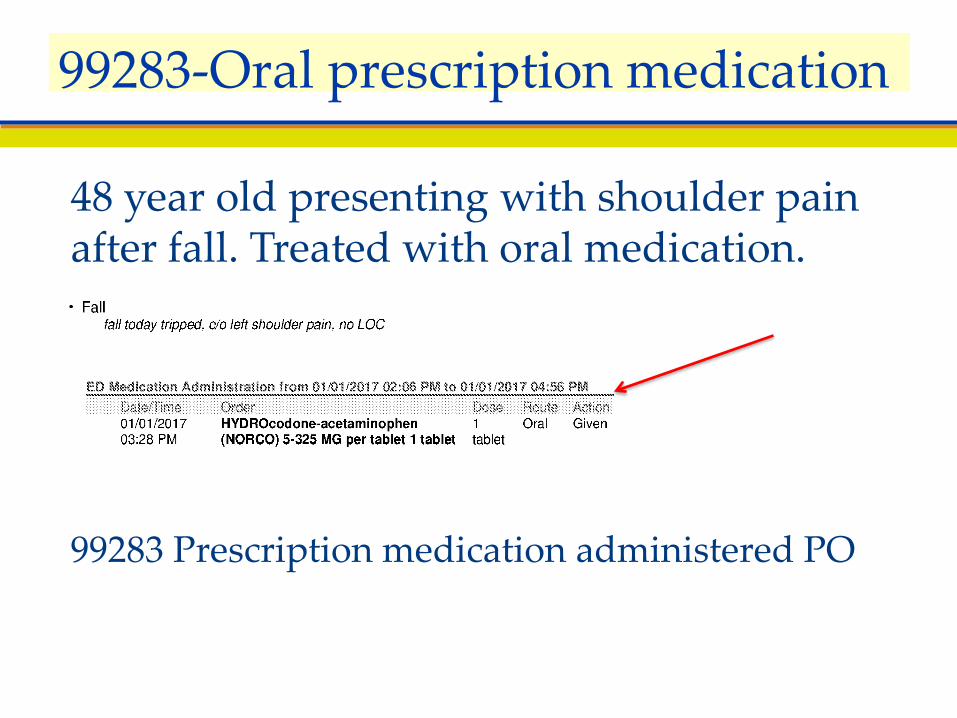
48 year old presenting with shoulder pain after fall. Treated with oral medication.
99283 Prescription medication administered PO
99283-Oral prescription medication
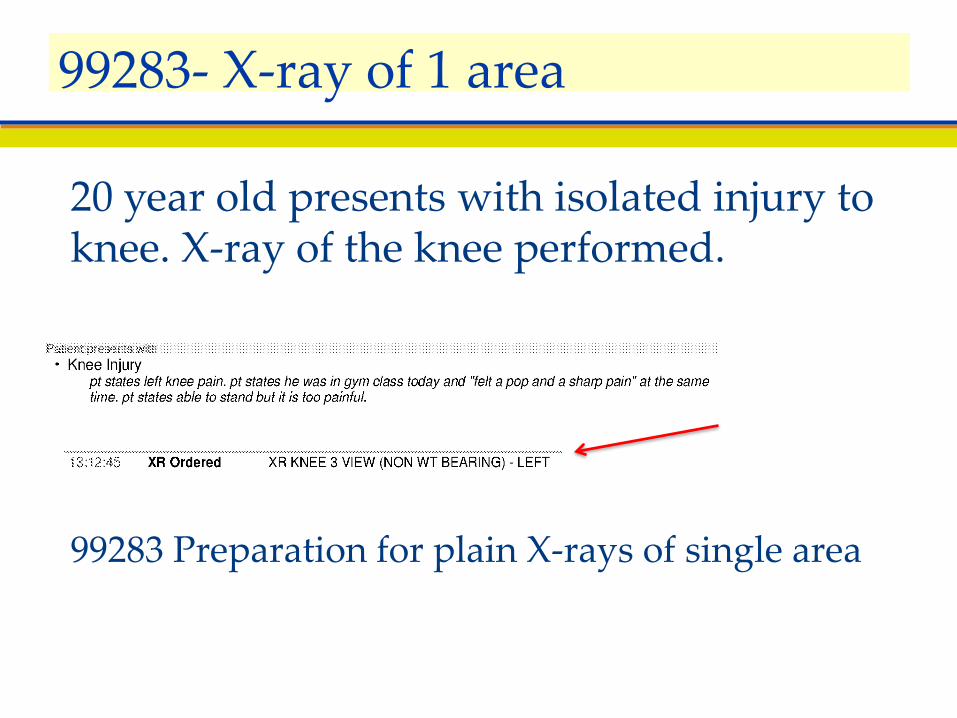
20 year old presents with isolated injury to knee. X-ray of the knee performed.
