Embed Size (px)
Citation preview

Corynebacteria
II MBBS
Dr Ekta ChourasiaMicrobiology

Dr Ekta, Microbiology14.12.08
Gram positive rods
Non spore-forming1. AEROBIC
Corynebacteria C. diphtheriae diphtheroids C. jeikeium
Listeria monocytogenes Erysipelothrix rusiopathiae
2. ANAEROBIC Lactobacillus spp.
Spore-forming1. AEROBIC
Genus: Bacillus B. anthracis B. cereus B. subtilis
2. ANAEROBIC Genus: Clostridium
C. tetani C. botulinum C. difficile C. perfringens

Dr Ekta, Microbiology14.12.08
Corynebacteria - Overview
Gram positive, non motile bacilli with irregularly stained segments
Frequently show club shaped swellings – corynebacteria (coryne = club)
C. diphtheriae : most important member of this genus, causes diphtheria
Diphtheroids : commensals of nose, throat, nasopharynx, skin, urinary tract & conjunctiva.

Dr Ekta, Microbiology14.12.08
Historical overview I.Corynebacterium diphtheriae
Bretonneau 1826Clinical characterisationof diphtheria – diphtherite
Klebs 1883Detecting the bacterium
Loeffler 1884Isolating the bacterium
Roux and Yersin 1888Discovering the diphtheria toxin
Behring and Kitasato1890-1892- Discovering the diphtheria
antitoxin- Antitoxic immunity (therapy and
prevention)
Roux 1894Treatment with antitoxin

Dr Ekta, Microbiology14.12.08
Historical overview I.Corynebacterium diphtheriae
Emil von Behring 1901
Nobel prize
Behring 1913
Active immunisation I.
with toxin-antitoxin mix
Schick 1913
Skin test
Ramon 1923
Active immunisation II.
Anatoxin = toxoid
Freeman 1951
PHAGE (lysogenia,
toxin production)

Dr Ekta, Microbiology14.12.08
Introduction – C. diphtheriae
Diphtheros – leather (tough, leathery pseudomembrane)
Also known as Klebs–Loeffler bacillus
Causes Diphtheria

Dr Ekta, Microbiology14.12.08
Important features of C. diphtheriae Slender Gram positive bacilli Pleomorphic, non motile, non sporing Chinese letter or Cuneiform arrangement Stains irregularly, tends to get easily
decolorised May show clubbing at one or both ends -
Polar bodies/ Metachromatic granules/ volutin or Babes Ernst granules
Metachromatic Granules: made up of polymetaphosphate Bluish purple color with Loeffler’s
Methylene blue Special stains: Albert’s, Neisser’s &
Ponder’s Grows aerobically at 37°C

Dr Ekta, Microbiology14.12.08
Virulence factor
Exotoxin – Diphtheria toxin: Protein in nature very powerful toxin Responsible for all pathogenic
effects of the bacilli Produced by all the virulent
strains Two fragments A & B

Dr Ekta, Microbiology14.12.08
Diphtheria toxin – Mechanism of action
Fragment A – inhibits polypeptide chain elongation by inactivating
the Elongation factor EF 2 in the presence of NAD
DT - Acts by inhibition of protein synthesis

Dr Ekta, Microbiology14.12.08
Diphtheria Toxin Toxigenicity can be induced by Lysogenic or phage
conversion – corynephages (tox+ phage) or beta phages
Can be toxoided by -1. Prolonged storage2. Incubation at 37°C for 4 - 6 weeks3. Treatment with 0.2 – 0.4 % formalin or4. Acid pH.
Stain used for toxin production – ‘Park Williams 8’ strain
Antibodies to fragment B - protective

Dr Ekta, Microbiology14.12.08
Epidemiology Habitat – nose, throat, nasopharynx & skin of carriers and patients
Spread by respiratory droplets, usually by convalescent or asymptomatic carriers
Nasal carriers harbour the bacilli for longer time than pharyngeal carriers
Local infection of throat - toxemia
Incubation period of diphtheria – 3 to 4 days
In tropics, cutaneous infection is more common than respiratory infection

