Embed Size (px)
DESCRIPTION
parathyroid
Citation preview
Intrathyroidal parathyroid adenoma
MB, 53/F, 2011632986
• c/o-– Generalized body
ache- 3 years– Progressive proximal
myopathy- 3 years– Low backache
• No history of-– Graveluria/ Renal
stones– Neck swelling– Epigastric pain– Acute abdomen– Mood swings
• No significant family history
Examination
• No neurocutaneous markers
• P/R- 80/min
• BP- 134/84 mm Hg
• Musculo-skeletal examination- Power grade V in all groups of muscles in all limbs
Examination
• Neck-– 3x3 cm midline swelling in left lower neck– Round, soft – Moving well with deglutition
• ? Thyroid• ? Parathyroid• ??? LN
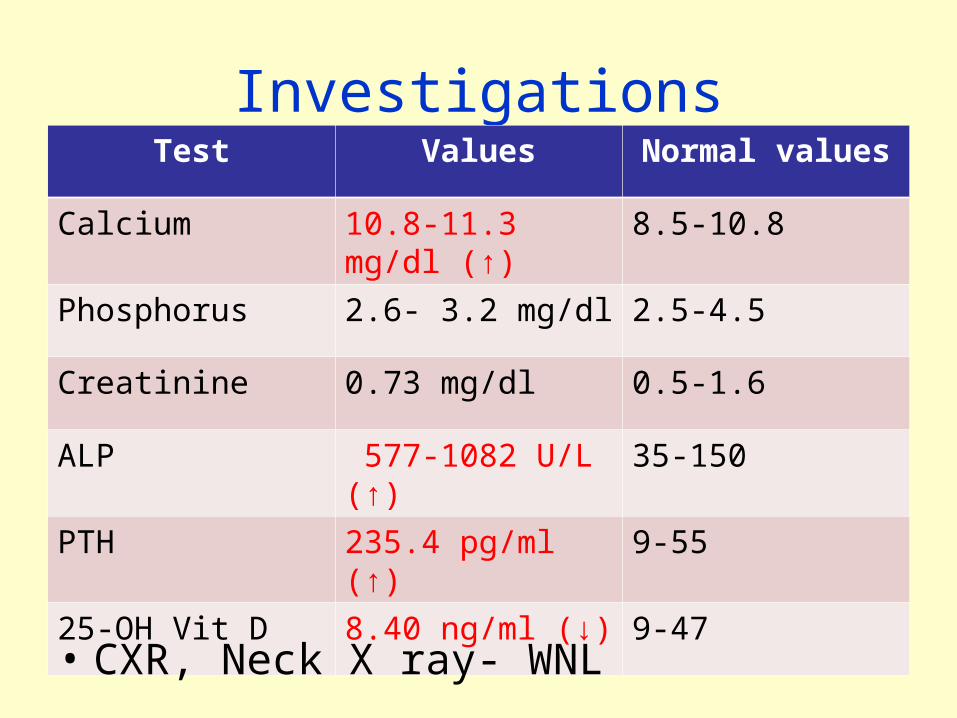
InvestigationsTest Values Normal values
Calcium 10.8-11.3 mg/dl (↑) 8.5-10.8
Phosphorus 2.6- 3.2 mg/dl 2.5-4.5
Creatinine 0.73 mg/dl 0.5-1.6
ALP 577-1082 U/L (↑) 35-150
PTH 235.4 pg/ml (↑) 9-55
25-OH Vit D 8.40 ng/ml (↓) 9-47
• CXR, Neck X ray- WNL
USG neck
• Left lobe thyroid replaced by complex cystic lesion with multiple echogenic septations measuring 3 x 2.2 x 1.6 cm
• Another 6 mm hypoechoic lesion in lower pole of left lobe thyroid
• Right lobe- 1 x 1 cm nodule