99283 Preparation for plain X-rays of single area
99283- X-ray of 1 area
Interventions▪ Plain x-ray multiple areas▪ MRI, CT, VQ Scans, US ▪ Cardiac monitoring▪ Multiple reassessments▪ Parenteral medications▪ 2 nebulizer treatments ▪ Parenteral medications▪ Discharge instructions complex
99284
▪ Headache with nausea/ vomiting▪ Dehydration requiring treatment▪ Dyspnea requiring oxygen▪ Respiratory illness with (2) nebulizer treatments▪ 2 diagnostic tests (e.g. chem 7 and CT)
– Chest pain– Abdominal pain– Neuro complaints
▪ Non-menstrual vaginal bleeding
99284 Clinical Presentations
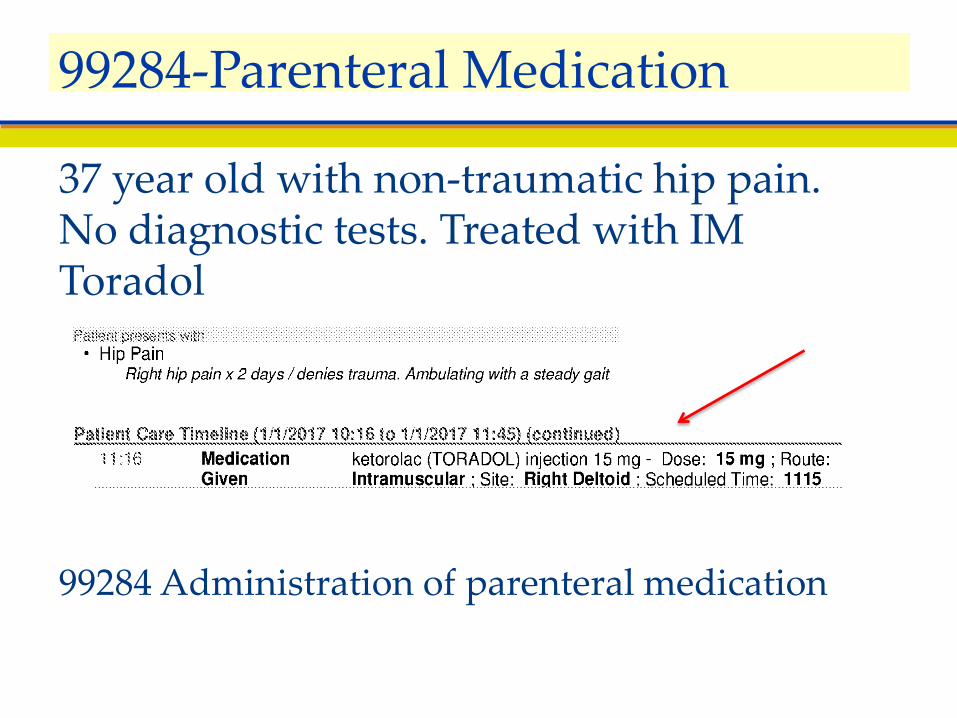
37 year old with non-traumatic hip pain. No diagnostic tests. Treated with IM Toradol
99284 Administration of parenteral medication
99284-Parenteral Medication
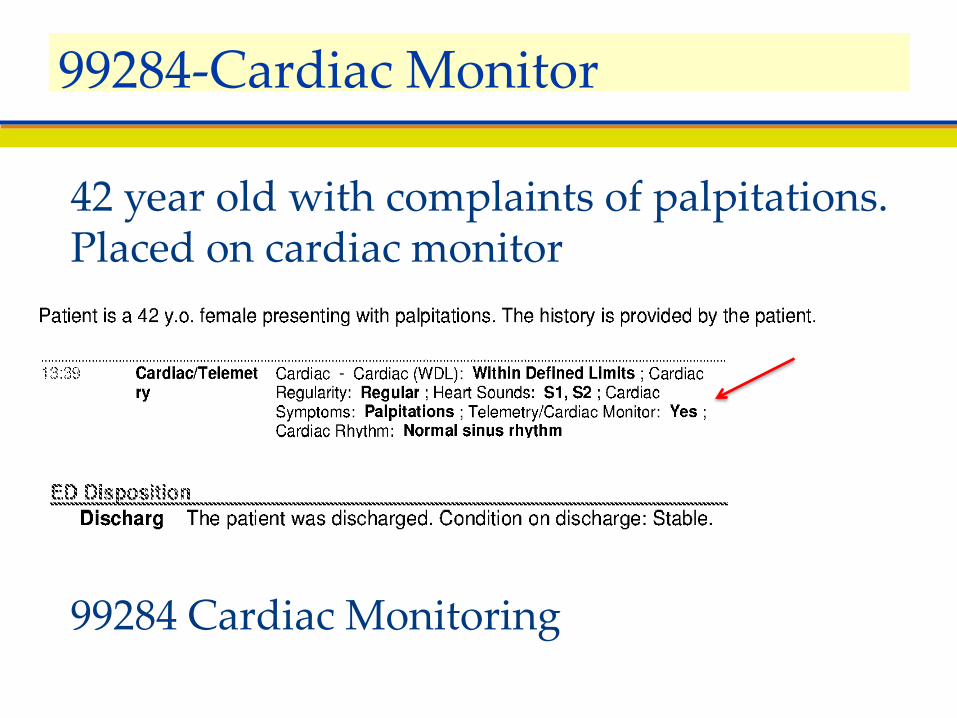
42 year old with complaints of palpitations. Placed on cardiac monitor
