Embed Size (px)
Citation preview

Non-PurulentSkinandSoftTissueInfectionsintheEmergencyDepartment
KrishanYadav
ThesissubmittedtotheFacultyofGraduateandPostdoctoralStudiesinpartial
fulfillmentofthedegreerequirementsfortheM.Sc.inEpidemiology
SchoolofEpidemiology
FacultyofMedicine
UniversityofOttawa
©KrishanYadav,Ottawa,Canada,2018

ii
AbstractNon-purulentskinandsofttissueinfections(SSTIs)involvetheepidermisand
dermisandarecommonlymanagedintheemergencydepartment(ED).Current
guidelineslackevidencetoguidecliniciansonoptimalmanagement.Theaimofthis
thesiswastodescribetheepidemiologyofadultswithnon-purulentSSTIs
presentingtotheED.Secondarygoalsweretoidentifyfactorsassociatedwithoral
antibiotictreatmentfailure;describeanoutpatientparenteralantibiotictherapy
(OPAT)clinic-to-EDprogram;anddeterminephysicianrationaleforselecting
intravenoustherapy.Weconductedahealthrecordsreviewandprospective
observationalcohortstudy.
Therewassignificantphysicianpracticevariationandanunexpectedlyhigh
hospitalizationrate.Weidentifiedfourfactorsassociatedwithoralantibiotic
treatmentfailure(tachypnea,chroniculcers,historyofmethicillinresistant
Staphylococcusaureuscolonizationorinfection,andcellulitisinthepast12months).
AnED-to-OPATclinicprogramwasfoundtobesafe,withlowtreatmentfailure
ratesandhighpatientsatisfaction.

iii
ExecutiveSummaryNon-purulentskinandsofttissueinfections(SSTIs)describeinfectionsofthe
superficialepidermisanddermis(erysipelas)orinvolvementofthedeepdermis
andsubcutaneoustissue(cellulitis).Theseinfectionsarecommonlydiagnosedand
managedintheemergencydepartment(ED)setting.Therearenostudiesthathave
describedtheepidemiologyofadultswithnon-purulentSSTIswhoaremanagedin
theED.Furthermore;currentguidelinesarebasedonexpertopinionandlack
evidencetoguidephysiciansontheoptimalrouteofantibiotictherapy(oralversus
intravenous).
Theaimofthisthesisprojectwastodescribetheepidemiologyofadultswithnon-
purulentSSTIswhopresenttotheED.Secondarygoalswereto:(1)identify
predictorsassociatedwithoralantibiotictreatmentfailure;(2)describeemergency
physicianrationaleforselectingtheintravenousroute;and(3)describetherateof
treatmentfailure,adverseeventsandoverallpatientsatisfactionforadultstreated
atanoutpatientparenteralantimicrobialtherapy(OPAT)clinicafterinitial
diagnosisandmanagementintheED.Tomeetthesegoals,weconductedahealth
recordsreviewandprospectiveobservationalcohortstudy.
Thefindingsfromthisthesisprojectareimportantfirststepstobetterunderstand
whatfactorspredisposetooralantibiotictreatmentfailure,whyemergency

iv
physiciansselecttheintravenousroute,andpatientoutcomesinanED-to-OPAT
clinicmodelformanagementofnon-purulentSSTIs.
ContributionsoftheAuthorsDr.KrishanYadavisthefirstauthorofbothmanuscriptsandwasprimarily
responsibleforstudydesign,datacollection,statisticalanalysisandwritingofthe
manuscripts.Bothmanuscriptswereco-authoredbyDr.Yadav’sthesissupervisors
Dr.IanGStiellandDr.GeorgeWells,andthesisadvisorycommitteememberDr.
KathrynSuh.Twomedicalstudents(Mr.JohnMacisaacandMr.DarmynRitchie)
aidedinchartreviewanddatacollectionforthehealthrecordsreview.Mr.Jordan
Bernickprovidedhelpfulfeedbackregardingstatisticalanalysis.Drs.Eaglesand
Thiruganasambandamoorthyprovidedhelpfulsuggestionsandfeedbackforboth
manuscripts.Drs.Stiell,WellsandSuhprovidedvaluablefeedbackthroughoutthe
entireprocess.

v
AcknowledgmentsIwouldliketothankmyprimarythesissupervisorDr.IanGStiellforhisimmense
support,mentorshipandguidanceoverthepastthreeyears.Iwillforeverbe
gratefulfortheopportunitytolearnfromDr.Stiell;Ihopetomakehimproudwith
myplannedfutureresearchendeavors.Itwasanequalhonourandprivilegetohave
theguidanceandexpertiseofmyco-supervisor,Dr.GeorgeWells.Ilearnedagreat
dealandalwaysenjoyedourmeetingstodiscussstatistics,researchandlifein
general.IoweahugedebtofgratitudetoDr.KathrynSuh.Herexpertise,
encouragementandmentorshipweregreatlyappreciated.Ilookforwardtofuture
researchcollaborationswithDr.Suhandherteam.
AsincerethankstoAngelaMarcantonio,CatherineClementandtheDepartmentof
EmergencyMedicineresearchteam.Ifeelveryfortunatetohavehadthe
opportunitytoworkwithandlearnfromsuchaterrificgroup.
Thankyoutomyfamilyforallofyoursupportandlove.MywifeJesshasbeen
integraltothisentireprojectandincrediblysupportiveeverystepoftheway–I
cannotthankyouenough.Iameternallygratefultomyparentsforencouragingme
topursuemydreamsandtofurthermyeducationeverystepoftheway.Finally,I
dedicatethisthesistotwoveryspeciallittlepeople:AnandYadavandPriyanka
(Bean)Yadav.Idohopethatthisworkonedayinspiresyoutopursueandachieve
yourowngoalsanddreams.

vi
TableofContentsAbstract......................................................................................................................................ii
ExecutiveSummary...............................................................................................................iiiContributionsoftheAuthors.............................................................................................iv
Acknowledgments....................................................................................................................v
TableofContents....................................................................................................................viListofTables............................................................................................................................ix
ListofFigures..........................................................................................................................xi
AbbreviationsUsedintheText........................................................................................xiiChapterOne:Introduction...................................................................................................11.Introduction...................................................................................................................................12.Rationale.........................................................................................................................................23.ThesisGoalsandObjectives......................................................................................................2ChapterOne........................................................................................................................................3ChapterTwo.......................................................................................................................................3ChapterThree....................................................................................................................................3ChapterFour.......................................................................................................................................4ChapterFive........................................................................................................................................4
ChapterTwo:Background...................................................................................................61.Introduction...................................................................................................................................62.Background....................................................................................................................................62.1Classification..............................................................................................................................................62.2Incidence&BurdenofDisease..........................................................................................................72.3Etiology&RiskFactors.........................................................................................................................82.4ClinicalFeatures&Complications....................................................................................................92.5Diagnosis..................................................................................................................................................102.6CurrentGuidelines...............................................................................................................................102.7OralversusIntravenousTherapy..................................................................................................122.8EDTreatment.........................................................................................................................................142.9QuestionsSurroundingOptimalEDManagementofSSTIs................................................212.10TreatmentFailure..............................................................................................................................212.11PredictorsofTreatmentFailureWithOralAntibiotics.....................................................252.12OralVersusTheIntravenousRoute:EmergencyPhysicianRationaleforSelectingIntravenousTherapy..................................................................................................................................26
3.Rationale......................................................................................................................................27References........................................................................................................................................29
ChapterThree:PredictorsofOralAntibioticFailureforNon-PurulentSkinandSoftTissueInfectionsintheEmergencyDepartment...............................................35ChapterOverview..........................................................................................................................35Introduction.....................................................................................................................................39Methods.............................................................................................................................................40

vii
StudyDesignandSetting..........................................................................................................................40Population.......................................................................................................................................................40StudyProtocolandDataAbstraction..................................................................................................41OutcomeMeasures......................................................................................................................................42StatisticalAnalysis.......................................................................................................................................43SampleSizeandFeasibility......................................................................................................................44
Results...............................................................................................................................................45Discussion.........................................................................................................................................48InterpretationofResults...........................................................................................................................48PreviousStudies...........................................................................................................................................49Strengths..........................................................................................................................................................49Limitations......................................................................................................................................................49ClinicalImplications...................................................................................................................................51ResearchImplications................................................................................................................................52
Conclusions......................................................................................................................................52References........................................................................................................................................53Figures...............................................................................................................................................56Tables.................................................................................................................................................57SupplementaryAppendix...........................................................................................................65
ChapterFour:OutpatientParenteralAntibioticTherapyFollowingEmergencyDepartmentTreatmentofNon-PurulentSkinandSoftTissueInfections.........77ChapterOverview..........................................................................................................................77Abstract.............................................................................................................................................80Methods.............................................................................................................................................83StudyDesignandSetting..........................................................................................................................83StudyPopulation..........................................................................................................................................84IntravenousAntibioticTreatment........................................................................................................84DataCollection..............................................................................................................................................84OutcomeMeasures......................................................................................................................................85DataAnalysis..................................................................................................................................................86SampleSize.....................................................................................................................................................87
Results...............................................................................................................................................87Discussion.........................................................................................................................................89InterpretationofResults...........................................................................................................................89PreviousStudies...........................................................................................................................................90Strengths..........................................................................................................................................................90Limitations......................................................................................................................................................91ClinicalImplications...................................................................................................................................92ResearchImplications................................................................................................................................93
Conclusion........................................................................................................................................93References........................................................................................................................................94Figures...............................................................................................................................................97Tables.................................................................................................................................................98SupplementaryAppendix.........................................................................................................105
ChapterFive:Discussion..................................................................................................114Introduction...................................................................................................................................114InterpretationofResults...........................................................................................................114PreviousStudies...........................................................................................................................116Strengths.........................................................................................................................................118

viii
Limitations.....................................................................................................................................118ClinicalImplications...................................................................................................................120ResearchImplications................................................................................................................122Conclusions....................................................................................................................................124References......................................................................................................................................126
AppendixA:OttawaHealthScienceNetworkResearchEthicsBoardApprovalLetter......................................................................................................................................129
AppendixB:MethodsforDevelopingaMultivariableLogisticRegressionModelforPredictorsofOralAntibioticTreatmentFailure.................................130Introduction...................................................................................................................................130ExploratoryAnalysis...................................................................................................................130Outliers...........................................................................................................................................................131MissingData.................................................................................................................................................131ExcludingVariables...................................................................................................................................131Associationsbetweencategoricalvariables...................................................................................133Correlationbetweencontinuousvariables.....................................................................................133
LogisticRegressionAnalysis....................................................................................................134UnivariateAnalysis...................................................................................................................................134AssessingforInteraction........................................................................................................................138MultivariableLogisticRegression:PreliminaryModel.............................................................139SecondaryAnalysis(ComparingOralvs.IntravenousTreatmentGroups).....................141
Discussion.......................................................................................................................................143Conclusion......................................................................................................................................144References......................................................................................................................................146

ix
ListofTablesChapterThreeTable1.BaselineCharacteristicsofAdultswithNonpurulentSkinandSoftTissueInfections
seenintheEmergencyDepartment(N=500)..................................................................................57Table2.PresentingPatientandInfectionCharacteristics(N=500).................................................58Table3.EmergencyDepartmentTreatment(N=500)...........................................................................59Table4.AntibioticTreatmentfor352PatientsDischargedfromtheED......................................60Table5.AdverseEventsfor352PatientsDischargedfromtheED..................................................61Table6.OutpatientParenteralAntibioticTherapy(OPAT)ClinicData(N=85).........................62Table7.TreatmentFailurewithOralAntibiotics(N=85of288PatientsTreatedwitha
Minimumof48HoursofOralTherapy).............................................................................................63Table8.PredictorsAssociatedwithOralAntibioticTreatmentFailureUsingMultivariable
LogisticRegression(N=288)...................................................................................................................64TableS1.VariableDefinitions...........................................................................................................................72TableS2.UnivariateAssociationwithOralAntibioticTreatmentFailurefor288EDPatients
TreatedwithaMinimumof48HoursofOralTherapy...............................................................73TableS3.TreatmentFailurewithIVAntibiotics(N=12of212PatientsTreatedwitha
Minimumof48HoursofIVTherapy).................................................................................................74TableS4.SecondaryAnalysisComparingOralversusIntravenousAntibioticGroupsfor
CategoricalVariablesforall500Patients.........................................................................................75TableS5.SecondaryAnalysisComparingOralversusIntravenousAntibioticGroupsfor
ContinuousVariablesforall500Patients.........................................................................................76ChapterFourTable1.BaselineCharacteristicsofAdultswihtNon-PurulentSkinandSoftTissue
Infections(SSTIs)seenintheED(N=153).....................................................................................98Table2.PresentingPatientandInfectionCharacteristics(N=153).................................................99Table3.IntravenousAntibioticTreatmentAdministeredWhileintheED(N=153).............100Table4.IntravenousAntibioticPrescriptionsforPatientsDischargedfromtheED(N=153)
............................................................................................................................................................................101Table5.EmergencyPhysicianRationaleforIVAntibioticsforall153Patients.......................102Table6.OutpatientParenteralAntibioticTherapy(OPAT)ClinicData(N=137)....................103Table7.Outcomesat14DaysfromIndexEDVisitfor137PatientsNotLosttoFollow-up104TableS1.ReasonsforHospitalizationwithin14DaysofEDVisitfor137Patientswho
attendedtheirOPATClinicAppointment........................................................................................113AppendixBTableB1.UnivariateAssociationofCharacteristicswithTreatmentFailureoftheStudy
Participants(N=288)................................................................................................................................132TableB2.AssessmentofSimpleCollinearityBetweenCategoricalVariablesUsingthePhi
Coefficient......................................................................................................................................................133

x
TableB3.CorrelationBetweenContinuousVariablesUsingPearsonCorrelationCoefficient(r)......................................................................................................................................................................134
TableB4.UnivariateLogisticRegressionforAgeasaPredictorofOralAntibioticTreatmentFailure.............................................................................................................................................................135
TableB5.UnivariateLogisticRegressionforSystolicBloodPressureasaPredictorofOralAntibioticTreatmentFailure................................................................................................................135
TableB6.UnivariateLogisticRegressionforHeartRateasaPredictorofOralAntibioticTreatmentFailure......................................................................................................................................136
TableB7.UnivariateLogisticRegressionforTemperatureasaPredictorofOralAntibioticTreatmentFailure......................................................................................................................................136
TableB8.UnivariateLogisticRegressionforRespiratoryRateasaPredictorofOralAntibioticTreatmentFailure................................................................................................................136
TableB9.SimpleUnivariateLogisticRegressionforCategoricalVariables...............................137TableB10.AssessmentofPossibleInteractionTerms........................................................................138TableB11.MultivariableLogisticRegressionModelofPredictorsAssociatedwithOral
AntibioticTreatmentFailure(N=288).............................................................................................139TableB12.MultivariableLogisticRegressionModelUsingBackwardsSelectionof
PredictorsofOralAntibioticTreatmentFailure(N=288).......................................................140TableB13.FinalMultivariableLogisticRegressionModelofPredictorsAssociatedwithOral
AntibioticTreatmentFailure(N=288).............................................................................................140TableB14.SecondaryAnalysisComparingOralversusIntravenousAntibioticGroupsfor
CategoricalVariablesforall500Patients.......................................................................................142TableB15.SecondaryAnalysisComparingOralversusIntravenousAntibioticGroupsfor
ContinuousVariablesforall500Patients.......................................................................................143

xi
ListofFiguresChapterTwoFigure1.Classificationofskinandsofttissueinfections(SSTIs).........................................................8Figure2.EDTreatmentPathwaysforPatientswithSSTIs..................................................................15ChapterThreeFigure1.FlowDiagramofPatientEligibilityandOutcomes...............................................................56FigureS1.StandardizedCaseRecordForm................................................................................................65ChapterFourFigure1.FlowDiagram........................................................................................................................................97FigureS1.OPATClinicReferralForm..........................................................................................................105FigureS2.StandardizedCaseRecordForm..............................................................................................106

xii
AbbreviationsUsedintheTextSSTI–skinandsofttissueinfections
ED–emergencydepartment
OPAT–outpatientparenteralantibiotictherapy
CA-MRSA–communityacquiredmethicillinresistantstaphylococcusaureus
MRSA–methicillinresistantstaphylococcusaureus
ABSSI–acutebacterialskinandskinstructureinfections
IDSA–InfectiousDiseaseSocietyofAmerica
CREST–clinicalresourceefficiencysupportteam
PICC–peripherallyinsertedcentralcatheter
CCAC–communitycareaccesscentre
LHIN–localhealthintegrationnetwork
CDER–centerfordrugevaluationandresearch
CI–confidenceinterval
OR–oddsratio
ICD-10-CA–InternationalClassificationofDiseases,10threvision,Canada
IQR–interquartilerange

1
ChapterOne:Introduction
1.IntroductionSkinandsofttissueinfections(SSTIs)refertoaspectrumofdiseaseprocessesthat
encompassbacterialinfectionsoftheepidermisanddeeperdermallayers.Severity
rangesfromsuperficialprocesses(erysipelasandcellulitis)tolife-orlimb-
threateninginfectionsofdeeperstructures(necrotizingfasciitis).Non-purulent
SSTIsarethesubsetofinfectionsthatdonotcontainpus(acollectionofwhiteblood
cells,nonviabletissuesanddegradedcellularcontents).Non-purulentSSTIsare
commonandaccountforapproximately14.5millioncasesannuallyintheUnited
Statesalone.1However,cliniciansarefacedwithmanychallengesinbothdiagnosis
andmanagementofthisseeminglysimplediseaseentity.
SSTIsremainaclinicaldiagnosis.Therearemanydiagnosticmimics,includingbut
notlimitedto:deepvenousthrombosis;stasisdermatitis;hematoma;gout;and
contactdermatitis.Attimesitmaybedifficulttodifferentiatenon-purulentSSTIs
fromabscesses.Thisisimportant,asthelatteristreatedwithsurgicalincisionand
drainageasopposedtoantibioticsalone.Therearenospecificlaboratoryteststo
confirmthediagnosis.The2014InfectiousDiseaseSocietyofAmericaguidelinesin
factrecommendagainstroutinelaboratorytestingfornon-purulentSSTIs–
includingbloodtests,biopsyculturesorswabs.2Oncethediagnosisismade,
cliniciansareexpectedtoselectappropriateantimicrobialtherapy.Decidingon
optimaltreatmentiscomplicatedbytheneedtoselectnotonlythecorrect
antimicrobialagent,butalsothecorrectrouteofdelivery(oralversusintravenous).

2
Duetothelackofevidence,currentguidelinesonmanagementofSSTIsarebased
onexpertopinion.2,3
2.RationaleAccuratediagnosisandappropriatetreatmentofSSTIsarecriticalforpatientsafety,
optimizingclinicaloutcomeanddecreasinghealthcarecostsandoverallburden.The
epidemiologyofSSTIshasbeenwelldocumentedintwodistinctpopulations:
hospitalizedpatientsandthosewhoseekcareatphysicians’offices.4-6However,
therearenostudiesthathavedescribedtheepidemiologyofadultswithSSTIswho
seekcareintheEmergencyDepartment(ED).Thisconstitutesasignificantevidence
gapwhenoneconsidersthatSSTIsaccountforasmuchas3%ofallEDvisits.7A
thoroughunderstandingoftheepidemiologyofnon-purulentSSTIsintheED
patientpopulationwouldprovideanimportantbasistowarddevelopingmore
appropriateevidence-basedrecommendationsformanagementofthiscommon
condition.
3.ThesisGoalsandObjectivesTheprincipalgoalofthisthesisistoobtainathoroughunderstandingofthe
epidemiologyofnon-purulentSSTIsinadultswhoaremanagedinaCanadianED
setting.Asecondarygoalwillbetoidentifyanyvariablesindependentlyassociated
withtheoutcomeoftreatmentfailurewithoralandintravenousantibioticsat14
daysfromtheindexEDvisit.Thesegoalswillbeaddressedthroughahealthrecords
review(StudyA)ofallpatientspresentingtotheEDwithnon-purulentSSTIs.A

3
thirdgoalwillbetodescribethefunctionandoutcomesofanOutpatientParenteral
AntibioticTherapy(OPAT)CliniconadultEDpatientswithSSTIsthatarefeltto
requireintravenoustherapy.Thisstudywillspecificallydescribetheoutcomeof
OPATtreatmentfailureandemergencyphysicianrationaleforselectingintravenous
antibioticsfornon-purulentSSTIs.AprospectiveobservationalcohortstudyofED
patientstreatedattheOPATClinicwillbeconducted(StudyB)toaddressthisfinal
goal.
Theobjectivesofeachchapterinthisthesisareasfollows:
ChapterOneAbriefintroductionthatprovides:(a)therationaleandimportanceofresearching
EDpatientswithnon-purulentSSTIs;(b)thethesisgoalsandobjectives;and(c)the
objectivesofeachchapter.
ChapterTwoThischapterprovidesthebackgrounddiscussionconcerningthepathophysiology,
diagnosisandoutpatientmanagementofnon-purulentSSTIsintheEDsetting.
ChapterThreeAmanuscriptofthehealthrecordsreview(StudyA).Thegoalsofthemanuscript
areto:1)describetheepidemiologyofnon-purulentSSTIsinadultswithSSTIswho
presenttotheED;and2)identifyvariablesindependentlyassociatedwiththe

4
clinicaloutcomeoftreatmentfailurewithoralantibioticsat14daysfromtheindex
EDvisit.
ChapterFourAmanuscriptoftheprospectiveobservationalcohortstudy(StudyB).Thegoalsof
themanuscriptareto:1)describeoutcomesoftheOPATClinicinEDpatients
includingOPATtreatmentfailureandpatientadverseevents;2)assesspatient
satisfactionwithOPAT;and3)identifyemergencyphysicianrationaleforselecting
intravenousantibiotics.
ChapterFiveAdiscussionbasedonthecombinedresultsofStudyAandStudyB.Inadditionto
summarizingtheresultsanddrawingconclusions,implicationsforfutureresearch
willbedetermined.

5
References
1. RaffAB,KroshinskyD.Cellulitis:AReview.JAMA.2016;316(3):325-337.doi:310.1001/jama.2016.8825.
2. StevensDL,BisnoAL,ChambersHF,etal.Practiceguidelinesforthediagnosisandmanagementofskinandsofttissueinfections:2014updatebytheInfectiousDiseasesSocietyofAmerica.ClinInfectDis.2014;59(2):e10-52.doi:10.1093/cid/ciu1444.
3. ClinicalResourceEfficiencySupportTeam(2005)Guidelinesonthemanagementofcellulitisinadults.CREST,Belfast..
4. Perello-AlzamoraMR,Santos-DuranJC,Sanchez-BarbaM,CanuetoJ,MarcosM,UnamunoP.Clinicalandepidemiologicalcharacteristicsofadultpatientshospitalizedforerysipelasandcellulitis.EurJClinMicrobiolInfectDis.2012;31(9):2147-2152.
5. ZervosMJ,FreemanK,VoL,etal.Epidemiologyandoutcomesofcomplicatedskinandsofttissueinfectionsinhospitalizedpatients.JClinMicrobiol.2012;50(2):238-245.
6. PallinDJ,EspinolaJA,LeungDY,HooperDC,CamargoCA,Jr.EpidemiologyofdermatitisandskininfectionsinUnitedStatesphysicians'offices,1993-2005.ClinInfectDis.2009;49(6):901-907.doi:910.1086/605434.
7. PallinDJ,EganDJ,PelletierAJ,EspinolaJA,HooperDC,CamargoCA,Jr.IncreasedUSemergencydepartmentvisitsforskinandsofttissueinfections,andchangesinantibioticchoices,duringtheemergenceofcommunity-associatedmethicillin-resistantStaphylococcusaureus.AnnEmergMed.2008;51(3):291-298.doi:210.1016/j.annemergmed.2007.1012.1004.Epub2008Jan1028.

