Embed Size (px)
Citation preview

Cellulitis and Soft Tissue Infections
Sally Williams MD

Cellulitis: A very common infection
25 cases per 1000 patient years
More common in men, obese patients
60% occurs in the lower extremities
74% handled as outpatients
82% of patients have just a single episode
High cause of hospital readmissions

Cellulitis: definition
A nonspecific term that includes a large collection of skin & soft tissue infections
Can include:– Erysipelas (the most common cellulitis)
– Cellulitis associated with abscesses
– Gangrenous cellulitis
– Secondary infection of pre-existing skin lesions
– Cutaneous involvement of systemic illness

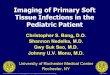
Normal Skin Structure

Locations of Skin Infections
Impetigo and ecthyma: upper epidermis
Erysipelas and cellulitis: lower epidermis and dermis
Carbuncles, furuncles, “boils” : deep dermis and hair follicles
Necrotizing fasciitis: deep, next to muscle

Microbiology of Cellulitis
The vast majority are strep and staph
More unusual etiologies:– Cat bite: Pasteurella
– Dog bite: Capnocytophaga (splenectomized)
– Rat bite: Streptobacillus
– Fresh water: Aeromonas
– Salt water:Vibrio and Mycobacterium marinum
– Hot tubs: Pseudomonas

Classic hot tub folliculitis

Mix and Match

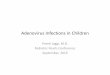
Impetigo
Very common skin infection in kids Has appearance of “honey colored crusts”,
often on face Etiology is always staph or strep Treat with topical bactroban or oral abx Bullous impetigo is always staph, forms
vesicles and bullae Impetigo quite infectious!

Impetigo

Erysipelas: Clinical Features
Often of rapid onset
Etiology is always streptococcal
Often preceded by fevers, chills and groin pain (for lower extremity cellulitis)
Often blisters after a few days
Usually has lymphangitic streaking
Almost always worsens in appearance before improving on antibiotics

Classic Leg Cellulitis

Facial Cellulitis

Erysipelas continued
Risk factors for erysipelas/strep cellulitis:– Leg edema
– Previous leg surgery
– Obesity
– Previous breast surgery (for arm and breast cellulitis)
– Tinea pedis (NOT onychomycosis)
– Uncontrolled diabetes

Natural History of Erysipelas
Is almost always preceded by fevers, chills, and rapid increase in erythema
ALWAYS gets “worse” before better– Will extend outside drawn “borders”
Almost always has fever and elevated wbc
Can take WEEKS to get better if has underlying edema, history of surgery etc
Will often blister

Is this Cellulitis??

Is this Cellulitis?

Rule #1
There is no entity of “BILATERAL lower extremity cellulitis”.
These are usually all chronic stasis dermatitis
True cellulitis almost always has:
– 1. Elevated wbc
– 2. Erythema above the knee
– 3. Fever, and often preceding chills
– 4. Often “patches” of cellulitis on upper thigh

Rule #2: Please do not culture this

Wound Cultures
Never culture a chronic open wound– The wounds will ALWAYS be colonized with
multiple bacteria– A wound without PMNs on gram stain is probably
not an infected wound– Countless unnecessary courses of antibiotics are
used, predisposing pts to C difficile
If you can unroof an abscess or express pus from something then culture that

Rule #3: Vancomycin not needed for cellulitis without boil
Classic cellulitis is streptococcal
Strep releases a streptozyme to dissolve layer underneath the skin, causing rapid spread.– Multiple different strep species may cause
cellulitis (A,B,C,F,G)
– Strep almost always causes lymphangiitis
Staph cellulitis is almost always associated with a boil or abscess

Staph skin boils

Cellulitis continued
Treatment of non-boil, non-nec fasc cellulitis is strep targeted- Rx cefazolin or ceftriaxone
As soon as they let the leg down will get bigger, redder, hotter – this is NOT treatment failure, just dependent edema.
We need to prepare patients that the leg may look abnormal for months in some cases
History of MRSA irrelevant if looks streptococcal– Please do NOT use vancomycin for diffuse cellulitis