99284 Cardiac Monitoring
99284-Cardiac Monitor
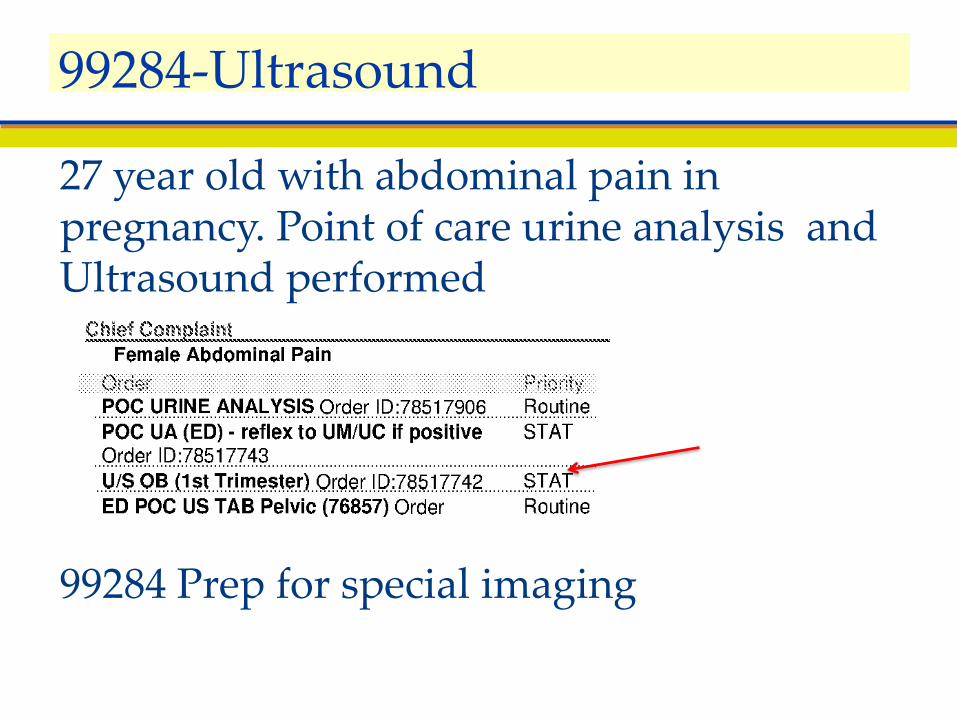
27 year old with abdominal pain in pregnancy. Point of care urine analysis and Ultrasound performed
99284 Prep for special imaging
99284-Ultrasound
▪ 37 year old with right flank pain▪ IV pain medication given
– Non-narcotic▪ CT scan of abdomen/pelvis
– No nurse monitoring required during study▪ Prescription provided for Percocet
99284 Vignette
▪ Frequent monitoring of multiple vital signs (e.g. 02 sat, BP, rhythm, RR
▪ Preparation for ≥ 3 diagnostic tests: (Labs, EKG, X-ray)▪ Prep for special imaging study (CT, MRI, Ultrasound)
with : parenteral medication; oral or IV contrast▪ Multiple Nebulizer Treatments: (3) or more, 1 hr. cont.▪ Procedures : central line insertion, gastric lavage, LP,
paracentesis▪ Coordination of hospital admission/ transfer or change
