Embed Size (px)
Citation preview
Policy Number
LCH-25
This document has been reviewed in line with the Policy Alignment Process for Liverpool Community Health NHS Trust Services. It is a valid Mersey Care document, however due to organisational change this FRONT COVER has been added so the reader is aware of any changes to their role or to terminology which has now been superseded. When reading this document please take account of the changes highlighted in Part B and C of this form.Part A – Information about this DocumentPolicy Name Intravenous Antibiotic Policy
Policy Type Board Approved (Trust-wide) ☐ Trust-wide ☐ Divisional / Team / Locality ☒
Action No Change ☐ Minor
Change ☐ MajorChange ☐ New
Policy ☒ No LongerNeeded ☐
Approval
As Mersey Care’s Executive Director / Lead for this document, I confirm that this document:a) complies with the latest statutory / regulatory requirements,b) complies with the latest national guidance, c) has been updated to reflect the requirements of clinicians and officers, andd) has been updated to reflect any local contractual requirements
Signature: Date:
Part B – Changes in Terminology (used with ‘Minor Change’, ‘Major Changes’ & ‘New Policy’ only)Terminology used in this Document New terminology when reading this Document
Part C – Additional Information Added (to be used with ‘Major Changes’ only)Section / Paragraph No
Outline of the information that has been added to this document – especially where it may change what staff need to do
Part D – Rationale (to be used with ‘New Policy’ & ‘Policy No Longer Required’ only)Please explain why this new document needs to be adopted or why this document is no longer required
Part E – Oversight Arrangements (to be used with ‘New Policy’ only)Accountable Director
Recommending Committee
Approving Committee
Next Review DateLCH Policy Alignment Process – Form 1
Policy for the Management & Administration of Intravenous Antibiotics
Page 2 of 27

SUPPORTING STATEMENTS
This document should be read in conjunction with the following statements:
SAFEGUARDING IS EVERYBODY’S BUSINESS
All Mersey Care NHS Foundation Trust employees have a statutory duty to safeguard and promote the welfare of children and adults, including: being alert to the possibility of child / adult abuse and neglect through their observation of
abuse, or by professional judgement made as a result of information gathered about the child / adult;
knowing how to deal with a disclosure or allegation of child / adult abuse; undertaking training as appropriate for their role and keeping themselves updated; being aware of and following the local policies and procedures they need to follow if they
have a child / adult concern; ensuring appropriate advice and support is accessed either from managers, Safeguarding
Ambassadors or the trust’s safeguarding team; participating in multi-agency working to safeguard the child or adult (if appropriate to your
role); ensuring contemporaneous records are kept at all times and record keeping is in strict
adherence to Mersey Care NHS Foundation Trust policy and procedures and professional guidelines. Roles, responsibilities and accountabilities, will differ depending on the post you hold within the organisation;
ensuring that all staff and their managers discuss and record any safeguarding issues that arise at each supervision session
EQUALITY AND HUMAN RIGHTS
Mersey Care NHS Foundation Trust recognises that some sections of society experience prejudice and discrimination. The Equality Act 2010 specifically recognises the protected characteristics of age, disability, gender, race, religion or belief, sexual orientation and transgender. The Equality Act also requires regard to socio-economic factors including pregnancy /maternity and marriage/civil partnership.
