Embed Size (px)
Citation preview

PRESENTATION OF IMMUNOLOGYPRESENTED TO:- DR.SHAHEEN SHEHZAD
PRESENTED BY: GROUP 5 MAHNOOR KHALIL NIDA-TUL-AIN MARYAM NISAR AYESHA MUJAHID MARZIA SAFDAR AYESHA SARDAR

AUTOIMMUNE DISEASE:
Arises from abnormal immune response of the bodyMay be restricted to certain organs eg AUTOIMMUNE THYROIDITIDSMay involve a particular tissue which may affect the basement membrane in both lungs and kidney. eg good Pasteur’s disease

CRITERIA:-
For a disease to be recognized as an autoimmune disease it must answer WITEBSKY’S POSTULATES (formulated by ERNST WITEBSKY & COLLEAGUES IN 1957 AND MODIFIED IN 1994).

POSTULATES:-Indirect evidence based on reproduction of autoimmune disease in experimental animals.Direct evidence from transfer of pathogenic antibodies or pathogenic T-cellCircumstanicial evidences from clinical clues.Genetic architechture clustering with other autoimmune disease

What is IgA Nephropathy??

DEFINITION:-
Primary IgA Nephropathy is characterized by the deposition of IgA antibody in the glomerulus, i.e it is a kidney disease that occurs when IgA (immunoglobulin A) lodges in your kidney. This results in local inflamation that, over time, may hampers kidneys ability to filter waste, excess water and electrolytes from blood.

ALSO CALLED AS:-Berger’s disease
IgA nephritis
IgAN
Berger’s syndrome
Synpharyngitic glomerulonephritis

HISTORY:-Immunoglobulin A (IgA)
nephropathy was first described by the
pathologist JEAN BERGER and thus is called
BERGER’S DISEASE.
JEAN BERGER published his description of glomerulo-nephritis with mesangial IgA deposition in winter 1968.

EPIDEMIOLOGYOccur in any age but more common in children and young adultMale>female (2 folds)Genetic predisposition: IGAN1, on 6q22-q23 Susceptibility to IgA
nephropathy has been associated with single nucleotide polymorphisms (SNPs) in the E-selectin and L-selectin genes as well as in polymeric immunoglobulin receptor gene (PIGR) .

IgA nephropathy is a
frequent cause of recurrent gross or
microscopic HEMATURIA and is
probably most common type of
GLOMERULONEPHRI
TIS worldwide

IgA NEPHROPATHY•It is typically an isolated renal disease •IgA deposits are present in systemic disorder of children, HENOCH-SCHONLEIN purpura which hasmany overlapping features with IgA nephropathy
•Secondary IgA nephropathy occurs in patients with liver and intestinal diseases.

Signs and Symptoms of IgA Nephropathy

of IgA Nephropathy

Early stages of disease
IgA nephropathy usually doesn't cause symptoms in the early stages. The disease can go unnoticed for decades and is sometimes first suspected when routine tests reveal protein and red blood cells in your urine that can't be seen without a microscope (microscopic hematuria).

Signs and symptoms of IgA nephropathy when kidney function is impaired include:Cola- or tea-colored urine
(caused by red blood cells in the urine)Repeated episodes of cola- or tea-colored urine, sometimes even visible blood in your urine, usually during or after an upper respiratory or other type of infectionPain in the side(s) of your back below your ribs (flank)Foam in the toilet water from protein in your urineSwelling (edema) in your hands and feetHigh blood pressure

Pain in the side(s) of your back below your ribs (flank)Foam in the toilet water from protein in your urineSwelling (edema) in your hands and feetHigh blood pressure

When to see a doctor :
Make an appointment with your doctor if you notice blood in your urine. Urinary bleeding may be
caused by strenuous exercise, some foods, medications or a urinary tract infection. But prolonged or repeated
bleeding may indicate a serious medical problem and should always be evaluated. Also see your doctor if your urine is foamy or if you develop sudden swelling in your hands and
feet.

