Embed Size (px)
Citation preview

1
EFFECTIVE INTERVENTIONS IN SCHIZOPHRENIATHE ECONOMIC CASE
A report prepared for the Schizophrenia Commission
November 2012

2
THE AUTHORS FOREWORD
EXECUTIVE SUMMARY
CURRENT COSTS OF SCHIZOPHRENIA INPATIENTTIME DISRUPTED/LOSSOFEMPLOYMENT DISRUPTEDEDUCATION HOMELESSNESS PHYSICALHEALTHPROBLEMS SUBSTANCEMISUSE CONTACTWITHTHECRIMINALJUSTICESYSTEM FAMILYIMPACT
EVALUATING VARIOUS INTERVENTIONS EARLYINTERVENTION INDIVIDUALPLACEMENTANDSUPPORTSCHEMES FAMILYTHERAPY CRIMINALJUSTICESYSTEMDIVERSION PHYSICALHEALTH SUBSTANCEMISUSE HOMELESSNESS-TARGETEDINTERVENTIONS/SUPPORTEDHOUSING CRISISTEAMS PEER-SUPPORTWORKERS ADVANCEDTREATMENTDIRECTIVES COGNITIVEBEHAVIOURTHERAPY
CONCLUSIONS
REFERENCES
3
4
5
789101111121313
141518212223252528293031
34
36
AUTHORS Alison AndrewMartin KnappPaul McCroneMichael ParsonageMarija Trachtenberg
CONTENTS

3
THE AUTHORS
AlisonAndrewisastudentofeconomicsattheUniversityofCambridge,withaspecialinterestinhealtheconomics.ShehaspreviouslyinternedattheWorldHealthOrganisationandisDirectorforPolicyatTheWilberforceSociety,theUK’sfirststudent-runthinktank.ShewasaResearchAssistantinPSSRUattheLondonSchoolofEconomicsin2012.
MartinKnappisProfessorofSocialPolicyandDirectorofthePersonalSocialServicesResearchUnit(PSSRU)attheLondonSchoolofEconomicsandPoliticalScience.HeisalsoProfessorofHealthEconomicsatKing’sCollegeLondon,basedintheInstituteofPsychiatry.HeisDirectoroftheNIHRSchoolforSocialCareResearch.
PaulMcCroneisProfessorofHealthEconomics,andDirectoroftheCentrefortheEconomicsofMentalandPhysicalHealth,attheInstituteofPsychiatry(King’sCollegeLondon).
MichaelParsonageisChiefEconomistandSeniorPolicyAdviserattheCentreforMentalHealthandalsoaVisitingSeniorFellowattheLondonSchoolofEconomicsandPoliticalScience.
MarijaTrachtenbergrecentlycompletedaMastersattheLondonSchoolofEconomicsspecializinginhealtheconomics.ShehasworkedforbothpublicandprivatesectorswiththeCentreforMentalHealthaswellasUnitedHealthGroup.
Alison Andrew
Martin Knapp
Paul McCrone
Michael Parsonage
Marija Trachtenberg

4
FOREWORD
ThisreporthasbeenproducedtosupporttheworkoftheSchizophreniaCommissionduringitsyear-longinquiryintothecare,treatmentandoutcomesforpeoplewithschizophreniaandpsychosis.Thisillnessishighlydistressing,witha15-20yearmortalitygapcomparedtothegeneralpopulation.Thehumancostsareimmense,butsotooarethefinancialcosts.Forexample,thecostofschizophreniatoEnglishsocietyis£11.8billionperyear.
Bringingtheinformationtogetherforthisreporthasbeenchallenging.Althoughbuildingonresearchthatsomeofus(Michael,Paul,myself)haveundertakenoveraperiodofmanyyears,ithasbeenhugelyinfluencedbytheothertwoauthors:byMarija’sMScworkonpeersupportandparticularlybyAlison’s‘summerjob’atLSE,whenshesearchedenergetically,analysedexpertlyandsummarisedresultsclearlyacrossawidespanoftopics.
Itwillbeclearfromthereportthatthereareareaswherewestillknowlittleaboutthecostsofdeliveringservicesandevenlessaboutthelonger-termeconomicimpacts.Nevertheless,thereisrobustevidencearoundsomeinterventions,makingastrongeconomiccaseforchange.WehopethattheworkoftheSchizophreniaCommissioncandriveforwardsomeofthechangesrequiredtoimprovequalityofcareandqualityoflives.
WearegratefultomembersoftheSchizophreniaCommissionfortheirsupport,especiallytoLizMeekandRobinMurrayforcomments,andweareparticularlygratefultoVanessaPinfoldforherenthusiasmthroughouttheprocessofpullingthistogether.WewouldalsoliketothankPaulRowlandsandMikeAkroydfromDerbyshireHealthcareNHSFoundationTrust,andSophiaWinterbourne(LSE)foraccesstoveryusefulinformation.
TheworkforthisreportwasfundedbythePersonalSocialServicesResearchUnitattheLSE.TheauthorshavenoconflictsofinteresttodeclareexceptthatIamaVicePresidentoftheBritishAssociationofCounsellingandPsychotherapy.
PROFESSOR MARTIN KNAPPPSSRU,LondonSchoolofEconomicsandPoliticalScienceInstituteofPsychiatry,King’sCollegeLondon

5
Thisreportdescribesthemaincostsassociatedwithschizophreniaandassessestheeconomiccaseforabroadrangeofeffectiveinterventionsthat,ifmademorewidelyavailable,couldleadtobetteroutcomesandpotentiallyreducecosts.
EXECUTIVE SUMMARY
CURRENT COSTS OF SCHIZOPHRENIA
Schizophreniahasverysignificanteconomicconsequences.Costsfallonmanydifferentpartsofsociety,especiallyonindividualswithschizophreniaandtheirfamilies.Overall,thetotalsocietalcostinEnglandisestimatedat£11.8billionperyearandthecosttothepublicsectorat£7.2billion.Thisequatestoanaverageannualcosttosocietyof£60,000andtothepublicsectorof£36,000perpersonwithschizophrenia.
Thesecostsariseinmanydifferentways.Somedirectcostsofschizophreniaappearbothascoststosocietyandtothepublicsector:examplesarein-patienthospitalcostsandsupportfromcommunitymentalhealthteams.Othercosts,suchasthoseassociatedwithunpaidcarebyfamilyorfriends,areveryrealcostsforsocietybutdonothaveadirectimpactonpublicspending.Lostpotentialoutputduetohigherunemploymentratesandprematuremortalityforpeoplewithschizophreniarepresenthugecostsforsocietyandalsotranslateintoindirectcostsforthepublicsectorviathelossoftaxrevenue.Weidentifyeightkeycostdriversassociatedwithschizophrenia:inpatienttime;disrupted/lossofemployment;disruptededucation;homelessness;physicalhealthproblems;substancemisuse;contactwiththecriminaljusticesystem;andtheimpactonthefamily.
Inourworkwefoundmanyareaswheretheavailabilityandqualityofeconomicevidenceweredisappointing,bothintermsofaccuratelyestimatingthetruecostsassociatedwithschizophreniaandinbeingabletodrawfirmconclusions.Weidentifiedaparticularlackofevidencerelatingtocostsincurredthroughdisruptededucationalopportunities,homelessnessandcontactwiththecriminaljusticesystem.
Duetothenatureofschizophrenia,manyrelatedcostsarenon-retrievable.OurworkfocusedonareasofthecurrentcareandtreatmentsysteminEnglandthatcouldpotentiallybemademorecost-effective.
EVALUATING VARIOUS INTERVENTIONS
Thereareawiderangeofinterventionsthatarerelevantforthecareandtreatmentofpeoplewithschizophrenia.Inthisworkwehavelookedat:earlyinterventions;IndividualPlacementandSupportschemes;familytherapy;diversionfromthecriminaljusticesystem;physicalhealth;substancemisuse;targetinghomelessnessandsupportedhousing;crisisteams;theroleofpeer-supportworkers;advancedtreatmentdirectives;andcognitivebehaviourtherapy.

6
Whenassessingthevariousinterventions,wewerehamperedbythelackofrobusteconomicevidencerelatingtosomeofthem,inparticularphysicalhealthinterventions,advancedtreatmentdirectivesandcriminaljusticeinterventions.
Thereisneverthelessstrongevidencethatseveralinterventionsnotcurrentlyinwidespreadusecouldreducetheoverallcostofschizophreniawhileimprovinghealthandqualityoflifeoutcomesforpeoplewiththeillnessandfortheirfamilies.Oneinterventionforwhichthereisstrongcost-effectivenessevidence,butwhichisnotavailabletomanypeople,isIndividualPlacementandSupport,whichaimstohelppeoplewithschizophreniafindcompetitiveemployment.Wealsofoundgoodevidencethatfamilytherapy,currentlyofferedtoveryfewpeoplewithschizophrenia,wascost-effective.Inotherareas–suchasphysicalhealth,substancemisuse,peer-support,advancedtreatmentdirectivesandinterventionstotacklehomelessness–wefoundsomeevidenceofcost-effectivenessbutnotenoughtodrawfirmconclusions.
Theevidenceweidentifiedcamedownstronglyinsupportofearlyinterventionservicesthat,althoughcurrentlyinwidespreaduse,mightbeunderthreatinaneraofausterity.Thereisalsoevidencethatotherinterventionswhicharealreadyinplace,suchascrisisteams,couldbeutilisedmoreeffectively.
Inmanycases,economicadvantagesmighttakemanyyearstobefullyrealised.Forexample,interventionstoimprovethephysicalhealthofpeoplewithschizophreniacanbeeffectiveandcost-effective,butwithimpactsthatshowthemselvesoverquitealongperiod.Thefulleconomicconsequencesofearlyinterventionserviceswillalsonotbeseenimmediately;andthe(sofarunmeasured)
consequencesofdisruptededucationwouldcertainlyhavelong-termeconomicconsequences.Whencostsandbenefitsoccuroverlongtimeperiodsitcanbedifficulttoobtainaccurateestimatesoftheeconomicimpactsofinterventions,sincethedataarerarelyavailable.Itmayalsobeparticularlydifficultinthecurrenteraofausteritytoarguesuccessfullyforinterventionswheresavingsonlybecomeapparentoverrelativelylongtimescales.
Costsandsavingsrelatingtointerventionsdonotalwaysariseinthesameareaofpublicspending.Oneconsequentchallengeislikelytobeaneedfornegotiationtoagreejointcoursesofactionacrossgovernmentdepartments,localcouncilbudgetareasormorewidely.Agoodexamplewouldbeinterventionstotacklehomelessnesswhichcanoriginateinanumberofdifferentsectors,andhavepay-offssimilarlyacrossawiderangeofbudgets.
Itisalsothecasethatmanyinterventionscancostmorethantheysave.Heredecision-makerswillneedtoaskwhethertheimprovedoutcomesthataregeneratejustifythecoststhatwillbeincurred.
CONCLUSIONS
Itwasnotourintentionwiththisreporttorecommendaparticular‘package’ofidealinterventions,rathertoofferasummaryofevidenceoncostsandcost-effectivenessasaplatformfordiscussion.OurreviewhasestablishedthatthereareareasofthecurrentsystemforthecareandtreatmentofpeoplewithschizophreniainEnglandthatcouldbemademorecost-effective.Thereisrobustevidencearoundsomeinterventionswhichsuggestsastrongeconomiccaseforchange.

7
CURRENT COSTS OF SCHIZOPHRENIA
1. Estimates made from uprating cost estimates by Mangalore and Knapp (2007) to 2010/11 prices (using price indices specific to each cost area), uprating estimated number of people with schizophrenia in England to the recent estimate by NICE of 197,000 (www.nice.org.uk/usingguidance/commissioningguides/schizophrenia) and using an 18% average indirect tax and an 18% average income tax on all earnings. Figures reported here do not include the more intangible costs of the pain and suffering incurred by individuals with schizophrenia and their loved ones.
Schizophreniahasverysignificanteconomicconsequences;thecostsimpactonmanydifferentpartsofsociety,especiallyonindividualswithschizophreniaandtheirfamilies.Overall,schizophreniaisestimatedtocostEnglishsociety£11.8billionperyearandthepublicsector£7.2billion.1Thisamountstoanaverageannualcosttosocietyof£60,000andtothepublicsectorof£36,000perpersonwithschizophrenia.
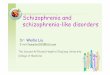
Figure 1: Annual costs of schizophrenia to society and the public sector (£,2010/11 prices, per person with schizophrenia)
60,000
50,000
40,000
30,000
20,000
10,000
0Societal
CostPublicSector
Cost
Indirecttaxforgone
Incometaxforgone
Socialsecuritypayments
Prematuremortality
Excessunemploymentofpeoplewithschizophrenia
Unpaidcare
Other
Institutionalcosts
Healthandsocialcare

8
Figure1showshowthesecostestimatesbreakdown.Somedirectcostsofschizophrenia,suchasin-patienthospitalcostsandsupportfromcommunitymentalhealthteams,arecommoncomponentsofboththecosttothepublicsectorandthecosttosociety.Othercosts,suchasunpaidcare,donotcostthepublicsectordirectlybutarestillveryrealcostsforsociety.Lostpotentialoutputduetoelevatedunemploymentratesandprematuremortalityforpeoplewithschizophreniatranslateintohugecostsforsocietyandalsotranslateintocostsforthepublicsectorviathelossoftaxrevenue.
Evidently,schizophreniaishugelyexpensivebothtothepublicpurseandsocietyatlarge.Duetothenatureoftheconditionmanyofthesecostsarenon-retrievable–notreatmentortherapywillbeabletogeteveryserviceuserintofull-timeemploymentforexample,andexpensivetreatmentsandmedicationsmayalwaysberequired.Inthisreport,however,wecontendthatthereareareasofthecurrentsystemforthecareandtreatmentofpeoplewithschizophreniainEnglandthatcouldbemademorecost-effective.Thepurposeofthereportistosummarisethemaineconomicimpactsofschizophrenia,andthentoconsiderarangeofinterventions(usingthattermbroadly)that,ifmademorewidelyavailable,couldleadtobetteroutcomesandlowercosts.Itisnotourintentiontorecommendaparticular‘package’ofidealinterventions,rathertoofferasummaryofevidenceoncostsandcost-effectivenessasaplatformfordiscussion.
ThereareanumberofimportantelementsintheoverallcostsofschizophreniasummarisedinFigure1,anditishelpfultofocusonsomeofthekeycost ‘drivers’.Infact,wecanidentifyeightkeycostdriversassociatedwithschizophrenia:areas,eventsorexperiencesthataccountfororhelptoexplainsignificantproportionsofthecostassociatedwithschizophrenia.Byconsideringeachofthesedriverswecansubsequentlyfocusoninterventionsthatmayhavethepotentialtoreducetheeconomicimpactofthesedriverswhilemaintainingorimprovingthehealthandwell-beingofindividualswithschizophreniaandtheirfamilies.
Mostoftheevidencethatwesummariseinthisreportrelatestopeoplewithschizophrenia,althoughsometimesthestudiesthatwediscusslookedatawidergroupofpeople,suchaspeoplewiththediagnosisofschizophreniaandotherpsychoticillnesses,orpeoplewithseriousorseverementalillnesses.Wehaveendeavouredtobeclearaboutthegroupsofpeoplecoveredaswediscusstheevidence.Werecognisethatthetermschizophreniaandpsychosisinclinicalservicesareusedinterchangeablybutmostresearchusestheterm‘schizophrenia’.
INPATIENT TIME
Mostindividualswithschizophreniahaveatleastoneinpatientstay,withahighprobabilityofreadmission(Allardyce&Os2010).Inpatienttimeaccountsforaverysignificantproportionofthecostsassociatedwithschizophrenia,roughly38%ofallhealth,socialcareandinstitutionalcostsassociatedwiththecondition,androughly21%ofallpublicsectorcosts.2TheaveragecostofanightinamentalhealthinpatientbedinEnglandis£321(Curtis2011).HospitalEpisodeStatistics(HESonline2011)showthatthemedianlengthofadmissionis38days,translatingintoanestimatedcostof£12,198peradmission.3Typically,compulsory(orformal)admissionsundertheMentalHealthActarelongerthanthis,andthustranslateintohighercoststhanvoluntaryadmissions.Duetotheveryhighcostsassociatedwithinpatientservices,interventionsthatreducetheprobabilityofadmissionorreducetheexpectedlengthofstaycantranslateintoverysignificantcostsavings,althoughthisshouldnotbeattheexpenseofpoorerhealth,qualityoflifeorotheroutcomes.
Formanypeoplewithschizophrenia,aninpatientadmissionisanecessaryandperhapsimportantturningpointinthecourseoftheirillness,butinotherinstancesadmissioncouldbeavoidedifmoreandbetterinterventionswereavailableoutsidetheinpatientsetting.Likewise,intermsofreducingthelengthofadmission,arecentCochranereview(althoughtheincludedstudiesweredated)foundnoevidenceofadverseoutcomesfromshorter
2. Calculated from Mangalore and Knapp (2007).3. Mean length of stay is 130 days. Data are heavily skewed due to a small proportion of individuals who are admitted to
long-stay units.

