Embed Size (px)
Citation preview

Journal ofNeurology, Neurosurgery, and Psychiatry, 1978, 41, 972-979
Coincidental aneurysms with tumours of pituitaryorigin
JAN JAKUBOWSKI AND BRIAN KENDALL
From the Gough Cooper Department of Neurological Surgery, Lysholm Radiological Department,The National Hospital for Nervous Diseases, Queen Square, and the Neurosurgical and RadiologicalDepartments, The Middlesex Hospital, London
SUMMARY Angiographic studies on 150 pituitary adenomas and 33 craniopharyngiomaspresenting for surgical treatment are reviewed. Eleven incidental silent aneurysms (four arisingfrom the intracavernous and four from the supraclinoid carotid artery, and three from theanterior cerebral artery complex) are shown. Intracavernous aneurysms were also present intwo acromegalic patients who had been treated previously with yttrium implantation. Althoughencasement of vessels by these tumours is unusual, the relevance of vascular abnormalities tosurgical treatment is sufficient to justify routine magnification angiography.
The occurrence of "silent" intracranial aneurysmsis well documented. Housepian and Pool (1958), ina detailed study of the cerebral arteries in 5762necropsy cases collected between 1914 and 1956,found 32 (0.56%) with aneurysms which had re-mained clinically silent. Du Boulay (1965) analysedcarotid angiograms performed for tumour andvascular disease in 2595 cases and found silentaneurysms in 0.27%. However, only 27% of theangiograms were bilateral, and the vertebro-basilar circulation was not outlined. Allowing forincomplete angiography, the incidence in the twostudies is comparable.
Silent intracranial aneurysms located distantfrom the lesion to be treated have little relevanceto surgical management of most patients. How-ever, aneurysms of the major arteries adjacent topituitary and suprasellar tumours are an additionalhazard to surgical treatment. Previous knowledgeof the presence and anatomy of such aneurysmsis important during separation of the tumourcapsule from the major vessels, or removal of anintracavernous extension of a tumour lying closeto the carotid artery.
Giant aneurysms in the parasellar region pre-senting clinically as pituitary tumours are well
Address for reprint requests: Mr J. Jakubowski, Department of Neuro-surgical Studies, The National Hospital, Queen Square, LondonWCIN 3BG.
Accepted 26 May 1978
recognised (Mitchell, 1889; Cushing, 1912; Jeffer-son, 1937; White and Ballantine, 1961; Raymondand Tew, 1978) but silent aneurysms associatedwith symptomatic pituitary and suprasellar tumourshave not received so much attention. Two casesare referred to by Hankinson and Banna (1976),and they, and also Ambrose (1973), consider thatone important reason for routine angiography onthese tumours is to show incidental aneurysms:individual cases are described by Cushing (1912),Love (1963), Lippman et al. (1971) and von Alphen(1975), and illustrated by Gado and Bull (1971).
In general, the tumours are diagnosed clinically,confirmed by plain skull radiographs and theirintracranial extension is assessed by pneumo-encephalography. More recently, computedtomograms with coronal and axial sections havegiven considerable information on the extent andcomposition of these lesions, but many surgeonsstill prefer pneumoencephalograms to assess therelationship of the optic chiasm and nerves beforea transcranial approach. In many neurosurgicalunits angiography is not performed unless thenature of the lesion is uncertain, especially if giantaneurysm or meningioma is suspected. Thenecessity of the procedure to show the preciserelationships of vessels to masses in the pituitaryregion is debatable, but the use of magnificationangiography for this purpose has revealed un-suspected vascular abnormalities with sufficientfrequency to merit discussion.
972
guest. Protected by copyright.
on Septem
ber 23, 2020 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.11.972 on 1 N
ovember 1978. D
ownloaded from

Coincidental aneurysms with tumours of pituitary origin
Patients and methods
We reviewed all proven cases of pituitary adenomaand craniopharyngioma presenting to the Depart-ment of Neurosurgical Studies at The NationalHospital for Nervous Diseases between 1968 and1978 and to the Middlesex Hospital between 1975and 1978, in which angiograms were available.The clinical features, tumour size, and angio-
graphic abnormalities, including the presence anddistribution of aneurysms, and the findings andresults of surgery were noted.