6
ChapterTwo:Background
1.IntroductionUncomplicated,non-purulentskinandsofttissueinfections(SSTIs)describe
infectionsofthesuperficialepidermisanddermis(erysipelas)oradditionaldeeper
involvementincludingthedeepdermisandsubcutaneoustissue(cellulitis).1
Patientswithnon-purulentSSTIspresentwithredness,painandswellingofthe
involvedskin.Itisimportanttonotethatthereisanabsenceofanypurulent(i.e.
pus-containing)materialorabscess.TheEmergencyDepartment(ED)physician
mustfirstestablishthediagnosis,andthendecideontheoptimalagent,dose,
frequency,routeandsettingforantimicrobialtherapy.Thesedecisionshavebeen
complicatedfurtherbytheincreasingprevalenceofcommunityacquired
methicillin-resistantStaphylococcusaureus(CA-MRSA).2,3Appropriatediagnosis
andmanagementofSSTIsiscrucialinordertopreventcomplicationssuchas
bacteremiaorthedevelopmentofnecrotizingfasciitis.
2.Background
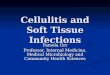
2.1ClassificationSSTIsmaybesubdividedintopurulentornon-purulentcategories(Figure1).
PurulentSSTIsareinfectionsthatcontainpus,whichisacollectionofwhiteblood
cells,nonviabletissueanddegradedcellularcontents.PurulentSSTIsinclude
furuncles(purulentmaterialfromthehairfollicle–alsocalledaboil);carbuncles
(collectionoffuruncleswithcommunicatingtracts);andabscesses(deeperwalled-
offcollectionofpurulentmaterial).Whenfeasiblethissubgroupistreatedwith

7
surgicalincisionanddrainage.Antibioticsarerecommendedonlyiftherearesigns
ofsystemicillness.4Non-purulentSSTIsarenotamenabletosurgicaldrainage.
Instead,thissubgroupistreatedwithantibiotics.Non-purulentSSTIsmaybe
furthersubdividedintouncomplicatedversuscomplicatedcategories.
Uncomplicatednon-purulentSSTIsincludecellulitisanderysipelas.Complicated
non-purulentSSTIsconsistoflife-threateningnecrotizinginfectionsofdeeper
tissues,includingthefasciaormuscle.Necrotizinginfectionsarerapidlyprogressive
andcreatesignificantdestructionoftissue.Patientswithnecrotizinginfections
classicallypresentwithseverepainoutofproportiontothefindingsonclinical
exam,andareatriskoflimblossorevendeath.Thefocusofthisthesisisonthe
mostcommonsubset:uncomplicated,non-purulentSSTIs.
2.2Incidence&BurdenofDiseaseSSTIsareacommonconditiondiagnosedandmanagedinEDsandcarrysignificant
financialburdenonhealthcaresystemsglobally.From1997to2005,thenumberof
AmericansseekingmedicalcareforSSTIsincreasedby50%,with14.2millionvisits
in2005alone.5PatientswithSSTIsaccountforupto3%ofallEDvisitsintheUnited
States,translatingto3.4millionvisits.6,7AlthoughCanadiandataarelacking,a
singleVancouverEDdiagnosed2234patientswithaSSTIbetweenJanuary2003
andSeptember2004,representing2%ofallEDvisits.8A2011reportbythe
CanadianInstituteforHealthInformationfoundthatcellulitiswasthe5thand7th
mostcommonreasonforanEDvisitinthe45to64andgreaterthan65yearsage
groups,respectively.9

8
Figure1.Classificationofskinandsofttissueinfections(SSTIs)
SSTIsareresponsibleforasignificanthealthcaresystemburdenduetohospital
admissionandsubsequentcosts.SSTIsmanagedintheEDresultina13.9–15.2%
hospitaladmissionrate,withthemostcommoncitedreasonbeingtheneedfor
intravenousantibiotics.10,11HospitalizationforcomplicatedSSTIs,termedacute
bacterialskinandskinstructureinfections12,resultinanaveragecostof$8023with
ameanhospitallengthofstayof4.9days.13Onestudyfoundthatfrom2005to
2011,therateofadmissionforABSSIincreasedby17%,accountingfor2%ofall
hospitaladmissionsintheUnitedStates.14
2.3Etiology&RiskFactorsGroupAstreptococcus(Streptococcuspyogenes),β-hemolyticgroupB,CandG
streptococci,andStaphylococcusaureusarethemostcommonoffendingbacteria.
Typically,aportalofentrythatdisruptstheprotectivecutaneousbarrier

9
predisposesapatienttodevelopinganSSTI.Examplesincludeskintrauma,surgical
incisions,injectiondruguse,andulcerformation.Additionalriskfactorsfornon-
purulentSSTIsinclude:lymphedema,venousinsufficiency,obesity,priorhistoryof
cellulitisandtineapedis.Ofnote,case-controlstudiesfailedtofindanyassociation
observedwithdiabetesmellitus,alcoholorsmoking.15,16Inaminorityofcases,the
sourceofinfectionmaybehematogenousseedingoridiopathic.
2.4ClinicalFeatures&ComplicationsPatientstypicallypresentwithpain,redness,swellingandindurationoftheaffected
skin.Patientswithcellulitishaveirregular,patchybordersofaffectedreddened
skin.Conversely,thebordersarewelldemarcated,raisedandpalpableinpatients
witherysipelas.Insomecases,theremaybelymphangitis(erythematousstreaking
alongtheaffectedextremityalongthedistributionofthebloodvessels)or
lymphadenopathy(painfulswellingoflymphnodes).Aminorityofpatientsmay
alsoexhibitsystemicsignssuchasfeverortachycardia.Iftreatedwithappropriate
antimicrobialtherapy,uncomplicatednon-purulentSSTIsshouldresolvewithinfive
tosevendays.Patientsmayexperiencemildpainandrednessforseveraldays
beyondthistimeframeastheresidualinflammationsubsides.
Somepatientsmaysuffercomplicationssuchassepsisorbloodstreaminfections
(bacteremia)thatwarranthospitaladmission.Onoccasion,apparentnon-purulent
infectionsdevelopintowalled-offabscessesthatrequiresurgicalincisionand
drainage.Ifnotpromptlytreated,cellulitisinvolvingapreexistingulcermay

10
progresstoinfectunderlyingbone(osteomyelitis),whichoftenrequiresseveral
weeksofantimicrobialtherapy.Seriousadverseeventssuchaslimbamputationor
deatharerare.
2.5DiagnosisWoundculturesarenotpossiblefornon-purulentSSTIs.Asystematicreviewfound
therateofbacteremiasecondarytocellulitisorerysipelasrangedfromlessthan1%
to7.9%.17Bloodculturesaretypicallylowyieldandrarelychangemanagement.
Thus,adjuncttestsareunhelpfulandthediagnosisofSSTIsremainsaclinicalone.
However,diagnosisofuncomplicatednon-purulentSSTIsremainschallenging.A
recentlargecross-sectionalstudyfounda30.5%misdiagnosisrateoflower
extremitycellulitis(termed‘pseudocellulitis’).Thestudyauthorsestimatedthis
misdiagnosisratewouldresultin50,000to130,000unnecessaryhospitalizations
and$195to$515millionUSdollarsinexcesshealthcarespending.18Thedifficulty
intheaccuratediagnosisofSSTIsisduetoseveralmimics,suchas:stasisdermatitis;
lymphedema;gout;deepveinthrombosis;andcutaneousdrugeruption.
2.6CurrentGuidelinesOwingtoalackofhighqualityevidence,empirictreatmentguidelinesbasedon
expertopinionhavebeenpublishedtoaidclinicians.4,19-21Therearecurrentlyno
CanadianguidelinesforthemanagementofSSTIs.Despitetheincreasingburdenof
thiscommonpresentation,currentevidenceislackingregardingtheoptimal

11
managementofSSTIs.ArecentCochranereviewconcludedthattheoptimal
antimicrobialtherapyforSSTIsremainsunclear,asnotworandomizedcontrolled
trials,amongthe25identifiedstudies,comparedthesametwoantibiotic
regimens.21Recentstudieshaveshownpromisefornovelonce-weeklyparenteral
lipoglycopeptideantibioticsforthetreatmentofSSTIs,whichmaybeespecially
usefulincommunitiesthatlacktheresourcestoimplementoutpatientparenteral
antibiotictherapy(OPAT).Thesehavethepotentialtodecreasethehealthcare
systemburden,lowercomplicationratesfromrepeatintravenousdoses,and
provideaddedconvenienceforpatients.22,23
PracticeguidelinespublishedbytheInfectiousDiseaseSocietyofAmerica(IDSA)
arebasedonexpertconsensus,againhighlightingthelackofpublisheddatato
determineanoptimalmanagementstrategy.4IntheUnitedKingdom,theEron
classificationsystemwasdevelopedbyanexpertpanelandhasbeenincorporated
intotheClinicalResourceEfficiencySupportTeam(CREST)guidelines.19,24An
alternativeDundeeclassificationwasdevelopedbasedonretrospectivedata,and
hasbeenshowntoreducethenumberofpatientstreatedbyparenteralantibiotics
by70%incomparisontotheEronclassification.25,26However,theDundee
classificationschemehasnotbeenincorporatedintoanyconsensusguidelines.
Ithasbeenpostulatedthatonlyasparseinoculumofbacterialpathogencauses
SSTIs,andthattheassociatedsignificantinflammatoryresponseisresponsiblefor
thephysicalfindingsofpain,rednessandindurationthatpatientsexperience.27

12
Basedonthisrationale,Hepburnandcolleaguesreportedthatashorter5-day
courseofantibioticswasequallyefficaciousasalonger10-daycourse.28Current
guidelinesrecommendthatuncomplicatednon-purulentSSTIsshouldbetreated
withanti-streptococcalantibioticsforadurationof5days.4
2.7OralversusIntravenousTherapySelectingtheoptimalrouteofantimicrobialtherapyisakeydecisionpointinthe
managementofSSTIsforemergencyphysicians.Oralantibiotictherapyholds
severaladvantagesovertheparenteralroute,includinglowerriskofcomplications,
decreasedcost,andincreasedpatientconvenienceandcomfort.29,30Oraltherapyis
generallypreferred,inparticularforinfectionsinotherwisewellappearing
immunocompetenthostswithoutsignsofsystemicillness,suchasfeverand
vomiting.
Patientswhoreceiveintravenouslinesareatriskofbothlocalandsystemic
intravenouscatheter-relatedinfections,suchasbacteremia.Thereisalsoariskof
thrombophlebitis–apainfulinflammationoftheveinduetoathrombus.
Intravenousformulationsaremorecostlythantheiroralcounterparts.Thereisalso
theadditionalcostofmedicalsupplies(intravenouslines,tubing,needles,etc.)and
trainedhealthcarepersonneltoadministerthemedication.InareaswhereanOPAT
serviceisnotavailable,thereisalsoasignificantcostincurredduetohospital
admission.Intravenoustherapycarriestheaddedinconvenienceofalackof

13
mobilityforpatientsandariskofhavingtoreturntotheEDduetocomplications
suchasablockedordislodgedperipheralintravenousline.
Theonlyabsoluteindicationsforintravenoustherapyare:1)aninabilitytoswallow
pillsorabsorbthemedicationfromthegastrointestinaltract;and2)theoral
medicationachievespoorconcentrationsinthecirculation(poorbioavailability).
TheformerindicationisuncommonintheEDforpatientswithSSTIs.Furthermore,
mostoralantibioticsusedtotreatSSTIshavegoodtoexcellentbioavailability.30,31
Therearecurrentlynostudiesthathaveexaminedwhyemergencyphysiciansselect
intravenousantibiotictherapy.
Onlytwostudieshavecomparedoralversusintravenoustherapywithinthesame
antibioticclassforthetreatmentofSSTIs.Jorupandcolleaguesconductedasmall
quasi-randomizedtrialcomparingoralversusintravenouspenicillinforerysipelas,
andfoundnobenefitwithintravenoustherapy.32Theoutcomesassessedinthis
studywerefeverduration,hospitallengthofstay,andsickleave.Amorerecent
smallrandomizedtrialbyAboltinsandcolleaguesfoundoralcephalexinwasnon-
inferiortointravenouscefazolinfortheprimaryoutcomeofdaysuntilno
advancementintheareaofcellulitis.33Unfortunately,neithertrialwaspoweredto
detectadifferenceintreatmentfailure,whichisanoutcomethatismoreclinically
importantandimpactful.Todate,therearenopublishedstudiesthathave
demonstratedabenefitofintravenousantibioticsoveroraltherapyforthe
managementofnon-purulentSSTIs.ItstandstoreasonthatifSSTIscanbe

14
adequatelytreatedwithoraltherapy,thenthisisclearlymorepreferable,giventhe
increasedcostandrisksassociatedwithintravenoustherapy.
2.8EDTreatmentSeveraltreatmentpathwaysexistforEDpatientsdiagnosedwithSSTIs(Figure2).
Theemergencyphysicianmustdecideonthemostappropriaterouteofantibiotic
therapy.Themajorityofpatientsaretreatedasoutpatientswithoralantibiotics.If
patientsareeithersystemicallyillorarefelttohavefailedoraltherapy,thenthe
intravenousrouteisselected.Forpatientsinwhichintravenoustherapyischosen,
patientsareeitheradmittedtohospitalormayreceivetheirtreatmentinthe
community,whichisalsoreferredtoasoutpatientparenteralantibiotictherapy
(OPAT).
2.8.1OralAntibioticTherapyThemajorityofpatientsdiagnosedwithnon-purulentSSTIsintheEDaretreatedas
outpatientswithoralantibiotics.Currentguidelinesrecommenda5-daycourseof
oralantibiotictherapy.4Despitethis,surveyedCanadianemergencyphysicians
indicatedthattheymorecommonlyprescribea7or10-daycourseoforal
antibiotics.34Patientsaretypicallyaskedtofollowupwiththeirfamilyphysicianin
48to72hoursforareassessment,butareinstructedtoreturntotheEDif
symptomsworsen(spreadingerythemaorsignsofsystemicillness).Some
emergencyphysiciansmarkthebordersoferythemawithapen,tohelppatients
determineiftheerythemaisspreadingwelloutsideofitsinitialborders.

15
Figure2.EDTreatmentPathwaysforPatientswithSSTIs
2.8.2Parenteral(Intravenous)AntibioticTherapyIntravenousantibioticsarechosenifpatientsaresystemicallyill,haveasevere
clinicalpresentationbasedonthephysician’simpression,orareunabletotolerate
oraltherapy.Thesepatientsareeithertreatedinthehospitalordischargedhometo
receiveOPAT(Figure2).

16
2.8.2.1InpatientParenteralAntibioticTherapyInpatientcaremaybewarrantedforseveralreasons.First,theremaybeconcerns
aboutapatient’sabilitytobecompliantwithoutpatienttherapy.Thismayinclude
socialissuessuchashomelessness,aninabilitytotravel,psychiatricillness,and
injectiondruguse.Second,theclinicianmaydecidethattheinfectionissevere
enoughtorequirecloserobservationandmanagementasaninpatient.Third,the
patientmayalreadyhavecomplicationssuchassepsisand/orunstablevitalsigns
(e.g.hypotension,tachycardia).Fourth,aminorityofpatientsmaybeworsening
clinically,despitealreadyreceivingintravenousantibioticsinthecommunity,and
aredeemedtohavefailedOPAT.
2.8.2.2OutpatientParenteralAntibioticTherapy(OPAT)TherearethreemethodsofintravenousantibioticdeliveryusingtheOPATmodel:
1)intheED;2)viaatrainednurseorself-administrationinthepatient’shome;or
3)viaatrainednurseatanambulatoryclinic.Firstreportedin1974,OPATis
generallydefinedastheadministrationofatleasttwodosesofparenteral
antimicrobialsondifferentdayswithoutinterimhospitalization.35OPATismost
commonlyusedtotreatSSTIs,butmayalsobeutilizedforavarietyofother
infections,including:urinarytractinfections,osteomyelitis,centralnervoussystem
infectionsandendocarditis.36,37ThefollowingdiscussionaboutOPATisinreference
toSSTIsonly.
AppropriatepatientselectioniscriticaltothesuccessofanOPATprogram.
Followingdiagnosis,theemergencyphysicianmustdecidethatthepatientrequires

17
parenteralratherthanoralantibiotictherapy.Therearecurrentlynopublisheddata
regardinghowemergencyphysiciansdecidethatparenteraltherapyisrequiredfor
patientswithSSTIs.Moreover,therearenoevidence-basedguidelinestohelp
cliniciansdecideonwhentheparenteralrouteisappropriate.Inadditiontothe
infectionitself,severalotherfactorsmayplayaroleinphysiciandecision-making,
suchas:comorbidities,triagevitalsignsandsignsofsystemicillness.Socialfactors
mustalsobeconsidered.Forexample,homelesspatientsorthosewithoutameans
oftravelmaybepoorcandidatesforOPAT.ManyOPATprogramsexclude
intravenousdrugusersduetosafetyconcerns,andonlyonesmallobservational
studysuggestsOPATinthispatientpopulationmaybesafeandeffective.38Finally,
useofOPATmustbeacceptabletothepatientandcaregivers.
Followingpatientselection,theemergencyphysicianmustselecttheoptimal
antimicrobialagent.Antibioticswithlonghalf-lives,suchasceftriaxone,maybe
attractivechoicesduetolessfrequentdosingthatwouldbemoreconvenientfor
patients.However,unnecessarilybroad-spectrumantibioticscarrytheriskof
selectingforantimicrobialresistanceduetoalterationsinthegutflorawith
subsequentovergrowthofresistantbacteria.Whensurveyed,76.5%ofCanadian
emergencyphysicianspreferredcefazolinasthefirstchoiceparenteralantibioticfor
SSTIs.34VancomycinorotherantimicrobialswithactivityagainstCA-MRSAshould
beconsideredinpatientswithapurulentSSTIandriskfactors,suchashepatitisCor
substanceabuse.39

18
Patientsareusuallydischargedwithaperipheralintravenouscatheterinplacefor
furtherantimicrobialdoses.Aperipherallyinsertedcentralcatheter(PICC),whichis
amorepermanentintravenouscatheterthatcangenerallyremaininplaceforthe
durationoftreatment,maybeplacedatalaterdateifitisdeterminedthat
prolongedtherapyisrequired.Thefinalstepistodeterminetheappropriatefollow-
upforpatientsreceivingOPAT.Dependingonlocallyavailableresources,patients
canreceivefollow-upwithemergencyphysicianintheED,withafamily
practitioner,orinahospitalclinicsettingwithaninfectiousdiseasespecialist.
2.8.2.2.1ReturntotheEDIncommunitiesthatdonothaveresourcestoadministerintravenousantibiotics
outsideofthehospital,patientsareaskedtoreturntotheEDforsubsequentdoses.
Anemergencyphysicianusuallyperformsaclinicalreassessmentwithin24to72
hourstodetermineiftheinfectionisrespondingtotherapy.Patientswithagood
responsearesteppeddowntooraltherapy,whereasthosewithlittleresponsebut
nosignsofsystemicillnessandnoworseningmaybecontinuedwithintravenous
therapy.ThesepatientswouldbescheduledforanotherEDreassessmentatalater
date.Patientswhoseinfectionsareclinicallyworseningdespiteparenteraltherapy
areadmittedtohospital.
Thisapproachisclearlycumbersomeforpatients,particularlyforthosewhodonot
haveanappropriatemeanstotraveltoandfromaclinicorhospital.Furthermore,
reassessmentatalaterdateisrarelywiththesameemergencyphysician,which

19
makesitdifficulttoprovideanobjectiveclinicalassessmentregardingresponseto
therapy.AnotherapproachinvolvestheuseofEDobservationunitstomonitor
patientswithSSTIsintheEDforupto24hoursbeforemakingafinaldecisionto
admittohospitalormanageasanoutpatient,resultinginhighadmissionrates
rangingfrom29.2to38%.40,41ItisgenerallyacceptedthatSSTIstakeatleast48to
72hoursbeforeimprovementmaybenoted.Itisthereforeunlikelythatashortstay
inanobservationunitwouldimpactthedecisiontoadmitordischargeapatientand
wouldinsteadaddtoEDcrowding.
2.8.2.2.2CommunityCareAccessCentre(CCAC)&FamilyPhysicianFollow-UpInOntario,Canada,theprovisionofhealthcareinthecommunityorathomeis
managedbyLocalHealthIntegrationNetworks(LHINs).TheLHINofaspecific
regionoverseestheCommunityCareAccessCentre(CCAC),whichprovidesnursing
servicesforwoundcareandadministrationofparenteralantibiotics.Apharmacist
isalsoinvolvedinmedicationreview.InOntario,CCACservicesareanintegralpart
oftheOPATmodel.Mostpatientsvisitaclinictoreceiveintravenousdosesbya
trainednurse.Asmallersubsetofpatients(usuallyolderpatientswhocannot
travel)receivesintravenousdoseswithintheirownhome.Incommunitieswith
CCACservicesbutwithouttimelyaccesstoinfectiousdiseasespecialists,patients
areadvisedtoseekaclinicalreassessmentfromtheirfamilyphysician.

20
2.8.2.2.3CCAC&ReturntoaHospitalClinicManyurbanhospitalshavesetupclinicsrunbyinfectiousdiseasespecialiststo
followandmanagepatientsbeingtreatedinthecommunitywithintravenous
antibiotics.Forexample,patientsatTheOttawaHospitalwhoaretreatedwithOPAT
receivefollow-upandreassessmentwithaninfectiousdiseasespecialistatthe
OPATClinic.Thismodelprovidesseveraltheoreticaladvantages:1)decreased
hospitaladmissions;2)increasedpatientconvenience;and3)decreasedEDvisits
forantimicrobialtherapyandreassessments.Whilethisintuitivelyappearstobethe
idealapproach,nopublisheddatacurrentlyexistregardingtheefficacyofOPATin
thecommunitysetting.42
2.8.2.2.4OPATAdverseOutcomesAdministrationofOPATforSSTIsisnotwithoutrisk.Thereisthepotentialof
progressionofinfectiondespiteOPAT,line-relatedcomplicationsoradversedrug
reactionsthatmaywarrantsubsequenthospitaladmission.Petraketal.43
recommendedthatstudiesabouttheefficacyofOPATshouldincorporaterobust
definitionsfortreatmentfailure.
ThereportedhospitaladmissionratefollowingOPATtreatmentfailurerangesfrom
2.6%to8%.43-45However,thesestudiesexaminedavarietyofinfectiousdiseases,
makingitdifficulttodeterminetheclinicalfailurerateforSSTIsinparticular.A
retrospectivestudyreportedareadmissionrateof5.5%forcellulitis,althoughthe
reasonsforhospitalizationwerenotdescribed.46Thereisalackofstudies
concerningnon-purulentSSTIsusingrobustdefinitionsforOPATtreatmentfailure.

21
2.9QuestionsSurroundingOptimalEDManagementofSSTIsBeforedeterminingtheoptimaloutpatientmanagementstrategyforEDpatients
withSSTIs,therearethreekeyquestionsthatarise:
1) Whatisthedefinitionof(i)oralantibiotictreatmentfailureand(ii)OPAT
treatmentfailure?
2) Aretherepredictorsoftreatmentfailurewithoralantibiotics?Inother
words,whichpatientsrequireparenteraltherapy?
3) Whenconsideringtheoptimalrouteoftherapy,whatistheEDphysician’s
rationalewhenselectingparenteraltherapy?
2.10TreatmentFailure
2.10.1TreatmentFailureasanOutcomeintheEDSettingIn2013,theUSCenterforDrugEvaluationandResearch(CDER)releasedguidelines
tohelpresearchersstandardizefutureclinicaltrialsforSSTIs.TheCDERdefines
clinicalresponseasareductioninlesionsizegreaterorequalto20%comparedto
baseline,evaluated48to72hoursaftertherapyisinitiated.12Basedonthis
definitionoftreatment‘improvement’,onecaninferthattreatmentfailurewould
thenbedefinedasareductioninlesionsizelessthan20%at48to72hours.
ThisdefinitionoftreatmentfailureisproblematicintheEDsetting.First,the
majorityofEDphysicianswillonlyseepatientswithSSTIsduringasingle
encounter.Second,manypatientsareprescribedoralantibioticsforSSTIsinthe

22
clinicsettingandthenpresenttotheED.Theemergencyphysicianisleftwiththe
dilemmaofwhethertheircurrentpresentationtrulyreflectsatreatmentfailure.The
emergencyphysicianalsooftendoesnothaveanyobjectivedata(photographsor
medicalrecords)toreasonablyestimatethelesionsizeandseveritywhenoral
antibioticswereinitiated.
AnumberofstudiesintheEDsettinghavereportedtreatmentfailureasan
outcome.Murrayandcolleaguesdefinedtreatmentfailureasanyofthefollowing:
specialistconsultation,hospitaladmission,surgicalprocedure(e.g.incisionand
drainage),an‘upgrade’fromoraltoparenteraltherapy,orachangeinclassof
intravenousantibioticsduetolackofclinicalresponse.47Thisdefinitionwasbased
onexpertopinionandtheauthors’ownobservationoftreatmentpatternsintheir
EmergencyDepartment.A2011EDstudyofpediatricpatientsthatdefined
treatmentfailureusedasimilardefinition,onceagainbasedonexpertopinion.48
Petersonandcoworkersdefinedtreatmentfailureassubsequenthospitalization,a
changeinclassofantibiotic,oraswitchfromoraltoparenteraltherapy.49Patients
requiringsubsequentincisionanddrainagewereexcludedfromthisdefinition.
Ofnote,theauthorsreportingtreatmentfailureasanoutcomeinthe
aforementionedstudiesdidnotspecifyatimeframeatwhichclinicalassessmentfor
treatmentfailureshouldbeundertaken.Thisisclinicallyimportantasassessinga
patienttoosoonaftertheinitiationofantibiotictherapymayresultinan
inappropriatediagnosisoftreatmentfailure.Additionally,itisnotablethattheseED

23
studiesdidnotincorporateachangeinlesionsizeintotheirdefinitionsoftreatment
failure,asthisisimpracticalintheEDsetting.Arecentsystematicreviewidentified
19randomizedcontrolledtrialswithreportedtreatmentfailureratesforcellulitis
rangingfrom6to37%.50Theauthorsspeculatedthatthishighdegreeofvariability
mightbeduetodifficultywithdiagnosisandconfusionwithcellulitismimics.In
addition,variabilityintreatmentfailureratesislikelyalsorelatedtothelackofa
uniformdefinitionfortreatmentfailure.
2.10.2TreatmentFailureDefinitionThereiscurrentlynovalidateddefinitionoftreatmentfailurefollowingantibiotic
therapyforSSTIs.Duetotheuniquenatureofthepatientpopulationandcare
deliveredintheED,itisimportanttouseadefinitiontailoredtothissetting.Usinga
specificpercentageinreductionoflesionsizeisimpracticalforthefollowing
reasons:1)physiciansmaynotdocumentdimensionsoftheinfection;2)manyED
(electronicmedical)recordsdonotallowforphotographstobeuploaded;and3)
patientsmaybealreadyonoralantibiotictherapyinitiatedbyafamilyphysician
anddonotpresentwithdocumentationoflesionsizeatonsetoftherapy.Instead,it
ismorepragmatictouseclinicaljudgmentwhendeterminingtreatmentfailure.It
wouldbeappropriatetoconcludeatreatmentfailurehasoccurredifthepatient
reportssignificantspreadofinfection,therearesystemicsignsofillness(e.g.fever,
tachycardia)oriftheclinicianfeelstheinfectionisseveredespiteanappropriate
durationoftherapy.

24
TheUnitedStatesFoodandDrugAdministrationrecommendsthatclinicalresponse
totreatmentshouldbeassessedat48to72hoursfrominitiatingtherapy.51When
surveyed,amajorityofCanadianemergencyphysiciansselected48hoursasthe
optimaltimeframefordeterminingiftreatmentfailurehadoccurredfollowing
initiationofantibiotictherapy.34Afterreviewoftheliterature40,47-49,52-54and
discussionwithlocalexpertsinemergencymedicineandinfectiousdisease,the
followingtwodefinitionsoftreatmentfailurefornon-purulentSSTIswere
developed:
A. OralAntibioticTreatmentFailure
Oralantibiotictreatmentfailureisdefinedasanyofthefollowingoutcomesthat
occurswithin14daysoftheinitialEDvisitandafteraminimumof48hoursoforal
antibiotictherapy:(i)subsequenthospitaladmissionforanSSTI;(ii)achangein
classoforalantibioticowingtoprogressionofinfectionandnotduetointolerance
orallergy;or(iii)achangeinantibioticroutefromoraltointravenoustherapy.
B. OPATTreatmentFailure
OPATtreatmentfailureisdefinedassubsequenthospitaladmissionaftera
minimumof48hoursofOPATforanyofthefollowing:(i)infectionprogression;(ii)
line-relatedcomplications(e.g.bacteremia,thrombophlebitis,venous
thromboembolism);or(iii)drug-relatedcomplications(e.g.Clostridiumdifficile
colitis).
Adverseeventssuchasoperativedebridement,amputationordeathwerefelttobe
unhelpfulcomponentsoftheaforementioneddefinitionsbecausetheyarerare.

