Embed Size (px)
DESCRIPTION
Review of clinical anatomy & physiology of the eyelids & common infective and inflammatory disorders of the eyelids. Dr. Ayesha S Abdullah 10.09.2012. Learning objectives. By the end of this lecture the students would be able to:- - PowerPoint PPT Presentation
Citation preview

Review of clinical anatomy & physiology of the eyelids & common infective and inflammatory
disorders of the eyelids
Dr. Ayesha S Abdullah10.09.2012

Learning objectives
By the end of this lecture the students would be able to:-
• Correlate the structure of the eyelids with their functions and clinical presentation in common infective and inflammatory disorders.
• Define stye, chalazion, trichiasis & blepharitis.• Differentiate between stye & chalazion on the
basis of clinical presentation and describe the treatment.

Important superficial anatomical landmarks
Lid margin
Upper lid creasePalpebral fissure height (max)
Palpebral fissure length (max)

Structure of the lids
The eyelid has five layers of different structures 1. Skin2. Subcutaneous tissue3. Muscular layer4. Tarsal plate5. Conjunctiva

Surgical anatomy
Anterior Lamina Skin Orbicularis muscle
Posterior Lamina Tarsal plate Conjunctiva



Anterior lamina Muscular layer
Orbital part
Preseptal part
Pretarsal part
Palp
ebra
l Pa
rt

Posterior lamina

Orbital Septum



Structures at the lid margin



Functions
• Protect the anterior surface of the globe • Aid in regulation of light reaching the eye• Tear film maintenance; distribution & flow• Lipid/ oily layer of the tear film

Disorders of eyelids
• Infective• Inflammatory• Neoplastic• Structural / disorders of malposition

Trichiasis
• In-turned eyelashes

Complications

Treatment
• Epilation - but recurrences within few weeks• Electrolysis - but frequently repeated
treatments• Cryotherapy - for many lashes• Laser ablation - for few scattered lashes• Surgical correction - for resistant, localized
crop• Ocular lubricants

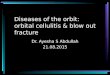
Blepharitis • “ inflammation of the lid margin”• Anterior Blepharitis– Affects base of eyelashes– Associated with staphylococcal infection or Seborrhea– Complicated by recurrent stye ,scarring of the lid margin and
loss of eyelashes• Posterior Blepharitis– Affects meibomian gland openings– Associated with meibomian gland dysfunction– Complicated by recurrent chalazia, tear film instability and
scarring of the lid margin

Anterior Blepharitis
Posterior Blepharitis

Management– Maintain lid hygiene• Apply warm compress • Gently massage posterior lid to express meibomian gland
contents• Scrub lashes and lid margins with dilute baby shampoo• Wipe lid margins with warm cloth after scrubbing
– Acute infectious flare-up (e.g. staphylococcal Blepharitis)• Antibiotic ophthalmic ointment
– Meibomian gland dysfunction• Ocular lubricants ( artificial tears/ tear substitutes) • Tetracycline / Doxycycline orally • Steriods for limited period

Stye
“ Acute staphylococcal infection (abscess) of a lash follicle”
• Common in children• Tender hot swelling at the lid margin• May spread to the entire lid causing prespetal
or at time orbital cellulitis



Treatment
• Hot compresses• Self-limiting; epilation of the infected lash
hastens resolution• If spread of infection is likely with gross
redness and swelling of the lid than topical and systemic antibiotics can be given along with analgesics/ NSAIDs

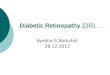
Chalazion
“Chronic granulomatous inflammation of the Meibomian glands secondary to blockage of the gland orifice”.
• Common in patients with posterior blepharitis• Non-tender swelling a little away from the lid
margin


Treatment
• Small – no treatment• Incision and curretage of the affected gland.

Summary
• Important anatomical landmarks• Trichiasis• Blepharitis• Stye• Chalazion