-
8/8/2019 Dolor de Espalda en Ancianos
1/19
Back Pain in the Elderly
Joshua Broder, MD*, Jaime T. Snarski, MDDivision of Emergency
Medicine, Department of Surgery,
Duke University Medical Center, Box 3096, Durham, NC 27710,
USA
Back pain in the elderly is a complex chief complaint. Numerous
life-
threatening or disabling diseases may present with acute back
pain. Signs
and symptoms of these catastrophic illnesses are often similar
to those of
more benign disorders. Understanding the limitations of the
history and
physical examination in elderly patients who have back pain is
essential to
avoid misdiagnosis and patient morbidity or mortality. This
article describes
the presentation and evaluation of dangerous causes of back
pain. Emphasis
is placed on vascular catastrophes, spinal cord compression
(SCC) syn-
dromes, and infectious disease processes. Spinal compression
fractures arediscussed briefly. Wherever possible, the authors
refer to primary research
articles for information on disease presentations and the
sensitivity of his-
torical, physical examination, laboratory, and imaging
tests.
Epidemiology
Thirty percent of adults age 65 years or older report low back
pain as
a significant complaint. Approximately 10% of all office visits
for back
pain occur among elderly patients [13]. Although malignancy,
heart dis-
ease, chronic lung disease, stroke, and diabetes are the leading
causes of
death in the elderly, aortic aneurysm and aortic dissection (AD)
are signif-
icant causes of mortality by the age of 65 years, accounting for
nearly 1% of
deaths. These statistics remain static for each advancing decade
[1,2,46].
Vascular catastrophes
Rupture of an abdominal aortic aneurysm (AAA) and AD account for
anestimated 15,000 deaths annually in the United States and are
consistently
* Corresponding author.
E-mail address: [email protected] (J. Broder).
0749-0690/07/$ - see front matter 2007 Elsevier Inc. All rights
reserved.
doi:10.1016/j.cger.2007.01.011 geriatric.theclinics.com
Clin Geriatr Med 23 (2007) 271289
mailto:[email protected]:[email protected]
-
8/8/2019 Dolor de Espalda en Ancianos
2/19
among the 15 leading causes of death according to the Centers
for Disease
Control [46]. Both diseases may present initially with back
pain. Rapid di-
agnosis and treatment of these two deadly disorders are
essential. Unfortu-nately, the history and physical examination
alone are limited in excluding
these diagnoses.
Abdominal aortic aneurysm
An AAA is defined as a dilated region of the aorta exceeding
twice the
normal diameter (or approximately 3 cm). They occur in
approximately
5% of the population above the age of 65 years [7]. Important
risk factors
for AAA include male gender, family history of AAA, and
cigarette smok-ing. Surprisingly, other risk factors for
atherosclerosis, including hyperten-
sion, elevated cholesterol, and the presence of coronary artery
or other
peripheral arterial disease, are more weakly associated with the
risk for an-
eurysm formation [8]. In fact, for reasons that are not well
understood, di-
abetes is negatively associated with the presence of AAA in
large studies [8].
Risk of aneurysm rupture becomes substantial when the diameter
rises
above 5 cm. Recent research, however, suggests that rupture may
occur at
smaller diameters in women [9]. For patients presenting with AAA
rupture,
mortality approaches 40% to 80% [10]. In contrast, elective AAA
repair hasan operative mortality of approximately 4% [10]. Thus,
early detection is es-
sential. At present, national guidelines recommend screening
only in men
age 65 years or older [7,11].
Limitations of the history and physical examination for
abdominal aortic
aneurysms
William Osler recognized the enigmatic presentation of aortic
aneurysm,
stating, There is no disease more conducive to clinical humility
than aneu-
rysm of the aorta [12]. Geriatricians always must consider AAA
in anyelderly patient presenting with back pain. Although acute
back pain may in-
crease suspicion for rupture, subacute or chronic presentations
of AAA can
occur. In a case series of unruptured aneurysms, the duration of
pain before
diagnosis ranged from 1 to 60 days, with a mean of 11.6 days
[13]. In a series
of ruptured aneurysms, time from onset of symptoms to emergency
depart-
ment presentation ranged from 44 minutes to 36 hours (Box 1)
[14].
The difficulty of making this diagnosis is highlighted by the
fact that 30%
to 60% of AAAs are misdiagnosed initially. The most common
misdiag-
noses for AAA are renal colic, diverticulitis, and
gastrointestinal hemor-rhage [15,16]. The reasons for misdiagnosis
probably are multifactorial.
AAA may present with symptoms similar to those of more benign
condi-
tions (eg, back pain mimicking renal colic, or left lower
quadrant pain re-
sembling diverticulitis). Findings such as hematuria (present in
87% of
ruptured AAAs in one series) or heme-positive stools may confuse
the diag-
nostic picture and delay diagnosis [17]. Moreover, in one series
of
272 BRODER & SNARSKI
-
8/8/2019 Dolor de Espalda en Ancianos
3/19
misdiagnosed AAA, hemodynamic shock was present in 57% of
patients
and probably compromised the patients ability to provide a
useful history
[15]. In addition, the classic finding of a pulsatile abdominal
mass was noted
in only 26% of patients who initially were misdiagnosed; the
absence of
a pulsatile abdominal mass probably obscured the diagnosis [15].
Delayed
presentations of disease, ranging from 10 hours to 14 days in
one series,
also are common in patients who are misdiagnosed [16]. This
delay may
reduce physicians suspicion of AAA, because the classic
presentation is
one of more acute and severe illness.Physical examination is
insensitive in identifying aortic aneurysms.
A normal examination never should exclude the diagnosis.
Numerous stud-
ies have shown the sensitivity of abdominal palpation to detect
a pulsatile
mass to be poor, reaching only 80% even in aneurysms up to 5 cm
in size
[1820]. Smaller aneurysms are even less readily detected by
examination.
Obesity further compromises examination sensitivity. Sensitivity
of physical
examination for aneurysm rupture is not well studied.
Hemodynamic stability should not be taken as a reassuring sign
or as per-
mission to perform a less urgent evaluation. In a study of
patients presentingto an emergency department with aneurysm
rupture, 50% of patients who
died within 2 hours had initial heart rates less than 71 beats
per minute
and systolic blood pressures greater than 110 mm Hg [14].