Results
There were 183 cases-150 pituitary adenomas and33 craniopharyngiomas. The histological diagnosis,age and sex distribution, and percentage ofaneurysms are shown in Table 1, and generalangiographic findings in Table 2. The cases re-
ferred for surgery in The National Hospital allhad visual failure, caused by a moderate or largesuprasellar extension. Many Middlesex Hospitalpatients presented with endocrine problems alone,but angiography was not performed in patientsselected for a trans-sphenoid hypophysectomy,which included all cases with a tumour confined tothe sella turcica or with only minor suprasellarextension. Nearly all the angiograms were per-formed to show vascular anatomy adjacent to a
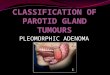
moderate or large suprasellar extension.Occasionally there was clinical doubt about thetype of tumour, and angiography was carried outto elucidate. In one hypertensive acromegalic(case 2), a pneumoencephalogram showed only5 mm suprasellar extension of the tumour, but it
revealed a small mass suggesting an aneurysm(Fig. 1). An angiogram was performed specificallyto confirm this and to exclude other aneurysms.In another acromegalic patient (case 12) who hadbeen previously treated with yttrium implants,pain over the left eye was a prominent symptom,and raised the possibility of intracavernousaneurysm which was confirmed by angiography.Only one other patient had been treated previously,and in no other case were there any symptomsspecifically suggestive of aneurysm.The relevant features of the 11 cases with
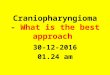
incidental aneurysms are set out in Table 3, andthe distribution of aneurysms is shown in Fig. 2.Their clinical presentation was similar to that ofthe patients without aneurysms. Only one patient(case 2) was hypertensive. In six cases theaneurysm was well seen at surgery, and the angio-graphic data were considered significant to thesafety of the procedure, but only one aneurysm(case 10) was treated. In the other patients,knowledge of the aneurysm was taken intoaccount in surgical planning.Two patients suffering from active acromegaly
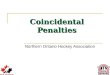
despite previous yttrium implants had aneurysmaldilatation of the cavernous segment of one carotidartery (Fig. 3). These aneurysms were consideredmore likely to be caused by the implant surgeryrather than spontaneous, and are, therefore, notincluded in Table 3.
Discussion
The value of cerebral angiography combined withplain radiographs in the aetiological diagnosis ofsuprasellar tumours is universally accepted.
Table 1 Statistical analysis of presented cases
Number Mean age (SD) Sex Aneurysm(yr)
F M
Chromophobe adenoma 117 48.5 (10.3) 50 67 6 ( 5.1%) -------- **
P<0.005
Eosinophilic or mixed adenoma 29 46.7 (11.4) 13 16 4 (13.8%)+2*=6 (20.7") -Basophilic adenoma 4 45 (8.6) 3 1 -
Craniopharyngioma 33 43 (15.1) 13 10 1
*Associated with previous yttrium implantation.**x test.
Table 2 General angiographic findings
Vessels Displaced Narrowed Occluded Aneurysms
Intracavernous and/or supraclinoid carotid 148 (81 %) 10 (5.4%) 1 10* (5.4°)Anterior cerebral 128 (70.3%) 3 (1.6%) - 3 (1.6%,)Middle cerebral 5 (2.7%) - - 0
*Two associated with previous yttrium implantation.
973
guest. Protected by copyright.
on Septem
ber 23, 2020 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.11.972 on 1 N
ovember 1978. D
ownloaded from

Jan Jakubowski and Brian Kendall
Table 3 Clinical and radiological features and operative findings of cases presented
Patient Histology Clinical picture Radiologicalfindings Site and description of Surgeryaneurysm
Case 1 Eosinophilic adenoma Visual failure Large eroded sella L. ophthalmic junction Radical removal
Eosinophilic adenoma
Mixed adenoma
Eosinophilic adenoma
Chromophobe adenoma
Chromophobe adenoma
3 years;amenorrhea 1 year;acromegaly.
Acromegaly 5 years;hypertension5 years;headache 5 years;BP 180/1 10 mmHg.Carpal tunnel syn.1 year;galactorrhoea on/off;mild acromegaly;visual deficits.
10 mm suprasellarextension, elevatedchiasmatic recess.L. ACA elevated. L.ICA displaced laterally.Sella expanded anderoded, mass in sphenoidsinus 5 mm suprasellarextension.
Eroded sella 25 mmlobulated extensionthird ventricleelevated. ICAdisplaced laterally.L. ACA elevated, R.ACA absent.
Acromegaly 10 Large sella, destroyedyears; floor, 15 mm supra-headache 1 year. sellar extension.
L. ICA displacedlaterally.
Visual failure8 months;headache 10 years.