25
2.11PredictorsofTreatmentFailureWithOralAntibioticsIdentifyingpredictorsoffailurewithoralantibioticsisimportantfortworeasons.
First,havingknowledgeofpredictorswithoraltherapywouldhelpemergency
physiciansidentifythesubsetofpatientsthatshouldbestartedonintravenous
therapyattheinitialvisit,limitingtheoveruseofparenteraltherapyand
subsequentlyreducingtheassociatedadverseeventsandcosts.Second,theriskof
sepsisandsubsequenthospitaladmissionsmaybereducedinpatients
inappropriatelystartedonoraltherapy.TherearecurrentlynoEDstudiesreporting
riskfactorsforfailurewithoralantibiotics.Anunderstandingoftheseriskfactors
wouldbecriticaltowarddevelopingevidence-basedcriteriaforpatientsthat
requireintravenoustherapy.
AsystematicreviewofSSTIsmanagedintheEDobservationunitreportedthat
fever,leukocytosisandknownMRSAexposurewerethemostcommonlyreported
riskfactorsfortreatmentfailure.55Petersonandcoworkersidentifiedfiverisk
factorsindependentlyassociatedwithtreatmentfailureforcellulitis:fever,chronic
legulcers,chronicedemaorlymphedema,priorcellulitisinthesamearea,and
cellulitisatawoundsite.49However,thesestudiesdidnotdiscriminatebetween
failureswithoralversusintravenoustherapy.

26
2.12OralVersusTheIntravenousRoute:EmergencyPhysicianRationaleforSelectingIntravenousTherapyTheidealantimicrobialagentinthetreatmentofnon-purulentSSTIswouldpossess
thefollowingcharacteristics:(i)optimalpharmacokineticpropertiesagainstthe
causativeorganism;(ii)minimaladverseeffects;(iii)inexpensive;and(iv)
acceptabletopatientsandhealthcareproviders.Oralantibioticsarepreferredto
intravenousantibioticsinthattheyposefewerrisksofadverseevents,arecheaper,
andarelessinvasivetopatients.Themainpointofcontentionliesintheabilityof
theantimicrobialagenttoachieveadequateconcentrationsinbloodandtissue,for
anadequatedurationtoarrestbacterialgrowth.Therefore,anoralagentwouldbe
clearlypreferableifitcanachievehightissueandserumconcentrationsthatare
comparabletotheirparenteralcounterparts.Forexample,oralcephalexinachieves
excellent(90to100%)bioavailability31andisanexcellentchoicetotreatnon-
purulentSSTIs.
YetED-basedstudieshaveshownthatintravenousantibioticsaremorecommonly
administered47,49andthatantibioticoveruseiscommon.56Mayandcoworkers
reportedthatwhile87%ofsurveyedattendingemergencyphysiciansfeltthat
antibioticswereoverusedintheED,only10%believedtheythemselves
overprescribedantibiotics.57Oneplausibleexplanationisthatpatientspresentingto
theEDmayhavemoresevereinfections.Otherpossibleexplanationsincludea
perceptionthatparenteraltherapyissuperior,aconsiderationofsignificant
comorbidities,orconcernsaboutcompliancewithoralmedications.

27
Surprisingly,thereisscantliteratureaddressingemergencyphysiciandecision-
makingregardingantibioticprescribing57,andtherearenopublishedstudies
describingphysicianrationaleforselectingintravenousantibioticsforinfections.
Identifyingthefactorsphysiciansconsiderwhenoptingforparenteraltherapy
wouldbehighlyusefulforcarryingoutclinicaltrialstotesttheseperceived
indications.
3.RationalePatientscommonlyseekEDcarefornon-purulentSSTIs,whichrequireextensive
healthcareresourcesforbothinpatient(hospitalresources)andoutpatient(CCAC;
physicianfollowup)management.Identifyingpredictorsoftreatmentfailurewith
oralantibioticswouldallowemergencyphysicianstomoreappropriatelyselect
patientsthatrequireintravenoustherapy.Thismayalsohelpreducethenumberof
patientsinappropriatelytreatedwithmorecostlyparenteraltherapythatcarries
theaddedriskofadverseevents.Furthermore,determiningthereasonsbehind
selectingparenteraltherapyisacriticalfirststepinunderstandingemergency
physiciandecision-makingforthemanagementofSSTIs.Finally,despitebeingthe
mostcommonindicationforOPAT,treatmentfailureintheOPATsettinghasnot
beendescribedforSSTIsinparticular.Thus,itisimportanttodescribetheoverall
performanceandsafetyofOPATtherapyforSSTIsintheCanadiansetting.
AccuratediagnosisandappropriatetreatmentofSSTIsarecriticalforpatientsafety
anddecreasinghealthcarecostsandoverallburden.TheepidemiologyofSSTIshas

28
beenwelldocumentedintwodistinctpopulations:hospitalizedpatientsandthose
whovisitphysicians’offices.58-60However,therearenostudiesthathavedescribed
theepidemiologyofadultswithSSTIswhoareseenandmanagedintheEDsetting.
AsamajorityofEDadultpatientsaretreatedasoutpatients,thisconstitutesa
significantevidencegap.Athoroughunderstandingoftheepidemiologyofnon-
purulentSSTIsseenintheEDisanimportantbasisfordevelopingmoreappropriate
evidence-basedrecommendationsforoptimalmanagementofthiscommon
condition.

29
References1. StevensDL,EronLL.Cellulitisandsoft-tissueinfections.AnnInternMed.
2009;150(1):ITC11.
2. WallinTR,HernHG,FrazeeBW.Community-associatedmethicillin-resistantStaphylococcusaureus.EmergMedClinNorthAm.2008;26(2):431-455,ix.
3. QuallsML,MooneyMM,CamargoCA,Jr.,ZucconiT,HooperDC,PallinDJ.Emergencydepartmentvisitratesforabscessversusotherskininfectionsduringtheemergenceofcommunity-associatedmethicillin-resistantStaphylococcusaureus,1997-2007.ClinInfectDis.2012;55(1):103-105.doi:110.1093/cid/cis1342.Epub2012Mar1028.
4. StevensDL,BisnoAL,ChambersHF,etal.Practiceguidelinesforthediagnosisandmanagementofskinandsofttissueinfections:2014updatebytheInfectiousDiseasesSocietyofAmerica.ClinInfectDis.2014;59(2):e10-52.doi:10.1093/cid/ciu1444.
5. HershAL,ChambersHF,MaselliJH,GonzalesR.Nationaltrendsinambulatoryvisitsandantibioticprescribingforskinandsoft-tissueinfections.ArchInternMed.2008;168(14):1585-1591.
6. PallinDJ,EganDJ,PelletierAJ,EspinolaJA,HooperDC,CamargoCA,Jr.IncreasedUSemergencydepartmentvisitsforskinandsofttissueinfections,andchangesinantibioticchoices,duringtheemergenceofcommunity-associatedmethicillin-resistantStaphylococcusaureus.AnnEmergMed.2008;51(3):291-298.doi:210.1016/j.annemergmed.2007.1012.1004.Epub2008Jan1028.
7. PallinDJ,CamargoCA,Jr.,SchuurJD.Skininfectionsandantibioticstewardship:analysisofemergencydepartmentprescribingpractices,2007-2010.WestJEmergMed.2014;15(3):282-289.doi:210.5811/westjem.2013.5818.18040.Epub12014Jan18046.
8. StenstromR,GrafsteinE,RomneyM,etal.Prevalenceofandriskfactorsformethicillin-resistantStaphylococcusaureusskinandsofttissueinfectioninaCanadianemergencydepartment.[ErratumappearsinCJEM.2009Nov;11(6):570].CJEM,Can.2009;11(5):430-438.
9. InformationCIfH.ASnapshotofHealthCareinCanadaasDemonstratedbyTop10Lists.2011;https://secure.cihi.ca/free_products/Top10ReportEN-Web.pdf.AccessedSeptember25,2017.

30
10. VenkateshAK,DaiY,RossJS,SchuurJD,CappR,KrumholzHM.VariationinUShospitalemergencydepartmentadmissionratesbyclinicalcondition.MedCare.2015;53(3):237-244.doi:210.1097/MLR.0000000000000261.
11. TalanDA,SalhiBA,MoranGJ,etal.Factorsassociatedwithdecisiontohospitalizeemergencydepartmentpatientswithskinandsofttissueinfection.WestJEmergMed.2015;16(1):89-97.
12. FDAGuidelineABSSSI2013.2013.
13. PollackCV,Jr.,AminA,FordWT,Jr.,etal.Acutebacterialskinandskinstructureinfections(ABSSSI):practiceguidelinesformanagementandcaretransitionsintheemergencydepartmentandhospital.JEmergMed.2015;48(4):508-519.
14. KayeKS,PatelDA,StephensJM,KhachatryanA,PatelA,JohnsonK.RisingUnitedStatesHospitalAdmissionsforAcuteBacterialSkinandSkinStructureInfections:RecentTrendsandEconomicImpact.PLoSOne.2015;10(11):e0143276.doi:0143210.0141371/journal.pone.0143276.eCollection0142015.
15. BjornsdottirS,GottfredssonM,ThorisdottirAS,etal.Riskfactorsforacutecellulitisofthelowerlimb:aprospectivecase-controlstudy.ClinInfectDis.2005;41(10):1416-1422.Epub2005Oct1413.
16. DupuyA,BenchikhiH,RoujeauJC,etal.Riskfactorsforerysipelasoftheleg(cellulitis):case-controlstudy.BMJ.1999;318(7198):1591-1594.
17. GundersonCG,MartinelloRA.Asystematicreviewofbacteremiasincellulitisanderysipelas.JInfect.2012;64(2):148-155.doi:110.1016/j.jinf.2011.1011.1004.Epub2011Nov1011.
18. WengQY,RaffAB,CohenJM,etal.CostsandConsequencesAssociatedWithMisdiagnosedLowerExtremityCellulitis.JAMADermatol.2016.
19. ClinicalResourceEfficiencySupportTeam(2005)Guidelinesonthemanagementofcellulitisinadults.CREST,Belfast..
20. ConsensusDocumentontheManagementofCellulitisinLymphoedema.BritishLymphologySociety.2016.
21. KwakYG,ChoiSH,KimT,etal.ClinicalGuidelinesfortheAntibioticTreatmentforCommunity-AcquiredSkinandSoftTissueInfection.InfectChemother.2017;49(4):301-325.doi:310.3947/ic.2017.3949.3944.3301.

31
22. KilburnSA,FeatherstoneP,HigginsB,BrindleR.Interventionsforcellulitisanderysipelas.CochraneDatabaseSystRev.2010(6):CD004299.doi:004210.001002/14651858.CD14004299.pub14651852.
23. CoreyGR,KablerH,MehraP,etal.Single-doseoritavancininthetreatmentofacutebacterialskininfections.NEnglJMed.2014;370(23):2180-2190.doi:2110.1056/NEJMoa1310422.
24. BoucherHW,WilcoxM,TalbotGH,PuttaguntaS,DasAF,DunneMW.Once-weeklydalbavancinversusdailyconventionaltherapyforskininfection.NEnglJMed.2014;370(23):2169-2179.doi:2110.1056/NEJMoa1310480.
25. EronLJ,LipskyBA,LowDE,NathwaniD,TiceAD,VolturoGA.Managingskinandsofttissueinfections:expertpanelrecommendationsonkeydecisionpoints.JAntimicrobChemother.2003;52(Suppl1):i3-17.
26. MarwickC,BroomhallJ,McCowanC,etal.Severityassessmentofskinandsofttissueinfections:cohortstudyofmanagementandoutcomesforhospitalizedpatients.JAntimicrobChemother.2011;66(2):387-397.doi:310.1093/jac/dkq1362.Epub2010Oct1095.
27. PhoenixG,DasS,JoshiM.Diagnosisandmanagementofcellulitis.BMJ.2012;345:e4955.(doi):10.1136/bmj.e4955.
28. SachsMK.Cutaneouscellulitis.ArchDermatol.1991;127(4):493-496.
29. HepburnMJ,DooleyDP,SkidmorePJ,EllisMW,StarnesWF,HasewinkleWC.Comparisonofshort-course(5days)andstandard(10days)treatmentforuncomplicatedcellulitis.ArchInternMed.2004;164(15):1669-1674.
30. LiHK,AgweyuA,EnglishM,BejonP.Anunsupportedpreferenceforintravenousantibiotics.PLoSMed.2015;12(5):e1001825.doi:1001810.1001371/journal.pmed.1001825.eCollection1002015May.
31. CyriacJM,JamesE.Switchoverfromintravenoustooraltherapy:Aconciseoverview.JPharmacolPharmacother.2014;5(2):83-87.doi:10.4103/0976-4500X.130042.
32. MacGregorRR,GrazianiAL.Oraladministrationofantibiotics:arationalalternativetotheparenteralroute.ClinInfectDis.1997;24(3):457-467.
33. Jorup-RonstromC,BrittonS,GavlevikA,GunnarssonK,RedmanAC.Thecourse,costsandcomplicationsoforalversusintravenouspenicillintherapyoferysipelas.Infection.1984;12(6):390-394.
34. AboltinsCA,HutchinsonAF,SinnappuRN,etal.Oralversusparenteralantimicrobialsforthetreatmentofcellulitis:arandomizednon-inferiority

32
trial.JAntimicrobChemother.2015;70(2):581-586.doi:510.1093/jac/dku1397.Epub2014Oct1021.
35. YadavK,GatienM,Corrales-MedinaV,StiellI.Antimicrobialtreatmentdecisionfornon-purulentskinandsofttissueinfectionsintheemergencydepartment.CJEM.2017;19(3):175-180.doi:110.1017/cem.2016.1347.Epub2016Aug1017.
36. TiceAD,RehmSJ,DalovisioJR,etal.Practiceguidelinesforoutpatientparenteralantimicrobialtherapy.IDSAguidelines.ClinInfectDis.2004;38(12):1651-1672.Epub2004May1626.
37. SeatonRA,BarrDA.Outpatientparenteralantibiotictherapy:principlesandpractice.EurJInternMed.2013;24(7):617-623.doi:610.1016/j.ejim.2013.1003.1014.Epub2013Apr1018.
38. GardiolC,VoumardR,CochetC,deValliereS.Settingupanoutpatientparenteralantimicrobialtherapy(OPAT)unitinSwitzerland:reviewofthefirst18monthsofactivity.EurJClinMicrobiolInfectDis.2016;35(5):839-845.doi:810.1007/s10096-10016-12606-z.Epub12016Feb10017.
39. HoJ,ArchuletaS,SulaimanZ,FisherD.Safeandsuccessfultreatmentofintravenousdruguserswithaperipherallyinsertedcentralcatheterinanoutpatientparenteralantibiotictreatmentservice.JAntimicrobChemother.2010;65(12):2641-2644.doi:2610.1093/jac/dkq2355.Epub2010Sep2623.
40. VayalumkalJV,SuhKN,ToyeB,RamotarK,SaginurR,RothVR.Skinandsofttissueinfectionscausedbymethicillin-resistantStaphylococcusaureus(MRSA):anafflictionoftheunderclass.CJEM.2012;14(6):335-343.
41. VolzKA,CanhamL,KaplanE,SanchezLD,ShapiroNI,GrossmanSA.IdentifyingpatientswithcellulitiswhoarelikelytorequireinpatientadmissionafterastayinanEDobservationunit.AmJEmergMed.2013;31(2):360-364.
42. MayL,MullinsP,PinesJ.DemographicandtreatmentpatternsforinfectionsinambulatorysettingsintheUnitedStates,2006-2010.AcadEmergMed.2014;21(1):17-24.
43. ChapmanAL.Outpatientparenteralantimicrobialtherapy.BMJ.2013;346:f1585.(doi):10.1136/bmj.f1585.
44. PetrakRM,SkorodinNC,FliegelmanRM,HinesDW,ChundiVV,HartingBP.ValueandClinicalImpactofanInfectiousDisease-SupervisedOutpatientParenteralAntibioticTherapyProgram.OpenForumInfectDis.2016;3(4):ofw193.eCollection2016Oct.

33
45. ChapmanAL,DixonS,AndrewsD,LilliePJ,BazazR,PatchettJD.Clinicalefficacyandcost-effectivenessofoutpatientparenteralantibiotictherapy(OPAT):aUKperspective.JAntimicrobChemother.2009;64(6):1316-1324.doi:1310.1093/jac/dkp1343.Epub2009Sep1319.
46. Hoffman-TerryML,FraimowHS,FoxTR,SwiftBG,WolfJE.Adverseeffectsofoutpatientparenteralantibiotictherapy.AmJMed.1999;106(1):44-49.
47. ZhangJ,MooreE,BousfieldR.OPATforcellulitis:itsbenefitsandthefactorsthatpredisposetolongertreatment.EurJClinMicrobiolInfectDis.2016;35(6):1013-1015.doi:1010.1007/s10096-10016-12631-y.Epub12016Apr10015.
48. MurrayH,StiellI,WellsG.Treatmentfailureinemergencydepartmentpatientswithcellulitis.CJEM.2005;7(4):228-234.
49. MistryRD,ScottHF,ZaoutisTE,AlpernER.Emergencydepartmenttreatmentfailuresforskininfectionsintheeraofcommunity-acquiredmethicillin-resistantStaphylococcusaureus.PediatrEmergCare.2011;27(1):21-26.doi:10.1097/PEC.1090b1013e318203ca318201c.
50. PetersonD,McLeodS,WoolfreyK,McRaeA.Predictorsoffailureofempiricoutpatientantibiotictherapyinemergencydepartmentpatientswithuncomplicatedcellulitis.AcadEmergMed.2014;21(5):526-531.
51. ObaitanI,DwyerR,LipworthAD,etal.Failureofantibioticsincellulitistrials:asystematicreviewandmeta-analysis.AmJEmergMed.2016;34(8):1645-1652.doi:1610.1016/j.ajem.2016.1605.1064.Epub2016May1626.
52. AdminstrationFaD.GuidanceforIndustry:AcuteBacterialSkinandSkinStructureInfections:DevelopingDrugsforTreatment.
53. AminAN,CerceoEA,DeitelzweigSB,PileJC,RosenbergDJ,ShermanBM.Hospitalistperspectiveonthetreatmentofskinandsofttissueinfections.MayoClinProc.2014;89(10):1436-1451.doi:1410.1016/j.mayocp.2014.1404.1018.Epub2014Jun1425.
54. JenkinsTC,KnepperBC,McCollisterBD,etal.Failureofoutpatientantibioticsamongpatientshospitalizedforacutebacterialskininfections:Whatistheclinicalrelevance?AmJEmergMed.2016;34(6):957-962.doi:910.1016/j.ajem.2016.1002.1013.Epub2016Feb1012.
55. PallinDJ,BinderWD,AllenMB,etal.Clinicaltrial:comparativeeffectivenessofcephalexinplustrimethoprim-sulfamethoxazoleversuscephalexinalonefortreatmentofuncomplicatedcellulitis:arandomizedcontrolledtrial.ClinInfectDis.2013;56(12):1754-1762.doi:1710.1093/cid/cit1122.Epub2013Mar1751.

34
56. AbetzJW,AdamsNG,MitraB.Skinandsofttissueinfectionmanagementfailureintheemergencydepartmentobservationunit:asystematicreview.EmergMedJ.2016:2016-205950.
57. MayL,HarterK,YadavK,etal.Practicepatternsandmanagementstrategiesforpurulentskinandsoft-tissueinfectionsinanurbanacademicED.AmJEmergMed.2012;30(2):302-310.doi:310.1016/j.ajem.2010.1011.1033.Epub2011Jan1028.
58. MayL,GudgerG,ArmstrongP,etal.Multisiteexplorationofclinicaldecisionmakingforantibioticusebyemergencymedicineprovidersusingquantitativeandqualitativemethods.InfectControlHospEpidemiol.2014;35(9):1114-1125.doi:1110.1086/677637.Epub672014Jul677623.
59. Perello-AlzamoraMR,Santos-DuranJC,Sanchez-BarbaM,CanuetoJ,MarcosM,UnamunoP.Clinicalandepidemiologicalcharacteristicsofadultpatientshospitalizedforerysipelasandcellulitis.EurJClinMicrobiolInfectDis.2012;31(9):2147-2152.
60. ZervosMJ,FreemanK,VoL,etal.Epidemiologyandoutcomesofcomplicatedskinandsofttissueinfectionsinhospitalizedpatients.JClinMicrobiol.2012;50(2):238-245.
61. PallinDJ,EspinolaJA,LeungDY,HooperDC,CamargoCA,Jr.EpidemiologyofdermatitisandskininfectionsinUnitedStatesphysicians'offices,1993-2005.ClinInfectDis.2009;49(6):901-907.doi:910.1086/605434.

35
ChapterThree:PredictorsofOralAntibioticFailureforNon-PurulentSkinandSoftTissueInfectionsintheEmergencyDepartment
ChapterOverviewThefollowingisamanuscriptpreparedforpublicationbasedonahealthrecords
review.Theobjectivesofthishealthrecordsreviewwere:1)todescribethe
epidemiologyofadultpatientswithnon-purulentskinandsofttissueinfectionswho
presenttotheemergencydepartment;and2)toidentifyriskfactorsassociatedwith
oralantibiotictreatmentfailure.
InAppendixAacopyoftheapprovalletterfromtheOttawaHealthScience
NetworkResearchEthicsBoardisprovided.
InAppendixBadetaileddescriptionisprovidedofthemethodsusedtodevelopa
multivariablelogisticregressionmodelforpredictorsoforalantibiotictreatment
failure.
Dr.KrishanYadavisthefirstauthorofthismanuscriptandwasresponsibleforthe
studydevelopment,datacollection,monitoringofdataabstraction,statistical
analysisandwritingofthemanuscript.Thismanuscriptwasco-authoredbyDr.Ian
Stiell,Dr.KathrynSuhandDr.GeorgeWells.JordanBernickprovidedvaluableinput
regardingdataanalysis.Dr.DebraEaglesandDr.Venkatesh
Thiruganasambandamoorthyprovidedvaluablefeedbackthroughouttheprocess.
Mr.JohnMacisaacandMr.DarmynRitchiewereinvolvedwithdataabstraction.

36
PredictorsofOralAntibioticFailureforNon-PurulentSkinandSoftTissue
InfectionsintheEmergencyDepartment
KrishanYadav1,KathrynSuh2,DebraEagles3,JohnMacIsaac4,DarmynRitchie4,
JordanBernick5,VenkateshThiruganasambandamoorthy3,GeorgeWells5,6,IanG
Stiell3
1DepartmentofEmergencyMedicine,UniversityofOttawa
2DepartmentofMedicine,DivisionofInfectiousDiseases,UniversityofOttawa
3DepartmentofEmergencyMedicine,TheOttawaHospitalResearchInstitute,
UniversityofOttawa
4DepartmentofUndergraduateMedicine,UniversityofOttawa
5CardiovascularResearchMethodsCentre,UniversityofOttawaHeartInstitute
6DepartmentofEpidemiologyandCommunityMedicine,UniversityofOttawa
Correspondenceto:KrishanYadav
Email:[email protected]
Date:January30,2018
WordCount:3248
Acknowledgments:Theauthorswouldliketothankthefollowingindividualsfor
theirassistanceinthisstudy:My-LinhTran,SherylDomingo,AngelaMarcantonio
andCatherineClement.ThisstudywasfundedbyagrantfromtheDepartmentof
EmergencyMedicine,UniversityofOttawa,Ontario,Canada.

37
Abstract
Introduction
Currentguidelinerecommendationsforoptimalmanagementofnon-purulentskin
andsofttissueinfections(SSTIs)arebasedonexpertconsensus,ratherthanon
evidence.Thereiscurrentlyalackofevidencetoguideemergencyphysicianson
whentoselectoralversusintravenousantibiotictherapy.
Methods
Weperformedahealthrecordsreviewofadults(age≥18years)withnon-purulent
SSTIstreatedattwotertiarycareemergencydepartments(EDs).Patientswere
excludediftheyhadapurulentinfectionorinfectedulcerswithoutsurrounding
cellulitis.Multivariablelogisticregressionwasusedtoidentifypredictors
independentlyassociatedwithoralantibiotictreatmentfailureafteraminimumof
48hoursoforaltherapy.
Results
Weenrolled500patients(meanage64years,279male(55.8%)and126(25.2%)
withdiabetes).Thehospitaladmissionratewas29.6%.Of288patientswhohad
receivedaminimumof48hoursoforalantibiotics,therewere85oralantibiotic
treatmentfailures(29.5%).Tachypneaattriage(oddsratio[OR]=6.31;95%CI
1.80,22.08),chroniculcers(OR=4.90;95%CI1.68,14.27),historyofMRSA
colonizationorinfection(OR=4.83,95%;CI1.51,15.44),andcellulitisinthepast

38
12months(OR=2.23,95%CI=1.01,4.96)wereindependentlyassociatedwithoral
antibiotictreatmentfailure.
Conclusion
Thisisthefirststudytoevaluatepotentialpredictorsoforalantibiotictreatment
failurefornon-purulentSSTIsintheED.Weobservedahighhospitaladmissionrate
andpracticevariabilityregardingantimicrobialagentandroute.Tachypneaat
triage,chroniculcers,historyofMRSAcolonizationorinfectionandcellulitiswithin
thepastyearwereindependentlyassociatedwithoralantibiotictreatmentfailure.
Emergencyphysiciansshouldconsidertheseriskfactorswhendecidingonoral
versusintravenousantimicrobialtherapyfornon-purulentSSTIsbeingmanagedas
outpatients.