Cellulitis Treatment
Most heavy weight people “fail” oral antibiotics due to insufficient blood levels – may need a course of iv antibiotics or high bioavailability oral antibiotic.
“Failing” keflex is not a reason to use vancomycin –they just need iv cefazolin
Strep itself is easy to kill but the infection causes a lot of “leftover damage” as the lymph system is often damaged. We have to prepare patients for slow improvement

Summary: Leg Cellulitis
Occurs most commonly in the obese or persons with a history of surgery in that leg
Warn them of “worsening” when they start ambulating, leg will get redder, hotter
If you use po antibiotic, need very high doses, e.g. 1-1.5g cephalexin qid
If they truly “failed” high dose keflex could consider oral levoflox, has high blood levels

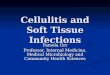
MRSA: Not a spider bite(courtesy of GiantMicrobes.com)

MRSA Epidemiology
First described in 1961
Previously hospital associated, now widely community acquired since 2002
Most C.A. MRSA strains are US 300 and carry the PVL (panton valentine leukocidin) gene, causes necrosis
C.A. most commonly skin/soft tissue infections, less likely bacteremia

Staphylococcal Cellulitis & BoilsRisk Factors
Young age
Immunocompromised
Contact sports
Crowded conditions
Sharing towels, sheets etc
Prior antibiotics, especially quinolones

Antibiotics for Staph skin boils-do they help?
Randomized studies are conflicting
Many studies show no benefit to antibiotics after incision and drainage
The studies that did show a benefit related a small one with using TMP-S + I&D.
Drainage is likely 95% of the battle-if the pt has extensive induration oral Rx may be helpful, especially if >2 cm.

Antibiotic treatment for MRSA
Vancomycin for the hospitalized patient, Daptomycin also useful but expensive
Clindamycin resistance up to 33%
Bactrim is still sensitive >90% of the time
Doxycyline resistance actually quite low
Linezolid effective, but has rare drug interactions– Serotonin syndrome <.1%, still black box warning
Dalbavancin/Oritavancin: likely to not be used due to >$1000 per dose of antibiotic

Does antibacterial soap help?
Antibacterial Soap? You Can Skip It, Use Plain Soap and Water (FDA November 2017)
Most contain triclosan, a pesticide– No proven efficacy
– Potential to cause antibiotic resistance
– Potential to affect hormones
Hand sanitizers ARE effective

Recurrent skin lesions
Most common in young overweight women
Essentially acquisition is bad luck, can be very difficult to eradicate
Nasal mupiricin for household sometimes effective, with mass washing
For severe cases Bactrim suppression for a few months is an option

Necrotizing Fasciitis
Uncommon severe infection
Etiologies may be:– Streptococcal (most common)
– Polymicrobial –usually associated with gut flora (e.g. perirectal abscess, Fourniers) or trauma
– Staphylococcal –usually post op, needs to be differentiated from necrotizing staph soft tissue infection which is very common.

Strep necrotizing fasciitis

Clinical Picture of Necrotizing Fasciitis
These patients are very ill – febrile, hypotensive, tachycardic, delerious
Pain out of proportion to exam
Cutaneous anesthesia
Very rapid spread
May have skin bullae (often black), ecchymoses, usually edema

Example of Leg Nec Fasc

Necrotizing Fasciitis
WBC almost always very high or very low
Cr usually about 2, pt often in toxic shock
Nec fasc is a SURGICAL EMERGENCY
Antibiotics are targeted toward strep, staph or polymicrobic- Vanco + Piptazo
Clindamycin is added as inhibits toxin production, but surgery is life saving

How does Necrotizing fasciitis/ toxic shock happen?
BAD LUCK
It requires a toxin producing strain of strep (rare) often in the setting of uncontrolled DM
AND a lack of immunity to the toxin (also rare)
IVIG is often used with toxic shock to give patient a large “antibody load” -someone in the large pool of donors likely has an antibody to the toxin

Summary: Skin Infections
Cellulitis is common and is usually strep
Most cellulitis gets worse before better
Boils are almost always staph/MRSA and need to be drained to achieve cure
Chronic stasis dermatitis is incredibly common and should not be mistaken for cellulitis
Nec fasciitis is rare and pts are very ill

IDSA SSTI guidelines

Antibiotic humor

Superbugs coming…