The trust is committed to equality of opportunity and anti-discriminatory practice both in the provision of services and in our role as a major employer. The trust believes that all people have the right to be treated with dignity and respect and is committed to the elimination of unfair and unlawful discriminatory practices.
Mersey Care NHS Foundation Trust also is aware of its legal duties under the Human Rights Act 1998. Section 6 of the Human Rights Act requires all public authorities to uphold and promote Human Rights in everything they do. It is unlawful for a public authority to perform any act which contravenes the Human Rights Act.
Mersey Care NHS Foundation Trust is committed to carrying out its functions and service delivery in line the with a Human Rights based approach and the FREDA principles of Fairness, Respect, Equality Dignity, and Autonomy
Policy for the Management & Administration of Intravenous Antibiotics
Page 3 of 27
Policy for the Management and Administration of Intravenous Antibiotics by staff working for
Liverpool Community Health NHS Trust
POLICY NUMBER 25
Policy for the Management & Administration of Intravenous Antibiotics
Page 4 of 27
TitlePolicy for the Management and Administration of Intravenous Antibiotics
Policy referencenumber 25
Aim and purpose of policy
To provide the Trust with a policy on the safe management and administration of IV Antibiotics services in the community
Author Medicines Management Pharmacist
TypeNew Policy
Reviewed Policy
Review date January 2020Person/group accountable for review
Community Intravenous Therapy Team
Type of evidence base used
C/ Evidence which includes published and or unpublished studies and expert opinion
ISSUE DATE January 2018
Authorised by Clinical Standards 24th January 2018Equality Assessment undertaken
Yes19/01/2018
No
Policy for the Management & Administration of Intravenous Antibiotics
Page 5 of 27
Version ControlVersion Number: 5
Ratified by: Clinical Standards Group
Date of Approval: 24th January 2018
Name of originator/author: IV Therapy Team
Name of reviewer: Hillary Smith
Approving Body / Committee: Clinical Standards Group
Date issued: January 2018
Review date: January 2020
Target audience: Staff employed by Liverpool Community Health NHS Trust
Name of Lead Director / Managing Director: Director of Nursing
Changes / Alterations Made To Previous Version:
Change in formattingInclusion of new referral formInclusion of new prescription sheetInclusion of cellulitis care pathway when referred by hospital or GP when prescribing responsibility remains with the referrerProcess detail expanded
Policy for the Management & Administration of Intravenous Antibiotics
Page 6 of 27
Contents Page
1. Introduction 52. Purpose 5
2.1 Scope 53. Definitions 64. Duties & Responsibilities 85. Policy 8
5.1 Eligibility Criteria 85.2 Consent 95.3 Medical Authorisation 95.4 Responsibilities 105.5 Procedures 115.6 Methods of intravenous drug administration 115.7 Routes of Administration 115.8 Equipment 125.9 General Process 125.10 Adverse Incidents 13
6. Training Requirements 147. Implementation, Monitoring & Review 148. Linked Information 159. References 16AppendicesAppendix 1 Antibiotic Formulary 17Appendix 2 Community IV Antibiotics referral Form 19Appendix 3 Community IV Prescription Sheet 20Appendix 4 Peripheral IV Cannula Visual Inspection of
Intravenous Access Devices (VIIAD) charts21
Appendix 5 Visual Inspection Phlebitis Score (VIP) 23Appendix 6 NPSA Heparin Alert 24
Policy for the Management & Administration of Intravenous Antibiotics
Page 7 of 27
1. Introduction