39
IntroductionUncomplicated,non-purulentskinandsofttissueinfections(SSTIs)describe
bacterialinfectionsofthesuperficialepidermisanddermis(erysipelas)ordeeper
dermisandsubcutaneoustissue(cellulitis)inwhichpatientsexperienceredness,
painandindurationoftheinvolvedskin.Non-purulentandpurulentSSTIsarea
commonclinicalproblem,accountingforupto3%ofallemergencydepartment
(ED)visitsintheUnitedStates,translatingto3.4millionvisits.1,2AlthoughCanadian
dataarelacking,asingleVancouverEDdiagnosed2234patientswithaSSTI,
representing2%ofallEDvisits.3Oncethediagnosisofanon-purulentSSTIismade,
theemergencyphysicianmustselecttheappropriateantibioticagent,dose,
durationandroute(oralorintravenous).
Duetoalackofhighqualityevidence,empirictreatmentguidelinesarebasedon
expertopinion.4-6Selectingtheappropriateantibioticrouteforoutpatient
managementisakeydecisionpoint.Oraltherapyholdsseveraladvantagesoverthe
parenteralroute,including:lowerriskofcomplications,decreasedcost,increased
patientconvenienceandcomfort.7-9Intravenoustherapymaybeselectedifapatient
hasfailedoraltherapy,issystemicallyunwellorhasasevereinfectionbasedonthe
clinician’simpression.Themainadvantageoftheintravenousrouteisoptimizing
bioavailability,whichisespeciallyusefulinpatientswithswallowingdifficultyora
gastrointestinalmalabsorptionsyndrome.Theintravenousrouteiscostlier,less
convenientforpatientsandhasanaddedriskofadverseevents.Therearecurrently
nostudiesthathaveaimedtoidentifypredictorsassociatedwithtreatmentfailure

40
withoralantibiotictherapy.Identificationofsuchpredictorswouldallow
emergencyphysicianstobetterselectpatientsthatrequireintravenousantibiotics.
Thismayalsohelpreducethenumberofpatientsinappropriatelytreatedwith
parenteraltherapy.
Theprimaryobjectiveofthisstudywastoidentifyriskfactorsassociatedwithoral
antibiotictreatmentfailurefornon-purulentSSTIs.Asecondaryobjectivewasto
describetheepidemiologyofadultswithnon-purulentSSTIspresentingtotheED.
Methods
StudyDesignandSettingWeperformedahealthrecordsreviewofconsecutiveadultpatientspresentingto
theEDwithdiagnosisandmanagementofanon-purulentSSTI.Thestudy
populationwasenrolledfromtheOttawaHospitalCivicandGeneralEDs,bothbeing
tertiarycareadultEDswithacombined170,000patientvisitsannually.TheOttawa
HealthScienceNetworkResearchEthicsBoardapprovedtheprotocolwithoutthe
needforinformedconsent.
PopulationWeenrolledaconsecutivesampleofpatientsmeetingeligibilitycriteriathat
presentedtotheEDoveraseven-monthperiod(January1toJuly31,2016).Eligible
patientswereadults(age≥18years)presentingtotheEDanddiagnosedwitha
non-purulentSSTIthatwastreatedwitheitheroralorintravenousantibiotics.
Patientswereconsideredeligibleiftheywerealreadytakingantibioticsattheindex
EDvisit.Weexcludedpatientsforthefollowingreasons:(i)patientspresentingfora

41
follow-upvisit(i.e.nottheindexEDvisitforthisclinicalproblem);(ii)age<18
years;(iii)adiagnosisofapurulentskinabscesswhereanincisionanddrainage
procedurewasperformed;(iv)infectedulcerswithoutsurroundingcellulitisor
erysipelas;or(v)necrotizinginfections.
StudyProtocolandDataAbstractionInordertominimizebias,wetookspecificstepswithrespecttocaseselection,
abstractortraining,definitionofvariables,useofastandardizedcaserecordform,
regularmeetingsandoversightofabstractorsinaccordancewithaccepted
methodologyforchartreviews.10-13WeidentifiedeligiblecasesbyInternational
ClassificationofDiseases,10threvision,Canada(ICD-10-CA)diagnosiscodesofL03*
(cellulitis,unspecified)andA46(erysipelas).Relevantpatientdatawereobtained
fromtheelectronichealthrecord(physicianandnursingnotes,outpatient
parenteralantibiotictherapy(OPAT)clinicrecords).
Theprincipalinvestigator(KY)trainedtwomedicalstudents(JM,DR)ontheuseof
theelectronichealthrecordssystem.Allvariablesandtheprimaryoutcomeof
interestwereexplicitlydefined(seesupplementaryappendix)apriori.Weuseda
standardizedcaserecordform(seesupplementaryappendix)toabstractdata.The
caserecordformwaspilotedtoremoveambiguousitemsandensurethedata
collectioninstrumentwasrobust.Thedataabstractorsheldregularmonthly
meetingstoresolveanydisagreementsbyconsensus.Theprincipalinvestigator
monitoredtheperformanceofthedataabstractorsbyreviewing25%ofthesample.

42
Cohen’skappastatisticwasusedtoassessinterobserveragreementforincluded
subjectsandtheprimaryoutcome.
OutcomeMeasuresTheprimaryoutcomewastreatmentfailurewithoralantibiotics.Thereiscurrently
novalidateddefinitionoftreatmentfailureintheliterature.TheUnitedStatesFood
andDrugAdministrationrecommendsthatclinicalresponsetotreatmentshouldbe
assessedat48to72hoursfrominitiatingtherapy.14Whensurveyed,amajorityof
Canadianemergencyphysiciansselected48hoursastheoptimaltimeframefor
determiningiftreatmentfailurehadoccurredfollowinginitiationofantibiotic
therapy.15Afterreviewoftheliterature16-22anddiscussionwithlocalexpertsin
emergencymedicineandinfectiousdisease,wedevisedatreatmentfailure
definition.Treatmentfailurewithoralantibioticswasdefinedasanyofthe
followingoutcomesoccurringafteraminimumof48hoursoforalantibioticsandat
nolaterthan14daysfromtheindexEDvisit:(i)subsequenthospitaladmissionfor
aSSTI;(ii)achangeinclassoforalantibioticowingtoprogressionofinfectionand
notduetointoleranceorallergy;or(iii)achangeinantibioticroutefromoralto
intravenoustherapyowingtoprogressionofinfectionandnotduetointoleranceor
allergy.
Asecondaryoutcomeofinterestwastreatmentfailurewithintravenousantibiotics.
Thiswasdefinedasanyofthefollowingoutcomesafteraminimumof48hoursof
intravenousantibioticsandatnolaterthan14daysfromtheindexEDvisit:(i)

43
subsequenthospitaladmissionforaSSTI;or(ii)achangeinclassofintravenous
antibioticowingtoprogressionofinfectionandnotduetointoleranceorallergy.
Thefollowingbaselinedemographicsandclinicaldatawereabstracted:patientage
andgender;comorbidities;EDtriagevitalsigns;andinfectioncharacteristics.We
anticipatedthataccurateinfectiondimensions(lengthandwidth)mightnotbe
consistentlyrecordedonpatientcharts.Inordertoestimatethepercentbody
surfaceareaofaffectedskin,themodifiedLund-Browderchartwasused.23,24ED
treatmentvariableswereabstractedasfollows:antibiotictreatmentapproach;and
settingforsubsequentintravenousantibiotics(ifchosen).Adverseoutcomes
includedantibioticeventsandintravenouscatheter-relatedevents.
StatisticalAnalysisTheprevalenceofnon-purulentSSTIsintheEDpopulation,theproportionof
patientswhoreceivedoralversusintravenoustherapy,andthepatientswhohada
treatmentfailurewerecalculated.Continuousdataarepresentedasmeanswith
standarddeviationsormedianswithaninterquartilerange(IQR,Q1–Q3)for
normallyandnon-normallydistributeddata,respectively.Categoricaldataare
presentedasproportionswith95%confidenceintervals.
Weemployedunivariateanalysestoexamineallclinicalvariableshypothesizedto
beriskfactorsfortreatmentfailurewithoralantibiotictherapy(seesupplementary
appendix).Variableswithp-valuesof0.10orlesswereconsideredformultivariable
analysis.Abackwardsselectionprocedurewasusedtoobtainamultivariable

44
logisticregressionmodeltodetermineclinicalpredictorsindependentlyassociated
withtheprimaryoutcomeoftreatmentfailurewithoralantibiotics.TheHosmer-
Lemeshowstatisticwasusedtoassessmodelfit.SAS(version9.4,SASInstitute,
CaryNC)wasusedfordescriptivestatistics,univariateandmultivariablelogistic
regressionanalysis.
SampleSizeandFeasibilityPreviousstudieshavesuggestedthataminimumof10eventspervariableis
requiredtoavoidbiasedestimateswhendevelopingmultivariableprediction
models.25-27Weestimatedthatnomorethanfivepredictorvariableswouldbe
includedinamodeltopredicttreatmentfailurewithoralantibiotics.Basedonthe
10eventspervariableworkingrule,aminimumof50treatmentfailureswouldbe
requiredtodeveloparobustmodel.Treatmentfailureratesreportedinthe
literaturerangefrom6to37%.28PreviouslypublishedstudiesinCanadianEDshave
indicatedthattheapproximatetreatmentfailurerateofSSTIswithantibiotics
rangesfrom18.7to20.5%.16,17Assumingaconservativeestimateofan18%
treatmentfailurerate,270patientswouldberequiredtoobtainaminimumof50
oralantibiotictreatmentfailures.Weestimatedthatupto40%ofpatientsmightbe
treatedwithintravenoustherapy.Therefore,wedeterminedanoverallsamplesize
of500patientswouldensurethatwesurpassedtheminimumrequirednumberof
patientstreatedwithoralantibiotics.FromJanuary1,2014untilDecember31,
2014,therewere2286uniquevisitstoeithertheCivicorGeneralcampusofThe
OttawaHospitalwithanICD-10diagnosisofcellulitisorerysipelas.Evenafter

45
accountingforpurulentSSTIs,ahealthrecordsreviewofpatientswithnon-purulent
SSTIsoversevenmonthswouldyieldwellovertheminimumrequiredsamplesize.
ResultsOvertheseven-monthstudyperiod,666caseswerescreenedforeligibilityand500
patientsmettheinclusioncriteria(Figure1).Thekappastatisticforincludedcases
betweentheprimaryinvestigator(KY)andeachabstractor(JMandDR)was0.96
(95%CI0.93,0.99)and0.91(95%CI0.86,0.97),respectively.Thekappastatistic
fortheprimaryoutcomeoforalantibiotictreatmentfailurewas0.94(95%CI0.90,
0.98).Ofthe500enrolledpatients,126(25.2%)haddiabetesand87(17.4%)hada
historyofcellulitisintheprior12months(Table1).Themostcommonlocationof
infectionwastheleg(54.2%)andmostinfections(80.2%)wereestimatedtobe
<5%totalbodysurfacearea(Table2).
Ofthetotalcohort,354patients(70.8%)receivedanintravenousantibioticinthe
ED,with148patients(29.6%)admittedtohospitalforfurtherparenteraltherapy.
Themostcommonoralagentusedwascephalexinandthemostcommonparenteral
agentwascefazolin(Table3).Ofpatientsreceivingintravenousantibiotics,20.6%
receivedtwoormoreantibiotics.
Ofthe352patientsthatweremanagedasoutpatients,themajority(61.4%)
receivedsolelyoralantibioticprescriptions(Table4).Asignificantproportionof

46
outpatients(19.9%)receivedanintravenousantibioticdoseintheEDbutwere
dischargedwithanoralantibioticprescription.Ofthe222patientsreceivingoral
antibioticprescriptions,cephalexinwasmostcommonlyselected(77.4%).Ofthe
136patientswhowereprescribedoutpatientintravenousantibiotics,99patients
(72.8%)werereferredtotheOPATclinicforassessmentandfollowupwithan
infectiousdiseasespecialist.Aminoritywasaskedtofollowupwiththeirprimary
careproviderorreturntotheEDforfollowup.Cefazolin(68.4%)wasthemost
commonlyprescribedintravenousantibiotic.
Asignificantnumberofoutpatients(40.6%)returnedtotheEDwithin14days
(Table5).Themajorityofpatientsreturnedforscheduledrepeatintravenous
antibiotics,becauseofadelayinarrangingintravenousantibioticsintheoutpatient
setting.Asmallproportionofunscheduledvisits(5.4%)wasforaworsening
infectionthatrequiredhospitaladmission.Therewerefewadverseeventsfor
outpatients:2.8%withadislodgedorblockedperipheralintravenousline;1.7%of
withgastrointestinalsymptomsand0.6%ofwitharashattributedtotheprescribed
antibiotic.
Forthe99patientsreferredtotheOPATclinic,85.8%ofpatientsattendedtheir
appointment(Table6).Emergencyphysiciansdiagnosedcellulitiswithahigh
degreeofaccuracy(96.5%),withonlythreepatientshavinganalternatediagnosis
assignedbytheinfectiousdiseasephysicians.Themediantimetofollowupforthe

47
firstOPATclinicvisitwas4daysandtherewasamedianof2clinicvisits.Patients
receivedamediandurationof7daysofintravenousantibiotics.
Of288patientswhoweretreatedwithatleast48hoursoforalantibiotics,85
patients(29.5%)sufferedanoralantibiotictreatmentfailure(Table7).Treatment
failuresweremanagedasfollows:51patients(60.0%)wereswitchedtooutpatient
intravenousantibiotics;30patients(35.3%)werehospitalizedforintravenous
therapy;and4patients(4.7%)wereswitchedtoadifferentclassoforalantibiotic.
Of212patientstreatedwithatleast48hoursofintravenousantibiotics,12patients
(5.7%)sufferedanintravenousantibiotictreatmentfailure(seethesupplementary
appendix).
Predictorsassociatedwithoralantibiotictreatmentfailureusingmultivariable
logisticregressionareshowninTable8.Tachypneaattriage(oddsratio[OR]=
6.31;95%CI1.80,22.08),chroniculcers(OR=4.90;95%CI1.68,14.27),historyof
MRSAcolonizationorinfection(OR=4.83;95%CI1.51,15.44),andcellulitisinthe
past12months(OR=2.23;95%CI1.01,4.96)werefoundtobeindependently
associatedwithoralantibiotictreatmentfailure.TheHosmer-Lemeshowchi-square
testyieldedap-valueof0.604(χ2=1.853,degreesoffreedom=3)andtheC-
statisticwas0.709.Thisindicatesthatourmodelhasgoodfit.

48
Discussion
InterpretationofResultsThisstudydescribesadultpatientspresentingtotheEDfornon-purulentSSTIs.A
substantialproportionofpatientswasadmittedtohospitalforfurthermanagement.
Weobservedsignificantpracticevariationwithrespecttoselectionofantimicrobial
routeandagent.AnumberofpatientsreceivedasingleintravenousdoseintheED
followedbyoutpatientoraltherapy,despitealackofevidencetosupportthis
approach.Thevariabilityintreatmentapproachreinforcesthelackofagreement
amongstemergencyphysiciansontheoptimalapproachtotherapyforthiscommon
clinicalcondition.
Wefoundanoralantibiotictreatmentfailurerateof29.5%,whichwashigherthan
expected.Murrayetal.16reportedanoralantibiotictreatmentfailurerateof6.8%,
butthiswasasmallsamplesize(2of29patients).Petersonetal.17reportedanoral
antibiotictreatmentfailurerateof21.0%.Asneitherstudyusedastricttimecutoff
intheirdefinitionoftreatmentfailure,somepatientsmayhavebeenclassifiedasan
oralantibiotictreatmentfailureprematurely.Weidentifiedpotentialriskfactorsfor
failurewithoralantibiotics.Tachypneaattriage,chroniculcers,historyofMRSA
colonizationorinfectionandcellulitiswithinthepastyearwereindependently
associatedwithoralantibiotictreatmentfailure.Theseriskfactorsmaybe
consideredaspotentialindicationsforintravenoustherapy.Thehightreatment
failureandhospitaladmissionratesareofconcern.Thesefindingsmayinpart
reflectthelackofevidencetoguideemergencyphysiciansontheoptimalrouteof
antimicrobialtherapy.

49
PreviousStudiesThemostrecentInfectiousDiseaseSocietyofAmericaguidelinessuggest
intravenousantibioticsfor‘moderate’(signsofsystemicillness)or‘severe’(failed
oraltherapy,signsofsystemicillness,clinicalsignsofdeeperinfection,or
immunocompromised)infections.4TheBritishClinicalResourceEfficiencySupport
Team(CREST)guidelinesrecommendoraltherapyin‘ClassI’patients,definedas
havingnosignsofsystemictoxicityandno‘uncontrolled’comorbidities,whichwas
notexplicitlydefined.5Duetoalackofevidence,theseguidelinesarebasedon
expertopinion.AstudybyPetersonetal.identifiedpredictorsoffailurewith
outpatientantibioticsforcellulitis,butdidnotdistinguishbetweenoralversus
intravenousroutes.17ArecentsurveyofCanadianemergencyphysiciansrevealed
that94.4%ofrespondentswouldconsideraclinicaldecisionruletopredictoral
antibiotictreatmentfailure.15Todate,evidenceregardingtheoptimalrouteof
antimicrobialtherapyfornon-purulentSSTIsislacking.
StrengthsThisisthefirststudytoidentifypotentialpredictorsassociatedwithoralantibiotic
treatmentfailurefornon-purulentSSTIs.Therewasexcellentagreementbetween
dataabstractorsforbothinclusionofstudiesandtheprimaryoutcome.Thestudy
findingsmaybetterguideemergencyphysicianstodeterminewhenoralantibiotic
treatmentfailureislikely–andwhentoselectintravenoustherapyattheonsetof
treatment.
LimitationsThishealthrecordsreviewhasseveralpotentiallimitations.First,potentially
clinicallyimportantvariables(infectionsizeandobesity)mayhavebeeninaccurate

50
ornotdocumented.Obtainingaccuratemeasuresofinfectionsizewasnotpossible
asitwasseldomdocumentedinthemedicalrecord.Weinsteadattemptedto
estimateinfectionsizeusingaLund-Browderburnchartasasurrogatefortotal
bodysurfaceareaofaffectedskin.Obesitywasnotconsistentlydocumentedinthe
medicalchartandwasnotvalidated(e.g.bycalculatingthebodymassindex).We
attemptedtomitigatethisbyreviewingallelectronichealthrecordsinthe6months
priortoandaftertheindexvisittoidentifyifthiscomorbiditywasdocumented.
Second,thedataabstractorswerenotblindedtothestudyoutcome.Thisisunlikely
tohaveresultedinsignificantbiasastheprimaryoutcomewasstrictlydefined
usinga48-hourcutoffforconsiderationoftreatmentfailure.Inaddition,therewas
excellentinter-observeragreementfortheprimaryoutcome.Weattemptedto
minimizebiasbytrainingabstractors,holdingregularmeetings,validating25%of
charts,definingvariablesapriori,andusingastandardizedcaserecordformin
accordancewithacceptedmethodologyforchartreviews.10-13
Third,thereisnovalidateddefinitionoforalantibiotictreatmentfailure.Following
areviewoftheliterature14-22,29wedevelopedacompositeendpointdefinitionafter
discussionandconsensusamonglocalexpertsinemergencymedicineand
infectiousdisease.Disadvantagesofusingacompositeendpointincludemisleading
resultsifonecomponentoftheoutcomeheavilydrivestheresult,especiallyifitis
theleastpatient-importantoutcome.However,95.3%ofthetreatmentfailureswere

51
drivenbythetwomostpatientcentredoutcomes:hostpitaladmissionfor
intravenoustherapyorswitchfromoraltointravenousoutpatienttherapy.
Fourth,therewasasmallamountofmissingdata(<2.5%),whichwasassumedtobe
missingcompletelyatrandom.Wehandledthemissingdatausingacompletecase
analysis.Lastly,wewereunabletomeasureadherencetotreatmentduetothe
natureofthestudydesign.
ClinicalImplicationsOurfindingsrevealimportantclinicalimplications,havingdemonstratedsignificant
practicevariabilitywithrespecttoselectionofantimicrobialagentandroute.
PatientswhoreceivedOPAThadamediandurationofantibiotictherapythatwas
longerthantheguideline-recommendedfivedays.4Patientsrequiringintravenous
therapyhavemorecomplicatedinfections,whichmayexplainwhytheyrequireda
longerdurationoftherapy.Thisvariationintreatmentapproachcoupledwitha
highhospitaladmissionrateislikelyduetoalackofevidence-based
recommendationsforoptimaltherapy.Severalriskfactorsassociatedwithoral
antibiotictreatmentfailurewereidentified.Webelievethatsuchfactorsshouldbe
consideredwhendecidingontheoptimalrouteoftherapy.Ultimately,ourfindings
highlightthatfurtherstudiesarecriticaltoimprovetreatmentofthiscommon
clinicalcondition.

52
ResearchImplicationsFutureresearchshouldinvolveaprospectivestudytofurtherassessthesepotential
riskfactorsfortreatmentfailureidentifiedinourstudyandideallyderiveaclinical
decisionruletoguideemergencyphysiciansontheoptimalrouteofantimicrobial
therapy.Furthermore,studiesexaminingrationaleforselectingintravenoustherapy
wouldprovidebetterinsightregardingphysiciandecision-making.
ConclusionsThisisthefirststudytoevaluatepotentialpredictorsoforalantibiotictreatment
failurefornon-purulentSSTIsintheED.Weobservedahighhospitaladmissionrate
andpracticevariabilityregardingantimicrobialagentandroute.Tachypneaat
triage,chroniculcers,historyofMRSAcolonizationorinfectionandcellulitiswithin
thepastyearwereindependentlyassociatedwithoralantibiotictreatmentfailure.
Emergencyphysiciansshouldconsidertheseriskfactorswhendecidingonoral
versusintravenousantimicrobialtherapyforpatientswithnon-purulentSSTIs.

53
References1. PallinDJ,EganDJ,PelletierAJ,EspinolaJA,HooperDC,CamargoCA,Jr.
IncreasedUSemergencydepartmentvisitsforskinandsofttissueinfections,andchangesinantibioticchoices,duringtheemergenceofcommunity-associatedmethicillin-resistantStaphylococcusaureus.AnnEmergMed.2008;51(3):291-298.doi:210.1016/j.annemergmed.2007.1012.1004.Epub2008Jan1028.
2. PallinDJ,CamargoCA,Jr.,SchuurJD.Skininfectionsandantibioticstewardship:analysisofemergencydepartmentprescribingpractices,2007-2010.WestJEmergMed.2014;15(3):282-289.doi:210.5811/westjem.2013.5818.18040.Epub12014Jan18046.
3. StenstromR,GrafsteinE,RomneyM,etal.Prevalenceofandriskfactorsformethicillin-resistantStaphylococcusaureusskinandsofttissueinfectioninaCanadianemergencydepartment.[ErratumappearsinCJEM.2009Nov;11(6):570].CJEM,Can.2009;11(5):430-438.
4. StevensDL,BisnoAL,ChambersHF,etal.Practiceguidelinesforthediagnosisandmanagementofskinandsofttissueinfections:2014updatebytheInfectiousDiseasesSocietyofAmerica.ClinInfectDis.2014;59(2):e10-52.doi:10.1093/cid/ciu1444.
5. ClinicalResourceEfficiencySupportTeam(2005)Guidelinesonthemanagementofcellulitisinadults.CREST,Belfast..
6. ConsensusDocumentontheManagementofCellulitisinLymphoedema.BritishLymphologySociety.2016.
7. LiHK,AgweyuA,EnglishM,BejonP.Anunsupportedpreferenceforintravenousantibiotics.PLoSMed.2015;12(5):e1001825.doi:1001810.1001371/journal.pmed.1001825.eCollection1002015May.
8. MacGregorRR,GrazianiAL.Oraladministrationofantibiotics:arationalalternativetotheparenteralroute.ClinInfectDis.1997;24(3):457-467.
9. CyriacJM,JamesE.Switchoverfromintravenoustooraltherapy:Aconciseoverview.JPharmacolPharmacother.2014;5(2):83-87.doi:10.4103/0976-4500X.130042.
10. GilbertEH,LowensteinSR,Koziol-McLainJ,BartaDC,SteinerJ.Chartreviewsinemergencymedicineresearch:Wherearethemethods?AnnEmergMed.1996;27(3):305-308.

54
11. BadcockD,KellyAM,KerrD,ReadeT.Thequalityofmedicalrecordreviewstudiesintheinternationalemergencymedicineliterature.AnnEmergMed.2005;45(4):444-447.
12. LowensteinSR.Medicalrecordreviewsinemergencymedicine:theblessingandthecurse.AnnEmergMed.2005;45(4):452-455.
13. KajiAH,SchrigerD,GreenS.Lookingthroughtheretrospectoscope:reducingbiasinemergencymedicinechartreviewstudies.AnnEmergMed.2014;64(3):292-298.doi:210.1016/j.annemergmed.2014.1003.1025.Epub2014Apr1018.
14. AdminstrationFaD.GuidanceforIndustry:AcuteBacterialSkinandSkinStructureInfections:DevelopingDrugsforTreatment.
15. YadavK,GatienM,Corrales-MedinaV,StiellI.Antimicrobialtreatmentdecisionfornon-purulentskinandsofttissueinfectionsintheemergencydepartment.CJEM.2017;19(3):175-180.doi:110.1017/cem.2016.1347.Epub2016Aug1017.
16. MurrayH,StiellI,WellsG.Treatmentfailureinemergencydepartmentpatientswithcellulitis.CJEM.2005;7(4):228-234.
17. PetersonD,McLeodS,WoolfreyK,McRaeA.Predictorsoffailureofempiricoutpatientantibiotictherapyinemergencydepartmentpatientswithuncomplicatedcellulitis.AcadEmergMed.2014;21(5):526-531.
18. VolzKA,CanhamL,KaplanE,SanchezLD,ShapiroNI,GrossmanSA.IdentifyingpatientswithcellulitiswhoarelikelytorequireinpatientadmissionafterastayinanEDobservationunit.AmJEmergMed.2013;31(2):360-364.
19. AminAN,CerceoEA,DeitelzweigSB,PileJC,RosenbergDJ,ShermanBM.Hospitalistperspectiveonthetreatmentofskinandsofttissueinfections.MayoClinProc.2014;89(10):1436-1451.doi:1410.1016/j.mayocp.2014.1404.1018.Epub2014Jun1425.
20. MistryRD,ScottHF,ZaoutisTE,AlpernER.Emergencydepartmenttreatmentfailuresforskininfectionsintheeraofcommunity-acquiredmethicillin-resistantStaphylococcusaureus.PediatrEmergCare.2011;27(1):21-26.doi:10.1097/PEC.1090b1013e318203ca318201c.
21. JenkinsTC,KnepperBC,McCollisterBD,etal.Failureofoutpatientantibioticsamongpatientshospitalizedforacutebacterialskininfections:Whatistheclinicalrelevance?AmJEmergMed.2016;34(6):957-962.doi:910.1016/j.ajem.2016.1002.1013.Epub2016Feb1012.

55
22. PallinDJ,BinderWD,AllenMB,etal.Clinicaltrial:comparativeeffectivenessofcephalexinplustrimethoprim-sulfamethoxazoleversuscephalexinalonefortreatmentofuncomplicatedcellulitis:arandomizedcontrolledtrial.ClinInfectDis.2013;56(12):1754-1762.doi:1710.1093/cid/cit1122.Epub2013Mar1751.
23. HettiaratchyS,DziewulskiP.ABCofburns:pathophysiologyandtypesofburns.BMJ.2004;328(7453):1427-1429.
24. WachtelTL,BerryCC,WachtelEE,FrankHA.Theinter-raterreliabilityofestimatingthesizeofburnsfromvariousburnareachartdrawings.Burns.2000;26(2):156-170.
25. ConcatoJ,PeduzziP,HolfordTR,FeinsteinAR.Importanceofeventsperindependentvariableinproportionalhazardsanalysis.I.Background,goals,andgeneralstrategy.JClinEpidemiol.1995;48(12):1495-1501.
26. PeduzziP,ConcatoJ,FeinsteinAR,HolfordTR.Importanceofeventsperindependentvariableinproportionalhazardsregressionanalysis.II.Accuracyandprecisionofregressionestimates.JClinEpidemiol.1995;48(12):1503-1510.
27. PeduzziP,ConcatoJ,KemperE,HolfordTR,FeinsteinAR.Asimulationstudyofthenumberofeventspervariableinlogisticregressionanalysis.JClinEpidemiol.1996;49(12):1373-1379.
28. ObaitanI,DwyerR,LipworthAD,etal.Failureofantibioticsincellulitistrials:asystematicreviewandmeta-analysis.AmJEmergMed.2016;34(8):1645-1652.doi:1610.1016/j.ajem.2016.1605.1064.Epub2016May1626.
29. FDAGuidelineABSSSI2013.2013.