Fortunately, isolated back pain is a relatively rare
presentation of aneur-
ismal rupture. In an emergency department study of patients who
had rup-
tured AAA, isolated back pain constituted the chief complaint in
only 4%,
Box 1. Key pearls and pitfalls: aortic disasters
Physical examination is inadequate to rule out an
aorticcatastrophe.
A chest radiograph is inadequate to rule out aortic
dissection.
In the office:
Obtain intravenous access.
Place the patient on a cardiac monitor.
Administer oxygen.
Arrange immediate emergency medical service transport to an
emergency department.
In the emergency department:Consult a surgeon immediately
(before imaging) for unstable
patients.
Perform rapid bedside ultrasound to evaluate for AAA.
Consider initial noncontrast CT to evaluate for ruptured
AAA.
Perform CT with intravenous contrast for definitive
diagnosis
of AAA or aortic dissection.
273BACK PAIN IN THE ELDERLY
-
8/8/2019 Dolor de Espalda en Ancianos
4/19
whereas the combination of abdominal and back pain occurred in
14% [14].
Back pain associated with syncope or near-syncope is an AAA
rupture until
proven otherwise. In the same emergency department study of
rupturedAAA, 20% had abdominal and back pain as well as collapse
[14]. Rapid
evaluation for AAA should be considered in any elderly patient
who has
acute nontraumatic back pain, because 12.5% of patients who have
rupture
may die within 2 hours of presentation [14].
Diagnostic evaluation for abdominal aortic aneurysms
Imaging modalities used to diagnose an AAA include plain-film
radiog-
raphy, ultrasound, CT, and MRI. Although an abdominal
radiograph
sometimes may reveal a calcified aortic contour, the sensitivity
for detectingAAA is not known. Therefore, plain films should not be
used alone to ex-
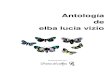
clude AAA. In contrast, ultrasound has excellent sensitivity for
the presence
of AAA (Fig. 1). Ultrasound has the advantage of being portable,
noninva-
sive, and can be performed several times during the evaluation
of an unsta-
ble patient. Unfortunately, ultrasound has limited sensitivity
for AAA
rupture. In some studies, sensitivity for rupture has been as
low as 4%
[21]. Nevertheless, an AAA seen on ultrasound in a symptomatic
patient
should be treated as a rupture until proven otherwise.
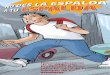
CT has excellent sensitivity and specificity for AAA rupture
[22]. Three-dimensional CT reconstructions of the aorta also are
used to plan endo-
vascular repair and are thus of particular value (Fig. 2). Oral
contrast is
contraindicated in CT conducted for aortic evaluation, because
it may
limit the ability of computer algorithms to render
three-dimensional views
of the aorta. Intravenous contrast is helpful in delineating
aortic and
Fig. 1. Transverse ultrasound image of an abdominal aortic
aneurysm. The aneurysm measures
4.75 cm by 4 cm. Ultrasound is highly sensitive for the
detection of aneurysm but insensitive for
rupture. Ultrasound is the preferred modality for diagnosis of
abdominal aortic aneurysms in
the unstable patient.
274 BRODER & SNARSKI
-
8/8/2019 Dolor de Espalda en Ancianos
5/19
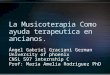
branch vessel anatomy, but aneurysm and even rupture can be
detected
without contrast (Fig. 3) [2325]. In some settings, noncontrast
CT is per-
formed as the test of first choice, allowing immediate
evaluation for AAA
rupture before laboratory test results have returned [25].
MRI with gadolinium is a definitive test with excellent
sensitivity and
specificity [26]. MRI is a poorer choice than CT for patients
who have sus-
pected rupture because the test is more time consuming than CT.
Also, the
high magnetic field, which precludes the presence of any
ferromagnetic ma-terials, makes patient treatment and monitoring in
the MRI suite more dif-
ficult. The use of MRI should be restricted to special
circumstances, such as
patients who have poor renal function in whom iodinated contrast
may
cause nephropathy. Even in these circumstances, the risk of
contrast ne-
phropathy must be weighed against the potential for rupture
resulting
from diagnostic delays.
Laboratory testing plays a limited role in the evaluation of
possible AAA
rupture. A normal hemoglobin value should not be interpreted as
a sign of
stability: in patients who died within 2 hours of emergency
department ar-rival, 50% had an initial hemoglobin of 9.0 g/dL or
greater [14].
When AAA rupture is suspected, definitive imaging must be
conducted as
rapidly as possible. Unstable patients who have suspected
ruptured AAA
require surgical consultation before imaging. Rapid emergency
medical ser-
vice (EMS) transportation of patients who have suspected
abdominal aortic
aneurysm rupture is necessary.
Fig. 2. Three-dimensional CT reconstruction of an abdominal
aortic aneurysm. Reconstruc-
tions such as this CT with intravenous contrast are particularly
helpful in planning endovascu-
lar repair. In an unstable patient, however, no delay should be
incurred for imaging before
surgical consultation.
275BACK PAIN IN THE ELDERLY
-
8/8/2019 Dolor de Espalda en Ancianos
6/19
Aortic dissection
Limitations of the history and physical examination
AD, once thought to be the most common aortic catastrophe, is
now be-
lieved to occur at a rate of 3.5 per 100,000, less often than
AAA rupture [27].
Inhospital mortality for AD ranges from 13% to 43% [28,29]. The
classic
presentation of AD is the sudden onset of tearing chest pain
that radiates
to the back. In the elderly, however, classic symptoms of
dissection are
less common. The International Registry of Aortic Dissection
(IRAD)found abrupt onset of pain to occur in only 77% of patients
age 70 years
or older, compared with 89% of those less than 70 years of age
[28]. More-
over, neurologic deficits produced from carotid dissection,
spinal cord ische-
mia, or peripheral ischemic neuropathy occur in 5% to 14% of
patients age
70 years or older [28]. AD must be included in the differential
diagnosis of
any patient who has back pain and neurologic signs or
symptoms.