The administration of IV medication by nurses has become more widespread in recent years. The practice has now become part of the core skills for general nursing practice, allowing a holistic approach to total patient care. With today’s emphasis on community care and patient empowerment, there is a growing need for community nurses to take on this role in order to facilitate home care. This policy is designed to give clarity around the management and administration of intravenous antibiotics in the community.
Administration of IV Antibiotics carries potential risks and should only be given if the benefits outweigh these risks. Stringent systems need to be in place to ensure that the correct product is given to the correct patient at the correct time and that any adverse reactions are dealt with promptly and efficiently.
This policy will cover the referral into the service, including responsibilities and clinical procedures relating to the administration of anti-infective intravenous therapy by appropriately trained staff.
2. Purpose
This policy will direct the safe management and administration of IV Antibiotics in the community by appropriately trained registered nurses employed by LCH.
By providing an Intravenous Antibiotic Service in the community it will reduce the necessity for hospital admission or prolonged hospital admission.
The advice contained within this policy is drawn from the latest research based evidence and has been agreed by a number of professionals.
Liverpool Community Health is committed to ensuring that all staff are trained and equipped to perform their role effectively.
2.1 Scope
This document describes the clinical procedures for patients who are suitable to have Intravenous Antibiotics in the community by the Community Intravenous Therapy Team, and District Nurses. It may be carried out in patients’ homes or in NHS Health Clinics.
This policy applies to all registered nurses employed by Liverpool Community Health NHS Trust who have been trained and maintain their competencies in IV therapies and peripheral cannulation.
Policy for the Management & Administration of Intravenous Antibiotics
Page 8 of 27
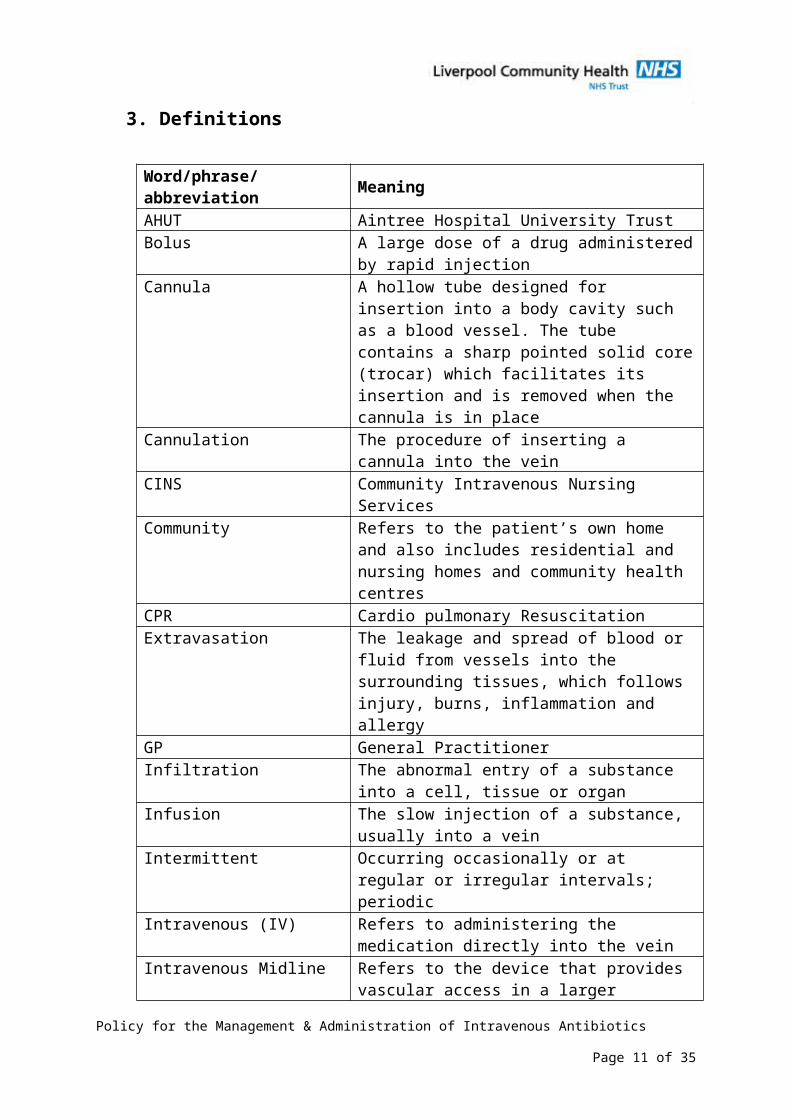
3. Definitions
Word/phrase/abbreviation MeaningAHUT Aintree Hospital University TrustBolus A large dose of a drug administered by rapid
injectionCannula A hollow tube designed for insertion into a body
cavity such as a blood vessel. The tube contains a sharp pointed solid core (trocar) which facilitates its insertion and is removed when the cannula is in place
Cannulation The procedure of inserting a cannula into the vein
CINS Community Intravenous Nursing ServicesCommunity Refers to the patient’s own home and also
includes residential and nursing homes and community health centres
CPR Cardio pulmonary ResuscitationExtravasation The leakage and spread of blood or fluid from
vessels into the surrounding tissues, which follows injury, burns, inflammation and allergy
GP General PractitionerInfiltration The abnormal entry of a substance into a cell,
tissue or organInfusion The slow injection of a substance, usually into a
veinIntermittent Occurring occasionally or at regular or irregular
intervals; periodicIntravenous (IV) Refers to administering the medication directly
into the veinIntravenous Midline Refers to the device that provides vascular
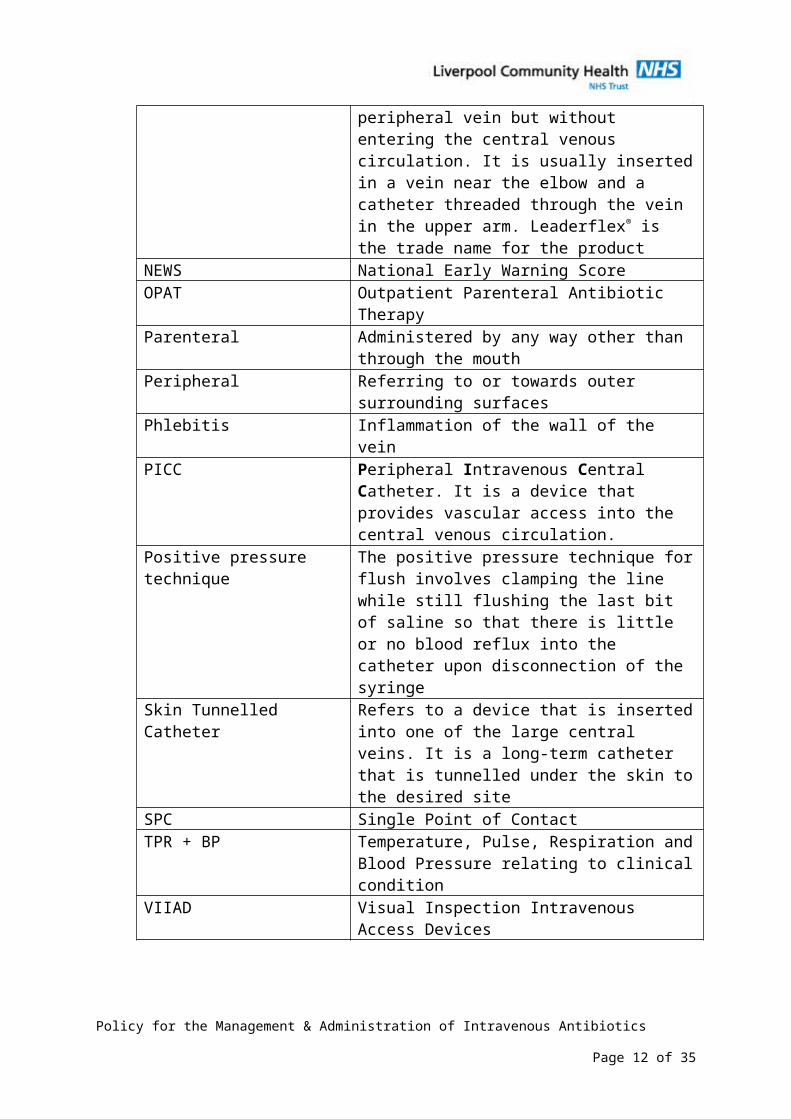
access in a larger peripheral vein but without entering the central venous circulation. It is usually inserted in a vein near the elbow and a catheter threaded through the vein in the upper arm. Leaderflex® is the trade name for the product
NEWS National Early Warning ScoreOPAT Outpatient Parenteral Antibiotic TherapyParenteral Administered by any way other than through
the mouthPeripheral Referring to or towards outer surrounding
surfacesPhlebitis Inflammation of the wall of the veinPICC Peripheral Intravenous Central Catheter. It is a
device that provides vascular access into the central venous circulation.
