Embed Size (px)
Citation preview

ENVIRONMENTAL, SOCIAL AND DEVELOPMENT PERFORMANCE REPORT 2013


Table of contents
TABLE OF CONTENTS
Abbreviations 6
1. Introduction 8
2. Overview 10 2.1 Structure IFHA 10 2.2 Investment policy 11 2.3 Portfolio companies 12
3. IFHA’s Development Matrix 14 3.1 Development objectives 14 3.2 Objectives per sector 14 3.2.1 Healthcare provision 14 3.2.2 Health insurance 15 3.2.3 Wholesale and distribution 15 3.2.4 Production and Manufacturing 16 3.3 Indicators (SMART) 16 3.4 Practice 16
4. IFHA’s portfolio companies: ESD impact 19 4.1 Ensure equitable access to products and services 19 4.2 Increase availability of health products and services 20
5. Conclusion 22
6. Annexes 25 Annex 1: Environmental, Social and Development Management System IFHA 1.1 IFHA’s Dvelopment philosophy 25 1.2 Environmental Social and Development policy 26 1.2.1 IFHA’s exclusion list 26 1.2.2 National laws on environment, health, safety and social issues 26 1.2.3 IFHA’s development matrix (KPMG) 26 Reviewed on: 1.2.3.1 Millennium Development Goals (MDGs) 27 1.2.3.2. IFC Performance Standards and IFC guidelines for specific sectors 27 Annex 2: Examples of ESD Impact within IFHA’s portfolio companies 29 1- Increase availability of products and services 29 2- Ensure equitable access to products and services 29 3- Increase affordability of products and services 29 4- Ensure quality of products and services 29 5- Stimulate (local) economy and equitable access to employment 30 6- Stimulate decent work 30 7- Reduce negative enironmental impact 31 8-Apply good governance and transparency 32 Annex 3: Data ESD audits subsidiaries IFHA Portfolio Companies 33 Annex 4: Data ESD audits per sector 36 Annex 5: Snapshot Portfolio Companies 44 Hygeia 44 Pyramid Pharma 45 Strategis 46 Hello Doctor 47 AAR 48 Sourcelink 49 ER Corporate 50 Kampala Hospital Limited 51 Eco Health Limited 52
4 ESD Performance Report 2013

5

A
bbreviations
6 ESD Performance Report 2013
ABBREVIATIONS
AfDB African Development Bank
AHSM African Health Systems Management Company (Manager)
ESD Environmental Social Development
ESDPR Environmental Social Development Progress Report
FAPA Fund for African Private Sector Assistance
GIIRS Global Impact Investing Ratings System
HMO Health Maintenance Organization
IFC International Finance Cooperation
IFHA Investment Fund for Health in Africa
IRIS Impact Reporting and Investment Standards
MDGs Millennium Development Goals
NGO Non-Governmental Organization
SIFA Social Investor Foundation for Africa
WHL Worldwide Healthcare Limited
WHO World Health Organization
WWCVL World Wide Commercial Ventures Limited
ESD audit at WWCVL Nigeria (October 2013)

A
bbreviations
7

Overview
1. INTRODUCTION
We hereby present you the fourth edition of the annual Environmental, Social and Development Perfomance
Report (ESDPR) of the Investment Fund for Health in Africa (IFHA). In 2013, three new investments were
completed being World Wide Commercial Ventures Limited (WWCVL, Nigeria), Worldwid Healthcare
Limited (WHL, Ghana) and Kampala Hospital Limited (Uganda). Eco Health Limited was incorporated to
merge WHL Ghana and WWCVL Nigeria for the purpose of an exit. In this report the ESD results are pre-
sented separately for each company.
In 2013, entry measurements by KPMG were carried out at our portfolio companies in Ghana
(WHL), Nigeria (WWCVL) and South Africa (Sourcelink and ER Corporate). The entry measurement for
Kampala Hospital Limited is scheduled for July 2014.
The main goal of this report is to make the annual ESD performance of our portfolio companies
transparent to our investors. Furthermore, we aim to give insight in how we measure the ESD performance
and how we attach this to the popular terminology surrounding ESD impact.
Introduction
AAR’s Beckmann Trust de-worming program (2013)

Overview
9
Introduction

Overview
10 ESD Performance Report 2013
2. OVERVIEW
Investing in African health systems is an opportunity to accelerate economic development and
growth, contribute to saving millions of lives and preventing life-long disabilities, and move coun-
tries closer to achieving objectives of national poverty reduction strategies and the Millennium
Development Goals (MDGs)1.
It is with this thought in mind that IFHA was established in 2007; a private equity capital fund dedi-
cated to investments in private healthcare companies in Africa.
IFHA’s first closing was in May 2008 in which €14.7
million was committed from anchor investors FMO,
Goldman Sachs and the Social Investor Foundation
for Africa (SIFA). In August 2010, the second clo-
sing was completed in which an additional amount
of €35.4 million was committed by FMO, Pfizer,
APB pension fund, the African Development Bank
(AfDB) and the International Finance Corporation
(IFC).
2.1 Structure IFHA
IFHA is managed by African Health Systems
Management Company (AHSM), “the Mana-
ger” consisting of an experienced management
team with several years of experience in the
private healthcare industry in Africa.
Historically, strong ties exist between “the Ma-
nager” and PharmAccess Foundation; a Dutch
Non-Profit Organization (NGO) specialized
in capacity building in private healthcare in
Sub-Saharan Africa. The corporate governance
structure is a solid structure including an Ad-
visory Committee, Investment Committee and
Supervisory Board. The IFHA team constitutes
of six professionals with substantial private
equity and finance experience, including one
1- Harmonization for Health in Africa (HHA-2011), Investing in Health in Africa; the case for strengthening Systems for Better Health outcomes. Accesible at: http://www.who.int/pmnch/media/membernews/2011/investing_health_ africa_eng.pdf

Overview
11
team member in South Africa.
Figure 1 presents IFHA’s corporate governance structure.
2.2 Investment Policy
IFHA is set up as a fund that invests in fast-growing
markets which show unique advantages over the
competition and uses several sectoral focus points
when investing in private healthcare in Africa:
* Health insurance and Health
Maintenance Organizations (HMOs)
* Healthcare provision
* Pharmaceutical wholesale and
distribution
* Manufacturing of pharmaceuticals and
medical supplies
* Other health related investments
Furthermore, IFHA maintains a number of
investment criteria when considering an investment:
- The size of investee companies in terms of
annual turnover should lie between EUR
1 to EUR 20 million, although investments in
larger companies may also be considered
- The minimum investment size is not smaller
than EUR 500,000 in a single investment
- The normal investment size ranges from
EUR 0,5 to EUR 7,5 million
- IFHA will focus on equity participations
with protections through board seats and
provisions, although it has the ability to invest
in other instruments
- Favorable assessment of management
capacities
ESD Performance Report 2013

Overview
12 ESD Performance Report 2013
- High growth rates in the domestic markets
and sufficient current market size
Figure: Geographical scope investments IFHA
2.3 Portfolio companies
In 2011 IFHA performed six investments:
- Hygeia
Hygeia is the largest HMO in Nigeria and offers both
health insurance and delivery of healthcare in Nige-
ria.
- Pyramid Pharma
Pyramid Pharma is a pharmaceutical wholesale and
distribution company based in Tanzania.
- Strategis
Strategis is a company which offers health insurance
in Tanzania.
- AAR
AAR is the largest private healthcare company in the
East African region and offers both health insurance
and delivery of healthcare in Kenya, Uganda and
Tanzania, and in Zambia from 1 May 2014.
- Hello Doctor
Hello Doctor is an innovative company which uses
medicine services to improve the access to healthcare
services and is based in South Africa.
- Sourcelink
Sourcelink is a South African based manufacutring
company which produces medical supplies.
In 2012 IFHA performed the following investment:
- ER Corporate
ER Corporate is a specialized medical administration
and training company and is part of the ER Group.
ER Corporate manage 18 Emergency and other spe-
cialist practices across South Africa.
In 2013 IFHA performed the following investments:
- Kampala Hospital Limited
Kampala Hospital Limited (KHL) is an urban hospi-
tal in Uganda with significant growth potential.
- Eco Health Limited (WWCVL and WHL):
Eco Health Limited and its wholly-owned group
companies WWCVL Nigeria and WHL Ghana are
engaged in the wholesale and retail distribution of
healthcare related products.

Overview
13

IFHA’s D
evelopment M
atrix
14ESD Performance Report 2013
3. IFHA’s DEVELOPMENT MATRIX
3.1. Development objectives
In collaboration with KPMG, IFHA has redesigned
the initial development objectives to a comprehen-
sive list of eight objectives which directly relate to
the MDGs which can be found in the figure below.
The first two development objectives 1- Increase
availability of products and services; and 2- Ensure
equitable access to products and service, are IFHA’s
main strategic indicators.
3.2 Objectives per sector
Because of the fact that IFHA’s portfolio compa-
nies are active in several sectors, namely healthcare
provision, health insurance, production and manu-
facturing, and wholesale and distribution, specific
objectives are applicable per sector on which will be
elaborated in the next sections.
3.2.1 Healthcare provision
The healthcare sector includes investments in hospi-
tals and clinics. Currently three of IFHA’s portfolio
companies can be labled under the healthcare provi-
sion sector, namely AAR Healthcare in East Africa,
Lagoon Hospitals of Hygeia in Nigeria and Kampala
Hospital Limited in Uganda.
For IFHA, the main development objectives for the
healtcare provision sector are (see next page):
This chapter gives an overview of the development and validation of IFHA’s Development Matrix.
Furthermore, it gives an insight in how IFHA measures the Social and Environmental Impact of its
portfolio companies.
Development objective
1- Increase availability of products and services.
2- Ensure equitable access to products and services.
3- Increase affordability of products and services.
4- Ensure quality of products and services.
5- Stimulate (local) economy and equit able access to employment.
6- Stimulate decent work.
7- Reduce environment impact.
8- Apply good governance and transparency.

IFHA’s D
evelopment M
atrix
15
- To ensure the quality of products and services
Examples:
* Number of pharmaceuticals which have expired
* Total value of pharmaceuticals dispensed
* Has the company a quality system in place?
- To ensurance equitable access to products and
services
Examples:
* Total number of patients
* Total number of clinic visits a year
* Total number of healthcare workers
* The bed occupancy rate (BOR)
3.2.2 Health insurance/HMO
IFHA has invested in three companies which are
providing health insurance: AAR Insurance in East
Africa, Hygeia HMO part of Hygeia in Nigeria and
Strategis in Tanzania. One main development objec-
tive that IFHA maintains is:
- To increase the affordability of products and
services
Examples:
* Lowest cost insurance package provided
* Services covered in the lowest cost package
* Services covered in the lowest package provided
3.2.3 Wholesale and distribution
Pyramid Pharma in Tanzania, WWCVL in Nigeria
and WHL in Ghana are IFHA’s portfolio companies
which are active in the wholesale and distribution sec-
tor. For IFHA, the two main development objectives of
this sector are:
- To increase the availability of products and services
Examples:
* Total number of drugs delivered which are
related to specific conditions/diseases
* Total number of medical equitment delivered
* Total number of companies supplied through distribu-
tion channel
* Total number of distribution warehouses
- To ensure the quality of products and services
Examples:
* Number of times not being able to deliver an order
* Number of times of late delivery
* Inventory and stock control system in place
ESD Performance Report 2013

IFHA’s D
evelopment M
atrix
16ESD Performance Report 2013
3.2.4 Production and manufacturing
In 2011, IFHA’s investment in Sourcelink Healthcare
in South Africa was completed. Sourcelink is a com-
pany which manufactures disposable medical sup-
plies. The two main objectives that IFHA maintains
for this manufacturing company are:
- To reduce the environmental impact
Examples:
* Procedures for waste disposal in place
* Total amount of hazardous waste generated
* Total amount of non-hazardous waste generated
- To ensure the quality of products and services
Examples:
* The appropriate infrastructure in the company is in
place to ensure the proper maintanance of products
3.3 Indicators (SMART)
In collaboration with KPMG, IFHA has created
SMART indicators which measure the development
objectives. SMART means that the indicators have
to be Specific, Measurable, Attainable, Relevant and
Time-bound.
3.4 Practice
As mentioned before in chapter 3, IFHA’s develop-
ment matrix is reviewed based on the several tools
used to measure the Environmental and Social
impact, namely the MDGs and the IFC Performance
Standards and Guidelines. Based on the outcome of
this review, IFHA created eight development objec-
tives, described in this chapter, which can be linked
to specific indicators and the healthcare sectors
IFHA invests in.
In preparation for the actual ESD audit in which
the consultants will visit IFHA’s portfolio compa-
nies to measure the ESD performance, IFHA sends
out a development matrix questionnaire. This is an
Excell sheet in which categories are combined with
questions relating to one of the eight development
objectives which in turn are linked to indicators.
Page one of the development matrix questionnaire
is visible in the figure on the next page. The red part
on the left represents the ESD category in which the
questions fall.
Besides answering the general questions in the co-
ver sheet and general questions section, each port-
folio company is asked to fill in the sheet which is
applicable to their branch.