Similar to AAA rupture, physical examination for AD has limited
sensi-
tivity and specificity. Prospective studies do not validate
traditional bedside
maneuvers, such as the measurement of bilateral upper extremity
bloodpressures and palpation of pulse deficits. In fact, studies of
asymptomatic
patients find large disparities in upper extremity blood
pressures, creating
false-positive test results and a very low positive predictive
value [30,31].
The sensitivity of blood pressure differences in dissection has
not been val-
idated in any large clinical study, and the absence of a
difference in upper
extremity blood pressures should not be used to exclude aortic
disease. In
Fig. 3. Noncontrast abdominal CT showing a very large ruptured
abdominal aortic aneurysm
(arrow). The calcified wall of the aorta appears white on this
study. Blood has leaked into the
retroperitoneum on the patients left side (arrowheads). CT is
very sensitive for detection of an-
eurysm and rupture, even without contrast. Noncontrast CT may be
a good option for the rapid
diagnosis of a stable patient with a suspected abdominal aortic
aneurysm, because no delay for
creatinine measurement is necessary.
276 BRODER & SNARSKI
-
8/8/2019 Dolor de Espalda en Ancianos
7/19
addition, pulse deficits occur in only 20% to 30% of patients
[28,29,32,33].
The diastolic murmur of aortic insufficiency occurs in only
about 30% of
patients who have AD and when present does not increase the
chance of dis-section significantly [34]. When dissection is
suspected, definitive testing
must be performed rapidly.
Diagnostic imaging for aortic dissection
Imaging modalities used in the evaluation of suspected AD
include chest
radiography (CXR), CT, MRI, and transesophageal
echocardiography.
CXR is inadequate to exclude aortic dissection. According to
IRAD data,
the CXR is normal in approximately 12% of dissections [35].
Additional
suggestive but nondiagnostic CXR findings, such as a widened
mediasti-num, occur in only about 60% of cases (Fig. 4) [35]. Any
patient suspected
of having AD should be transported rapidly to the closest
emergency de-
partment, regardless of normal blood pressures, pulses, and CXR.
Once
in the emergency department, CT with intravenous contrast, MRI
with
gadolinium, and transesophageal echocardiography are all nearly
100%
sensitive for dissection [36,37].
Spinal cord compressive syndromes
SCC is a true emergency in which early diagnosis and
intervention can
prevent further morbidity. Causes of SCC include spinal
epidural
Fig. 4. (A). A normal chest radiography in a patient with back
pain and a Stanford type A aor-
tic dissection, involving the ascending aorta, arch, and
descending aorta. ( B) Coronal CT recon-
struction from the same patient. The dissection can be seen
involving segments of the aorta in
both the chest and abdomen (arrowheads). The upper arrow points
to a circular cross-section
through the aorta, showing a true lumen (lighter gray area) and
a false lumen (darker gray
area) separated by an intimal flap. The lower arrow points to an
elliptical aortic cross-section
showing the same features.
277BACK PAIN IN THE ELDERLY
-
8/8/2019 Dolor de Espalda en Ancianos
8/19
metastases, infectious processes such as spinal epidural abscess
(SEA), and
spinal epidural hematoma (SEH). Of these, spinal epidural
metastases ac-
count for the majority of cases [3840]. SEH typically occurs in
patients re-ceiving oral anticoagulant medications [41]. It is
important to have a low
threshold for rapid evaluation and treatment whenever cord
compression
is suspected (Box 2).
Spinal cord compression caused by spinal epidural metastases
Four percent to 6% of patients who have cancer ultimately
develop SCC,
and up to 80% complain of back pain before the onset of
neurologic deficits
[42]. A retrospective study of patients diagnosed with cord
compressionfound a median duration of symptoms of back pain of 3
months. In
many cases, patients experienced subtle sensory or motor
symptoms up to
20 days before diagnosis. As a result of delays in diagnosis,
more than
80% of patients in this study were unable to walk unassisted by
the time
of diagnosis [43]. Back pain in a patient who has cancer should
be con-
sidered a consequence of spinal metastatic disease until proven
otherwise.
Once neurologic signs and symptoms have developed, the prognosis
for re-
covery is grim. In patients who are unable to walk at
presentation, only 15%
to 22% regain the ability to ambulate with treatment
[44,45].
Box 2. Key pearls and pitfalls: spinal compressive syndromes
A normal neurologic examination does not rule out the
diagnosis.
Evaluation should precede the development of neurologic
abnormalities whenever possible, because deficits often
areirreversible.
Plain-film radiographs are inadequate to rule out the
diagnosis.
In the office:
Consider immediate steroid administration if neurologic
deficits are present.
Arrange immediate transport to an emergency department.
In the emergency department:
Consult a neurosurgeon and radiation oncologist immediately
(before imaging) for patients who have neurologic
deficits.Administer steroids for patients who have neurologic
deficits.
Perform definitive imaging with MRI with gadolinium
contrast.
In stable patients suspected of having infection, defer
antibiotics until CT-guided aspiration is performed.
278 BRODER & SNARSKI
-
8/8/2019 Dolor de Espalda en Ancianos
9/19
Limitations of the history and physical examination
A thorough history and complete neurologic examination are
important,
but neither is sufficiently sensitive in detecting SCC. The
majority of patientscomplain of back pain (37%82%) or radicular
pain (41%) [42,45,46]. A
smaller percentage has subjective weakness (30%) or gross
weakness with
inability to walk (16%67%) [4246]. Sensory loss and bowel and/or
blad-
der dysfunction occur variably; in one series they were present
in up to 90%
and 70% of cases, respectively [45]. Often these symptoms, once
present, are
irreversible, so early suspicion in patients complaining of pain
alone is war-
ranted. On physical examination, increased deep tendon reflexes
(20%), ab-
normal plantar reflexes (20%), decreased rectal sphincter tone
or distended
bladder (9%), spinal tenderness (35%), and objective weakness
(41%) maybe noted [46]. As stated, none of these signs or symptoms
is sufficiently sen-
sitive to rule out SCC.