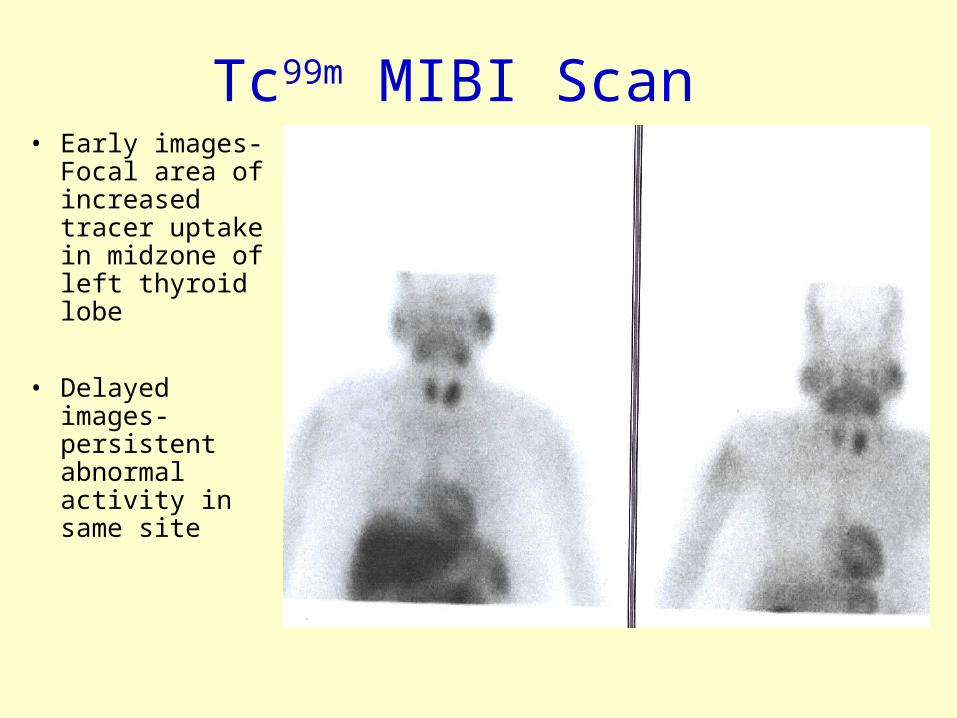
Tc99m MIBI Scan • Early images-
Focal area of increased tracer uptake in midzone of left thyroid lobe
• Delayed images- persistent abnormal activity in same site
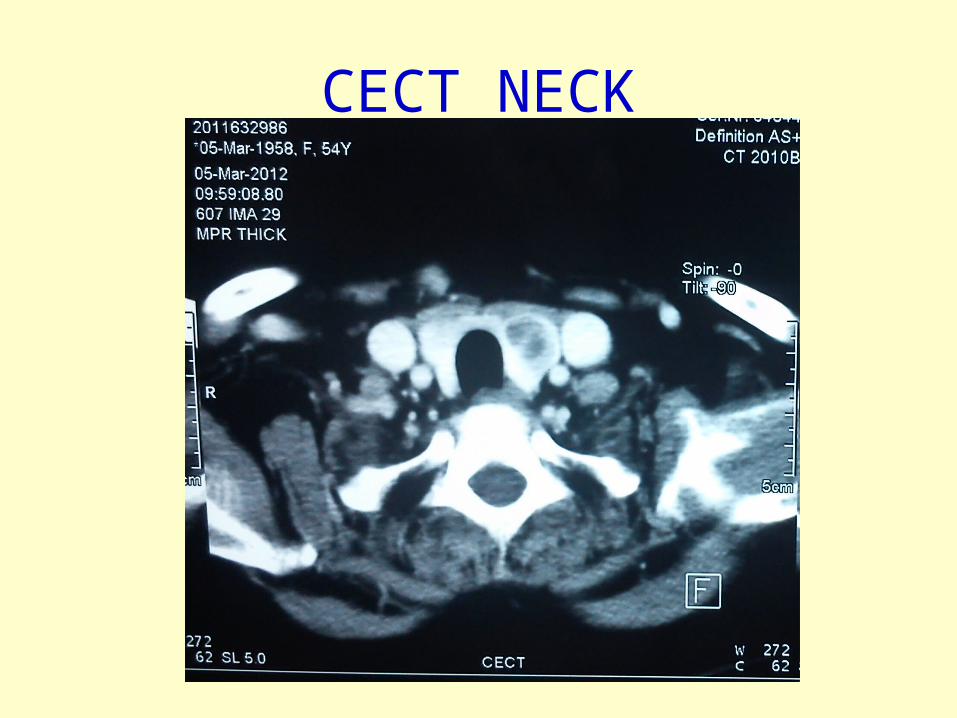
CECT NECK
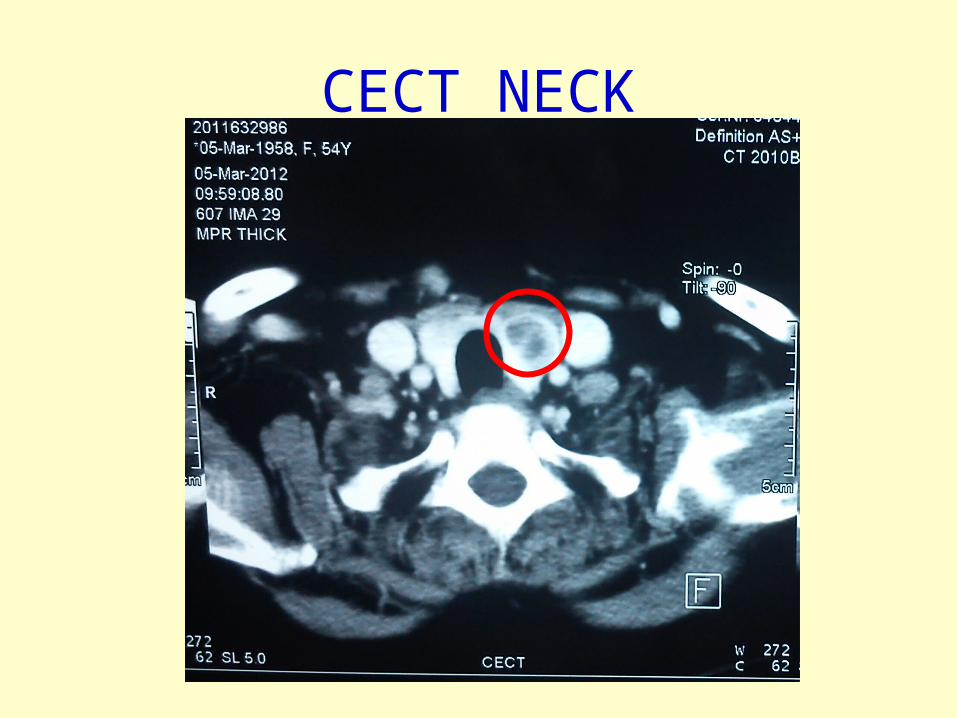
CECT NECK
FNAC Thyroid
• Occasional clusters of benign follicular epithelial cells
• Minimal amount of colloid
• Impression- Follicular pattern lesion
Surgery, 14-Mar-2012
• B/L Neck exploration with left hemithyroidectomy, frozen section biopsy, conversion to total thyroidectomy with IOPTH monitoring
• Left superior and left inferior parathyroid glands not localized in normal position

Intrathyroidal parathyroid adenoma
Surgery, 14-Mar-2012

Intrathyroidal parathyroid adenoma
13
Surgery, 14-Mar-2012
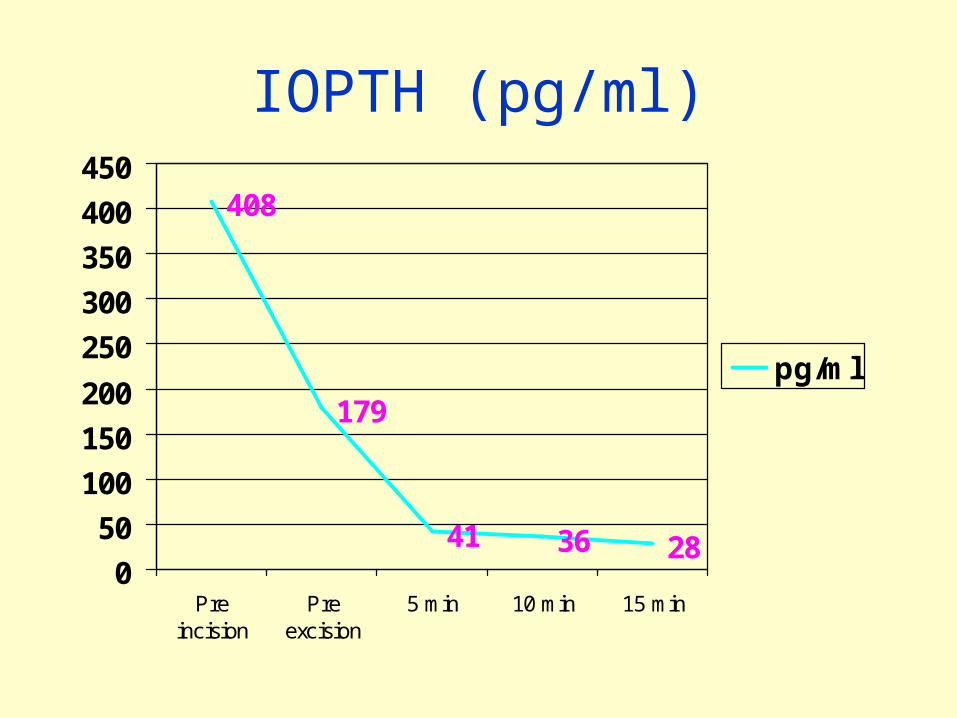
IOPTH (pg/ml)
408
179
41 36 280
50
100
150
200
250
300
350
400
450
Preincision
Preexcision
5 min 10 min 15 min
pg/ml
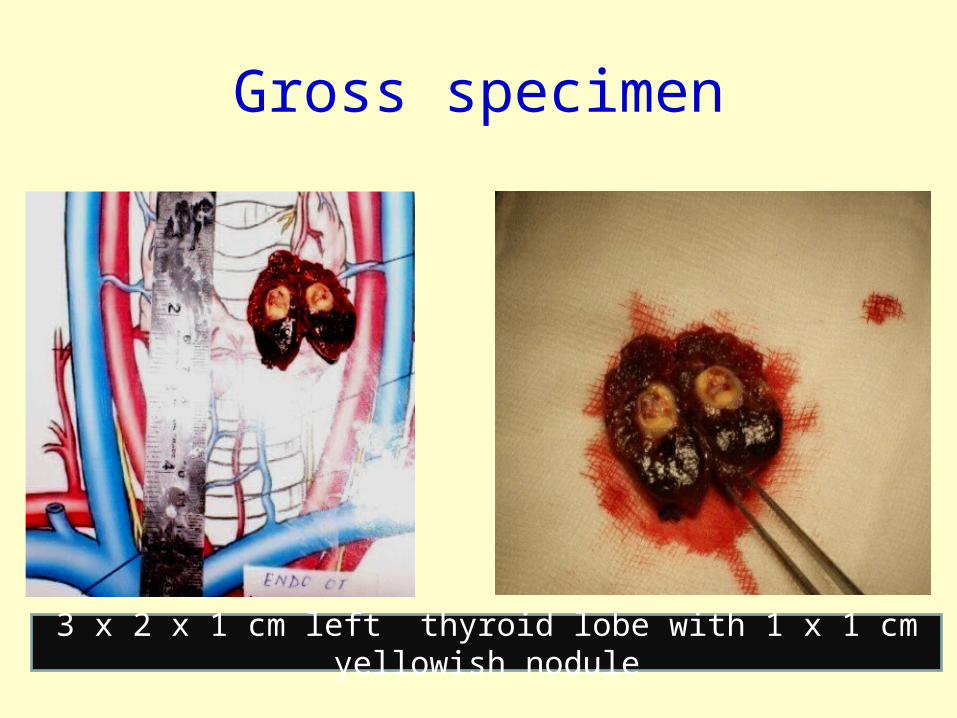
Gross specimen
3 x 2 x 1 cm left thyroid lobe with 1 x 1 cm yellowish nodule
Surgery, 14-Mar-2012
• Left hemithyroidectomy done & sent for frozen section biopsy