IFHA’s D
evelopment M
atrix
17
When the actual audit takes place, the questionnaire
serves as a guidance tool after which the questions in
the audit are streamlined. At the end of each audit the
consultants give a so-called “Close-out presentation”
in which they share their findings with the portfolio
company and where they share their suggestions for
improvement. Eventhough IFHA’s ESD audits are not
intended as an obligatory instrument to which the
portfolio company has to comply; the first (entry) sta-
ge of measurement creates a sense of ESD awareness
which will hopefully stimulate the portfolio company
to improve their ESD impact not only on a topdown,
but also at a grassroots level. Once the mid-term audit
results are in, IFHA will compare these with the entry
level outcomes in order to find out whether the port-
folio companies have taken the improvement suggesti-
ons for better use and if ESD improvement has set in.
Figure : First page of IFHA’s development matrix questionnaire
ESD Performance Report 2013
ESD audit at WWCVL Nigeria (October 2013)

IFHA’s D
evelopment M
atrix
18ESD Performance Report 2013

19
IFHA’s D
evelopment M
atrix
4. IFHA’s PORTFOLIO COMPANIES: ESD IMPACT
This chapter gives an overview of the ESD impact at IFHA’s portfolio companies and connects them to IFHA’s
two main strategic objectives; “To increase availability of products and services” and “To ensure equitable ac-
cess to products and services”. As IFHA’s development objectives are connected to each other, the data pre-
sented below can also be linked to IFHA’s other development objectives. The data is obtained via ESD impact
measurements at IFHA’s portfolio companies and its subsidiaries. In 2011 Pyramid Pharma and AAR Heal-
thcare Tanzania were audited, in 2012 the other AAR subsidiaries and Hygeia; and in 2013 Sourcelink, ER
Corporate, WWCVL Nigeria and WHL Ghana. For a more detailed overview of the outcomes see Annex 2.
4.1 Ensure equitable access to products and services
Introduction
IFHA’s investments in health insurance, telemedicine,
and pharmaceutical distribution result in more equit-
able access to health.
Increasing the total number of customers having a
health insurance, in addition to implementing low-
income schemes and offering products and services
both in urban and rurals areas improve access to
health. This has a direct impact on the reduction of
diseases (MDG 6), improved health (MDG 3, MDG
4, MDG 5), and hence a more and stable predicta-
ble income (MDG 1). Some examples of improved
access to health products and services are set out in
this chapter. For specific examples of the progress
of IFHA’s portfolio companies in 2013 in relation to
IFHA’s development objectives, see Annex 3.
Insured customers
The number of people with health insurance has in-
creased during the lifetime of IFHA’s investments.
Enrollment data in 2007 and 2008 include customers of Hygeia. 2009 include Hygeia and Strategis. 2010 , 2011 and 2012 and 2013 include customers of Hygeia, Strategis and AAR.
Note: the number of people with managed healthcare insurance in 2013 is less than in 2012 due to a reduction of 10,000 enrolles in a donor funded pogram of the Health Insurance Fund implemented by the Hygeia Community Health Care (HCHC) programme.
ESD Performance Report 2013
Number of people insured2006 2007 2008 2009 2010 2011 2012 2013
High income 105,646 149,322 175,547 222,247 305,901 301,600 319,318 340,183 Middle income 43,250 63,149 65,849 66,324 135,734 161,485 173,393 141,193 Low income 6,483 29,529 52,225 63,388 96,843 137,338 139,961 144,800
Total 155,379 242,000 293,621 351,958 538,478 600,423 632,671 626,175

IFHA’s Portfolio C
ompanies: ESD
Impact
20 ESD Performance Report 2013
General trend: Rural and urban insured.Enrollment data in 2007 and 2008 include customers of Hygeia. 2009 include Hygeia and Strategis. 2010, 2011, 2012 and 2013 include Hy-geia, Strategis and AAR.
Out-patient visits
In 2013, a total number of approximately 800,000
out-patient visits took place at clinics of Hygeia and
AAR. This is a growth of about 125,000 compared
to 2012 without the addition of an extra portfolio
company (which contributed to the strong growth
between 2009-2010).
Increased focus on solvency and capital requirements
have led to higher pricing and less growth in insured.
In 2013, IFHA’s portfolio companies Hygeia, Strategis
and AAR insured approximately 626.000 customers.
When more people are insured, their health will im-
prove which will give them the opportunity to work
and to provide for a more stable and predictable
income. The table below shows a substantial increase
in the number of people insured in IFHA’s lifetime.
Insured high/middle/low income levelEnrollment data in 2007 and 2008 include customers of Hygeia. 2009 include Hygeia and Strategis. 2010 , 2011, 2012 and 2013 include Hygeia, Strategis and AAR.
-
100,000
200,000
300,000
400,000
500,000
600,000
700,000
2007 2008 2009 2010 2011 2012 2013
Insured: high, middle, low income level
High income Middle income Low income
IFHA’s insurance companies follow the natural evo-
lution from high income to middle and low-income
customer, as illustrated in the graph.
Closely related to the natural evolution of the in-
surance customer base from high to middle and
low-income customers (see graph), is the evolution
of urban to rural based customers.The number of
customers based in urban areas increased from over
106,000 customers by the end of 2006 to roughly
500,000 customers by the end of 2013. The number
of customers based in rural areas increased from
roughly 49,000 to 120,000 in the same period.
-
100,000
200,000
300,000
400,000
500,000
600,000
700,000
2007 2008 2009 2010 2011 2012 2013
Rural and urban insured
Urban Rural
-
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
900,000
2007 2008 2009 2010 2011 2012 2013
Out-patient visits
Outpatient visits
Number of out-patient visitsNumber of visits in 2007, 2008 and 2009 include Hygeia. 2010, 2011, 2012 and 2013 include Hygeia and AAR.

21
4.2 Increase availabilty of health products and
services
Introduction
With IFHA’s investment in health insurance and
wholesale and distribution, the availability of pro-
ducts and services increases. Adding services to exis-
ting insurance packages, and extending the product
portfolio as well as sustaining the delivery of phar-
maceuticals (MDG 8), are examples of increasing the
availability of healthcare. This has a direct impact on
the reduction of diseases (MDG 6), improved health
(MDG 3, MDG 4, MDG 5), and hence a more and
stable predictable income (MDG 1).
In the table above is visible how the number of
people insured are divided amongst several sectoral
groups (Corporate and Governmental Organisations,
Civil servants and Community program).
The group which falls under the Community pro-
gram- sector has dencreased the past year due to
a reduction of enrollees in a pogram of the Health
Insurance Fund implemented by the Hygeia Com-
munity Health Care (HCHC) programme.
Number of people insured.Enrollment data in 2007 and 2008 include customers of Hygeia. 2009 include Hygeia and Strategis. 2010, 2011, 2012 and 2013 include Hy-geia, Strategis and AAR.
-
500
1,000
1,500
2,000
2,500
3,000
2007 2008 2009 2010 2011 2012 2013
Division male/female
Female Male
Employee division male/female. Data in 2007 include employees of Hygeia. 2008 include Hygeia and Pyramid Pharma. 2009 include Hygeia, Pyramid Pharma and Strateg-is. 2010 include Hygeia, Strategis, Pyramid Pharma, Hello Doctor and AAR. 2011 include employees of Hygeia, Strategis, Pyramid Pharma, Hello Doctor, AAR and Sourcelink. 2012 include Hygeia, Pyramid Pharma, Strategis, Hello Doctor, AAR, Sourcelink and ER Corporate. In 2013, data of Kampala Hospital and Eco Health Limited is added.
Employees
Another indicator which shows that IFHA’s invest-
ments are having an impact on the availability of
health products and services is the number of people
that are employed. After all, a company that is in-
creasing its operations needs to expand its capacity
in order to meet the growing need for products and
services. The graph on this page shows the employ-
ee-trend over the last years. It is important to note
that women represent more than half of all employ-
ees within the companies in IFHA’s portfolio. Provi-
ding equal opportunities for men and women is well
presented here (see graph below). The total work-
force in 2013 increased with 900, primarily because
of IFHA’s three new portfolio companies in 2013.
-
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
450,000
2006 2007 2008 2009 2010 2011 2012 2013
Number of people insured
Corporate and governmental organizations Civil servants Community program
ESD Performance Report 2013

C
onclusion
22ESD Performance Report 2013
5. CONCLUSION
This fourth edition of the ESD performance re-
port described the performance of IFHA’s portfolio
companies in 2013. The development and validation
of IFHA’s development matrix was outlined and an
explanation has been given on how IFHA uses the
matrix in order to measure the ESD impact of its
portfolio companies.
Entry level ESD measurements have taken place in
2013 at all of IFHA’s portfolio companies, except for
Kampala Hospital Limited which is scheduled for
July 2014. All these measurements have created ESD
awareness and monitoring of the ESD results is pre-
cisely monitored by IFHA’s Environmental & Social
Manager.
Moreover, an important achievement during 2013 is
that Pyramid Pharma Tanzania has received an ISO
9001:2008 Quality Standard Certification, which is
an international quality accreditiation.
Furthermore, AAR’s membership of the UN Global
Compact allowed it to take part in the putting toge-
ther of the Code of Ethics for Business in Kenya. In
March 2012, AAR became the signatory of this Code
as well as supporter for the ‘Rights of the Child in
Business’ which was launched in Nairobi in October
2012. Besides this, in 2013 AAR’s CEO has signed the
United Nations Global Compact Water Mandate.
Achievements of AAR’s Beckmann Trust in 2013 are
as followed:
- 35,000 children have been de-wormed
- 170 schools are on board for the “Trees for Health”
project and 4,468 trees were planted
AAR’s Beckmann Trust Trees for Health project (2013)

23
C
onclusion

A
nnexes
24 ESD Performance Report 2013
6. ANNEXES: TABLE OF CONTENTS
Annex 1: Environmental, Social and Development Management System IFHA 25 1.1 IFHA’s Dvelopment philosophy 25 1.2 Environmental Social and Development framework 26 1.2.1 IFHA’s exclusion list 26 1.2.2 National laws on environment, health, safety and social issues 26 1.2.3 IFHA’s development matrix (KPMG) 26 Reviewed on: 1.2.3.1 Millennium Development Goals (MDGs) 27 1.2.3.2. IFC Performance Standards and IFC guidelines for specific sectors 27 Annex 2: Examples of ESD Impact within IFHA’s portfolio companies 29 1- Increase availability of products and services 29 2- Ensure equitable access to products and services 29 3- Increase affordability of products and services 29 4- Ensure quality of products and services 29 5- Stimulate (local) economy and equitable access to employment 30 6- Stimulate decent work 30 7- Reduce negative enironmental impact 31 8-Apply good governance and transparency 32
Annex 3: Data ESD audits subsidiaries IFHA Portfolio Companies 33
Annex 4: Data ESD audits per sector 36
Annex 5: Snapshot Portfolio Companies 44
Hygeia 44 Pyramid Pharma 45 Strategis 46 Hello Doctor 47 AAR 48 Sourcelink 49 ER Corporate 50 Kampala Hospital Limited 51 Eco Health Limited 52
AAR’s Beckmann Trust Trees for Health project (2013)
A
nnexes
25 ESD Performance Report 2013
The African healthcare market offers attractive investment opportunities, not only in terms of finan-
cial returns, but also in terms of social returns. Private sector development is essential in order to
achieve a better healthcare system in Africa and hence a better quality of life. In recent years, leading
international institutions such as the World Bank and IFC have stressed this fact and have put incre-
ased focus on stimulating private sector initiatives.
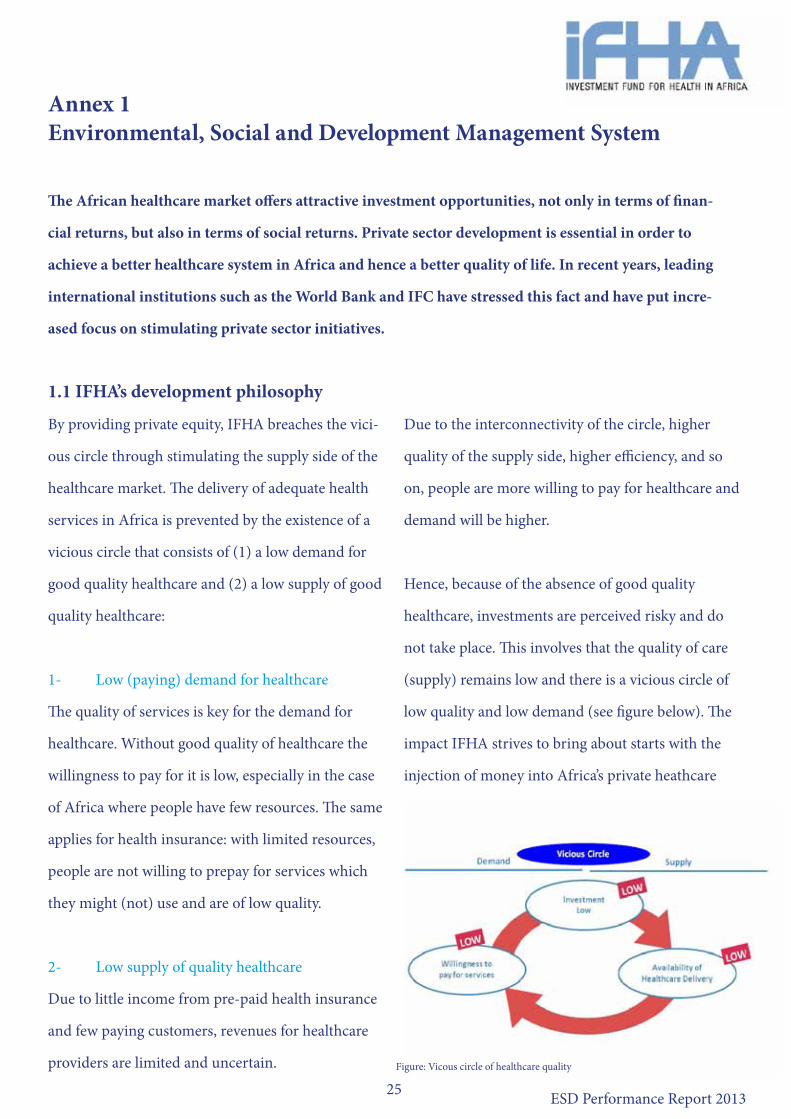
1.1 IFHA’s development philosophy
By providing private equity, IFHA breaches the vici-
ous circle through stimulating the supply side of the
healthcare market. The delivery of adequate health
services in Africa is prevented by the existence of a
vicious circle that consists of (1) a low demand for
good quality healthcare and (2) a low supply of good
quality healthcare:
1- Low (paying) demand for healthcare
The quality of services is key for the demand for
healthcare. Without good quality of healthcare the
willingness to pay for it is low, especially in the case
of Africa where people have few resources. The same
applies for health insurance: with limited resources,
people are not willing to prepay for services which
they might (not) use and are of low quality.
2- Low supply of quality healthcare
Due to little income from pre-paid health insurance
and few paying customers, revenues for healthcare
providers are limited and uncertain.
Due to the interconnectivity of the circle, higher
quality of the supply side, higher efficiency, and so
on, people are more willing to pay for healthcare and
demand will be higher.
Hence, because of the absence of good quality
healthcare, investments are perceived risky and do
not take place. This involves that the quality of care
(supply) remains low and there is a vicious circle of
low quality and low demand (see figure below). The
impact IFHA strives to bring about starts with the
injection of money into Africa’s private heathcare
Annex 1Environmental, Social and Development Management System
Figure: Vicous circle of healthcare quality