Policy for the Management & Administration of Intravenous Antibiotics
Page 9 of 27
Positive pressure technique The positive pressure technique for flush involves clamping the line while still flushing the last bit of saline so that there is little or no blood reflux into the catheter upon disconnection of the syringe
Skin Tunnelled Catheter Refers to a device that is inserted into one of the large central veins. It is a long-term catheter that is tunnelled under the skin to the desired site
SPC Single Point of ContactTPR + BP Temperature, Pulse, Respiration and Blood
Pressure relating to clinical conditionVIIAD Visual Inspection Intravenous Access Devices
Policy for the Management & Administration of Intravenous Antibiotics
Page 10 of 27
4. Duties and ResponsibilitiesLiverpool Community Health NHS Trust is responsible for Ensuring that appropriate training is in place so that qualified nurses can fulfil
their duties in accordance with this policy Providing the Hepatitis B vaccine free of charge to all employees at risk of
exposure to blood and body fluids in the course of their duties
Senior Managers and Team Leaders are responsible for The operational implementation of this policy and associated procedures Ensuring that appropriately trained staff are used to deliver the services (this
includes Bank staff and Agency staff) Ensuring that a planned audit cycle is in place
Registered health practitioners are responsible for Securing the Hepatitis B vaccine series Observing standard infection control precautions in particular hand hygiene,
wearing of protective clothing and safe handling and disposal of sharps Complying with the requirements of all relevant NHSLiverpool Community
Health policies applicable to their area of operation Reporting all potential adverse incidents in line with Liverpool Community
Health Risk Management Policy (including serious untoward incidents)
5. Policy5.1 Eligibility criteriaThe clinician responsible for care must use their professional judgement to determine the appropriateness of the individual patient for IV therapy based on the following criteria:
The medical condition of the patient is suitable and stable ( HR = 50-110; RR 9-20; BP systolic = 90-200; temp between 37-39C; alert; orientated) and does not require complex nursing/ medical interventions or care
The psychological condition of the patient is suitable and stable and does not require complex nursing/ medical interventions or care
The following conditions may be treated in the community:
o Bronchiectasiso Endocarditiso Hepatic abscesso HIVo Intravenous access device infectionso MRSA infectionso Osteomyelitiso Prosthetic joint infectionso Septic arthritis/ bursitiso Soft tissue infections/ cellulitis
Policy for the Management & Administration of Intravenous Antibiotics
Page 11 of 27
o Urinary tract infections (UTI)o Wound infections
This list is not exhaustive or exclusive
Satisfactory (minimal risks associated with hygiene, pets or children) home conditions exist, including access to a landline telephone or a mobile connection
The type of antibiotic must be suitable for administration in the community It is the duty of the prescribing clinician/GP/Consultant to liaise with a Consultant Microbiologist/Outpatient Parenteral Antibiotic Lead to establish a treatment plan that is suitable for community management (see Appendix 1 for list of antibiotics) i.e. once or twice daily administration ONLY.
Consideration is given to the arrangements for first and subsequent doses, where anaphylaxis is considered to be a high risk
The patient/carer/family understands the implications of the treatment and how to recognise and report potential complications relating to treatment
Patients meeting eligibility criteria will need to be referred into the service using the Community IV Antibiotics Referral Form (see Appendix 2)
5.2 ConsentInformed consent must be obtained before any procedure is undertaken. Every adult has the right to make their own decisions and must be assumed to have capacity to do so unless it is proved otherwise.
5.3 Medical authorisationWritten medical authorisation should be obtained and include:
Date of authorisation
Patients name and date of birth
Antibiotic name
Dose and rate of administration
Duration of treatment
Signature of medical officer
Special directions
Allergy status
The above constitutes a Patient Specific Direction and the prescribing responsibility and supply of the antibiotic (and diluents required to administer and flush) remains with the authoriser, either secondary care or the patient’s GP (see Appendix 3 for the Community IV Prescription Sheet).
Policy for the Management & Administration of Intravenous Antibiotics
Page 12 of 27
The patients will remain under the care of the Consultant once discharged from secondary care. If patient is referred by GP then the GP will retain medical responsibility.
If the patient is to be treated for cellulitis (excluding facial or peri-orbital) under a PGD when referred into the service by the GP, please refer to Policy 93 Administration of Intravenous Antibiotics via a Patient Group Direction (PGD) in the Community for Patients with Cellulitis who are referred by Liverpool General Practitioners (GP).
5.4 ResponsibilitiesMedical Microbiology/Outpatient Parenteral Antibiotic Lead will be responsible for:
Recommending relevant antibiotics in relation to the infection Available for 24 hr advice
Consultant will be responsible for:
The medical care of the patient prior to discharge In the case of hospital discharges referred to the community, the consultant
will retain medical responsibility and will assess and prescribe IV antibiotics (supply of complete course to be given on discharge)
General Practitioner will be responsible for:
Any unrelated medical conditions In the case of GP referrals, the GP will retain medical responsibility and will
assess and prescribe IV antibiotics Liaising with Medical Microbiology if required
The Intravenous Therapy Team will be responsible for:
Taking referrals from secondary care trusts across Merseyside and the North West for Liverpool patients
To advise regarding suitability for treatment in the community To provide advice and information to patients concerning the condition,
treatment and follow up including emergency telephone numbers To care for intravenous access devices in accordance with NHS Liverpool
Community Health clinical guidance documents and corporate policies To cannulate or insert midline venous access devices To alert medical staff to any reaction to the antibiotics and report
according to the yellow card scheme To be a point of contact for professional advice, support and training for
patients and District Nurses To collate the results of blood tests and alert the patient’s
Consultant/GP/Outpatient Parenteral Antibiotic lead of any significant event.