• Reported as-– Oncocytic lesion/ Parathyroid adenoma

Histopathology with IHC
Histopathology- Left lobe
• Thin encapsulated tumor• Cells arranged in diffuse sheets• Microfollicles at places• Thin vascular channels• Cells monomorphic with round nucleus and
moderate cytoplasm• No capsular or vascular invasion• IHC- Thyroglobulin was negative in nodule• IMPRESSION- Intrathyroidal parathyroid
adenoma
Histopathology- Right lobe
• Nodular goiter
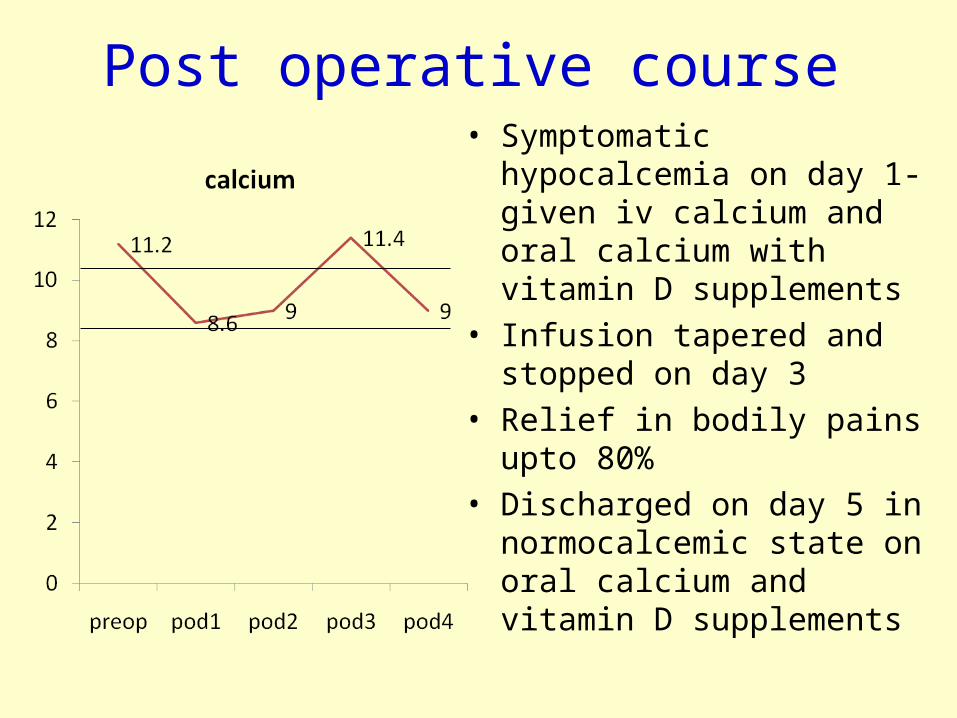
Post operative course• Symptomatic hypocalcemia
on day 1- given iv calcium and oral calcium with vitamin D supplements
• Infusion tapered and stopped on day 3
• Relief in bodily pains upto 80%
• Discharged on day 5 in normocalcemic state on oral calcium and vitamin D supplements
Follow up visit
• Eucalcemic
• Free of myalgias
• Bony pains relieved by 80%
• On oral Calcium and vitamin D supplements
Review of literature
Definition
Defined as a parathyroid gland, normal or abnormal, situated totally within the thyroid, surrounded on all aspects by thyroid parenchyma
Intra-thyroidal Parathyroid
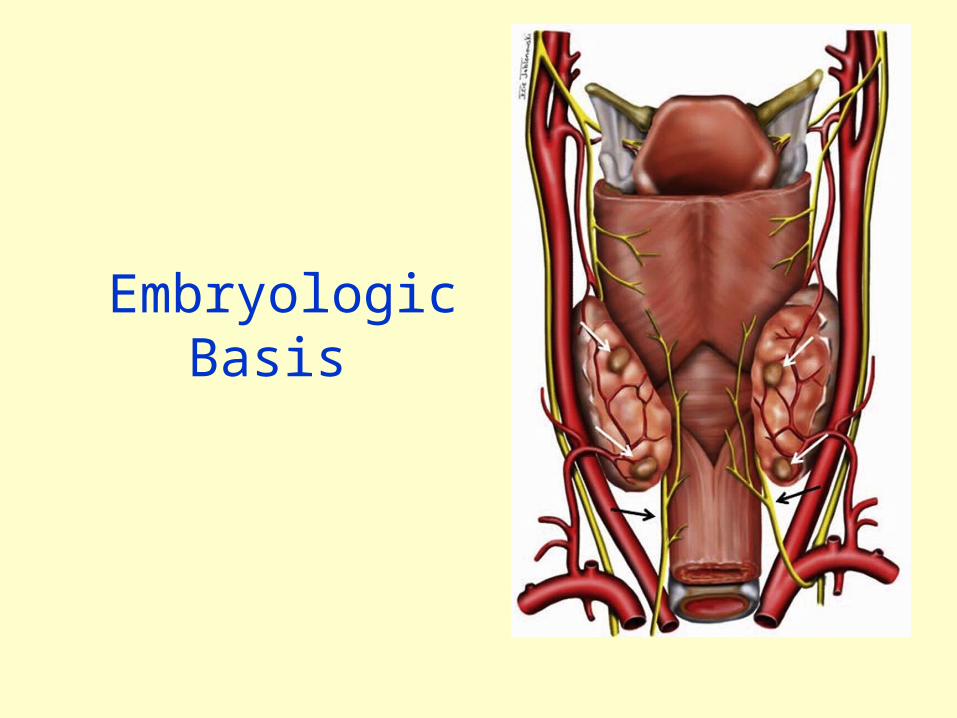
Embryologic Basis
Wang’s Hypothesis IV branchial pouch