A
nnexes
26 ESD Performance Report 2013
sector. This induces market movements enlarging the
development impact. For example, before the year of
inception of IFHA (2007), health insurance for low-
income groups within Africa was mainly provided
by public funds of governments and NGOs. Capital
investment in private insurance companies, such as
a Health Maintenance Organization (HMO) leads to
increased risk pooling and subsequent lower reli-
ance on out-of-pocket payments by individuals. This
results in more stable cash flows for health providers
and a risk reduction for private investors implicating
a lower cost of capital. Through lower perceived risk
more private investments can be attracted. Hence,
IFHA’s capital injection creates additional funds in
the system that have a social impact.
1.2 Environmental, Social and
Development (ESD) Framework
IFHA’s ESD Framework is embedded in its invest-
ment policy, in which reference is made to specific
guidelines with respect to environmental, social and
development impact of investee companies.
The ESD policy includes (1) IFHA’s exclusion list, (2)
Standards as set down in applicable national laws on
environment, health, safety and social issues and (3)
IFHA’s development matrix.
1.2.1 IFHA’s exclusion list
IFHA developed a list which defines the types of
activities of investee companies that IFHA does not
invest in or finance, e.g. production and trade in
wapons, the tobacco industry, or radiactive materials.
1.2.2 National laws on environment, health,
and safety
IFHA makes sure that the activities of IFHA’s
investee companies align with the national laws on
environment, health and safety.
1.2.3 IFHA’s development matrix
IFHA ensures that all activities undertaken by the
portfolio companies are consistent with IFHA’s ESD
policy, through periodic review and analysis of the
portfolio companies. This is done via IFHA’s deve-
lopment matrix which is an important component of
the ESD Framework. With the development matrix,
besides the social impact brought about by capital
investment in private companies, other impact areas
can be identified. These areas are captured and mea-
sured along predefined indicators in IFHA’s develop-
ment matrix in order to make the contribution to the
MDGs measurable.
IFHA has collaborated with KPMG in order to deve-
lop and review the development matrix which is in
the first place based on the (1) MDGs and is designed
to make IFHA’s contribution to the MDGs measura-
ble. Besides the fact that IFHA’s development matrix

A
nnexes
27 ESD Performance Report 2013
is based on the MDGs, IFHA’s E&S Manager (in
collaboration with KPMG) has reviewed the com-
pleteness of the development matrix against specific
globally recognized standards which are the IFC
Performance Standards and Guidelines for specific
sectors.
1.2.3.1 Millennium Development Goals
The MDGs were established in September 2000 when
world leaders came together at the United Nations
Headquarters in New York to adopt the United Nati-
ons Millennium Declaration. In this Declaration they
committed their nations at a new global partnership
to reduce extreme poverty and setting out a series
of time-bound targets (with a deadline of 2015).
The eight goals in the Declaration are known as the
MDGs.1 Because of the fact that IFHA aims to con-
tribute to the global partnership to reduce extreme
poverty and make it visible; IFHA monitors indica-
tors that are based on the MDGs. These indicators
include the increase in labor productivity, increase in
local knowhow, and the increase in access to health-
care (i.e. increase in number of hospitals / clinics; or
increased affordability of services) since better health
will allow people to work. Three of the eight MDGs
relate directly to the sectors in which IFHA invests.
These are the following: MDG 4 ‘Reduce child mor-
tality’, MDG 5 ‘Improve maternal health’ and MDG
6 ‘Combat HIV/Aids, malaria and other diseases’. By 1 Source: http://www.un.org/millenniumgoals/bkgd.shtml, April 2012
investing in health, IFHA has a direct impact on these
MDGs. In addition, IFHA’s investments, targeting the
African population, affect MDG 1 ‘Eradicate extreme
poverty and hunger’ as well as MDG 3 ‘Promote gen-
der equality and empower women’. Measuring along-
side the MDGs will enable IFHA to show development
impact such as increased access to quality healthcare
in Sub-Saharan Africa. IFHA’s indicators measure
development impact within the areas: affordability,
accessibility, availability and quality of healthcare, as
well as improvement of the working conditions of the
companies’ employees. Below is set down how deve-
lopment impact for each MGD is realized.
1.2.3.2 IFC Performance Standards and
Guidelines for specific sectors
The International Finance Corporation (IFC) applies
its Performance Standards to manage social
and environmental risks and impacts and to enhance
development opportunities in its private sector
financing in its member countries eligible for finan-
cing. 2 These Performance Standards define the roles
and responsibilities for managing projects and requi-
rements for IFC support. They also include require-
ments to disclose information.
In addition to these Performance Standards, IFC
developed guidance notes which provide guidance
2 Source: International Finance Corporation’s Performance Standards on Social & Environmental Sustainability, 30 April 2006.

A
nnexes
28 ESD Performance Report 2013
for meeting the Performance Standards in specific
sectors. IFHA linked IFC’s Performance Standards
to the indicators of the development matrix in order
to get a better overview and understanding of the
environmental and social status (and improvement)
of the investee companies.
MDG 4: Reduce child mortality.Reached by increasing the number of children with insurance, inclusion of treatments in insurance packages and improved accessebility, availability and affordabilty of services.
MDG 5: Improve maternal health.Reached by increasing the number of mothers/women with insurance, inclusion of treatments in insurance packages and improved accessibility, availability and affordability of services.
MDG 6: Combat HIV/AIDS, malaria and other diseases.Reached by the inclusion of these treatments in insurance packages, proved healthcare and better available and af-fordable services.
MDG 7: Ensure environmental sustainability.An environmental and sustainable (work) environment is created by increased and professional attention to workking conditions and compliance with international standards on environmental and social issues, sucha s the IFC Perfor-mance Standards.
MDG 8: Develop a global partnership for development.Providing access to affordable and qualified drugs and creating a reliable healthcare network contributes to the development of a global partnership for development.
MDG 1: Eradicate extreme hunger and poverty. This is realized by reducing the out of pocket expenses paid by people when healthcare is needed, and hence providing them with a more stable income and better health. As well, by increased job opportunities and training, local knowhow will increase.
MDG 3: Promote gender equality and empower women.Reached by a better health for women (including maternal health insurance packages), training on the job and incre-ased job opportunities.
Overview Millenium Development Goals:

A
nnexes
29 ESD Performance Report 2013
Annex 2: Examples of the ESD impact within IFHA’s portfolio companiesIn this Annex examples are given of the ESD im-
pact within IFHA’s portfolio companies and the ac-
complishments of IFHA’s portfolio companies with
regard to (inter)national awards, certificates and
accreditations that were obtained in 2013. These
examples are linked to the development objectives.
1- Increase availability of health products and
services
In April 2013, Pyramid Pharma Tanzania has re-
ceived an ISO:2008 Quality Standard Certification,
which is an international quality accreditiation. This,
among other things, resulted in a turnover growth
and entails an expansion of Pyramid Pharma’s distri-
bution activities and thereby increasing the availabi-
lity of health products in the region.
2- Ensure equitable access to products and services
The main goal of Hello Doctor is to connect doctors
to patients via telemedicine services and hereby to
ensure equitable acces to healthcare products and
services. The services that Hello Doctor provides are
especially interesting for people with a lower income
as contact with the doctor
will occur via telephone or
email and thereby re-
ducing the doctor’s fee.
Patients living in remote areas can have easy access
to the service as they do not have to travel to see a
doctor, but can contact the doctor from their home.
IFHA has exitted in Hello Doctor in 2013.
3- Increase affordability of products and services
IFHA’s portfolio company in Nigeria ‘Hygeia’ in colla-
boration with PharmAccess and the Health Insurance
Fund, provides equitable access to affordable and
qualtiy healthcare services to selected low-income
communities in the region via the Hygeia Commu-
nity Health Care (HCHC) programme.
4- Ensure quality of products and services
Besides ensuring quality of products and services on
a business profit-making level, IFHA’s portfolio com-
panies are also contributing to the quality of health-
care not directly aimed at direct financial returns. An
example is the Hygeia Foundation which depends on
external funding and which main aim is to improve
skills and abilities in the Nigerian healthcare sector.1
Moreover, in 2012 Sourcelink received an ISO 13485
Quality Standard Certification and in 2013, Pyramid
Pharma Tanzania received an ISO 9001:2008 certifi-
cation which shows a high-standard of their products
which is internatiolly recognised.

A
nnexes
30 ESD Performance Report 2013
In April 2011 Hygeia’s Lagoon hospitals became the
first hospitals in Sub-Saharan Africa to earn accre-
ditation from the Joint Commission International
(JCI). JCI is the worldwide leader in improving the
quality of healthcare.
5- Stimulate (local) economy and equitable access
to employment
As at 31 December 2013, the direct total employ-
ment of our portfolio companies is 2,384 employees
of which 1,249 female employees. This shows that
women have equitable access to employment and the
new jobs are stimulating the local economy.
6 Stimulate decent work
In 2012 Pyramid Pharma has improved in several
ways regarding the stimulation of decent work.
First of all the company hired a HR manager which
resulted in the fact that all employees received an
official employment contract. A system has been set
up in which all employees who did not have a bank-
account were offered one. Pyramid Pharma now pays
out salaries via banktransfers, a much safer payment
way and a clear indicator in the stimulation to decent
work. All Pyramid Pharma warehouse-workers
received a formal tenue with strong closed shoes.
The new clothes and shoes are a contribution to their
safety on the workfloor.
Hygeia Foundation - Statistics
- Active in 24 States in Nigeria
- Almost 12,000 people placed on HIV/Aids
treatment
- The only indigenous NGO implementing a free
comprehensive Anti-Retroviral Treatment
programme across all the States of Nigeria
- Integrating HIV/AIDS medical intervention with a
peer support system

A
nnexes
31 ESD Performance Report 2013
7 Reduce environmental impact
The most obvious example in which one of IFHA’s
portfolio companies creates environmental aware-
ness and reducess negative environmental impact is
the AAR Beckmann Trust (named after the founder
of the company). The Trust is leveraging on AAR’s
expertise in health delivery, and combining it with
the Beckmann family’s commitment towards health
around the world. The Trust creates programmes
that provide hands-on opportunities for East African
communities to improve their environment, and en-
gage in income-generating and sustainable activities
to obtain access to health.
AAR - Trees for Health
One programme in the AAR Beckmann Trust is
called “Trees for Health” . The programme enables
schools to grow trees and provide a self-sustaining
source of firewood.
The programme aims at:
- Re-forestation
- Encouraging schools to grow their own firewood
- Generated/ saved funds used for basic preventive
health needs of the school children
- Directly involving children in the tree planting
process and hence creating environmental
awareness.
By the end of 2013, AAR has 170 schools on board of
the program and 4,468 trees were planted.

