Embed Size (px)
Citation preview
CHEMICAL INJURIES OF THE EYE Ayesha S Abdullah
07.04.2015
Learning outcomes
By the end of this lecture the students would be able to Describe the epidemiology of chemical ocular injuries Correlate the pathophysiology of chemical injury with
acids and alkali to the clinical presentation & complications
explain the first aid measure and later management of a case with chemical injury.
Identify the complications of chemical injury and correlate it with the underlying pathology, suggest ways for the primary, secondary and tertiary prevention of such injuries
Case
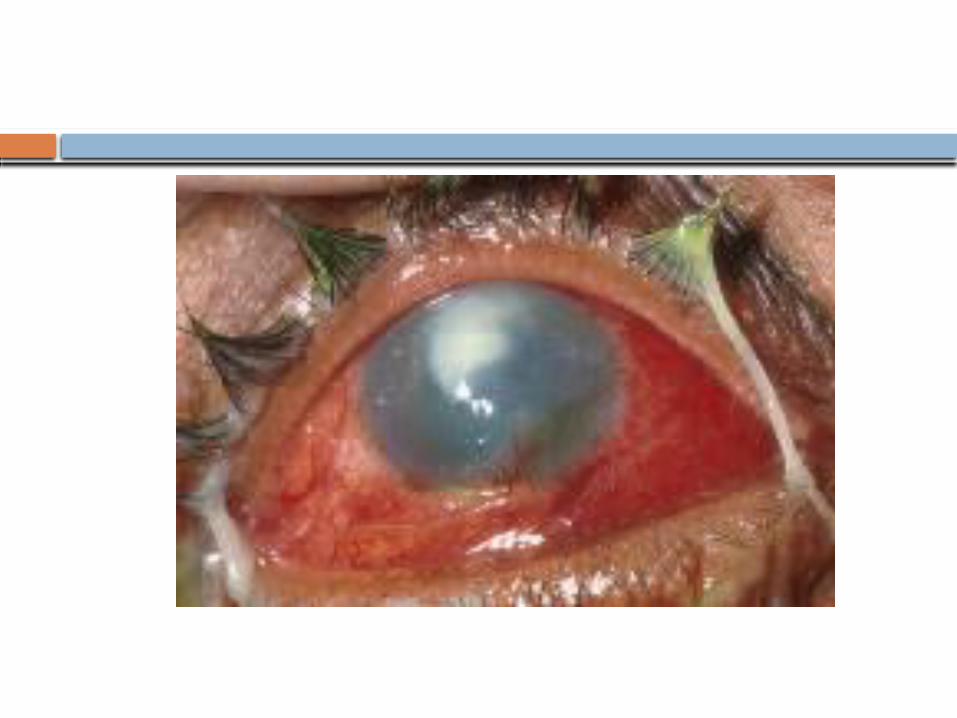
Gul Nawaz aged 35 years presented to emergency deparment with injury to the right eye while working in a cement factory. He had severe ocular irritation with watering, pain and photophobia.
The eye was extensively washed till the normal pH was restored
On examination VA OD=CF 1 m, OS=6/5 He had red eye with corneal haze There was limbal ischemia affecting less than 1/3rd
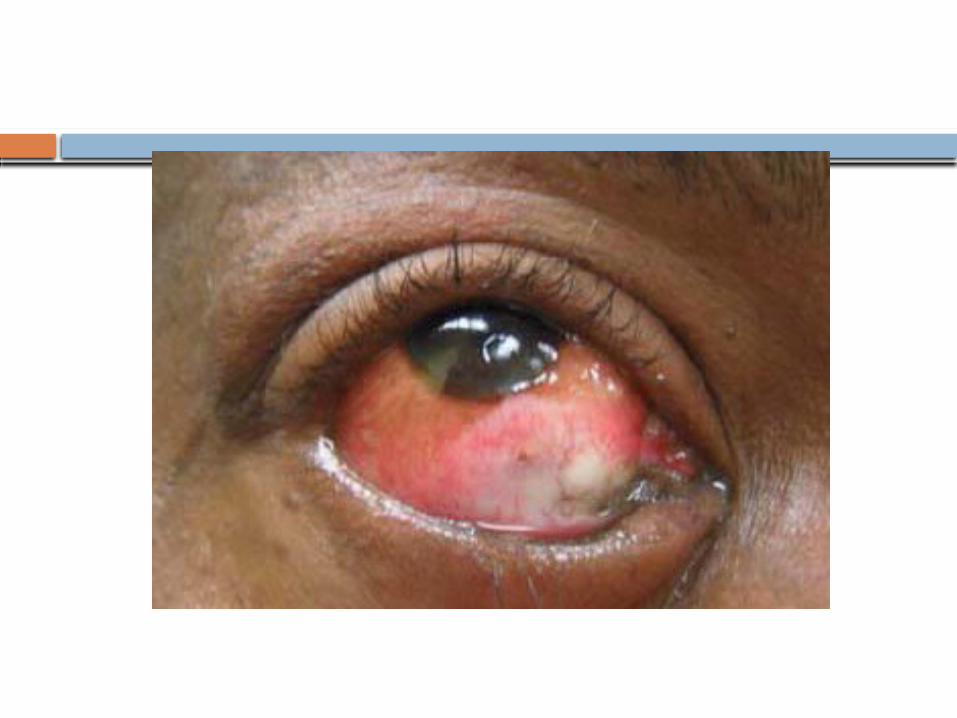
of the limbus (3 clock hours) The IOP was 24 mmHg OD, 11 mmHg OS Examine the given photograph
Questions
What kind of injury is this? Acidic/ alkaline- would it make any difference? Why was the eye washed first? What is limbal ischemia and what is its
significance in this patient? Why was the IOP raised? Why such an extensive damage? What would be the prognosis of this kind of
