Embed Size (px)
Citation preview
Archives ofDisease in Childhood 1990; 65: 1162-1164
Capillary haemangioma presenting as a lungpseudocyst
J J Bowyer, M Sheppard
AbstractA girl who developed a lung cyst at 24 hours ofage during gentle ventilation for respiratorydistress syndrome is reported. Instead ofresolving as expected of a pseudocyst itcontinued to expand. Resection at 1 year ofage showed a cyst entirely surrounded bycapiliary haemangioma. Aspiration of thiscyst would have been dangerous.
Pulmonary pseudocyst formation is a recognisedcomplication of ventilation in neonates withrespiratory distress syndrome. We report aninfant where the cyst did not resolve as ex-pected. '
Case reportA girl of 30 weeks' gestation and birth weight1200 g was born by emergency caesarean sectionfor abruption. Dates were confirmed by an earlyscan and the pregnancy had been normal until
Department ofPaediatrics,St Peter's Hospital,Guildford Road,Chertsey, SurreyKT16 OPZJ J BowyerDepartment ofPathology,Brompton Hospital,LondonM SheppardCorrespondence to:Dr Bowyer.Accepted 10 May 1990
slowing of fetal growth at 28 weeks. She wasintubated and ventilated for five minutesinitially and reintubated at 15 minutes forrecession and cyanosis in 60% oxygen.
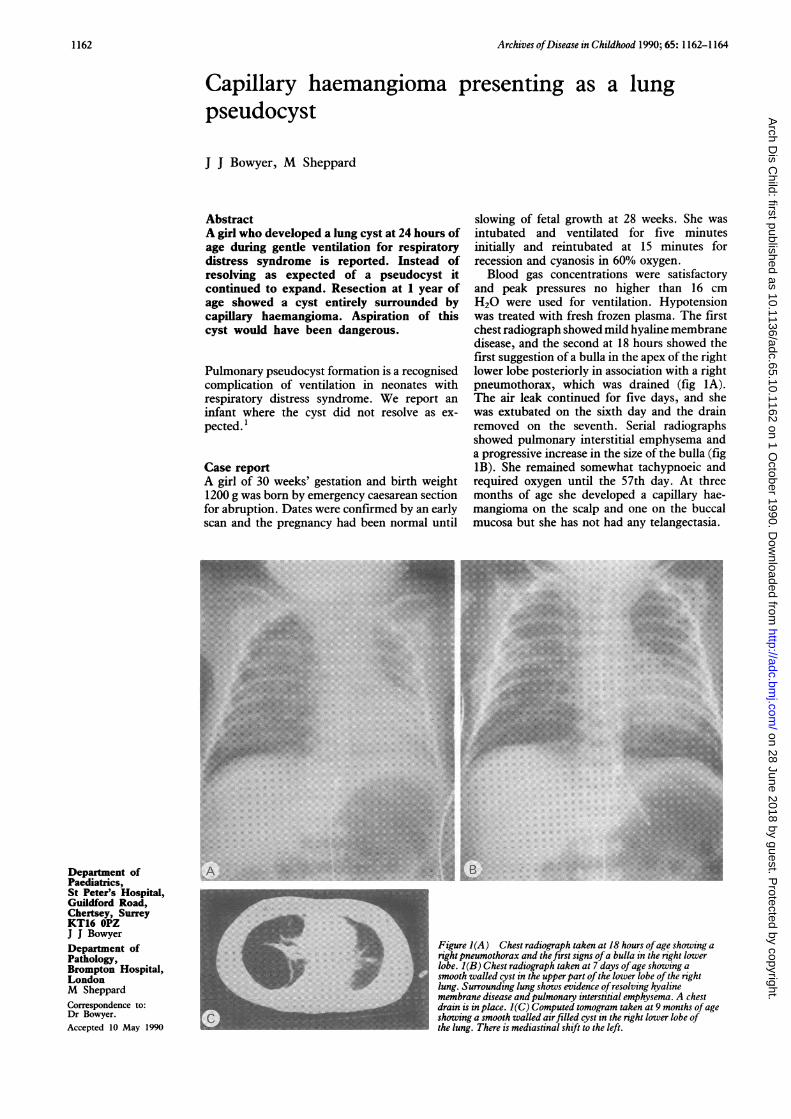
Blood gas concentrations were satisfactoryand peak pressures no higher than 16 cmH20 were used for ventilation. Hypotensionwas treated with fresh frozen plasma. The firstchest radiograph showed mild hyaline membranedisease, and the second at 18 hours showed thefirst suggestion of a bulla in the apex of the rightlower lobe posteriorly in association with a rightpneumothorax, which was drained (fig IA).The air leak continued for five days, and shewas extubated on the sixth day and the drainremoved on the seventh. Serial radiographsshowed pulmonary interstitial emphysema anda progressive increase in the size of the bulla (fig1B). She remained somewhat tachypnoeic andrequired oxygen until the 57th day. At threemonths of age she developed a capillary hae-mangioma on the scalp and one on the buccalmucosa but she has not had any telangectasia.