Hypopituitarism2 years;visual failure2 months.
Destruction of sella30 mm suprasellarextension, thirdventricle indented.Cavernous and supra-clinoid ICA displacedlaterally. ACA elevated.Enlarged eroded sella25 mm suprasellarextension, thirdventricle indented.L. cavernous carotidlat.R. carotid occluded.
5 mm diameter, projecting of the tumour.superiorly. Aneurysm seen
and avoided.
Anterior communicating10 mm diameter,projecting inferiorly.Fig. 1
L. cavernous carotidartery 4 mm diameterprojecting inferiorly.Fig. 4
R. intracavernouscarotid artery, 5 mmdiameter, projectingmedially and anteriorly.
R. ophthalmic junction4 mm diameterprojecting medially.Fig. 5
L. anterior cerebral3 mm diameter.Projecting superiorly.Fig. 6
Trans-sphenoid.
Partial removalof the tumour.Aneurysm notseen. Smallpart of L.cavernous sinusextension wasleft in situ.Radical removalof the tumour.Aneurysm notseen.
Radical removalof the tumour.Aneurysm notseen.
Partial removalof tumour.Aneurysm notseen, part oftumour erodingcavernoussinus leftin situ.
Fig. 1 Case 2. Pneumoencephalogram: erect lateraltomogram. Slight suprasellar extension of pituitarytumour (long arrows). Slightly lobulated anteriorcommunicating aneurysm (arrow heads). Anteriorcerebral arteries indicated by short arrows.
974
PPF 36 yr
Case 2PJM 57 yr
Case 3EEM45yr
Case 4CwM 64 yr
Case 5FMF 46 yr
Case 6LCM 47 yr
guest. Protected by copyright.
on Septem
ber 23, 2020 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.11.972 on 1 N
ovember 1978. D
ownloaded from

Coincidental aneurvsms with tumours of pituitary origin
Table 3 Clinical and radiological features and operative findings of cases presented (continued)
Patient Histology Clinical picture Radiologicalfindings Site and description of Sutrgeryaneurysm
Case 7 Chromophobe adenoma Visual failure Large eroded sella R. distal carotid Partial removalEH 18 months; 25 mm suprasellar artery 8 mm diameter of the tumour.M 53 yr hypopituitary extension. Anterior part projecting superiorly Aneurysm seen,
syndrome. of third ventricle and anteriorly. capsuleindented ACA Fig. 7 attached toelevated (L. hypoplastic). aneurysm leftICA displaced in situ.laterally.
Case 8 Chromophobe adenoma Hypopituitarism Sella expanded. 20 mm R. intracavernous 3 mm Radical removalEL 11 years; suprasellar extension. diameter, projecting of the tumour.M 56 yr visual failure Cavernous ICA laterally. Aneurysm not.
I year. displaced laterally seen.ACA elevated.
Case 9 Chromophobe adenoma Visual failure Large expanded sella R. carotid artery Radical removalCD 2 years; 10 mm posterior origin of posterior of the tumour.F 57 yr hypopituitarism suprasellar extension communicating artery Aneurysm seen in
3 months. post-fixed chiasma. 4 mm diameter in contact withR. cavernous ICA projecting inferiorly. tumour. Smalldisplaced laterally. piece of capsuleACA elevated. attached to the
aneurysm wasleft in situ.
Case 10 Chromophobe adenoma Visual failure Enlarged eroded sella R. anterior cerebral Partial removalWL 18 months; 10 mm suprasellar artery 12 mm diameter, of tumour.F 62 yr headache 18 extension, lobulated. multilocular projecting Aneurysm seen in
months; Chiasmatic recess posteriorly perforating contact withhypopituitarism. elevated. Aneurysmal arteries close to neck. tumour. Proximal
mass seen. ACA Fig. 8 R. ACA clipped.elevated. ICA displacedlaterally.
Case 11 Craniopharyngioma Hypopituitarism Large eroded sella R. intracavernous Partial removalis 8 years; 30 mm suprasellar carotid artery, 7 mm of the tumour.M 38 yr visual failure extension, third diameter projecting Aneurysm not
6 months. ventricle indented. medially. seen.Cavernous ICA displaced Fig. 9laterally. ACA elevated.