A
nnexes
32 ESD Performance Report 2013
8 Apply good governance and transparancy
All of IFHA’s portfolio companies have a supervi-
sory board which monitors the operations. IFHA
has a minimum of one boardseat in each portfolio
company and can therefore have an influence on the
operational process and make sure good governance
and transparancy are well executed.
AAR’s Beckmann Trust Trees for Health project (2013)

A
nnexes
33 ESD Performance Report 2013
Annex 3: Data ESD audits subsidiaries IFHA Portfolio Companies
Subs
idar
ies I
FHA
Port
folio
co
mpa
nies
whi
ch h
ave
been
m
easu
red
sepe
rate
ly >
>>
AAR
HC
Tanz
ania
(2
013)
Pyra
mid
Ph
arm
a (2
013)
Hyge
ia H
MO
(2
013)
Hyge
ia
Hosp
itals
(201
3)
AAR
HC
Keny
a (2
013)
AAR
HC
Ugan
da
(201
3)
AAR
Insu
ranc
e Ta
nzan
ia
(201
3)
AAR
Insu
ranc
e Ug
anda
(201
3)
AAR
Insu
ranc
e Ke
nya
(201
3)
Sour
celin
k He
alth
care
(2
013)
ER C
orpo
rate
Ad
min
istra
tion
(201
3)
Kam
pala
Ho
spita
l (20
13)
WW
CVL
Nig
eria
(201
3)W
HL G
hana
(2
013)
Obj
ectiv
e: S
timul
ate
(loca
l) ec
onom
y an
d eq
uita
ble
acce
ss to
em
ploy
men
t
Fina
ncia
l yea
r is
from
1 A
pril
- 31
Mar
ch
Fina
ncia
l yea
r is
from
1 A
pril
- 31
Mar
ch
Tota
l rev
enue
TZS
6,35
7,92
4,04
6TZ
S 22
,706
,048
,672
NGN
8,
350,
360,
188
NGN
3,
217,
770,
975
KES
884,
569,
072
UGX
12,4
76,4
89,8
11TZ
S 36
,248
,218
,000
UGX
22,5
74,3
09,2
21KE
S 2,
619,
874,
265
ZAR
839,
030
ZAR
18,5
23,7
71UG
X 3,
668,
555,
000
NGN
20
,682
,080
,356
CEDI
8,5
00,0
00
Subs
idie
s and
free
goo
ds re
ceiv
ed0
N/A
00
00
00
00
00
00
New
inve
stm
ents
(inc
ludi
ng p
rivat
e in
vest
men
ts a
nd d
onor
/ pub
lic
fund
ing)
.0
00
0AA
R HC
Ho
ldin
gs:
USD
353,
000
IFHA
&
Swed
fund
: US
D 35
3,00
00
0IF
HA: Z
AR
3,10
4,31
2IF
HA: Z
AR
5,00
5,00
0
IFHA
: USD
3.8
m
(not
all
avai
labl
e ye
t)
Chai
nrai
Fam
ily:
NGN
3,5
00,0
00
(wor
king
capi
tal
loan
)
0
Inve
stm
ents
rece
ived
in p
revi
ous
year
s tha
t con
tinue
d to
be
rece
ived
in
the
repo
rtin
g ye
ar (i
nclu
ding
pr
ivat
e in
vest
men
ts a
nd d
onor
/ pu
blic
fund
ing)
.
00
00
00
00
IFHA
: EUR
8,
434,
853
00
00
0
Tota
l cos
t of p
urch
ases
from
su
pplie
rs th
at p
rodu
ce th
eir g
oods
/ se
rvic
es in
you
r cou
ntry
:N
/ATZ
S 2,
080,
665,
557
NGN
6,
903,
196,
826
0N
ot a
vaila
ble
UGX
16,3
55,7
00TZ
S 31
,911
,595
,609
UGX
16,9
01,6
83,6
29KE
S 2,
153,
884,
419
ZAR
2,87
7,00
6ZA
R 6,
592,
686
UGX
2,00
0,00
0 pe
r mon
thN
GN 1
44,9
37,5
05CE
DI 1
00,0
00
Tota
l cos
t of p
urch
ases
from
su
pplie
rs w
hich
pro
duce
thei
r go
ods o
r ser
vice
s in
othe
r Afr
ican
co
untr
ies:
N/A
00
Not
ava
ilabl
eUG
X 10
4,38
5,70
0TZ
S 1,
026,
029,
329
UGX
272,
589,
838
KES
5,21
6,78
9N
/A0
UGX
6,00
0,00
0 pe
r mon
thN
GN 8
60,3
55,3
280
Tota
l cos
t of p
urch
ases
from
su
pplie
rs w
hich
pro
duce
thei
r go
ods o
r ser
vice
s in
coun
trie
s tha
t ar
e no
t in
Afric
a:
N/A
TZS
12,6
26,0
31,2
650
Unkn
own
KES
262,
692,
879
UGX
2,53
8,36
7,80
6TZ
S 78
0,13
1,06
10
KES
11,3
94,8
16ZA
R 46
,234
0UG
X 12
3,80
0,00
0N
GN
17,4
76,2
15,6
42CE
DI 6
,000
,000
Com
pany
's fa
cilit
ies t
hat w
ere
built
/exp
ande
d/im
prov
ed w
hich
al
so h
ave
a pu
blic
ben
efit.
If ye
s, p
leas
e ex
plai
n.
Sinz
a Cl
inic
st
arte
d it'
s op
erat
ion
May
20
13. L
ocat
ed
at S
inza
M
aduk
ani
whe
re it
's ac
cess
ible
to
both
priv
ate
and
heal
th
insu
red
mem
bers
from
di
ffer
ent
insu
ranc
e co
mpa
nies
NO
NO
Yes,
new
ge
nera
l ou
tpat
ient
pr
efab
ricat
ed
build
ing
in
Apap
a
YES,
1.
Emba
kasi
and
M
ount
ain
Mal
l Clin
ics
open
ed in
N
ov
2013
&De
c 20
13 2
. Ki
sum
u Cl
inic
ex
pand
ed (3
co
nsul
tatio
n ro
oms)
3.
Eldo
ret C
linic
ex
pand
ed to
(2
co
nsul
tatio
n ro
oms)
NO
NO
NO
Yes,
AAR
In
sura
nce
Nye
ri &
N
aiva
sha
bran
ches
w
ere
reno
vate
d
NO
NO
YES:
im
prov
emen
t of
the
road
lead
ing
to th
e Ho
spita
l fr
om K
aboj
ja
Juni
or S
choo
l
YES:
new
Enu
gu
depo
t - S
ep
2012
. WH
expa
nsio
ns in
Ab
a &
Oni
tsha
Non
e, e
xcep
t for
a
cold
room
All t
axes
(inc
ome,
corp
orat
e, V
AT,
etc)
and
levi
es m
ade
to th
e go
vern
men
t:Un
know
nTZ
S 75
0,00
0,00
0N
GN 2
6,59
4,91
5Un
know
nKE
S 44
,396
,103
UGX
350,
920,
568
TZS
733,
309,
000
UGX
19,6
47,2
02KE
S 11
9,77
8,46
8ZA
R 35
7,17
7ZA
R 1,
769,
276
UGX
48,7
11,0
00N
GN 1
10,0
00,0
00CE
DI 1
,200
,000
Num
ber o
f em
ploy
ees o
n pa
yrol
l:Pe
rman
ent s
taff
149
5817
859
321
915
072
5012
41
6615
434
337
Tem
pora
rily
staf
f43
422
011
785
143
823
2N
A77
7N
umbe
r of n
atio
nal e
mpl
oyee
s on
payr
oll:
149
5519
059
333
614
671
4820
64
6615
431
840
Num
ber o
f nat
iona
l hig
hly
skill
ed
empl
oyee
s on
payr
oll
122
4113
844
829
414
966
4812
44
313
211
635
Tota
l hou
rs o
f tra
inin
g:N
ot re
cord
ed39
0896
Not
reco
rded
3071
160
618
Not
reco
rded
Not
reco
rded
120
994
Not
reco
rded
560
584

A
nnexes
34 ESD Performance Report 2013
Subs
idar
ies I
FHA
Port
folio
co
mpa
nies
whi
ch h
ave
been
m
easu
red
sepe
rate
ly >
>>
AAR
HC
Tanz
ania
(2
013)
Pyra
mid
Ph
arm
a (2
013)
Hyge
ia H
MO
(2
013)
Hyge
ia
Hosp
itals
(201
3)
AAR
HC
Keny
a (2
013)
AAR
HC
Ugan
da
(201
3)
AAR
Insu
ranc
e Ta
nzan
ia
(201
3)
AAR
Insu
ranc
e Ug
anda
(201
3)
AAR
Insu
ranc
e Ke
nya
(201
3)
Sour
celin
k He
alth
care
(2
013)
ER C
orpo
rate
Ad
min
istra
tion
(201
3)
Kam
pala
Ho
spita
l (20
13)
WW
CVL
Nig
eria
(201
3)W
HL G
hana
(2
013)
Obj
ectiv
e: A
pply
goo
d go
vern
ance
and
tr
ansp
aren
cyAn
ti-co
rrupt
ion
proc
edur
es in
pl
ace:
YES
YES
NONO
YES
YES
YES
NOYE
SYE
SNO
NOYE
SYE
S
Tota
l num
ber o
f em
ploy
ees
that
ha
ve b
een
train
ed in
com
pany
's
anti-
corru
ptio
n pr
oced
ures
:0
50
00
035
40
00
011
35
Tota
l num
ber o
f new
cas
es o
f co
rrupt
ion:
00
Not r
ecor
ded
Not r
ecor
ded
Not r
ecor
ded
00
0No
t rep
orte
d0
00
00
Proc
edur
es in
pla
ce fo
r co
mpl
aint
s of
(grie
vanc
e pr
oced
ure)
:YE
SYE
SYE
SYE
SYE
SYE
SYE
S YE
SYE
SYE
SYE
SNO
, but
fe
edba
ck fo
rms
for c
lient
sYE
SIn
form
al
proc
edur
e
Num
ber o
f com
plai
nts:
Clie
nts
0;
Empl
oyee
s 3
Clie
nts
12;
Empl
oyee
s 0
Clie
nts
42;
Empl
oyee
s no
t re
cord
ed
Clie
nts
35;
Empl
oyee
s:
not r
ecor
ded
Clie
nts
330;
Em
ploy
ees
not r
ecor
ded
0Ci
ents
41;
Em
ploy
ees
4Cl
ient
s 7;
Empl
oyee
s 0
Not
regi
ster
ed0
Clie
nts:
0,
Empl
oyee
s: 0
Not r
egis
tere
dCl
ient
s: 3
0,
Empl
oyee
s: 0
Clie
nts:
6,
Empl
oyee
s: n
ot
reco
rded
Does
the
com
pany
repo
rt in
form
atio
n pu
blic
ly:
YES
NONO
NO
NO
Fi
nanc
ial n
o,
non-
finan
cial
ye
sFi
nanc
ial y
esNO
Fi
nanc
ial y
esNO
NONO
NONO
Num
ber o
f loc
al m
embe
rs (f
rom
th
e sa
me
coun
try) r
epre
sent
ed o
n th
e Bo
ard
at th
e en
d of
the
prev
ious
yea
r:
22
44
21
31
42
311
10
Writ
ten
Hum
an R
esou
rce
polic
y in
clud
ing
the
follo
win
g is
sues
:If
not,
plea
se s
peci
fy w
hy.
Abol
ition
of c
hild
and
forc
ed la
bor
YES
YES
NONO
NO*
NO*
YES
NO*
NO*
YES
NONO
NO**
YES
Free
dom
of A
ssoc
iatio
nYE
SYE
SNO
NONO
*NO
*YE
SNO
*NO
*YE
SNO
NONO
**YE
SEl
imin
atio
n of
disc
rimin
atio
nYE
SYE
SYE
SYE
SYE
SYE
SYE
SYE
SYE
SYE
SYE
SNO
NO**
YES
Gend
er e
quity
YES
YES
YES
YES
YES
NOYE
SYE
SYE
SYE
SYE
SNO
NO**
YES
Qua
lity
syst
em in
pla
ce:
YES
YES
YES
YES
YES
YES
NONO
NOYE
SYE
SNO
YES
SOP
in p
lace
If ye
s, p
leas
e sp
ecify
whi
ch
syst
em a
nd w
heth
er it
is
certi
fied/
accr
edite
d or
not
and
st
ate
how
ofte
n pe
rform
ance
is
mon
itore
d.
Bi-a
nnua
l Re
gion
al
Inte
rnal
Aud
it,
bi-a
nnua
l Ex
tern
al
Labo
rato
ry
Qua
lity
Asse
ssm
ent
Sche
me,
qu
arte
rly D
rug
Form
ular
y Re
view
ISO
: ann
ual
mon
itorin
g by
ext
erna
l pa
rty
In-h
ouse
qua
lity
mon
ityor
ing
syst
em: y
early
re
view
Join
t Co
mm
issi
on
Inte
rnat
iona
l:tri
enni
al s
urve
y du
e th
is y
ear
lab
serv
ices
m
onito
ring
(inte
rnal
and
ex
tern
al),
Stan
dard
Tr
eatm
ent
Guid
elin
es,
Stan
dard
O
pera
ting
Proc
edur
es
regi
onal
aud
it fo
rmul
ary
revi
ew (b
i-an
nual
) &
Drug
Fo
rmul
ary
revi
ew
(qua
rterly
)
ISO
134
85,
annu
al
mon
itorin
g
Shar
epoi
nt,
ongo
ing
mon
itorin
g
NAFD
AC:
mon
itorin
g tw
ice
a ye
ar,
ISO
900
1 (a
ccre
dita
tion
is fo
rese
en in
fu
ture
)
Pfize
r and
GSK
in
tern
al a
udits
ta
ke p
lace
bi-
annu
ally
Corp
orat
e gi
ving
sN/
A
USD
21,0
00
to V
illag
e of
Ho
pe.
Hosp
ital
incl
udin
g an
or
phan
gae
for H
IV
infe
cted
ch
ildre
n
All c
orpo
rate
gi
ving
is
cond
ucte
d th
roug
h th
e Hy
geia
fo
unda
tion
All c
orpo
rate
gi
ving
is
cond
ucte
d th
roug
h th
e Hy
geia
fo
unda
tion
174
hour
s,
Free
med
ical
ca
mps
, de
wor
mon
g sc
hool
ch
ildre
n
Clea
ning
at a
ba
bies
' hom
e,
heal
th
prom
otio
n ac
tiviti
es in
th
e co
mm
unity
, pa
rtici
patio
n in
cha
rity
mar
atho
n
Mw
anan
yam
ala
Hosp
ital:
dona
tion
of
mos
quito
ne
ts&
beds
heet
s. If
tar
Day:
25
staf
f pa
rtici
pate
d in
ser
ving
fo
od. E
nviro
nm
enta
l Day
: 10
sta
ff pa
rtici
pate
d in
cl
eani
ng&
don
ated
cl
eani
ng
equi
pmen
ts.
Mal
aria
day
: do
natio
n of
m
osqu
ito
nets
180
hour
s m
onth
ly
Ever
y em
ploy
ee is
ob
ligat
ed to
sp
end
at
leas
t 5 h
rs in
ch
arita
ble
activ
ities
. Co
ordi
nate
d th
roug
h Be
ckm
ann
Fund
N/A
None
KHL
offe
rs th
e ch
ange
for
med
ical
st
uden
ts to
co
me
to th
e ho
spita
l fro
m
Lago
s in
ord
er
to b
e ex
pose
d to
the
MRI
sy
stem
and
le
arn
from
it
(this
is d
one
for
free)
. No
estim
antio
n of
ho
urs
used
by
empl
oyee
s is
av
aila
ble.
NGN
2,38
0,00
0 NA
FDAC
, PSN
, AC
PN
Conf
eren
ces
and
NGN
3,50
0,00
0 do
natio
n to
TCF
fo
r Eye
care
Pr
ojec
ts
None
** P
lan
in p
lace
to im
plem
ent
* By
nat
ure
of A
AR b
usin
ess
we
do n
ot h
ave
such
cas
es. F
urth
er A
AR is
mem
ber o
f the
UN
Glob
al C
ompa
ct th
at u
phol
ds th
ese
prin
cipl
es