9
hospitalstaysandsomeevidenceofbenefits(Alwanetal.2010).RecentworkbytheAuditCommission(2010)foundlargevariationsininpatientusebetweendifferentPrimaryCareTrusts;specificallyitfoundafive-foldvariationinadmissionratesforpsychosis,12-foldvariationinpsychosisbeddaysanda14-foldvariationinlengthofstay.4Thereportestimatedthatifalltrustsachievedthemedianrateofbeddaysthenthiswouldreducetotalbeduseby15%,resultinginaneconomicbenefitof£221million5tomentalhealthservices.
DISRUPTED / LOSS OF EMPLOYMENT
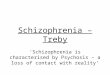
Whilsttheemploymentrateforalladultsaged16-64yearsinEnglandiscurrently71%6,recentestimatesplacetheemploymentrateforpeoplewithschizophreniaasbetween5and15%7(Marwaha&Johnson2004).EvidencesummarisedinFigure2suggeststhattheemploymentrateforpeoplewithschizophreniahasfallensignificantlyoverthepasthalfcentury–atimeframeoverwhichtheemploymentrateforthepopulationasawholehasrisen.ThereisanoticeablelackofmorerecentstatisticsreportingtheemploymentrateforpeoplewithschizophreniaintheUK.
4. All rates weighted for need.5. Updated to reflect current prices using the Pay and Prices Index in Curtis (2011).6. Source: www.ons.gov.uk/ons/about-ons/who-we-are/services/unpublished-data/social-survey-data/aps/index.html7. Estimates between 1990 and 2004.
Figure 2: Reported employment rates in 15 studies of people with schizophrenia in the UK; circle areas represent sample size. Data taken from Marwaha and Johnson (2004)
70
60
50
40
30
20
10
0
1950 1960 1970 1980 1990 2000 2010

10
Theexceptionallylowemploymentrateforpeoplewithschizophreniarepresentsahugelossofproductivecapacity.Assuminganemploymentrateof7%forpeoplewithschizophrenia(theweightedaverageofallstudiessince1995)andanemploymentrateof71%inthegeneralpopulation,thenschizophreniacauses–orisassociatedwith–a64-percentagepointdecreaseintheprobabilityofbeingcompetitivelyemployed.Usinganestimateofgrossannualmedianearningsof£21,3008thisisequivalenttoanexpectedlossofproductivecapacityof£13,600peryearperindividual(2011/12pricelevels).Theuseofmeangrossannualearnings9(£26,900)givesanestimatedlossofproductivecapacityof£17,200perindividual,whichcanbescaleduptogiveanexpectedlosstotheEnglisheconomyof£3.4billioneachyear.
Thelowemploymentratehasknock-oneffectsonthefinancesofthepublicsectorthroughlossesintaxrevenueandpaymentsofsocialsecuritybenefits.Assumingan18%averagedirecttaxrate(incometax)andan18%averageindirecttaxrate(VAT),10thistranslatesinto£715millionoftaxrevenueforgone(or£5500perserviceuser)perannum.
Lowratesofemploymentalsotranslateintohigherdependenceonsocialsecuritybenefits.UpdatingtheevidencepresentedbyMangaloreandKnapp(2007)tocurrentpricesgivesanestimatedreceiptofbenefitsof£5500perserviceuserperyear(assumingthat77.6%ofeconomicallyinactivepeoplewithschizophreniaareinreceiptofbenefits).If,intheabsenceofotherinformation,weassumethatthesameproportionofthegeneralpopulationwhoareeconomicallyinactiveareinreceiptofbenefitstothesamevalue,wefindanaveragebenefitreceiptforthegeneralpopulationofaround£1900.(Thisislikelytobeanover-estimatesincemostmembersofthegeneralpopulationwouldnotbeentitledtoincapacitybenefit.)Theseestimatessuggestanexcessof£3600ispaidinbenefitsperserviceuserperyear,oratotalof£470millionperyear.
Ofcoursethecounterfactualusedintheabovescenarioisunrealistic–eventhemosteffectiveinterventionsinschizophreniadonotproduceemploymentratesandwageratesonaparwiththeaverageforthegeneralpopulation–sotheabovesuggestedlossesintermsoftaxrevenueandbenefitscouldneverbefullyrecovered.However,thereareverysignificantsavingsthatcouldbemadeiftheemploymentrateforpeoplewithschizophreniacouldbeimproved.Theeconomicgainstosocietyresultingfromacautiousscenariowhere50%ofpeoplewithschizophreniawereemployedatanaverageof20hoursaweekattheNationalMinimumWagewouldbeintheorderof£350million,includingasavingofaround£120milliontothepublicfinances.
Thereisnoevidencetosuggestthatincreasingemploymentratesforpeoplewithschizophrenialeadstodetrimentaloutcomes.Indeedthereisevidencethattheconverseistrue,thatsuccessfulgainofcompetitiveemploymentbyindividualswhowantit(andthevastmajoritydo)leadstoimprovedclinicaloutcomes(Kilianetal.2012).Thisimprovementinclinicalstatecangenerateknock-onsavingselsewhere,forexampleinhealthservicecosts.
DISRUPTED EDUCATION
Schizophreniamostoftendevelopsinlateadolescenceorearlyadulthood–yearsthatarekeyfordevelopingskillsandknowledgethatwillprovidebenefitandincreaseearningspotentialthroughoutlife.Thedebilitatingnatureofthecondition,particularlyinthefirstfewyearsafteronset,oftenforcespeoplewithschizophreniatoleaveeducationortrainingearlierthantheywouldotherwisehavedone.Surprisinglyfewstudieshaveaddressedthecostsofmissededucationalandtrainingopportunitiesduetothecondition.
ArecentreportforthedepartmentofBusiness,InnovationandSkillsfoundthatthemarginalreturntoanundergraduatedegreewas27.4%(whencomparedtohavingtwoormoreGCEAlevels)(LondonEconomics2011b).
8. Taken from the annual survey of hours and earnings (ASHE), 2011. Source: www.ons.gov.uk/ons/publications/re-reference-tables.html?edition=tcm%3A77-235202
9. Taken from the annual survey of hours and earnings (ASHE), 2011. Source: www.ons.gov.uk/ons/publications/re-reference-tables.html?edition=tcm%3A77-235202
10. The use of an indirect tax rate in this estimation accounts for the tax revenue forgone due to reduced consumer spending as a result of the fall in earnings. Rate taken from Adam and colleagues (2012).

11
Thistranslatedintoalifetimenetbenefittotheindividualof£108,000(currentprices,discountedat3.5%perannum)andtotheexchequerof£89,000.Thus,foreveryyoungpersonwhohastoforgoauniversityeducationbecauseofschizophreniatheresultwouldbealostnetbenefitof£197,000tosociety.
Likewise,formanyyoungpeoplethedevelopmentofschizophreniameanstheymissvocationaleducationandtrainingopportunities.Forexample,ifayoungpersonenrolledforaBTEClevel2qualificationcouldnotcompletethisqualificationbecauseofdevelopingschizophrenia,thisisestimatedtoresultinforgoinga12%wagegain,resultinginaforgonenetbenefittosocietyofbetween£54,000and£104,000overalifetime(LondonEconomics2011a).
HOMELESSNESS
Arecentnaturalisticstudyfoundthat33%ofasampleofpeoplewithschizophreniadrawnfromLondonandLeicesterhadbeenhomelessatsomestageand13%hadbeenroofless.Thiscomparedtofiguresof9%and6%forFrance,and8%and3%forGermany(Bebbingtonetal.2005).WhilstthesefiguresmaynotberepresentativeoftheUKmorewidely,sincelargeconurbationssuchasLondonandLeicesterwillhavehigherratesofhomelessnessashomelesspeoplefromotherareastendtodrifttolargecities,theydosuggestmajorfailingsinthecurrentsystemsthatleavelargeproportionsofpeoplewithschizophreniahighlyvulnerabletoviolence,theft,substancemisuseandfurtherdeterioratingmentalandphysicalhealth.
Homelessnessrepresentsahugewasteofpotentialinoursociety.Unemploymentisbothacauseandconsequenceofhomelessness.Thehomelessarefivetimeslesslikelytobeemployedthanthepopulationasawhole(CrisisUK2012)andbeinghomelesscreatesverysignificantbarrierstosubsequentlyre-enteringemployment.Formanypeople,beinghomelessmeanshavingnofixedaddressformailingsandnotbeingabletoopenamainstreambankaccount,makingithardertofindwork(Stansbury&Phakey2011).
Homelessnessalsohassignificantdirectcoststotheexchequer.Estimatesofthe(gross)annualcostsofhomelessnesstothepublicsectorliebetween£24,000and£30,000perhomelessperson(DepartmentforCommunitiesandLocalGovernment2012).Itisnoteasytoattributecostsspecificallytohomelessnessasmanycostlyphenomena,suchassubstancemisuse,criminalbehaviourandpoorhealth,arebothcausesandresultsofhomelessness.However,itisclearthathomelessnessisnotonlyanappallingexperienceforanindividual,butthatitalsohaswide-rangingeconomicconsequencesforthemandsociety.
PHYSICAL HEALTH PROBLEMS
Itisnowwidelyrecognisedthatschizophreniaincreasestheprobabilityofpoorphysicalhealth(Leucht,etal.,2007).Asaresult,thereisasignificantmortalitygapbetweenpeoplewithschizophreniaandthegeneralpopulation:arecentsystematicreviewestimatedthattheage-adjustedall-causemortalityrateamongstpeoplewithschizophreniawas2.58timeshigherthanforthegeneralpopulation(Sahaetal.2007).Aproportionofthiselevatedmortalityrateisduetoanincreasedriskofsuicide,butindividualswithschizophreniawerefoundtohaveincreasedmortalityratesinmostmajor‘causeofdeath’categories.
Schizophreniaincreasesriskfactorsformanyphysicalhealthproblems.Analysisoftheclinicalrecordsof1.7millionpeoplefoundthat61%ofpeoplewithschizophreniasmokedcomparedto33%ofpeoplewithoutschizophrenia,andthat33%ofpeoplewithschizophreniawereobesecomparedto21%ofpeoplewithout(Hippisley-Cox&Pringle2005).Manyantipsychoticmedications(particularlysecondgenerationones)areassociatedwithweightgain(Connolly2005).Combined,thesefactorsmeanthatpeoplewithschizophreniafaceahigherriskofdevelopingmanyphysicalhealthproblems.
Untilfairlyrecentlythephysicalhealthofpeoplewithschizophreniahasnotbeenapolicyprioritydespitethisverysubstantialphysicalhealthinequality:individualswithschizophreniaaresignificantlylesslikelytohavehadarecentcervicalsmear,arecentbloodpressurerecording,arecentcholesteroltestorbeonaspirinasaprophylaxisforstroke

12
(Hippisley-Cox&Pringle2005).Therearealsoeconomicargumentstobemade:physicalhealthproblemstranslateintoadditionalhealthserviceexpenditure,lostproductivityandincreasedrelianceonsocialcareservices,resultinginsignificanteconomiclosses.
SUBSTANCE MISUSE
Quiteahighproportionofindividualswithschizophreniaaresubstancemisusers.DatafromtheEuropeanSchizophreniaCohortidentifiedanoverallsubstancedependencein42%ofparticipantsinLondonand28.3%inLeicester,placingthetwoUKcitiesfirstandthirdoutofeightEuropeancitieslookedatinthatstudy(Carràetal.2012).Thatstudyalsoestimatedaprevalencerateforalcoholmisuseof26.1%comparedto11.9%inthegeneralpopulation,andaprevalencerateforthemisuseofallothersubstancesof17.8%comparedto7%forthegeneralpopulation.Sincethedataaretakenfromurbanareas,figuresmaybesomewhathigherthanforthecountryasawhole(Carràetal.2009),butitisclearthatthereisastrongassociationbetweenschizophreniaandsubstancemisuse.
Inadditiontothepersonalcoststhatsubstanceabusecancause,therearealsowidereconomicconsequences.Thereisevidencethatindividualswithadualdiagnosisofschizophreniaandsubstancemisuseincurhigherserviceusecosts.Turkingtonandcolleagues(2009)foundthatpersistentsubstancemisuseincreasedtheprobabilityofrelapse,suggestingadditionaladmissionsandservicecosts.McCroneandcolleagues(2000)foundthatinasamplefromSouthLondon,‘core’costs(mentalhealthservicecosts,emergencycliniccostsanddaycarecosts)overasix-monthperiodwere£1913higherforthedualdiagnosisgroupthanforotherpatients(95%CI:£309to£3865),non-accommodationcostswere£1910higher(95%CI:£281to£3820)andtotalcosts(includingsupportedaccommodation)were£1469higher(95%CI:-£954to£4292).Whilstthereareproblems
ofself-selectionintothesubstancemisusestate–perhapsindividualswithmoreseverepsychosis,whowouldincurmorecostsanyway,aremorelikelytobesubstancesmisusersandthustheabovecostsmaynotrepresentthetruemarginaldifferenceincostsduetosubstancemisuse–thereisstrongevidencethatsubstancemisuseisassociatedwithhigherservicecostsinschizophreniacare.
Anothercostthatmaybeassociatedwithsubstanceabuseforpeoplewithschizophreniaisbecauseofcrime.InalargelongitudinalstudyinSweden(80025people,ofwhich8003hadadiagnosisofschizophrenia)Fazelandcolleagues(2009)showedthattheelevatedriskofsomeonewithschizophreniacommittingaviolentcrimecanbealmostentirelyaccountedforbyhighlevelsofsubstanceabuseinthisgroup.
Itwasfoundthatindividualswithschizophreniaandsubstance-useco-morbidityhadariskofcommittingaviolentcrimethatwas4.4timesgreater(95%CI:3.9to5.0)thanforthegeneralpopulation,whereasindividualswhohadschizophreniabutdidnotabusesubstanceshadanelevatedriskofjust1.2greater(95%CI:1.1to1.4).Similarfindingswerefoundinarecentsystematicreview(Fazeletal.2009).GiventheHomeOffice(2005)estimatesthatviolentcrimecauseseconomicandsocialcoststotalling£44.6billion11inEnglandandWaleseachyear,elevatedviolentcrimeduetothisco-morbiditybetweenschizophreniaandsubstancemisuseisclearlyverycostly.
Othercostsmayalsobeincurredasaresultofadualdiagnosiswithsubstancemisuse.Itislikelythatsubstancemisusereducesemploymentopportunities,resultinginwastedeconomicpotentialandlossestotheexchequerintaxrevenueforgone.
11. Uprated to reflect current prices using the GDP deflator (ONS).

13
CONTACT WITH THE CRIMINAL JUSTICE SYSTEM
Peoplewithschizophreniaareover-representedinthecriminaljusticesystem.Themostrecent(althoughnowquitedated)estimatesarethataround8%oftheprisonpopulationhaspsychosis,with2%qualifyingforaformaldiagnosisofschizophrenia(Singletonetal.1998).Thiscomparestofiguresofbetween0.2%to0.5%forthegeneralhouseholdpopulation(Singletonetal.2000;Sahaetal.2005;Mangaloreetal.2007).
Questionsareincreasinglybeingaskedabouttheappropriatenessofprisonsentencesformanyofthesepeople–frombothmoralandeffectivenessperspectives.Itisalsoclearthatprisonmaybeaneconomicallyinefficientinterventionformanywithschizophreniaorothermentalhealthproblems.Thecostofaprisonplaceforoneyearisestimatedtobe£40,000(MinistryofJustice2011b)andyetitisremarkablyineffectiveatpreventingreoffending;resultsfromtheSurveyingPrisonerCrimeReductionsurvey12foundthat54.2%ofprisonerswhohadbeentreatedforamentalhealth/emotionalproblemintheyearbeforecustodyhadbeenreconvictedwithinoneyearofrelease(at51.7%thereconvictionratewasalsoveryhighforprisonerswithoutsuchproblems).
ManypeoplewithschizophreniawhohavecommittedcrimesendupinsecurecareprovidedorfundedbytheNHS.Theseunitsaredifferentfromprisonsbecauseoftheiremphasisoncareandtreatmentasopposedtopunishment.Thereareanumberofroutesbywhichanindividualcanbeadmittedtosecurecare:theycanbereferredfromprison,onarestrictedorunrestrictedhospitalorderfromcourtasanalternativetoprison,ordirectlyfromcommunitytreatment.Securementalhealthbedsaredividedintohigh,mediumandlowsecure,aswellasspecialisedmediumsecureunitsforwomen.Nearly97%ofpeopletransferredonrestrictionordersfromprisongointohighormediumsecurebeds,whereaslowsecurebedsaremainlyusedforpeopledetaineddirectlyfromthecommunityundertheMentalHealthAct,orpeople‘stepped-down’frommoresecurebeds(Rutherford&Duggan2007).
Secureunitsrepresentaveryexpensiveelementofmentalhealthcare:secureandhigh-dependencyservicesaccountedfor19%ofdirectinvestmentinmentalhealthservicesin2010/11,withinvestmenttotallingover£1billion(MentalHealthStrategies2011).Inadditiontohighunitcosts,totalcostsaresohighpartlybecausestaysaretypicallyverylong,with27%ofpeopledetainedremaininginforensicservicesforover10years(Rutherford&Duggan2007).
FAMILY IMPACT
Manyrelativesandotherunpaidcarersofpeoplewithschizophreniawillgiveupemploymentortaketimeoffworkinordertoprovidecareandsupport.UsingresultsfromtheUK-SCAPstudy,MangaloreandKnapp(2007)estimatedthat4.8%ofcarershadterminatedemploymentand15.5%tookameanof12.5daysoffworkperyearspecificallyasaresultofbeingacarer.Thistranslatesintoameanannualeconomiclossof£517(2011/12prices)perindividualwithschizophrenialivinginthehouseholdpopulation.
Inadditiontothelossofproductivityasaresultofbeingacarer,itisalsopossibletoputaneconomicvalueontheunpaidcarethattheseindividuals(whoareusuallyfamilymembers)providetopeoplewithschizophrenia,ontheassumptionthatiftheydidnotprovidesuchcaresomeoneelsewouldhaveto.IfsuchcareandsupportisvaluedathowmuchitwouldcosttheNHStoprovidesimilarcare(thesalaryofanassistantnurseornursingauxiliary)thenbasedontheassumptionthattheunpaidcarerprovidesameanof5.6hourssupportperday,thiscomestoanaverageof£34,000perpersonwithschizophreniabeinglookedafterbyafamilyorothercarer.Roughly31%ofpeoplewithschizophreniaarelivinginprivatehouseholds(Mangalore&Knapp2007b),sothiscouldtranslateintoanaggregatecosttosocietyofasmuchas£1.24billionperyear.
12. Source: www.justice.gov.uk/downloads/statistics/mojstats/spcr-full-tables-paper-5-2-prisoners-backgrounds-reconviction-a.xls