Dr Ekta, Microbiology14.12.08
Diphtheria
Site of infection 1. Faucial (palatine tonsil) – commonest type2. Laryngeal3. Nasal4. Otitic5. Conjunctival6. Genital – vulval, vaginal, prepucial7. Cutaneous – usually a secondary infection on pre-
existing lesion, caused by non toxigenic strains

Dr Ekta, Microbiology14.12.08
Pathogenesis & Clinical Manifestations Human Disease
1. Usually begins in respiratory tract 2. Virulent diphtheria bacilli lodge in throat of
susceptible individual 3. Multiply in superficial layers of mucous
membrane 4. Elaborate toxin which causes necrosis of
neighboring tissue cells 5. Inflammatory response eventually results in
pseudomembrane (fibrinous exudate with disintegrating epithelial cells, leucocytes, erythrocytes & bacteria)
Usually appears first on tonsils or posterior pharynx and spreads upward or down
In laryngeal diphtheria, mechanical obstruction may cause suffocation
Regional lymphnodes in neck often enlarged (bull neck)

Dr Ekta, Microbiology14.12.08

Dr Ekta, Microbiology14.12.08
Diphtheria - Clinical Classification Based on the severity of clinical presentation:
1. Malignant or hypertoxic – severe toxemia with marked adenitis
2. Septic – ulceration, cellulitis, & gangrene around the pseudomembrane
3. Hemorrhagic – bleeding from the edge of membrane, epistaxis, conjunctival hemorrahge, purpura & generalized bleeding tendency.

Dr Ekta, Microbiology14.12.08
Complications of diphtheria
Mechanical complications are due to the pseudomembrane, while the systemic effects are due to the toxin.
1. Asphyxia – due to obstruction of respiratory passage
2. Acute circulatory failure 3. Postdiphtheritic paralysis – occurs in 3rd or 4th week
of disease, palatine & ciliary, spontaneous recovery
4. Sepsis – pneumonia & otitis media

Dr Ekta, Microbiology14.12.08

Dr Ekta, Microbiology14.12.08
Laboratory Diagnosis Specimen – swab from the
lesions
1. Microscopy Gram stain: Gram +ve bacilli,
chinese letter pattern Immunofluorescence Albert’s stain for
metachromatic granules

Dr Ekta, Microbiology14.12.08
Laboratory Diagnosis
2. Culture – isolation of bacilli requires media enriched with blood, serum or egg
a. Blood agar
b. Loeffler’s serum slope – rapid growth, 6 to 8 hrs
c. Tellurite blood agar – tellurite is reduced to tellurium, gives gray or black color to the colonies
d. Hoyle’s media modifications of TBA
e. McLeod’s media

Dr Ekta, Microbiology14.12.08
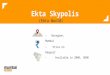
Growth of diphtheria bacilli
Blood agar
Loeffler’s serum slope
Tellurite blood agar

Dr Ekta, Microbiology14.12.08
Biotypes of Diphtheria bacilli Based on colony morphology on the tellurite medium & other
properties, McLeod classified diphtheria bacilli into three types:
Features 1. Gravis 2. Intermedius 3. Mitis
Case fatality rate High High Low
Complications Paralytic, hemorrhagic
Hemorrhagic Obstructive
Predominance In epidemic areas Epidemic areas Endemic areas
Spread Rapid Rapidly than mitis Less rapid
Colony on TBA ‘Daisy head” colony
‘Frog’s egg colony
‘Poached egg’ colony
Hemolysis Variable Nonhemolytic Usually hemolytic

Dr Ekta, Microbiology14.12.08
Laboratory Diagnosis
3. Biochemical reactions a. Hiss's serum water - ferments sugar with acid
formation but not Gasferments: glucose, galactose, maltose and dextrin
b. Resistant to light, desiccation and freezing
c. Sterilization: sensitive to heat (destroyed in 10mins at 58°C or 1min in 100°C), chemical disinfectants