in living situation or site
99285
▪ New-onset altered mental status▪ Headache (severe): CT and/or LP▪ Chest Pain--multiple diagnostic tests/treatments▪ Respiratory illness--relieved by (3) or more
nebulizer▪ Abdominal Pain--multiple diagnostic
tests/treatments▪ Uncontrolled DM▪ Major musculoskeletal injury▪ Mental health problem - suicidal/ homicidal
99285 Clinical Examples
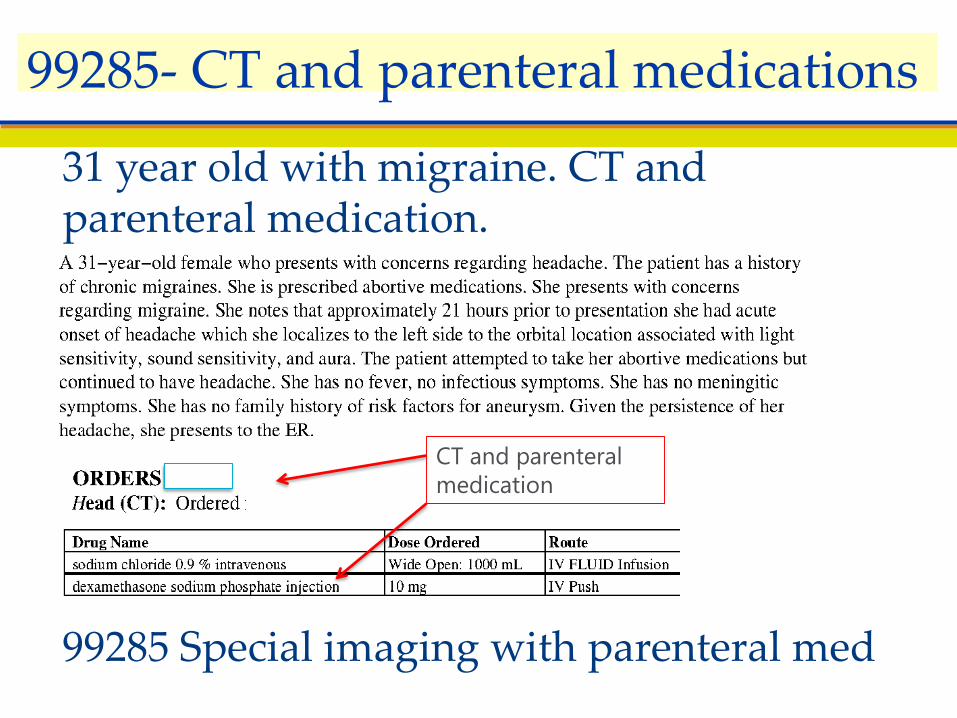
31 year old with migraine. CT and parenteral medication.
99285 Special imaging with parenteral med
99285- CT and parenteral medications
CT and parenteral medication
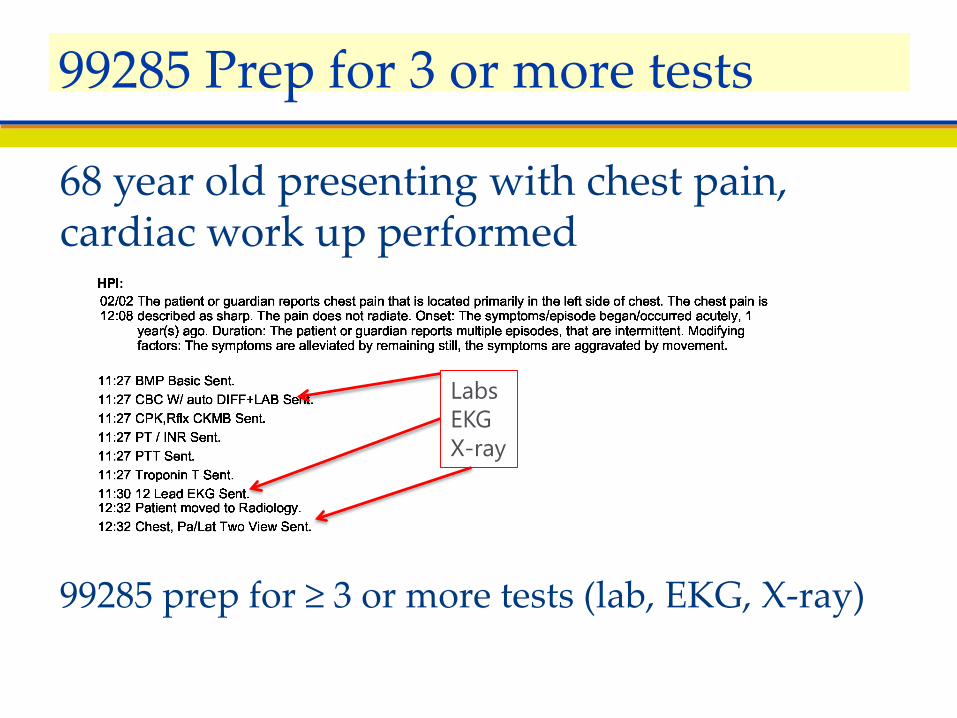
68 year old presenting with chest pain, cardiac work up performed
99285 prep for ≥ 3 or more tests (lab, EKG, X-ray)
99285 Prep for 3 or more tests
LabsEKGX-ray
19 y.o healthy male presents for suture removal from well healed wound.What ED Facility Level might be assigned?