14
Havingdiscussedsomeofthekeycostdriversinrelationtoschizophrenia,wenowmoveontolookattheeconomicconsequencesofavarietyofinterventions.TheextensiveevidencecollectedbytheSchizophreniaCommissionfromawiderangeofpeoplewithexpertiseaboutand/orexperienceofpsychosisguidesthescopeandnatureofinterventionsdiscussedhere.Ingatheringandcollatingeconomicevidenceoneachoftheseinterventionswehavetriedtobeasbalancedandfairaspossible.
differentcircumstances.Interventionsarenotindependentfromoneanotherinthattheoutcomesofonemaybepositivelyornegativelyimpactedbyotherinterventionsthatanindividualisreceivingorhaspreviouslyreceived.Forexample,itwouldperhapsbeunrealistictoassumethesamereductionininpatientuseasaresultofaspecifictalkingtherapy,suchascognitivebehaviouraltherapy(CBT),whentheindividualalreadyreceivesothertypesofpsychologically-informedinterventionsaswhenhe/shereceivesCBTalone.Becauseofthisinterdependence,thecostestimatesreportedhereareincertainlynotadditive.WediscussthisfurtherinSection3.
Anotherpointtobearinmindistheoftenelusivenatureofthesocalled‘standardcare’or‘treatmentasusual’againstwhichinterventionsaretypicallycompared.Oftentrialsgivelimitedinformationaboutthenatureofsuchstandardservicestowhichtheyarecomparingtheinterventioninquestion,yetsincestandardpracticesofcarevarytremendouslyacrossthecountry(letalonebetweencountriesandovertime),thisleadstoseriousquestionsaboutextrapolatingeconomicevidencefromonecontexttoanother.Ifaparticularinterventionsaved£Xperpatientinonelocalitywhencomparedtostandardcareinthatarea,itis
EVALUATING VARIOUS INTERVENTIONS
However,duetotimeconstraints,asystematicreviewineachcasewascertainlynotpossible.Instead,asastartingpointforeachintervention,wecontactedresearchersintheareatoidentifythemostsignificantexistingeconomicevidence,includingextantreviews.Thisinformationwassupplementedwithextensive,albeitnotsystematic,literaturesearchingforeachinterventioninturn.
Wheretheeconomicevidenceforinterventionswasconsideredtobestrongwehaveattemptedtodrawconclusionsfortheeconomicimplicationsoftheseinterventionsonthreedifferentlevels–fortheNHS,forthepublicpursemoregenerally,andforsocietyasawhole.Forthoseinterventionswheretheeconomicevidenceisnotstrongenoughtodrawfirmconclusions,keyevidencehasbeensummarisedandareasforfutureworkhighlighted.
Attentionmustbedrawntothefactthattheseinterventionsareneithermutuallyexclusivenorindependent.Schizophreniaisacomplexconditionandmostindividualswiththeconditioncanbenefitfromacombinationofinterventions,andofcourse,theyandtheirfamilieswouldhavepreferencesaboutwhichinterventionsareappropriatein

15
notnecessarilythecasethatthesamesavingof£Xwillbeobtainedinanotherlocalityifthestandardcarepracticedinthisareaisdifferent.Havingsaidthat,withoutextensiveinformationabouttheroutinepracticeofdifferentmentalhealthservicesthereisoftenlittleoptionbuttoassumeasimilarstandardcareandthusthatanycostsorbenefitswillbegeneralisable.
Someoftheinterventionsdiscussedbelow,suchasEarlyInterventionandCrisisTeamsarealreadywidelyinplace,atleastinname;andfortheseouranalysisattemptstoevaluatetheeconomicevidenceformaintainingthem.Otherinterventionsdiscussedhere,suchasIndividualPlacementandSupport,HomelessnessInterventionsandPeerSupportareasyetnotwidelyavailable;hereweattempttoevaluatetheevidenceformakingsuchinterventionsmore widely available.
Allcostsinthisreporthavebeenupratedforinflationto2010/11pricelevelsusinganappropriatepriceindex.Allfuturecostimplicationshavebeendiscountedbacktothepresentatarateof3.5%perannum.
EARLY INTERVENTION
Someearlyinterventionservices(EIS)inpsychosisaimatearlydetectionofpeoplewithprodromalsymptomsofpsychosis(orthosewhosepsychosishasnotalreadybeenadequatelydetectedandtreated),butmostearlyinterventionteamsareworkingwithpeoplewhoseillnesshasbeendiagnosed.Treatmentintheearlyinterventionstageideallyinvolvesacombinationof‘pharmacological,psychological,social,occupationalandeducationalinterventions’(NationalInstituteforHealthandClinicalExcellence2009).Therationaleforinterveningearlyinpsychosisisbasedonevidencethatsuggestsanassociationbetweenthedurationofuntreatedpsychosisandoverallprognosis(Marshalletal.2005).
EarlyinterventionserviceswereformallyintroducedintotheNHSin2001/2002asoutlinedinThe Mental Health Policy Implementation Guide(DepartmentofHealth2001).Sincethen,earlyinterventionteamshavebeenintroducedquitewidelyacrossEngland(Shiers&Smith2010)althoughthereremaininequalitiesinaccess(IRIS2011).
ClinicalevidencesuggestsEarlyInterventioninPsychosiscanhavepositiveeffects.Arecentsystematicreviewandmeta-analysissuggestedthatspecialisedFirstEpisodePsychosisprogrammescansignificantlyreducetheriskofrelapsewhencomparedtousualtreatment(Alvarez-Jiménezetal.2011).ArecentCochranereviewwaslesspositive,findingfewsignificantresultsinfavourofEIS(Marshall&Rathbone2011).However,theusefulnessoftheCochranemethodologyinevaluatingservicemodelssuchasEarlyInterventionhasbeenquestioned.McGorry(2012)claimsthatmanywell-designedstudiesevaluatingtheeffectivenessofEISwereexcludedfromtheCochranereview.HedisputestherelevanceofmanyoftheCochranefindingssince‘thereviewfocusedlargelyontrialscomparingthe“componentinterventions”ofEIPservices.…SuchinterventionsweretypicallystudiedagainstthebackdropoftherangeofcareprovidedwithinstreamedEIPservices.Itisnotsurprisingthatsomeoftheseindividualtrialswere“ineffective”giventhatthecontrolgroupsinthesetrialsweretherecipientsofanalreadycomprehensivemodelofcare.’
Inadditiontopatientoutcomestherehasbeenattentiongiventopotentialcostsavingsthattheuseofearlyinterventionservicesmayoffer–inboththeimmediateandlongerterm.Thefirststudiesthataimedtotacklethisissuewererelativelynarrowinscope–focusinglargelyondirectcoststomentalhealthservices.Morerecently,however,workhasbeendonetotakeamorecomprehensivelookattheeconomicconsequencesofEarlyInterventionservices.RecentstudieshaveconsideredtheimplicationsofEISformoreofthecostdriversdiscussedinSection1,includingcriminaljusticecostsandlostemploymentcosts(McCroneetal.2010).
InarecenteconomicevaluationofEIS,McCroneandcolleagues(2010)usedadecisionmodellingapproach,derivingprobabilitiesfromtheliterature,toestimatethecostconsequencesofEarlyInterventionServices.TheresultswerestronglyinfavourofEIS.ThisreportupdatesthecostsreportedbyMcCroneetal.(2010)sotheyreflectcurrentcostsandprices,andalsoaddsinanexpectedincreaseintaxrevenue.BelowweoutlinethekeymechanismsthroughwhichEarlyInterventionServicesmayleadtocostsavings.

16
Mental Health Service UseSinceEarlyInterventionServiceshavebeenshowntohaveclinicalbenefitsitisperhapsunsurprisingthattheirintroductionwouldreduceserviceuse,inparticularhigh-costinpatienttime.Indeed,usingdatafromtheLambethEarlyOnset(LEO)team,routinedatafromWorcestershireandNorthumberlandEIServicesandtheHealthcareCommissiontheauthors(McCrone,etal.2009a)estimatedthatEarlyInterventionServicesreducetheprobabilityofaformaladmission(compulsoryadmissionundertheMentalHealthAct)from44%to23%inthefirst2monthsofpsychosisandfrom13%to6%ineach2-monthperiodthereafter.Thistranslatesintoverysizeablecostsavingsforthementalhealthservices:itisestimatedthat,at2010/11prices,theintroductionofanEarlyInterventionServicesaves£5,493perserviceuserinthefirstyearofpsychosisand£15,742duringthefirstthreeyears(costsdiscountedat3.5%peryear).
Suicide and Homicide CostsEarlyInterventionServiceshavebeenshowntobeeffectiveinreducingtheriskofbothsuicideandhomicide.Associatedcostsavingsfromthereductionofsuiciderisk(throughcoststotheNHSandthelostproductivityofthedeceased)areestimatedat£481inthefirstyearofpsychosis.Theassociatedcostsavingsfromthereductioninhomicideriskaresmall(just£28overthreeyears)becauseoftheverylowstartingprobabilitythataserviceuserwillcommithomicide,yetEarlyInterventionServicesdosignificantlyreducethisrisk.However,weneedtobecautiouswiththesefiguresonsuicideand(especially)onhomicidegiventhelimiteddatathatwereavailableasabasisfortheeconomiccalculation.
EarningsEarlyInterventionServiceshaveapositiveimpactontheretentionandgainofcompetitiveemployment.McCroneetal.(2010)estimatethat12%ofstandardcarepatientswillbeinemployment,comparedto35%ofpeoplesupportedbyEIS.Ifahumancapitalapproachisassumed,valuingemploymentattheminimumwagerate,theresultwouldbeagaininearningsof£4299evenwhenassumingthatnoemploymentoccursinthefirstyearforeithergroup.
Thisincreaseinemploymentrate,whenviewedfromasocietalperspective,increasesproductionintheeconomyasawholeand,whenviewedfromapublicsectorperspective,increasestaxrevenue.Inthisreportitisassumedthattheonlynetbenefitintermsoftaxrevenuecomesfromthemeanindirecttaxrateof18%(Adametal.2012);sincethesizeoftheearningsweareconsideringisrelativelymodest,weassumenoincometaxispaid,whichmakestheestimatesofcostsavingstothepublicsectorconservative.
Net Cost SavingsWhenwesumtheseindividualcoststogethertofindthenetsavingsaccruedbytheintroductionofEISwefindthefollowingresults:
� TheintroductionofEarlyInterventionServicesisestimatedtosavetheNationalHealthService£5536perserviceuserinthefirstyearofpsychosis.Thisrisestoatotalof£15862inthefirstthreeyears.
� Intermsofthepublicpurseviewedasawhole,theintroductionofEISisestimatedtohaveanetbenefitof£5545inthefirstyearofpsychosis,risingto£16663overthefirstthreeyears.ThesefiguresincludecostsaccruedtotheNHS,criminaljusticesystemandextrataxrevenuegained.
� TakingasocietalviewofthenetbenefitsofEISbyincludingallincreasedproductionthatoccursasaresult(notonlythatwhichissubsequentlycollectedbygovernmentintaxes)givesafigureof£6015savedinthefirstyearofpsychosisand£21512savedoverthethree-yearperiod.
Thereareothercoststhathavenotbeenintegratedintothismodelthatwould,itseemslikely,increasethepotentialsavingsofEIservices.Oneisthecostincurredbyfamiliesandcarersthroughreducingtheirownemploymentandprovidingunpaidcareandsupport.ItisexpectedthatthroughtheclinicalbenefitsassociatedwithEI,thiscostincurredbyfamilieswouldbereduced.

17
CaveatsTheaboveestimatesofcostsavingsfromimplementationofEISareobtainedusingonespecificsetofmodelparameters:aspecificsetofprobabilitiesofadmissionunderstandardcareandEIS,andaspecificsetofcostsofadmissionandcommunitycare.EstimatedcostsavingsfromtheimplementationofEISwillvaryfromlocalitytolocalitydependingonprioradmissionrates,thefidelityofEIStoevidence-basedmodels,thenatureandqualityof‘standardcare’servicesandthequalityandcostofinpatientcare.TheabovemodelislargelyestimatedusingparameterstakenfromLondon-basedstudies,soresultsmaynotbeimmediatelytransferabletootherareasofthecountry,whereservicemodelsandpopulationscouldbedifferent.However,EISinverydifferentpartsofthecountryhavebeensuccessfulinreducingadmissions.Forexample,followingtheimplementationoftheNorth
EastDerbyshireEarlyInterventionservice,thepercentageofpeoplewithschizophreniawithafirstepisodeofpsychosis(whocameintocontactwithregularservicesandthespecialistEISrespectively)thatwereadmittedtohospitalwithinthefirstyearfellfrom62%tolessthan31%(Rowlands2012;Phillipsonetal.2012).13
WhenconsideringtheeconomicconsequencesofEarlyInterventionitisalsoimportanttobearinmindthatschizophreniaisalifelongconditionandthebenefitsofthespecialisedmodelthatEISprovidesmaynotbesustainedaftertheserviceuserisnolongereligiblefortheservice.Intwomajorstudies,significantbenefitsofEISwerenolongerseenatafive-yearfollow-up(Gafooretal.2010;Bertelsenetal.2008).This,though,maybebecauseoftheservicesthatrecipientsofEIweredischargedtoratherthantodeficienciesinEIitself.
13. It must be noted that the eligible populations for the two services are different, mainly in that NE Derbyshire EIS only deals with people under the age of 35. Thus, whilst this figure is indicative of the success of EIS in bringing about fewer inpatient admissions it must not be interpreted as a precise estimate of the impact of the service.
Figure 3: Cost savings accrued through the introduction of Early Intervention Services (2010/2011 £)
8,000
7,000
6,000
5,000
4,000
3,000
2,000
1,000
0
HealthServiceSavings
PublicSectorSavings
SocietalBenefit
Net
Sav
ing
/B
enefi
t(2
011
/12
£)
Year
1 2 3

18
INDIVIDUAL PLACEMENT AND SUPPORT SCHEMES
Mostpeoplewithschizophreniaandotherseverementalhealthissueswanttowork(Grove1999;Mueseretal.2001;Marwaha2005).However,onlybetween5and15%areactuallyinemployment,representingahugewasteofpotentialaswellasdenyingpeopleopportunitiesforsocialinclusion,meaningfuldaytimeactivityandasenseofpersonalidentityandachievement.IndividualPlacementandSupport(IPS)isatypeofsupportedemploymentaimedathelpingthosewithseverementalhealthproblemstogainpaidcompetitiveemployment.IPSservicesareverydifferenttothekindsofvocationalrehabilitationservicesconventionallyavailable(andtheservicesthatstillexistinmanypartsofEngland)inthatIPSservicesaimtoplacepeoplewithschizophreniaincompetitiveemploymentassoonaspossibleandthenprovideadditionalsupportandtraining.Incontrast,standardvocationalschemeslargelytaketheapproachthataconsiderableamountoftrainingisneededbeforepeoplewithschizophreniaarereadytobegincompetitiveemployment.
Suchtrainingpriortoobtainingcompetitiveemploymentishighlyexpensiveandhasoftenbeensomewhatineffectiveinhelpingpeoplewithschizophreniagaincompetitiveemployment(SainsburyCentreforMentalHealth2009a;Crowtheretal.2010).ThereisnowasubstantialbodyofevidencefromacrosstheworldthatIPSissignificantlymoreeffectiveathelpingpeoplewithschizophreniatogaincompetitiveemploymentthanstandardvocationalservices(Crowtheretal.2010)
ThedetailedcharacteristicsofeffectiveIPSschemesarereportedelsewhere(Beckeretal.2008).Belowarelistedthekeyconceptsofhigh-fidelityIPSschemes(copiedfromtheSainsburyCentreforMentalHealth’sreport(2009):
� Competitiveemploymentistheprimarygoal
� Everyonewhowantsitiseligibleforemploymentsupport
� Jobsearchisconsistentwithindividualpreferences
� Jobsearchisrapid:beginningwithinonemonth
� Employmentspecialistsandclinicalteamsworkandarelocatedtogether
� Supportistime-unlimitedandisindividualisedtoboththeemployedandtheemployee
� Welfarebenefitscounsellingsupportsthepersonthroughthetransitionfrombenefitstowork
PerhapsthemostobviouspublicsectorcostsavingthatwemightexpecttoaccompanytheimplementationofIPSservicesistheadditionaltaxrevenuereceivedandthesocialsecuritybenefitpaymentssaved.However,moreimportantislikelytobethereductioninservicecostsresultingfromtheimprovementinmentalhealththatcompetitiveemployment(ortheactivesearchforit)canbring.IPSserviceshaveconsistentlybeenshowntohaveverypositiveoutcomesintermsofclinicalmeasures.Meta-analysishasshownthatIPSschemessignificantlyimprovesymptomsofthoughtdisturbance(p=0.069),anergia(p=0.094)anddepression(p=0.022)andimprovetotalsymptoms(p=0.009)14(Campbelletal.2011).
InadditiontothebetterdocumentedshortertermeffectsofIPSservicesonmentalwellbeingthereisalsoemergingevidencethatthereareverysignificantlong-termbenefitsassociatedwiththegainofstablecompetitiveemploymentwhichcorrespondtosignificanteconomicsavings(SainsburyCentreforMentalHealth2009).
MuchoftheevidenceontheeconomicconsequencesofIPSschemesissomewhatlimited,withmanystudiesfocusingprimarilyonsavingsintermsofincreasedearningsandnotconsideringbroadercostconsequences.
14. All symptoms measured using the Brief Psychiatric Rating Scale (BPRS)

19
Mental Health Service UseThemostrecentlypublishedeconomicevaluationofIPSwasbasedonarandomisedcontrolledtrialcarriedoutinsixEuropeancities;thisisEQOLISEstudy(Burnsetal.2007;Knappetal.2012).Thisstudyrandomised312participants(around80%hadschizophrenia,othershadbipolarorotherseverementalhealthproblems)toeitherIPSservicesorstandardvocationalservicesandfollowedthemfor18months.InaccordancewithotherstudiesofIPS,largelyoriginatingfromtheUSA,IPSprovedmuchmoreeffectivethanstandardvocationalservices,bothintermsofgainingcompetitiveemploymentandintermsofclinicaloutcomes(Burnsetal.2007;Burnsetal.2009;Kilianetal.2012)
TheeconomicanalysisoftheEQOLISEstudyshowedencouragingresultsforIPSintermsofserviceuseandassociatedcosts(Knappetal.2012).ItwasfoundthatIPSgeneratedsignificantsavingsininpatientcosts,asavingof£4,400overthe18-monthfollow-upperiod,althoughmostofthissavingoccurredinthefirstsixmonths.Effectsonotherareasofmentalhealthservicecostsweresmaller:IPSwasfoundtoincreaseoutpatientserviceand
communityservicecostsbyatotalofaround£1,000overthe18months,whilsteffectsonotherareasweremixed.Totalmentalhealthservicecosts(excludinginterventioncosts)were£4,000lowerfortheIPSgroupcomparedtothevocationalservicesgroupoverthe18-monthperiod.
EarningsEarningsforIPSandstandardcarewereestimatedfromtheEQOLISEstudyusingahumancapitalapproach.DatafromtheEQOLISEstudyrevealthathoursworkedincreasedoverthe18-monthperiodforboththeIPSandthecomparisongroups,butIPSparticipantsworkedmoreineachandeveryperiodwiththedifferencebetweenthegroupsincreasing(seeFigure4).Reassuringly,theestimatedhoursworkedfromtheEQOLISEstudywereverysimilartothoseestimatedinarecentmeta-analysisoffourhigh-qualityRCTsconductedintheUSA(Campbelletal.2011)whichtogetherincluded681participants.Itwas,however,decidedtousedataonlyfromtheEQOLISEstudysinceUKlabourmarketsaremoresimilartoEuropethantheUSA.
Figure 4: Hours worked by IPS and standard Vocational Services participants (adapted from Burns et al 2007)
250
200
150
100
50
0
IPS
VS
Ho
urs
Wo
rked
0-6Months 6-12Months 12-18Months