Policy for the Management & Administration of Intravenous Antibiotics
Page 13 of 27
To maintain accurate records, reviewing care pathway (variances) of each patient receiving care from the Community Intravenous Therapy Team and District Nurses
Enter clinical information contemporaneously on EMIS and hand held patient records
To audit any infections or problems relating to vascular access devices
5.5 Procedures Peripheral cannulation – see Policy 102
Insertion of Midline devices – this is generally done in hospital and should be in place before patient is accepted. However the IV Team is trained to insert using an ultrasound to aid placement
Administration of intravenous medication via bolus - see CINS policy
Administration of intravenous medication via intermittent infusion – see CINS policy
Administration of intravenous medication via continuous infusion – see CINS policy
Management of phlebitis and infiltration
Management of extravasation
5.6 Methods of intravenous drug administration A bolus dose of medication
An intermittent infusion of medication
A continuous infusion of medication – this will not be accepted for community and needs to be referred back to secondary care
5.7 Routes of administration Peripherally inserted cannula
o Short term cannula (may be inserted by a suitably trained health care practitioner)
o Midline cannula (may be inserted by IV Team)
o Peripherally inserted central catheter (PICC line)
Central venous catheter
Care of each access device is almost identical for each procedure. The only differences are with monitoring of complications and flushing solution.Flushing solution is usually 0.9% sodium chloride for each flush unless otherwise stated. Heparinised saline will be used for the final flush for central lines and some
Policy for the Management & Administration of Intravenous Antibiotics
Page 14 of 27
PICC lines – see referral information. See Appendix 6 for NPSA Alert on Heparin flushes.
When monitoring for complications, it is important to monitor the insertion point for all devices but midline and central venous access devices and PICC lines will also require monitoring at the point of termination of the device. For complications to IV line, District Nurses to contact the IV Team.
A cannula inserted in an emergency situation i.e. when existing cannula displaced/ fallen out or if dressing is soiled and where asepsis has been compromised, should be replaced within 24 hours of placement when it is safe to do so rather than leaving for 48-72 hours.
5.8 Equipment Dressing Pack containing sterile towel and Gloves
Plastic Apron
Goggles (only required if patient known to have a blood-borne infection)
Procedure tray
Arm support with disposable procedure towel covering
Surgical tape
2% Chlorhexidine in 70% Isopropyl alcohol impregnated applicator ( SEPP)
Chlorhexidine 2% wipe (e.g. sani cloth)
Skin fixation device (e.g. Stat lock or grip lock)
Semi- Permeable transparent IV dressing
Alcohol hand rub or gel
Small sharps container
For more information see CINS Policy
5.9 General process Suitable patients will be referred between the working hours of 9.00am and
5pm
o By telephone enquiry to Single Point of Contact call centre who pass the information on to the IV Team. Telephone number: 0300 323 0240
o AND by faxing the Referral Form received via safe haven fax machine: 0151 296 7848
o IV Team telephone number: 0151 285 4696
A clear management plan is required prior to patient being discharged from hospital
Patients from AHUT will be discharged on IV antibiotics that are suitable for community management via a community proforma
Policy for the Management & Administration of Intravenous Antibiotics
Page 15 of 27
Patients will generally commence their antibiotic therapy in hospital prior to discharge to the community
Patients being referred by their GP will commence their antibiotics in the community/ at home
If the patient is mobile, arrangements to be made to attend the clinic
If the patient has renal impairment, referrer to confirm antibiotic dose with advice from Consultant Microbiologist
Aseptic technique must be followed
At each visit the health care practitioner must conduct NEWS
At each visit the health care practitioner must assess the cannulation site using the VIADD and VIP score
Active consideration must be given to re-siting the cannula every 48-72 hours by a suitably trained health care practitioner
Plan and document continuing care ensuring that the Patients Electronic Record is contemporaneously updated
Use the smallest gauge cannula most suitable for the patient’s needs
For secondary care referrals a Midline, PICC or Skin Tunnelled Catheter or peripheral cannula will be inserted dependant on the patient’s venous access and the length of intravenous antibiotic therapy required
The Intravenous Therapy Team can insert a midline or cannula in the patient’s home/clinic
If there are any signs of vascular access device infection then this will be reported to the Consultant Microbiologist, Consultant, GP, Outpatient Parenteral Antibiotic Lead and Infection Control Team and reported via Datix
The IV Team/ District Nurses will observe exit site and undertake VIIAD score(see Appendix 4) and VIP score (see Appendix 5) which is kept in patients notes
The IV Team/ District Nurses will prepare IV antibiotics according to manufacturer’s guidelines
The IV Team/ District Nurses will administer IV antibiotics according to prescribed instructions and manufacturers product information sheet which will be supplied with the drug and prescription.
Exceptions to using within the licence are where specialist guidance is in place, when the specialist guidance or formulary should be followed.