Risk assessment for patients who have known cancers has been
proposed
for selecting patients for diagnostic imaging. In women, breast
cancer is the
most common cause of metastatic epidural SCC , and a study in
this pop-
ulation identified four independent predictors of cord
compression: bone
metastases for 2 or more years, metastatic disease at
presentation with can-
cer, objective weakness on physical examination, and vertebral
compression
fracture on spine radiograph. Unfortunately, although the
presence of mul-tiple risk factors increases the risk of SCC, with
85% of those with SCC hav-
ing three or four risk factors, 12% of patients who had SCC had
none of
these risk factors [46]. Moreover, approximately 2% of patients
presenting
with SCC have an undiagnosed malignancy [45].
Diagnostic imaging for spinal cord compression caused by
spinal
epidural metastases
Plain films of the spine are insensitive and nonspecific for the
diagnosis of
SCC. The reported sensitivity is as low as 30% to 76% [46,47],
and this sen-sitivity includes nonspecific findings such as spinal
compression fractures.
Nuclear medicine imaging modalities also may yield
false-negative results
in as much as 6% of cases [46,48]. By comparison, MRI with
gadolinium
intravenous contrast is extremely sensitive for the diagnosis,
nearing
100% [47,49]. As a result, emergent MRI should be obtained for
any patient
when cord compression or spinal metastatic disease is suspected.
For pa-
tients who cannot undergo MRI, CT myelography can be used
[50].
Treatment of spinal cord compression caused by spinalepidural
metastases
Urgent administration of steroids is recommended for suspected
meta-
static SCC. Randomized trials have shown improvement in patients
receiv-
ing adjuvant steroid therapy with dexamethasone in addition to
radiation
therapy. The doses used are large (dexamethasone 96 mg
intravenous bolus
followed by 96 mg orally for 3 days and then tapered) [51]. In
some patients
279BACK PAIN IN THE ELDERLY
-
8/8/2019 Dolor de Espalda en Ancianos
10/19
who do not have motor deficits and in whom steroids are
relatively contra-
indicated for reasons such as poorly controlled diabetes,
radiation without
steroid therapy may be possible, although larger trials are
needed [52].Single doses of steroids are unlikely to have
deleterious effects, so immediate
administration of dexamethasone before imaging confirmation is
appropri-
ate if SCC is suspected [53].
Radiation therapy with laminectomy is associated with better
functional
outcomes than radiation alone. Recent randomized, controlled
trials con-
firm that combination therapy results in better outcomes [5456].
Early con-
sultation with a radiation oncologist and neurosurgeon should be
obtained.
Spinal cord compression caused by spinal infections: spinal
epiduralabscess and vertebral osteomyelitis
Although uncommon, spinal infections remain a serious cause of
morbid-
ity and mortality in patients presenting with back pain. SEA
account for 0.2
to 2 cases per 10,000 hospital admissions and can affect
patients of any age
[57,58]. A meta-analysis of 915 cases of epidural abscess from
1954 to 1997
demonstrated a mortality rate of approximately 15% [58,59]. The
majority
of SEAs are caused by bacteria, with Staphylococcus aureus being
the most
common organism. Infections caused by fungal, parasitic, and
mycobacte-rial infections occur less commonly. In a significant
number of cases, no or-
ganism is isolated. As in previously described back pain
emergencies, initial
symptoms and signs are nonspecific and insensitive [59].
Limitations of the history and physical examination
Back pain is the presenting symptom in 71% of patients who have
SEA.
Fever is present in only two thirds of patients who have SEA
[59]. Neuro-
logic deficits are relatively rare initial presenting symptoms.
Twenty-five per-
cent of patients report muscle weakness, 25% report some degree
ofincontinence, and 13% have sensory deficits [59]. Localized
spinal tender-
ness is also unreliable, present initially in only 17% of
patients [59].
Risk factors for SEA include immunocompromised states, trauma,
sur-
gery, and infection. Immunocompromised states that increase the
possibility
of SEA include malignancy, HIV infection, cirrhosis, steroid
use, and diabe-
tes. Of these, diabetes is reported as an important risk factor
for SEA, occur-
ring in 15% of cases in one series [59]. A history of
intravenous drug abuse is
also a concerning risk factor, found in approximately 9% of
cases [59]. Dis-
tant or contiguous infections constitute perhaps the largest
risk factor, foundin more than 40% of cases [59]. A history of
trauma is present in 10% of cases
[59]. Degenerative vertebral disease is reported as a risk
factor in 6% of cases
[59]. Alcohol abuse has been reported in up to 5% of cases [59].
The precise
role and prevalence of these risk factors is unknown, because
many of
the published reports on spinal infections come from inner-city
populations
in which diabetes and injection drug use are particularly common
[58].
280 BRODER & SNARSKI
-
8/8/2019 Dolor de Espalda en Ancianos
11/19
Diagnostic evaluation for spinal epidural abscess
Laboratory findings are insensitive and unreliable in screening
for SEA.
Leukocytosis is variable. Leukocyte counts in patients who have
SEA rangefrom 1500 to 42,000 cells/mL, and normal white blood cell
counts are found
in one fourth to one third of patients [59]. Never exclude the
possibility of
SEA based upon a normal white blood cell count. The erythrocyte
sedimen-
tation rate (ESR) is reportedly more sensitive for detecting
SEA, with more
than 90% of patients having an ESR greater than 20 mm [59].
Subtle or
moderate elevations may occur, however, with approximately one
third of
patients having an ESR below 60 mm [58].
Although plain-film radiographs may reveal destruction of
vertebrae,
they are not helpful in the diagnosis of SEA (Fig. 5A) [60]. In
contrast,MRI with gadolinium has a reported sensitivity of nearly
100% for epidural
abscess [61]. It is the imaging modality of choice when
evaluating patients
for SEA (Fig. 5B). Single-photon emission CT and nuclear
medicine bone
scanning with gadolinium-67 are also very accurate means of
detecting ver-
tebral infection [6163].
Treatment of spinal epidural abscess
Antibiotic therapy should be started with a bactericidal agent
effective
against Staphylococcus aureus, Streptococci, and gram-negative
organisms.Antibiotics should be broad spectrum, able to penetrate
bone, and have rel-
atively low toxicity because the duration of treatment will be 4
to 6 weeks.