20
Thisincreaseinearningstranslatesdirectlyintosocietalbenefitof£1700over18months(conservatively,employmentwasvaluedatthenationalminimumwageof£6.08perhour).Forpresentpurpose,tocreateanestimateofthebenefitaccruingtotheExchequerasaresultofthisincreaseinearnings,anaverageindirecttaxof18%canbeused,resultinginanincreasedrevenueof£300over18monthsfortheExchequer.
SincetheestimatedaverageearningsresultingfromIPSarerelativelysmall–onlyeightofthe312EQOLISEparticipantswereestimatedtohaveannualearningsabovethelowerthresholdforincometax(£8105)15–noincreasedrevenueduetoincometaxesornationalinsurancecontributionswereestimated.
Other Economic ImpactsAnalysisofthecostimplicationsofIPSpresentedinthisreportcoversonlycostsandbenefitsrelatedtomentalhealthserviceuseandearnings.WehavenotattemptedtoestimatethecostconsequencesofanyeffectthatIPSmighthaveonphysicalhealth,criminaljusticecontactsorhousingbecause,althoughitispossiblethattheseeffectsmightresult,thereisinsufficientrobustevidenceonthem.Arecentmeta-analysisofIPSservicesintheUSAsuggestedthatIPScouldpossiblyreducehomelessnessandsubstanceabuseandhencegeneratefurthersavings,althoughtheresultsofthemet-analysiswerepositivebutnotstatisticallysignificant.Additionally,inthepresentreportwehaveassumednoreductioninbenefitreceiptresultingfromIPS,whereasinrealityitislikelythatbenefitreceiptwouldfallwiththeincreaseinthecompetitiveemploymentrate.
Figure 5: Estimated cost savings per service user following the introduction of an IPS service
4,500
4,000
3,500
3,000
2,500
2,000
1,500
1,000
500
0
HealthServiceSavings
PublicSectorSavings
SocietalBenefit
Est
imat
edc
ost
sav
ing
per
ser
vice
use
r(£
)
0-6Months 6-12Months 12-18Months
15. This is an underestimate since a minimum wage rate was assumed for all participants whereas in reality some would be earning significantly more. Thus the actual benefit accrued to the exchequer is likely to be more than the figure estimated here.

21
Net SavingsInterventioncostsweretakenfromtheLondonsiteoftheEQOLISEstudy.Inreality,intervention‘costs’whenIPSwascomparedtostandardvocationalserviceswereactuallynegativesinceIPSwassignificantlycheapertoprovidethanthesestandardservices.Whilstthismaynotrepresentarealisticcostsavingformentalhealthservicesthatcurrentlyofferlittleornovocationalservices,suchasituationmayresultinlargersavingsinotherareasasaresultofanevengreaterdifferentialintheemploymentrate.
PuttingtogetherthesevariouscostcomponentswearriveatestimatednetsavingsperserviceuserofimplementinganIPSservice:
� TheintroductionofIndividualPlacementandSupportServicesisestimatedtosavetheNationalHealthService£5193peruseroftheserviceoveran18monthperiod.
� ItisestimatedthattheintroductionofIPSserviceswouldsavethepublicsectorasawhole£5501peruserover18monthsthroughreducedhealthservicecostsandincreasedtaxrevenue.
� TakingasocietalviewthenetbenefitsofIPSareestimatedtobe£6906peruserover18monthswhichincludestheincreaseintotalproduction,notjustthecomponentcollectedintaxrevenuebythegovernment.
ThesenetsavingsarerepresentedinFigure5.
Figure5representsestimatedcostsavingsperserviceuserengagingwithanIndividualPlacementandSupportservice.TheEQOLISEstudy,onwhichthecalculationsinthisreportarebased,studiedonlypeoplewithschizophreniawhowishedtofindcompetitiveemployment(Burnsetal.2007)andtherefore,sinceIPSwouldnotbesuitableforallpeoplewithschizophrenia,itisdifficulttocalculateaggregatesavingsthatmightflowfromthenationalroll-outofIPSservices.
CaveatsManypeoplehaveexpresseddoubtsabouttheapplicabilityofIPS,aservicemodeldevelopedintheUSA,toaUKcontext(Heslinetal.2011).TheyarguethatthedifferingstructureofsocialsecurityandthelabourmarketsmeansthatIPSwouldbelesseffectiveintheUKduetoalessernecessitytofindworkinordertosurviveintheUSA.Thisargumentisslightlymisleading,sinceitdoesnottakeintoaccountthattherearealsomajoreconomicdisincentivestoregainingemploymentintheUSA–peoplewilloftenlosetheirentitlementtoprogrammeslikeMedicaidwhentheybecomeemployed.
Therearelegitimateargumentstobemadeaboutthedifferingincentivestoworkacrossnations,buttheoverarchingpremiseandmotivationofanIPSapproachisthatthemajorityofindividualswithschizophreniawanttofindcompetitiveemployment.Thisisoftennotonly(orperhapsatall)foreconomicreasons,andgainingsuchcompetitiveemploymentisclinicallybeneficial.However,someresultsdosuggestthattheworkincentivesintheUKaresuchastodiscouragethepursuitofcompetitiveemploymentforindividualswithschizophrenia.IntheEQOLISEstudy,Burnsandcolleagues(2007)foundthatLondonwasatthehighestriskoutofthesixEuropeancentresofhavingabenefittrapdespitetherebeingmeasuresinplacetoreducethedisincentivesforwork(SainsburyCentreforMentalHealth2004).CurrentreformstosocialsecurityentitlementsinEnglandmight,ofcourse,reduceanyfinancialdisincentivetowork.
FAMILY THERAPY
Familytherapyreferstoarangeofpsychosocialinterventionsforpeoplewhohaveasignificantemotionalconnectiontosomeonewithschizophrenia,herereferredtoforsimplicityas‘thefamily’.Thetherapytypicallyinvolvesprovidinginformationaboutschizophrenia,searchingformethodsofsupportinganindividualwithschizophreniaandresolvingpracticalproblems.Interventionsareaimedatreducingthelevelofexpressedemotionwithinthefamily,sinceexpressedemotionhaslongbeenrecognisedasarobustpredictorofrelapse(Butzlaff&Hooley2012).

22
Althoughfamilytherapyhasbeenanacceptedinterventioninschizophreniatreatmentforalongtime,relativelyfewstudieshaveformallyattemptedtoassessitseconomicimpact(Mihalopoulosetal.2004;Knapp2000;Leffetal.2001;Goldstein1996;McFarlaneetal.1995;Tarrieretal.1991;Libermanetal.1987).Inthisreport,webaseoureconomicanalysisoffamilytherapyprimarilyonarecentdecisionmodelbytheauthorsofthisreport(tobepublishedseparately).ThismodelusestheestimatedriskratiosassociatedwiththeprobabilityofrelapsewithfamilytherapyderivedfromarecentCochranesystematicreview(Pharoahetal.2010)toupdateprobabilitiesofrelapseunderstandardcaretoestimatethetotalserviceusecostsunderfamilytherapyandstandardcare.
Themodelestimatesacostsaving(netofinterventioncost)of£1,004overathree-yearperiod,meaningthatfamilyinterventionwouldbeseentobesuperiortostandardcareinthatitisassociatedwithbothbetterclinicaloutcomesandlowercosts.Insensitivityanalysisthisresultheldusingavarietyofdifferentadmissioncosts.
CRIMINAL JUSTICE SYSTEM DIVERSIONManypeopleinthecriminaljusticesystemhavecomplexmentalhealthneedswhicharepoorlyrecognisedandinadequatelymanaged.Largenumbersendupinprison:ahigh-costinterventionwhichisinappropriateasasettingformentalhealthcareandineffectiveinreducingsubsequentoffending.Theoverallsizeoftheprisonpopulationhasmorethandoubledinthelast20yearsandoneprisonerintenhasaseverementalillnesssuchasschizophrenia.
Diversionseekstoensurethatpeoplewithmentalhealthproblemswhocomeintocontactwiththecriminaljusticesystemareidentifiedanddirectedtowardsappropriatementalhealthcare,particularlyasanalternativetoimprisonment.Diversioncanbewithinoroutsidethejusticesystemandneednotreplacesanctionsforanyoffenceapersonhascommitted.
Forsomeoffenderswithseverementalillness,themostappropriatealternativetoprisonisplacementinanNHSsecureunit.Theseunitsare,however,intendedonlyforthosewhohavecommittedseriousoffencesandthegreatmajorityofprisonerswithseverementalillnessareonshortsentencesandhavenotcommittedseriousenoughcrimestowarranttransfertoasecurehospital.
Aboutthree-quartersofallpeoplesenttoprisoneachyearreceivesentencesoflessthan12monthsandparticularlyforthoseinthisgroupwithseverementalillnessthereisastrongcost-effectivenesscasefortheuseofsuspendedsentencesorcommunityordersinsteadofimprisonment,togetherwithanappropriatepackageofcommunity-basedmentalhealthsupport.
Intermsofcostsacommunitysentenceisfarcheapertoprovidethanaprisonsentence.FiguresfromtheNationalAuditOffice(Accenture2007)suggestthatonaverageacommunitysentencecostsbetween£720and£4,10016dependingonitstype.EventheMentalHealthTreatmentRequirement,whichisthemostexpensiveofthetwelvecommunityorders,costsonlyroughly10%ofthecostoftheaverageprisonsentence(MinistryofJustice2011b).
Intermsofeffectivenesstooitappearsthatcommunitysentencesdominateprisonintheoutcomestheyachieve–bothclinicallyandinreducingreoffending.Peoplewithschizophreniacangetmuchbettermentalhealthcareinthecommunitythaninprison:prisonisaverypoortherapeuticenvironmentwhich,ifanything,islikelytoexacerbateamentalhealthproblem.Sincethepeopleforwhomcommunityordersaredesignedareonshortprisonsentences(typicallylessthanoneyear)theyareunlikelytobeenrolledon,orbenefitfrom,behaviouralprogrammesaimedatreducingre-offending.Withaprisonsentencetheyarealsonotrequiredtoseeaprobationofficerafterreleasewhichmeanstheygetlittleornosupportoncebackinthecommunity,incontrasttowhatwouldhappeniftheywereonacommunitysentence.Partlybecauseofthesefactorsre-offendingratesaresignificantlyhigheronalike-for-likebasiscomparingpeopleonashortprisonsentenceandthoseonacommunitysentence.Indeed,
16. Uprated to reflect current prices using the GDP deflator, ONS.

23
usingamatchedpairstechnique,theMinistryofJusticeestimatedthatCommunityOrders(ofalltypes)resultinan8percentagepointdecreaseinre-offendingrateswhencomparedwithcustodialsentencesoflessthanoneyear(MinistryofJustice2011a).
Itistobenotedthatthereisnostrongargumentforprisonsentencesovercommunityordersonpublicsafetygroundsgiventhatthetypeofoffencesinvolvedarerelativelyminor.
TheMentalHealthTreatmentRequirement(MHTR)isoneofthetwelverequirementsthatmagistratesandjudgescanplaceonindividualswhoreceiveaCommunityOrderoraSuspendedSentenceOrder.Therequirementmeansthattheindividualisthenrequiredtoreceivementalhealthtreatmentforadefinedperiodoftime.Despiteitsintroductionin2005,recentdatafromtheMinistryofJusticeshowaverylowuptakeoftherequirement.Whilst43%ofpeopleservingcommunitysentenceshavesomesortofmentalhealthproblem(Solomon&Silvestri2008),only0.3%aregivenaMentalHealthTreatmentRequirement.BarrierstomorewidespreaduseofMHTRsincludedifficultiesinobtainingpsychiatricassessments,
ineffectiveidentificationofmentalhealthproblemsinthecriminaljusticesystem,alackofawarenessoftherequirementswithinthecriminaljusticesystemworkforceandalackofcommunicationandtrustbetweenhealthservicesandthecriminaljusticesystem(Khanometal.2009;Seymouretal.2008).17
Itis,however,importanttoemphasisethatthecasefordiversionforpeoplewithschizophreniadoesnotstandorfalldependingonwhetherornottheygetanMHTR.IfanMHTRisdeemedtobeunsuitable,perhapsbecauseofaninappropriatenessofprovidingtreatmentonacompulsorybasis,thecost-effectivenesscaseforthediversionofpeoplewithschizophreniaoutofprisonandintothecommunitystillstands.
PHYSICAL HEALTH
AsdiscussedinSection1.5,thephysicalhealthofindividualswithschizophreniaandtheassociatedeconomicconsequenceshavelongbeenoverlooked.Interventionsforschizophreniaarerarelyanalysedfromaphysicalhealthperspective;thein-depthcost-
Figure 6: Mean Differences in change in body weight between the treatment and control groups. End of treatment results include follow up, up to 6 months (95% CI in parentheses). Source: Faulkner et al. (2010)
Cognitive/BehaviouralIntervention
PharmacologicalIntervention
PreventingWeightGain
Mediumterm:
-3.38kg(-4.81kgto-1.96kg)
Endoftreatment:
-4.87kg(-7.11kgto-2.64kg)
Endoftreatment:
-1.16kg(-1.90kgto-0.41kg)
TreatingWeightGain
Mediumterm:
-1.69kg(-2.77kgto-0.61kg)
Endoftreatment:
-3.85kg(-4.25kgto-3.44kg)
17. The reports make detailed recommendations as to how MHTRs could be better implemented.

24
consequenceanalysisoftheantipsychoticmedicationaripiprazolewhichtookintoaccountrisksofdiabetesandcardio-vasculardiseaseundertakenbyBarnettandcolleagues(2009)isarareexception.Itisimportantthatphysicalhealthimplicationsofalltreatmentsberoutinelyconsideredinanalysesthatinformpolicydecisions.Belowwediscussevidenceoninterventionsthatarespecificallydesignedtotargetthephysicalhealthofindividualswithschizophrenia.
Interventions to reduce weight Respondingtohigherthanusuallevelsofoverweightandobesityamongstindividualswithschizophrenia,arangeofinterventionshavebeendevisedwhichaimtoreduceweight(eitherpreventweightgainortreatweightgain).Suchinterventionscanfallintothebroadcategoriesofcognitive-behaviouralinterventionsthatworkthroughchanginglifestylechoicesandpharmacologicalinterventions.
ArecentCochranereview(Faulkneretal.2010)ofsuchinterventionsfoundthatbothtypesofinterventions(withinwhichtherearemanydifferentspecificinterventions)wereeffectivebothatpreventingandtreatingweightgainintheshorttomediumterm.Figure6offersasummary.
Evenwhenthereissignificantweightreductionintheshortrunitisverydifficulttodrawconclusionsabouttheeconomicimpactofsuchinterventions.Thereislittleevidencewithwhichtodeterminewhetherornotanyreductioninweightissustainedintothelongerrun.Sincemanyoftheseinterventionsaredesignedtobeadministeredintheearlystagesofschizophrenia,theparticipants’riskofsufferingamajorphysicalhealthevent(suchasaheartattackorstroke)issmallintheshortterm,andsoevenifareductionofweightoccursthismaybeoflittleimportanceinincreasingoveralllifeexpectancyifweightreductionisnotsustained.Thus,tofullyunderstandtheeconomicconsequencesofinterventionsthataimtoreduceweightinpeoplewithschizophrenia,moreresearchisneededlookingattheextenttowhichweightlossissustained.18
Exercise TherapyExercisetherapyisaninterventionthatissometimesusedwiththeaimofincreasingmentalandphysicalwellbeing.ClinicaloutcomesreportedinarecentCochranereview(Gorczynski&Faulkner2011)weregenerallypositive,recordingsignificantimprovementsinmeasuresofmentalhealthandphysicalfitness.However,thelimitednumberofstudiesaddressingExerciseTherapyasatreatmentinschizophreniaandthelackofevidenceastohowchangesinphysicalfitnesstranslateintoeconomicconsequencesmeansthatnomoreanalysisispossiblehere.
Smoking CessationAsdiscussedinSection1.5,schizophreniaisassociatedwithalmostadoublingoftheriskoftobaccouse,whichinturnhasmanyadverseaffectsonphysicalhealth.Inresponse,avarietyofinterventionshavebeenconceptualisedinordertohelppeoplewithschizophreniastopsmoking,manyofwhicharebasedoninterventionsthathavepreviouslybeenshowntobeeffectiveforthepopulationasawhole.InarecentCochranereview,Tsoiandcolleagues(2010)foundevidencetosuggestthattheantidepressantbupropioncouldbeeffectiveathelpingpeopletoquit.However,toolittleevidencewasfoundinourreviewtodrawanymeaningfulconclusionsabouttheeffectsofothertreatmentssuchasnicotinereplacementtherapyandpsychosocialinterventions.
Intermsofcost-effectivenessevidence,littleanalysishasspecificallyaddressedthequestionofwhetherinterventionsdesignedtohelppeoplewithschizophreniatostopsmoking.OnerecentanalysisusedaMarkovmodeltoconsidertheeconomicimplicationsoften-weekinterventionofbupropionandco-interventions(grouptherapyeitheraloneorwincombinationwithnicotinereplacementtherapy)andcomparedthistoco-interventionsonly.Themodelestimatedthattheincrementalcost-effectivenessratioofthecombinedinterventionwas£385perQALY,wellbelowNICE’srecommendedthresholdforcosteffectiveness.Themodelpredictedthattherewasa95%chancethatthecombinedinterventionwasmorecost-effectivethantheco-interventionsonly(Winterbourne2012).
18. Current research in PSSRU at the LSE is looking at the economic case for weight loss/avoidance interventions for people in the early stage of their psychosis.