The IV Team/ District Nurses will record and monitor the patient’s condition and take blood weekly FBC, U+E, LFT, CRP, ESR, eGFR and antibiotic levels
The IV Team/ District will liaise with the patients Consultant /GP and Consultant Microbiologist/Outpatient Parenteral Antibiotic Lead and they will be informed of any significant event
Policy for the Management & Administration of Intravenous Antibiotics
Page 16 of 27
All nurses will report any hearing loss to the patients Consultant/ GP/ Outpatient Parenteral Antibiotic Lead as Amikacin, Teicoplanin and tobramycin may cause tinnitus, mild hearing loss or vestibular disorders. An auditory assessment may be required
The Consultant/ GP/ Outpatient Parenteral Antibiotic Lead will clearly state in the patient’s notes how they intend to review the patient, when and where and an appointment made
Patients who feel unwell during working hours can contact the Community Intravenous Therapy Team/District Nurses, but out of hours patients will be advised to telephone SPC for advice. Contact Numbers will be given to the patients
Any patient who requires urgent medical attention will be referred to secondary care. Their GP will be informed immediately
If patients have diarrhoea and vomiting advice will be sought from Medical Microbiology and patient’s GP/ consultant. A stool sample will be obtained to determine cause of diarrhoea. All advice will be clearly documented in patient’s notes. Liaise with infection control if appropriate
The Vascular Access Device will be removed by Community Teams upon completion of treatment as detailed in referral
5.10 Adverse incidentsAll patients with an intravenous access device in place must have the IV site checked daily or on each shift for signs of infusion phlebitis. The subsequent score and action(s) taken (if any) must be documented. Use the VIADD and VIP score (see appendix 4 and 5).
The IV site must also be observed: When bolus injections are administered
IV flow rates are checked or altered
When solution containers are changed
The incidence of infusion phlebitis varies; the following Good Practice Points may assist in reducing the incidence of infusion phlebitis:
Observe IV site at least daily
Secure venous access device with a proven highly permeable intravenous dressing
Replace loose, contaminated dressings
Venous access device must be inserted away from joints whenever possible
Aseptic technique must be followed
Active consideration must be given to re-siting the cannula every 48-72 hours
Policy for the Management & Administration of Intravenous Antibiotics
Page 17 of 27
Plan and document continuing care
Use the smallest gauge cannula most suitable for the patient’s need
Replace the cannula at the first indication of infusion phlebitis (stage 2 on the VIP score – See Appendix 5)
6. Training Requirements
All members of the IV Team receive the level of training necessary for them to fulfil their individual responsibilities identified in this policy and have responsibility for maintaining their competencies.
The Community Intravenous Therapy Team will also provide support and competency based training (both practically and theoretically) to all District Nurses.
Before undertaking IV therapy administration, health care practitioners should ensure that they have attended an annual update of management of anaphylaxis and CPR within the last year.
7. Implementation, Monitoring and Review
The Director of Nursing is responsible for ensuring the implementation of this policy. This has been delegated to the IV Team Service Lead
The Director of Nursing is responsible for ensuring that this document is reviewed, and if required revised in the light of legislative guidance or organisational change. This process has been delegated to the IV Team Service Lead
