Embed Size (px)
Citation preview

J. Eduardo Rame MD MPhil
Director of Mechanical Circulatory Support
University of Pennsylvania Health System
Trasplante Cardiopulmonar
State of the art, Rol actual,
condiciones del candidato y
resultados

Presenter Disclosure Information
•I will discuss off label/ investigational use in my presentation: HeartWareHVAD
•I have financial relationships to disclose:
•Research support from:
Thoratec Corporation – PI of HM II Trial (ROADMAP) and HMIII (MOMENTUM) and National co- PI of Re_STAGE HF
HeartWare Corporation – PI of HVAD Trial (ENDURANCE)

S 𝒊ntesis
• Desde que el primer trasplante de corazón - pulmón exitoso fue realizado por Norm Shumway, John Wallwork y Bruce Reitz en 1981 por Hipertensión Arterial Pulmonar, esta terapia avanzada ha evolucionado para proporcionar beneficio en pacientes con enfermedad cardiopulmonar avanzada.
• Con el advenimiento de terapias para la hipertensión arterial pulmonar, incluyendo antagonistas de la endotelina, agonistas y análogos de la prostaciclina y terapias de selección de óxido nítrico, el trasplante de pulmón se ha convertido en el procedimiento de elección para la hipertensión pulmonar avanzada. Con las terapias dirigidas a la hipertensión arterial pulmonar, la función cardíaca derecha está más preservada permitiendo el trasplante de pulmón para ser suficiente

S 𝒊ntesis-2
• Sin embargo, la hipertensión arterial pulmonar y la cardiopatía congénita cianótica siguen siendo la principal indicación para el trasplante combinado de corazón y pulmón
• En los pacientes con cardiopatía congénita avanzada, especialmente aquellos que requieren reparación del corazón nativo (defecto del septo ventricular con Eisenmenger) o con disfunción ventricular derecha profunda y dilatación, el trasplante corazón - pulmón ha demostrado ofrecer una supervivencia superior en el candidato apropiado.

S 𝒊ntesis - 3
• Selección de Pacientes: Hemos aprendido de manera difícil que la probabilidad de supervivencia y rehabilitación exitosa después de HLTxen pacientes que están excesivamente enfermos y debilitados es menor que después del trasplante de otros órganos (trasplante de un solo órgano)
• La mortalidad en el primer año es alta, hasta 30 a 40 por ciento. Las causas más comunes de muerte en el período inicial de 30 días se deben a fracaso de aloinjerto post-trasplante, complicaciones técnicas e infección, mientras que el síndrome de bronquiolitis obliterante (BOS) y la disfunción crónica del injerto pulmonar (CLAD) siguen siendo las principales causas de mortalidad después 1 año. Así, la morbilidad y mortalidad del trasplante de corazón-pulmón es impulsada por los pulmones
• Comparando la década más reciente (2002-2013) con la década inicial (1982-1991), la proporción de pacientes sometidos a HLTx para la enfermedad cardiovascular adquirida ha aumentado progresivamente (de 2,6 a 10,6%), mientras que el número de pacientes con CF sometidos al trasplante de corazón y pulmón ha disminuido (6,8 frente a 17,2%), más en Estados Unidos que en Europa

Mary Gohlke, March 9 1981
Bruce Reitz. The first successful combined heart–lung transplantation, Journal of Thoracic and Cardiovascular Surgery 2011
• End –Stage PPH (iPAH)
• Noted Pre Prostacyclin Era
• Two early rejections diagnosed by cardiac biopsy
• Several years later –asynchronous heart and lung rejection more common (serial bronchoscopy)
• Second patient, Eisenmengerdue to VSD, unrepaired (May 1981)

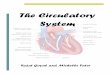
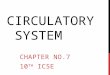
Adult Heart-Lung TransplantsNumber of Transplants Reported by Year
0
50
100
150
200
250
300
Nu
mb
er o
f Tr
ansp
lan
ts
NOTE: This figure includes only the heart-lung transplants that are reported to the ISHLT Transplant Registry. As such, this should not be construed as evidence that the number of heart-lung transplants worldwide has declined in recent years.
2016JHLT. 2016 Oct; 35(10): 1149-1205