25
SUBSTANCE MISUSE
AsdiscussedinSection1.8,substancemisuseamongstpeoplewithschizophreniahassignificantadverseeconomicconsequences,inpartthroughinflatingNHScostsandcriminaljusticesystemcosts.Thecomplexneedsofthispopulationareincreasinglybeingrecognised;NICEhasrecentlypublishedaguidelineonassessingandmanaging‘psychosiswithco-existingsubstancemisuse’.ClinicalpracticerecommendationsbyNICEaddressmanybroadareastoequipmentalhealthandsubstancemisuseservicestoworkeffectivelywithpeoplewhofallundertheremitofbothservices.Here,wesummarisetheavailableeconomicevidenceonpsychologicalandpsychosocialinterventionsthathavebeenspecificallydesignedforapopulationwithco-existingschizophreniaandsubstancemisuse.
Avarietyofpsychologicalandpsychosocialinterventionsarerecommendedforpeoplewithoneofschizophreniaorsubstancemisuse,butsomeevidencesuggeststhatindividualswithadualdiagnosiscanbeexcludedfromtheseinterventions(inparticular,manydonotreceiveanytreatmentforsubstancemisuse)(DepartmentofHealth2006).Thereforepsychologicalandpsychosocialinterventionshavebeendesignedspecificallyforthispopulationwithadualdiagnosis;theseinterventionsgenerallyinvolvesomecombinationofCBTandmotivationalinterviewing.
Theclinicaloutcomesrecordedbymeta-analysesinarecentCochranereview(Clearyetal.2010)andbyNICE(2011)aremixed,withsomeevidenceofsignificantimprovementsinsubstancemisuseandmentalhealth,althoughmanymeasuresshowednosignificantdifference.Samplesizesweregenerallysmall,aswerethenumberofrelevantstudiesavailable.
OnerandomisedtrialhasattemptedtostudytheeconomicconsequencesofaninterventionthatcombinedCBT,familyinterventionandmotivationalinterviewing(Haddock2003).Awiderangeofcostswastakenintoaccount,includinghealthservicecosts,travelcosts,productivitylossesandout-of-pocketexpenditures.Netofinterventioncosts(the
interventioncost£281319overan18monthperiod)itwasfoundthatmeantotalcostswere£1627lower(p=0.25)fortheinterventiongroupthanforthecontrolgroup(95%CI:£9012lessto£5759more).Netofinterventioncosts,meancostsincurredbythehealthservicewere£1554lowerfortheinterventiongroup.Theauthorsestimatedthattherewasa69.3%chancethattheinterventionwascost-saving(awillingnesstopayofzero).Ifthefavourableclinicalresultsproducedbytheinterventionweregivenvalue,theprobabilityoftheinterventionbeingcost-effectivewouldincrease.Whilstthisstudyshowssomepromisingresultsforsuchinterventions,thesmallsamplesizeandlackofothersimilartrialsmeancautionmustbeapplied.
HOMELESSNESS- TARGETED INTERVENTIONS / SUPPORTED HOUSING
AsdiscussedinSection1.4,peoplewithschizophreniaintheUKarehighlyvulnerabletobecominghomeless,withmajorimplicationsfortheirmentalandphysicalwell-being,andfordirectservicecosts,aswellasrepresentingahugewasteofeconomicpotential.Inrecognitionofthisproblemavarietyofdifferentinterventionshavebeenconceptualisedwhichaimtoreducetheincidenceofhomelessnessamongstpeoplewithseverementalillness.
Critical Time InterventionsACriticalTimeIntervention(CTI)is‘anindividual-levelinterventiondesignedtoreducetheriskofhomelessnessandotheradverseoutcomesinadultswithmentalillnessfollowingdischargefrominstitutionstocommunityliving’(Hermanetal.,2007).Suchinterventionstypicallylastaround9monthsandconsistofthreephases–thetransitionphase,thetry-outphaseandthetransferofcarephase.ACTIworkeroverseesthewholeinterventionandperformskeyrolesincludinghomevisits,co-ordinatingcare-givers(meetingwith,givingadvicetoandmediatingconflicts)anddevelopingplansforlong-termgoals(Hermanetal.,2007).
19. Updated to reflect current prices using PSSRU’s Pay and Prices Index.

26
Arandomisedcontrolledtrialtoexaminetheeffectivenessandcost-effectivenessofCTIwascarriedoutwithasampleof96mendischargedfromashelterinNewYorkCitybetween1991and1993.ThisstudyshowedtheCTIgroupexperiencedsignificantlyfewernightsofhomelessnessascomparedtothecontrolgroup(p=0.003)andsignificantlyfewerperiodsofextendedhomelessness(over54nights)(p=0.45)(Susseretal.1997).Are-analysisofthedataalsosuggestedasignificantreductioninchronichomelessness(Lennonetal.,2005).Acost-effectivenessanalysisofthesametrialrevealedthatmeancosts(includinginterventioncosts,mentalhealthcare,otherhealthcare,acuteservices,substanceabuseservices,housingservices,criminaljusticeandpublictransfers)werebroadlysimilaracrossthetwogroups:costsincurredbytheCTIgroupwere1.4%higherthanthoseincurredbythecontrols.
Thecostoftheinterventionwasalmostoffsetbyareductioninserviceuse(inparticularinacuteservices,supportedhousing,shelterservices).Theauthorsconcludedthatawillingnesstopayofmorethan£14720pernon-homelessnightmadeCTIacost-effectiveintervention.ThissuggestsCTIcouldpossiblybeacost-effectiveinterventionintheUKtoo,althoughmoreworkwouldneedtobedonetoseehowsuchinterventionscouldbeadaptedtoaUKcontext.
ArecentRCThascomparedoutcomesfollowingdischargefromapsychiatrichospitalinNewYorkCityofagroupreceivinga9-monthCTIserviceinadditiontousualcareandacontrolgroupreceivingonlyusualcare.ThisstudyestimatedthattheCTIserviceledtoafive-folddecreaseintheriskofhomelessness(Oddsratio:0.22,95%CI:0.06,0.88)(Hermanetal.2011).WhilstthisstudymakesnomentionofserviceuseorthecostsofprovidingCTI,suchadramaticreductioninhomelessnesssuggeststhisisanimportantinterventiontoconsider.
Althoughnodataareyetavailable,astudyledbytheUniversityofManchesteriscurrentlyevaluatingCTIforpeoplewithmentalhealthproblemsreleasedfromprison,
Assertive Community TreatmentAssertiveCommunityTreatment(ACT)referstoanoutpatientservicemodelgroundedonamobileteamdeliveringpsychiatriccareandcasemanagementtopeoplewithschizophreniawhomakeintensiveuseofinpatientservices.Theapproachwasnotdesignedspecificallytoaddresstheissueofhomelessnessamongstpeoplewithseverementalillness,althoughithasbeensuggestedthatACTmaybeaneffectiveinterventiontotackletheissue.
Wolffandcolleagues(1997)conductedacost-effectivenessanalysisofanRCTexaminingtheeffectofprovidingthreeformsofcasemanagementtoindividualswithseverementalillnesswhowereeitherhomelessoratriskofhomelessnessfromSt.Louis.WhilstACTservicesdidnotsignificantlyreducetheincidenceofhomelessnesstheauthorsdidfindthattherewasnosignificantdifferenceintotalcostsincurred(areductioninserviceuselargelyoffsethigherinterventioncostsofACT)andanimprovementinsymptomsandsatisfaction,indicatingACTmaybeacost-effectiveinterventionfordeliveringmentalhealthservicestothehomeless.AnotherRCTstudyingtheoutcomesofprovidingACTtohomelesspeoplewithseverementalillness,thistimeinBaltimore,foundpositive,butlargelyinsignificant,effectsonhousingoutcomes(Lehmanetal.1997).ThisstudysuggestednetsavingsfromtheimplementationofanACTservice:meancostpercase(netofinterventioncosts)wasfoundtobe24%lowerfortheACTgroupthanthecontrol.WhilstthesetwostudiesdoprovidesupportingevidenceforthepremisethatACTisacost-effectiveinterventionforhomelesspeoplewithseverementalillness,Rosenheck(2000)hasquestionedthegeneralizabilityoffindingssincebothstudieshadpatientswhoincurredmuchhighercosts(atbaseline)thantheUSnationalaverageandthusitmaybeeasiertoprovecost-effectivenessorcost-neutrality.
Arecentlarge-scale(non-randomised)studyofACTintheUSAsuggestedthatACTdidnotsignificantly(inthematchedsample)reducedhomelessnessyetcausedanetincreaseincosts,thusquestioningwhetherthisisthemosteffectivewaywithwhichtodealwiththeproblemofhomelessnessamongstpeoplewithschizophrenia(Sladeetal.2012).
20. Figure converted from US$ using PPP rates in 1992 and then uprated for inflation using the GDP deflator.

27
TheabovestudieswereallconducedintheUSAandthefirsttwoarenowquitedated,meaningquestionsmustbeaskedabouttherelevanceofthesefindingsfortheUKtoday.ThemostrecentRCTstudyinghigh-fidelityACTintheUKfoundnoreductioninserviceuseforACTserviceusers–indeedtotalin-patientdayswerehigher(butinsignificant)fortheACTgroupthanforthecommunitymentalhealthteamgroup(Killaspyetal.2009).Whilstthestudydidnotreportonhomelessnessdirectly,itraisesquestionsabouttheaddedbenefitthatACTservicesbringaboveandbeyondCommunityMentalHealthTeamsinaUKcontext,notleastbecausemany‘standard’communityservicesnowembodytheprinciplesofassertiveoutreach(Burnsetal2001).
Outreach ProgrammesOutreachprogrammesaimtoimproveoutcomesforhomelesspeoplewithmentalillnessbyengagingwithhomelesspeoplewhoareunwillingtofindhelpontheirownandprovidinghelptosuchgroups.
TheonlyoutreachprogrammeevaluatedwithanexperimentaldesignistheNewYorkChoicesprogramme.Thisconsistedoffourmainelements:(1)outreachandengagement,(2)invitationtotheChoicesCentre,(3)respitehousing,and(4)in-communityandon-siterehabilitationservices(Shernetal.2000).Byusingavailableserviceusedata,Rosenheck(2000)estimatedthattheserviceincreasedcosts,boththroughtheadditionalinterventioncostsandthroughincreasedserviceusecostsasmorepeoplewerebroughtintoservices.
Similarly,byestimatingthecostimplicationsfromserviceutilisationdata,Rosenheck(2000)estimatedthattheAccesstoCommunityCareandEffectiveSupportiveServicesProgram(Lam&Rosenheck1999)wasacost-increasinginterventionbutwaseffectiveinimprovingaccesstohousingandimprovingsymptoms.Likewise,anobservationalstudyoftheDepartmentforVeteran’sAffairsveteran’sprogramshowedhealthcarecosts(bothinpatientandoutpatient)increasedsignificantlywithoutreachcontact,withanobservedincreaseinhealthcarecostsof13%.Whenthecostsoftheinterventionarealsoadded,the
observedincreaseincostsintheyearafterfirstoutreachcontactwas36%(Rosenhecketal.1993).
Bythedefinitionofoutreach,theseprogrammesveryoftenbringpeopleintocontactwithserviceswhomaynototherwisehavebeenso,andthusmaywellincreaseserviceusecostsaswellasimprovingoutcomes.Thisdoesnotmeantheseprogrammesarenotcost-effective,buttheircosteffectivenessliesinthebalanceoftheextracoststheyincur,theimprovementinoutcomesandthevaluesocietyplacesonthoseimprovements.
Supported HousingSupportedhousingforpeoplewithschizophreniaisseenasacrucialcomponentofcareforthosewhomaynotbeabletoliveindependentlyinthecommunity(Lelliottetal.1996;Priebeetal.2009).High-qualitysupportedhousinginterventionsmayreducethenumberofpeoplewithschizophreniawhobecomehomeless(Macpherson2004).Surprisinglyveryfewhigh-qualitystudieshaveattemptedtoaddresstheimplicationsofsupportedhousingforpeoplewithschizophrenia(orseverementalillnessingeneral).Indeed,arecentCochranereviewonthesubjectfoundthatnostudiesmettheirinclusioncriteria(Chilversetal.2010).
Studieshaveaddressedtheissuebutgiventheirmethodologicalweaknessesresultsmustbeinterpretedwithcaution.OnestudyinBoston,MassachusettsrandomisedparticipantstoeitherEvolvingConsumerHouseholds(wherepeoplewithschizophrenialivedingroupsand,intheearlystages,hadmuchsupportfromprogrammeworkers)orIndependentLivingapartments.Housingandclinicaloutcomeswerenotsignificantlydifferentbetweenthetwogroups,butcostsfortheEvolvingConsumerHouseholdsgroupweremuchgreaterduetotheadditionalhousingcosts(Dickeyetal.1997;Rosenheck2000).AnobservationalstudyoftheDepartmentforVeteran’sAffairsHomelessChronicallyMentallyIllVeteransPrograminwhichhomelesspeoplewithmentalillnessweregiventime-limitedtreatmentinahalfwayhousesuggestedthatresidentialtreatmentledtosuperioroutcomes

28
butincreasedcosts:meancostsfortheresidentialtreatmentgroupwere53%higherthanforthecasemanagementgroup(Liptonetal.1988;Rosenheck2000).
Theevidenceonthecost-effectivenessofsupportedhousinginterventionsinthecontextoftacklinghomelessnessismixed.Thereisaneedforrobuststudiesinthisarea.
CRISIS TEAMS
CrisisResolutionHomeTreatment(CRHT)teamswereestablishedintheNHSfollowingtheirrecommendationintheNationalServiceFrameworkin1999(DepartmentofHealth1999).Theaimoftheseteamsistoprovideintensivetreatmentandsupportinthecommunitytothoseundergoingaseverementalhealthcrisisthatwouldotherwiseresultinadmissiontoaninpatientunit.EffectiveCRHTteamsreduceinpatientusage,boththroughreducingtheprobabilitythatanadmissionwouldoccur(actingasasocalled“gatekeeper”)andbyallowingforearlierdischarge.
StudiessuggestsavingscanbemadefromCRHTteamswhentheyareimplementedwithhighfidelity.Aprospectivenon-randomisedstudycomparedservicecostsofpatientsbeforeandaftertheimplementationofaCRHTteaminSouthIslington(McCroneetal.2009b).ItwasfoundthatmeancostsforthecohortfollowingtheimplementationoftheCrisisResolutionteamwere£173821lowerthanbeforetheservice,althoughthisdifferencewasnotstatisticallysignificant.AsubsequenteconomicevaluationalongsidearandomisedcontrolledtrialexaminingtheeffectsofaCrisisResolutionTeaminNorthIslingtonfoundthatmeantotalserviceusecostswere£252022(90%CI:£969to£4054)lowerforthoserandomisedintotheCRTgroup(McCroneetal.2009c).
However,studieslookingattheeffectsoftheimplementationofCRHTteamsastheyhavebeenimplementedandareworkinginpracticehavebeenslightlymoremixed.Aninitialanalysisshowedapositiveeffectoninpatientadmissionswithadmissionsfallingbyanaverageof10%(95%CI:1.7%to18.1%)moreinthe34areaswhichhadhadCRHTteamsinplaceforthepasttwoyearsandby23%(95%CI:7.1%to38.4%)moreinthe12areas
whichoperated24hoursaday,comparedwiththe130areaswithoutCRHTteams(Gloveretal.2006).However,reanalysisofthesameadmissiondatareachedadifferentconclusion.Thereanalysisusedadifference-in-differencemodelandcontrolledforconfoundingvariablessuchasdeprivation,substancemisuse,age,gender,populationdensity,region,lengthofstayandfidelityofservices.TheCRHTindicatorvariablewasnotsignificant.ThisanalysisledtheauthorstotheconclusionthattheimplementationofaCRHT per se didnotdecreaseadmissionrates(Jacobs&Barrenho2011).However,thisperhapsreflectsthefactthatwhileinpatientuseforthosereceivingCHRTinputfalls,beduseforanareamaybemaintainedduetotheexistenceofexcessdemand.
EarlierworkbytheNationalAuditOffice(2007)suggestedthatwhileCRHTteamswerehavingapositiveimpactoninpatientbeduse,teamswereoftennotutilisedtotheirfullpotential.Thesurveyof500admissionstheycarriedoutsuggestedthatonlyhalf(asopposedtoall)ofadmissionshadbeenassessedbyaCRHTteamandthat20%ofadmissionscouldhavebeensuitableforCRHTinstead.EconomicanalysisfortheNAO,usingadecisionmodellingframework,estimatedasavingof£69023percrisisepisodewithfullutilisationofaCRHTteamversuswhennosuchservicewasavailable.Thiseconomicanalysisconcludedthatatleast£13.7millioncouldbesavedeachyearifteamsinwhichabelow-averageproportionofcasesinvolvedCRHTinvolvementcouldincreaseinvolvementtotheaveragerateof53%.Theyestimatedpotentialsavingsof£59millionayeariftheinvolvementratewas90%forallteams.
LikewiseareportbytheHealthcareCommission(2008)suggestedthatCRHTteamswerenotasfullyutilisedasintended.Duringasix-monthstudyperiod,CRHTswereinvolvedinonly61%ofalmost40,000admissionstoacutewards,withverysubstantialvariationsacrossthecountry(ratesrangedfrom9%to100%).Likewise,only25%ofalmost40,000dischargesfromacutewardsoccurredearlywithCRHTsupport(ratesrangedfrom0%to70%).ThisevidencesuggeststhatthereducedinpatientbedusefollowingtheintroductionofCRHTteamsisnotasgreatasitcouldbe,whichinturnsuggeststhatfurthercostsavingscouldbemadeiffullerusewasmadeofCRHTteams.