Fig. 5. (A) Abnormal plain-film radiograph in a patient who has
an epidural abscess and ver-
tebral osteomyelitis. The patient has undergone resection of a
damaged vertebral body, a risk
factor for infection. (B) Spinal epidural abscess. MRI shows
bony destruction adjacent to an
area of epidural abscess. The epidural abscess (arrowheads, dark
gray material) surrounds
and compresses the spinal cord (lighter gray material).
281BACK PAIN IN THE ELDERLY
-
8/8/2019 Dolor de Espalda en Ancianos
12/19
Blood cultures should be obtained to guide antibiotic treatment
[5759]. In
addition to antibiotic therapy, laminectomy is performed
traditionally, al-
though CT-guided percutaneous drainage may be effective in
selected cases[64]. A retrospective review of patients undergoing
antibiotic therapy and
percutaneous drainage found outcomes similar to those of
patients undergo-
ing surgical decompression, although prospective, randomized
trials are
needed to determine whether these therapies are truly equally
effective [65].
Vertebral osteomyelitis
Vertebral osteomyelitis in the elderly is another rare but
potentially dan-
gerous disease process. The risk factors, presentation,
evaluation, and treat-ment are similar to those of epidural
abscess. Compared with younger hosts,
elderly patients are more likely to be infected with
gram-negative organisms,
particularly urinary tract organisms, and to have had recent
surgery [66].
Staphylococcal species are the major infectious organism,
although myco-
bacteria are also common organisms in some populations.
Vertebral osteo-
myelitis is more common in older men [67].
Elevation of ESR and C-reactive protein is common, occurring in
ap-
proximately 80% of cases [68]. Radiographic changes may occur in
only
50% to 60% of cases (see Fig. 5A) [68]. MRI and CT are more
helpful,showing abnormalities in 70% to 99% of cases [68]. Patients
typically pres-
ent with back pain that has developed over weeks to months. The
prognosis
is poor in patients who have neurologic dysfunction at
diagnosis, chronic
debilitating diseases, and diagnosis delayed more than 8 weeks
from the
start of symptoms [69]. Delay in diagnosis is common, exceeding
1 month
from symptom onset in one third of patients [68,69].
Once the diagnosis of osteomyelitis is made, a spine surgeon
should be
consulted, and treatment with broad-spectrum antibiotics should
be initi-
ated. Antibiotics should be given for 6 to 12 weeks and can be
tailoredwith culture results. A CT-guided tissue biopsy should be
performed, pref-
erably before antibiotic administration. Nonoperative management
with an-
tibiotics and analgesia may be appropriate in patients who have
a stable
spine and minor or no neurologic deficit; this strategy is
effective in 60%
to 95% of such patients [70,71]. Surgical treatment with de
bridement and
possible spinal reconstruction is indicated in patients with
failure of medical
treatment, cord compression, and presence of a fluid collection
[71].
Cauda equina syndrome
Cauda equina syndrome classically presents with perineal
numbness and
urinary and fecal incontinence or retention. Sciatica may
accompany these
neurologic deficits. Bilateral foot weakness and occasional
weakness of
the quadriceps may occur also. Symptoms may progress rapidly
over hours
in 85% of patients. Lumbar disc herniation is a common cause,
although
282 BRODER & SNARSKI
-
8/8/2019 Dolor de Espalda en Ancianos
13/19
infection and metastatic disease also may result in the
syndrome. Delays in
diagnosis are common, occurring in roughly half of cases and are
caused by
delayed patient presentation in 17% of cases and by
physician-related delaysin the remaining 83% [72]. Delay in surgery
of more than 48 hours has been
associated with poor clinical outcome, although no difference in
outcome
has been shown in patients undergoing surgery within 5 hours
compared
with those undergoing surgery within 24 hours of diagnosis
[72,73]. Diag-
nostic evaluation with gadolinium-contrast MRI is recommended
[74].
Spinal compression fractures
Spinal compression fractures are a common problem in the elderly
andmay occur without preceding trauma. Although less time-sensitive
than
the conditions previously described, these fractures have
significant sequelae
including inability to perform activities of daily living, and
need for analge-
sics, with a litany of medication side effects (eg, sedation and
constipation
from opioids, gastrointestinal bleeding and renal insufficiency
from nonste-
roidal anti-inflammatory agents). Proving the presence of a
compression
fracture does not rule out the presence of other more ominous
disease, be-
cause metastatic disease can result in compression fractures
[75].
Diagnostic imaging for spinal compression fractures
Although plain-film radiographs may demonstrate the presence of
com-
pression fractures, more advanced imaging modalities may provide
useful
prognostic and therapeutic information. Patients who have risk
factors for
malignancy-related fractures, such as past or current cancer,
require MRI,
because plain films may not delineate fully the degree of
pathology [75].
In fact, multiple myeloma has been diagnosed in patients being
treated
for presumed osteoporotic compression fractures [76].
High-resolution CThas been shown in small studies to distinguish
benign from malignant com-
pression fractures, based on a number of criteria including
destruction of
bony elements and adjacent soft tissue or epidural masses
[77].
When a compression fracture is found and is considered to be the
sole
cause of the patients symptoms, treatment options exist,
including vertebro-
plasty. Thus evaluating a patient for compression fracture
serves multiple
purposes, including ruling out emergent pathology and
establishing treat-
ment goals. Vertebroplasty has been shown to be safe and
effective, with
demonstrated improvements in pain and quality of life [7881].
Unfortu-nately, up to a quarter of patients undergoing
vertebroplasty experience
a second compression fracture within the first year after
treatment, with
half of these fractures being symptomatic [82]. An association
has been ob-
served between vertebroplasty and rapid subsequent fracture of
adjacent
vertebral bodies, although studies are retrospective and do not
prove
a causal relationship. Pain from spinal fractures may be
significantly
283BACK PAIN IN THE ELDERLY
-
8/8/2019 Dolor de Espalda en Ancianos
14/19
-
8/8/2019 Dolor de Espalda en Ancianos
15/19
dangerous causes of back pain. Physicians caring for elderly
patients must
be vigilant in considering serious causes, including vascular
disasters, com-
pressive spinal lesions, and serious infections. Awaiting overt
signs andsymptoms may guarantee a poor outcome for many of these
disease pro-
cesses. Advanced imaging may be necessary to avoid misdiagnosis
and avert
patient morbidity and mortality (Box 3).