injury? What complications can happen? How can chemical injuries be prevented?
Epidemiology
Why should you know this? About 2/3rd of the chemical injuries happen at
workplace the rest at home Almost any chemical can cause ocular irritation Serious damage however happen with acids and
alkalis Alkali injuries are more common because they
are used more frequently Bilateral chemical exposure could be extremely
damaging resulting in blindness and disfigurement
Calcium hydroxide is the most common cause of alkali ocular burns, ammonia tends to cause the most serious burns
Sulfuric acid is the most common acidic caustic agent but hydrofluoric acid causes the most devastating injury
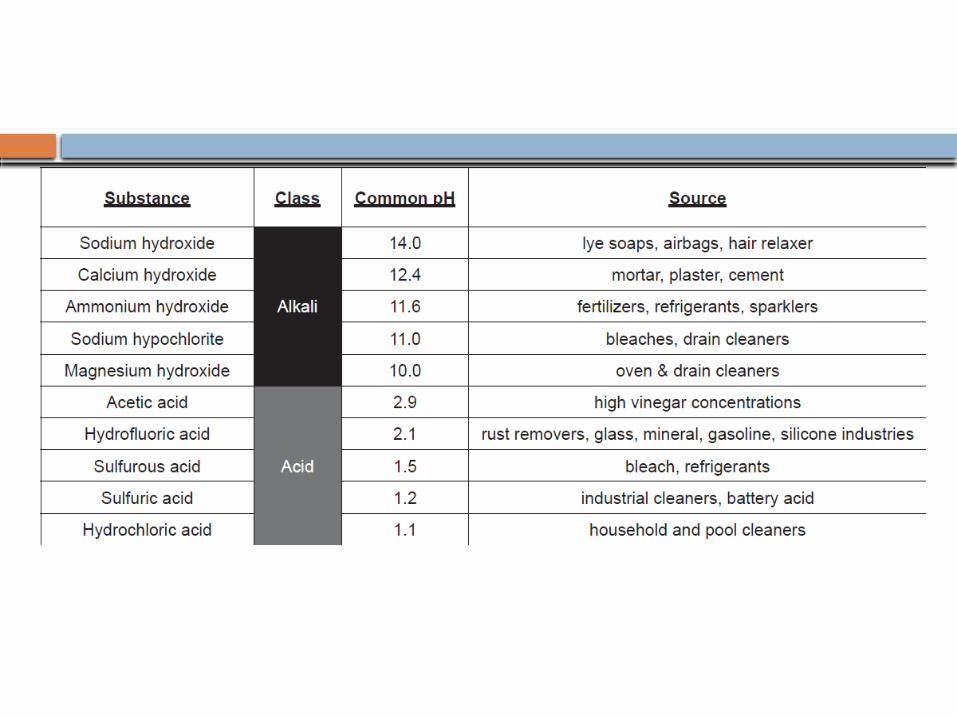
Sources
Common sources of alkali are Cleaning products (eg, ammonia) Fertilizers (eg, ammonia) Drain cleaners (e.g, lye) Cement, plaster, mortar (e.g, lime) Airbag (automobile) rupture (e.g, sodium
hydroxide) Fireworks (eg, magnesium hydroxide) Potash (eg, potassium hydroxide)
Commonest alkalis causing chemical injury are ammonia, sodium hydroxide & lime
Sources
Common sources of acids are as follows: Battery acid (eg, sulfuric acid) Bleach (eg, sulfurous acid) Glass polish (eg, hydrofluoric; behaves like an alkali) Vinegar (eg, acetic acid) Chromic acid (brown discoloration of conjunctiva) Nitric acid (yellow discoloration of conjunctiva) Hydrochloric acid
Commonest acids are sulphuric, sulphurous, hydrofluoric, acetic , chromic and hydrochloric acid.