Parathyroid, ultimobrancial body
Fusion with medial lobe thyroid
Intrathyroidal superior parathyroid
Wang CA. Hyperfunctioning intrathyroid parathyroid gland: A potential cause of failure in parathyroid surgery. JR Soc Med 1981
III Pharyngeal pouch
Thymus Inferior parathyroid (Intrathymus gland)
Primordium trapped in thyroid
Intrathyroidal inferior parathyroid
Feliciano DV. Parathyroid pathology in an intrathyroidal position. Am J Surg 1992;164:496–50
Intrathyroidal Parathyroid Adenomas as a cause for PHPT
• 1.4-3.4%- Primary cases
• 0.9% to 27.2%- Persistent/ recurrent cases

INVESTIGATIONS
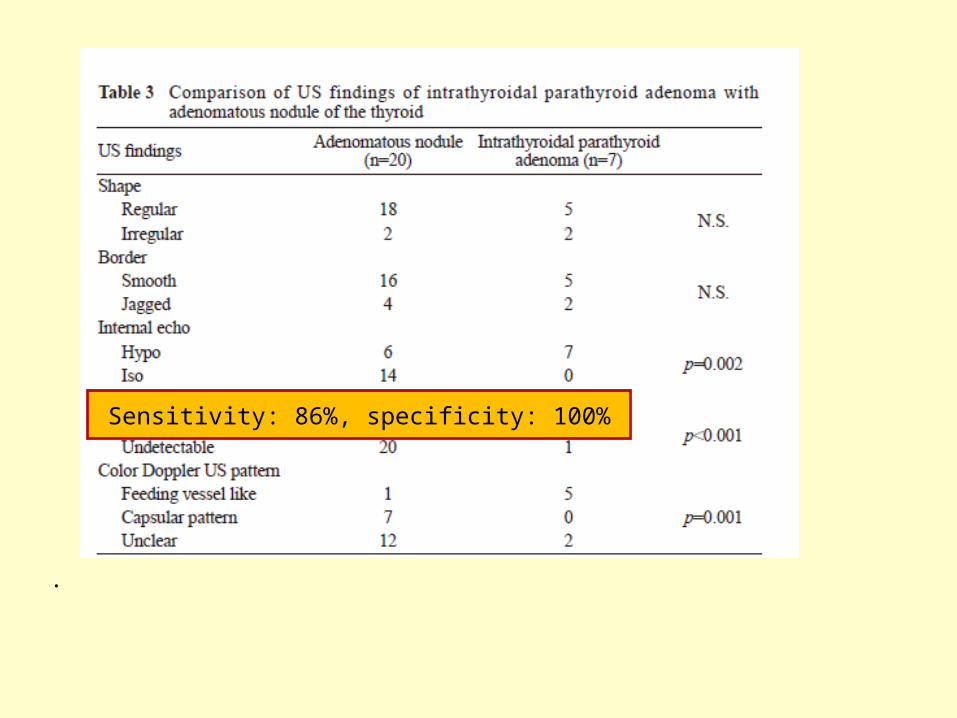
ULTRASOUND AND COLOR DOPPLER
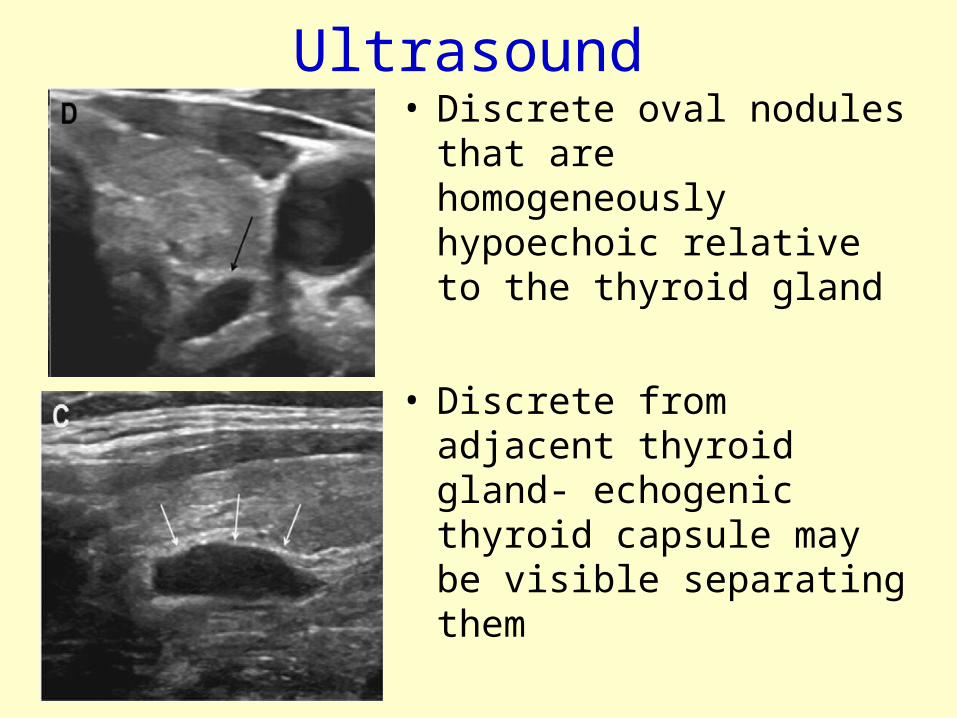
Ultrasound• Discrete oval nodules that
are homogeneously hypoechoic relative to the thyroid gland
• Discrete from adjacent thyroid gland- echogenic thyroid capsule may be visible separating them
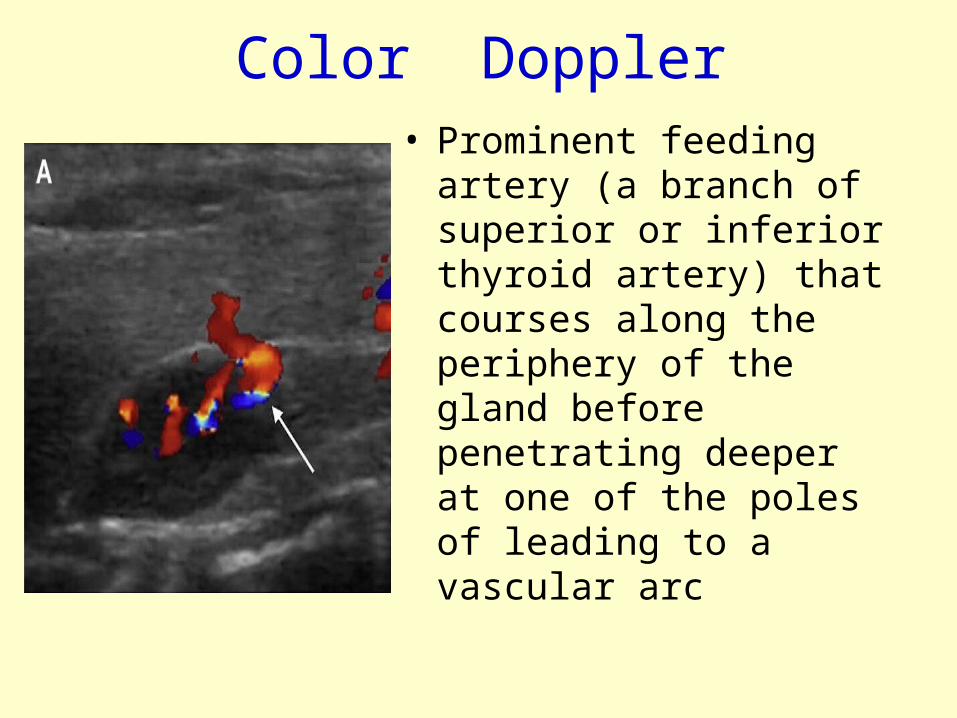
Color Doppler• Prominent feeding artery (a
branch of superior or inferior thyroid artery) that courses along the periphery of the gland before penetrating deeper at one of the poles of leading to a vascular arc
33
.
.