A
nnexes
35 ESD Performance Report 2013
Subs
idar
ies I
FHA
Port
folio
co
mpa
nies
whi
ch h
ave
been
m
easu
red
sepe
rate
ly >
>>
AAR
HC
Tanz
ania
(2
013)
Pyra
mid
Ph
arm
a (2
013)
Hyge
ia H
MO
(2
013)
Hyge
ia
Hosp
itals
(201
3)
AAR
HC
Keny
a (2
013)
AAR
HC
Ugan
da
(201
3)
AAR
Insu
ranc
e Ta
nzan
ia
(201
3)
AAR
Insu
ranc
e Ug
anda
(201
3)
AAR
Insu
ranc
e Ke
nya
(201
3)
Sour
celin
k He
alth
care
(2
013)
ER C
orpo
rate
Ad
min
istra
tion
(201
3)
Kam
pala
Ho
spita
l (20
13)
WW
CVL
Nig
eria
(201
3)W
HL G
hana
(2
013)
Obj
ectiv
e: R
educ
e en
viro
nmen
tal i
mpa
ctPr
oced
ures
in p
lace
rela
ted
to th
e fo
llow
ing
aspe
cts:
Was
te m
anag
emen
tYE
SYE
SNO
YES
YES
YES
NOYE
SNO
YES
NONO
YES
YES
Ener
gy u
seNO
NOYE
SYE
SNO
NONO
NONO
NONO
NOYE
SYE
SW
ater
man
agem
ent
NONO
YES
YES
NONO
NONO
YES
NONO
NOYE
SYE
SOc
cupa
tiona
l Hea
lth a
nd S
afet
yYE
SYE
SYE
SYE
SYE
SNO
YES
YES
YES
YES
YES
NOYE
SYE
S
Envi
ronm
enta
l, he
alth
and
saf
ety
licen
ses
requ
ired
for t
he
com
pany
's o
pera
tion:
YES,
med
ical
w
aste
in
cine
ratio
n ce
rtific
ates
, an
nual
pr
actic
ing
certi
ficat
es
for m
edic
al
wor
kers
, fire
ce
rtific
ates
Tanz
ania
Fo
od a
nd
Drug
Au
thor
ity,
Priv
ate
Heal
th
Labo
rato
ry
Boar
d
N/A
Lice
nse
for a
ll fa
cilit
ies
from
He
alth
Fac
ility
M
onito
ring
and
Accr
edita
tion
Agen
cy
Natio
nal
Envi
ronm
ent
al
Man
agem
ent
Aut
horit
y au
dits
don
e
Ope
ratin
g lic
ence
s fo
r cl
inic
s,
Prac
ticin
g lic
ence
s fo
r m
edic
al
pers
onne
l
Heal
th a
nd
safe
ty
licen
ce
thro
ugh
OSH
A
Med
ical
w
aste
in
cine
ratio
n ce
rtific
ates
, an
nual
pr
actic
ing
certi
ficat
es
for m
edic
al
wor
kers
Occ
upat
iona
l he
alth
and
sa
fety
No
neNo
ne
Lice
nse
to
pose
ss a
nd u
se
radi
atio
n.
Ope
ratio
nal
licen
se o
f He
alth
Uni
t Pr
emis
es
N/A
Phar
mac
y lic
ense
, fire
sa
fety
and
fu
mig
atio
n lic
ense
, fo
od
and
drug
au
thor
ity
licen
se
Are
all r
equi
red
licen
ses
in p
lace
?YE
SYE
SNO
YES
YES
YES
NOYE
SYE
SN/
AN/
AYE
SN/
AYE
SNu
mbe
r of n
ew li
tigat
ion
char
ges
rela
ted
to e
nviro
nmen
tal i
ssue
s in
th
e la
st 1
2 m
onth
s:0
00
00
0N/
A0
00
N/A
00
0
Num
ber o
f (in
ter)n
atio
nal
envi
ronm
enta
l cer
tific
atio
n(s)
/ ac
cred
itatio
n(s)
:If
any
accr
edita
tion
is a
vaila
ble
plea
se s
peci
fy w
hich
.
00
N/A
2 - F
ire
certi
ficat
e of
fa
cilit
ies
and
Radi
atio
n Pr
otec
tion
certi
ficat
e
NEM
A ce
rtific
atio
n fro
m th
e au
dits
0N/
A0
00
N/A
00
N/A
Tota
l ene
rgy
cons
umpt
ion
Elec
trici
ty:
4,24
8,64
8 KW
H Di
esel
: 46
80 li
ters
Non-
rene
wab
le
sour
ces
(Tan
esco
): 2,
9321
,016
Elec
trici
ty: N
GN
9,31
2,50
9 /
Dies
el N
GN:
24,6
72,5
00
No d
ata
avai
labl
e
Rene
wab
le:
KES
608,
335,
No
n-re
new
able
: KE
S 1,
693,
307
Non
rene
wab
le
sour
ces:
Di
esel
260
0 lit
ers
Elec
trici
ty
KWH:
60,
000
- Die
sel
21,6
00
Elec
trici
ty:
KWH
26,1
81
Elec
trici
ty:
KES
1,32
1,32
4
Non-
rene
wab
le:
ZAR
26,5
70
No d
ata
avai
labl
egr
id (h
ydro
) KW
H: 2
96,8
37
Dies
el: 2
91,2
44
litre
s, G
asol
ine
40,5
89 li
ters
No d
ata
avai
labl
e
Plea
se s
tate
whi
ch lo
catio
ns a
re
incl
uded
in th
is m
easu
rem
ent.
Heal
th
Cent
res,
Ad
min
istra
tion
offi
ces,
Am
bula
nces
(re
scue
)
Offi
ce a
nd
war
ehou
se
214
Broa
d St
reet
, Ele
phan
t Ho
use,
Lag
osN/
AAl
l 13
clin
ics
Heal
th
cent
res,
Ad
min
istra
tion
offi
ces,
am
bula
nces
Chat
o &
Ar
usha
, M
ikoc
heni
, Ha
ider
y Co
mpl
ex,
Soph
ia P
laza
Lt
d.
Head
offi
ce,
Sale
s of
fice
Amou
nt
incl
udes
El
ectri
city
&W
ater
at t
he
bran
ches
.For
th
e He
ad
Offi
ce,
Elec
trici
ty
cost
is
incl
uded
in
the
Rent
Onl
y 1
loca
tion
N/A
Kam
pala
Ho
spita
l
War
ehou
se,
Lago
s an
d Em
ma
Plaz
a,
Lago
s
Prem
ises
in
Accr
a (K
umas
si
not i
nclu
ded)
Tota
l wat
er w
ithdr
awal
(lite
rs):
No d
ata
avai
labl
e
TZS
3,15
8,00
0 (li
ters
un
know
n)
Unkn
own
No d
ata
avai
labl
e1,
908,
000
N/A
1200
02,
254,
000
No d
ata
avai
labl
e12
2,55
0Un
know
n6,
562,
000
600,
000
liter
s76
2
Plea
se s
tate
whi
ch lo
catio
ns a
re
incl
uded
in th
is m
easu
rem
ent.
N/A
War
ehou
se21
4 Br
oad
Stre
et, E
leph
ant
Hous
e, L
agos
N/A
All 1
3 cl
inic
sN/
AM
ikoc
heni
, Ar
usha
, M
wan
za
Head
offi
ce,
Sale
s of
fice
N/A
Onl
y 1
loca
tion
N/A
N/A
War
ehou
se,
Lago
s
Prem
ises
in
Accr
a (K
umas
si
not i
nclu
ded)

A
nnexes
36 ESD Performance Report 2013
Annex 4: ESD audits per sector
Sect
or: H
ealth
care
pro
visi
onAA
R HC
Ken
ya (2
013)
Lago
on H
ospi
tals
Hyge
ia N
iger
ia
(201
3)AA
R HC
Uga
nda
(201
3)AA
R HC
Tan
zani
a (2
013)
Kam
pala
Hos
pita
l (20
13)
Obj
ectiv
e: In
crea
se a
vaila
bilit
y of
pr
oduc
ts a
nd se
rvic
esTo
tal n
umbe
r of h
ealth
care
faci
litie
sFo
r eac
h fa
cilit
y, li
st th
e ty
pe a
nd lo
catio
n (a
ddre
ss).
13 u
rban
faci
litie
s5
urba
n fa
cilit
ies
7 ur
ban
faci
litie
s 5
urba
n fa
cilit
ies
1 ur
ban
faci
lity
Will
iam
son
Hous
e -
Nairo
biHo
spita
l - A
papa
, Lag
osAc
acia
Hea
lth c
entre
- Ka
mpa
laCh
ato
Heal
th C
entr
e, C
hato
Str
. Dar
es S
alaa
mKa
mpa
la H
ospi
tal,
plot
6 C
Mak
indu
Cl
ose,
Kol
olo
Sarit
Cen
tre C
linic
- Na
irobi
Hosp
ital-
Ikej
a, L
agos
City
cen
tre h
ealth
cen
tre -
Kam
pala
City
Cen
tre
Clin
ic (H
ealth
Cen
tre)
, Mak
taba
Sq
uare
Str
. Dar
es S
alaa
mCi
ty C
entre
Ciln
ic -
Nairo
biCl
inic
- Vi
ctor
ia Is
land
, Lag
osBu
golo
bi H
ealth
cen
tre -
Kam
pala
Arus
ha H
ealth
Cen
tre,
Phi
llips
Roa
d, A
rush
a
Mom
basa
Clin
ic -
Mom
basa
Spec
ialis
t clin
ic -
Vict
oria
Isla
nd, L
agos
Bwey
oger
ere
Heal
th c
entre
- Bw
egog
erer
eSi
nza
Heal
th C
entr
e, S
inza
Mad
ukan
i, Da
r es
Sala
amEl
dore
t Clin
ic -
Eldo
ret
Clin
ic -
Ikej
a, L
agos
Gulu
Hea
lth c
entre
- Gu
lu
Kisu
mu
Clin
ic -
Kisu
mu
Ntin
da H
ealth
cen
tre -
Kam
pala
Naku
ru C
linic
- Na
kuru
Kaba
laga
la H
ealth
cen
tre -
Kam
pala
Kare
n Cl
inic
-
Na
irobi
Thik
a Ro
ad C
linic
- Na
irobi
Park
land
s Cl
inic
- Na
irobi
Adam
s Cl
inic
- Na
irobi
Emba
kasi
Clin
ic,
Nairo
biM
ount
ain
Mal
l, Na
irobi
Tota
l num
ber o
f mob
ile c
linic
s ow
ned
by th
e co
mpa
ny:
00
00
0
MRI
01
00
1Ne
onat
al in
cuba
tor
07
00
4X
ray
mac
hine
s2
20
01
CT sc
anne
rs0
10
01
ECGs
107
24
1Ul
traso
und
54
11
2Ne
bulis
ers
185
64
2EE
G 0
00
00
TB d
iagn
osis
mac
hine
s13
00
00
Phar
mac
ies
133
77
1La
bora
torie
s13
37
71
Num
ber o
f hea
lthca
re fa
cilit
ies
whi
ch o
ffer
serv
ices
for e
ach
of th
e fo
llow
ing
cond
ition
s/ca
re
area
s M
edic
alHy
perte
nsio
n13
57
81
Hype
rlipi
dem
ia13
57
81
Diab
etes
135
78
1As
thm
a13
57
81
Card
iac
cond
ition
s13
57
41
Surg
ical
Card
iac
01
00
0Ca
rdio
thor
acic
01
00
0Ne
urol
ogic
al0
10
01
Num
ber o
f pat
ient
s tre
ated
for e
ach
of th
e fo
llow
ing
cond
ition
s/ca
re a
reas
:M
edic
alHy
perte
nsio
n16
4637
5839
6260
0un
know
nHy
perli
pide
mia
261
7129
1no
t rec
orde
dun
know
nDi
abet
es63
120
0383
0no
t rec
orde
dun
know
nAs
thm
a12
3035
264
1no
t rec
orde
dun
know
nCa
rdia
c co
nditi
ons
5026
9457
36Su
rgic
alCa
rdia
c0
2593
0N
/A0
Card
ioth
orac
ic0
280
N/A
0Ne
urol
ogic
al22
10
N/A
0
Fac
tory
Clin
ics (
Waz
o, C
oca
Cola
, Po
lyce
m/R
affia
, Sou
ther
n Su
n -D
ar e
s Sal
aam
, Ta
nga
Clin
ic-T
anga
)-(D
ispe
nsar
ies)