Pathophysiology
Severity depends upon The nature/ properties & concentration of
the chemical Area of the affected surface Length of exposure Associated damage e.g. thermal /electrical/
explosive
Pathophysiology
Alakli burns are more damaging than acid burns because it penetrates deeper1
Necrosis and shedding of the corneal and conjunctival epithelium
Damage to the limbal vasculature Limbal ischemia Persistent corneal epithelial defects Conjunctivaliztion & vascularization of the cornea Corneal ulceration and perforation Conjunctival and adnexal scarring
Corneal healing
Loss of epithelium Migration of cell derived from the limbal
stem cells Phagocytosis of the necrosed collagen
by the keratocytes and new collagen is laid down
Clinical presentation
History Ascertain the nature of the chemical and
mode of injury Complaints are
Pain (often extreme) Foreign body sensation Blurred vision Excessive tearing Photophobia Red eye(s)
Physical examination
Physical examination: General and Ocular A thorough physical examination should be deferred
until the affected eye is irrigated copiously, and the pH of the ocular surface is neutralized.
After irrigation, a thorough eye examination is performed focusing on 1. clarity and integrity of the cornea2. degree of limbal ischemia3. Anterior chamber reaction4. Signs of deeper penetration of the chemical5. IOP.
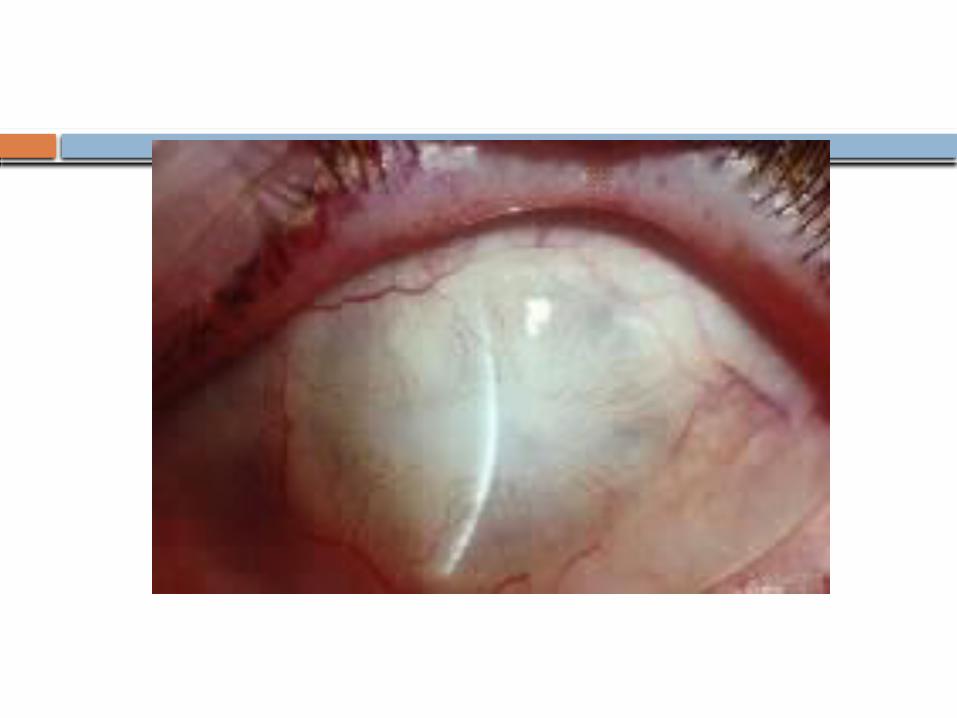
Signs
Conjunctival inflammation: Particles in the conjunctival fornices. Perilimbal ischemia (LI-blanching) The most
significant prognostic indicator for corneal healing. Greater the extent of blanching, the worse the prognosis. LI is documented as number of clock hours
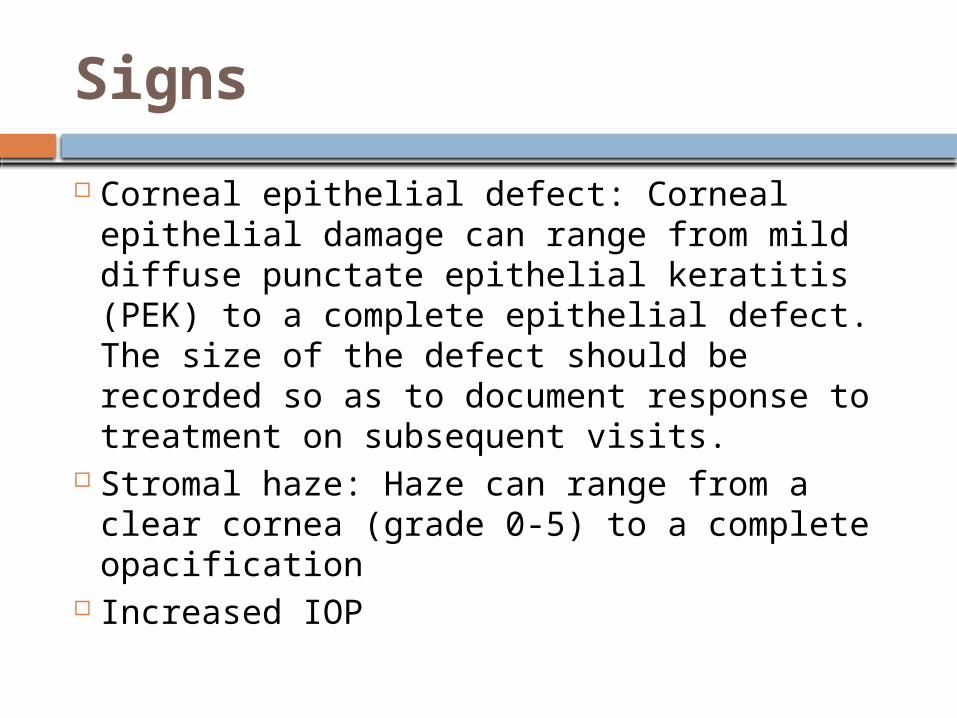
Signs
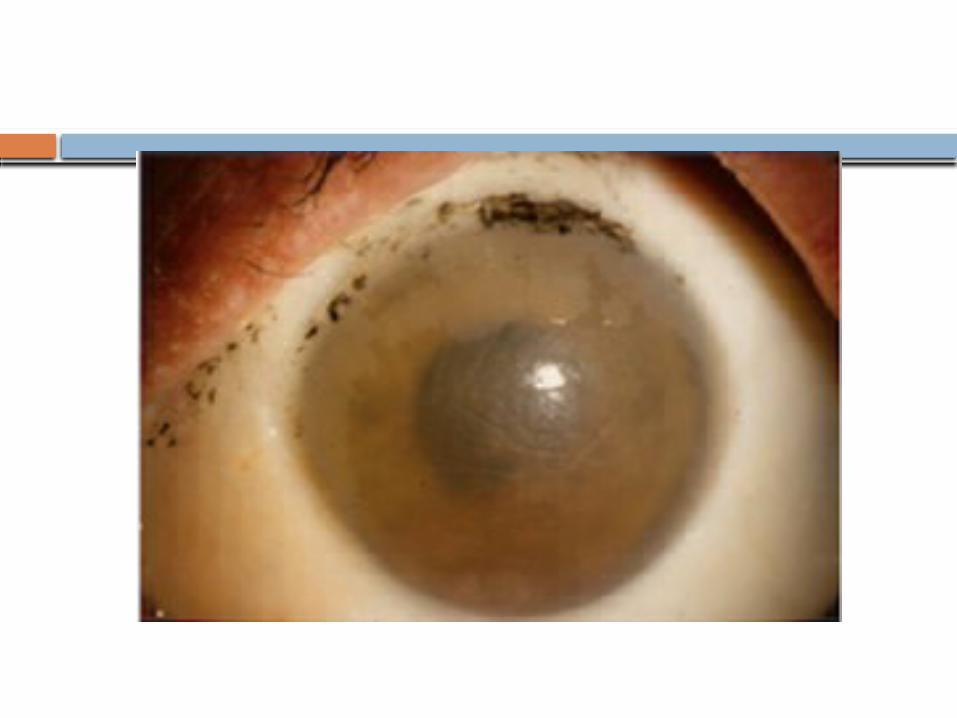
Corneal epithelial defect: Corneal epithelial damage can range from mild diffuse punctate epithelial keratitis (PEK) to a complete epithelial defect. The size of the defect should be recorded so as to document response to treatment on subsequent visits.