56
FiguresFigure1.FlowDiagramofPatientEligibilityandOutcomes
PatientsScreened
(N=666)
ExcludedPatients,total(N=166)Didnotmeetinclusioncriteria(N=62)
Didnotreceiveantibiotic(N=25)NotdiagnosedwithSSTI(N=37)
Metexclusioncriteria(N=104)
I&Dofabscess(N=40)Follow-upvisit(N=58)Ulcerwithoutcellulitis(N=4)DeclinedConsent(N=2)
EligiblePatients
(N=500)
Home(N=352)(70.4%)
HospitalAdmission(N=148)(29.6%)

57
Tables
Table1.BaselineCharacteristicsofAdultswithNonpurulentSkinandSoftTissueInfectionsseenintheEmergencyDepartment(N=500)
Variable N=500Age(years),mean± SDRange
Male(%)HospitalSite(%)
TOHCivicCampusTOHGeneralCampus
ComorbiditiesDiabetesmellitusCellulitisinpast12monthsCoronaryarterydiseaseCongestiveheartfailureHistoryofMRSAinfectionorcolonizationPeripheralvasculardiseaseLiverdiseaseChronickidneydiseaseActivecancerLymphedemaObesityInjectiondruguseOrgantransplantrecipient
TakingantibioticsatthetimeofEDpresentationOralIV
64±1918–98
279(55.8)
278(55.6)222(44.4)
126(25.2)87(17.4)58(11.6)48(9.6)43(8.6)40(8.0)37(7.4)35(7.0)34(6.8)33(6.6)27(5.4)14(2.8)4(0.8)
85(17.0)13(2.6)
SD=standarddeviation;TOH=TheOttawaHospital;MRSA=methicillinresistantStaphylococcusaureus;ED=emergencydepartment;IV=intravenous

58
Table2.PresentingPatientandInfectionCharacteristics(N=500)
Variable N=500TriageVitalSignsTemperature,°C(mean±SD)HeartRate,beats/min(mean±SD)BloodPressure,mmHg(mean±SD)RespiratoryRate,breaths/min(median,IQR)OxygenSaturation,%(median,IQR)
InfectionLocation(%)LegFootArmHandFaceTorsoGroin
InfectionCharacteristics(%)ChroniclegulcersSurgicalsiteinfectionBiteSizeTBSA<5%TBSA5–10%TBSA>10%
LaboratoryTestsWhitebloodcellcountordered(%)Whitebloodcellcount,×109/L(median,IQR)
36.6±0.987±19136±2418,16–1897,96–98
271(54.2)85(17.0)51(10.2)37(7.4)29(5.8)22(4.4)5(1.0)
56(11.2)30(6.0)12(2.4)
401(80.2)97(19.4)2(0.4)
378(75.6)9.2,7–13
SD=standarddeviation;IQR=interquartilerange;TBSA=totalbodysurfacearea

59
Table3.EmergencyDepartmentTreatment(N=500)
AntibioticSelection Numberofpatients,N=500N(%)
IVantibioticsonlyOralantibioticsonlyOralandIVantibioticsNumberofIVAntibiotics(N=354)OneTwoThree
OralAntibioticsCephalexinClindamycinAmoxicillin-ClavulanateCiprofloxacinTrimethoprim-SulfamethoxazoleDoxycyclineAmoxicillin
IVAntibioticsCefazolinCeftriaxoneVancomycinPiperacillin-TazobactamClindamycinCiprofloxacinMeropenem
339(67.8)146(29.2)15(3.0)
281(79.4)64(18.1)9(2.5)
121(24.2)11(2.2)9(1.8)7(1.4)6(1.2)4(0.8)3(0.6)
202(40.4)80(16.0)59(11.8)46(9.2)40(8.0)3(0.6)3(0.6)
IV=intravenous

60
Table4.AntibioticTreatmentfor352PatientsDischargedfromtheED
OutpatientManagement Numberofpatients,N=352N(%)
PrescribedoralantibioticsPrescribedIVantibioticsPrescribedoralandIVantibioticsOralantibioticinEDandsenthomeonoralantibioticIVantibioticinEDandsenthomeonIVantibiotic*IVantibioticinEDandsenthomeonoralantibioticIntendedlocationforoutpatientIVantibioticsCCACandOPATclinicCCAConlyED
OralantibioticsprescribedCephalexinClindamycinAmoxicillin-ClavulanateTrimethroprim-sulfamethoxazoleCiprofloxacinDoxycyclineAmoxicillin
IVantibioticsprescribedCefazolinCeftriaxoneClindamycinVancomycinMeropenemMultipleIVAntibiotics
216(61.4)130(36.9)6(1.7)
146(41.5)136(38.6)70(19.9)
99(28.1)26(5.6)11(2.2)
222(63.1)172(48.9)19(5.4)13(3.7)7(2.0)5(1.4)5(1.4)1(0.3)
136(38.6)93(26.4)31(8.8)4(1.1)3(0.8)1(0.3)4(1.1)
IV=intravenous,CCAC=communitycareaccesscentre;OPAT=outpatientparenteralantibiotictherapy;ED=emergencydepartment*6patientsweredischargedwithbothintravenousandoralantibiotics

61
Table5.AdverseEventsfor352PatientsDischargedfromtheED
AdverseEvents Numberofpatients,N=352N(%)
ReturntotheEDwithin14DaysReasonforreturnEDvisitRepeatantibioticsForSSTIandnoadmissionUnrelatedmedicalproblemForSSTIandhospitaladmissionDiagnosedwithabscessrequiringI&D
AdversedeviceeventsDislodged/blockedperipheralIVlineOther*
AdverseantibioticeventsNauseaand/orvomitingRashDiarrhea
143(40.6)
60(17.0)39(11.1)21(6.0)19(5.4)4(1.1)
10(2.8)0(0)
4(1.1)2(0.6)2(0.6)
*Other=thrombophlebitis,lineinfectionorbacteremiaED=emergencydepartment;IV=intravenous;SSTI=skinandsofttissueinfection;I&D=incisionanddrainage

62
Table6.OutpatientParenteralAntibioticTherapy(OPAT)ClinicData(N=85)
OPATClinicMetric Numberofpatients,N=85N(%)
Cellulitiswasthecorrectdiagnosis**Alternatediagnoses,totalGoutLymphedemaVenousStasis
Timetofollow-up(days),median,IQRNumberofvisits,median,IQRDurationofIVantibiotics(days),median,IQRDurationofIVandoralantibiotics(days),median,IQR
82(96.5)111
4,3–6
2,1–3
7,7–14
19,14–28
*Atotalof99patientswerereferredtotheOPATclinicfromtheemergencydepartmentOPAT=outpatientparenteralantibiotictherapy;IV=intravenous;IQR=interquartilerange

63
Table7.TreatmentFailurewithOralAntibiotics(N=85of288PatientsTreatedwithaMinimumof48HoursofOralTherapy)
OralAntibioticTreatmentFailures Numberofpatients,N=85N(%)
PatientoutcomesSwitchedtooutpatientIVantibioticsHospitalizedforIVantibioticsSwitchedtooutpatientoralantibioticsofdifferentclass
TreatmentfailureoninitialEDvisit*TreatmentfailureonreturnEDvisitwithin14days
51(60.0)30(35.3)4(4.7)
68(80.0)17(20.0)
*Patientwasalreadyon≥48hoursoforalantibiotictherapyattimeofindexEDvisitIV=intravenous;ED=emergencydepartment

64
Table8.PredictorsAssociatedwithOralAntibioticTreatmentFailureUsingMultivariableLogisticRegression(N=288)
PredictorVariable AdjustedOR 95%CI PValueTachypneaattriage(RR>20)ChroniculcersHistoryofMRSAcolonizationorinfectionCellulitisinthepast12monthsChronickidneydiseaseDiabetesmellitus
6.314.904.832.232.601.70
1.80,22.081.68,14.271.51,15.441.01,4.960.82,8.220.87,3.32
0.0040.0040.0080.050.100.12
TheHosmer-Lemeshowchi-squaretestyieldedap-valueof0.604(χ2=1.853,degreesoffreedom=3).C-statistic=0.709.Thisindicatesnoevidenceofpoorfit.RR=respiratoryrate;MRSA=methicillinresistantStaphylococcusaureus;OR=oddsratio;CI=confidenceinterval

65
SupplementaryAppendixFigureS1.StandardizedCaseRecordForm
CASE#:____________________ AbstractorLastName:____________________DoesthiscasemeetINCLUSIONcriteria?oYes oNo(if‘No’,stophere)
- InclusionCriteria:o Age≥18yearso DiagnosedwithSSTI(cellulitisorerysipelas)o Prescribed/receivedanantibioticforSSTI
DoesthiscasemeetEXCLUSIONcriteria?oYes oNo(if‘Yes’,stophere)- ExclusionCriteria:
o Incisionanddrainageofanabscesso Follow-upvisit(i.e.nottheindexvisitforthisSSTI)o Infectedulcerwithnocellulitis
DemographicsHospital: qTOHCivic qTOHGeneralGender: qMale qFemaleDateofbirth:__________/_____/_____(Y/M/D)DateofindexEDvisit:__________/_____/_____(Y/M/D)PastMedicalHistory(qNoneofbelow)qActiveCancer(onchemotherapyorpalliative)qChronickidneydiseaseqChronicvenousinsufficiencyqCongestiveheartfailureqCoronaryarterydiseaseqCorticosteroids(systemic)qDiabetesqHepaticdiseaseqHIVqIntravenousdruguse(IVDU)qLymphedema/VenousStasisqMRSApositiveqObesityqOrgantransplantrecipientqPeripheralvasculardiseaseqPriorcellulitis

66
InfectionCharacteristicsLocationofcellulitis: qArm qLeg qHand qFoot qTorso qGroin qAxilla qFaceChroniculcers: qYes qNoSurgicalsiteinfection: qYes qNoBite(humanoranimal) qYes qNoMaximumlengthoferythema(cm):__________qNotrecordedMaximumwidthoferythema(cm):__________qNotrecordedAreaoferythema(cm2):__________qNotrecorded Areadeterminedby:qDiagram qPhotograph
qText(dimensions) qText(non-specific)PercentTBSAinvolved: q<5% q5–10% q10–20% q>20%TriageVitalSignsTemperature:__________°CHeartrate:__________bpmRespiratoryrate:__________breaths/minuteSystolicBP:__________mmHgSaO2:__________% qRAqSupplementalO2WBCCount:__________(x109/L)CurrentTreatment(PriortoEDVisit)IspatientcurrentlytakingantibioticsforSSTI? oYes oNo
Ifyes,completethefollowing(checkallthatapply):Antibioticpatientiscurrentlytaking:qPOAmoxicillin-Clavulanate(Clavulin) qPOAmoxicillin qPOTMP-SMX(Septra) qPOCephalexin(Keflex)qPOClindamycin qPOCiprofloxacinqPOPenicillinqIVCeftriaxone qIVCefazolin(Ancef)qIVClindamycin qIVPipercillin-TazobactamqIVVancomycin qIVPenicillin
qIVCiprofloxacin qIVMeropenem qOther:_________________________ Duration(fromstarttoEDvisit;days):____________________

67
EDTreatment(whatwasgivenintheED)Route:
qOralAntibioticsonly? qIVAntibioticsonly? qOralandIVAntibiotics?
NumberofOralAntibiotics: q0 q1 q2NumberofIVAntibiotics: q0 q1 q2OralCephalexin(Keflex)? qYes qNo
IfYes,Dose(mg): q250 q500 q1000OralAmoxicillin-Clavulanate? qYes qNo
IfYes,Dose(mg): q500 q875 OralAmoxicillin? qYes qNo
IfYes,Dose(mg): q250 q500 q1000OralClindamycin? qYes qNo
IfYes,Dose(mg): q300 q450 q600OralTMP-SMX(Septra)? qYes qNo
IfYes,Dose(mg): q800(1DStab) q1600(2DStabs)OralCiprofloxacin? qYes qNo
IfYes,Dose(mg): q250 q500 q1000IVCefazolin(Ancef)? qYes qNo
IfYes,Dose(mg): q500 q1000 q1500q2000IVCeftriaxone? qYes qNo
IfYes,Dose(mg): q1000 q1500 q2000IVClindamycin? qYes qNo
IfYes,Dose(mg): q300 q450 q600q900IVMeropenem? qYes qNo
IfYes,Dose(mg): q500 q1000 q1500q2000IVVancomycin? qYes qNo
IfYes,Dose(mg): q500 q1000 q1500q2000IVPiperacillin-Tazobactam? qYes qNo
IfYes,Dose(mg): q3375 q4500 IVCiprofloxacin? qYes qNo
IfYes,Dose(mg): q200 q400

68
WhatwasEDpatientdisposition?qHome qHospitaladmission(Ifadmitted,lengthofstay(days):__________)Ifsenthome:WherewillpatientgetsubsequentIVdoses? qOPAT/CCACqCCAConlyqReturntoEDqNoIVABXIfsenthome:EDPrescription:OralCephalexin(Keflex)? qYes qNo
IfYes,Dose(mg): q250 q500 q1000Frequency: qBID qTID qQID Duration(days):____________________
OralAmoxicillin-Clavulanate? qYes qNo
IfYes,Dose(mg): q500 q875 Frequency: qBID qTID qQID Duration(days):____________________
OralAmoxicillin? qYes qNo
IfYes,Dose(mg): q250 q500 q1000Frequency: qBID qTID qQID Duration(days):____________________
OralClindamycin? qYes qNo
IfYes,Dose(mg): q300 q450 q600Frequency: qBID qTID qQID Duration(days):____________________
OralTMP-SMX(Septra)? qYes qNo
IfYes,Dose(mg): q800(1DStab) q1600(2DStabs)Frequency: qOD qBID qTID Duration(days):____________________
OralCiprofloxacin? qYes qNo
IfYes,Dose(mg): q250 q500 q1000Frequency: qOD qBID qTID Duration(days):____________________

69
IVCefazolin(Ancef)? qYes qNoIfYes,Dose(mg): q500 q1000 q1500q2000
Frequency: qBID qTID qQID Duration(days):____________________
IVCeftriaxone? qYes qNo
IfYes,Dose(mg): q1000 q1500 q2000Frequency: qOD qBID Duration(days):___________________
IVClindamycin? qYes qNo
IfYes,Dose(mg): q300 q450 q600q900Frequency: qBID qTID qQID Duration(days):___________________
IVMeropenem? qYes qNo
IfYes,Dose(mg): q500 q1000 q1500q2000Frequency: qBID qTID qQID Duration(days):___________________
IVVancomycin? qYes qNo
IfYes,Dose(mg): q500 q1000 q1500q2000Frequency: qOD qBID qTID Duration(days):___________________
IVPiperacillin-Tazobactam? qYes qNo
IfYes,Dose(mg): q3375 q4500 Frequency: qBID qTID qQID Duration(days):___________________
IVCiprofloxacin? qYes qNo
IfYes,Dose(mg): q200 q400Frequency: qBID qTID qQID Duration(days):___________________

70
Ifsenthome:ReturntoEDwithin14days: oYes oNo Ifyes(chooseONEonly):
oReturntoEDforSSTIandhospitaladmission oReturntoEDforSSTIbutnoadmission oReturntoEDwithabscess(Ifyes,I&Dperformed? oYes oNo) oReturntoEDforrepeatantibiotics:numberofsubsequentvisits_____oReturntoEDforunrelatedmedicalproblem
Ifsenthome:ChangestotreatmentinEDatrepeatvisit: oYes oNo qN/A
Ifyes(chooseONEonly):oChangefromPOtoIVantibiotics(nameofnewantibiotic:_______________)oChangetodifferentPOantibiotic(nameofnewantibiotic:_______________) oChangetodifferentIVantibiotic(nameofnewantibiotic:_______________)oChangetodifferentantibioticdose(newdose:________________mg)Iftreatmentwasaltered,reasonforchangeintreatmentplan:
oWorseninginfection oNoimprovementoVomiting oDiarrhea oRash/hivesoOther Indicate:_____________________
POTreatmentFailure? qYesqNo Ifyes,reasonfortreatmentfailure(checkallthatapply): qStep-upfromPOtoIVantibiotic qChangeinclassofantibiotic(duetoworseninginfection) qInitialoutpatientmanagementwithsubsequenthospitaladmissionIVTreatmentFailure? qYesqNo Ifyes,reasonfortreatmentfailure(checkallthatapply): qChangeinclassofantibiotic(duetoworseninginfection) qInitialoutpatientmanagementwithsubsequenthospitaladmission

71
Ifsenthome,AdverseEvents: Adversedrugreaction: qYesqNo Ifyes: qRash qNauseaonly(novomiting) qVomiting qDiarrhea qOther:____________________
Adversedeviceevent: qYesqNo Ifyes: qBlockedperipheralIV qDislodgedperipheralIV qLinethrombosis qLineinfection
Subsequenthospitaladmissionat14daysfromindexEDvisit?qYesqNo Ifyes: qForworseningSSTI
qForunrelatedmedicalproblem(specify:_______________)IfreferredtoOPATClinic(qYes qNo[STOPhere]):DidpatientattendOPATappointment? qYesqNo–losttofollow-upCellulitiswascorrectdiagnosis: qYesqNo IfNO–specifyalternatediagnosis:____________________NumberofdaysfrominitialEDvisittofirstOPATappointment:__________TotalnumberofvisitstoOPATclinic:__________TotalnumberofdaysonIVantibiotics:__________TotalnumberofdaysonIVandPOantibiotics:__________(qN/A)

72
TableS1.VariableDefinitions
Variable DefinitionActivecancer Cancerbeingtreatedwithchemotherapyor
palliative;documentedonEDROTorrecentconsult
Chronickidneydisease Impairedrenalfunction≥3months.CKDshouldbechartedoneitherEDrecordoftreatment(ROT)orrecentconsult
Chronicvenousinsufficiency Duplexultrasoundshowingvenousreflux(reversedflowfor>0.5seconds)orchartedontheEDROTorrecentconsult
Congestiveheartfailure DocumentedonROTorrecentconsult.Coronaryarterydisease Priormyocardialinfarction,percutaneous
coronaryinterventionorasotherwisestatedoncardiologyconsult,EDROTorrecentconsult
Corticosteroids(systemic) PatienttakingoralorintravenouscorticosteroidsatthetimeofEDvisit
Diabetesmellitus Takinginsulinororalmedications(e.g.metformin,gliclazide,etc.)atthetimeofEDpresentation,ordocumentedonrecentconsultorEDROT
Hepaticdisease DocumentationonEDROTorrecentconsultofanyofthefollowing:hepatitisB,hepatitisCorlivercirrhosisfromanycause
Injectiondruguse DocumentationonEDROTorrecentconsultofeitherintravenousorsubcutaneousinjectionofmedicationsorrecreationaldrugs
Lymphedema DocumentedonEDROTorrecentconsultMRSApositive Documentedonelectronichealthrecordtohave
knownMRSAcolonizationorpriorMRSAinfectioninthepast12months
Obesity DocumentedonEDROTorrecentconsultOrgantransplantrecipient DocumentedonEDROT,operativereportsora
recentconsult.Includesfollowingtransplants:heart,liver,kidney,andbonemarrow
Peripheralvasculardisease Operativereportofbypassgraftingforperipheralvasculardisease,ordocumentedonEDROTorrecentconsult
Priorcellulitis DocumentedEDvisitfornon-purulentcellulitisorerysipelasinthepast12months
Recentconsult Consultonelectronichealthrecordwithin3monthsofthepatient’sindexEDvisit

73
TableS2.UnivariateAssociationwithOralAntibioticTreatmentFailurefor288EDPatientsTreatedwithaMinimumof48HoursofOralTherapyVariable
OralAntibioticTreatmentFailure(N=85)
NoOralAntibioticTreatmentFailure(N=203)
PValue*
Age,years(mean± SD)Malegender(%)Comorbidities(%)ChronickidneydiseaseCongestiveheartfailureCoronaryarterydiseaseDiabetesmellitusHepaticdiseaseIntravenousdruguseLymphedemaObesityPeripheralvasculardiseaseHistoryofMRSAinfectionPriorcellulitisinpast12months
VitalSignsTemperature,°C(mean±SD)HeartRate,beats/min(mean±SD)BloodPressure,mmHg(mean±SD)RespiratoryRate,breaths/min(median,IQR)OxygenSaturation,%(median,IQR)
InfectionCharacteristics(%)ChronicUlcersBiteSurgicalSiteInfectionSize:TBSA≥5%
67±19
48(56.5)
8(9.4)8(9.4)12(14.1)23(27.1)5(5.9)3(3.5)5(5.9)3(3.5)5(5.9)11(12.9)19(22.4)
36.6±0.884±17140±2216,16–18
97,96–98
13(15.3)1(1.2)7(8.2)14(16.5)
63±20
110(54.2)
7(3.4)10(4.9)17(8.4)32(15.8)12(5.9)1(0.5)9(4.4)5(2.5)12(5.9)5(2.5)19(9.4)
36.3±0.783±16138±2416,16–18
97,96–98
7(3.4)7(3.4)13(6.4)25(12.3)
0.15
0.72
0.040.150.140.030.990.090.560.690.990.0010.003
0.010.680.690.85
0.11
0.00030.440.580.35
*UsingChiSquaredorFisher’sExactTestforcategoricalvariables;t-testsfornormallydistributedcontinuousvariables;Wilcoxontestsfornon-normallydistributedcontinuousvariablesSD=standarddeviation;IQR=interquartilerange;MRSA=methicillinresistantStaphylococcusaureus;TBSA=totalbodysurfacearea

74
TableS3.TreatmentFailurewithIVAntibiotics(N=12of212PatientsTreatedwithaMinimumof48HoursofIVTherapy)
IVAntibioticTreatmentFailures Numberofpatients,N=12N(%)
PatientOutcomesHospitalizedforIVantibioticsSwitchedtooutpatientIVantibiotics
TreatmentfailureoninitialEDvisit*TreatmentfailureonreturnEDvisitwithin14days
11(91.7)1(8.3)
5(41.7)7(58.3)
*Patientwasalreadyon≥48hoursofIVantibiotictherapyattimeofindexEDvisitIV=intravenous;ED=emergencydepartment

75
TableS4.SecondaryAnalysisComparingOralversusIntravenousAntibioticGroupsforCategoricalVariablesforall500Patients
Variable(n)
OralAntibioticGroupFrequency,n(%)
(n=288)
IVAntibioticGroupFrequency,n(%)
(n=212)
PValue*
Male(279) 158(54.9) 121(57.1) 0.62
ChronicUlcers(56) 20(6.9) 36(17.0) 0.0004SurgicalSiteInfection(30)
20(6.9) 10(4.7) 0.30
Bite(12) 8(2.8) 4(1.9) 0.52
>5%TBSA(99) 39(13.5) 60(28.3) <0.0001
Coronaryarterydisease(58)
29(10.1) 29(13.7) 0.21
Congestiveheartfailure(48)
18(6.2) 30(14.1) 0.003
Chronickidneydisease(35)
15(5.2) 20(9.4) 0.07
Chronicvenousinsufficiency(10)
8(2.8) 2(0.9) 0.20
Diabetesmellitus(126)
55(19.1) 71(33.5) 0.0002
HepaticDisease(37) 17(5.9) 20(9.4) 0.14HIV(8) 2(0.7) 6(2.8) 0.08IVDU(14) 4(1.4) 10(4.7) 0.02Lymphedema(33) 14(4.9) 19(9.0) 0.07MRSAHistory(43) 16(5.6) 27(12.7) 0.005Obesity(27) 8(2.8) 19(9.0) 0.002Priorcellulitis(87) 38(13.2) 49(23.1) 0.004PVD(40) 17(5.9) 23(10.8) 0.04
OnSupplementalO2(36)
12(4.2) 24(11.7) 0.002
*UsingChi-SquaredorFisher’sExactTestIV=intravenous;TBSA=totalbodysurfacearea;HIV=humanimmunodeficiencyvirus;IVDU=intravenousdruguse;MRSA=methicillinresistantStaphylococcusaureus;PVD=peripheralvasculardisease

76
TableS5.SecondaryAnalysisComparingOralversusIntravenousAntibioticGroupsforContinuousVariablesforall500Patients
Variable(n)
OralAntibioticGroup
Frequency,n(%)(N=288)
IVAntibioticGroup
Frequency,n(%)(N=212)
PValue*
Age(mean±SD) 64.4±20.0 64.3±16.9 0.95SystolicBP(mean±SD) 139±23 131±25 0.0007Heartrate(mean±SD) 84±16 90±21 <0.0001Temperature(mean±SD) 36.4±0.8 36.8±1.2 <0.0001RespiratoryRate(median,IQR)
16(16–18) 18(16–20) 0.02
SaO2(median,IQR) 97(96–98) 97(96–98) 0.88WBCcount(median,IQR) 8.2(6.6–11.2) 10.4(7.7–14.7) <0.0001*Usingt-testsfornormallydistributedvariables,Wilcoxontestsfornon-normallydistributedvariablesSD=standarddeviation;IQR=interquartilerange;IV=intravenous;BP=bloodpressure;HR=heartrate;SaO2=oxygensaturation;WBC=whitebloodcell

77
ChapterFour:OutpatientParenteralAntibioticTherapyFollowingEmergencyDepartmentTreatmentofNon-PurulentSkinandSoftTissue
Infections
ChapterOverviewInthepreviouschapter,weidentifiedpotentialpredictorsassociatedwithoral
antibiotictreatmentfailurefornon-purulentskinandsofttissueinfections.Most
patientsinthisstudycohortreceivedatleastonedoseofintravenousantibiotic,and
morethanonethirdofdischargedpatientswereprescribedoutpatientparenteral
antibiotictherapy.Duetothestudydesign,itwasnotpossibletoidentifyemergency
physicianrationaleforselectingintravenoustherapy,whichisanimportantfirst
stepinthedecisiontorefertoanoutpatientparenteralantibiotictherapyprogram.
Furthermore,itwasnotpossibletodescribeoutpatientparenteralantibiotic
therapyclinicprocessesortodeterminepatientsatisfactionwiththistreatment
approach.
Thefollowingisamanuscriptpreparedforpublicationbasedonaprospective
observationalcohortstudy.Theobjectivesofthemanuscriptwere:1)describethe
performanceofanemergencydepartment-to-outpatientparenteralantibiotic
therapyclinicprograminthetreatmentofadultswithnon-purulentskinandsoft
tissueinfections;2)identifyemergencyphysicianrationaleforselecting
intravenoustherapy;and3)determinepatientsatisfactionwiththistreatment
approach.