A
nnexes
37 ESD Performance Report 2013
Sect
or: H
ealth
care
pro
visi
onAA
R HC
Ken
ya (2
013)
Lago
on H
ospi
tals
Hyge
ia N
iger
ia
(201
3)AA
R HC
Uga
nda
(201
3)AA
R HC
Tan
zani
a (2
013)
Kam
pala
Hos
pita
l (20
13)
Num
ber o
f pat
ient
s tre
ated
for e
ach
of th
e fo
llow
ing
cond
ition
s/ca
re a
reas
:M
alar
ia11
6666
7017
9030
00No
t rec
orde
dDi
arrh
eal d
iseas
e (e
.g. C
hole
ra)
3458
173
299
480
Not r
ecor
ded
Mal
nutri
tion
50
2No
t rec
orde
dNo
t rec
orde
dHI
V/AI
DS13
112
012
11N/
ANo
t rec
orde
dTB
9558
24N/
ANo
t rec
orde
dM
ater
nal c
are
545
8504
2483
1140
Not r
ecor
ded
Num
ber o
f hea
lthca
re fa
cilit
ies
whi
ch o
ffer
serv
ices
for e
ach
of th
e fo
llow
ing
cond
ition
s/ca
re
area
:M
alar
ia13
57
91
Diar
rhea
l dise
ase
(e.g
. Cho
lera
)13
57
91
Mal
nutri
tion
135
74
1HI
V/AI
DS13
57
01
TB13
57
01
Mat
erna
l car
e13
57
41
Obj
ectiv
e: In
crea
se a
ffor
dabi
lity
of
prod
ucts
and
serv
ices
Num
ber o
f hea
lthca
re fa
cilit
ies
whi
ch o
ffer
serv
ices
for e
ach
of th
e fo
llow
ing
care
are
as:
Child
car
e re
late
d to
the
5 m
ain
caus
es o
f dea
th13
57
41
Mea
sles i
mm
uniza
tion
134
71
1Ot
her i
mm
uniza
tions
KE
PI: 1
3He
patit
is B
:4 ,
OPV
:4, D
PT:4
7He
patit
is B
Vac
cine
: 40
Surg
ery
01
00
0Tr
aum
a0
50
00
Num
ber o
f pat
ient
s tre
ated
for e
ach
of th
e fo
llow
ing
care
are
as:
Child
car
e re
late
d to
the
5 m
ain
caus
es o
f dea
th95
931
14No
t rec
orde
dNo
t rec
orde
dNo
t rec
orde
dM
easle
s im
mun
izatio
n11
3349
0No
t rec
orde
dNo
t rec
orde
dNo
t rec
orde
d
Othe
r im
mun
izatio
nsTe
tanu
s:10
36He
ptat
itis
B - 2
681,
OPV
- 39
43, D
PT -
2836
Hepa
titis
B:2
516,
Yel
low
feve
r:468
, Rot
a vi
rus:
490,
Pne
umoc
occa
l:118
8No
t rec
orde
dNo
t rec
orde
d
Pedi
atric
Not r
ecor
ded
Not r
ecor
ded
Surg
ery
059
030
00
Trau
ma
028
360
00
Do y
ou o
ffer s
ervi
ces
for t
he fo
llow
ing
cond
ition
s fo
r fre
e? If
yes
, ple
ase
spec
ify w
hich
ser
vice
s.
Mal
aria
NONO
NONO
NODi
arrh
eal d
iseas
(e.g
Cho
lera
)NO
NONO
NONO
Mal
nutri
tion
NONO
NONO
NO
HIV/
Aids
NOYE
SYE
SNO
(giv
en fo
r fre
e un
der N
atio
nal A
ids
Cont
rol P
rogr
amm
e)NO
TBNO
NONO
NO (
give
n fo
r fre
e un
der N
atio
nal T
B Co
ntro
l Pro
gram
me)
NO
Mat
erna
l Car
eNO
NONO
NONO
Child
car
e re
late
d to
the
5 m
ain
caus
es o
f dea
thNO
NONO
YES
NO
Mea
sles i
mm
uniza
tion
YES
- und
er K
EPI
imm
unia
tion
NOYE
SYE
SYE
S

A
nnexes
38 ESD Performance Report 2013
Sect
or: H
ealth
care
pro
visi
onAA
R HC
Ken
ya (2
013)
Lago
on H
ospi
tals
Hyge
ia N
iger
ia
(201
3)AA
R HC
Uga
nda
(201
3)AA
R HC
Tan
zani
a (2
013)
Kam
pala
Hos
pita
l (20
13)
Low
est p
riced
ser
vice
s of
fere
d:GP
con
sulta
tion
KES
700
- # 1
,267
pa
tient
s tre
ated
Mar
k up
= -3
0%, m
anag
ed c
are
patie
nts
pay
30%
less
than
priv
atel
y in
sure
d.
Chec
king
Blo
od P
ress
ure
(200
0 TZ
S)
List
pha
rmac
eutic
als
(and
thei
r cor
resp
ondi
ng
cond
ition
s) w
hich
hav
e ex
perie
nced
sho
rtage
s in
th
e pr
evio
us y
ear:
Phar
mac
eutic
al (c
ondi
tion)
- Fr
eque
ncy
- Rea
son
for s
horta
ge
Phar
mac
eutic
al (c
ondi
tion)
- Fr
eque
ncy
- Re
ason
for s
horta
ge
Phar
mac
eutic
al (c
ondi
tion)
- Fr
eque
ncy
- Re
ason
for s
horta
ge
Phar
mac
eutic
al (c
ondi
tion)
- Fr
eque
ncy
- Rea
son
for s
horta
ge
Tote
rodi
ne 2
mg
- 6 -
com
pany
had
pr
oble
ms
at m
anuf
actu
ring
plan
tCo
arte
m (M
alar
ia) -
1 -
Shor
tage
of t
he
AMFM
Pro
ject
-sub
sidi
sed
drug
sNi
lTa
b. P
iogl
itazo
ne -
regu
latio
n fro
m N
DANo
rmal
sal
ine
nasa
l - 5
- log
istic
s pr
oble
m w
ith im
porta
tion
of d
rug
ARVs
(HIV
-AID
S) -
1 - I
ncon
sist
ence
in th
e lo
gist
ics
and
supp
ly d
epar
tmen
t at J
MS
Inj.
Phen
ytoi
n - o
ut o
f sto
ck fr
om
supp
liers
Mid
azol
am in
ject
ions
- 4
- log
istic
s pr
oble
m w
ith im
porta
tion
of d
rug
Bact
ocla
v 37
5mg
Tabl
ets
(Infe
ctio
ns) -
1 -
Out
of s
tock
with
our
pre
-qua
lifie
d su
pplie
r
I.V. M
anni
tol -
out
of s
tock
from
su
pplie
rs
Feno
fibra
te -
3 - c
ompa
ny s
topp
ed
prod
ucin
g be
caus
e of
redu
ced
dem
and
in N
iger
ia
Inj.
Fent
anyl
- ou
t of s
tock
from
su
pplie
rs
Amio
daro
ne in
ject
ion
- 3 -
logi
stic
s pr
oble
m w
ith im
porta
tion
of d
rugs
Salb
utam
ol in
hale
r - 2
- Su
pplie
r out
of
stoc
k
Obj
ectiv
e: E
nsur
e qu
ality
of p
rodu
cts
and
serv
ices
Drug
- am
ount
- ty
pe o
f uni
t - to
tal
valu
eDr
ug -
amou
nt -
type
of u
nit -
tota
l val
ueDr
ug -
amou
nt -
type
of u
nit -
tota
l val
ueDr
ug -
amou
nt -
type
of u
nit -
to
tal v
alue
List
pha
rmac
eutic
als
(and
thei
r cor
resp
ondi
ng
cond
ition
s) w
hich
hav
e ex
pire
d in
the
prev
ious
ye
ar:
Adre
nalin
e - 2
3 -1
MG/
ML
inje
ctio
n -
NGN
276
PRIO
RIX
0.5M
L (M
MR)
VAC
CINE
- 56
- VI
AL -
UGX
1,25
9,34
4Is
opha
ne B
i-pha
sic
Inj 1
0IU/
ml-w
osul
in -
1 -
am
p - T
ZS 1
5400
Zyce
l 100
mgs
- 40
- ta
bs -
UGX
6,40
0
Antis
nake
ven
om -
3 -in
ject
ion
- N
32,5
00VA
XIGR
IP S
H AD
ULT
1ML
(INFL
UENZ
A)-1
0-VI
AL-U
GX 3
58,9
00Tr
amad
ol 1
00m
g In
j-urg
endo
l - 2
- am
p -
TZS
5600
Am
ino
Acid
s - 3
- bo
ttles
- UG
X 10
5,00
0Ch
loph
enira
min
e ta
bs -
140
- tab
lets
- N3
0LI
PICA
RD 2
00M
G-22
4-Ca
psul
es-U
GX
192,
000
Emes
et 4
mg/
2ml -
5 -
amp
- TZS
125
00Do
pam
ine
- 3 -
Inje
ctio
n - U
GX
45,0
00Hu
mal
og in
sulin
e - 4
- 10
iu/m
l -
N32,
500
CIM
ETID
INE
400
MG
TABL
ETS-
666-
Tabl
ets-
UGX
64,4
36Vi
tam
in B
com
plex
Inj.
im/iv
10m
ls-e
styp
lex
- 24
- am
p - T
ZS 3
00,0
00Ni
fedi
pine
Dro
ps -
90 -
UGX
8,00
0
Teta
nu im
mun
oglo
bulin
- 2
- 250
iu
inje
ctio
ns -
N3,8
50PI
ONO
RM 3
0MG
TABL
ETS-
718-
Tabl
ets-
UGX
219,
968
Chlo
rhex
idin
e Tu
lle G
ras-
bact
igra
s - 6
9 -
each
- TZ
S 10
0,05
0
List
the
tota
l val
ue o
f pha
rmac
eutic
als
disp
ense
d in
the
prev
ious
yea
r:Ge
neric
dru
gs: N
GN 1
41,1
57,5
79Ge
neric
dru
gs: U
GS 2
,134
,153
,476
Gene
ric d
rugs
: UGX
80,
000,
000
Bran
ded
drug
s: N
GN 7
,429
,346
Bran
ded
drug
s: U
GS: 5
24,9
55,7
30Br
ande
d dr
ugs:
UGX
25,
000,
000
List
the
med
ical
sup
plie
s w
hich
hav
e ex
perie
nced
sh
orta
ges
mor
e th
an o
nce:
Med
ical
sup
ply
Freq
uenc
yRe
ason
fo
r sh
orta
ge
Elas
topl
ast
3O
ut o
f st
ock
None
Tong
ue D
epre
ssor
s - 2
- no
sup
plie
r had
it
in s
tock
None
Phen
ytoi
n in
j - 2
- ou
t of s
tock
fro
m s
uppl
iers
Prim
apor
e m
ediu
m2
Out
of
stoc
kUl
tra s
ound
gel
- 2
- no
supp
lier h
ad it
in
stoc
kCe
ll Pa
ck -
3 - o
ut o
f sto
ck fr
om
supp
liers
Need
les
25G
4O
ut o
f st
ock
Typh
oid
Strip
s - 2
- O
ut o
f sto
ck w
ith o
ur
pre-
qual
ified
sup
plie
rM
anni
tol I
V - 1
- ou
t of s
tock
from
su
pplie
rs
Sutu
res
reve
rse
cut
5O
ut o
f st
ock
Plas
tic c
onta
iner
s3
Out
of
stoc
k
Hexa
niou
s so
lutio
n2
Out
of
stoc
kBa
ctrig
ras
3
Num
ber o
f tot
al h
ealth
faci
litie
s th
at a
re
certi
fied/
accr
edite
d an
d w
ith w
hich
bo
dy/o
rgan
izatio
n:0
2 - J
CI0
00
Typh
im m
ultid
ose
- vac
ine
- 19
- via
l - K
ES
8,22
9
Cym
alta
30m
g - A
nxie
ty -
6 - K
ES 9
86
Cycl
ogyl
eye
dro
ps -
1 - t
ube
- KES
410
Tam
oxife
n - C
a br
east
- 15
- ta
blet
- KE
S 65
0
1,01
2,52
0,23
1 TZ
S (F
or b
oth
Gene
ric &
Br
ande
d)Br
ande
d dr
ugs:
KES
85,
133,
968
Co-m
icar
dis
- 1 -
out o
f sto
ck
Esos
ip 4
0mg
- 2 -
out o
f sto
ck
Gene
ric d
rugs
: KES
127
,251
,292
Dexa
-G -
4 - o
ut o
f sto
ck
Duof
ilm s
olut
ion
- 6 -
out o
f sto
ck
Glyf
orm
in 5
00/8
50m
g - 3
- ou
t of s
tock
Alda
cton
e 25
- 2
- out
of s
tock
Zolid
plu
s - 3
- ou
t of s
tock
Epan
utin
- 1
- out
of s
tock
Phar
mac
eutic
al (c
ondi
tion)
- Fr
eque
ncy
- Re
ason
for s
horta
ge
Drug
- am
ount
- ty
pe o
f uni
t - to
tal v
alue
Piog
lit 3
0mg
- Dia
btes
- 30
- ta
blet
- KE
S 85
0.00
Hum
alog
Car
t - D
iabt
es -
25 -
cartr
idge
- KE
S 19
,605