-99283-99282-99281-99281**
Audience Vignette 1
27 y.o. male presents with ankle sprain after tripping playing basket ball. X ray of the ankle is negative and he is DC’d home with an Rx for motrin.What ED Facility Level would be assigned?
-99282-99284-99283-99283**
Audience Vignette 2
37 y.o. female presents with fleeting atypical chest pain for 2 seconds at a time. She has no family history of CAD and had a normal stress test as part of a routine physical 2 years ago. Cardiac work up with EKG, CBC, 7, CPK, Trop, and CXR are negative and she is DC’d home.What ED facility Level would be assigned?-99284-99285-99283
Audience Vignette 3
Prep for 3 or more diagnostic test
▪ 70,000 visit ED▪ Level 1 trauma center▪ ED coding using institutional specific
guidelines▪ Partial use of EMR ▪ No updating of processes▪ No consistent coder training or QA
process
APC Task Force Model Experience
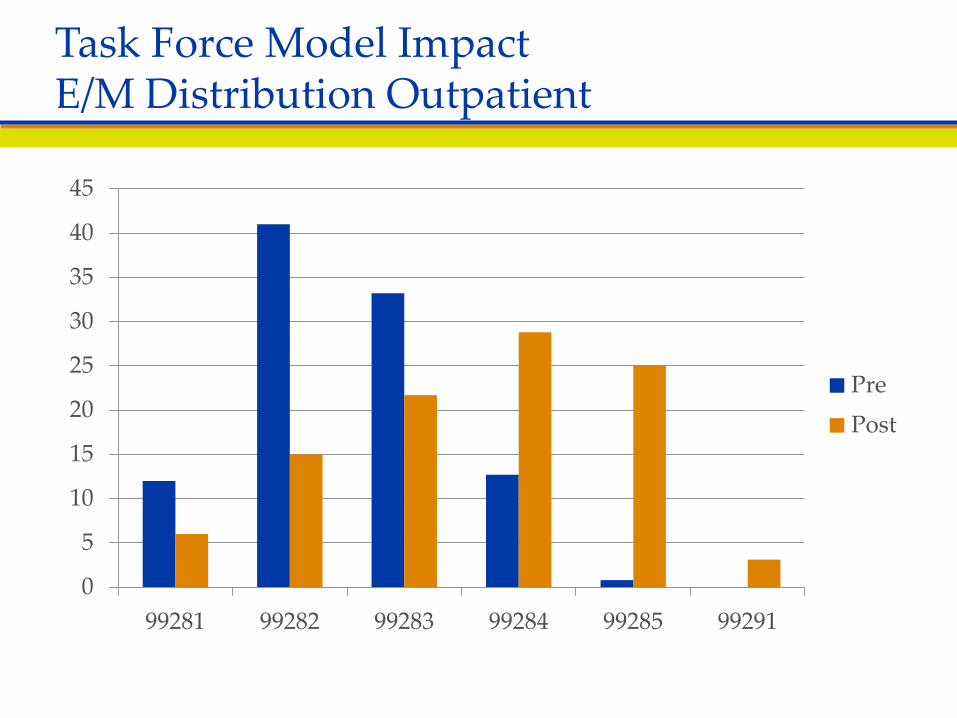
0
5
10
15
20
25
30
35
40
45
99281 99282 99283 99284 99285 99291
PrePost
Task Force Model ImpactE/M Distribution Outpatient
▪ Increase in over $40 per patient▪ Over $3,500,000 in additional charges▪ ED revenue center went from a $2m loss
to a $1.1M profit▪ Changed the entire economic perception
of the ED
Economic ImpactAPC Task Force Facility Coding System
▪ Review annually:– Consistency of Documentation– Updated Chargemaster– E/M Level assignment tool– Coding review with aggregate data or audit
Best Practices
Michael A. Granovsky MD CPC FACEP
President, Logix Healthwww.logixhealth.com
Contact Information