Diagnosis N (%)
CHD 1,203 (35.4%)
PAH 931 (27.4%)
CF 460 (13.5%)
CM 193 (5.7%)
COPD 141 (4.2%)
ILD 131 (3.9%)
A1ATD 63 (1.9%)
Sarcoidosis 58 (1.7%)
Retransplant 57 (1.7%)
Bronchiectasis 31 (0.9%)
OB (non-Retransplant) 26 (0.8%)
Other 103 (3.0%)
Adult Heart-Lung TransplantsDiagnosis (Transplants: January 1982 – June 2015)
2016JHLT. 2016 Oct; 35(10): 1149-1205

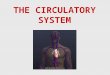
Adult Heart-Lung TransplantsMajor Indications by Year (%)
0
10
20
30
40
50
60
70
80
90
100
% o
f Tr
ansp
lan
ts
Transplant Year
CHD PAH CF CM COPD ILD
Since only major indications are shown, sum of percentages for each year is less than 100%.
2016JHLT. 2016 Oct; 35(10): 1149-1205

Adult Heart-Lung TransplantsMajor Indications by Year (Number)
0
20
40
60
80
100
120
140
160
180
Nu
mb
er o
f Tr
ansp
lan
ts
Transplant Year
CHD PAH CF CM COPD ILD
2016JHLT. 2016 Oct; 35(10): 1149-1205
• Increased confidence in double lung transplantation for PAH and CF
• Not clear why HLTx for CHD are down in numbers (expertise?)

Beyond Indication: Patient Selection
• Ideally, patients who are ambulatory with excellent end-organ function and YOUNG should be considered
• In idiopathic PAH – a recent study demonstrated comparable survival with HLTx and Dual Lung Tx –except in patients hospitalized in the ICU with critical illness/shockincreased survival with HLTx in this group
• In Eisenmenger’s with unrepaired shunt (especially VSD) study identified HLTx to be superior to bilateral lung transplantation (PGD and unmasked left ventricular dysfunction and pulmonary venous congestion)

(N = 1,659)
Risk Factors For 1 Year Mortality with 95% Confidence Limits
Adult Heart-Lung Transplants (1997-6/2014)
2016JHLT. 2016 Oct; 35(10): 1149-1205

0,5
1,0
1,5
2,0
2,5
3,0
15 20 25 30 35 40 45 50 55 60
Haz
ard
Rat
io o
f 1
Yea
r M
ort
alit
y
Donor age
p = 0.0168
(N = 1,659)
Donor age
Risk Factors For 1 Year Mortality with 95% Confidence Limits
Adult Heart-Lung Transplants (1997-6/2014)
2016JHLT. 2016 Oct; 35(10): 1149-1205

J. Eduardo Rame, Chronic Heart Failure: A Reversible Metabolic Syndrome? Circulation June 2012
Chokshi, et al. Circulation, 2012. 125(23): p. 2844-53

Candidate Selection Case 1: Complex Congenital Heart Disease with Severe Pulmonary Hypertension
• 45 female, L-type (congenitally corrected) Transposition of great arteries, repaired secundum ASD, mechanical TVR for systemic A-V valveheart block post PPM and severe pulmonary hypertension (WHO Group I and II with associated CHD)
• 2014 Diagnosis of systemic PH: RA 22, PA 120/55 (81), PWP 20, CO/CI 2.77/ 1.6) PVR 18.3
• Vasoreactive to inhaled flolan with PVR drop to 7 Wood Units and increase in PWP 31 mmHg to 40 mmHg and increase in Cardiac index form 1.6 to 2.0
• After 2 years of Sildenafil 80mg tid she began to rapidly decline with heart failure and cyanosis and cachexia and sarcopenia