References
[1] National Center for Health Statistics. Health, United
States, 2005 with chartbook on trends
in the health of Americans. Hyattsville (MD): 2005.
[2] Hing E, Cherry DK, Woodwell DA. National Ambulatory Medical
Care Survey: 2004 sum-
mary. Advance data from vital and health statistics; no 374.
Hyattsville (MD): National Cen-
ter for Health Statistics; 2006.
[3] Turner JA, LeResche L, Von Korff M, et al. Back pain in
primary care. Patient characteris-
tics, content of initial visit, and short-term outcomes. Spine
1998;23(4):4639.
[4] Minin o AM, Heron MP, Smith BL. Deaths: preliminary data for
2004. National Vital Sta-
tistics Reports, vol. 53, no. 21. Available at:
www.cdc.gov/nchs. Accessed June 28, 2005.
[5] Hoyert DL, Heron MP, Murphy SL, et al. Deaths: final data
for 2003. National Vital Sta-
tistics Reports 2006;54(13):1120.
[6] Gillum RF. Epidemiology of aortic aneurysm in the United
States. J Clin Epidemiol 1995;
48(11):128998.
[7] Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005
practice guidelines for the man-agement of patients with peripheral
arterial disease (lower extremity, renal, mesenteric, and
abdominal aortic): a collaborative report from the American
Association for Vascular Sur-
gery/Society for Vascular Surgery, Society for Cardiovascular
Angiography and Interven-
tions, Society for Vascular Medicine and Biology, Society of
Interventional Radiology,
and the ACC/AHA Task Force on Practice Guidelines (Writing
Committee to Develop
Guidelines for the Management of Patients With Peripheral
Arterial Disease): endorsed
by the American Association of Cardiovascular and Pulmonary
Rehabilitation; National
Heart, Lung, and Blood Institute; Society for Vascular Nursing;
TransAtlantic Inter-Society
Consensus; and Vascular Disease Foundation. Circulation
2006;113(11):e463654.
[8] Lederle FA, Johnson GR, Wilson SE, et al. The Aneurysm
Detection and Management
Study screening program: validation cohort and final results.
Aneurysm Detection and Man-agement Veterans Affairs Cooperative
Study Investigators. Arch Intern Med 2000;160(10):
142530.
[9] Forbes TL, Lawlor DK, Derose G, et al. Gender differences in
relative dilatation of abdom-
inal aortic aneurysms. Ann Vasc Surg 2006;20(5):5648.
[10] Wainess RM, Dimick JB, Cowan JA Jr, et al. Epidemiology of
surgically treated abdominal
aortic aneurysms in the United States, 1988 to 2000. Vascular
2004;12(4):21824.
[11] Fleming C, Whitlock EP, Beil TL, et al. Screening for
abdominal aortic aneurysm: a best-ev-
idence systematic review for the U.S. Preventive Services Task
Force. Ann Intern Med 2005;
142:198202.
[12] Verma A, Lindsay TF. Regression of aortic aneurysms through
pharmacologic therapy?
N Engl J Med 2006;354(19):20678.[13] Cambria RA, Gloviczki P,
Stanson AW, et al. Symptomatic, nonruptured abdominal aortic
aneurysms: are emergent operations necessary? Ann Vasc Surg
1994;8(2):1216.
[14] Lloyd GM, Bown MJ, Norwood MG, et al. Feasibility of
preoperative computer tomogra-
phy in patients with ruptured abdominal aortic aneurysm: a
time-to-death study in patients
without operation. J Vasc Surg 2004;39(4):78891.
[15] Marston WA, Ahlquist R, Johnson G Jr, et al. Misdiagnosis
of ruptured abdominal aortic
aneurysms. J Vasc Surg 1992;16(1):1722.
285BACK PAIN IN THE ELDERLY
http://www.cdc.gov/nchshttp://www.cdc.gov/nchs
-
8/8/2019 Dolor de Espalda en Ancianos
16/19
[16] Akkersdijk GJ, van Bockel JH. Ruptured abdominal aortic
aneurysm: initial misdiagnosis
and the effect on treatment. Eur J Surg 1998;164(1):2934.
[17] Pomper SR, Fiorillo MA, Anderson CW, et al. Hematuria
associated with ruptured abdom-
inal aortic aneurysms. Int Surg 1995;80(3):2613.
[18] Lederle FA, Simel DL. The rational clinical examination.
Does this patient have abdominal
aortic aneurysm? JAMA 1999;281(1):7782.
[19] Fink HA, Lederle FA, Roth CS, et al. The accuracy of
physical examination to detect
abdominal aortic aneurysm. Arch Intern Med 2000;160(6):8336.
[20] Venkatasubramaniam AK, Mehta T, Chetter IC, et al. The
value of abdominal examina-
tion in the diagnosis of abdominal aortic aneurysm. Eur J Vasc
Endovasc Surg 2004;27(1):
5660.
[21] Shuman WP, Hastrup W Jr, Kohler TR, et al. Suspected
leaking abdominal aortic aneurysm:
use of sonography in the emergency room. Radiology
1988;168(1):1179.
[22] Hayter RG, Rhea JT, Small A, et al. Suspected aortic
dissection and other aortic disorders:
multi-detector row CT in 373 cases in the emergency setting.
Radiology 2006;238(3):84152
[Epub 2006 Feb 1].
[23] Sharma U, Ghai S, Paul SB, et al. Helical CT evaluation of
aortic aneurysms and dissection:
a pictorial essay. Clin Imaging 2003;27(4):27380.
[24] Sprouse LR 2nd, Meier GH 3rd, Parent FN, et al. Is
three-dimensional computed tomogra-
phy reconstruction justified before endovascular aortic aneurysm
repair? J Vasc Surg 2004;
40(3):4437.
[25] Novelline RA, Rhea JT, Rao PM, et al. Helical CT in
emergency radiology. Radiology 1999;
213(2):32139.
[26] Vosshenrich R, Fischer U. Contrast-enhanced MR angiography
of abdominal vessels: is
there still a role for angiography? Eur Radiol 2002;12(1):21830
[Epub 2001 Aug 9].[27] Clouse WD, Hallett JW Jr, Schaff HV, et al.