Once a specific diagnosis has been established,the degree of intracranial extension and therelationship of neural structures can generally bedetermined more precisely by pneumoencepha-lography and computed tomography than byangiography, though in our selected series only5.5% of the angiograms failed to show displace-ment of vessels caused by the tumour extension.It is rare for arteries to be enclosed within thetumour, and vessel displacement can usually bepredicted from the extent of a mass shown onthe other studies. In only one case in this wholeseries was an artery definitely narrowed, and inanother occluded (Fig. 6) by encasement in thetumour. Considerable narrowing of the intra-cavernous carotid artery occurred in anotherpatient, but it was probably part of moregeneralised atheroma. In the patient with carotidartery occlusion (case 6), collateral circulationthrough the meninges adjacent to the tumour wasshown on the angiogram, and demonstration ofthese vessels may have a significant bearing onsurgery in rare cases. It is the previous knowledge
of incidental aneurysms which we consider to beof greater importance since this may allow plannedmodification of surgical approach to avoid damag-ing them or to include their treatment.The high frequency of aneurysms demonstrated
in this series may be due partly to angiographictechnique. In 80% of the cases bilateral carotidangiography was performed, and in the other 20%good cross flow was obtained, usually with reflux
Middle cerebral arteryAn,ter,or cerebral artery go
Dost comimunicatingq artery _ K x 0 t
Ophthalmic artery ) t
Intra cav,ernous carotid 0 t
Fig. 2 Diagram indicating position of aneurysms.Numerals refer to case numbers (see text).
975
guest. Protected by copyright.
on Septem
ber 23, 2020 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.11.972 on 1 N
ovember 1978. D
ownloaded from

976 Jan Jakubowski and Brian Kendall
.............. ...v.....,
:~~~~~ ~ ~ ~ ~ ~ ~~~~~~~~~~~ ~.......::
:.~~~~~~~~~~~~~~
.. jA.,~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.....
Fig. 3 Case 12. Left carotid angiogramnsubtractionXprints: (a) lateral, (b) antero-posterior projection.Theiayttrium implants are visible in contact withmediallyaprojecting aneurysmal dilatation of cavernous segmentof internal carotid artery.
~~~ .;
... ........ ..............
Fig. ...Case.3.Left ..oi niga,ltrlpoecin nrcvrosaers(arrowheads)projecting inferiorly and slightly medially, partially superimposedon~~~~~~~~~~~~~.............carotid~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~;
guest. Protected by copyright.
on Septem
ber 23, 2020 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.11.972 on 1 N
ovember 1978. D
ownloaded from

Coincidental aneurysms with tumours of pituitary origin
Fig. 6 Case 6. Right common carotid aizgiogramsubtraction print, lateral projection. (a) The internalcarotid artery is occluded. There is filling of thecavernous carotid artery (short arrows) throughmeningeal branches of the ascending pharyngealartery (crossed arrow), middle meningeal artery(long arrow) and artery of foramen rotundum(arrow heads). (b) Tumour blush is shown aroundthe cavernous carotid artery. (c) Left carotidangiogram subtraction print, antero-posteriorprojection. The cavernous segment is displacedlaterally. There is a small anterior cerebral aneurysm(arrow head).
Fig. 5 Case 5. Right carotid angiogram, subtractionprint antero-posterior projection. The intracavernousand supraclinoid segments of the internal carotidartery are displaced laterally. The anterior cerebralartery is elevated. There is an unilocular aneurysmprojecting superiorly and medially from thesupraclinoid carotid, at the origin of the ophthalmicartery.
6(1))
(1)(16(r)
977
f(I{(a
.............................
...
guest. Protected by copyright.
on Septem
ber 23, 2020 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.11.972 on 1 N
ovember 1978. D
ownloaded from

Jan Jakubowski and Brian Kendall
Fig. 7 Case 7. Right internal carotid angiogramsubtraction print lateral projection. Distal carotidaneurysm projecting anteriorly and superiorly(arrow head).
Fig. 8 Case 10. Right carotid angiogram antero-posterior projection with cross
compression. Lateral displacement of both supraclinoid segments and elevation ofanterior cerebral arteries. Multilocular right anterior cerebral aneurysm projectingsuperiorly and posteriorly.
down the contralateral artery, so that angiographywas generally complete. Though all the aneurysmswere larger than 3 mm in diameter and couldhave been shown by conventional methods,magnification was routine. Radiographic sub-traction was performed as indicated.Angiograms had not been performed previously
in the two cases with aneurysms adjacent toyttrium implants, so that it is not possible to be
sure whether these aneurysms were incidental,post-traumatic, or associated with the radiation inthe immediate proximity. It is probable that amajority of these aneurysms were traumatic butthe incidence of this complication is unknownbecause of lack of previous angiographic studiesof these cases. However, cavernous sinus syn-dromes and fistulas have not been noted afterpituitary implants so that progressive growth
978
guest. Protected by copyright.