Candidate Selection Case 1: Complex Congenital Heart Disease with Severe Pulmonary Hypertension
• Congestive hepatopathy : Liver biopsy consistent with venous outflow obstruction no fibrosis
• Cachexia and sarcopenia:– Prealbumin 7 improved to
18 after 3 months of restored Cardiac output and high caloric intake
– Weight increased by 8lbs (4%)
• Congenital Heart Disease with previous surgery (TVR and repaired secundumASD)

0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Surv
ival
(%
)
Years
2016JHLT. 2016 Oct; 35(10): 1149-1205
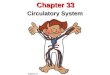
Adult Heart-Lung TransplantsKaplan-Meier Survival
• Median survival = 3.3 years• Conditional median survival = 10.3 years
N = 3,831
(Transplants: January 1982 – June 2014)
• 71% 3 months posttransplant, • 63% 1 year posttransplant, • 52% 3 years posttransplant,• 45% 5 years posttransplant, • 32% at 10 years posttransplant

0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Surv
ival
(%
)
Years
1982-1993 (N=1,596)
1994-2003 (N=1,392)
2004-6/2014 (N=843)
2016JHLT. 2016 Oct; 35(10): 1149-1205
Adult Heart-Lung TransplantsKaplan-Meier Survival by Era
Median survival (years):1982-1993=2.1; Conditional 1 year survival 91994-2003=3.9; Conditional 1 year survival 11.52004-6/2014=5.8; Conditional median survival (years)
1982-1993 vs. 1994-2003: p<0.00011982-1993 vs. 2004-6/2014: p<0.00011994-2003 vs. 2004-6/2014: p=0.0432
(Transplants: January 1982 – June 2014)

0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Surv
ival
(%
)
Years
CM (N=168) CF (N=375) CHD (N=1,016)
COPD (N=102) ILD (N=99) PAH (N=695)
2016JHLT. 2016 Oct; 35(10): 1149-1205
Adult Heart-Lung TransplantsKaplan-Meier Survival by Diagnosis
Median survival (years):CM=2.3 yearsCF=5.7 yearsCHD=4.8 yearsCOPD=2.7 yearsILD=2.4 yearsPAH=4.5 years
No pair-wise comparisons were significant at p < 0.05 except CF vs. COPD
(Transplants: January 1990 – June 2014)

0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Surv
ival
(%
)
Years
CM (N=89) CF (N=261) CHD (N=649)
COPD (N=61) ILD (N=59) PAH (N=470)
2016JHLT. 2016 Oct; 35(10): 1149-1205
Adult Heart-Lung TransplantsKaplan-Meier Survival by Diagnosis Conditional on Survival
to 1 Year
Median survival (years):CM=9.5; CF=11.8; CHD=12.2; COPD=6.2; ILD=8.3; PAH=10.4
No pair-wise comparisons were significant at p < 0.05
(Transplants: January 1990 – June 2014)

• Survival after heart–lung transplant has improved with transplant era, such that median survival for patients transplanted in the last decade has improved to 5.8 years with a median survival of >10 years conditional to survival 1 year after transplant.
• Clearly there is a very significant upfront cost the first year with mortality up to 45% this first year (Cardiomyopathy with elevated PVR); 36% (CHD); 31% (PAH)
• In comparison with lung-only transplantation, primary heart-lung transplantation has a more pronounced early mortality but better long-term survival.
• When survival after heart–lung transplant is stratified by diagnosis, younger patients transplanted for CF, PAH and CHD have better survival as compared with those transplanted for COPD and cardiomyopathy
Professor Christian Bermudez
Summary : Survival after Heart and Lung Tx