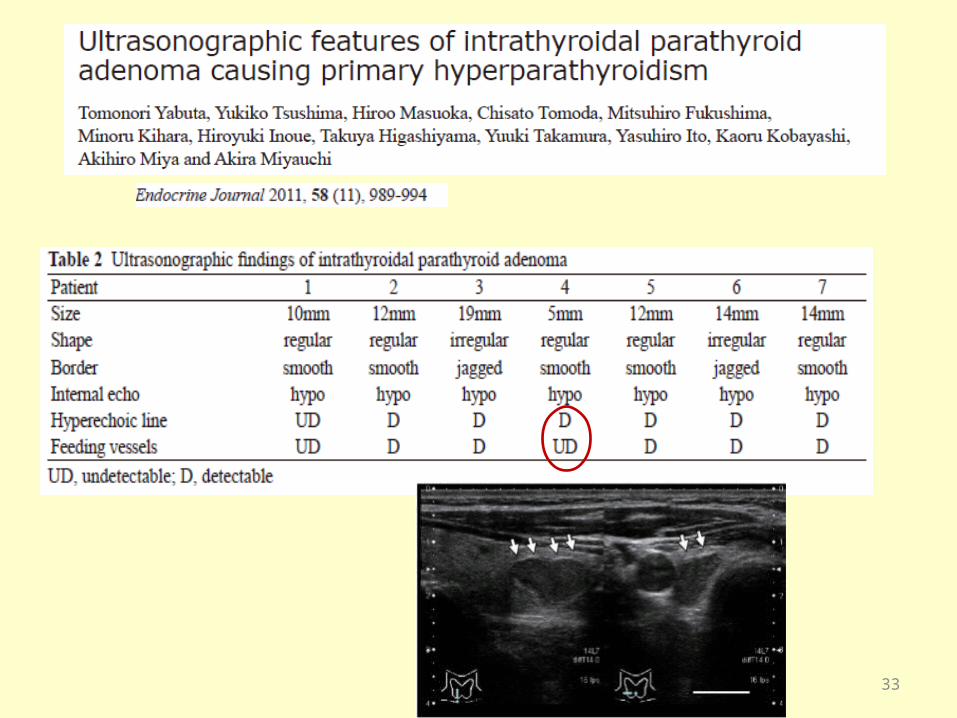
Sensitivity: 86%, specificity: 100%
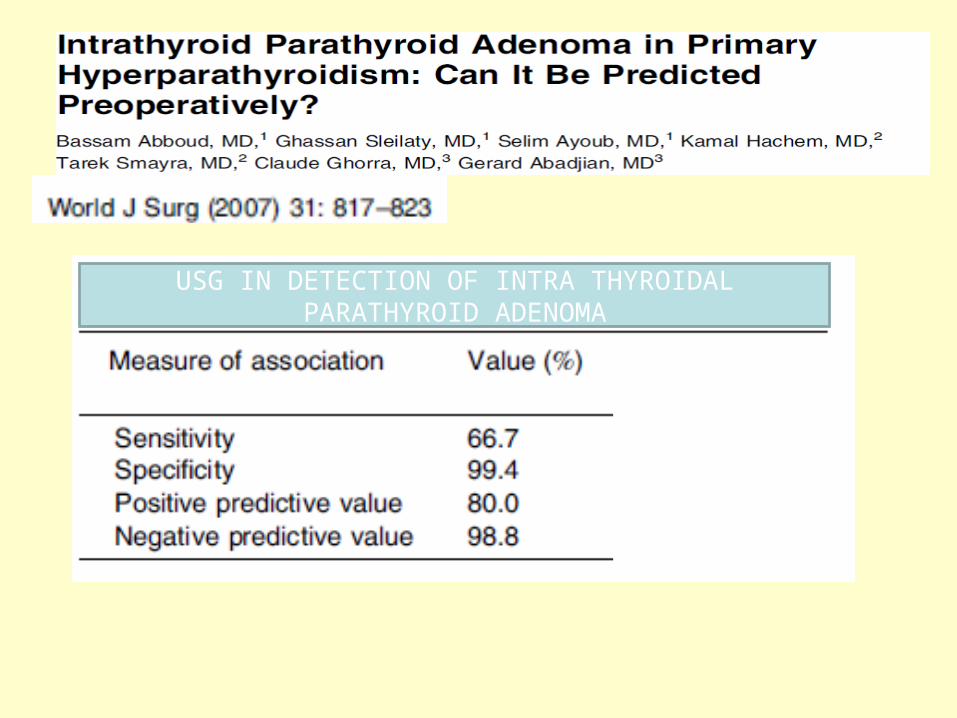
USG IN DETECTION OF INTRA THYROIDAL PARATHYROID ADENOMA

MIBI SCAN
Tc99m MIBI Scan• Early-phase uptake- Hyper/ Iso intense
within abnormal parathyroid- focus of activity separate from the thyroid gland/ a bulge or asymmetry of the thyroid contour can help
• Late phase uptake- Differential washout of radiotracer, with retention of contrast in parathyroid tissue
False positive studies
• Thyroid adenoma/ carcinoma/ Hürthle cell lesion• Multinodular goiter• Reactive lymph node• Ectopic thyroid tissue• Thymus, brown fat
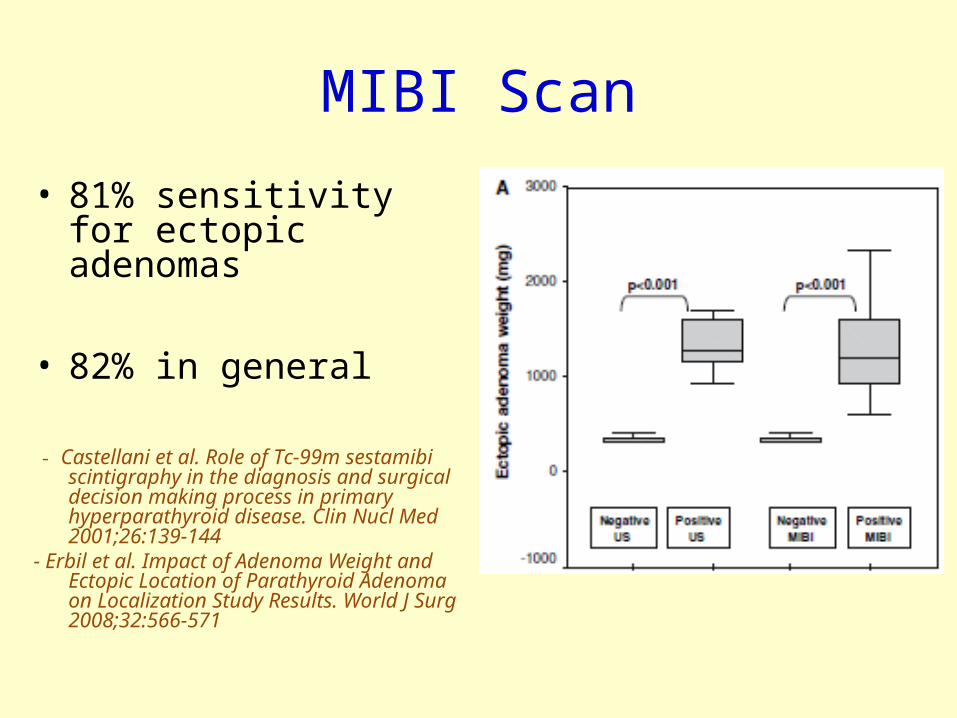
MIBI Scan
• 81% sensitivity for ectopic adenomas
• 82% in general
- Castellani et al. Role of Tc-99m sestamibi scintigraphy in the diagnosis and surgical decision making process in primary hyperparathyroid disease. Clin Nucl Med 2001;26:139-144
- Erbil et al. Impact of Adenoma Weight and Ectopic Location of Parathyroid Adenoma on Localization Study Results. World J Surg 2008;32:566-571
SPECT CT
• Sestamibi SPECT CT- Improves localization of ectopic tumors
FNAC• Easily confused with thyroid due to overlap
in cytomorphologic features of the aspirated cells