Acute aortic dissection: population-based inci-
dence compared with degenerative aortic aneurysm rupture. Mayo
Clin Proc 2004;79(2):
17680.
[28] Mehta RH, OGara PT, Bossone E, et al, International
Registry of Acute Aortic Dissec-
tion (IRAD) Investigators. Acute type A aortic dissection in the
elderly: clinical charac-
teristics, management, and outcomes in the current era. J Am
Coll Cardiol 2002;40(4):
68592.
[29] Suzuki T, Mehta RH, Ince H, et al. International Registry
of Aortic Dissection. Clinical
profiles and outcomes of acute type B aortic dissection in the
current era: lessons from
the International Registry of Aortic Dissection (IRAD).
Circulation 2003;108(Suppl 1):
II3127.[30] Singer AJ, Hollander JE. Blood pressure. Assessment
of interarm differences. Arch Intern
Med 1996;156(17):20058.
[31] Pesola GR, Pesola HR, Lin M, et al. The normal difference
in bilateral indirect blood pres-
sure recordings in hypertensive individuals. Acad Emerg Med
2002;9(4):3425.
[32] Teece S, Hogg K. Best evidence topic report. Peripheral
pulses to exclude thoracic aortic dis-
section. Emerg Med J 2004;21(5):589.
[33] Bossone E, Rampoldi V, Nienaber CA, et al, International
Registry of Acute Aortic Dissec-
tion (IRAD) Investigators. Usefulness of pulse deficit to
predict in-hospital complications
and mortality in patients with acute type A aortic dissection.
Am J Cardiol 2002;89(7):
8515.
[34] Klompas M. Does this patient have an acute thoracic aortic
dissection? JAMA 2002;287(17):226272.
[35] Hagan PG, Nienaber CA, Isselbacher EM, et al. The
International Registry of Acute
Aortic Dissection (IRAD): new insights into an old disease. JAMA
2000;283(7):
897903.
[36] Moore AG, Eagle KA, Bruckman D, et al. Choice of computed
tomography, transesopha-
geal echocardiography, magnetic resonance imaging, and
aortography in acute aortic
286 BRODER & SNARSKI
-
8/8/2019 Dolor de Espalda en Ancianos
17/19
dissection: International Registry of Acute Aortic Dissection
(IRAD). Am J Cardiol 2002;
89(10):12358.
[37] Sommer T, Fehske W, Holzknecht N, et al. Aortic dissection:
a comparative study of diag-
nosis with spiral CT, multiplanar transesophageal
echocardiography, and MR imaging.
Radiology 1996;199(2):34752.
[38] Hentschel SJ, Woolfenden AR, Fairholm DJ. Resolution of
spontaneous spinal epidural
hematoma without surgery: report of two cases. Spine
2001;26(22):E5257.
[39] Joseph AP, Vinen JD. Acute spinal epidural hematoma. J
Emerg Med 1993;11(4):43741.
[40] Parman SC. Spontaneous spinal epidural hematoma. Ann Emerg
Med 1980;9(7):36870.
[41] Seet RC, Lim EC, Wilder-Smith EP, et al. Spontaneous
epidural haematoma presenting
as cord compression in a patient receiving clopidogrel. Eur J
Neurol 2005;12(10):
8112.
[42] Pedersen AG, Bach F, Melgaard B. Frequency, diagnosis, and
prognosis of spinal cord com-
pression in small cell bronchogenic carcinoma. A review of 817
consecutive patients. Cancer
1985;55(8):181822.
[43] Levack P, Graham J, Collie D, et al. Scottish Cord
Compression Study Group. Dont wait
for a sensory levellisten to the symptoms: a prospective audit
of the delays in diagnosis of
malignant cord compression. Clin Oncol (R Coll Radiol)
2002;14(6):47280.
[44] Bach F, Larsen BH, Rohde K, et al. Metastatic spinal cord
compression. Occurrence, symp-
toms, clinical presentations and prognosis in 398 patients with
spinal cord compression. Acta
Neurochir (Wien) 1990;107(12):3743.
[45] Bach F, Agerlin N, Sorensen JB, et al. Metastatic spinal
cord compression secondary to lung
cancer. J Clin Oncol 1992;10(11):17817.
[46] Lu C, Stomper PC, Drislane FW, et al. Suspected spinal cord
compression in breast cancer
patients: a multidisciplinary risk assessment. Breast Cancer Res
Treat 1998;51(2):12131.[47] Husband DJ, Grant KA, Romaniuk CS. MRI
in the diagnosis and treatment of suspected
malignant spinal cord compression. Br J Radiol
2001;74(877):1523.
[48] Portenoy RK, Galer BS, Salamon O, et al. Identification of
epidural neoplasm. Radiography
and bone scintigraphy in the symptomatic and asymptomatic spine.
Cancer 1989;64(11):
220713.
[49] Li KC, Poon PY. Sensitivity and specificity of MRI in
detecting malignant spinal cord com-
pression and in distinguishing malignant from benign compression
fractures of vertebrae.
Magn Reson Imaging 1988;6(5):54756.
[50] Carmody RF, Yang PJ, Seeley GW, et al. Spinal cord
compression due to metastatic disease:
diagnosis with MR imaging versus myelography. Radiology
1989;173(1):2259.
[51] Sorensen S, Helweg-Larsen S, Mouridsen H, et al. Effect of
high-dose dexamethasone in car-cinomatous metastatic spinal cord
compression treated with radiotherapy: a randomised
trial. Eur J Cancer 1994;30A(1):227.
[52] Maranzano E, Latini P, Beneventi S, et al. Radiotherapy
without steroids in selected
metastatic spinal cord compression patients. A phase II trial.
Am J Clin Oncol 1996;
19(2):17983.
[53] Wessling H, de las Heras P. Cervicothoracolumbar spinal
epidural abscess with tetraparesis.
Good recovery after non-surgical treatment with antibiotics and
dexamethasone. Case
report and review of the literature. Neurocirugia (Astur)
2003;14(6):52933.
[54] Sorensen S, Borgesen SE, Rohde K, et al. Metastatic
epidural spinal cord compression.
Results of treatment and survival. Cancer 1990;65(7):15028.