Figure 1(A) Chest radiograph taken at 18 hours ofage showing aright pneumothorax and the first signs ofa bulla in the right lowerlobe. I(B) Chest radiograph taken at 7 days ofage showing asmooth walled cyst in the upper part ofthe lower lobe ofthe rightlung. Surrounding lung shows evidence ofresolving hyalinemembrane disease andpulmonary interstitial emphysema. A chestdrain is in place. I(C) Computed tomogram taken at 9 months ofageshowing a smooth walled airfilled cyst in the right lower lobe ofthe lung. There is mediastinal shift to the left.
1162
on 28 June 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.10.1162 on 1 October 1990. D
ownloaded from
Capillary haemangioma presenting as a lung pseudocyst
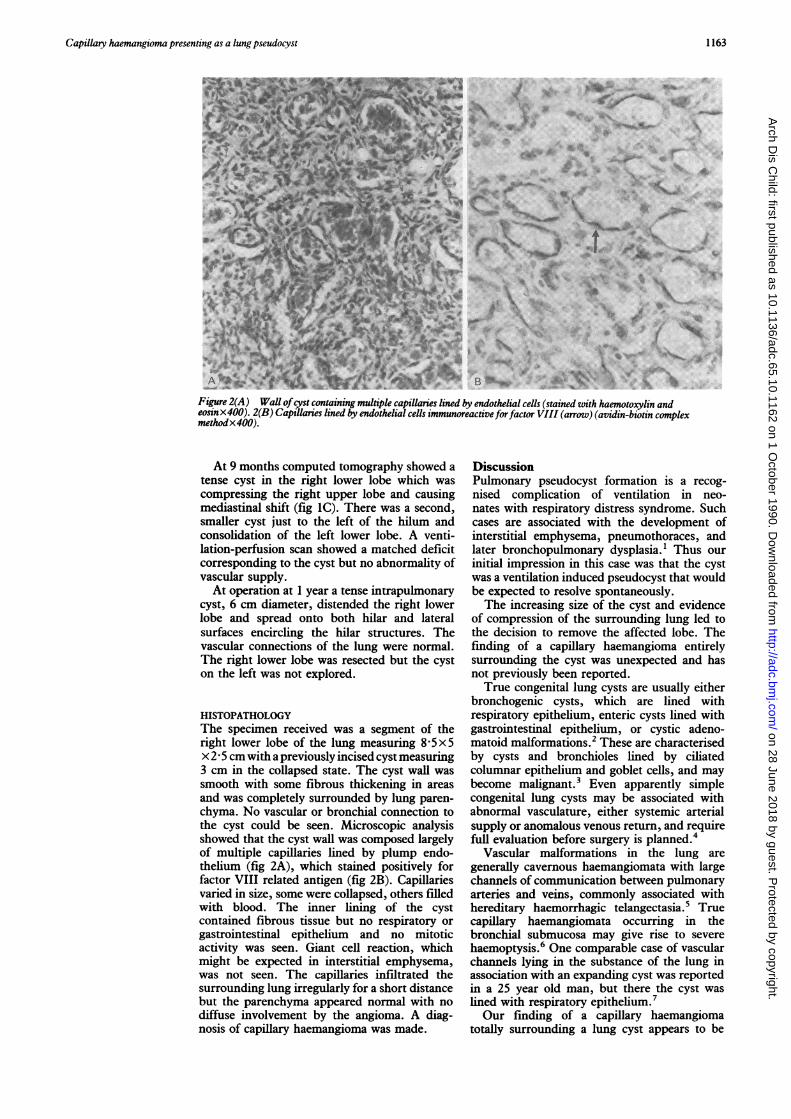
Figure 2(A) Wall ofcyst containing multiple capillaries lined by endothelial cells (stained with haemotoxylin andeosinx400). 2(B) Capillaries lned by endothelial cells immunoreactiveforfactor VIII (arrow) (avidin-biotin complexmethodx400).