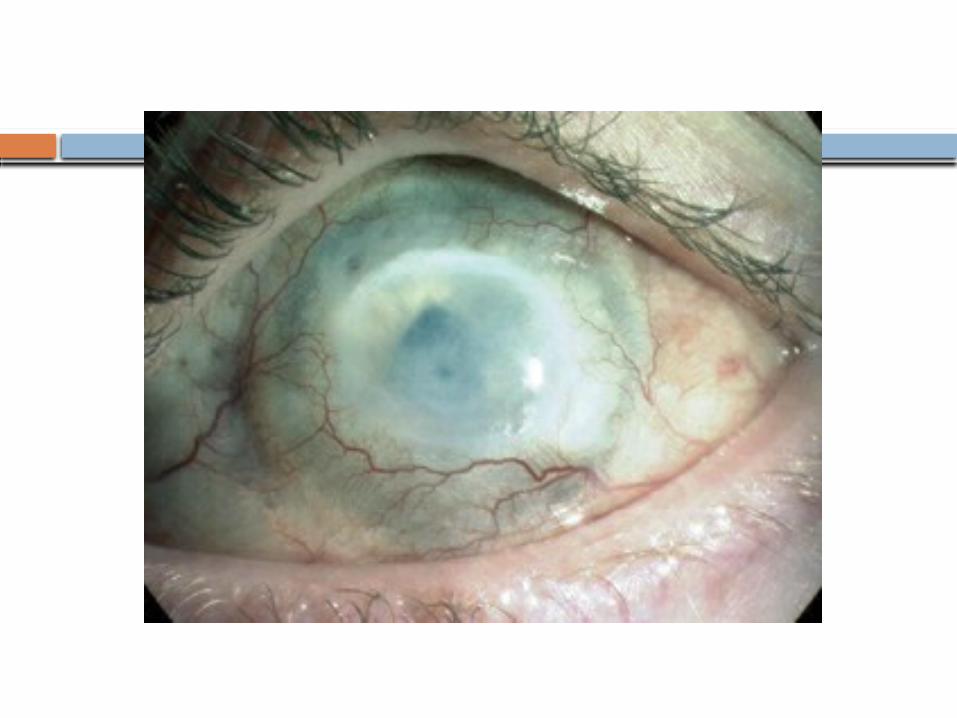
Stromal haze: Haze can range from a clear cornea (grade 0-5) to a complete opacification
Increased IOP
Signs
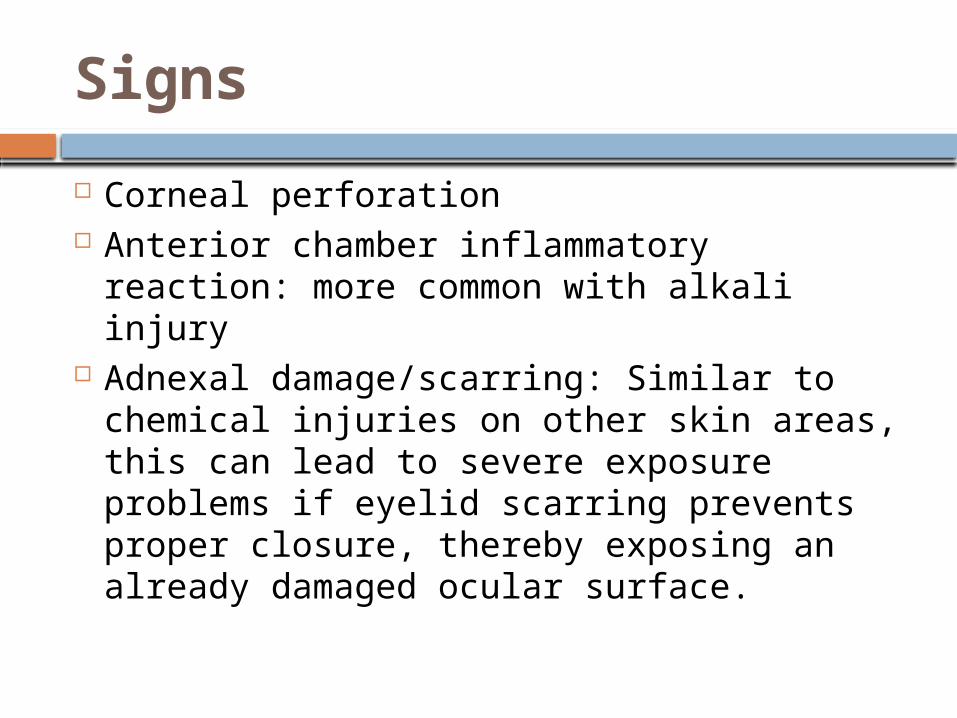
Corneal perforation Anterior chamber inflammatory reaction:
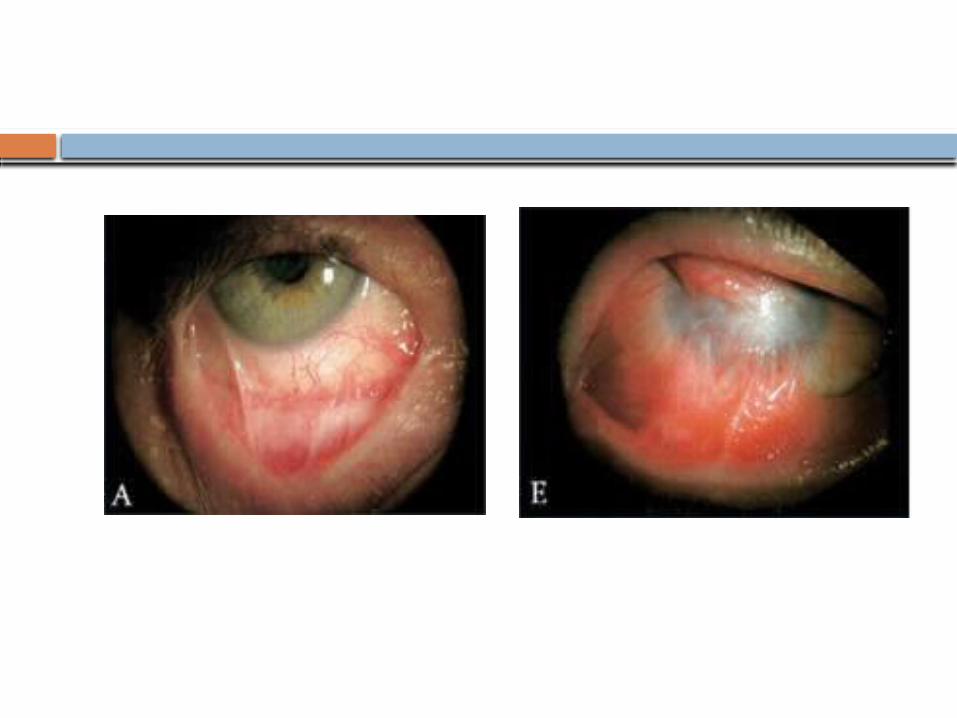
more common with alkali injury Adnexal damage/scarring: Similar to
chemical injuries on other skin areas, this can lead to severe exposure problems if eyelid scarring prevents proper closure, thereby exposing an already damaged ocular surface.