• For heart–lung transplant recipients who have the 2 most common diagnostic indications (CHD and PAH)
– The most common identifiable causes of death in the first 30 days post-transplant are graft failure (lung or heart) and technical complications
– Acute graft failure appears to occur more frequently among HLTxpatients compared to isolated lung transplantation or heart transplantation. ISHLT data noted HLTx recipients had higher rates of early graft failure (6.8% vs 2.3%), which is defined as intrinsic graft failure resulting in death or retransplantation in the first 30 days following transplantation. A possible explanation: HLTx recipients are at risk for both primary cardiac and lung allograft failures, the etiologies of which have not been fully elucidated
– After the first year, obliterative bronchiolitis (OB) / bronchiolitis obliterans syndrome (BOS), late graft failure (lung or heart), and non-CMV infections are the most common causes of mortality. Cardiovascular causes of death account for a small, but important proportion of deaths
Professor Christian Bermudez
Summary : Survival after Heart and Lung Tx

0
10
20
30
40
0-30 Days (N=447) 31 Days - 1 Year(N=350)
>1-3 Years (N=283) >3-5 Years (N=171) >5 Years (N=495)
% o
f D
eat
hs
OB/BOS Infection (non-CMV) Graft Failure Cardiovascular Technical
2016JHLT. 2016 Oct; 35(10): 1149-1205
Adult Heart-Lung TransplantsRelative Incidence of Leading Causes of Death
(Deaths: January 1992 – June 2014)

• HLTx patients are at higher risk for certain mechanical complications due to the nature of the surgical procedure:
– Phrenic nerve dysfunction: A retrospective review noted a higher rate of PND in HLTx compared to LTx recipients (42.8% vs 9.3%, respectively). These patients also required longer mechanical ventilation and ICU length of stay (p < 0.005)
– Severe gastroparesis from vagus nerve disruption (proximity to tracheal anastomosis)
– Chylothorax—especially in CHD patients with abnormal lymphatic drainage
Early Survival after HLTx: Technical Complications

0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10
Bro
nch
iolit
is O
blit
era
ns
Syn
dro
me-
Free
Su
rviv
al (
%)
Years
CHD (N=210) PAH (N=122)
2016JHLT. 2016 Oct; 35(10): 1149-1205
Adult Heart-Lung TransplantsBronchiolitis Obliterans Syndrome-Free Survival by Diagnosis
(Transplants: January 1994 – June 2014)
p = 0.2491

0
25
50
75
100
0 1 2 3 4 5 6 7 8 9
CA
V-F
ree
Su
rviv
al (
%)
Years
CHD (N=181) PAH (N=100)
2016JHLT. 2016 Oct; 35(10): 1149-1205
Adult Heart-Lung TransplantsCoronary Artery Vasculopathy-Free Survival by Diagnosis
(Transplants: January 1994 – June 2014)
p = 0.0327
CAV less common in HLTx as compared to Heart Transplanation (Protection from Pulmonary Graft)

Cardiac Allograft Protection by Lung Allograft
Stanford Experience: • Number of rejection episodes predictive of
outcome (median survival for no rejection: 8.6 years)
• Number of HLA-DR mismatches (new antibodies) directly correlated with the number of acute rejection episodes within the first year, and hence patient survival.
J HeartLungTransplant2014;33:636–643
N=79N=141
1996-2006: Rennes and Paris Sud• Acute Rejection
only predictor
Ann Thorac Surg 2010;90:329 –37

Immunosuppresion and Antimicrobial Prophylaxis: Reflected in Stanford
Experience
Ann Thorac Surg 2010;90:329 –37

Surveillance of Graft Function and Sub-Clinical Rejection
• Cardiac Allograft Function: Scheduled routine 2D echocardiography– Rates of cardiac allograft rejection are low so routine
endomyocardial biopsy is not performed– Dobutamine stress echocardiograms annually
(coronary angiography if positive or symptoms)
• Lung Allograft (Susceptible Organ)– Surveillance bronchoscopy with transbronchial
biopsies as per Lung Tx protocol– Spirometry: Reduction in FEV1more than 10% --
possible rejection -- protocol to rule out infections and biopsy for decision on rejection
Ann Thorac Surg 2010;90:329 –37