29
PEER-SUPPORT WORKERS
Soloman(2004)definespeersupportas‘socialemotionalsupport,frequentlycoupledwithinstrumentalsupport,thatismutuallyofferedorprovidedbypersonshavingamentalhealthconditiontootherssharingasimilarmentalhealthconditiontobringaboutadesiredsocialorpersonalchange.’Suchsupportmaybedeliveredvoluntarilyorbefinanciallyremunerated.Itcantakedifferentforms:self-helpgroups,internetsupportgroups,peer-deliveredservices,peer-runoroperatedservicesandpeeremployees(Solomon2004).Generallyanimportantdistinctionisthattheseservicesareunlikemutualsupportbecausepeer-supportworkersreceivetrainingandsupervision(RepperandCarter2011).Whilstsomeoftheseserviceslikeself-helpgroupshavelongformedapart,albeitoftenaninformalpart,ofrecoveryfrommentalillnessintheNationalHealthService,othersarerelativelynewandhaveyettobecomemainstreamcomponentsofcare.
Peer-supportworkersare,atthesimplestlevel,peoplewhohaveexperiencedlivingwithadiagnosisofseverementalillnessandhavebeenabletorecover.RecoveryemergedasapsychiatricconceptintheEnglish-speakingworldinthe1970sandhaslargelyovertakentheprevioustraditionalmedicalmodelintheUS(Davidson2005).Itdefinesthehealthoutcomeasoverallwellbeingbeyondsymptommanagement.Ofcentralimportanceinthe‘recovery’approachistheverydifferentexpectationthatpatientscanleadnormallives,secureemployment,furthereducationandtraining,andindependenthousing.Peer-supportworkersarethosethatare‘furtheralongtheirroadtorecovery‘(Deegan1996;Repper&Carter2011;Davidsonetal.2006).Peer-supportworkersarethoughttobenefitpatientsbysharingtheirexperience,provideanempatheticandreciprocalrelationship,andarebetterabletoprovidehopeandencouragement,whichincombinationprovidepatientswithempowerment,confidence,andincreasedself-esteemthatfacilitatestherecoveryprocess(Kleinetal.1998;Forchuketal.2005;Davidsonetal.2006;Lawn2007;Riveraetal.2007;Repper&Carter2011).
Theevidencebaseonpeer-supportworkerslargelycomesfromtheUSandasrecentlyas2003itbecameafederallyreimbursedservice(ThePresident’sNewFreedomCommissiononMentalHealth2003).InaforthcomingreportfromtheCentreforMentalHealth,itwasfoundthatpeer-supportworkersareacost-effectivecomponentofservicedelivery.
Theevidencebaseonpeer-supportworkersstaffedinadjunctpositionsisgrowingandfairlyextensive,althoughisalsoheterogeneouswithrespecttothefunctionsandservicemodelsinwhichtheyareemployed.IntheforthcomingreportfromtheCentreforMentalHealth,theauthorsidentifiedsevenstudiesofgooddesign,amajorityofwhichwereeitherrandomizedorobservationalstudies,withonestudyrelyingonexpertopinionfortheestimationofhospitaldayssaved.Generallyitwasfoundthatonepeer-supportworkercouldsaveasignificantnumberofhospitaldaysperindividualperyearandtheevidencebaseseemsverypositiveinthisregard.TheestimatesusedbytheCentreforMentalHealthareconservative,reflectingminimumsavings,althoughthestudiesthemselveshavereportedgreaterreductions.TheCentreforMentalHealth,usingUKcosts,foundthatthereisanalmostcertainlikelihoodthatpeer-supportworkers,ifemployedandpaidascommunitysupportworkers,wouldgeneratenetcostsavings.Acrosstheeightstudies,thetotalsamplesizeforthecontrolandinterventiongroupswascloseto1,000each(CentreforMentalHealth,forthcoming).Intheseincludedstudies,healthbenefitswereeitherthesameas,ifnotbetterthanforindividualswithoutpeersupport.
Analternativemodelforpeersupportiswhenworkersareemployedinexistingcasemanagerroles.Here,threestudiesfoundnoworsenedoutcomesandpeer-supportworkerscouldfunctioninthesamewayascasemanagerswithnoexperienceofseverementalillness(Solomon&Draine1995;Clarkeetal.2000;Schmidtetal.2008).Thestudiesfoundnostatisticallysignificantdifferencebetweenindividualsinrelationtohealthorserviceuseoutcomesattheendofthestudy.Whileitwasexpectedthatpatientswouldexperienceimprovedoutcomes,atleastinserviceuse,
21. Uprated to reflect current prices using PSSRU’s Pay and Prices Index22. Uprated to reflect current prices using PSSRU’s Pay and Prices Index.23. All costs uprated to reflect current prices using PSSRU’s Pay and Prices Index.

30
Schmidt(2008)hypothesizesthismaybeduetopeer-supportworkersadoptingtheprofessionalculturetofitinandthusdownplaytheirmedicalhistoryandrelylessontheirpersonalexperience.Thesestudieswererandomizedcontroltrialswithsamplesizesoflessthan50ineachgroup;Clarkeetal(2000)replicatedthesamestudydesignasSolomonandDraine(1995),comparinganinterventionteamfullystaffedwithpeer-supportworkersascasemanagersandthecontrolteamstaffedwithcasemanagerswithnopersonalexperienceofasevermentalillnessdiagnosis.ThestudybySchmidt(2008)maybelimitedinitsabilitytodetectdifferencesbecausetheinterventionwasstaffedbyonlyonepeer-supportworkerasacasemanagerinateamofsixwiththeanalysisongroupdifferences,limitingtheabilitytodetectanydifferencesiftherewereany.
Itis,however,difficulttodrawfirmconclusionsfromjustthreestudiesfocusingonthecost-effectivenessintermsofhospitalization,andfurtherresearchinthisareaisclearlyneeded.
Itisalsoworthnotingthatthebenefitsofemployingpeer-supportworkersincludenotjustbenefitsrelatingtothepeopletheysupport,butalsobenefitstotheworkersthemselvesintermsofbeingingainfulemploymentandalltheassociatedrewardsthatthisbrings.
Inconclusion,furtherresearchwouldhelptogeneratestrongerconclusionsabouttheeconomicimplicationsofpeer-supportworkers.Weareawareofanumberofongoingprojectsinvolvingpeersupport(Williams2011;MentalHealthFoundation2012)anditishopedthatthesewillcontributehelpfullytotheevidencebase.However,themostrecentworkbytheCentreforMentalHealthreachesasimilarconclusiontopreviousliteraturereviews(Davidsonetal.1999;Simpson&House2002;Doughty&Tse2011;Repper&Carter2011;Wright-Berrymanetal.2011;Davidsonetal.2012)thattheresultsarepromisingandthattherearehealthbenefits.TheCentre’srecentwork,however,placesmoreconfidencethanpreviousreviewsintheassertionthattherearesignificantreductionsinhospitaldays,giventheenhancedevidencebasenowavailable.
ADVANCED TREATMENT DIRECTIVES
AdvancedTreatmentDirectivesaredocumentsdrawnuptoexpressapatientorserviceuser’spreferencesconcerningtreatmentoptionsandotherarrangementsintheeventoftheindividuallosingthecapacitytomakethatdecisioninthefuture.ThepreferencesexpressedinsuchdocumentscanbeoverriddenusingtheMentalHealthAct,buttheNICEguidelines(2009)statethat‘healthcareprofessionalsshouldendeavourtohonouradvancedecisionsandstatementswhereverpossible’.Suchdirectiveshavestrongethicalappealastheygivepeoplewithschizophreniaarighttoself-determination(includingtherighttorefusetreatment)attimeswhentheymaylackcapacity.Inaddition,therearehopesthatsuchdirectivescoulddecreasetheuseofcoercionandinvoluntaryadmissionduringperiodsofrelapse,possiblyresultinginreducedserviceuse.
ArecentCochranesystematicreviewofAdvancedTreatmentDirectivesfoundjusttwopublishedstudiesthatmetitsinclusioncriteria(moststudiesonthesubjectwerenon-randomisedandthereforeexcluded).ThefirstincludedstudywasanRCTexaminingtheeffectsofmakingalow-intensityAdvancedTreatmentDirectiveinterventionwherepeoplewithschizophreniawereencouragedtofillinabookletcontainingsevenpreferencestatements(e.g.‘IfIdoseemtobebecomingillagainIwouldlike…’and‘IfIhavetobeadmittedtohospitalagainIwouldlike…’).Thestudyinvestigatedtheeffectsoftheinterventiononcompulsoryre-admissionratesfor156individualsabouttobedischargedfromtwopsychiatricinpatientunitsinLondon(Papageorgiouetal.2002).Thestudyfoundnosignificantdifferencesinvoluntaryorinvoluntaryreadmissionintheone-yearfollow-upperiod.
Thesecondstudywasasingle-blindRCTmeasuringtheeffectsofajointcrisisplanthatwas‘formulatedbythepatient,carecoordinator,psychiatristandtheprojectworkerandcontainedcontactinformation,detailsofmentalandphysicalillnesses,treatments,indicatorsforrelapse,andadvancestatementsofpreferencesforcareintheeventoffuturerelapse’(Hendersonetal.2004).ThisstudywasalsocarriedoutintheUK.Itfoundthat

31
compulsoryadmissionsweresignificantly(p=0.028)lowerfortheinterventiongroupthanforthecontrolgroup,withariskratioof0.48(95%CI:0.25to0.95).Inotherwords,thestudyestimatedthattheinterventionreducedcompulsoryadmissionsbymorethanonehalf.Aneconomicevaluationofthestudyestimatedthattheservicecostsincurredbytheinterventiongroupwere£121024lower,althoughthisdifferencewasnotstatisticallysignificant(95%CI:-£3109to£5529).Theauthorsconcludedthattherewasagreaterthan78%chancethattheJointCrisisPlansaremorecost-effectivethanstandardserviceinformation(Floodetal.2007).
Jankovic(2010)suggestedtheobserveddifferencesinoutcomesbetweenthesetwostudiescouldbeduetothefactthatPapageorgiuoandcolleagues’studylookedonlyatpeopleabouttobedischargedwhohadbeenundergoingtreatmentundersections2,3or4oftheMentalHealthAct,whereasHendersonandcolleagueslookedatabroadergroupofpeople–anyonewithanoperationaldiagnosisofpsychoticillnessornon-psychoticbipolardisorderwhohadexperiencedhospitaladmissionwithintheprevioustwoyears.Additionally,theinterventionswereverydifferent,onebeingalow-intensitybookletnotsupportedbytheserviceuser’smentalhealthteam,whilsttheotherinterventionfullyinvolvedmanystakeholders.
Thereseemstobesomepositiveevidencethat,aswellasincreasingself-determinationofserviceusers,AdvanceDirectivesmayresultinlowerserviceuseandservicecosts.Moreevidenceis,however,neededbeforeafirmconclusioncouldbedrawnonthisissue.TwostudyprotocolshavebeenidentifieddescribingRCTscurrentlyinprogressexaminingtheeffectsofAdvancedDirectivesonserviceuseandcosts(Thornicroftetal.2010;Ruchlewskaetal.2009).ThesestudiesaretakingplaceintheUKandtheNetherlandsrespectively.TheresultsandanalysisofthesestudieswillhopefullyallowmoreconclusiveinferencestobemadeontheeconomicimplicationsofAdvanceDirectives.
COGNITIVE BEHAVIOUR THERAPY
CognitiveBehaviourTherapy(CBT)isashort-termtalkingtherapytypicallycomprisingofbetweenfiveandtwentyweeklysessionswithhomeworkbetweensessions.Asitsnamewouldsuggest,CBTfocusesonthinkingpatternsandbehaviour,oftenbreakingdownproblemsintosmallcomponentssothatstraightforwardinterventionscanbeidentifiedtoaddresstheseproblems.CBTsessionsoftencompriseofdiscussionswiththetherapistaboutnegativebeliefsandbehaviouralexperimentsinwhichbeliefsaretestedthrough
24. Uprated to reflect current prices using the Pay and Prices Index reported in the PSSRU unit costs volume.
Figure 7: Re-hospitalisation rates with CBT from Jones and colleagues (2012)
Rehospitalisation Pooledsamplesize EstimatedRiskRatio95%Confidence
interval
Shortterm 136 0.36 0.11to1.13
Mediumterm 132 0.59 0.27to1.30
Longterm 294 0.86 0.61to1.20

32
behaviouralchanges.TheelementsofCBTthataredifferentfromotherpsychologicaltherapiesarethehighlystructurednatureofthetherapy,thefocuspredominantlyonthehere-and-nowanditspracticalnature.CBThasbeenshowntobebeneficialinthetreatmentofawiderangeofmentalhealthconditionsincludingdepressionandanxietydisorders.MorerecentlyithasbeenrecognisedthatCBTmayalsobebeneficialforindividualswithschizophreniabyhelpingthemcopewithunhelpfulthoughtsandbehaviours.CBTisformallyrecommendedbyNICEyetinpracticethetherapyisnotavailableinEnglandforthemajorityofpeoplewithschizophrenia.
Byhelpingpeoplewithschizophreniatoaddressnegativethoughtsandbehaviours,CBTmaybehelpfulinreducingrelapsethusreducingserviceusage.Inaddition,CBTmayequipindividualswithcopingmechanismstoreturntoemployment,thusprovidingadditionaleconomicbenefits.
Service UseArecentCochranesystematicreview(Jonesetal.2012)comparedCBTwithotherpsychosocialtreatments(both‘active’and‘non-active’therapies).Ameta-analysisofrelevantstudiesthatmettheinclusioncriteriaestimatedthatCBTreduced(butnotsignificantly)readmissionratesintheshort,mediumandlongrun.AsshowninFigure7,theestimatedeffectsizewasfairlylarge,butresultswerenotstatisticallysignificantduetoalargevarianceandrelativelysmallpooledsamplesize.MoreevidenceisneededbeforeafirmerconclusioncouldbedrawnastohowCBTimpactsonadmissionratesvis-à-visotherpsychologicaltherapies.
However,sincemanypeoplewithschizophreniadonothaveaccesstoanykindofpsychologicaltherapy,thequestionofwhichpsychologicaltherapymaybeseenaslessrelevant.Formentalhealthserviceswhodonot,asyet,offeranyformofpsychologicaltherapy,amorerelevantquestionforeconomicevaluationiswhatarethecostsandbenefitsofofferingCBToranotherpsychologicaltherapyascomparedtoofferingnosuchservice.Anotherpsychologicaltherapythathasbeenevaluated
forpeoplewithschizophreniaiscognitiveremediationtherapy,forwhichthereissomeencouragingevidenceonbotheffectivenessandcost-effectiveness(Wykesetal.2007,Pateletal.2010).Anearlierstudyevaluatedwhatwascalled‘compliance(oradherence)therapy’forpeoplewhowereleavinganinpatientsettingtoreturntothecommunity(Healeyetal.1998).Itfoundcost-effectivenessadvantagesfortheintervention,whichincludedmotivationalinterviewing,butasubsequentmulti-siteEuropeanstudydidnotreplicatethefindingsofeffectivenessorcost-effectiveness(Pateletal.2012).
SimpleeconomicmodellingbyNICEinvolvedameta-analysisoffiveRCTs(themostrecentbeing2003)toobtainarelativeriskratioofhospitalisationof0.74forCBTplusstandardcarecomparedtostandardcarealone(95%CI:0.61to0.94).ThisanalysisestimatedthatafullcourseofCBT,involving16individuallydeliveredsessionswithaclinicalpsychologist,eachofonehourinduration,cost£1184.25However,thereductioninhospitalisationratesimpliedbythemeta-analysisledNICEtoestimateareductioninhospitalisationcostof£2277,resultinginanetsavingduetoCBTof£989.Intheirsensitivityanalysis,varyingrehospitalisationratestotheboundsofthe95%confidenceinterval,theestimatednetcostofprovidingCBTrangedbetween-£1124(anetsaving)and£829.However,morerecentcontrolledtrialssuggestthattheeffectivenessofCBTonreducingrelapseandhospitalisationratesmaybelowerthanthatassumedusedinNICE’smodelling.TheRCTsidentifiedbyarecentreview(Lynchetal.2010)foundnosignificantdifferenceinrelapseratesbetweenCBTandcontrolgroups(Bechdolfetal.2004;Tarrieretal.2004;Valmaggiaetal.2005;Barrowcloughetal.2006;Garetyetal.2008),althoughsomeofthesetrialsweretestinggroupCBTwhichmayaffectfidelityandoutcomes.
OtherstudieshaveattemptedtoanalysethecostimplicationsofCBTdirectlybyrecordingserviceuseandcalculatingassociatedcosts.EconomicoutcomeswererecordedinanRCTofCBTforacuteschizophreniainNorthWales(Startupetal.2005).Positiveclinicaloutcomes
25. This and other costs quoted in this paragraph were uprated to reflect current prices using the Pay and Prices Index in the PSSRU volume.

33
werereported,withtheCBTgroupscoringsignificantlyhigherthanthecontrolgrouponpositivesymptoms,negativesymptomsandsocialfunctionataone-yearfollow-up,andsignificantlyhigheronnegativesymptomsandsocialfunctioningatthetwo-yearfollow-up.(Theyalsoappearedtoscorehigheronpositivesymptomsatthetwo-yearfollow-up,butthedifferencewasnotstatisticallysignificant.)TheeconomicevaluationofthetrialshowedthatthemeancostofprovidingCBTwas£914,26butthiscostwasoffsetbyareductioninserviceuse.Meantotalcostsoverthetwo-yearperiodwereslightlylowerfortheCBTgroupbutthedifferencewasnotsignificant(p=0.94).ThistrialprovidespositiveevidencefortheclaimthatCBTisacost-effectivetreatmentforschizophrenia,providingsuperiorclinicaloutcomesforthesamecost.
AmorerecentRCTinvestigatingcostsassociatedwithCBTintheNetherlands(VanDerGaagetal.2011)foundthatCBTwasassociatedwithbetterclinicaloutcomesthantreatmentasusual(183daysofnormalsocialfunctioningvs.106,p<0.05)buthighercosts:theCBTgrouphadmeantotalcostsof£286027higherthanthecomparisongroupoveran18-monthperiod,althoughthisdifferencewasnotsignificant.Theauthorscalculatedacostof£3928peradditionaldayofnormalfunctioninggained,whichsuggestedthatCBTforschizophreniacouldbeacost-effectiveinterventioninschizophreniaifsocietyiswillingtopaythisprice.
EmploymentIfCBTdoesimproveoutcomesandpreventrelapseinschizophrenia,thismayleadtoincreasesinemployment,inturnleadingtoadditionalbenefits,bothtotheExchequerandtosociety.However,fewstudiescouldbeidentifiedthatincludedemploymentasameasuredoutcome.Gumleyandcolleagues(2003)foundemploymentincreased2.1timesmorefrombaselineintheCBTgroupthaninthetreatmentasnormalgroupbutthiswasnotsignificantatconventionallevels.
Anotherstudy(Lysakeretal.2005)investigatedtheuseof‘enhancedcognitive–behaviouraltherapyforvocationalrehabilitationinschizophrenia.’Fiftyparticipantswereoffered6-monthworkplacements,andwererandomisedtoreceiveeitherstandardvocationalservicesoraprogrammebasedonCBTtechniquestotargetbeliefsthatmightaffectvocationalfunctioning.Resultswereencouraging:comparedtostandardvocationalservicesgroup,theCBTgroupworkedformoreweeks(p=0.02)andmorehours(p=0.06).CautionmustbeexercisedinapplyingtheseconclusionstohowstandardCBTmightaffectemploymentoutcomessincethisCBTprogrammewasdesignedspecificallytohelpitsparticipantsinaworkenvironment,andthereforetheeffectmaybelargerthanformoretypicalCBTcourses.However,thisstudydoessuggestthattheremaybeadditionaleconomicbenefitstoCBT(inadditiontoanyreductioninserviceuse)throughanincreaseinpaidemployment(andthusanincreaseintaxrevenueandareductioninbenefitsdependence).
26. Uprated to reflect current prices. 27. Converted into pounds sterling using PPP exchange rate as reported by OECD iLibrary. 28. Converted into pounds sterling using PPP exchange rate as reported by OECD iLibrary.