78
InAppendixAacopyoftheapprovalletterfromtheOttawaHealthScience
NetworkResearchEthicsBoardisprovided.
Dr.KrishanYadavisthefirstauthorofthismanuscriptandwasresponsibleforthe
studydevelopment,datacollection,dataanalysisandwritingofthemanuscript.
Thismanuscriptwasco-authoredbyDr.IanStiell,Dr.KathrynSuhandDr.George
Wells.Dr.DebraEaglesandDr.VenkateshThiruganasambandamoorthyprovided
valuablefeedbackthroughouttheprocess.

79
OutpatientParenteralAntibioticTherapyFollowingEmergencyDepartment
TreatmentofNon-PurulentSkinandSoftTissueInfections
KrishanYadav1,KathrynSuh2,DebraEagles3,Venkatesh
Thiruganasambandamoorthy3,GeorgeWells4,5,IanGStiell3
1DepartmentofEmergencyMedicine,UniversityofOttawa
2DepartmentofMedicine,DivisionofInfectiousDiseases,UniversityofOttawa
3DepartmentofEmergencyMedicine,TheOttawaHospitalResearchInstitute,
UniversityofOttawa
4CardiovascularResearchMethodsCentre,UniversityofOttawaHeartInstitute
5DepartmentofEpidemiologyandCommunityMedicine,UniversityofOttawa
Correspondenceto:KrishanYadav
Email:[email protected]
Date:January30,2018
WordCount:2978
Acknowledgments:Theauthorswouldliketothankthefollowingindividualsfor
theirassistanceinthisstudy:My-LinhTran,SherylDomingo,AngelaMarcantonio
andCatherineClement.ThisstudywasfundedbyagrantfromtheDepartmentof
EmergencyMedicine,UniversityofOttawa,Ontario,Canada.Thisstudywasfunded
byagrantfromtheDepartmentofEmergencyMedicine,UniversityofOttawa.

80
AbstractIntroduction
Emergencydepartment(ED)patientswithnon-purulentskinandsofttissue
infections(SSTIs)requiringintravenousantibioticsmaybemanagedviaoutpatient
parenteralantibiotictherapy(OPAT).Todate,therearenoprospectivestudies
describingtheperformanceofanED-to-OPATclinicprogram.Furthermore,there
arenostudiesthathaveexaminedphysicianrationaleforintravenoustherapy,
despitethisbeingacriticalfirststepinthedecisiontorefertoanOPATprogram.
TheprimaryobjectivewastodeterminetheOPATtreatmentfailurerateforadults
withnon-purulentSSTIswhoareinitiallymanagedintheED.
Methods
Weconductedaprospectiveobservationalcohortstudyofadults(age≥18years)
withnon-purulentSSTIsreceivingparenteraltherapyattwotertiarycareEDs.
Patientswereexcludediftheyhadpurulentinfectionsorcouldnotprovideconsent.
OPATtreatmentfailurewasdefinedaprioriashospitalizationafteraminimumof
48hoursofOPATfor:(i)infectionprogression;(ii)line-relatedcomplications(e.g.
bacteremia,thrombophlebitis,venousthromboembolism);or(iii)drug-related
complications(e.g.Clostridiumdifficilecolitis).Secondaryoutcomeswereto
describeOPATclinicprocessesandadverseevents,assesspatientsatisfaction,and
identifyEDphysicianrationaleforselectingintravenousantibiotics.Theemergency
physiciancompletedaformdocumentingrationaleforintravenoustherapy,

81
infectionsizeandchoiceofantimicrobialagent,doseandduration.Patient
satisfactionwasassessedata14-daytelephonefollowup.
Results
Weenrolledaconsecutivesampleof153patients(meanage60years,82male
(53.6%)and38(24.8%)withdiabetes).Atotalof137patients(89.5%)attended
theirOPATclinicappointment.Ofthe101patientsprescribedcefazolin,50.5%
received1000mgand48.5%received2000mg.TherewerelowratesofOPAT
treatmentfailure(4.4%).Noneoftheadverseperipheralintravenouslineevents
(10.9%)andadverseantibioticevents(8.0%)requiredhospitalization.Patients
reportedahighdegreeofsatisfactionwithtimelinessofclinicreferral(median
score9outof10)andoverallcarereceived(medianscoreof10outof10).Thetop
5reasonsgivenbyphysiciansforselectingintravenoustherapywere:clinical
impressionofseverity(52.9%);failedoralantibiotictherapy(41.8%);diabetes
(17.6%);severepain(7.8%);andperipheralvasculardisease(7.8%).
Conclusion
Thisisthefirststudytoidentifyphysicianrationalefortheuseofintravenous
antibioticsforSSTIs.Therewassignificantvariabilityinantibioticprescribing
practicesbyEDphysicians.ThisprospectivestudydemonstratesthatanED-to-
OPATclinicprogramfornon-purulentSSTIsissafe,hasalowrateoftreatment
failuresandresultsinhighpatientsatisfaction.

82
Introduction
Firstdescribedin1974,outpatientparenteralantibiotictherapy(OPAT)isdefined
astheadministrationofatleasttwodosesofparenteralantimicrobialsondifferent
dayswithoutinterimobservation.1OPATisanattractiveoptionforadultswithnon-
purulentskinandsofttissueinfections(SSTIs)whorequireintravenousantibiotics.
Patientsdischargedfromtheemergencydepartment(ED)canreceiveOPATfollow
upinanumberofsettings:returntotheED,afamilyphysicianclinic,ahomecare
clinicrunbynurses,oradedicatedOPATclinic.Duetodifficultieswithprimarycare
access2andassociationsbetweenEDovercrowdingandincreasedadverseevents3,
anED-to-OPATclinicprogrammaybeapreferredoptionduetoimportant
advantages:1)decreasedhospitaladmissions;2)increasedpatientconvenience;
and3)decreasedEDvisits.
ED-basedstudieshaveshownthatintravenousantibioticsarefrequently
administered4,5andthatantibioticoveruseiscommon.6Surprisingly,thereisscant
literatureregardingEDantibioticprescribingforSSTIs.7-9Furthermore,thereareno
publishedstudiesdescribingEDphysicianrationaleforselectingintravenousover
oralantibiotics,despitethisbeingacriticalfirststepinthedevelopmentofanOPAT
program.1,8AdministrationofOPATisnotwithoutrisk.Potentialadverseeventsfor
anyinfectiontreatedwithOPATincludeinfectionprogression,peripheralline-
relatedcomplicationsoradverseantibioticeventsthatmaywarrantsubsequent
hospitalization.9,10PriorstudiesreportthehospitaladmissionratefollowingOPAT
rangingfrom2.6to8%.9,11,12However,thesestudiesincludedanumberof

83
infections,makingitdifficulttodeterminethetrueclinicalfailurerateforSSTIsin
particular.Arecentretrospectivestudyreportedahospitaladmissionrateof5.5%
foracellulitisOPATcohort,althoughthereasonsforhospitalizationwerenot
described.13
TheprimaryobjectiveofthisstudywastodeterminetheOPATtreatmentfailure
rateforadultswithnon-purulentSSTIswhoareinitiallymanagedintheED.
SecondaryobjectivesweretodescribeOPATclinicprocesses(timetofirst
appointment,totalnumberofclinicvisitsanddurationoftherapy),adverseevents,
assesspatientsatisfaction,andidentifyemergencyphysicianrationaleforselecting
intravenousantibiotics,
Methods
StudyDesignandSettingWeconductedaprospectiveobservationalcohortstudyofadultpatientswithnon-
purulentSSTIsinitiallymanagedintheEDwithintravenousantibioticsandreferred
totheOPATclinic.ThestudypopulationwasenrolledfromtheOttawaHospital
CivicandGeneralEDs(twotertiarycareadultEDswithacombined170,000patient
visitsannually).AllenrolledpatientswerereferredtotheOPATclinic,locatedatthe
OttawaHospitalCivicCampus.TheOttawaHospitalOPATclinicwasestablishedin
2014andoperatesonthreehalfdaysperweekbyappointmentonly.TheOttawa
HealthScienceNetworkResearchEthicsBoardapprovedthisstudy.

84
StudyPopulationWeenrolledaconsecutivesampleofpatientsmeetingeligibilitycriteriafrom
January15toJune20,2017.Eligiblepatientswereadults(age≥18years)
presentingtotheEDanddiagnosedwithanon-purulentSSTIthatwasfeltbythe
emergencyphysiciantorequireintravenousantibioticsandfollowupintheOPAT
clinic.Patientswereexcludedforthefollowingreasons:(i)age<18years;(ii)
diagnosisofapurulentSSTIwhereanincisionanddrainageprocedurewas
performed;(iii)necrotizinginfections;(iv)significantcognitiveorverbal
impairmentsuchthatinformedconsentwasnotfeasible;or(v)thosewhowerenot
localresidentsorwhodidnothaveatelephone.
IntravenousAntibioticTreatmentTheemergencyphysicianselectedtheagent,dose,frequencyanddurationof
parenteralantibioticattheirowndiscretion.Allpatientsreceivedintravenous
antibioticsinthecommunityviathelocalhomecareprogram.Patientsreturnedto
theEDforsubsequentintravenousdosesiftherewasadelayinestablishing
homecareasanoutpatient.Patientsthenfollowedupwithaninfectiousdisease
specialistattheOPATclinic,atthenextavailableclinicdate(rangingfromtwoto
tendays).Theinfectiousdiseasespecialistwasresponsiblefordeterminingif
furtherintravenoustherapywaswarrantedorifthepatientcouldbesteppeddown
tooraltherapy.
DataCollectionAllpatientswereassessedbyemergencyphysiciansorresidentssupervisedby
attendingemergencyphysicians.Studydetailsweredistributedbyelectronicmailto
familiarizephysicianswiththestudy.Theemergencyphysicianwasresponsiblefor

85
completingtheOPATreferralform(seethesupplementaryappendix),whichalso
requiredthephysiciantoindicaterationaleforselectingintravenoustherapy.
Physicianswereaskedtousearulerontheright-marginofthereferralformto
obtainaccurateinfectiondimensions.Patientswereprovidedwithaninformation
sheetoutliningthestudydetailsandverbalconsentwasobtainedfora14-day
telephonefollow-upcall.Theprincipalinvestigator(KY)screenedallreferralstothe
OPATclinictoensurethatnocasesweremissed.
Allpatientsreceiveda14-daytelephonefollowuptoassesspatientsatisfaction.
Participantswereconsideredlosttotelephonefollowupiftheycouldnotbe
reachedafteramaximumofthreephonecalls.Theprincipalinvestigatorabstracted
allrelevantclinicaldatafromtheelectronichealthrecord(EDphysicianandnursing
notes,OPATclinicrecords)ontoastandardizedcaserecordform(seethe
supplementaryappendix).Eligiblepatientswereenrolledregardlessofwhetherthe
OPATreferralformwasfullycompleted.
OutcomeMeasuresTheprimaryoutcomewasOPATtreatmentfailure.Thereisnoestablished
definitionofOPATtreatmentfailureforSSTIsintheliterature.TheUnitedStates
FoodandDrugAdministrationrecommendsthatclinicalresponsetotreatment
shouldbeassessedat48to72hoursfrominitiatingtherapy.14Whensurveyed,a
majorityofCanadianemergencyphysiciansselected48hoursastheoptimal
timeframefordeterminingiftreatmentfailurehadoccurredfollowinginitiationof
antibiotictherapy.15Afterreviewoftheliterature4,5,16-20anddiscussionwithlocal

86
expertsinemergencymedicineandinfectiousdisease,wedevisedadefinitionof
OPATtreatmentfailure.Patientswereconsideredtohaveatreatmentfailureifa
patientwassubsequentlyadmittedtohospitalafteraminimumof48hoursofOPAT
foranyofthefollowingreasons:(i)worseninginfection;(ii)line-related
complications(e.g.bacteremia,venousthrombosis);or(iii)drug-related
complications(e.g.Clostridiumdifficilecolitis).
SecondaryoutcomesincludedEDphysicianrationaleforselectingtheintravenous
route,OPATclinicdataandpatientsatisfaction.Thetreatingphysicianwasallowed
toselectmorethanonereasonforselectingintravenoustherapy.Forclinicdata,we
recordedtimetofirstvisit,totalnumberofvisits,andthenumberofpatientslostto
follow-up.Ata14-daytelephonefollowup,weaskedpatientstogiveanumerical
ratingfromone(leastsatisfied)toten(mostsatisfied)withrespecttotimelinessof
referralfromtheEDandoverallpatientsatisfaction.Adverseoutcomesincluded
antibioticeventsanddeviceevents.
DataAnalysisWeuseddescriptivestatisticstodescribetheproportionofpatientswhohadan
OPATtreatmentfailure,adverseantibioticordeviceevents,OPATclinicdataand
patientsatisfaction.Continuousdataarepresentedasmeanswithstandard
deviationsormedianswithaninterquartilerange(IQR,Q1–Q3)fornormallyand
non-normallydistributeddata,respectively.Categoricaldataarepresentedas
proportionswith95%confidenceintervals.

87
SampleSizeTheOPATclinicattheOttawaHospitaltreatsapproximately30newpatientswith
SSTIspermonth.Afteradjustingfor10%dropout,weestimatedaconsecutive
enrolmentofapproximately135patientsovera5-monthperiod.Thissamplesize
wasbasedonfeasibilityduetofundingandtimeconstraints.
ResultsWescreened214casesreferredtotheOPATclinicoverthefive-monthstudyperiod
andidentified153eligiblecases(Figure1).Atotalof137patients(89.5%)attended
theirclinicappointment.Oftheremaining16patients(10.5%),fivepatientswere
admittedtohospitalpriortotheirclinicappointmentand11werelosttofollowup.
Forpatientswhoattendedtheirappointment,wewereabletocontact118patients
(86.0%)fora14-daytelephonefollowup.
Tables1and2highlightthebaselinepatientandinfectioncharacteristics,
respectively.Themeanageofenrolledpatientswas60years,andalmostaquarter
ofpatientshaddiabetes(24.8%)orlymphedema(23.5%).Almosthalfofpatients
(48.4%)weretakingoralantibioticsatthetimeoftheirpresentationtotheED.The
mostcommonlocationofinfectionwastheleg(45.1%)andthemedianareaof
erythemawas150cm2(IQR40–300).Emergencyphysiciansorderedbloodtestsin
themajorityofthesepatients(68.0%)andthemedianwhitebloodcellcountwas
9.0×109/L(IQR6.8–11.6).Thetreatingphysicianorderedbloodculturesfor22
patients(14.4%);therewereclinicallysignificantpositivebloodcultures(one
positivebloodculturewasconsideredtobeacontaminant).

88
Table3showsthevariationinantimicrobialtherapyadministeredintheED.Most
patientsreceivedasingleintravenousantibiotic(93.5%).Cefazolinwasthemost
commonlyadministeredantibioticandwasadministeredin99patients(64.7%).Of
thosethatreceivedcefazolin,33patients(33.3%)and66patients(66.7%)received
1000mgand2000mg,respectively.
InTable4,thevariationinantibioticprescribingpracticesforpatientssenthome
fromtheEDispresented.Cefazolinwasthemostcommonlyprescribedantibiotic
(66.0%).Thechosendoseofcefazolinfor101patientswasasfollows:1000mg(n=
51,50.5%);1500mg(n=1,1.0%);and2000mg(n=49,48.5%).Aftercefazolin,
themostcommonlyprescribedantibioticswereceftriaxone(19.6%)and
clindamycin(10.5%).
Emergencyphysicianrationaleforselectingintravenousantibioticsisshownin
Table5.Treatingphysiciansprovidedatotalof22differentrationales.Thetopfive
reasonsforselectingintravenoustherapywere:clinicalimpression(52.9%);failed
oralantibiotictherapy(41.8%);diabetes(17.6%);severepain(7.8%);and
peripheralvasculardisease(7.8%).
Ofthetotal153patientsreferredtotheOPATclinic,137patients(89.5%)attended
theirscheduledappointment.TheOPATclinicdataareshowninTable6.The
emergencyphysicianandinfectiousdiseasespecialistdiagnosisofanon-purulent

89
SSTIwereconcordantin93.4%ofcases.Themediantimetothefirstclinicvisitwas
5days(IQR4–7).Themediandurationofintravenoustherapywas9days(IQR7–
14).Patientsreportedahighdegreeofsatisfactionwithtimelinessofclinicreferral
(medianscore9outof10)andoverallcarereceived(medianscoreof10outof10).
Ofthe118patientswhocouldbereachedfortelephonefollowup,110patients
(93.2%)indicatedtheywouldpreferfollow-upwiththeOPATcliniciftheyrequired
intravenousantibioticsinthefuture.
Table7shows14-dayoutcomesforthe137patientswhoattendedtheirinitial
OPATclinicappointment.Themajorityofpatients(63.5%)returnedtotheED
within14days.Themostcommonreasonwasareturnforscheduledintravenous
dosesifthehomecareprogramcouldnotbeinitiatedintimeforthenextrequired
dose.OnlysixpatientssufferedanOPATtreatmentfailure(4.4%);allweredueto
worseninginfection.Fifteenpatients(10.9%)hadanadversedeviceevent(blocked
ordislodgedperipheralintravenousline)andtherewerenocasesoflineinfection
orbacteremia.Elevenpatients(8.0%)hadanadverseantibioticeventwiththe
majorityexperiencingdiarrhea.Noneoftheadversedeviceorantibioticevents
resultedinhospitalization.
Discussion
InterpretationofResultsThisprospectiveobservationalcohortstudydescribesED-to-OPATclinic
performanceinthemanagementofadultswithnon-purulentSSTIs.Therewas

90
significantpracticevariationamongstemergencyphysiciansregardingantibiotic
agent,doseandduration.Cefazolinwasthemostcommonlyprescribedparenteral
antibioticandemergencyphysiciansweresplitregardingthedose.Thisisthefirst
studytoprospectivelyevaluateemergencyphysicianrationaleforintravenous
antibiotics.Thetopfivereasonsforselectingintravenoustherapywere:clinical
impression;failedoralantibiotictherapy;diabetes;severepain;andperipheral
vasculardisease.TherewasaverylowrateofbothOPATtreatmentfailuresand
adverseantibioticorperipherallineevents.Patientsreportedaveryhighdegreeof
satisfactionwiththeircare.OurfindingsstrengthentheargumentthatanED-to-
OPATclinicmodeliseffective,safe,andresultsinahighdegreeofpatient
satisfaction.
PreviousStudiesOurstudyfoundalowOPATtreatmentfailurerate(4.4%)thatissimilarto
previouslypublishedstudies.9,11,12However,thisisthefirstprospectivestudyto
assessOPATfornon-purulentSSTIsinparticular.Appropriatepatientselectionfor
outpatientintravenoustherapyisacriticalfirststeptothesuccessofanOPAT
program.1,8However,therearenopublishedstudiestodatethathaveexamined
physicianrationaleforselectingparenteraltherapy.Currentguidelines1,21,22list
patientsatisfactionasakeyelementtoanOPATprogram.Wefoundahighdegreeof
patientsatisfactionthatissimilartopriorstudies.12,23
StrengthsAconsecutivesampleofpatientswasenrolledandwescreenedallOPATclinic
referralssoasnotmissanypotentialcasesoverthestudyperiod.Thedatawere

91
collectedprospectivelyandwewerethusabletoaccuratelyidentifyphysician
rationaleforselectingparenteraltherapy.Thisisthefirstprospectivestudythat
providesimportantinsightintophysiciandecision-makingregardingpatient
selectionforintravenoustherapy.
LimitationsTherearestudylimitationsthatwarrantmention.First,thisstudywasconductedat
twotertiarycareEDsbuthadasmallsamplesizeduetofeasibility.Somepatients
didnotattendtheirclinicappointmentandwerelosttofollow-up(7.2%).Itis
possiblethatsomeofthesepatientslosttofollowupmayhaveexperienceda
treatmentfailure.However,wefeelitisunlikelythatpatientswhoreceived
treatmentatourcentrewouldpresenttoanotherhospitalforfurthercare.Another
limitationwasthat14.0%ofpatientswhoattendedtheclinicvisitcouldnotbe
reachedbytelephoneordeclinedconsent.Itispossiblethattheirpatient
satisfactionscoresmayhavedifferedsignificantlyfromthegroupthathada
completefollowup.Third,theconfidenceintheresultsmaybeaffectedbythesmall
samplesize.
Afurtherlimitationisthatwecouldnotrecordpatientweightorcategorizethe
degreeofobesityduetofeasibilityinobtainingthisdata.Itispossiblethatatleast
someofthevariationobservedinantimicrobialdosing,durationandfrequency
mightberelatedtopatientbodyhabitus.However,wefeelthisisunlikelybecause
thesmallproportionofpatientswithobesity(12.4%)wouldnotfullyexplainthe
highdegreeofobserveddosingvariability.

92
Lastly,thereisnovalidateddefinitionofOPATtreatmentfailure.Petraketal.
recommendedthatfuturestudiesexaminingOPATefficacyshouldincluderobust
definitionsfortreatmentfailure.11Weattemptedtodeveloparobustdefinitionby
reviewingtheliterature4,5,16-20andreachingconsensusamonglocalexpertsin
emergencymedicineandinfectiousdisease.Thisdefinitionwasacomposite
endpoint.Disadvantagesofusingacompositeendpointincludemisleadingresultsif
onecomponentoftheoutcomeheavilydrivestheresult,especiallyifitistheleast
patient-importantoutcome.However,thecomponentsofourdefinitionallresulted
inthesamefinaloutcomeofhospitaladmission.
ClinicalImplicationsThereareimportantclinicalimplicationsthatdeservemention.Ourstudy
demonstratedahighdegreeofvariationinantimicrobialprescribingpractices.
Whilethismayinpartbeduetovariationinpatientpresentation(e.g.animalbite,
antibioticallergy),theresultsstillreflectalackofconsensusamongstemergency
physiciansregardingoptimalmanagementofthiscommonclinicalcondition.For
example,thedoseforthemostcommonlyprescribedantibiotic(cefazolin)was
nearlyevenlysplit–whichcannotbeexplainedbyheterogeneityinpatient
presentationalone.TheratesofadverseeventsandOPATtreatmentfailurewere
verylow,suggestingthattheED-to-OPATclinicmodelissafe,effectiveandresultsin
highpatientsatisfaction.Thismodelcanbeintroducedinothercommunitiesto
potentiallydecreasehospitaladmissionsandassociatedhealthcarecosts.

93
ResearchImplicationsOurstudyidentifiedreasonsemergencyphysiciansinstituteintravenousantibiotic
therapyfornon-purulentSSTIs.Futurestudiesshouldseektoassesswhether
patientswiththeseidentifiedrationalestrulyrequireintravenoustherapy,or
whethertheycanbetreatedwithlessinvasiveandcheaperoralantibiotics.Wealso
identifiedalargedegreeofvariationwithantibioticprescriptionpractices.
Randomizedclinicaltrialscomparingvariousdosesanddurationsofintravenous
therapywillaidinmakingmorerobustguidelinestoaidemergencyphysicians
whenselectingtheappropriateantibioticroute.
ConclusionThisisthefirststudytoidentifyphysicianrationalefortheuseofintravenous
antibioticsforSSTIs.Therewassignificantvariabilityinantibioticprescribing
practicesbyEDphysicians.ThisprospectivestudydemonstratesthatanED-to-
OPATclinicprogramfornon-purulentSSTIsissafe,hasalowrateoftreatment
failuresandresultsinhighpatientsatisfaction.

94
References1. TiceAD,RehmSJ,DalovisioJR,etal.Practiceguidelinesforoutpatient
parenteralantimicrobialtherapy.IDSAguidelines.ClinInfectDis.2004;38(12):1651-1672.Epub2004May1626.
2. WilsonK,RosenbergMW.AccessibilityandtheCanadianhealthcaresystem:squaringperceptionsandrealities.HealthPolicy.2004;67(2):137-148.
3. McCuskerJ,VadeboncoeurA,LevesqueJF,CiampiA,BelzileE.Increasesinemergencydepartmentoccupancyareassociatedwithadverse30-dayoutcomes.AcadEmergMed.2014;21(10):1092-1100.doi:1010.1111/acem.12480.
4. MurrayH,StiellI,WellsG.Treatmentfailureinemergencydepartmentpatientswithcellulitis.CJEM.2005;7(4):228-234.
5. PetersonD,McLeodS,WoolfreyK,McRaeA.Predictorsoffailureofempiricoutpatientantibiotictherapyinemergencydepartmentpatientswithuncomplicatedcellulitis.AcadEmergMed.2014;21(5):526-531.
6. MayL,HarterK,YadavK,etal.Practicepatternsandmanagementstrategiesforpurulentskinandsoft-tissueinfectionsinanurbanacademicED.AmJEmergMed.2012;30(2):302-310.doi:310.1016/j.ajem.2010.1011.1033.Epub2011Jan1028.
7. MayL,GudgerG,ArmstrongP,etal.Multisiteexplorationofclinicaldecisionmakingforantibioticusebyemergencymedicineprovidersusingquantitativeandqualitativemethods.InfectControlHospEpidemiol.2014;35(9):1114-1125.doi:1110.1086/677637.Epub672014Jul677623.
8. TimbrookTT,CaffreyAR,OvalleA,etal.AssessmentsofOpportunitiestoImproveAntibioticPrescribinginanEmergencyDepartment:APeriodPrevalenceSurvey.InfectDisTher.2017;6(4):497-505.doi:410.1007/s40121-40017-40175-40129.Epub42017Oct40119.
9. KamathRS,SudhakarD,GardnerJG,HemmigeV,SafarH,MusherDM.GuidelinesvsActualManagementofSkinandSoftTissueInfectionsintheEmergencyDepartment.OpenForumInfectDis.2018;5(1):ofx188.doi:110.1093/ofid/ofx1188.eCollection2018Jan.
10. GilchristM,SeatonRA.Outpatientparenteralantimicrobialtherapyandantimicrobialstewardship:challengesandchecklists.JAntimicrobChemother.2015;70(4):965-970.doi:910.1093/jac/dku1517.Epub2014Dec1023.