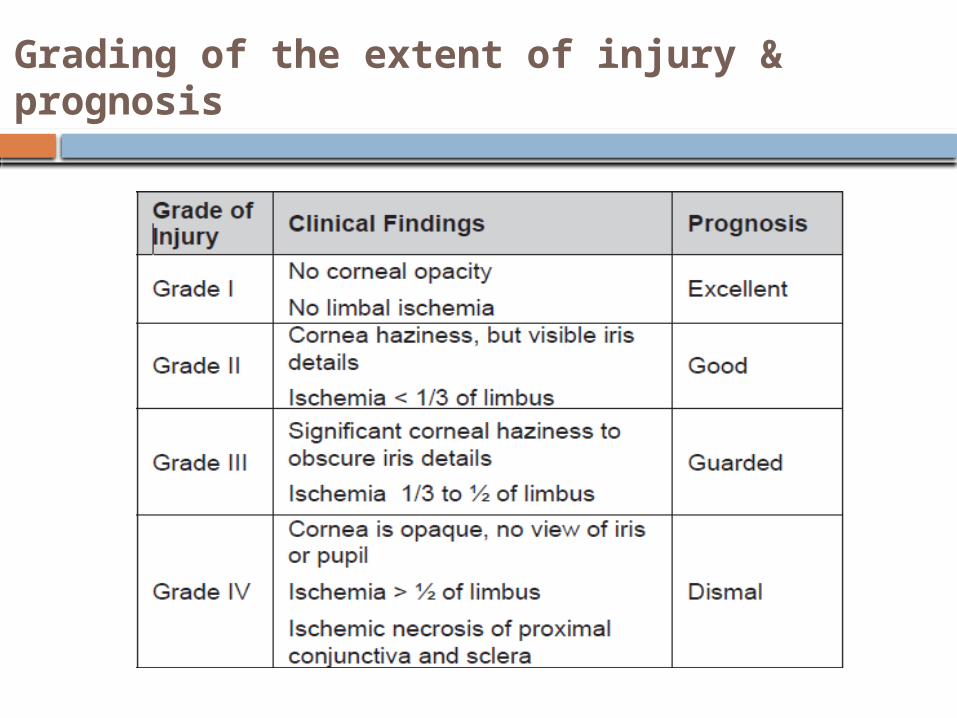
Grading of the extent of injury & prognosis



Goals of management
Treat Systemic injury Goals for ocular involvement
removing the offending agent controlling inflammation promoting ocular surface healing preventing infection controlling IOP REMOVE
CONTROL PROMOTE PREVENT
Remove the chemical (irrigation)
Immediate copious irrigation remains the single most important therapy for treating chemical injuries.
Ideally, the eye should be irrigated with a sterile balanced buffered solution, such as normal saline solution or Ringer's lactate solution. However, immediate irrigation with even plain tap water is preferred without waiting for the ideal fluid.
The irrigation solution must contact the ocular surface. Irrigation should be continued until the pH of the ocular surface is neutralized, usually requiring 1-2 liters of fluid.
Promote ocular surface (epithelial) healing
Artificial tears Bandage contact lens Ascorbate plays a fundamental role in
collagen remodeling, leading to an improvement in corneal healing.
Amniotic membrane transplant topical Sodium Ascorabte 10% given 2
hourly and 1-2 g of vitamin C given orally ( not recommended in renal disease)
Control inflammation
Inflammatory mediators Inhibits reepithelialization but also
increases the risk of corneal ulceration and perforation
Controlling inflammation with topical steroids can help break this inflammatory cycle
Citrate both promotes corneal wound healing and inhibits PMNs via calcium chelation.
Prevent infection
When the corneal epithelium is absent, the eye is susceptible to infection.
Prophylactic topical antibiotics during the initial treatment stages
Control IOP
• Oral acetazolamide and topical medications
Control pain
Severe chemical burns can be extremely painful.
Oral NSAIDS Ciliary spasm can be managed with the
use of cycloplegic agents
Surgical Care
Early Debridement Temporary amniotic membrane Limbal stem cell transplant Lysis of conjunctival symblepharon
Late Surgery for conjunctival adhesions Keratoplasty Cataract extraction Keratoprosthesis Glaucoma surgery
Follow up
In patients with severe chemical injuries, short hospitalization in an ophthalmic care unit to closely monitor
In general, the prognosis of ocular chemical injuries is directly correlated with the severity of insult to the eye and adnexal structures.
Roper-Hall grading system
Complications
Primary complications include the following: Conjunctival inflammation Corneal abrasions Corneal haze and edema Acute rise in IOP Corneal melting and perforations
Complications
Secondary complications include the following: Secondary glaucoma Secondary cataract Conjunctival scarring Corneal thinning and perforation Complete ocular surface disruption with corneal
scarring and vascularization Corneal ulceration (sterile or infectious) Complete globe atrophy (phthisis bulbi) Blindness
Management summary
Immediate, prolonged irrigation Followed by referral to ophthalmologist
for aggressive early management Close long-term monitoring Are essential to promote ocular surface
healing and to provide the best opportunity for visual rehabilitation