A
nnexes
39 ESD Performance Report 2013
Sect
or: H
ealth
care
pro
visi
onAA
R HC
Ken
ya (2
013)
Lago
on H
ospi
tals
Hyge
ia N
iger
ia
(201
3)AA
R HC
Uga
nda
(201
3)AA
R HC
Tan
zani
a (2
013)
Kam
pala
Hos
pita
l (20
13)
Obj
ectiv
e: E
nsur
e eq
uita
ble
acce
ss
to p
rodu
cts a
nd se
rvic
esTo
tal n
umbe
r of p
atie
nts:
67,6
7914
,506
215,
000
Not r
ecor
ded
14,4
85To
tal n
umbe
r of v
isits
a y
ear:
250,
444
49,0
3121
5,00
011
3,99
614
,011
Tota
l num
ber o
f hos
pita
l adm
issi
ons:
230,
958
2,43
90
Not r
ecor
ded
474
Num
ber o
f hea
lthca
re w
orke
rs:
395
7011
580
29To
tal n
umbe
r of G
Ps:
140
5728
136
Tota
l num
ber o
f nur
ses:
6514
547
2587
Tota
l num
ber o
f spe
cial
ists
:44
2423
1955
Bed
occu
panc
y ra
te (B
OR)
:N/
A76
.00%
Not r
ecor
ded
Not r
ecor
ded
20
Obj
ectiv
e: R
educ
e en
viro
nmen
tal
impa
ctPr
oced
ures
for w
aste
dis
posa
l in
plac
eYE
SYE
SYE
SYE
SNO
Tota
l am
ount
of h
azar
dous
was
te g
ener
ated
(in
tonn
es):
15.5
56No
t rec
orde
d8,
416
6 to
nnes
Not r
ecor
ded
Tota
l am
ount
of n
on-h
azar
dous
was
te g
ener
ated
(in
tonn
es):
7.34
9No
t rec
orde
d11
,3No
reco
rded
Not r
ecor
ded
Obj
ectiv
e: S
timul
ate
dece
nt w
ork
Heal
th a
nd s
afet
y pr
oced
ures
in p
lace
:YE
SYE
SYE
SYE
SNO
Prot
ectio
n eq
uipm
ent f
or e
mpl
oyee
s ag
ains
t ha
zard
ous
subs
tanc
es a
nd d
isea
ses
avai
labl
e at
he
alth
care
faci
litie
s:YE
SYE
SYE
SYE
SYE
S
Num
ber o
f wor
k re
late
d in
jurie
s:0
00
0No
t reg
iste
red
Num
ber o
f fat
aliti
es:
00
00
Not r
egis
tere
dTo
tal h
ours
wor
ked:
141,
520
926,
592
309,
000
199,
760
360,
976
Num
ber o
f pe
ople
pro
vide
d w
ith b
asic
med
ical
tra
inin
g:15
127
915
014
60

A
nnexes
40 ESD Performance Report 2013
Sect
or: H
ealth
Insu
ranc
e
Obj
ectiv
e: In
crea
se a
vaila
bilit
y of
pro
duct
s and
serv
ices
Tota
l num
ber o
f pro
vide
rs:
Num
ber o
f hea
lth in
sura
nce
brok
ers/
sal
es
repr
esen
tativ
es:
Plea
se li
st in
sura
nce
pack
ages
pro
vide
d by
th
e co
mpa
ny, i
nclu
ding
pric
e an
d to
tal
num
ber o
f mem
bers
:
Insu
ranc
e pa
ckag
e
Pric
e pe
r ye
ar (a
nd
curre
ncy)
# m
embe
rs
urb
an
Insu
ranc
e pa
ckag
e P
rice
per y
ear
(and
cur
renc
y)
#
mem
bers
ur
ban
Insu
ranc
e pa
ckag
ePr
ice
per y
ear
(and
cur
renc
y)
# m
embe
rs
urba
n
Insu
ranc
e pa
ckag
ePr
ice
per y
ear (
and
curre
ncy)
# m
embe
rs
urba
n
HYES
SENT
IAL
Plus
26
,450
.00
4
5,47
3 C
orpo
rate
4
00,0
00.0
0
7,71
2.00
Go
ldUS
D 55
1 - 2
968
2,9
31
Gold
KES
790
57
6,0
56
HYPR
IORI
TY P
lus
28
,750
.00
1
7,27
2 B
ronz
e
5
50,0
00.0
0 2
6,69
5.00
Si
lver
USD
471-
234
0
9
,991
Si
lver
KE
S 71
881
28,
462
HYCL
ASSI
C Pl
us
39,8
00.0
0
32,
375
Silv
er
1
,250
,000
.00
1,
072.
00
Bron
zeUS
D 31
8- 1
578
29,6
96
Bron
zeKE
S 3
1147
21,
196
HYPR
ESTI
GE P
lus
143
,750
.00
3,4
98.0
0 G
old
2
,200
,000
.00
698.
00
HMO
USD
300-
771
9
17
Cove
r Me
KES
1048
2
3,0
72
GCUS
D 32
5
45
,477
Gr
oupc
are
IPCu
stom
ised
3
,368
In
patie
ntUS
D 16
5-81
9
293
Re
scue
US
D 25
0
9 Af
ya M
aish
aUS
D 89
2
19
Out
patie
ntUS
D 17
5 N
A
Obj
ectiv
e: E
nsur
e eq
uita
ble
acce
ss to
pro
duct
s and
serv
ices
Num
ber o
f fem
ales
mem
bers
and
de
pend
ents
:53
,273
16,9
7834
,220
35,4
56
Num
ber o
f chi
ld d
epen
dent
s:33
,887
12,9
4311
,271
16,7
89
Hyge
ia H
MO
(201
3)AA
R In
sura
nce
Keny
a (2
013)
Ow
n pr
ovid
ers:
15,
pre
ferre
d pr
ovid
ers:
404
6057
6
AAR
Insu
ranc
e Ta
nzan
ia (2
013)
AAR
Insu
ranc
e Ug
anda
(201
3)
Ow
n pr
ovid
ers:
3 P
reffe
red
prov
ider
s: 5
Ow
n pr
ovid
ers
9, p
reffe
red
prov
ider
s 17
8
923
Ow
n pr
ovid
ers:
8, p
reffe
red
prov
ider
s 25
1

A
nnexes
41 ESD Performance Report 2013
Sect
or: H
ealth
Insu
ranc
e
Obj
ectiv
e: In
crea
se
affo
rdab
ility
of p
rodu
cts a
nd
serv
ices
Low
est c
ost i
nsur
ance
pac
kage
pro
vide
d.Pl
ease
spe
cify
pric
e (a
nd c
urre
ncy)
and
to
tal m
embe
rs:
HYGE
IA
ESSE
NTIA
L NG
N 26
450
- 454
73
mem
bers
Corp
orat
e Ca
rd
UGX
400,
000
- 7,
712
mem
bers
Bron
ze T
ZS
3946
80-
2072
070
-28
696
mem
bers
Cove
r me:
KES
10
,482
- 32
247:
307
2 m
embe
rs
Serv
ices
cov
ered
in th
e lo
wes
t cos
t in
sura
nce
pack
age:
Med
ical
Hype
rtens
ion
YES
YES
YES
NOHy
perli
pide
mia
YES
YES
YES
NODi
abet
esYE
SYE
SYE
SYE
SAs
thm
aYE
SYE
SYE
SNO
Card
iac
cond
ition
sYE
SYE
SYE
SNO
Surg
ical
Card
iac
NO
YES
YES
NOCa
rdio
thor
acic
NOYE
SYE
SNO
Neur
olog
ical
NOYE
SYE
SNO
Pedi
atric
Surg
ery
YES
YES
YES
NOTr
aum
aYE
SYE
SYE
SYE
SDi
seas
es o
f pov
erty
Mal
aria
YES
YES
YES
YES
Mal
nutri
tion
YES
YES
YES
NOHI
V/Ai
dsYE
SYE
SYE
SYE
STB
YES
YES
YES
YES
Mat
erna
l car
eYE
SYE
SYE
SYE
SCh
ild c
are
rela
ted
to 5
mai
n ca
uses
of
deat
hYE
SYE
SNO
YES
Mea
sles i
mm
uniza
tions
YES
YES
YES
YES
Low
cos
t ins
uran
ce p
acka
ges
prov
ided
in
partn
ersh
ip.
If ye
s, p
leas
e st
ate
the
tota
l num
ber o
f m
embe
rs c
omin
g fro
m e
ach
of th
ese
sche
mes
.
YES:
HIF
NONO
YES:
HIF
: tot
al
mem
bers
2,
347
Obj
ectiv
e: E
nsur
e qu
ality
of
prod
ucts
and
serv
ices
Num
ber o
f hea
lthca
re p
rovi
ders
in y
our
netw
ork
whi
ch re
ceiv
ed (i
nter
)nat
iona
l ce
rtific
atio
n/ac
cred
itatio
n:6
187
1N/
A
Qua
lity
of c
are
of th
e he
alth
care
pro
vide
rs
in y
our n
etw
ork
is m
onito
red.
If ye
s, s
tate
in w
hat f
requ
ency
(mon
thly
/ ye
arly
/ etc
) and
with
wha
t res
ult
(resu
lt/m
axim
um re
sult
poss
ible
).
YES,
yea
rly re
sult
= 65
%
YES,
qua
rterly
. Re
sult:
Con
tinue
/ Di
scon
tinue
Yes,
sem
i-an
nual
ly.
Resu
lt:
Aver
age
YES,
on
a ne
ed b
asis
- if
qual
ity is
be
low
AAR
st
anda
rd th
e pr
ovid
er is
re
mov
ed fr
om
the
AAR
pane
l
Hyge
ia H
MO
(201
3)AA
R In
sura
nce
Ugan
da (2
013)
AAR
Insu
ranc
e Ta
nzan
ia (2
013)
AAR
Insu
ranc
e Ke
nya
(201
3)