34
Inthisreportwehavedescribedboththemaincostsassociatedwithschizophreniaandtheeconomicimplicationsofavarietyofinterventions.Theinterventionsconsideredincludesomethatarecurrentlywidelyusedinpractice,aswellassomethathaveyettobefullyexploredorappliedintheUK,andarenot,generallyspeaking,incorporatedintomainstreamcare,supportandtreatmentarrangements.Inconcludingweofferafewbriefcomments.
CONCLUSIONS
First,wehavefoundmanyareaswhereboththeavailabilityandqualityofeconomicevidencearedisappointing.Thishaslimitedourabilitytosayverymuchaboutthelikelyeconomicconsequencesofsomepromising-lookinginterventions,andinsomeothercasesithasmeantthatwecanonlysetoutsuchconsequencesoverrelativelyshorttimeperiods.Schizophreniaisanillnesswithpotentiallylifelongimplicationsforindividualsandfamilies,anditwouldbehelpfuliftheassociatedeconomicimpactsofboththeillnessandinterventionsthatmightbeaccessedcouldbemorereliablyprojected.
Whatisclearfromtheevidencethatwewereabletocollateinthisreportisthatschizophreniahasverysignificanteconomicconsequencesforsociety.Whilstsomeofthecostsestimatedinpreviousstudiesareunavoidable,giventhenatureofschizophrenia–because,formostpeople,theillnesswillneedtreatmentofsomekindforsomeperiodoftime–thereisneverthelessstrongevidencethatseveralinterventionsthatarenotcurrentlyinwidespreadusecouldreducetheoverallcostofschizophreniawhileimprovehealthandqualityoflifeoutcomesforpeoplewiththeillnessandfortheirfamilies.
Buttherearechallengesingettingtherightresponsestothisevidence.Onechallengeisobviouslythegeneraleconomicclimate,particularlyinviewoftheausteritymeasuresbeingimplementedacrosspublicandnon-publicsectorsalike.Itishardlyagreattimetobeproposingadditionalpublicexpenditureunlesssavingscanbeexpected.Moreover,thosesavingswillneedtobesecuredinrelativelyshorttimescales,whereassomeoftheevidenceinsupportofinterventionsdiscussedinthisreportsuggeststhattheeconomicadvantagesmighttakeanumberofmanyyearstobefullyrealised.
Alinkedchallengeisthatmanyinterventionsrequireexpenditurebyonepartofthepublicsector(andoftenthiswillbetheNHS),whilemanyofthepayoffsintermsofsavings,improvedproductivityandsooncouldwellbeseeninotherpartsofthepublicsectororelsewhere.Oneconsequenceandchallengeislikelytobeaneedfornegotiationtoagreejointcoursesofactionacrossgovernmentdepartments,localcouncilbudgetareasormorewidely.Withoutsuchcoordination,itcouldhardtoaddresswhatareclearlypressingissuesforindividuals,familiesandcommunities.

35
Someinterventionswillnotproducesavingsthataresufficienttocoverthefullcostoftheinitialinvestmentorthecontinuedsupportofindividualswithschizophrenia.Inotherwords,thoseinterventionscouldcostmorethantheysave.Thisisabsolutelynoreasonfornotexploringthoseoptionsfurther,becausethevastmajorityofinterventionsin,forexample,thehealthfieldorthecriminaljusticesystemalsodonotgeneratesavingsthatexceedexpenditures.Thecrucialquestioniswhetherthereturnstothoseexpendituresarejustified,andthatmeansmakingcomparisonsofcostsandoutcomesbetweeninterventions,notjustforpeoplewithschizophreniabutforpeoplewithotherhealthneeds,andindeedincomparisontootherareasofpublicexpenditure.
Thereis,finally,alsothequestionofinequalities,whichwehavebarelytouchedoninthisreport.Becauseofthedevastatingimpactofanillnesslikeschizophrenia,peoplewiththeconditionoftenfindthemselvesinpersonaleconomicdifficulties.Manypeoplewithschizophreniaaresociallyisolatedorinotherwayssociallyaswellaseconomicallyexcluded.Interventionsthathavethepotentialtoimprovetheirqualityoflifeshouldbeconsiderednotjustongroundsofefficiency(i.e.whetherthehealthorqualityoflifegainsjustifythecosts),butalsoonthegroundsofequity.Inotherwords,dothoseinterventionshelptobreakdownotherwiseentrenchedpositionsofsocialexclusion,creatingbetterlifechances?

36
REFERENCES
Accenture(2007)Final Report: Costing of Community Order Requirements,London,UK:NationalAuditOffice.
AdamS,BrewerM,BrowneJ,CroawfordR,EmmersonC,FitzsimonsEetal(2012)IFS Green Budget:February2012.London,UK:InstituteforFiscalStudies.
Allardyce,J.&Os,J.,2010.TheNaturalHistoryoftheCourseandOutcomeofSchizophrenia.Advances in Schizophrenia Research 2009.
Alvarez-JiménezM,ParkerAG,HetrickSE,McGorryPD,GleesonJF(2011)Preventingthesecondepisode:asystematicreviewandmeta-analysisofpsychosocialandpharmacologicaltrialsinfirst-episodepsychosis.Schizophrenia Bulletin,37(3),619–630.
AlwanN,JohnstoneP,ZoleseG(2010) Length of hospitalisation for people with severe mental illness (Review) (11),TheCochraneSchizophreniaGroup,TheCochraneCollaboration.Publishedonline.
AuditCommission(2010)Maximising resources in adult mental health.London,UK:AuditCommission.
BarnettAH,MillarHL,LozeJY,L’ItalienGJ,vanBaardewijkM,KnappM(2009)UKcost-consequenceanalysisofaripiprazoleinschizophrenia:diabetesandcoronaryheartdiseaseriskprojections(STARstudy).European Archives of Psychiatry and Clinical Neuroscience,259(4),239–247.
BarrowcloughC,HaddockG,LobbanF(2006)Groupcognitive–behaviouraltherapyforschizophreniaRandomisedcontrolledtrial.BritishJournal of Psychiatry,189,527-532.
BebbingtonPE,AngermeyerM,AzorinJM,BrughaT,KilianR,JohnsonS,ToumiM,KornfeldA,EuroSCResearchGroup(2005)TheEuropeanSchizophreniaCohort(EuroSC):anaturalisticprognosticandeconomicstudy.Social Psychiatry and Psychiatric Epidemiology,40(9),707–717.
BechdolfA,KnostB,KuntermannC,SchillerS,KlosterkötterJ,HambrechtM,PukropR(2004)Arandomizedcomparisonofgroupcognitivebehaviouraltherapyandgrouppsychoeducationinpatientswithschizophrenia.Acta Psychiatrica Scandinavica,110(1),21-28.
BeckerD,SwansonS,BondG(2008)Evidence-based supported employment fidelity scale.Dartmouth,UK:DartmouthIPSSupportedEmploymentCentre.
BertelsenM,JeppesenP,PetersenL,ThorupA,ØhlenschlaegerJ,leQuachPetal(2008)Five-yearfollow-upofarandomizedmulticentertrialofintensiveearlyinterventionvsstandardtreatmentforpatientswithafirstepisodeofpsychoticillness:theOPUStrial.Archives of General Psychiatry,65(7),762–771.
Burns,T.,Fioritti,A.&Holloway,F.,2001.CasemanagementandassertivecommunitytreatmentinEurope.Psychiatric Services,52(5),pp.631-636
BurnsT,CattyJ,BeckerT,DrakeRE,FiorittiA,KnappMetal(2007)Theeffectivenessofsupportedemploymentforpeoplewithseverementalillness:arandomisedcontrolledtrial.Lancet,370(9593),1146–1152.
BurnsT,CattyJ,WhiteS,BeckerT,KoletsiM,FiorittisAetal(2009)Theimpactofsupportedemploymentandworkingonclinicalandsocialfunctioning:resultsofaninternationalstudyofindividualplacementandsupport.Schizophrenia Bulletin,35(5),pp.949–58.
ButzlaffRL,HooleyJM(1998)Expressedemotionandpsychiatricrelapse;ameta-analysis.Archives of General Psychiatry,55,547–552.
CampbellK,BondGR,DrakeRE(2011)Whobenefitsfromsupportedemployment:ameta-analyticstudy.Schizophrenia Bulletin,37(2),370–80.
CarràG,JohnsonS,BebbingtonP,AngermeyerMC,HeiderD,BrughaTetal(2012)Thelifetimeandpast-yearprevalenceofdualdiagnosisinpeoplewithschizophreniaacrossEurope:findingsfromtheEuropeanSchizophreniaCohort(EuroSC).European Archives of Psychiatry and Clinical Neuroscience.
CarràG,JohnsonS(2009)VariationsinratesofcomorbidsubstanceuseinpsychosisbetweenmentalhealthsettingsandgeographicalareasintheUK:asystematicreview.Social Psychiatry and Psychiatric Epidemiology,44(6),429–447.
ChilversR,MacdonaldG,HayesA(2010)Supported housing for people with severe mental disorders.Devon,UK:CochraneSystematicReview(4):CD000453.

37
ClarkeGN,HerinckxHA,KinneyRF,PaulsonRI,CutlerDL,LewisK,OxmanE(2000)Psychiatrichospitalizations,arrests,emergencyroomvisits,andhomelessnessofclientswithseriousandpersistentmentalillness:findingsfromarandomizedtrialoftwoACTprogramsvs.usualcare. Mental Health Services Research,2(3),155–164.
ClearyM,HuntG,MathesonS,SiegfriedN,WalterG(2010)Psychosocialinterventionsforpeoplewithbothseverementalillnessandsubstancemisuse.Sydney,Australia:CochraneSystematicReview(1):CD001088.
ConnollyM(2005)Lifestyleandphysicalhealthinschizophrenia.Advances in Psychiatric Treatment,11(2),125–132.
CrisisUK(2012)Abouthomelessness:WorkandSkills.Availableat:http://www.crisis.org.uk/pages/work-and-skills.html[AccessedAugust17,2012].
CrowtherR,MarshallM,BondGR,HuxleyP(2010)Vocationalrehabilitationforpeoplewithseverementalillness(Review).http://summaries.cochrane.org/CD003080/vocational-rehabilitation-for-people-with-severe-mental-illness
CurtisL(2011)Unit Costs of Health & Social Care 2011.Kent,UK:PSSRUatUniversityofKent.
DavidsonLarry,ChinmanM,KloosB,WeingartenR,StaynerD,KraemerTebesJ(1999)Peersupportamongindividualswithseverementalillness:areviewoftheevidence.Clinical Psychology: Science and Practice,6(2),165–187.
DavidsonL,ChinmanM,SellsD,RoweM(2006)Peersupportamongadultswithseriousmentalillness:areportfromthefield.Schizophrenia Bulletin,32(3),443–450.
DavidsonL,BellamyC,GuyK,MillerR(2012)Peersupportamongpersonswithseverementalillnesses:areviewofevidenceandexperience.World psychiatry : official journal of the World Psychiatric Association (WPA),11(2),123–128.
DavidsonL(2005)Recovery,selfmanagementandtheexpertpatient:changingthecultureofmentalhealthfromaUKperspective.Journal of Mental Health,14,25–35.
DeeganP,(1996)Recoveryasajourneyoftheheart.Psychiatric Rehabilitation Journal,19(3),91–98.
DepartmentforCommunitiesandLocalGovernment(2012)Evidence review of the costs of homelessness.http://www.communities.gov.uk/publications/housing/costsofhomelessness
DepartmentofHealth(1999)A National Service Framework for Mental Health: Modern Standards and Service Models.http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4009598
DepartmentofHealth(2006)Dual diagnosis in mental health inpatient and day hospital settings.http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_062649
DepartmentofHealth(2001)The Mental Health Policy Implementation Guide.http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4009350
DickeyB,LattimerE,PowersK,GonzalezO,GoldfingerSM(1997)Housingcostsforadultswhoarementallyillandformerlyhomeless.Journal of Mental Health Administration,24(3),291–305.
DoughtyC,TseS(2011)Canconsumer-ledmentalhealthservicesbeequallyeffective?AnintegrativereviewofCLMHservicesinhigh-incomecountries.Community Mental Health Journal,47(3),252–266.
FaulknerG,CohnT,RemingtonG(2007)Interventionstoreduceweightgaininschizophrenia.Toronto,Canada:CochraneDatabaseSystematicReview,(1):CD005148.
FazelS,GulatiG,LinsellL,GeddesJR,GrannM(2009)Schizophreniaandviolence:systematicreviewandmeta-analysis.PLOS Medicine,6(8),p.e1000120.
FazelS,LångströmN,HjernA,GrannM,LichtensteinP(2009)Schizophrenia,substanceabuse,andviolentcrime.Journal of the American Medical Association,301(19),2016–2023.
FloodC,ByfordS,HendersonC,LeeseM,ThornicroftG,SutherbyK,SzmuklerG(2007)Jointcrisisplansforpeoplewithpsychosis:economicevaluationofarandomizedcontrolledtrial.BMC Psychiatry,7(Suppl1),S129.
ForchukC,MartinML,ChanYL,JensenE(2005)Therapeuticrelationships:frompsychiatrichospitaltocommunity.Journal of Psychiatric and Mental Health Nursing,12(5),556–64.

38
GafoorR,NitschD,McCroneP,CraigTK,GaretyPA,PowerP,McGujireP(2010)Effectofearlyinterventionon5-yearoutcomeinnon-affectivepsychosis.British Journal of Psychiatry,196(5),372–376.
GaretyP,FowlerDG,FreemanD,BebbingtonP,DunnG,KuipersE(2008)Cognitive-behaviouraltherapyandfamilyinterventionforrelapsepreventionandsymptomreductioninpsychosis:randomisedcontrolledtrial.British Journal of Psychiatry,192(6),412–423.
GloverG,ArtsG,BabuKS(2006)Crisisresolution/hometreatmentteamsandpsychiatricadmissionratesinEngland.British Journal of Psychiatry,189,441–445.
Goldstein,M.,(1996)PsychoeducationalfamilyprogramsintheUnitedStates.Handbook of Mental Health Economics and Health.
GorczynskiP,FaulknerG(2010)Exercise therapy for schizophrenia.Toronto,Canada:CochraneDatabaseSystematicReview(5):CD004412.
GroveB(1999)MentalHealthandEmployment:Shapinganewagenda.Journal of Mental Health,8(2),131–140.
HESonline(2011)Primary Diagnosis: 3 character table.http://www.hesonline.nhs.uk/Ease/servlet/ContentServer?siteID=1937&categoryID=203
HaddockG(2003)Cognitive-behaviouraltherapyandmotivationalinterventionforschizophreniaandsubstancemisuse:18-monthoutcomesofarandomisedcontrolledtrial.British Journal of Psychiatry,183(5),418–426.
HealthcareCommission(2008)The pathway to recovery: A review of NHS acute inpatient mental health services.
HealeyA,KnappM,AstinJ,BeechamJ,KempR,DavidA,KirovG(1998)Cost-effectivenessevaluationofcompliancetherapyforpeoplewithpsychoses.British Journal of Psychiatry,172,420-424.
HendersonC,FloodC,LeeseM,ThornicroftG,SutherbyK,SzmuklerG(2004)Effectofjointcrisisplansonuseofcompulsorytreatmentinpsychiatry:singleblindrandomisedcontrolledtrial.British Medical Journal,329,136.
HermanD,ConoverS,GorroochurnP,HinterlandK,HoepnerL,SusserE(2011)ARandomizedTrialofCriticalTimeInterventiontoPreventHomelessnessinPersonswithSevereMentalIllnessfollowingInstitutionalDischarge.Psychiatric Services,62(7),713–719.
HermanD,ConoverS,FelixA,NakagawaA,MillsD(2007)CriticalTimeIntervention:anempiricallysupportedmodelforpreventinghomelessnessinhighriskgroups.The Journal of Primary Prevention,28(3-4),295–312.
Heslin,M.etal.,2011.RandomizedcontrolledtrialofsupportedemploymentinEngland:2yearfollow-upoftheSupportedWorkandNeeds(SWAN)study.World psychiatry: official journal of the World Psychiatric Association (WPA),10(2),pp.132–7.
Hippisley-CoxJ,PringleM(2005)ReporttotheDisabilityRightsCommission.Health Inequalities experienced by people with Schizophrenia and Manic Depression: Analysis of general practice data in England and Wales.http://www.leeds.ac.uk/disability-studies/archiveuk/pringle/Qresearch_%20initial_analysis_gen_practice_data.pdf
HomeOffice(2005)Home Office Online Report:The economic and social costs of crime against individuals and households 2003/04.http://webarchive.nationalarchives.gov.uk/20110218135832/rds.homeoffice.gov.uk/rds/pdfs05/rdsolr3005.pdf
IRIS(2011)Joint working at the interface: Early Intervention in Psychosis and specialist Child and Adolescent Mental Health Services. England:SocialCareInstituteforExcellence.www.scie-socialcareonline.org.uk/profile.asp?guid=092fca7f-f50b-428e-a56a-baec510c37c1
JacobsR,BarrenhoE(2011)ImpactofcrisisresolutionandhometreatmentteamsonpsychiatricadmissionsinEngland. British Journal of Psychiatry,199(1),71–76.
JankovicJ,RichardsF,PriebeS(2010)Advancestatementsinadultmentalhealth.Advances in Psychiatric Treatment,16(6),448–455.
JonesC,HackerD,CormacI,MeadenA,IrvingCB(2012)Cognitive behaviour therapy versus other psychosocial treatments for schizophrenia.Birmingham,UK:CochraneDatabaseSystematicReview,(4):CD008712.