[55] Lewis S. Direct decompressive surgery and radiation therapy
improved walking ability inmetastatic epidural spinal cord
compression. J Bone Joint Surg Am 2006;88(5):1169.
[56] Patchell RA, Tibbs PA, Regine WF, et al. Direct
decompressive surgical resection in
the treatment of spinal cord compression caused by metastatic
cancer: a randomised trial.
Lancet 2005;366(9486):6438.
[57] Hlavin ML, Kaminski HJ, Ross JS, et al. Spinal epidural
abscess: a ten-year perspective.
Neurosurgery 1990;27(2):17784.
287BACK PAIN IN THE ELDERLY
-
8/8/2019 Dolor de Espalda en Ancianos
18/19
[58] Grewal S, Hocking G, Wildsmith JA. Epidural abscesses. Br J
Anaesth 2006;96(3):292302
[Epub 2006 Jan 23].
[59] Reihsaus E, Waldbaur H, Seeling W. Spinal epidural abscess:
a meta-analysis of 915 patients.
Neurosurg Rev 2000;23(4):175204 [discussion: 205].
[60] An HS, Seldomridge JA. Spinal infections: diagnostic tests
and imaging studies. Clin Orthop
Relat Res 2006;444:2733.
[61] Ledermann HP, Schweitzer ME, Morrison WB, et al. MR imaging
findings in spinal infec-
tions: rules or myths? Radiology 2003;228(2):50614 [Epub 2003
Jun 11].
[62] Love C, Patel M, Lonner BS, et al. Diagnosing spinal
osteomyelitis: a comparison of bone
and Ga-67 scintigraphy and magnetic resonance imaging. Clin Nucl
Med 2000;25(12):
96377.
[63] Concia E, Prandini N, Massari L, et al. Osteomyelitis:
clinical update for practical guidelines.
Nucl Med Commun 2006;27(8):64560.
[64] Lyu RK, Chen CJ, Tang LM, et al. Spinal epidural abscess
successfully treated with
percutaneous, computed tomography-guided, needle aspiration and
parenteral antibiotic
therapy: case report and review of the literature. Neurosurgery
2002;51(2):50912 [dis-
cussion: 512].
[65] Siddiq F, Chowfin A, Tight R, et al. Medical vs surgical
management of spinal epidural ab-
scess. Arch Intern Med 2004;164(22):240912.
[66] Belzunegui J, Intxausti JJ, De Dios JR, et al.
Haematogenous vertebral osteomyelitis in the
elderly. Clin Rheumatol 2000;19(5):3447.
[67] Nather A, David V, Hee HT, et al. Pyogenic vertebral
osteomyelitis: a review of 14 cases.
J Orthop Surg 2005;13(3):2404.
[68] Beronius M, Bergman B, Andersson R. Vertebral osteomyelitis
in Goteborg, Sweden:
a retrospective study of patients during 199095. Scand J Infect
Dis 2001;33(7):52732.
[69] Solis Garcia Del Pozo J, Soto MV, Solera J. Vertebral
osteomyelitis: long-term disability as-
sessment and prognostic factors. J Infect 2007;54(2):12934.
[70] Carragee EJ. Pyogenic vertebral osteomyelitis. J Bone Joint
Surg Am 1997;79(6):87480.
[71] Nakase H, Matsuda R, Tamaki R, et al. Two-stage management
for vertebral osteomyelitis
and epidural abscess: technical note. Neurosurgery
2006;58(6):E1219.
[72] Shapiro S. Medical realities of cauda equina syndrome
secondary to lumbar disc herniation.
Spine 2000;25(3):34851 [discussion: 352].
[73] Hussain SA, Gullan RW, Chitnavis BP. Cauda equina syndrome:
outcome and implications
for management. Br J Neurosurg 2003;17(2):1647.
[74] Coscia M, Leipzig T, Cooper D. Acute cauda equina syndrome.
Diagnostic advantage ofMRI. Spine 1994;19(4):4758.
[75] Ho CS, Choi WM, Chen CY, et al. Metastasis in vertebra
mimicking acute compression frac-
tures in a patient with osteoporosis: MRI findings. Clin Imaging
2005;29(1):647.
[76] Togawa D, Lieberman IH, Bauer TW, et al. Histological
evaluation of biopsies obtained
from vertebral compression fractures: unsuspected myeloma and
osteomalacia. Spine 2005;
30(7):7816.
[77] Kubota T, Yamada K, Ito H, et al. High-resolution imaging
of the spine using multidetector-
row computed tomography: differentiation between benign and
malignant vertebral com-
pression fractures. J Comput Assist Tomogr 2005;29(5):7129.
[78] Kumar K, Verma AK, Wilson J, et al. Vertebroplasty in
osteoporotic spine fractures: a qual-
ity of life assessment. Can J Neurol Sci 2005;32(4):48795.[79]
Cheung G, Chow E, Holden L, et al. Percutaneous vertebroplasty in
patients with intractable
pain from osteoporotic or metastatic fractures: a prospective
study using quality-of-life as-
sessment. Can Assoc Radiol J 2006;57(1):1321.
[80] Do HM, Kim BS, Marcellus ML, et al. Prospective analysis of
clinical outcomes after per-
cutaneous vertebroplasty for painful osteoporotic vertebral body
fractures. AJNR Am J
Neuroradiol 2005;26(7):16238.
288 BRODER & SNARSKI
-
8/8/2019 Dolor de Espalda en Ancianos
19/19
[81] Liliang PC, Su TM, Liang CL, et al. Percutaneous
vertebroplasty improves pain and physical
functioning in elderly osteoporotic vertebral compression
fracture patients. Gerontology
2005;51(1):349.
[82] Voormolen MH, Lohle PN, Juttmann JR, et al. The risk of new
osteoporotic vertebral com-
pression fractures in the year after percutaneous
vertebroplasty. J Vasc Interv Radiol 2006;
17(1):716.
[83] Lyritis GP, Ioannidis GV, Karachalios T, et al. Analgesic
effect of salmon calcitonin sup-
positories in patients with acute pain due to recent
osteoporotic vertebral crush fractures:
a prospective double-blind, randomized, placebo-controlled
clinical study. Clin J Pain
1999;15(4):2849.
289BACK PAIN IN THE ELDERLY