• No single cytomorphologic feature is diagnostic
• A combination raises the possibility of a parathyroid lesion

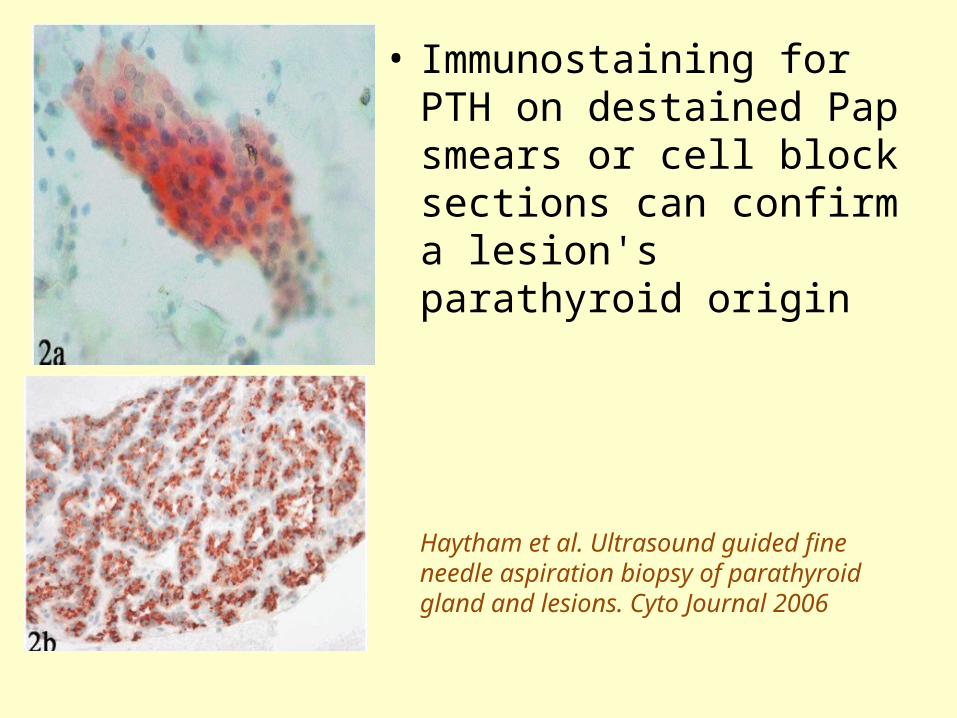
• Immunostaining for PTH on destained Pap smears or cell block sections can confirm a lesion's parathyroid origin
Haytham et al. Ultrasound guided fine needle aspiration biopsy of parathyroid gland and lesions. Cyto Journal 2006
Parathyroid hormone assay in needle aspirates
• PTH assay using needle aspirates
• Should be performed only if localization of the adenoma is missed by non-invasive study
Marcocci et al. Preoperative localization of suspicious parathyroid adenomas by assay of parathyroid hormone in needle aspirates. Eur J Endocrinology 1998;139:72-77
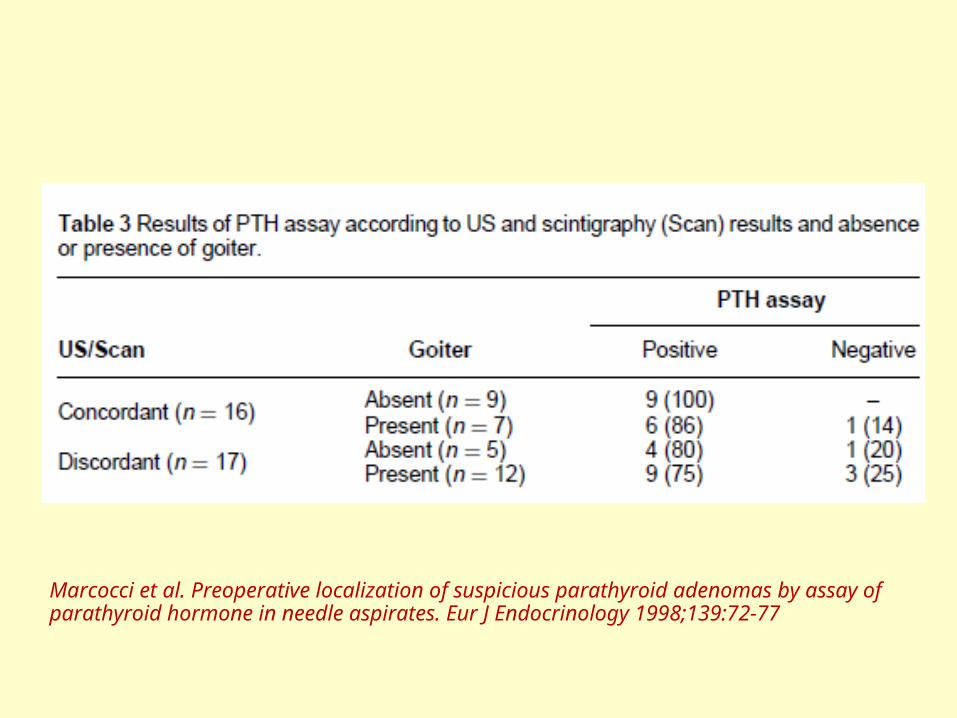
Marcocci et al. Preoperative localization of suspicious parathyroid adenomas by assay of parathyroid hormone in needle aspirates. Eur J Endocrinology 1998;139:72-77
OTHER MODALITIES
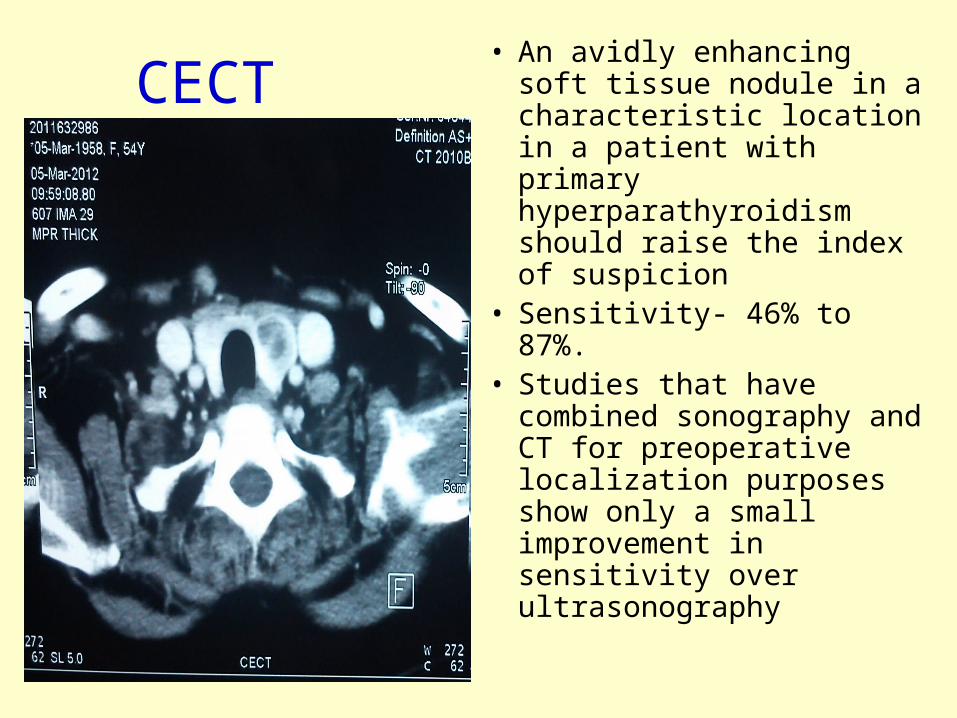
CECT• An avidly enhancing soft
tissue nodule in a characteristic location in a patient with primary hyperparathyroidism should raise the index of suspicion
• Sensitivity- 46% to 87%.• Studies that have
combined sonography and CT for preoperative localization purposes show only a small improvement in sensitivity over ultrasonography