At 9 months computed tomography showed atense cyst in the right lower lobe which wascompressing the right upper lobe and causingmediastinal shift (fig IC). There was a second,smaller cyst just to the left of the hilum andconsolidation of the left lower lobe. A venti-lation-perfusion scan showed a matched deficitcorresponding to the cyst but no abnormality ofvascular supply.At operation at 1 year a tense intrapulmonary
cyst, 6 cm diameter, distended the right lowerlobe and spread onto both hilar and lateralsurfaces encircling the hilar structures. Thevascular connections of the lung were normal.The right lower lobe was resected but the cyston the left was not explored.
HISTOPATHOLOGYThe specimen received was a segment of theright lower lobe of the lung measuring 8 5x5x 2 5 cm with a previously incised cyst measuring3 cm in the collapsed state. The cyst wall wassmooth with some fibrous thickening in areasand was completely surrounded by lung paren-chyma. No vascular or bronchial connection tothe cyst could be seen. Microscopic analysisshowed that the cyst wall was composed largelyof multiple capillaries lined by plump endo-thelium (fig 2A), which stained positively forfactor VIII related antigen (fig 2B). Capillariesvaried in size, some were collapsed, others filledwith blood. The inner lining of the cystcontained fibrous tissue but no respiratory orgastrointestinal epithelium and no mitoticactivity was seen. Giant cell reaction, whichmight be expected in interstitial emphysema,was not seen. The capillaries infiltrated thesurrounding lung irregularly for a short distancebut the parenchyma appeared normal with nodiffuse involvement by the angioma. A diag-nosis of capillary haemangioma was made.
DiscussionPulmonary pseudocyst formation is a recog-nised complication of ventilation in neo-nates with respiratory distress syndrome. Suchcases are associated with the development ofinterstitial emphysema, pneumothoraces, andlater bronchopulmonary dysplasia.1 Thus ourinitial impression in this case was that the cystwas a ventilation induced pseudocyst that wouldbe expected to resolve spontaneously.The increasing size of the cyst and evidence
of compression of the surrounding lung led tothe decision to remove the affected lobe. Thefinding of a capillary haemangioma entirelysurrounding the cyst was unexpected and hasnot previously been reported.True congenital lung cysts are usually either
bronchogenic cysts, which are lined withrespiratory epithelium, enteric cysts lined withgastrointestinal epithelium, or cystic adeno-matoid malformations.2 These are characterisedby cysts and bronchioles lined by ciliatedcolumnar epithelium and goblet cells, and maybecome malignant.3 Even apparently simplecongenital lung cysts may be associated withabnormal vasculature, either systemic arterialsupply or anomalous venous return, and requirefull evaluation before surgery is planned.4
Vascular malformations in the lung aregenerally cavernous haemangiomata with largechannels of communication between pulmonaryarteries and veins, commonly associated withhereditary haemorrhagic telangectasia.5 Truecapillary haemangiomata occurring in thebronchial submucosa may give rise to severehaemoptysis.6 One comparable case of vascularchannels lying in the substance of the lung inassociation with an expanding cyst was reportedin a 25 year old man, but there the cyst waslined with respiratory epithelium.7Our finding of a capillary haemangioma
totally surrounding a lung cyst appears to be
1163
on 28 June 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.10.1162 on 1 October 1990. D
ownloaded from

1164 Bowyer, Sheppard
new. Aspiration of pseudocysts in ventilatedneonates has been advocated,8 but in thepresent case that might have been disastrous. Inview of the known association of congenitalparenchymal and vascular abnormalities,4 andin the light of this experience, we wouldrecommend full evaluation of all cysts beforeplanned surgery.We are grateful to Dr J Warner and Mr P Goldstraw forpermission to report the patient in their care.
1 Williams DW, Merten DF, Effman EL, Scatliff JH. Venti-lator induced pulmonary pseudocysts in preterm neonates.American Journal of Radiology 1988;150:885-7.
2 Spencer H. Congenital abnormalities of the lung, pulmonaryvessels and lymphatics. Pathology of the lung. 4th Ed.London: Pergamon Press, 1985:79-130.