A
nnexes
42 ESD Performance Report 2013
Sector: Wholesale & DistributionObjective: Increase availability of products and servicesTotal number of drugs delivered related to the following conditions/diseases
Medical: Urban Rural Medical: Urban Rural Medical: Urban Rural
Hypertension 7466 8782 Hypertension N/A Hypertension 1575080 N/AHyperlipidemia 1271 521 Hyperlipidemia N/A N/A Hyperlipidemia 94704 N/ADiabetes 12732 10428 Diabetes 166,290 N/A Diabetes 268545 N/AAsthma 2163 603 Asthma N/A N/A Asthma 6868 N/ACardiac conditions 4024 938 Cardic
conditionsN/A N/A Cardiac
conditions246914 N/A
Malaria 36634 560550 Malaria 1143021 N/A Malaria 33750 N/ADiarrhoeal disease (e.g. Cholera)
N/A N/A Diarrhoeal disease (e.g. Cholera)
N/A N/A Diarrhoeal disease (e.g. Cholera)
254550 N/A
Malnutrition N/A N/A Malnutrition N/A N/A Malnutrition Unknown N/AHIV/AIDS HIV/AIDS
35 N/A
HIV/AIDS
None
N/A
TBC N/A N/A TBC 0 0 TBC None N/AMaternal care 154837 1670 Maternal care N/A N/A Maternal care 678870 N/AChild care Multivit
amin and mineral
2 Child care 14,306 N/A Child care Unknown N/A
Total number of medical equipment delivered (e.g. Xray, MRI, CT, ECG)
Urban Rural Urban Rural Urban Rural
0 0 0 0 0 0Total number of companies supplied through distribution channel
Urban Rural Urban Rural Urban Rural
96 0 750 0
Total number of warehouses 3 10 1 0
Objective: Ensure quality of products and services
Urban Rural Urban Rural Urban Rural Number of times not being able to deliver an order 10 20 0 0Number of times of late delivery 10 18 59 0.25% 0.50%Average time to deliver orders for rural/urban areas 2 days 5 days 48 hrs in Lagos within 24 hours within 48 hours
Inventory and stock control system in place, which ensures expiry dates are monitored
YES
Total value of items which has at least one unit at stock at the end of the previous year
unknown
Appropriate infrastructure to ensure the cold chain is maintained and in placeNumber or inventory losses due to failures within the cold train
0 0
Objective: Stimulate (local) economy and equitable access to employmentOrigin of drugs purchased Same country: 617608
In Africa: ? In Africa: 17Outside Africa: 1049468
Number of distribution accidents 0 1 0Number of fatalities 0 Unknown 0Total hours worked 127,224 609,168 Unknown
Objective: Reduce environmental impact
Policy for pharmaceuticals disposal in place YES YES YES
Outside Africa: 472
YESYES
YES
0
Same country: 0
Outside Africa:balanceIn Africa: 2
TZS 2,415,675,802 NGN 4,306,856,485
YES YES
Same country: 5
Pyramid Pharma (2013)
500 (Incl. centers throughout country)
WWCVL Nigeria (2013) WHL Ghana (2013)
Unknown
Mylan products sold, but ordered through government
Nr of units Nr of units Nr of units

A
nnexes
43 ESD Performance Report 2013
Sector: ProductionObjective: Increase availability of products and servicesMedical supplies and respective quantitites approved Type Amount
Masks 948,000Total R&D expenditures 0R&D expenditures invested in the diseases of poverty 0
Objective: Increase affordability of products and servicesPricing policies in place to ensure affordability of pharmaceuticals addressing the diseases of poverty
N/A
Patents in place for pharmaceuticals addressing the diseases of poverty
N/A
Pricing policy in place to ensure affordability of basic medical supplies
N/A
Objective: Ensure quality of products and servicesTotal number of pharmaceuticals developed N/ANumber of pharmaceuticals developed which were tested according to an (inter)nationally recognized quality standard
N/A
Total number of medical supplies developed 0Number of medical supplies developed and tested according to (inter)nationally recognized quality standards
0
Inventory and stock control systems in place, which ensures expiry dates are monitored
Inputs
YES N/ATotal value of input inventory at year end ZAR 1,057,233Total value of input losses due to expired dates NoneTotal value of produced pharmaceuticals which has at least one unit at stock at the end of the previous year
N/A
Objective: Reduce environmental impactProcedures for hazardous waste disposal in place N/ATotal amount of hazardous waste generated (in tonnes) N/ATotal amount of non-hazardous waste generated (in tonnes)
0
Total waste water generated 0
Objective: Stimulate (local) economy and equitable access to employmentImported equivalent products protected by the government in company's portfolio
NO
Local raw materials used in production process NOExisting partnerships with multi-nationals NO
Objective: Stimulate decent workOccupational Health & Safety procedures in place addressing the following topics:Maximum number of hours an employee can be working with a machine
YES
Restricted access to company's area YESSafe handling of hazardous substances YESProtection equipment for employees against hazardous substances available
YES
Number of work related injuries Own employees
0Number of fatalities Own
employees0
Total hours worked Own employees
11,310
Contractors
0
Contractors
0Contractors
0
Sourcelink Healthcare (2013)
Produced pharmaceuticals

A
nnexes
44 ESD Performance Report 2013
HYGEIA
Snapshot
How it began: Hygeia began operating in 1986, as
what has now become its flagship hospital, Lagoon
Hospital Apapa in Lagos, currently one of the four
hospitals in Nigeria offering both MRI and CT scans.
Since then the company has expanded its business to
include two further hospitals in the Ikeja and Vic-
toria Island districts of Lagos as well as two subsi-
diaries operating in the health insurance market:
Hygeia HMO and Hygeia Community Health Plan.
Hygeia HMO is a health maintenance organization
providing managed care to an enrollee base of over
300,000 individuals through a network of more than
1,200 providers across Nigeria. Hygeia Community
Health Plan is a donor-funded initiative that aims to
improve access to quality healthcare to low income
groups in Nigeria. Through the Hygeia Nigeria Li-
mited Foundation, the company also builds capacity
for medical personnel in and beyond its provider
network.
Sector: Healthcare provision, HMO
Geographic focus: Nigeria
Based in: Lagos, Nigeria
Year of investment: 2007
Business mission: Through its four companies,
Hygeia delivers primary and secondary healthcare
to the Nigerian population and strives to be the
first choice for healthcare solutions of internatio-
nal standards in Nigeria.
Annex 5: Snapshot Portfolio Companies

A
nnexes
45 ESD Performance Report 2013
Pyramid Pharma
Snapshot
How it began: Pyramid Pharma was established in
2001 as a wholesaler and retailer of quality pharma-
ceutical products and represented 13 regional and
international pharmaceutical companies in Tanzania.
It was acquired by GM Pharmacy Ltd in 2004. Pyra-
mid Pharma was the first pharmaceutical wholesaler
with a regional presence. The company has shown
significant growth and is positioned to become the
premier distributor of branded and generic drugs
in the country, as well as medical and laboratory
equipment. The company is handling importation,
distribution, marketing and distribution of drugs to
government and NGOs. Many of the supplies have
reached areas in parts of Tanzania where basic health
care did not exist or was severely interrupted. The
company has excellent relations in the private sector,
government, and development agencies. The com-
pany currently owns four branches: Ruvuma, Rukwa,
Mwanza and Mbeya.
Sector: Pharmaceutical import- and distribution
Geographic focus: Tanzania
Based in: Dar es Salaam, Tanzania
Year of investment: 2008
Business mission: to provide good quality affordable
pharmaceuticals and medical and laboratory equipment
and supplies in Tanzania.

A
nnexes
46 ESD Performance Report 2013
Strategis
Snapshot
How it began: Strategis Insurance Tanzania started
operations in 2002, as joint venture between Strate-
gis International, Heritage All Insurance Company
and Mac Group. It was registered as the first private
health insurance company in Tanzania in March
2003. Strategis offers medical insurance services. The
company utilizes various service suppliers (both local
and international). Since the start of its operations
the company has seen considerable growth in recent
years. Strategis has currently over 75,000 members
compared to 58,000 members in 2009 and 27,000 in
2008.
Sector: Health insurance
Geographic focus: Tanzania
Based in: Dar es Salaam, Tanzania
Year of investment: 2009
Business mission: to be the undisputed brand leader
in the Tanzanian health insurance arena by providing
access to quality healthcare and wellness solutions
through flexible, innovative and realistically priced
health plans.

A
nnexes
47 ESD Performance Report 2013
Hello Doctor
Snapshot
How it began: the founders of Hello Doctor ex-
perienced that across Africa there is a challenge to
provide equitable access to high quality healthcare at
low cost. Utilizing technology could help overcome
the overspending on health in the developed world
and under provisioning in the poor world. In South
Africa there is both a world class private healthcare
sector and lack of capacity and funding in the public
healthcare sector. Therefore the opportunity existed
to create a technical platform to enable the delivery
of medical resources not just in South Africa but also
throughout Africa.
Sector: Telemedicine1, healthcare delivery
Geographic focus: South Africa with potential to
collaborate throughout Africa with local HMOs
Based in: Johannesburg, South Africa
Year of investment: 2010
Year of exit: 2013
1 Telemedicine is the use of Information and Communication Technology (ICT) to provide and support healthcare activities, when distance separates the patients.
Business mission: Tele-health as a model of healthcare
delivery is expected to alleviate problems such as acces-
sibility, affordability and quality of healthcare particu-
larly in the developing world. The business is based on
four value pillars: 1) Trust; 2) Convenience; 3) Choice;
and 4) Affordability.

A
nnexes
48 ESD Performance Report 2013
AAR
Snapshot
How it began: AAR started operating in 1984 with
evacuation of medical and accident causalities,
both by road and air as its primary business. As its
membership increased, so did the need of its clients,
creating more opportunities to comprehensively
provide healthcare packages for its clients. AAR cur-
rently is the largest private healthcare company with
a footprint in the East African region. AAR operates
23 health centers located in Kenya, Uganda, and
Tanzania, providing preventive and curative primary
healthcare, rescue and evacuation and local and
international medical insurance to clients of various
income brackets. AAR has membership of around
135,000 people and is the preferred provider for both
the public and private sector in East Africa.
Sector: Healthcare, health insurance
Geographic focus: East Africa
Based in: Nairobi, Kenya
Year of investment: 2010
Business mission: AAR strives to continue to run
a sustainable and socially responsible business,
with its core values Timeliness, Caring Attitude,
Quality, Integrity and Team-ness being incorpora-
ted as the pillars in every decision and action the
company makes.

A
nnexes
49 ESD Performance Report 2013
Sourcelink
Snapshot
How it began: In 2011, IFHA finalized its investment
in Sourcelink South Africa. The core of the South
African business is the manufacturing and distribu-
tion of disposable masks, gowns, pillowslips and bed
linen. Today the factory in South Africa is establis-
hed and is in the process of manufacturing disposa-
ble products and distributing them within regional
African markets.
Sector: Production and manufacturing
Geographic focus: South Africa
Based in: Johannesburg, South Africa
Year of investment: 2011
Business mission: In Africa there is very little manu-
facturing of medical products. Besides the products
manufactured by Sourcelink South Africa, almost all
disposable masks, gowns and linen used in Africa are
imported. In many cases inferior quality products
are being imported from places like China. Kim-
berly Clark and 3M, large US listed multinationals
and manufacturers of such products, have seen their
market share reduced in many African countries due
to the unaffordable cost of their products. There is thus
a great need for affordable, but high quality disposable
infection control products in Africa.

A
nnexes
50 ESD Performance Report 2013
ER Corporate
Snapshot
How it began: In July 2012, IFHA finalized its invest-
ment in ER Corporate. ER Coporate (Pty) Ltd is a spe-
cialized medical administration and training company
and is part of the ER Group. ER Corporate manage 18
emergency and other specialist practices across South
Africa.
Sector: Medical administration and training
Geopraphic focus: South Africa
Based in: Bryanston, South Africa
Year of investment: 2012
Business mission: Training in the South African medical
landscape is essential for the development of the heal-
thcare system. Through a broad bouquet of emergency
medical courses for doctors, nurses, paramedics and
the public, the training centre completes the circle of
services for the busy medical practitioner at any level.
In partnership with IFHA, the ER Training and Deve-
lopment Centre plans to extend its services first across
South Africa and then onwards into Africa. The training
centre offers consistent quality and service to all
students on the courses and the high standards and
professionalism will ensure an excellent training
experience. The ER Training and Development
Centre has its main facility in Bryanston, Johan-
nesburg and will be rolling out further centres in
the coming months. Remote training is one of the
key differentiators of the ER training and Develop-
ment Centre. The training centre team will take the
training courses to the clients in the same profes-
sional manner as if the course was done on site at
our main facilities.

A
nnexes
51 ESD Performance Report 2013
Kampala Hospital Limited
Snapshot
How it began: In November 2013, IFHA finalized its
investment in Kampala Hospital Limited (KHL) which is
an urban hospital in Uganda with significant growth po-
tential. The total bed capacity is 109 of which 27 beds are
currently in use, with another ~30 beds almost ready for
use with limited investments. KHL is centrally located in
Kampala, the capital city of Uganda, at Kololo Hill. KHL
has a network of experienced, highly regarded and locally
well networked specialist consultants from a wide range
of specialties. Its service mix includes basic high volume
services including maternity care, malaria-related care and
simple theatre interventions. KHL will be positioned as
one of Kampala’s top mid-tier private hospitals.
Sector: Healthcare provision
Geopraphic focus: Uganda
Based in: Kampala, Uganda
Year of investment: 2013
Business mission: To establish a center of excel-
lence equipped with diagnostic facilities to enable
a quick diagnosis, irrespective of the complexity of
the disease process.

A
nnexes
52 ESD Performance Report 2013
Eco Health Limited
Snapshot
How it began:
In March 2013, IFHA finalized its investment in Eco Health
Limited. Eco Health Limited was incorporated to merge
World Wide Commercial Ventures Limited (WWCVL,
Nigeria) and Worldwide Healthcare Limited (WHL, Gha-
na) for the purpose of an exit. Eco Health Limited and its
wholly-owned group companies are engaged in the who-
lesale and retail distribution of healthcare related products
(ethical and generic pharmaceutical products, vaccines,
medical equipment, reagents and supplies, over the counter
products and veterinary medicine. The current operation
in Anglophone West Africa is the largest private healthcare
distribution business in this region.
Sector: Wholesale and distribution of healthcare
products
Geopraphic focus: Nigeria/Ghana
Based in: Mauritius
Year of investment: 2013
Business mission: To provide quality healthcare
products and services across Africa ensuring af-
fordability, availability, visibility and accessibility
within arm’s reach of the consumer .





