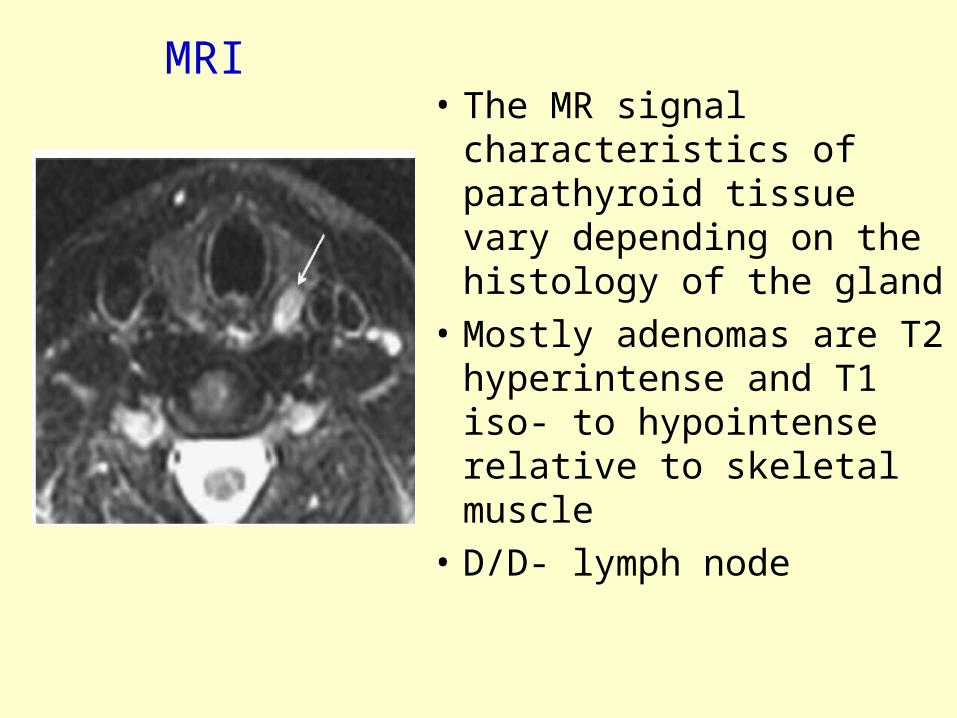
• The MR signal characteristics of parathyroid tissue vary depending on the histology of the gland
• Mostly adenomas are T2 hyperintense and T1 iso- to hypointense relative to skeletal muscle
• D/D- lymph node
MRI
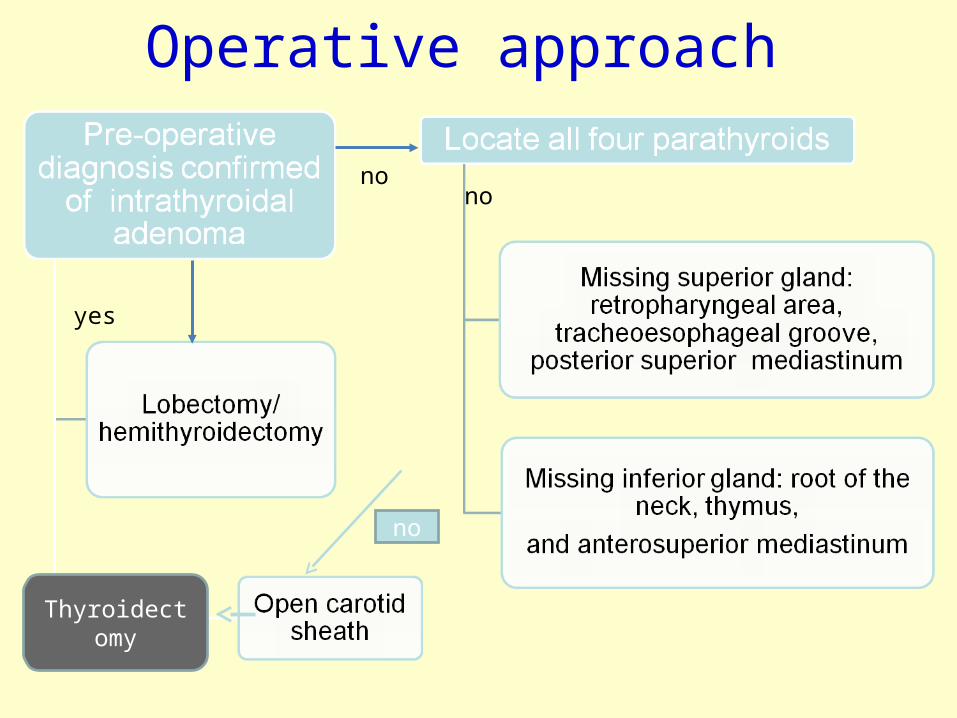
Operative approach
no
Thyroidectomy
nono
yes
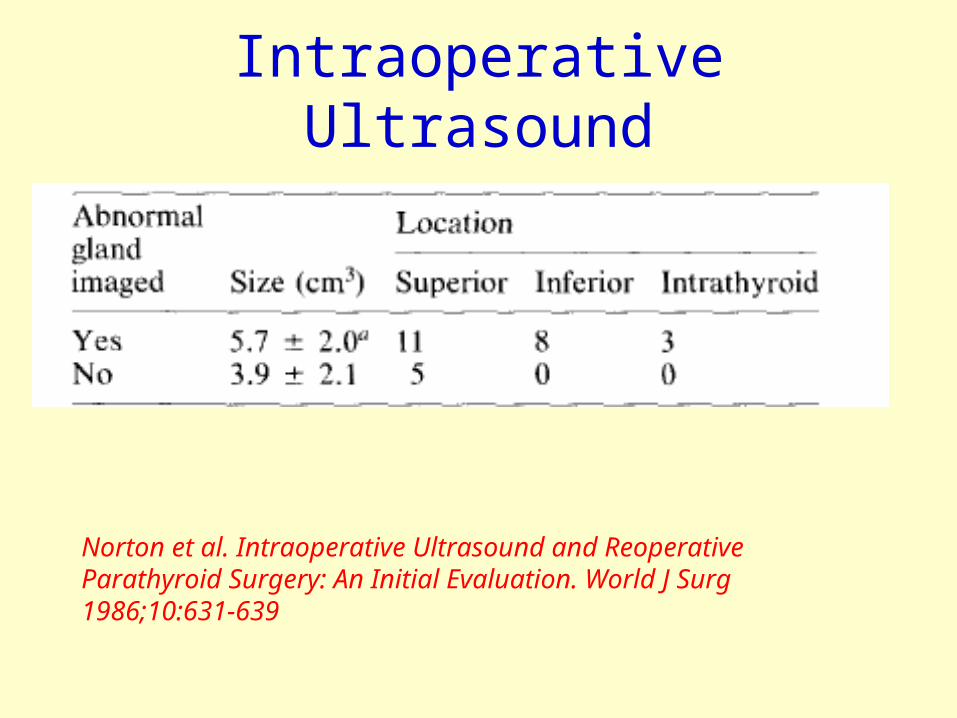
Intraoperative Ultrasound
Norton et al. Intraoperative Ultrasound and Reoperative Parathyroid Surgery: An Initial Evaluation. World J Surg 1986;10:631-639
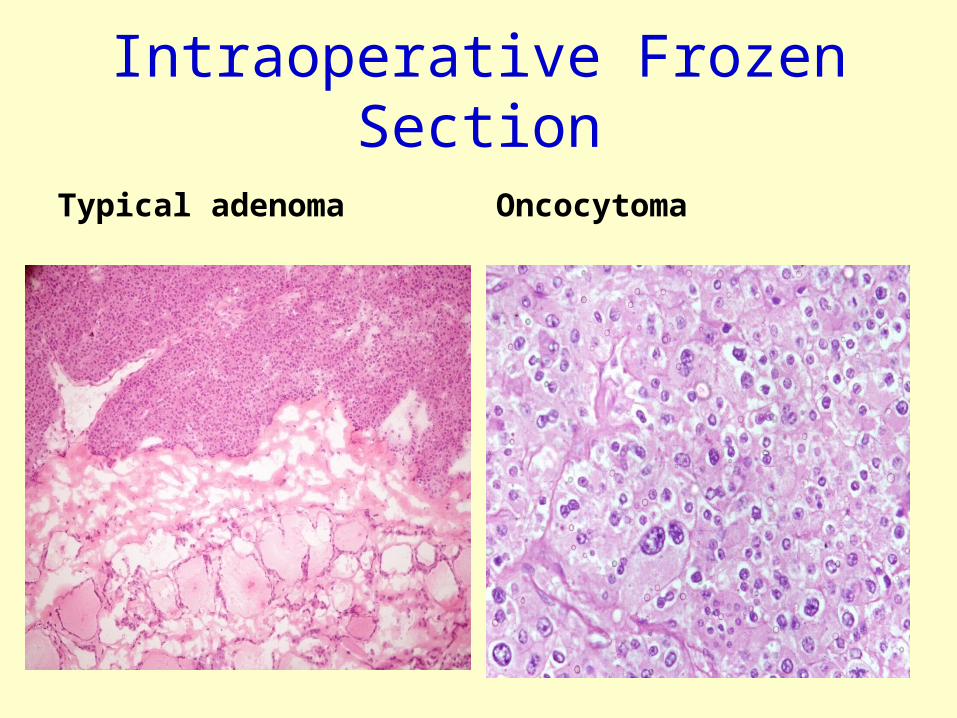
Intraoperative Frozen Section
Typical adenoma Oncocytoma
Sources of error
• Frozen section artifact, sampling error, judgmental error contributed to deferred or incorrect diagnoses
• The coexistence of parathyroid and nodular thyroid disease- Intrathyroidal parathyroid glands showing conspicuous follicle formations or abundant oncocytic cells and thyroid nodules with fatty stroma
Additional pathological features
• Examination for oxalate crystals
• Argyrophilia
• Electron microscopy for secretary granules
• Immunohistochemistry for thyroglobulin
PERSISTENT PHPT
Persistent PHPT-Sites of ectopic glands