95
11. Hoffman-TerryML,FraimowHS,FoxTR,SwiftBG,WolfJE.Adverseeffectsofoutpatientparenteralantibiotictherapy.AmJMed.1999;106(1):44-49.
12. HodgsonKA,HuynhJ,IbrahimLF,etal.Theuse,appropriatenessandoutcomesofoutpatientparenteralantimicrobialtherapy.ArchDisChild.2016;101(10):886-893.doi:810.1136/archdischild-2015-309731.Epub302016May309710.
13. PetrakRM,SkorodinNC,FliegelmanRM,HinesDW,ChundiVV,HartingBP.ValueandClinicalImpactofanInfectiousDisease-SupervisedOutpatientParenteralAntibioticTherapyProgram.OpenForumInfectDis.2016;3(4):ofw193.eCollection2016Oct.
14. ChapmanAL,DixonS,AndrewsD,LilliePJ,BazazR,PatchettJD.Clinicalefficacyandcost-effectivenessofoutpatientparenteralantibiotictherapy(OPAT):aUKperspective.JAntimicrobChemother.2009;64(6):1316-1324.doi:1310.1093/jac/dkp1343.Epub2009Sep1319.
15. ZhangJ,MooreE,BousfieldR.OPATforcellulitis:itsbenefitsandthefactorsthatpredisposetolongertreatment.EurJClinMicrobiolInfectDis.2016;35(6):1013-1015.doi:1010.1007/s10096-10016-12631-y.Epub12016Apr10015.
16. AdminstrationFaD.GuidanceforIndustry:AcuteBacterialSkinandSkinStructureInfections:DevelopingDrugsforTreatment.
17. YadavK,GatienM,Corrales-MedinaV,StiellI.Antimicrobialtreatmentdecisionfornon-purulentskinandsofttissueinfectionsintheemergencydepartment.CJEM.2017;19(3):175-180.doi:110.1017/cem.2016.1347.Epub2016Aug1017.
18. VolzKA,CanhamL,KaplanE,SanchezLD,ShapiroNI,GrossmanSA.IdentifyingpatientswithcellulitiswhoarelikelytorequireinpatientadmissionafterastayinanEDobservationunit.AmJEmergMed.2013;31(2):360-364.
19. AminAN,CerceoEA,DeitelzweigSB,PileJC,RosenbergDJ,ShermanBM.Hospitalistperspectiveonthetreatmentofskinandsofttissueinfections.MayoClinProc.2014;89(10):1436-1451.doi:1410.1016/j.mayocp.2014.1404.1018.Epub2014Jun1425.
20. MistryRD,ScottHF,ZaoutisTE,AlpernER.Emergencydepartmenttreatmentfailuresforskininfectionsintheeraofcommunity-acquiredmethicillin-resistantStaphylococcusaureus.PediatrEmergCare.2011;27(1):21-26.doi:10.1097/PEC.1090b1013e318203ca318201c.

96
21. JenkinsTC,KnepperBC,McCollisterBD,etal.Failureofoutpatientantibioticsamongpatientshospitalizedforacutebacterialskininfections:Whatistheclinicalrelevance?AmJEmergMed.2016;34(6):957-962.doi:910.1016/j.ajem.2016.1002.1013.Epub2016Feb1012.
22. PallinDJ,BinderWD,AllenMB,etal.Clinicaltrial:comparativeeffectivenessofcephalexinplustrimethoprim-sulfamethoxazoleversuscephalexinalonefortreatmentofuncomplicatedcellulitis:arandomizedcontrolledtrial.ClinInfectDis.2013;56(12):1754-1762.doi:1710.1093/cid/cit1122.Epub2013Mar1751.
23. ChapmanAL,SeatonRA,CooperMA,etal.Goodpracticerecommendationsforoutpatientparenteralantimicrobialtherapy(OPAT)inadultsintheUK:aconsensusstatement.JAntimicrobChemother.2012;67(5):1053-1062.doi:1010.1093/jac/dks1003.Epub2012Jan1031.
24. SeatonRA,BarrDA.Outpatientparenteralantibiotictherapy:principlesandpractice.EurJInternMed.2013;24(7):617-623.doi:610.1016/j.ejim.2013.1003.1014.Epub2013Apr1018.
25. CorwinP,ToopL,McGeochG,etal.Randomisedcontrolledtrialofintravenousantibiotictreatmentforcellulitisathomecomparedwithhospital.BMJ.2005;330(7483):129.Epub2004Dec2016.

97
FiguresFigure1.FlowDiagram
PatientsScreened(N=214)
ExcludedPatients,total(N=61)Abscess(N=17)Osteomyelitis(N=16)Infectedulcerwithoutcellulitis(N=15)NotdiagnosedwithSSTI(N=10)Givenoralantibiotics(N=1)Previouslyenrolled(N=2)
EligiblePatients(N=153)
AttendedOPATclinic(N=137)(89.5%)
Admittedtohospital(N=5)(3.3%)Losttofollowup(N=11)(7.2%)
14-Daytelephonefollowup(N=118)(86.0%)
Losttofollowup(N=12)(8.8%)Declinedconsent(N=7)(5.2%)

98
TablesTable1.BaselineCharacteristicsofAdultswithNon-PurulentSkinandSoftTissueInfections(SSTIs)seenintheED(N=153)
Variable N=153Age(years),mean± SDRange
Male(%)HospitalSite(%)
TOHCivicCampusTOHGeneralCampus
ComorbiditiesDiabetesmellitusLymphedemaPriorcellulitisinpast12monthsObesityPeripheralvasculardiseaseCoronaryarterydiseaseActivecancerChronickidneydiseaseCongestiveheartfailureLiverdiseaseInjectiondruguseHistoryofMRSAcolonizationorinfectionOrgantransplantrecipient
MedicationsCurrentlytakingoralantibiotics
60±1921–100
82(53.6)
80(52.3)73(47.7)
38(24.8)36(23.5)26(17.0)19(12.4)12(7.8)10(6.5)8(5.2)8(5.2)7(4.6)7(4.6)7(4.6)5(3.3)1(0.6)
74(48.4)
SD=standarddeviation;TOH=TheOttawaHospital;MRSA=methicillinresistantStaphylococcusaureus;IV=intravenous

99
Table2.PresentingPatientandInfectionCharacteristics(N=153)
Variable N=153TriageVitalSignsTemperature,°C(mean±SD)HeartRate,beats/min(mean±SD)BloodPressure,mmHg(mean±SD)RespiratoryRate,breaths/min(mean±SD)OxygenSaturation,%(median,IQR)
InfectionLocation(%)LegFootArmHandFaceTorso
InfectionCharacteristics(%)ChronicLegUlcersBiteSurgicalSiteInfectionInfectiondimensionsrecorded(%)Areaoferythema,cm2(median,IQR)
LaboratoryTestsWhitebloodcellcountordered(%)Whitebloodcellcount,×109/L(median,IQR)
BloodCultureSentNegativeBloodCultureContaminantPositiveBloodCulture
36.5±0.786±17138±2117±2
97,96–98
69(45.1)21(13.7)23(15.0)19(12.4)16(10.5)5(3.3)
20(13.1)11(7.2)4(2.6)
124(81.0)150,40–300
104(68.0)9.0,6.8–11.6
22(14.4)21(13.7)1(0.6)0(0)
SD=standarddeviation;IQR=interquartilerange;TBSA=totalbodysurfacearea

100
Table3.IntravenousAntibioticTreatmentAdministeredWhileintheED(N=153)
AntibioticSelection Numberofpatients,N=153N(%)
IVantibioticsonlyOralandIVantibioticsNumberofIVantibioticsOneTwo
IVantibioticagentandsingledoseCefazolinDose=1000mgDose=2000mg
CeftriaxoneDose=1000mgDose=2000mg
ClindamycinDose=300mgDose=600mgDose=900mg
VancomycinDose=1000mgDose=1500mgDose=2000mg
Piperacillin-Tazobactam(3375mg)Meropenem(1000mg)Ciprofloxacin(400mg)
Oralantibiotics*ClindamycinCiprofloxacinTrimethoprim-Sulfamethoxazole
148(96.7)5(3.3)
143(93.5)10(6.5)
99(64.7)33(21.6)66(43.1)37(24.2)31(20.3)6(3.9)
17(11.1)1(0.6)12(7.8)4(2.6)5(3.3)3(2.0)1(0.6)1(0.6)2(1.3)2(1.3)1(0.6)
2(1.3)2(1.3)1(0.6)
IV=intravenous*Giveninadditiontointravenousantibiotics

101
Table4.IntravenousAntibioticPrescriptionsforPatientsDischargedfromtheED(N=153)
EDIVAntibioticPrescription Numberofpatients,N=153N(%)
CefazolinSingleDose1000mg1500mg2000mg
FrequencyTwicedailyThreetimesdailyFourtimesdaily
Duration,days(median,IQR)Range
CeftriaxoneSingleDose1000mg2000mg
FrequencyOncedailyTwicedaily
Duration,days(median,IQR)Range
ClindamycinSingleDose300mg450mg600mg900mg
FrequencyTwicedailyThreetimesdaily
Duration,days(median,IQR)Range
VancomycinPiperacillin-TazobactamMeropenemCiprofloxacin
101(66.0)
51(33.3)1(0.6)49(32.0)
5(3.3)94(61.4)2(1.3)
7,7–73–14
30(19.6)
25(16.3)5(3.3)
1(0.6)29(19.0)7,7–93–10
16(10.5)
1(0.6)1(0.6)11(7.2)3(2.0)
1(0.6)15(9.8)7,7–75–14
3(2.0)2(1.3)2(1.3)1(0.6)
IQR=interquartilerange(Q1–Q3);Range=min–max;IV=intravenous,ED=emergencydepartment

102
Table5.EmergencyPhysicianRationaleforIVAntibioticsforall153Patients
RationaleforIVAntibiotics* Numberofpatients,N(%)N=153
ClinicalImpressionFailedoralantibiotictherapyDiabetesSeverepain(>8/10)PeripheralvasculardiseaseBitePriorSSTIthatrequiredIVantibioticsSocial/complianceissuesAbnormalskinatinfectionsite**PriororalantibioticfailurePriorSSTIinsameareaHypotensionorfeverandtachycardiaRapidlyspreadingerythemaorlymphangitisIndwellingIVcatheterBlunttraumaEarinvolvementInjectiondruguseImmunocompromised
81(52.9)64(41.8)27(17.6)12(7.8)12(7.8)7(4.6)5(3.3)5(3.3)3(2.0)2(1.3)2(1.3)2(1.3)2(1.3))1(0.6)1(0.6)1(0.6)1(0.6)1(0.6)
*Emergencyphysiciansindicated>1rationaleforsomepatients**Surgicalsiteinfection,underlyingburn,underlyingmelanomaIV=intravenous;SSTI=skinandsofttissueinfection

103
Table6.OutpatientParenteralAntibioticTherapy(OPAT)ClinicData(N=137)
OPATClinicMetric Numberofpatients,N(%)
N=137Cellulitisconfirmedasdiagnosis*AlternatediagnosesAbscessOsteomyelitisDrugrashStasisdermatitis
Timetofollow-up(days),median,IQRRange
Totalclinicvisits,median,IQRTotalDurationofIVantibiotics(days),median,IQRTotalDurationofIVandoralantibiotics(days),median,IQRPatientfollowupat14daysPatientsatisfaction(scaleof1to10**)TimelinessofreferraltoOPATclinicOverallsatisfactionwithcarereceived
PatientpreferenceforfollowupinfutureOPATclinicFamilydoctorEDUnknown(losttofollowup)
128(93.4)
3(2.2)3(2.2)2(1.4)1(0.7)
5,4–71–18
2,1–3
9,7–14
17,12–28
118(86.1)
9,8–1010,9–10
110(80.3)5(3.6)3(2.2)19(13.9)
*Theinfectiousdiseasespecialistagreedwiththeemergencyphysiciandiagnosisofanon-purulentSSTI**1isleastsatisfiedand10ismostsatisfiedOPAT=outpatientparenteralantibiotictherapy;IV=intravenous;IQR=interquartilerange,Q1–Q3

104
Table7.Outcomesat14DaysfromIndexEDVisitfor137PatientsNotLosttoFollow-up
AdverseEvents Numberofpatients,N=137,N(%)
ReasonforReturnEDVisitWithin14DaysRepeatIVantibioticdosesNumberofrepeatvisits,median,IQRRange
ForSSTIanddischargedhomeForSSTIandhospitaladmission(OPATTreatmentFailure)DiagnosedwithabscessrequiringI&DUnrelatedmedicalproblem
AdverseDeviceEventsBlockedperipheralIVlineDislodgedperipheralIVlineThrombophlebitis,lineinfectionorbacteremia
AdverseAntibioticEventsDiarrheaRashOralthrushNauseaand/orvomiting
55(40.1)1,1–21–5
18(13.1)6(4.4)
4(2.9)4(2.9)
15(10.9)9(6.6)6(4.4)0(0)
11(8.0)8(5.8)2(1.4)1(0.7)0(0)
IQR=interquartilerange(Q1–Q3);Range=min–maxED=emergencydepartment;IV=intravenous;SSTI=skinandsofttissueinfection;I&D=incisionanddrainage

105
SupplementaryAppendixFigureS1.OPATClinicReferralForm

106
FigureS2.StandardizedCaseRecordForm
CASE#:____________________ AbstractorLastName:____________________DemographicsHospital: qTOHCivic qTOHGeneralGender: qMale qFemaleDateofbirth:__________/_____/_____(Y/M/D)DateofindexEDvisit:__________/_____/_____(Y/M/D)PastMedicalHistory(qNoneofbelow)qActiveCancer(onchemotherapyorpalliative)qChronickidneydiseaseqChronicvenousinsufficiencyqCongestiveheartfailureqCoronaryarterydiseaseqCorticosteroids(systemic)qDiabetesqHepaticdiseaseqHIVqIntravenousdruguse(IVDU)qLymphedema/VenousStasisqMRSApositiveqObesityqOrgantransplantrecipientqPeripheralvasculardiseaseqPriorcellulitisInfectionCharacteristicsLocationofcellulitis: qArm qLeg qHand qFoot qTorso qGroin qAxilla qFaceChroniculcers: qYes qNoSurgicalsiteinfection: qYes qNoBite(humanoranimal) qYes qNoMaximumlengthoferythema(cm):__________qNotrecordedMaximumwidthoferythema(cm):__________qNotrecordedAreaoferythema(cm2):__________qNotrecorded Areadeterminedby:qDiagram qPhotograph
qText(dimensions) qText(non-specific)PercentTBSAinvolved: q<5% q5–10% q10–20% q>20%

107
TriageVitalSignsTemperature:__________°CHeartrate:__________bpmRespiratoryrate:__________breaths/minuteSystolicBP:__________mmHgSaO2:__________% qRAqSupplementalO2WBCCount:__________(x109/L)BloodCulturessent? oYes oNo IfYes: oPositive oNegative oContaminated IfPositive: oMSSA oMRSA oGroupAStrep oPseudomonas oProteus oStrepPneumoniae oSerratia oEikenella oVibrio oH.influenzae oContaminatedCurrentTreatment(PriortoEDVisit)IspatientcurrentlytakingantibioticsforSSTI? oYes oNo
Ifyes,completethefollowing(checkallthatapply):Antibioticpatientiscurrentlytaking:qPOAmoxicillin-Clavulanate(Clavulin) qPOAmoxicillin qPOTMP-SMX(Septra) qPOCephalexin(Keflex)qPOClindamycin qPOCiprofloxacinqPOPenicillin qPODoxycyclineqIVCeftriaxone qIVCefazolin(Ancef)qIVClindamycin qIVPipercillin-TazobactamqIVVancomycin qIVPenicillin
qIVCiprofloxacin qIVMeropenem qOther:_________________________ Duration(fromstarttoEDvisit;days):____________________

108
EDTreatment(whatwasgivenintheED)Route:
qOralAntibioticsonly? qIVAntibioticsonly? qOralandIVAntibiotics?
NumberofOralAntibiotics: q0 q1 q2 q3NumberofIVAntibiotics: q0 q1 q2 q3OralCephalexin(Keflex)? qYes qNo
IfYes,Dose(mg): q250 q500 q1000OralAmoxicillin-Clavulanate? qYes qNo
IfYes,Dose(mg): q500 q875 OralAmoxicillin? qYes qNo
IfYes,Dose(mg): q250 q500 q1000OralClindamycin? qYes qNo
IfYes,Dose(mg): q300 q450 q600OralTMP-SMX(Septra)? qYes qNo
IfYes,Dose(mg): q800(1DStab) q1600(2DStabs)OralCiprofloxacin? qYes qNo
IfYes,Dose(mg): q250 q500 q1000IVCefazolin(Ancef)? qYes qNo
IfYes,Dose(mg): q500 q1000 q1500q2000IVCeftriaxone? qYes qNo
IfYes,Dose(mg): q1000 q1500 q2000IVClindamycin? qYes qNo
IfYes,Dose(mg): q300 q450 q600q900IVMeropenem? qYes qNo
IfYes,Dose(mg): q500 q1000 q1500q2000IVVancomycin? qYes qNo
IfYes,Dose(mg): q500 q1000 q1500q2000IVPiperacillin-Tazobactam? qYes qNo
IfYes,Dose(mg): q3375 q4500 IVCiprofloxacin? qYes qNo
IfYes,Dose(mg): q200 q400

109
EDPrescription:OralCephalexin(Keflex)? qYes qNo
IfYes,Dose(mg): q250 q500 q1000Frequency: qBID qTID qQID Duration(days):____________________
OralAmoxicillin-Clavulanate? qYes qNo
IfYes,Dose(mg): q500 q875 Frequency: qBID qTID qQID Duration(days):____________________
OralAmoxicillin? qYes qNo
IfYes,Dose(mg): q250 q500 q1000Frequency: qBID qTID qQID Duration(days):____________________
OralClindamycin? qYes qNo
IfYes,Dose(mg): q300 q450 q600Frequency: qBID qTID qQID Duration(days):____________________
OralTMP-SMX(Septra)? qYes qNo
IfYes,Dose(mg): q800(1DStab) q1600(2DStabs)Frequency: qOD qBID qTID Duration(days):____________________
OralCiprofloxacin? qYes qNo
IfYes,Dose(mg): q250 q500 q1000Frequency: qOD qBID qTID Duration(days):____________________
OralDoxycycline? qYes qNo
IfYes,Dose(mg): q100 q200 Frequency: qOD qBID qTID
Duration(days):____________________

110
IVCefazolin(Ancef)? qYes qNoIfYes,Dose(mg): q500 q1000 q1500q2000
Frequency: qBID qTID qQID Duration(days):____________________
IVCeftriaxone? qYes qNo
IfYes,Dose(mg): q1000 q1500 q2000Frequency: qOD qBID Duration(days):___________________
IVClindamycin? qYes qNo
IfYes,Dose(mg): q300 q450 q600q900Frequency: qBID qTID qQID Duration(days):___________________
IVMeropenem? qYes qNo
IfYes,Dose(mg): q500 q1000 q1500q2000Frequency: qBID qTID qQID Duration(days):___________________
IVVancomycin? qYes qNo
IfYes,Dose(mg): q500 q1000 q1500q2000Frequency: qOD qBID qTID Duration(days):___________________
IVPiperacillin-Tazobactam? qYes qNo
IfYes,Dose(mg): q3375 q4500 Frequency: qBID qTID qQID Duration(days):___________________
IVCiprofloxacin? qYes qNo
IfYes,Dose(mg): q200 q400Frequency: qBID qTID qQID Duration(days):___________________

111
ReturntoED(RTED)within14days: oYes oNo Ifyes(chooseONEonly):
oReturntoEDforSSTIandhospitaladmission oReturntoEDforSSTIbutnoadmission oReturntoEDwithabscess(Ifyes,I&Dperformed? oYes oNo) oReturntoEDforrepeatantibiotics:numberofsubsequentvisits_____oReturntoEDforunrelatedmedicalproblem
IfRTED:ChangestotreatmentinEDatrepeatvisit: oYes oNoIfyes(chooseONEonly):oChangefromPOtoIVantibiotics(nameofnewantibiotic:_______________)oChangetodifferentPOantibiotic(nameofnewantibiotic:_______________) oChangetodifferentIVantibiotic(nameofnewantibiotic:_______________)oChangetodifferentantibioticdose(newdose:________________mg)Iftreatmentwasaltered,reasonforchangeintreatmentplan:
oWorseninginfection oNoimprovementoVomiting oDiarrhea oRash/hivesoOther Indicate:_____________________
OralAntibioticTreatmentFailure? qYesqNo Ifyes,reasonfortreatmentfailure(checkallthatapply): qStep-upfromPOtoIVantibiotic qChangeinclassofPOantibiotic(duetoworseninginfection) qInitialoutpatientmanagementwithsubsequenthospitaladmissionOPATTreatmentFailure? qYesqNo
Ifyes(i.e.hospitalizedfrom48hours–2weeks),reasonfortreatmentfailure(checkallthatapply):
qWorseninginfection qDrug-relatedcomplication qLine-relatedcomplicationAdverseEvents: Adversedrugreaction: qYesqNo Ifyes: qRash qNauseaonly(novomiting) qVomiting qDiarrhea qOther:____________________ Adversedeviceevent: qYesqNo Ifyes: qBlockedperipheralIV qDislodgedperipheralIV qLinethrombosis qLineinfection
Subsequenthospitaladmissionat14daysfromindexEDvisit?qYesqNo Ifyes: qForworseningSSTI
qForunrelatedmedicalproblem(specify:_______________)

112
OPATClinic:DidpatientattendOPATappointment? qYesqNo(STOPHERE)Cellulitiswascorrectdiagnosis: qYesqNo IfNO–specifyalternatediagnosis: qDVT qLymphedema qStasisdermatitis qAbscess qHematoma qDrugrash NumberofdaysfrominitialEDvisittofirstOPATappointment:__________TotalnumberofvisitstoOPATclinic:__________TotalnumberofdaysonIVantibiotics:__________TotalnumberofdaysonIVandPOantibiotics:__________IVAntibioticsfor>7d? qYesqNoIVAntibioticsfor>10d? qYesqNoTimetostep-down(days)fromIVtoPOantibiotics:__________
RationaleforIVantibiotics(checkallthatapply):
qFailedoralantibiotictherapy
qHypotension
qSeverepain(>8/10)
qClinicalimpression(severeinfection)
qDiabetes
qPainoutofproportion
qPeripheralvasculardisease
qIndwellingIVcatheter
qBite
qSocial/complianceissues
qOther:______________________________________________________________________Patientagreedtotelephonecall? oYes oNo oLosttofollow-upPatientexpectedtobereferredtoanoutpatientclinicformanagementofinfection?oYes oNoSettingpatientwouldpreferforreceivingfollow-upinthefuture?oOPATclinic oED oFamilydoctorSatisfactionwiththetimelinessofthereferraltotheOPATclinic._____/10OverallsatisfactionwithcareintheOPATclinic:_____/10

113
TableS1.ReasonsforHospitalizationwithin14DaysofEDVisitfor137PatientswhoattendedtheirOPATClinicAppointment
ReasonforHospitalization Numberofpatients,N(%)N=137
WorseninginfectionOthermedicalproblemAcutecoronarysyndromeRenalfailureGoutHipfracture
6(4.4)
4(2.9)1111

114
ChapterFive:Discussion
IntroductionThegoalofthisthesiswastodescribetheepidemiologyofadultswithnon-purulent
SSTIswhopresenttotheED.Additionalgoalswereto:(a)identifypredictors
associatedwithoralantibiotictreatmentfailure;(b)determineemergency
physicianrationaleforselectingintravenoustherapy;and(c)describethe
performanceofanED-to-OPATclinicprogram.Thischapterwillsummarizethe
resultsofthehealthrecordsreview(ChapterThree)andtheprospective
observationalcohortstudy(ChapterFour)inordertohighlightclinical
recommendationsandareasforfutureresearch.
InterpretationofResultsThehealthrecordsreview(ChapterThree)describedtheepidemiologyofadults
withnon-purulentSSTIsseekingcareintheED.Therewasasurprisinglyhigh
hospitaladmissionrate,whichinpartreflectstheneedformorerobustevidence-
basedguidelinestoimprovemanagementofthiscommonclinicalcondition.Many
patientshaddiabetesandcellulitiswithinthepreceding12months.Wedidobserve
alargevariationinselectionoftheantimicrobialagentandroute.Themajorityof
patientsreceivedatleastonedoseofintravenousantibioticintheED.Despitealack
ofevidencetosupportthispractice,manypatientsreceivedasingleintravenous
doseandweresenthomewithanoralantibioticprescription.Theobserved
variabilityintreatmentapproachhighlightsaclearlackofagreementamongst
emergencyphysiciansregardingoptimalantimicrobialtherapyforthiscommon

115
clinicalcondition.Duetothestudydesign,thereasonsbehindselectingintravenous
therapyremainedunclear.
Wefoundanoralantibiotictreatmentfailureratethatwashigherthanexpectedin
thehealthrecordsreviewwhencomparedtopriorstudies.1,2Thesepriorstudies
didnotuseastricttimecutofftodefinetreatmentfailure,whichmayhaveledto
somepatientsbeingmisclassifiedastreatmentfailureorsuccess.Weused
multivariablelogisticregressiontoidentifyfactorsassociatedwithoralantibiotic
treatmentfailure.Adetaileddescriptionofthemethodsusedtodevelopa
multivariablelogisticregressionmodelcanbefoundinAppendixB.Wefirstused
clinicalreasoningtodeterminewhichvariablescouldplausiblypredictoral
antibiotictreatmentfailure.Ultimately,sevenvariableswerechosenforinclusion
intoamultivariablemodel.Fourvariableswerefoundtobeassociatedwiththe
primaryoutcome:tachypneaattriage;chroniculcers;ahistoryofMRSA
colonizationorinfection;andpriorcellulitisinthelast12months.Thisisthefirst
studytoidentifypotentialpredictorsassociatedwithoralantibiotictreatment
failure.
Toaddresstheissuesweidentifiedsurroundingintravenousantibioticuse,we
conductedaprospectiveobservationalcohortstudy(ChapterFour)to:(a)describe
theperformanceofanED-to-OPATclinicmodel;and(b)identifyphysicianrationale
forselectingintravenoustherapy.WefoundlowratesofOPATtreatmentfailure.
Noneoftheadverseperipheralintravenouslineeventsoradverseantibioticevents

116
wasseriousenoughtorequirehospitalization.Thediagnosisofnon-purulentSSTIs
wasconcordantbetweenemergencyphysiciansandinfectiousdiseasespecialistsin
themajorityofcases.Patientsreportedahighdegreeofsatisfactionwithtimeliness
ofreferralandoverallcarereceived.OurfindingssuggestthatanED-to-OPATclinic
modelissafeandacceptabletopatients.
Therewassignificantemergencyphysicianpracticevariationintheprospective
observationalcohortstudy.Themostcommonlyprescribedintravenousantibiotic
wascefazolin;physicianswerealmostevenlysplitregardingthechosendose.The
topfivereasonsforselectingtheintravenousroutewere:clinicalimpression;failed
oralantibiotictherapy;diabetes;severepain;andperipheralvasculardisease.Oral
antibioticfailurewasthesecondmostcommonreasonforselectingtheparenteral
route,whichisinterestinggiventhelackofavalidateddefinitionoftreatment
failure.Thepresenceofcomorbidities(diabetesandperipheralvasculardisease)as
rationaleforintravenoustherapywasnoteworthygiventhatneitherwasfoundto
beassociatedwithoralantibioticfailureinthehealthrecordsreview.
PreviousStudiesThe2014InfectiousDiseaseSocietyofAmericaguidelinesarelargelybasedon
expertopinion,andsuggestintravenousantibioticsfor‘moderate’(signsofsystemic
illness)or‘severe’(failedoraltherapy,signsofsystemicillness,clinicalsignsof
deeperinfection,orimmunocompromised)infections.3TheBritishClinicalResource
EfficiencySupportTeam(CREST)guidelinesrecommendoralantibioticsin‘ClassI’

117
patients,whichisdefinedasalackofsystemicsignsofillnessandtheabsenceof
‘uncontrolledcomorbidities’.4Thelatterwasnotexplicitlydefined.Thereare
currentlynoCanadianguidelinesforthisimportanttopic.Petersonandcoworkers
identifiedpredictorsoftreatmentfailurewithoutpatientantibiotictherapy,butdid
notdistinguishbetweenoralversusintravenousroutes.2Despitethelackof
evidence,arecentnationalsurveyofCanadianemergencyphysiciansfoundthat
94.4%ofrespondentswouldconsideraclinicaldecisionruletopredictoral
antibiotictreatmentfailure.5
TheobservedlowOPATtreatmentfailurerateintheprospectiveobservational
cohortstudywassimilartopreviouslypublishedstudies.6-8Currentguidelineslist
patientsatisfactionasacriticalelementofanOPATprogram.9-11Wefoundahigh
degreeofpatientsatisfactionthatissimilartopreviousstudies.Anadditionalaimof
ourstudywastoanswertheclinicalquestion:whydoemergencyphysiciansselect
theintravenousrouteforantimicrobialtherapy?Wefeltthatthiswasanimportant
clinicalquestion,asappropriatepatientselectionforoutpatientintravenous
therapyisacriticalfirststeptothesuccessofanOPATprogram.9,12Thereareno
previouslypublishedprospectivestudiesthathaveexaminedphysicianrationalefor
selectingtheintravenousroute.