DIAGNOSIS OF IGA NEPHROPATHYIgA nephropathy is often detected after we notice blood
in our urine or when a routine test shows we have protein(proteinuria) or blood(microhematuria) in our urine. These could be signs of several types of kidney disease. To identify problem, these tests may be performed:
URINE TEST: Blood or protein in the urine may be the first sign of IgA nephropathy. This may be discovered as part of a routine checkup. If doctor suspects that you have problems with your kidneys, you may need to collect your urine for a 24-hour period for additional kidney function tests.

BLOOD TEST: If you have kidney disease, such as IgA nephropathy, a blood test may show increased blood levels of the waste product creatinine. Based on a 24-hour urinalysis, this test ascertains how well kidneys are performing their vital task of clearing creatinine, the end product of muscle metabolism, from the blood. The results show the kidneys’ glomerular

This test is not diagnostic of a particular disease but, rather, of the severity of the inflammation and, possibly, the extend of damage to the kidneys. Your kidneys ordinarily filter about five ounces of blood each minute, but in IgA Nephropathy, the filtration rate may decline because infiltration of the glomerular capillaries by inflammatory cells reduces the amount of surface area available for filtering work.Blood and urine testing and the absence of certain hallmarks of other kidney diseases, such as azotemia [excessive nitrogen in the blood] and pronounced edema [swelling of tissues from retained fluid], may suggest IgA Nephropathy, but only a biopsy can confirm it.

KIDNEY BIOPSY:
The only way for your doctor to confirm a diagnosis of IgA nephropathy is with a kidney biopsy. This procedure involves using a special biopsy needle to extract small pieces of kidney tissue for microscopic examination to determine if there are IgA deposits in the glomeruli.

RENAL IMAGING: It is a diagnostic procedure that uses gamma rays to examine the anatomy and functioning of kidneys. During this procedure, radioisotope releases gamma rays, which a gamma camera or scanner can detect from outside the body. The gamma camera scans the kidney area. The camera also works together with the computer to create images. These images detail the structure and functioning of kidneys. Images from a renal scan can show structural and functional abnormalities, helping doctors to diagnose a kidney problem.

Complications of IgA !!

The course of IgA nephropathy varies from person to person. Some people have the disease for years with few problems. In fact, many cases may go undiagnosed. Other people develop one or more of the following complications:
•High blood pressure. Damage to your kidneys from IgA deposits can raise your blood pressure, and high blood pressure can cause further damage to your kidneys.
•High cholesterol. High levels of cholesterol may increase your risk of a heart attack.

•Acute kidney failure: If your kidneys lose their filtering ability due to IgA deposits, waste products build up quickly in your blood.
•Chronic kidney failure: IgA nephropathy can cause your kidneys to gradually stop functioning. In such cases, permanent dialysis or a kidney transplant is needed to sustain life.
•Nephritic syndrome:This is a group of problems that can be caused by damage to the glomeruli, including high urine protein levels, low blood protein levels, high cholesterol and lipids, and swelling of your eyelids, feet and abdomen.
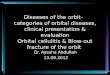
Normal kidney
Acute kidney
Chronic kidney

Researchers don't know exactly what causes IgA deposits in the kidneys, but these conditions or factors may be associated with the development of IgA nephropathy:
•Genes, because IgA nephropathy is more common in some families and in certain ethnic groups
•Liver diseases, including cirrhosis, a condition in which scar tissue replaces normal tissue within the liver, and chronic hepatitis B and C infection.
•Celiac disease, a digestive condition triggered by eating gluten, a protein found in most grains
•Dermatitis herpetiformis, an itchy, blistering skin disease that stems from gluten intolerance
• Infections, including HIV infection and some bacterial infections