39
KhanomH,SameleC,RutherfordM(2009)A Missed Opportunity? Community Sentences and the Mental Health Treatment Requirement.London,UK:SainsburyCentreforMentalHealth.
KilianR,LauberC,KalkanR,DornW,Rössieretal(2012)Therelationshipsbetweenemployment,clinicalstatus,andpsychiatrichospitalisationinpatientswithschizophreniareceivingeitherIPSoraconventionalvocationalrehabilitationprogramme.Social Psychiatry and Psychiatric Epidemiology,47(9),1381–1389.
KillaspyH,KingettS,BebbingtonP,BlizardR,JohnsonS,NolanF,KingM(2009)Randomisedevaluationofassertivecommunitytreatment:3-yearoutcomes.British Journal of Psychiatry,195(1),81–2.
KleinA,CnaanR,WhitecraftJ(1998)Significanceofpeersocialsupportwithduallydiagnosedclients:Findingsfromapilotstudy.Research on Social Work Practice,8(5),529-551.
KnappM(2000)Schizophreniacostsandtreatmentcost-effectiveness.ActaPsichiatricaScandinavica,102(supplement407),15-18.
KnappM,PatelA,CurranC,LatimerE,CattyJ,BeckerTetal(2012)Supportedemployment:cost-effectivenessacrosssixEuropeansites. World Psychiatry,forthcoming.
LamJA,RosenheckR(1999)Streetoutreachforhomelesspersonswithseriousmentalillness:isiteffective?Medical Care,37(9),894–907.
LawnS(2007)SouthernMentalHealthPeerService:Reportonthefirst12months,
LeffJ,SharpleyM,ChisholmD,BellR,GambleC(2001)Trainingcommunitypsychiatricnursesinschizophreniafamilywork:Astudyofclinicalandeconomicoutcomesforpatientsandrelatives.Journal of Mental Health,101(2),189–197.
LehmanAF,DixonLB,KernanE,DeForgeBR,PostradoLT(1997)Randomizedtrialofassertivecommunitytreatmentforhomelesspersonswithseverementalillness.Archives of General Psychiatry,54(11),1038–1043.
LelliottP,AudiniB,KnappM,ChisholmD(1996)Thementalhealthresidentialcarestudy:classificationoffacilitiesanddescriptionofservices. British Journal of Psychiatry,169,2,139-147.
LennonMC,McAllisterW,KuangL,HermanDB(2005)Capturinginterventioneffectsovertime:reanalysisofacriticaltimeinterventionforhomelessmentallyillmen.American Journal of Public Health,95(10),1760–6.
LeuchtS,BurkardT,HendersonJ,MajM,SartoriusN(2007)Physicalillnessandschizophrenia:areviewoftheliterature.Acta Psychiatrica Scandinavica,116(5),317–33.
LibermanR,(1987)Behavioralfamilymanagementofschizophrenia:Clinicaloutcomeandcosts.Psychiatric Annals,17(9),610-619.
LiptonF,NuttS,SabatiniA(1988)Housingthehomelessmentallyill:Alonghitudinalstudyofatreatmentapproach.Hospital & Community Psychiatry,39(1),40–45.
LondonEconomics(2011a)Returns to Intermediate and Low Level Vocational Qualifications.London,UK:LondonEconomics.
LondonEconomics(2011b)Returns to Higher Education Qualifications.London,UK:LondonEconomics.
LynchD,LawsKR,McKennaPJ(2010)Cognitivebehaviouraltherapyformajorpsychiatricdisorder:doesitreallywork?Ameta-analyticalreviewofwell-controlledtrials.Psychological Medicine,40(1),9–24.
LysakerPH,BondG,DavisLW,BrysonGJ,BellMD(2005)Enhancedcognitive-behavioraltherapyforvocationalrehabilitationinschizophrenia:Effectsonhopeandwork.Journal of Rehabilitation Research and Development,42(5),673-682.
MacphersonR(2004)Supportedaccommodationforpeoplewithseverementalillness:areview.Advances in Psychiatric Treatment,10(3),180–188.
MangaloreR,KnappM(2007)CostofschizophreniainEngland.Journal of Mental Health Policy and Economics,10(1),23–41.
MarshallM,RathboneJ(2011)Earlyinterventionforpsychosis.Schizophrenia Bulletin,37(6),1111-1114.
MarshallM,LewisS,LockwoodA,DrakeR,JonesP,CroudaceT(2005)Associationbetweendurationofuntreatedpsychosisandoutcomeincohortsoffirst-episodepatients:asystematicreview.Archives of general psychiatry,62(9),975–83.

40
Marwaha,S.&Johnson,S.,2004.Schizophreniaandemployment-areview.Social psychiatry and psychiatric epidemiology,39(5),pp.337–49.
MarwahaS(2005)Viewsandexperiencesofemploymentamongpeoplewithpsychosis:aqualitativedescriptivestudy.International Journal of Social Psychiatry,51(4),302–316.
McCroneP,MenezesPR,JohnsonS,ScottH,ThornicroftG,MarshallJetal(2000)ServiceuseandcostsofpeoplewithdualdiagnosisinSouthLondon.Acta Psychiatrica Scandinavica,101(6),464–72.
McCroneP,JohnsonS,NolanF,PillingS,SandorA,HoultJetal(2009c)Economicevaluationofacrisisresolutionservice:arandomisedcontrolledtrial.Epidemiologia e psichiatria sociale,18(1),54–8.
McCroneP,JohnsonS,NolanF,SandorA,HoultJ,WhiteIR,BebbingtonP(2009b.)ImpactofacrisisresolutionteamonservicecostsintheUK.Psychiatric Bulletin,33,17–19.
McCroneP,KnappM,DhanasiriS(2009a)Economicimpactofservicesforfirst-episodepsychosis:adecisionmodelapproach.EarlyInterventioninPsychiatry,3(4),266–273.
McCroneP,ParkAL,KnappM(2010)EconomicEvaluation of Early Intervention (EI) Services: Phase IV Report.PSSRUDiscussionPaper2475.London,UK:PSSRU,LondonSchoolofEconomicsandPoliticalScience.
McFarlaneWR,LukensE,LinkB,DushayR,DeakinsSA,NewmarkMetal(1995)Multiple-familygroupsandpsychoeducationinthetreatmentofschizophrenia.Archives of General Psychiatry,52(8),679–687.
McGorryP(2012)Atissue:Cochrane,earlyintervention,andmentalhealthreform:analysis,paralysis,orevidence-informedprogress?Schizophrenia Bulletin,38(2),221–4.
MentalHealthFoundation,2012.Peer Support in mental health and learning disability.London,UK:MentalHealthFoundation.
MentalHealthStrategies(forDepartmentofHealth)(2011)2010/11Working age adult and older adult National Survey of investment in Mental Health Services.London,UK:DepartmentofHealth.
MihalopoulosC,MagnusA,CarterR,VosT(2004)Assessingcost-effectivenessinmentalhealth:familyinterventionsforschizophreniaandrelatedconditions.The Australian and New Zealand Journal of Psychiatry,38(7),511–519.
MinistryofJustice(2011a)2011 Compendium of re-offending statistics and analysis.http://www.justice.gov.uk/statistics/reoffending/compendium-of-reoffending-statistics-and-analysis
MinistryofJustice(2011b)Costs per place and costs per prisoner by individual prison.http://www.justice.gov.uk/downloads/statistics/prison-probation/prison-probation-performance-stats/prison-costs-summary-10-11.pdf
MueserKT,SalyersMP,MueserPR(2001)Aprospectiveanalysisofworkinschizophrenia.Schizophrenia bulletin,27(2),pp.281–96.
NationalAuditOffice(2007)Helping people through mental health crisis: The role of Crisis Resolution and Home Treatment services.London,UK:NationalAuditOffice.
NationalInstituteforHealthandClinicalExcellence(2011)Psychosis with coexisting Substance Misuse: The NICE guideline on assessment and management in adults and young people.
NationalInstituteforHealthandClinicalExcellence(2009) Schizophrenia: Core interventions in the treatment and management of schizophrenia in adults in primary and secondary care.NICEclinicalguideline82.
Papageorgiou,A,KingM,JanmohamedA,DavidsonO,DawsonJ(2002)Advancedirectivesforpatientscompulsorilyadmittedtohospitalwithseriousmentalillness:Randomisedcontrolledtrial.British Journal of Psychiatry,181(6),513–519.
PatelA,KnappM,WykesT,ReederC,RomeoR(2010)Cognitiveremediationtherapyinschizophrenia:cost-effectivenessanalysis.Schizophrenia Research,120,217-224.
PatelA,McCroneP,KnappM,LeeseM,AmaddeoF,TansellaM,KilianR,AngermeyerM,KikkertM,ScheneA(2012)Economicevaluationofadherencetherapycomparedtoahealtheducationinterventionforpeoplewithschizophrenia.Submitted.PatelA.(2012)paperunderreview.

41
PharoahF,MariJ,RathboneJ,WongW(2010)Family intervention for schizophrenia (Review).London,UK:TheCochraneCollaboration,Wiley.
PhillipsonA,AkroydM,Carley,J(2012)An audit of discharges from a regional service in the United Kingdom.Manuscriptsubmittedforpublication
President’s New Freedom Commission on Mental Health (2003).USA:MentalHealthCommission.
PriebeS,SaidiM,WantA,MangaloreM,KnappM(2009)HousingservicesforpeoplewithmentaldisordersinEngland:Patientcharacteristics,careprovisionandcosts,Social Psychiatry and Psychiatric Epidemiology,44,805-814.
Repper,J.&Carter,T.,2011.Areviewoftheliteratureonpeersupportinmentalhealthservices.Journal of mental health (Abingdon, England),20(4),pp.392–411.
RiveraJJ,SullivanAM,ValentiSS(2007)Adding consumer-providers to intensive case management: does it improve outcome? Psychiatric Services,58(6),802–9.
RosenheckR(2000)Cost-effectivenessofservicesformentallyillhomelesspeople:theapplicationofresearchtopolicyandpractice.American Journal of Psychiatry,157(10),1563–70.
RosenheckR,GallupP,FrismanL(1993)Healthcareutilizationandcostsafterentryintoanoutreachprogramforhomelessmentallyillveterans.Hospital Community Psychiatry,44(12),1166–71.
RowlandsP(2012)Personal communication.
RuchlewskaA,MulderCL,SmuldersR,RoosenschoonBJ,KoopmansG,WierdsmaA(2009)Theeffectsofcrisisplansforpatientswithpsychoticandbipolardisorders:arandomisedcontrolledtrial.BMC Psychiatry,9,41.
RutherfordM,DugganS(2007)Forensic Mental Health Services: Facts and figures on current provision.London,UK:SainsburyCentreforMentalHealth.
SahaS,ChantD,WelhamJ,McGrathJ(2005)A systematic review of the prevalence of schizophrenia. PLoS Medicine,2(5),p.e141.http://www.plosmedicine.org/article/info%3Adoi%2F10.1371%2Fjournal.pmed.0020141
SahaS,ChantD,McgrathJ(2007)Asystematicreviewofmortalityinschizophrenia.Archives of General Psychiatry,64(10),1123–1131.
SainsburyCentreforMentalHealth(2004)Benefits and work for people with mental health problems : A briefing for mental health workers.London,UK:SainsburyCentreforMentalHealth.
SainsburyCentreforMentalHealth,2009.Briefing 41: Commissioning what works, the economic and financial case for supported employment.London,UK:SainsburyCentreforMentalHealth.
SchmidtLT,KJGill,WilsonPrattC,SolomonP(2008)Comparisonofserviceoutcomesofcasemanagementteamswithandwithoutaconsumerprovider.American Journal of Psychiatric Rehabilitation,11(4),310–329.
SeymourL,RutherfordM(2008)The Community Order and the Mental Health Treatment Requirement.London,UK:SainsburyCentreforMentalHealth.
ShernDL,TsemberisS,AnthonyW,LovellAM,RichmondL,FeltonCJetal(2000)Servingstreet-dwellingindividualswithpsychiatricdisabilities:outcomesofapsychiatricrehabilitationclinicaltrial.American Journal of Public Health,90(12),1873–8.
ShiersD,SmithJ(2010)Early intervention in psychosis: a briefing for service planners.London,UK:NationalMentalHealthDevelopmentUnit.
SimpsonEL,HouseAO(2002)Involvingusersinthedeliveryandevaluationofmentalhealthservices:systematicreview.British Medical Journal,325(November),1–5.
SingletonN,BumpsteadR,O’BrienM,LeeA,MeltzerH(2000)Psychiatricmorbidityamongadultslivinginprivatehouseholds,2000.International Review of Psychiatry,15(1-2),65–73.
SingletonN,MeltzerH,GatwardR,CoidJ,DeasyD(1998)Psychiatric morbidity among prisoners : Summary report.London,UK:OfficeofNationalStatistics.
SladeEP,McCarthyJF,ValensteinM,VisnicS,DixonLB(2012)Costsavingsfromassertivecommunitytreatmentservicesinaneraofdecliningpsychiatricinpatientuse. Health Services Research,1–23.

42
SolomonE,SilvestriA(2008)Community Sentences Digest.London,UK:CentreforCrimeandJusticeStudies.
SolomonP,DraineJ(1995)Theefficacyofaconsumercasemanagementteam:2-yearoutcomesofarandomizedtrial.Journal of Mental Health Administration,22(2),135–46.
SolomonP(2004)Peersupport/peerprovidedservicesunderlyingprocesses,benefits,andcriticalingredients.Psychiatric Rehabilitation Journal,27(4),392–402.
StansburyA.PhakeyA(2011)Tackling Homelessness.Cambridge:TheWilberforceSociety.http://thewilberforcesociety.co.uk/policy_paper/tackling-homelessness/
StartupM,JacksonMC,EvansKE,BendixS(2005)NorthWalesrandomizedcontrolledtrialofcognitivebehaviourtherapyforacuteschizophreniaspectrumdisorders:two-yearfollow-upandeconomicevaluation.Psychological Medicine,35(9),1307–16.
SusserE,ValenciaE,ConoverS,FelixA,TsaiWY,WyattRJ(1997)Preventingrecurrenthomelessnessamongmentallyillmen:A‘criticaltime’interventionafterdischargefromashelter.87(2),256–262.
TarrierN,LewisS,HaddockG,BentallR,DrakeR,KindermanPetal(2004)Cognitive-behaviouraltherapyinfirst-episodeandearlyschizophrenia18-monthfollow-upofarandomisedcontrolledtrial.British Journal of Psychiatry,184,231-239.
TarrierN,LowsonK,BarrowcloughC(1991)Someaspectsoffamilyinterventionsinschizophrenia.II:Financialconsiderations.British Journal of Psychiatry,159(4),481–484.
ThornicroftG,FarrellyS,BirchwoodM,MarshallM,SzmuklerG,WaheedWetal(2010)CRIMSON[CRisisplanIMpact:SubjectiveandObjectivecoercionandeNgagement]protocol:arandomisedcontrolledtrialofjointcrisisplanstoreducecompulsorytreatmentofpeoplewithpsychosis.Trials,5(11),102.
TsoiD,PorwalM,WebsterA (2010) Interventions for smoking cessation and reduction in individuals with schizophrenia (Review).London,UK:TheCochraneCollaboration,Wiley.
TurkingtonA,MulhollandC,RusheT,AndersonR,McCaulR,BarrettSetal(2009)Impactofpersistentsubstancemisuseon1-yearoutcomeinfirst-episodepsychosis.British Journal of Psychiatry,195,242–8.
ValmaggiaL,vanderGaagMVD,TarrierN,PijnenborgM,SlooffCJ(2005)Cognitive–behaviouraltherapyforrefractorypsychoticsymptomsofschizophreniaresistanttoatypicalantipsychoticmedicationRandomisedcontrolledtrial.British Journal of Psychiatry,186,324-330.
VanderGaagM,StantAD,WoltersKJ,BuskensE,WiersmaD(2011)Cognitive-behaviouraltherapyforpersistentandrecurrentpsychosisinpeoplewithschizophrenia-spectrumdisorder:cost-effectivenessanalysis.British Journal of Psychiatry,198(1),59–65,sup1.
WilliamsA(2011)Valuing peer support: A review of literature on peer support in helping people with mental health issues towards personal recovery.Kent:KentandMedwayNHSSocialCare.http://www.kmpt.nhs.uk/Downloads/Getting-involved/Valuing-Peer-support.pdf
WinterbourneS(2012)Preventing future physical morbidity and premature mortality in first-episode psychosis patients: an economic evaluation of smoking cessation interventions. MSc Thesis.London,UK:LondonSchoolofEconomicsandPoliticalScience.
WolffN,HelminiakTW,MorseGA,CalsynRJ,LinkenbergWD,TrustyML(1997)Cost-effectivenessevaluationofthreeapproachestocasemanagementforhomelessmentallyillclients.American Journal of Psychiatry,154(3),341–348.
Wright-BerrymanJ,McGuireA,SalyersM(2011)Areviewofconsumer-providedservicesonAssertiveCommunityTreatmentandintensivecasemanagementteams:Implicationsforfutureresearchandpractice.Journal of the American Psychiatric Nurses Association,17(1),37–44.
WykesT,ReederC,LandauS,EverittB,KnappM,RomeoR,PatelA(2007)Arandomisedcontrolledtrialofcognitiveremediationtherapyinpatientswithschizophrenia.British Journal of Psychiatry,190,421-427.

43

44
The authors can be contacted through: Personal Social Services Research UnitLondon School of Economics and Political ScienceHoughton StreetLondon, WC2A 2AE Email: [email protected]: +44 (0)20 7955 6238Fax: +44 (0)20 7955 6131Twitter: @PSSRU_LSEwww.pssru.ac.uk
To read more about the work of the Schizophrenia Commission, go to www.schizophreniacommission.org.uk
This report should be referenced as: Andrews A, Knapp M, McCrone P, Parsonage M, Trachtenberg M (2012) Effective interventions in schizophrenia the economic case: A report prepared for the Schizophrenia Commission. London: Rethink Mental Illness.
The Schizophrenia Commission is an independent group set up and funded by Rethink Mental Illness (Registered charity number 271028).
For further information on Rethink Mental Illness telephone: 0300 5000 927, email: [email protected], website: www.rethink.org