• Tracheo esophageal groove (27%)• Thymus (17%)• Intrathyroidal (10%)• Undescended glands (8.6%)• Carotid sheath (3.6%)• Retroesophageal space (3.2%)
Jaskowiak N et al. A Prospective Trial Evaluating a Standard Approach to Reoperation for Missed Parathyroid Adenoma. Ann Surg 224:308-322
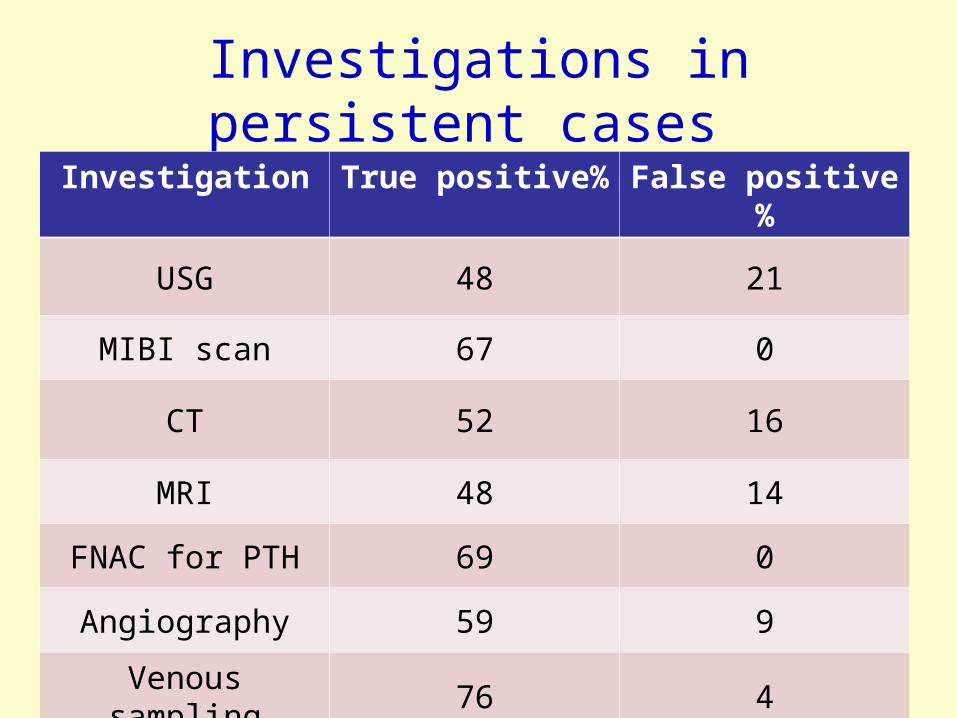
Investigations in persistent cases
Investigation True positive% False positive%
USG 48 21
MIBI scan 67 0
CT 52 16
MRI 48 14
FNAC for PTH 69 0
Angiography 59 9
Venous sampling 76 4
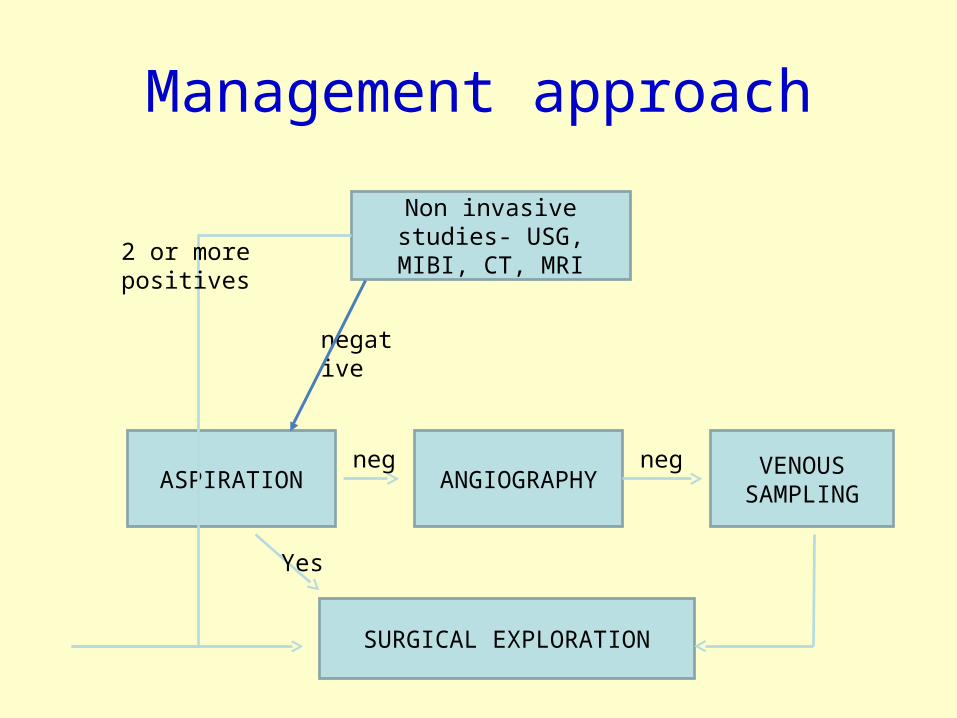
Management approach
Non invasive studies- USG, MIBI, CT, MRI
ASPIRATION ANGIOGRAPHY VENOUS SAMPLING
SURGICAL EXPLORATION
2 or more positives
negative
neg neg
Yes
Take home message
• Rare entity
• High degree of suspicion pre- and intra-operatively
• Careful search for ectopic locations in suspicious cases
• Intraoperative ultrasound, FNA for PTH aspirate, frozen- useful adjuncts
THANK YOU




















![Parathyroid Adenoma/Thymoma Case Reportadenoma and thymoma without mention of sestamibi uptake by the thymoma (whether such imaging was performed or not). Byrne et al. [13] demonstrated](https://img.pdfslide.us/doc/110x75/5e2f040ac0577556e1278f0b/parathyroid-adenomathymoma-case-adenoma-and-thymoma-without-mention-of-sestamibi.jpg)