This policy will be reviewed in 3 years unless practice alters in the interim This policy will be audited by
oPatient/ carer satisfaction bi-annuallyoActivityoResponse TimesoTreatment durationoOutcomes
8. Linked InformationThis document should be read in conjunction with NHS Liverpool Community Health policies as below:
Risk Management Strategy (Corporate Policy; Health Safety & Risk)
Policy for the Management & Administration of Intravenous Antibiotics
Page 18 of 27
Assessment Please detail below assessment of patients condition
LCH Waste Management Policy (Corporate Policy; Health Safety & Risk) Clinical Policy 135: Infection Prevention Control Clinical Policy 163 – Venepuncture Clinical Policy 95 – Patient Identification Clinical Policy 54 – Blood Transfusion Clinical Policy 91 – Consent to Treatment Clinical Policy 95 – Patient Identification Clinical Policy 32 - Cold Chain Clinical Policy 93 - Administration of Intravenous Antibiotics via a Patient
Group Direction (PGD) in the Community for Patients with Cellulitis who are referred by Liverpool General Practitioners (GP)
Guideline 15 HIV
9. References
This following guidance was used in the production of this document:
Royal College of Nursing October 2003 Standards for Infusion Therapy Nursing and Midwifery Council April `Standards for Medicine
Management`(2008)
Nursing and Midwifery Council ( March 2015) The Code CINS guidelines 2012-2014 Care and Maintanence of Venous Access
Devices
Pan Mersey Antimicrobial Guidelines and Management of Common Infections in Primary Care 2015/16
Pratt et al; National evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England; Journal of Hospital Infection (2007) 65S, S1-s64, 5th February 2007
Policy for the Management & Administration of Intravenous Antibiotics
Page 19 of 27
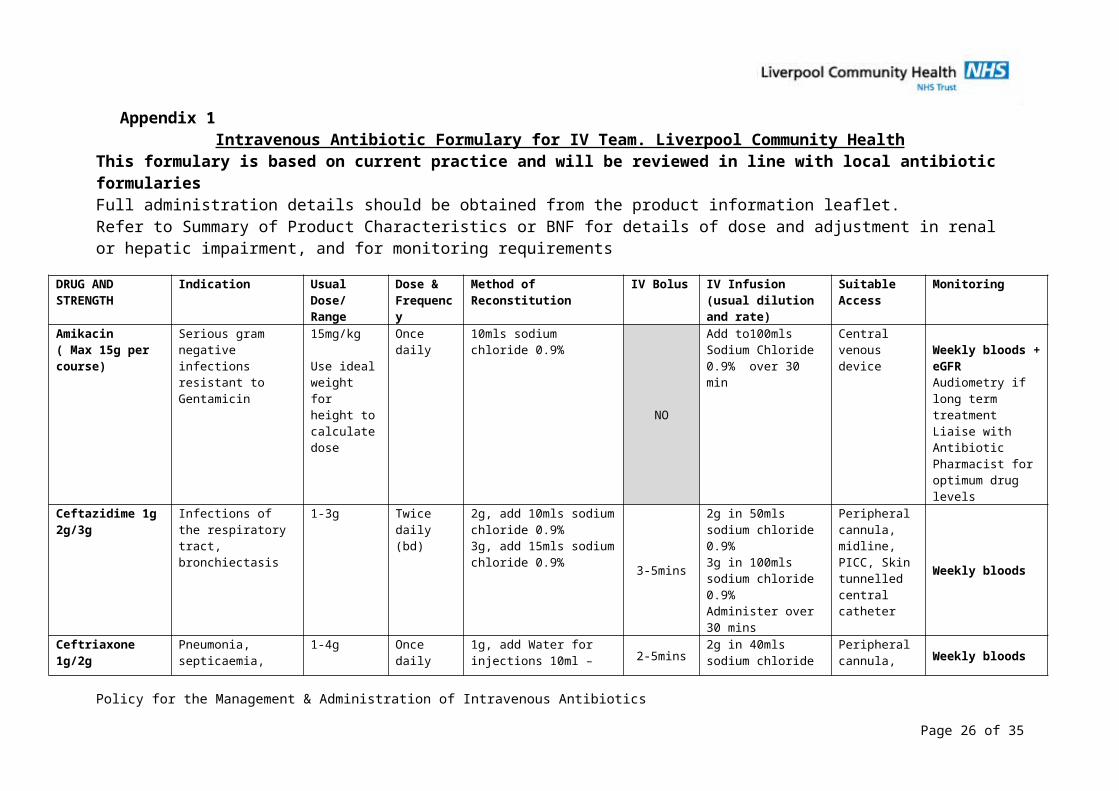
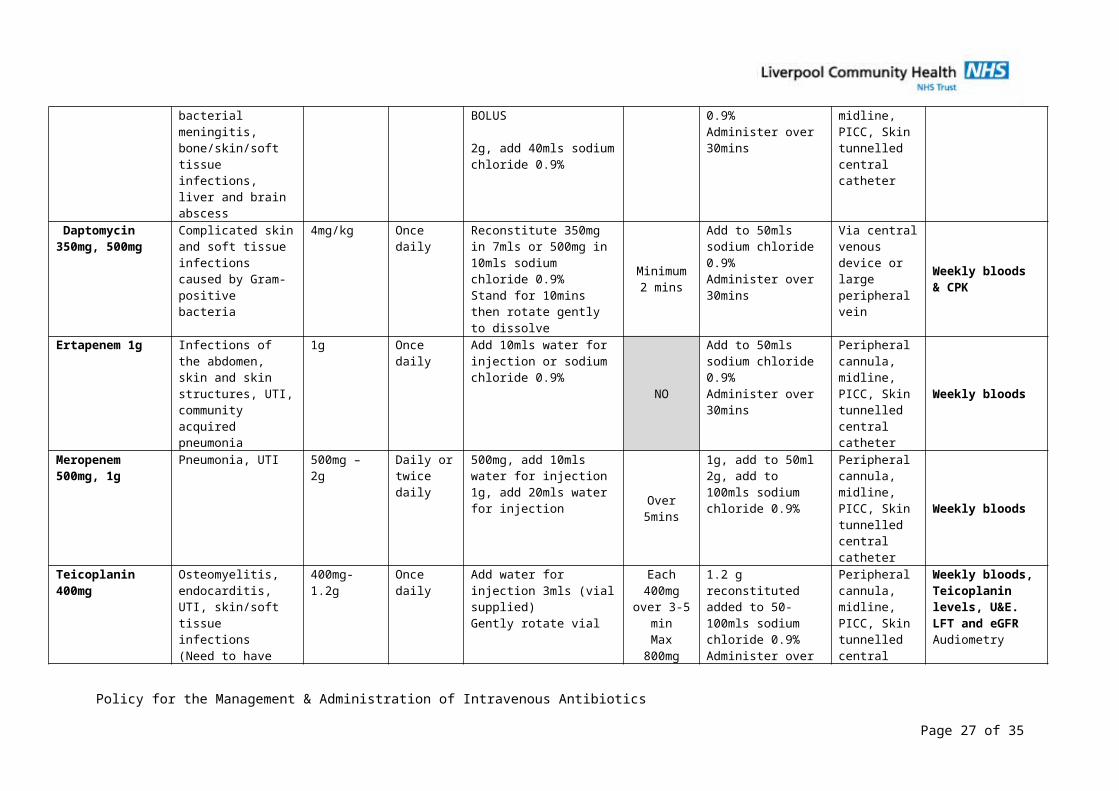
Appendix 1Intravenous Antibiotic Formulary for IV Team. Liverpool Community Health
This formulary is based on current practice and will be reviewed in line with local antibiotic formulariesFull administration details should be obtained from the product information leaflet.Refer to Summary of Product Characteristics or BNF for details of dose and adjustment in renal or hepatic impairment, and for monitoring requirements
DRUG AND STRENGTH
Indication Usual Dose/ Range
Dose & Frequency
Method of Reconstitution IV Bolus IV Infusion (usual dilution and rate)
Suitable Access
Monitoring
Amikacin( Max 15g per course)
Serious gram negative infections resistant to Gentamicin
15mg/kg
Use ideal weight for height to calculate dose
Once daily 10mls sodium chloride 0.9%
NO
Add to100mls Sodium Chloride 0.9% over 30 min
Central venous device Weekly bloods +
eGFRAudiometry if long term treatmentLiaise with Antibiotic Pharmacist for optimum drug levels
Ceftazidime 1g 2g/3g
Infections of the respiratory tract, bronchiectasis
1-3g Twice daily (bd)
2g, add 10mls sodium chloride 0.9%3g, add 15mls sodium chloride 0.9% 3-5mins
2g in 50mls sodium chloride 0.9%3g in 100mls sodium chloride 0.9%Administer over 30 mins
Peripheral cannula, midline, PICC, Skin tunnelled central catheter
Weekly bloods
Ceftriaxone 1g/2g Pneumonia, septicaemia, bacterial meningitis, bone/skin/soft tissue infections, liver and brain abscess
1-4g Once daily 1g, add Water for injections 10ml – BOLUS
2g, add 40mls sodium chloride 0.9%
2-5mins
2g in 40mls sodium chloride 0.9% Administer over 30mins
Peripheral cannula, midline, PICC, Skin tunnelled central catheter
Weekly bloods
Daptomycin 350mg, 500mg
Complicated skin and soft tissue infections caused by Gram-positive bacteria