0
10
20
30
40
50
60
70
80
90
100
% o
f P
atie
nts
Any induction Polyclonal ALG/ATG IL-2R Antagonist
Analysis is limited to patients who were alive at the time of the discharge.
2016JHLT. 2016 Oct; 35(10): 1149-1205
Adult Heart-Lung Transplants Induction Immunosuppression
(Transplants: January 2004 – December 2014)

0
20
40
60
80
100
Cyclosporine Tacrolimus Sirolimus/Everolimus
MMF/MPA Azathioprine Prednisone
% o
f P
atie
nts
Year 1 (N=230) Year 5 (N=121)
Analysis is limited to patients who were alive at the time of the follow-up.
NOTE: Different patients are analyzed in Year 1 and Year 5
2016JHLT. 2016 Oct; 35(10): 1149-1205
Adult Heart-Lung Transplants Maintenance Immunosuppression at Time of Follow-up
(Follow-ups: January 2004 – June 2015)

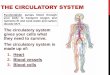
Adult Heart-Lung TransplantsCumulative Post Transplant Morbidity Rates in Survivors within 1 and 5
Years (Transplants: January 1994 – June 2014)
OutcomeWithin 1 Year
Total number with known
response
Within 5 Years
Total number with known
response
Hypertension 59.1% (N=433) 87.2% (N=180)
Renal Dysfunction 19.6% (N=496) 42.6% (N=235)
Abnormal Creatinine ≤ 2.5 mg/dl 11.9% 28.1%
Creatinine > 2.5 mg/dl 3.2% 10.6%
Chronic Dialysis 4.2% 3.0%
Renal Transplant 0.2% 0.9%
Hyperlipidemia 28.0% (N=453) 70.4% (N=189)
Diabetes 17.7% (N=508) 28.7% (N=247)
Coronary Artery Vasculopathy 3.0% (N=396) 7.5% (N=120)
Bronchiolitis Obliterans Syndrome 7.5% (N=466) 30.7% (N=205)
2016JHLT. 2016 Oct; 35(10): 1149-1205

• 36 year old college counselor
• Diagnosed 3 months ago with PAH
• Workup revealed this to be iPAH
• Progressive symptoms, including several spells of syncope
• In office, low pulse volume, pulsus alternans
Case Presentation 2: Newly Diagnosed Idiopathic Pulmonary Arterial Hypertension With Cardiogenic Shock







FICK CO: 1.8 (CI = 1.1 L/min/m2) ; Mixed Venous Saturation 41%

Followup
• Flolan initiated with retained PA line in the ICU• Patient tolerating this well and improving• On post hospitalization day 2 code blue was called
for loss of consciousness at the time of radial arterial line placement
• CPR x 3 minutes; epi x 2; no intubation• Systolic arterial pressure = 70; PA 110/30; Mixed
venous saturation 30% = CO 1.3 l/min• Patient kept supine, with high oxygen and NO
delivery on epinephrine drip 0.08 mcg/kg/min

Followup
• Taken to the OR for central cannulation of ECLS circuit (extra corporal life support)– ECMO (blood drawn from RA to pump to oxygenator
and back to patient – proximal aorta)
– Hemodynamics: Systolic arterial pressure 120, CO 4.6 liters minute (pump flow; i.e. bypassing lung circuit), PA 28/15
– Ambulatory on central VA ECMO; heart – lung transplantation 2 weeks later
– Doing well almost 10 years post heart and lung transplantation



Adult Heart-Lung Transplantation
Courtesy: Dr. Katherine Kunkel and Professor Joyce Wald2016
JHLT. 2016 Oct; 35(10): 1149-1205
• Increasing the last ten years is the indication of advanced cardiomyopathy with refractory pulmonary vascular disease (third most common indication for HLTx up to 11%)
“Generally, pulmonary vascular resistance greater than 5 Wood units, a pulmonary vascular resistance index greater than 6, or a transpulmonary gradient greater than 16-20 mm Hg despite maximal medical therapy should be considered contraindications for heart transplant alone and should prompt evaluation for HLTx”