THERAPY:-

IgA nephropathy is a common cause of glomerulonephritis.
Although it is a benign disease in most patients, chronic kidney disease and end-stage renal
disease (ESRD) occur in about 20-40% of patients within 20 years of presentation. Currently, no cure exists for IgA nephropathy, but
therapies that can delay the onset of need for dialysis and
transplantation are available. Current recommendations include
the following:

Monitor patients with isolated hematuria without proteinuria or hypertension with urinalysis, renal
function testing, and blood pressure measurement.Treat hypertension early and aggressively. A reasonable goal is to aim for a blood pressure of 125/75–130/80 mm
Hg.Angiotensin-converting enzyme inhibitors (ACEIs) are the preferred agents for lowering blood pressure. They are
beneficial in decreasing proteinuria and should be strongly considered even in normotensive patients with proteinuria.The decrease in proteinuria with ACEIs may be an effect of decreasing the intraglomerular pressure
and of changing the glomerular size selectivity.Reports have demonstrated that ACEIs are more effective
than other antihypertensive drugs in slowing the progression of proteinuric renal disease.

The goal for proteinuria control is 500 mg/day or less, so ACEIs should be started in patients with 24-hour urine
protein of 500 mg or more.[7]
In a randomized, controlled trial that followed patients for a mean of approximately 6 years, the group that received ACEIs had an improved renal survival rate compared with
the group receiving other antihypertensive agents.Angiotensin II receptor blockers (ARBs) should be used for patients who cannot tolerate ACEIs. ACEIs and ARBs may
have an additive effect in decreasing proteinuria. Whether high-dose ACEIs better preserve renal function than
combination therapy with ACEIs and ARBs is unknown.The combination of an ACEI and the ARB losartan has
shown an additive urinary protein–lowering effect compared with doubling the dose of monotherapy.
However, patients on combination therapy should be monitored closely for the development of hyperkalemia, and combination therapy should be avoided in patients
with advanced kidney disease.

Administer prednisone for 4-6 months to patients who have IgA nephropathy with preserved renal
function, nephrotic syndrome, and minimal-change findings on light microscopy.
Early treatment with prednisone in patients with proliferative IgA nephropathy has been shown to
be effective in reducing proteinuria and improving histologic findings, such as proliferation and
cellular crescents. Additionally, corticosteroids given for 6 months have been seen to be
beneficial against deterioration in renal function in patients with moderate proteinuria (1.5-3.5 g/d).Results of a prospective, open-label, multicenter,
centrally randomized, controlled trial in 97 patients suggested that the combination of the ACEI ramipril and prednisone was more effective
than ramipril alone in discouraging progression of renal disease associated with IgA nephropathy.

A randomized, controlled, long-term study on the effectiveness of steroids in IgA nephropathy showed
improved 10-year renal survival in the steroid-treated group compared with the control group. Patients had a
proteinuria of 1.9 g/d on average in the treatment group and 1.7 g/d in the control group. Steroids were given for 6
months.Mycophenolate mofetil has been used in patients with IgA
nephropathy associated with proteinuria, even though some reports have shown some benefit and others have
not. The studies are of small size, and longer-term studies are required for more information. At this time, the
evidence for the use of mycophenolate in IgA nephropathy is inconclusive.
Patients with crescentic rapidly progressive glomerulonephritis (RPGN) can be treated similarly to
patients with idiopathic RPGN by using intravenous pulse prednisone followed by oral prednisone and
cyclophosphamide.

Fish oil (omega-3 fatty acids) at a dose of 12 g/d has been used with controversial and conflicting results, but it is
frequently used in patients with declining renal function. Deficiencies of essential fatty acids have been detected in IgA nephropathy, and fish oil is rich in long-chain omega-3
polyunsaturated fatty acids. These produce altered and less biologically effective prostaglandins and
leukotrienes, as well as reduced platelet aggregation.A study by Liu examined the effect of calcitriol on urinary protein excretion among patients with IgA nephropathy.
The study found that adding calcitriol to a renin-angiotensin system inhibitor resulted in a safe decrease
in proteinuria.