4mg/kg Once daily Reconstitute 350mg in 7mls or 500mg in 10mls sodium chloride 0.9%Stand for 10mins then rotate gently to dissolve
Minimum2 mins
Add to 50mls sodium chloride 0.9%Administer over 30mins
Via central venous device or large peripheral vein
Weekly bloods& CPK
Ertapenem 1g Infections of the abdomen, skin and skin structures, UTI, community acquired
1g Once daily Add 10mls water for injection or sodium chloride 0.9%
NO Add to 50mls sodium chloride 0.9%Administer over 30mins
Peripheral cannula, midline, PICC, Skin tunnelled
Weekly bloods
Policy for the Management & Administration of Intravenous Antibiotics
Page 20 of 27
pneumonia central catheter
Meropenem 500mg, 1g
Pneumonia, UTI 500mg – 2g Daily or twice daily
500mg, add 10mls water for injection1g, add 20mls water for injection
Over 5mins
1g, add to 50ml2g, add to 100mls sodium chloride 0.9%
Peripheral cannula, midline, PICC, Skin tunnelled central catheter
Weekly bloods
Teicoplanin 400mg Osteomyelitis, endocarditis, UTI, skin/soft tissue infections(Need to have eGFR above 20)
400mg-1.2g Once daily Add water for injection 3mls (vial supplied) Gently rotate vial
Each 400mg
over 3-5 minMax
800mg
1.2 g reconstituted added to 50-100mls sodium chloride 0.9%Administer over 30mins
Peripheral cannula, midline, PICC, Skin tunnelled central catheter
Weekly bloods,Teicoplanin levels, U&E. LFT and eGFR Audiometry
Tigecycline 50 mg
Complicated intra-abdominal infection, complicated skin and soft tissue infections
50mg (following initial dose of 100mg
Twice daily (bd)
5.3mls sodium chloride 0.9%
NO
Add to 100mls sodium chloride 0.9%Administer over 30-60 minutes
Peripheral cannula, midline, PICC, Skin tunnelled central catheter
Weekly bloods
Tobramycin 40mg /ml
Infections of respiratory tract including pneumonia, biliary tract infections
3mg/kg daily Twice daily(bd)
Does not need reconstitution
Slow IV injection
50 -100mls sodium chloride 0.9% over 20-60 mins
Peripheral cannula, midline, PICC, Skin tunnelled central catheter
Weekly bloodsAudiometry
Policy for the Management & Administration of Intravenous Antibiotics
Page 21 of 27
Appendix 2
Appendix 3
Appendix 4
VIIAD Charts
Policy for the Management & Administration of Intravenous Antibiotics Page 24 of 27
Policy for the Management & Administration of Intravenous Antibiotics Page 25 of 27
Appendix 5
Visual Inspection Phlebitis Score (VIP)
Policy for the Management & Administration of Intravenous Antibiotics Page 26 of 27
Appendix 6
NPSA Heparin AlertAll health care professionals should be aware of the NPSA Rapid Response Report NPSA/2008/RRR002 re risks with Intravenous Heparin Flush Solutions.
IV Heparin flushes are widely used in healthcare to keep both indwelling and peripheral lines patent. Risk of harm to patients can be caused through poor practice such as the use of heparin flushes which are not formally prescribed or subject to a patient group direction, mis-selection for other medicine products, miscalculation and mis-preparation.
The report reviewed patient safety incident reports concerning mis-selection of sodium heparin products and at time of report had received 28 incidents.
Supporting information on this Rapid Response Report is available at www.npsa.nhs.uk/patientsafety
Liverpool Community Health recommends Heparin Sodium 10 iu/ml (50 units in 5ml) for the flushing of Skin Tunnelled Central Venous Catheters, open ended Peripherally Inserted Central Catheters (PICC) and peripheral midlines.
Heparin Sodium 100 units/ml (usual dose 400 units in 4ml) for the monthly flushing of Portacaths or as directed.
For any advice contact the IV therapy team on 0151 285 4696
Policy for the Management & Administration of Intravenous Antibiotics Page 27 of 27