3 Sheffield EA, Addis BJ, Corrin B, McCabe MM. Epithelialhyperplasia and malignant change in congenital lung cysts.J Clin Pathol 1987;40:612-4.
4 Clements BS, Warner JO. Congenital bronchopulmonaryvascular malformations: clinical application of a simpleanatomical approach in 25 cases. Thorax 1987;42:409-16.
5 Dunnill MS. Rare pulmonary tumours. Pulmonary pathology.London: Churchill Livingstone, 1987:353-6.
6 Masson RG, Altose MD, Maycock RL. Isolated bronchialtelangiectasia. Chest 1974;65:450-2.
7 Holden WE, Mulkey DD, Kessler S. Multiple peripherallung cysts and haemoptysis in an otherwise asymptomaticadult. Am Rev Resp Dis 1982;126:930-2.
8 Roberton NRC. Treatment of cystic ventilator lung disease.Proceedings of the Royal Society ofMedicine 1976;69:344-5.
Forty years ago
Infantile cortical hyperostosis(Caffey's syndrome)Caffey, an eminent American paediatric radio-logist, was the first to describe a syndromeoccurring mainly in the first six months of lifeand characterised by tender soft tissue swellingsand cortical thickening ofthe underlying bones.'The first case of Caffey's syndrome to be
reported in the United Kingdom was a 2 monthold baby boy who was admitted to hospital witha one week history of swelling of the face andfever.2 On examination there were moist soundsin the right lung and a tender swelling of the leftside of the face. He was given antibacterialtreatment without improvement; the fever per-sisted and after 10 days he was noticed to havegeneralised lymphadenopathy and a tenderswelling over the shaft of the left humerus. Overthe next few days similar swellings developedover the right ramus of the mandible, bothradii, and both tibiae. Radiographs of the longbones, ribs, pelvis, and mandible showedperiosteal elevation and irregular new boneformation. Blood examination showed ananaemia with polymorphonuclear leucocytosisand the blood chemistry was normal apart froma raised alkaline phosphatase. There was noevidence of syphilis, tuberculosis, or scurvy. Abiopsy specimen of the left tibia showed pro-liferation of osteoblasts but no evidence ofinfection or malignancy. The clinical signsgradually subsided over the next three months,and one year after the onset the child was welland the radiographs showed a return to normal.
Thrush in infancyIn a 12 month period in Liverpool necropsieswere carried out on 204 infants under the age of1 year, ofwhom 28 were aged less than 4 weeks.In seven (25%) of the neonates and 19 (11%) ofthe older infants pharyngeal or oesophageallesions ofthrush were found and were considered
directly or indirectly responsible for the deathof the child.3 Of the 26 infants with thrush onlythree had been breast fed and only two were oflow birth weight. The commonest clinicalfeatures on admission were oral lesions ofthrush, vomiting with or without diarrhoea, andsevere dehydration. Otitis media developedlater in 10 cases, in four of which Moniliaalbicans (now Candida albicans), was found onsmear or culture.At postmortem examination 21 of the 26
infants were found to have oesophageal lesionsof thrush, some with ulceration or sloughing.Eleven had histological evidence of inhalation ofvomit with aspiration pneumonia and six haddied suddenly due to obstruction of the airwaysby aspirated material. In two infants infectionhad spread from the oesophagus to the pleuralcavity causing an empyema. Pyaemic abscesses,which were presumed to have originated in theulcerated oesophagus, were found in variousorgans in five cases. In two there were metastaticthrush lesions in the kidneys. Ulcerated areas inthe intestine were present in four cases but onlyin one of these was this proved to be due tothrush.The authors warn that thrush may pass
unnoticed at necropsy unless histologicalexamination is undertaken, as the macroscopicalappearances may be non-specific. In their viewthe histology suggests that monilia is the primaryinfection and that the damaged epithelium isinvaded by bacteria, rather than the moniliabeing an opportunistic secondary invader of aprimary bacterial lesion.
1 Caffey J. Syphilis of the skeleton in early infancy. The non-specificity of many of the roentgenological changes. AJR1939;42:637-55.
2 O'Reilly JN. Infantile cortical hyperostosis. Arch Dis Child1949;24:67-70.
3 Lederer H, Todd R McL. Thrush in infancy. Arch Dis Child1949;24:200-7.
A D M JACKSON
on 28 June 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.10.1162 on 1 October 1990. D
ownloaded from





