Dr Ekta, Microbiology14.12.08
Laboratory Diagnosis
4. Virulence tests - Test for toxigenicityA. Invivo tests – animal inoculation (guinea
pigs)a. Subcutaneous test
b. Intracutaneous test
B. Invitro testsa. Elek’s gel precipitation test
b. Tissue culture test

Dr Ekta, Microbiology14.12.08
Laboratory Diagnosis Virulence tests - Invivo tests Bacterial growth from Loeffler’s serum slope is emulsified in 2-4 ml
broth. Two guinea pigs (GP A and GP B)
I. Subcutaneous test – 0.1 ml of emulsion is injected SC into each guinea pig
GP A - has diphtheria antitoxin (500 units injected 18 to 24 hours before) GP B - Doesn't have antitoxin
II. Intracutaneous test - 0.1 ml of emulsion is injected IC into each guinea pig
GP A - has diphtheria antitoxin (500 units injected 18 to 24 hours before) GP B – 50 units of antitoxin IP four hrs after the skin test

Dr Ekta, Microbiology14.12.08
Laboratory Diagnosis
Virulence tests - Invitro tests
I. Elek's gel precipitation test filter paper saturated with antitoxin (1000units/ ml) is placed on
agar plate with 20% horse serum bacterial culture streaked at right angles to filter paper

Dr Ekta, Microbiology14.12.08
Laboratory Diagnosis
Virulence tests - Invitro tests
II. Tissue culture test- incorporation of bacteria into agar overlay of eukaryotic cell culture monolayers.
Result: toxin diffuses into cells and kills them

Dr Ekta, Microbiology14.12.08
Treatment
specific treatment must not be delayed if clinical picture suggests of diphtheria
rapid suppression of toxin-producing bacteria with antimicrobial drugs (penicillin or erythromycin)
early administration of antitoxin: 20,000 to 1,00,000 units for serious cases, half the dose being given IV

Dr Ekta, Microbiology14.12.08
Prophylaxis
1) Active Immunization (Vaccination)
i. Formol toxoid (fluid toxoid) incubation of toxin with 0.3% formalin at pH 7.4 - 7.6 at
37°C for 3 to 4 weeks fluid toxoid is purified and standardized in flocculating
units (Lf doses)
ii. Adsorbed toxoid (more immunogenic than fluid toxoid) purified toxoid adsorbed onto insoluble aluminium
phosphate or aluminium hydroxide given IM (DTP or TD)

Dr Ekta, Microbiology14.12.08
Prophylaxis Adsorbed Toxoid
a. DPT - triple vaccine given to children; contains diphtheria toxoid, Tetanus toxoid and pertussis vaccine
b. DaT - contains absorbed tetanus and ten-fold smaller dose of diphtheria toxoid. (smaller dose used to diminish likelihood of adverse reactions)
Schedulei) Primary immunization - infants and children
- 3 doses, 4-6 weeks interval- 4th dose after a year- booster at school entry
ii) Booster immunization - adults-Td toxoids used (travelling adults may need more)
SHICK test - to test susceptibility to vaccine, not done now-a-days

Dr Ekta, Microbiology14.12.08
Prophylaxis2. Passive immunization
ADS (Antidiphtheritic serum, antitoxin) - made from horse serum- 500 to1000 units subcutaneously
3. Combined immunizationFirst dose of adsorbed toxoid + ADS, to be continued by the full course of active immunisation

Dr Ekta, Microbiology14.12.08
CONTROL
1. isolate patients
2. treat with antibiotics actively
3. complete vaccination schedule should be used with booster every 5 years

Dr Ekta, Microbiology14.12.08
Other Corynebacteria
C. ulcerans – diphtheria like lesions in guinea pigs & cows, may get transmitted to humans by cow’s milk
Diphtheroids – Normal commensals of nose, throat, nasopharynx, skin, urinary
tract & conjunctiva Stain uniformly Few or no metachromatic granules Arranged in parallel rows (palisades) Nontoxigenic