ISHLT Listing Criteria for Heart Transplantation
Class I:
1. Right heart catheterization (RHC) should be performed on all
candidates in preparation for listing for cardiac transplantation
and annually until transplantation (Level of Evidence: C).
2. RHC should be perfomed at 3- to 6-month intervals in listed
patients, especially in the presence of reversible pulmonary
hypertension or worsening of heart failure symptoms) (Level of
Evidence: C).
3. A vasodilator challenge should be administered when the
pulmonary artery systolic pressure is 50 mm Hg and either the
transpulmonary gradient (TPG) is greater than 15 or the
pulmonary vascular resistance (PVR) is 3Wood units while
maintaining a systolic arterial blood pressure 85 mm Hg (Level
of Evidence: C).
Class I (cont’d)
4. When an acute vasodilator challenge is unsuccessful, hospitalization with continuous hemodynamic monitoring should be performed, as often the PVR will decline after 24 to 48 hours of treatment consisting of diuretics, inotropes and vasoactive agents such as inhaled nitric oxide (Level of Evidence: C).
Class IIb
1. If medical therapy fails to achieve acceptable hemodynamics and, if the left ventricle cannot be effectively unloaded with mechanical adjuncts, including an intra-aortic balloon pump (IABP) and/or left ventricular assist device (LVAD), it is reasonable to conclude that the pulmonary hypertension is irreversible (Level of Evidence: C).
If THAT is ALL….Why do contemporary registry data continue to show that up to 20% of early mortality post OHTx is due to RIGHT HEART FAILURE ?
Mehra, et al. Journal Heart and Lung Transplantation 2006, Updated January 2016
Rame, JE. AHA Scientific Sessions 2016. Heart Transplant Selection “What to Do with Pulmonary Hypertension”

Mechanics of Allografted Right Ventricle
Abel FL, Waldhausen JA. Thorac Cardiovasc Surg.1967;54:886–894.
RVALLO ?
Rame, JE. AHA Scientific Sessions 2016. Heart Transplant Selection “What to Do with Pulmonary Hypertension”

Mechanics of Allografted RV:RV Coupled to What LOAD?
RESISTIVE LOAD PULSATILE LOAD
Pulmonary Vascular ResistancePVR = mPAP – PCWP
CO
Pulmonary Arterial CompliancePAC = SV
PASP – PADP
Transpulmonary GradientTPG = mPAP – PCWP
PA Diastolic to Wedge Pressure GradientDPG = PADP - PCWP
Courtesy , Will Grandin MD MSc.
Rame, JE. AHA Scientific Sessions 2016. Heart Transplant Selection “What to Do with Pulmonary Hypertension”

Relationship Between PVR and Pumonary Artery Compliance (PAC)
Adapted from Tedford, Circulation 2012, Courtesy of EW Grandin
1.7 WU 8.3 WU
PAH
Normals
LHD-PH: Spectrum of
PAC
5 WU

• Pre-Transplant Hemodynamics Do Matter,
even in those patients deemed acceptable
for OHTx ({PVR < 2.5 Wood Units)
• Not included any data on “prophylactic”
treatment of high risk patients in the peri-
operative and post – operative period
– Heterotopic Heart Transplantation
– Prostaglandin E1 being trialed to improve
outcomes
Pre - OHTx Parameters of Pulmonary Vascular Resistance,
Not Compliance Have Been Reported
A. Costard-Jaeckle and Michael Fowler, JACC 1991
Reversible PVR and SBP>85mm
PVR < 2.5
Reversible PVR and SBP < 85mm
RHF
PVR not reversible Rame, JE. AHA Scientific Sessions 2016. Heart Transplant Selection “What to Do with Pulmonary Hypertension”

Paradigm 2 : “Reversible but Risky” – Vasoreactive PH is a facet of advanced HF • Report from 182 patients
transplanted with either baseline PVR<2.5 Wood Units or demonstrated to reverse to PVR < 2.5
• From this analysis by Butler et al, there is a strong signal for increased mortality in patients with PAS > 50 mm Hg at the time of the baseline RHC.
Javed Butler, et al. , Journal Heart Lung Transplant 2005
Residual Risk