on Septem
ber 23, 2020 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.11.972 on 1 N
ovember 1978. D
ownloaded from

Coincidental aneurysms with tumours of pituitary origin
g.4
Fig. 9 Case 11. Right carotid angiogram, obliqueprojection, subtraction print. A wide-neckedintracavernous aneurysm is shown projectingmedially (arrow heads).
and rupture of any complicating aneurysms mustbe rare. The demonstration of two such aneurysmsin our sample suggests that angiography shouldcertainly be performed before implantation orsubsequent surgery in the region of implants. Theintracavernous segments of the carotid arteriesmay encroach up to the midline. Their anatomyshould be determined before pituitaryimplantation.The reason for the higher frequency of
aneurysms in association with these tumours thanthat of incidental aneurysms previously recorded isunknown. There were no obvious clinical differ-ences between these cases and the rest of ourseries, and, apart from case 2 previouslymentioned. there was no evidence of diffusevascular disease or hypertension. With the ex-ception of the anterior communicating aneurysmin case 2, the aneurysms were all on vesselsadjacent to the tumours. This suggests the pos-sibility of a mechanical effect, perhaps associatedwith increased tension on or flow through smallvessels supplying the tumour. There was, however,no obvious difference in the vascularity of thetumours with aneurysms and that of the rest ofour cases.A relationship between acromegaly and
vascular disease is established, and the proportionof aneurysms was much greater in our cases withacromegaly. It may be that abnormal pituitary
hormone levels, which were present in all ourcases, affect the arterial walls and predispose toaneurysm formation.
We wish to thank Mr John Andrew, ConsultantNeurosurgeon at The Middlesex Hospital,London, and Professor Lindsay Symon of TheNational Hospital, Queen Square and Maida Vale,for their helpful criticism of the paper.
References
Alphen, von H. A. M. (1975). Microsurgical fronto-temporal approach to pituitary adenomas withextrasellar extension. Clinical Neurology and Neuro-surgery, 78, 247-256.
Ambrose, J. (1973). Radiological diagnosis of pituitarytumours. In Pituitary Tumours, pp. 79-121. Editedby J. S. Jenkins. Butterworths: London.
Cushing, H. (1912). The Pituitary Body and its Dis-orders. Clinical states produced by disorders of thehypophysis cerebri. J. B. Lippincott: Philadelphia.
Du Boulay, G. H. (1965). Some observations on thenatural history of intracranial aneurysms. BritishJournal of Radiology, 38, 721-757.
Gado, M., and Bull, J. W. D. (1971). The carotidangiogram in suprasellar masses. Neuroradiology,2, 136-153.
Hankinson, J., and Banna, M. (1976). Pituitary andParapituitary Tumours. W. B. Saunders: Eastbourne.
Housepian, E. M., and Pool, J. L. (1958). A systematicanalysis of intracranial aneurysms from the autopsyfile of the Presbyterian Hospital 1914-1956. Journalof Neuropathology and Experimental Neurology,17, 409-423.
Jefferson, G. (1937). Compression of the chiasma,optic nerves and optic tracts by intracranialaneurysms. Brain, 60, 444-497.
Lippman, H. H., Onotrio, B. M., and Baker, H. L.(1971). Intrasellar aneuryEm and pituitary adenoma:report of a case. Proceedings of the Mayo Clinic,46, 532-535.
Love, J. G. (1963). Association of carotid aneurysmwith neoplasm compressing the optic chiasm. Pro-ceedings of the Staff Meetings of the Mayo Clinic,38, 156-161.
Mitchell, S. W. (1889). Aneurysm of an anomalousartery causing antero-posterior division of thechiasma of the optic nerves and producingbitemporal hemianopia. Journal of Nervous andMental Disease, 14, 14-62.
Raymond, L. A., and Tew, J. (1978). Large supra-sellar aneurysms imitating pituitary tumour. Journalof Neurology, Neurosurgery, and Psychiatry, 41,83-87.
White, J. C., and Ballantine, H. (1%91). Intrasellaraneurysms simulating hypophyseal tumors. Journalof Neurosurgery, 18, 34-50.
979
guest. Protected by copyright.
on Septem
ber 23, 2020 byhttp://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.11.972 on 1 N
ovember 1978. D
ownloaded from