Pulmonary Hypertension with PVR: The Driver to Bridge Patients with LVAD

Risk Despite Reversibility with LVAD:
Columbia Experience
53
Tsukashita…Naka. Effect of pulmonary vascular resistance prior to left ventricular assist device implantation on short- and long-term post-transplant survival. J Thoracic and CV Surgery. 2015
• Three – fold increased risk of post-OHTx30-day mortality [5.8% vs 20.7%, p<0.05]• 40% of high PVR on Sildenafil/Tadalafil, versus 19% in low PVR group (p=0.17)
PVR > 5 Wood Units (pre-LVAD)

• Despite PVR reduction with LVAD support, reversal of pulmonary vascular remodeling is heterogeneous or incomplete• Pulmonary arteriopathy that remains may provide a substrate for a PH crisis triggered by perioperative insults, including insulin resistance from CPB and depletion of nitric oxide associated with the transfusion of stored packed red cells.

Paradigm 3: Optimizing RVA – PAR
Coupling
RVA
PA
R
Sorel Goland, et al. , Journal Heart Lung Transplant 2007
• No Heterotopic Heart Transplantation• Oversized Donor Heart Procurement : RVA Mass• Loss of Longitudinal Shortening/TAPSE in Allografted RV• RV Load: Perioperative iNO, long term PDE5i

Candidate Selection Case 3: End-Stage Cardiomyopathy with Associated Pulmonary Vascular Disease in 22 yr old Scleroderma Man
• 26 year old male with Scleroderma, initially presenting with Raynaud’s syndrome in 2013. Developed progressive dyspnea at a rapid pace
• Biventricular dysfunction: 2015 cMRI dilated RA/RV (RVEDVI=160ml/m2), RVEF 21%; LVEDVI=96ml/m2; LVEF=31%. Sub-endocardial to mid-myocardial late gadiniumenhancement/inferolateral wall
• Initiated on ERA (Ambrisentan), Sildenafil, and attempted prostacyclin therapy (Remodulin) but could not tolerate
• On Milrinone since 2015 with refractory bisided failure• No supplemental oxygen and no parenchymal lung disease
identified; FEV1=2.59(60%); FEV1/FVC=93%; TLC = 4.85 (72%) DLCO = 18ml/min-mmHg (53%)
• Hemodynamics (Revatio 60mg tid, Ambrisentan 10mg, Milrinone: RA 7; RV 41/8; PA39/16 (29), PWP 9, TPG 9; C.O 3.76, CI 2.39; PVR = 5.31

Candidate Selection Case 3: End-Stage Cardiomyopathy with Associated Pulmonary Vascular Disease in 22 yr old Scleroderma
Man
• Scleroderma Myositis (Cellcept, methotrexate since 2014) –now compensated
• Esophageal Dysmotility(pre-Barret’s pathology on EGD/biopsy)
• Right pleural effusion, recurrent (transudative)
• Ventricular tachycardia

Conclusions
• Heart-lung transplantation is an established treatment option for patients suffering from cardiopulmonary disease who are not candidates for isolated heart or lung.
• Unfortunately, as the number of patients considered for thoracic organ transplant has increased with limted organ availability, the current allocation systems have favored single-organ transplantation, limiting options and experience for HLTx
• The outcomes in the most recent era have been associated with up to 40% survival 10 years posttransplant with excellent quality of life especially in YOUNG and otherwise robust candidates
• Early mortality is significant (PGD) and late morbidity and mortality is driven by lung pathology (OB/BOS)

Muchas Gracias!
• Michael Acker• Christian Bermudez• Pavan Atluri
• Mariell Jessup• Joyce Wald• Rhondalyn McLean• Anjalie Owens• Sue Brozena• Ken Margulies• Lee Goldberg• Tom Cappola
• Josef Stehlek
• Duane Davis
• Charles Hoopes
• James Kirklin