118
StrengthsThehealthrecordsreviewisthefirststudytoidentifypotentialpredictors
associatedwithoralantibiotictreatmentfailurefornon-purulentSSTIs.Weused
strictinclusionandexclusioncriteria,predefinedvariables,astandardizedcase
recordform,andheldregularmeetingsbetweendataabstractorstoresolve
outstandingissuesandtoperformappropriateoversight.Thesespecificstepswere
takeninordertominimizebias,inaccordancewithacceptedmethodologyforchart
reviews.13-16Therewasexcellentagreementamongdataabstractorsforbothstudy
inclusionandtheprimaryoutcome.
Fortheprospectiveobservationalcohortstudy,weenrolledaconsecutivesampleof
patientsandscreenedallOPATclinicreferralstoensurenoeligiblecaseswere
missed.Thedatawerecollectedprospectively,whichallowedustoaccurately
identifyemergencyphysicianrationaleforselectingtheintravenousroute.Thisis
thefirststudytoprovideimportantinsightintophysiciandecision-making
regardingselectionofintravenousantibiotictherapy.
LimitationsThehealthrecordsreviewhasseveralpotentiallimitations.First,wefeltthatthe
sizeofaninfection(areaoferythema)couldbeaclinicallyimportantmarkerof
infectionseverity.However,wesuspectedthatmostemergencyphysiciansmight
notaccuratelydocumentinfectionsizeoromitthisinformation.Inordertomitigate
thisproblemforthehealthrecordsreview,wedevelopedanapriorimethodto
estimateinfectionsizeusingtotalbodysurfaceareaextrapolatedfromaLund-

119
Browderburndiagram.17,18Giventhelimitationsofthestudydesign,thisprovided
thebestestimateofinfectionsize.Second,obesityasacomorbiditymayhavenot
beenconsistentlydocumentedinthechart.Toaddressthisissue,wereviewed
electronichealthrecordsinthesixmonthspriortoandaftertheindexEDvisitto
determineifobesitywasdocumentedelsewhere.
Third,thedataabstractorswerenotblindedtotheprimaryoutcomeoforal
antibiotictreatmentfailure.However,weusedadefinitionoforalantibiotic
treatmentfailurethatincorporatedaclearminimumof48hoursoforaltherapy
beforeapatientcouldbeconsideredapossibletreatmentfailure.Therewasalso
excellentinterobserveragreementfortheprimaryoutcome.Therefore,wefeelthe
lackofblindingofthestudyabstractorswouldnothaveintroducedsignificantbias.
Afourthpotentiallimitationofthehealthrecordsreviewwasoverfittingofdata
duetothenumberofvariablesconsideredaspossiblepredictorsoforalantibiotic
treatmentfailure.Weinitiallyinvestigated18variablesusingunivariateanalysis
andidentifiedsevenvariablesthatwereassociatedwiththeprimaryoutcome.
Thesesevenvariableswerethenenteredintoamultivariablemodel.However,this
wasahealthrecordsreviewintendedtohelpidentifypotentialpredictors.Basedon
theresultsofthehealthrecordsreview,weintendtoassessasmallernumberof
variablesinafutureprospectivecohortstudy.

120
Alimitationofbothstudies(healthrecordsreviewandprospectiveobservational
cohortstudy)isthelackofavalidateddefinitionfororalorintravenousantibiotic
treatmentfailure.Wefirstreviewedtheliterature1,2,5,19-24andthendeveloped
treatmentfailuredefinitionsafterdiscussionamonglocalexpertsinemergency
medicineandinfectiousdisease.
Fortheprospectiveobservationalcohortstudy,thereareadditionallimitationsthat
deservemention.First,thesamplesizewaslimitedduetofeasibility.Second,some
patientsdidnotattendtheirclinicappointment.Itispossiblethatsomeofthese
patientslosttofollow-upexperiencedatreatmentfailureandsoughtcareat
anotherhospital.However,wefeelitwouldbeunlikelyforpatientstovisita
hospitaldifferentfromthecentrethatinitiatedtheircareforaninfection.Third,it
wasnotfeasibletoaccuratelyweighpatientstodeterminebodymassindexand
degreeofobesity.Whileitispossiblethattheobservedvariationinantibioticdosing
maybeinpartduetopatientbodyhabitus,thiswouldbeaminorissueasonlya
smallpercentageofpatientswererecordedasobeseinthisstudycohort.
ClinicalImplicationsTheresultsfromthehealthrecordsreviewhighlightimportantclinicalimplications
giventhepracticevariationwithrespecttoantibioticagent,dose,frequencyand
route.Inaddition,wefoundanunexpectedlyhighhospitaladmissionrateandoral
antibiotictreatmentfailurerate.Thesefindingsarelikelyduetoalackofevidence-
basedrecommendationstoguidecliniciansonoptimaltreatmentofthiscommon

121
clinicalcondition.Weidentifiedriskfactorsassociatedwithoralantibiotic
treatmentfailure.Thesefactorsshouldbeconsideredbyemergencyphysicians
whendecidingontheoralversusintravenousrouteofantibiotictherapy;thismay
inturndecreaseoveruseofmoreinvasiveandcostlyintravenoustreatment.
Theprospectiveobservationalcohortstudyalsoidentifiedalackofconsensus
regardingantibioticprescribingpracticesamongemergencyphysicians.Itisthe
firststudytoidentifyemergencyphysicianrationaleforselectingintravenous
therapyfornon-purulentSSTIs.Thisisanimportantfirststeptobetterunderstand
physiciandecision-makingwhenselectingtheintravenousroute.TherateofOPAT
treatmentfailurewaslow,andnoneoftheadverseantibioticeventsoradverse
peripheralintravenouslineeventsrequiredhospitalization.AnED-to-OPATclinic
modelwasfoundtobeeffective,safeandresultsinahighdegreeofpatient
satisfaction.Thismodelmaybeintroducedinothercommunitiestopotentially
reducehospitaladmissionsandoverallhealthcarecosts.
Tosummarize,basedonthetwostudiesconducted,wecanmakethefollowing
clinicalrecommendations:
1. Emergencyphysiciansshouldconsidercertainfactors(tachypnea,chronic
legulcers,ahistoryofMRSAcolonizationorinfection,andpriorcellulitisin
thepast12months)whendecidingonintravenous(overoral)antibiotic
therapyfornon-purulentSSTIs.

122
2. AnED-to-OPATclinicmodelissafeandresultsinahighdegreeofpatient
satisfaction.Thismodelmaybeimplementedinothercommunitiestohelp
reducehospitaladmissionsandoverallhealthcarecosts.
ResearchImplicationsThefindingsfromthisthesisprojecthavehighlightedimportantissuesthatweaim
toaddressinfuturestudies:
1. Developandvalidatearobustdefinitionfororalandintravenousantibiotic
treatmentfailureusingtheDelphimethod.Thesedefinitionsmaybeusedin
futurestudiesonthistopic.
2. Conductaprospectiveobservationalcohortstudytoderiveamodelto
identifyfactorsassociatedwithoralantibiotictreatmentfailure.Wewill
selectafewernumberofpotentialpredictorvariablesaprioribasedonthe
resultsofthisthesisproject.Thismodelwillthenbevalidatedinaseparate
EDpopulation.
3. Designandimplementapilotrandomizedcontrolledtrialcomparingoral
versusintravenousantibioticsinthetreatmentofadultpatientswithnon-
purulentSSTIs.
PriorED-basedstudieshaveuseddifferenttreatmentfailuredefinitionsasthe
primaryoutcome.1,2,22Futurestudieswouldbemoreimpactfulbyincorporatinga
uniformandrobusttreatmentfailuredefinition.WeplantousetheDelphimethod
todevelopandvalidatedefinitionsoforalandintravenousantibiotictreatment

123
failure.TheDelphimethodisasystematicapproachthathasbeenusedtodevelop
clinicaldefinitions25andguidelines26basedonexpertopinion.Consensuswillbe
definedapriorias≥75%,whichisthemostcommonthresholdusedinpriorDelphi
studies.27Relevantstakeholderswillincludeemergencyphysicians,infectious
specialists,pharmacistsandpatients.TheDelphiprocesswillbeconductedin
sequentialroundsuntilconsensushasbeenachieved.Structureddefinitionsfororal
andintravenousantibiotictreatmentfailureforSSTIsmaybeutilizedinfuture
studies.
ChapterThreeidentifiedpossiblepredictorsassociatedwithoralantibiotic
treatmentfailure.Weplantoconductaprospectiveobservationalcohortstudyto
identifypredictorsassociatedwithoralantibiotictreatmentfailure.Theresearch
teamwillrecordinfectionsizeandbodymassindex(measureofobesity)foreligible
patients,andbothvariableswillbeassessedaspotentialpredictorsoftreatment
failure.InChapterFour,severalphysicianrationalesforselectingtheintravenous
routewereidentified,includingdiabetesandperipheralvasculardisease.Forour
plannedprospectivecohortstudy,afewernumberofpredictorvariableswillbe
selectedbasedontheresultsofthehealthrecordsreview(ChapterThree),
prospectiveobservationalcohortstudy(ChapterFour)andexpertopinionfrom
emergencyphysicianandinfectiousdiseasespecialists.Fortheprimaryoutcome,
wewillusethedefinitionoforalantibiotictreatmentfailuredevelopedfromour
plannedDelphistudy.Thisstudywillmoreaccuratelyidentifywhichfactorspredict
oralantibiotictreatmentfailure,andmayhelpemergencyphysiciansdecidewhich

124
patientsrequireintravenousversusoralantimicrobialtherapy.Thismayhelplimit
overuseofintravenousantibioticsandlowerratesofadverseeventsandoverall
healthcarecosts.
Ultimately,weaimtoconductafuturerandomizedcontrolledtrialcomparingoral
versusintravenousantibiotictherapyfornon-purulentSSTIs.Beforeconducting
suchalarge-scalestudy,weintendtodesignandimplementapilotrandomized
controltrialtoassessfeasibility.EligibleadultEDpatientswithnon-purulentSSTIs
wouldberandomizedtoreceiveeitheroralcephalexinorintravenouscefazolin,and
theprimaryoutcomewouldbeoralorintravenousantibiotictreatmentfailure.
ConclusionsThisthesisprojecthasaccomplishedspecificgoalsregardingnon-purulentSSTIs
thataremanagedintheED.Ourfirststudy(healthrecordsreview)describesthe
managementofallpatientswithnon-purulentSSTIspresentingtotheED.Thestudy
findingshighlighttheheterogeneityinantimicrobialtreatmentrouteandagent.
Furthermore,weobservedbothanunexpectedlyhighhospitaladmissionrateand
oralantibiotictreatmentfailurerate.Ultimately,wewereabletodevelopa
multivariablelogisticregressionmodeloffactorsassociatedwithoralantibiotic
treatmentfailure.Oursecondstudy(prospectiveobservationalcohortstudy)
showedthatanED-to-OPATclinicmodelisbothsafeandresultsinhighpatient
satisfaction.Wealsoidentifiedphysicianrationalesforselectingtheintravenous
route.

125
Theresultshavehighlightedkeyareasinwhichfuturestudiesarerequiredtobetter
informemergencyphysiciansregarding:(a)optimaltherapyofthiscommonclinical
condition;and(b)appropriatepatientselectionforoutpatientintravenoustherapy.
Boththeidentifiedfactorsassociatedwithoralantibioticfailureandemergency
physicianrationalesforintravenoustherapydeservefuturestudy.Morerobust
evidenceregardingwhichfactorstrulypredictoralantibioticfailurewouldhelp
emergencyphysiciansmoreappropriatelyselectpatientsforintravenoustherapy
andreducetheincidenceoftreatmentfailure.Weareoptimisticthatthiswillinturn
resultinbetterpatientcare,animportantimprovementintheappropriateuseof
intravenousantibiotictherapy,andareductioninhealthcarecosts.

126
References1. MurrayH,StiellI,WellsG.Treatmentfailureinemergencydepartment
patientswithcellulitis.CJEM.2005;7(4):228-234.
2. PetersonD,McLeodS,WoolfreyK,McRaeA.Predictorsoffailureofempiricoutpatientantibiotictherapyinemergencydepartmentpatientswithuncomplicatedcellulitis.AcadEmergMed.2014;21(5):526-531.
3. StevensDL,BisnoAL,ChambersHF,etal.Practiceguidelinesforthediagnosisandmanagementofskinandsofttissueinfections:2014updatebytheInfectiousDiseasesSocietyofAmerica.ClinInfectDis.2014;59(2):e10-52.doi:10.1093/cid/ciu1444.
4. ClinicalResourceEfficiencySupportTeam(2005)Guidelinesonthemanagementofcellulitisinadults.CREST,Belfast..
5. YadavK,GatienM,Corrales-MedinaV,StiellI.Antimicrobialtreatmentdecisionfornon-purulentskinandsofttissueinfectionsintheemergencydepartment.CJEM.2017;19(3):175-180.doi:110.1017/cem.2016.1347.Epub2016Aug1017.
6. Hoffman-TerryML,FraimowHS,FoxTR,SwiftBG,WolfJE.Adverseeffectsofoutpatientparenteralantibiotictherapy.AmJMed.1999;106(1):44-49.
7. PetrakRM,SkorodinNC,FliegelmanRM,HinesDW,ChundiVV,HartingBP.ValueandClinicalImpactofanInfectiousDisease-SupervisedOutpatientParenteralAntibioticTherapyProgram.OpenForumInfectDis.2016;3(4):ofw193.eCollection2016Oct.
8. ChapmanAL,DixonS,AndrewsD,LilliePJ,BazazR,PatchettJD.Clinicalefficacyandcost-effectivenessofoutpatientparenteralantibiotictherapy(OPAT):aUKperspective.JAntimicrobChemother.2009;64(6):1316-1324.doi:1310.1093/jac/dkp1343.Epub2009Sep1319.
9. TiceAD,RehmSJ,DalovisioJR,etal.Practiceguidelinesforoutpatientparenteralantimicrobialtherapy.IDSAguidelines.ClinInfectDis.2004;38(12):1651-1672.Epub2004May1626.
10. ChapmanAL,SeatonRA,CooperMA,etal.Goodpracticerecommendationsforoutpatientparenteralantimicrobialtherapy(OPAT)inadultsintheUK:aconsensusstatement.JAntimicrobChemother.2012;67(5):1053-1062.doi:1010.1093/jac/dks1003.Epub2012Jan1031.
11. SeatonRA,BarrDA.Outpatientparenteralantibiotictherapy:principlesandpractice.EurJInternMed.2013;24(7):617-623.doi:610.1016/j.ejim.2013.1003.1014.Epub2013Apr1018.

127
12. GilchristM,SeatonRA.Outpatientparenteralantimicrobialtherapyandantimicrobialstewardship:challengesandchecklists.JAntimicrobChemother.2015;70(4):965-970.doi:910.1093/jac/dku1517.Epub2014Dec1023.
13. GilbertEH,LowensteinSR,Koziol-McLainJ,BartaDC,SteinerJ.Chartreviewsinemergencymedicineresearch:Wherearethemethods?AnnEmergMed.1996;27(3):305-308.
14. BadcockD,KellyAM,KerrD,ReadeT.Thequalityofmedicalrecordreviewstudiesintheinternationalemergencymedicineliterature.AnnEmergMed.2005;45(4):444-447.
15. LowensteinSR.Medicalrecordreviewsinemergencymedicine:theblessingandthecurse.AnnEmergMed.2005;45(4):452-455.
16. KajiAH,SchrigerD,GreenS.Lookingthroughtheretrospectoscope:reducingbiasinemergencymedicinechartreviewstudies.AnnEmergMed.2014;64(3):292-298.doi:210.1016/j.annemergmed.2014.1003.1025.Epub2014Apr1018.
17. HettiaratchyS,DziewulskiP.ABCofburns:pathophysiologyandtypesofburns.BMJ.2004;328(7453):1427-1429.
18. WachtelTL,BerryCC,WachtelEE,FrankHA.Theinter-raterreliabilityofestimatingthesizeofburnsfromvariousburnareachartdrawings.Burns.2000;26(2):156-170.
19. AdminstrationFaD.GuidanceforIndustry:AcuteBacterialSkinandSkinStructureInfections:DevelopingDrugsforTreatment.
20. VolzKA,CanhamL,KaplanE,SanchezLD,ShapiroNI,GrossmanSA.IdentifyingpatientswithcellulitiswhoarelikelytorequireinpatientadmissionafterastayinanEDobservationunit.AmJEmergMed.2013;31(2):360-364.
21. AminAN,CerceoEA,DeitelzweigSB,PileJC,RosenbergDJ,ShermanBM.Hospitalistperspectiveonthetreatmentofskinandsofttissueinfections.MayoClinProc.2014;89(10):1436-1451.doi:1410.1016/j.mayocp.2014.1404.1018.Epub2014Jun1425.
22. MistryRD,ScottHF,ZaoutisTE,AlpernER.Emergencydepartmenttreatmentfailuresforskininfectionsintheeraofcommunity-acquiredmethicillin-resistantStaphylococcusaureus.PediatrEmergCare.2011;27(1):21-26.doi:10.1097/PEC.1090b1013e318203ca318201c.

128
23. JenkinsTC,KnepperBC,McCollisterBD,etal.Failureofoutpatientantibioticsamongpatientshospitalizedforacutebacterialskininfections:Whatistheclinicalrelevance?AmJEmergMed.2016;34(6):957-962.doi:910.1016/j.ajem.2016.1002.1013.Epub2016Feb1012.
24. PallinDJ,BinderWD,AllenMB,etal.Clinicaltrial:comparativeeffectivenessofcephalexinplustrimethoprim-sulfamethoxazoleversuscephalexinalonefortreatmentofuncomplicatedcellulitis:arandomizedcontrolledtrial.ClinInfectDis.2013;56(12):1754-1762.doi:1710.1093/cid/cit1122.Epub2013Mar1751.
25. Shankar-HariM,PhillipsGS,LevyML,etal.DevelopingaNewDefinitionandAssessingNewClinicalCriteriaforSepticShock:FortheThirdInternationalConsensusDefinitionsforSepsisandSepticShock(Sepsis-3).JAMA.2016;315(8):775-787.doi:710.1001/jama.2016.0289.
26. SunBC,ThiruganasambandamoorthyV,CruzJD.Standardizedreportingguidelinesforemergencydepartmentsyncoperisk-stratificationresearch.AcadEmergMed.2012;19(6):694-702.doi:610.1111/j.1553-2712.2012.01375.x.
27. DiamondIR,GrantRC,FeldmanBM,etal.Definingconsensus:asystematicreviewrecommendsmethodologiccriteriaforreportingofDelphistudies.JClinEpidemiol.2014;67(4):401-409.doi:410.1016/j.jclinepi.2013.1012.1002.

129
AppendixA:OttawaHealthScienceNetworkResearchEthicsBoardApprovalLetter

130
AppendixB:MethodsforDevelopingaMultivariableLogisticRegressionModelforPredictorsofOralAntibioticTreatment
Failure
IntroductionWeconductedahealthrecordsreviewof500adultemergencydepartment(ED)
patientswithnon-purulentskinandsofttissueinfections(SSTIs).Ouraimwasto
identifypredictorsassociatedwiththeprimaryoutcomeoforalantibiotictreatment
failure.Ofthetotalcohortof500patients,288patientsweretreatedwithoral
antibioticsand85patientsexperiencedanoralantibiotictreatmentfailure.
ExploratoryAnalysisTableB1summarizesthecharacteristicsofthe288patientstreatedwithoral
antibioticsbasedonwhetherornottheyexperiencedatreatmentfailure.For
continuousvariables,weplottedhistogramstoassessthedistributionofthe
variables.Age,systolicbloodpressure,heartrateandtemperaturewere
approximatelynormallydistributed.Respiratoryrate,oxygensaturation,white
bloodcellcountandareaoferythemawerenon-normallydistributed.Comparing
thepatientswhodidanddidnotexperienceanoralantibiotictreatmentfailure,
categoricalvariableswereassessedusingthechi-squareorFisher’sexacttest,and
continuousvariableswereassessedusingt-testsfornormallydistributedvariables
andWilcoxontestsfornon-normallydistributedvariables.

131
OutliersTherewasasingleoutlierforeachofthefollowingvariables:whitebloodcellcount
(75×109/L),respiratoryrate(40breaths/minute)andoxygensaturation(82%).
Thepatientwithahighwhitebloodcellcounthadleukemia.Noneoftheseoutliers
arephysiologicallyimpossible,andsothesewerenotremoved.
MissingDataThevariableareaoferythemawasmissingin88.2%ofcases.Becausewefeltthat
infectionsizemaybeapotentiallyimportantpredictorfortheprimaryoutcome,we
estimatedthepercenttotalbodysurfaceareaforallcasesusingaLund-Browder
burndiagram.1,2Whitebloodcellcountwasmissingin24.4%ofcases.Allremaining
continuousvariableshadlessthan4%missingdata.
ExcludingVariablesThevariableareaoferythemawasexcludedbecauseofasignificantproportionof
missingdata.Thevariableswhitebloodcellcountandoxygensaturationwere
excludedbecausewedetermineditdidnotmakeclinicalsensethateithervariable
wouldbeassociatedwithtreatmentfailure.Fourvariableshadasparsedistribution
(i.e.lowfrequency(<1%)cellsoncrosstabsofthevariablesbyoralantibiotic
treatmentfailure):bite,HIV,injectiondruguseandorgantransplantrecipient;we
removedthesevariablesforconsiderationaspotentialpredictorsinourmodel.
Thuswewereleftwith18variables(5continuous,13categorical)thatwefeltcould
plausiblybeassociatedwithoralantibiotictreatmentfailure.

132
TableB1.UnivariateAssociationofCharacteristicswithTreatmentFailureoftheStudyParticipants(N=288)
Variable(N)
OralTreatmentFailure
Frequency,n(%)(N=85)
NoOralTreatmentFailureFrequency,n(%)
(N=203)
PValue*
Male(158) 48(56.5) 110(54.2) 0.72Chroniculcers(20) 13(15.3) 7(3.4) 0.0003Surgicalsiteinfection(20) 7(8.2) 13(6.4) 0.58Bite(8) 1(1.2) 7(3.4) 0.44>5%TBSA(39) 14(16.5) 25(12.3) 0.35Coronaryarterydisease(29) 12(14.1) 17(8.4) 0.14Congestiveheartfailure(18) 8(9.4) 10(4.9) 0.15Chronickidneydisease(15) 8(9.4) 7(3.4) 0.04Chronicvenousinsufficiency(8)
1(1.2) 7(3.4) 0.44
Diabetesmellitus(55) 23(27.1) 32(15.8) 0.03Liverdisease(17) 5(5.9) 5(5.9) 0.99HIV(2) 2(2.4) 0(0) 0.09Injectiondruguse(IVDU)(4) 3(3.5) 1(0.5) 0.08Lymphedema(14) 5(5.9) 9(4.4) 0.56HistoryofMRSAcolonizationorinfection(16)
11(12.9) 5(2.5) 0.001
Obesity(8) 3(3.5) 5(2.5) 0.69Priorcellulitisinpast12months(38)
19(22.4) 19(9.4) 0.003
Peripheralvasculardisease(17)
5(5.9) 12(5.9) 0.99
Age(mean±SD) 67.1±19.0 63.3±20.3 0.15Systolicbloodpressure(mean±SD)
140±22 138±24 0.69
Heartrate(mean±SD) 84±17 83±16 0.68Temperature(mean±SD) 36.6±0.8 36.3±0.7 0.01Respiratoryrate(median,IQR)
18(16–18) 16(16–18) 0.85
SaO2(median,IQR) 97(96–98) 97(96–98) 0.11WBCcount(median,IQR) 8.6(7.0–12.1) 8.2(6.4–11.1) 0.21TBSA=totalbodysurfacearea;HIV=humanimmunodeficiencyvirus;SaO2=oxygensaturation;WBC=whitebloodcell;SD=standarddeviation;IQR=interquartilerange(Q1–Q3)

133
AssociationsbetweencategoricalvariablesWeconsideredseveralcategoricalvariableswhereitwasclinicallyplausiblethat
theymaybecollinear.TableB2showsthedegreeofcollinearitybetweenthe
categoricalvariablesusingthePhicoefficient.3
TableB2.AssessmentofSimpleCollinearityBetweenCategoricalVariablesUsingthePhiCoefficient
Gender ChronicUlcers
%TBSA
DM Lymphedema MRSA Obesity PriorSSTI
PVD
Gender 0.05 -0.02 0.07 -0.13 0.0001
0.03 0.005 -0.005
ChronicUlcers
0.05 0.05 0.13 0.08 0.12 0.08 0.17 0.24
%TBSA -0.02 0.05 DM -0.07 0.13 0.16 0.05 0.12 0.15 0.12 0.22Lymphedema -0.13 0.08 0.17 0.05 0.005 0.15 0.11 0.01MRSA 0.0001 0.12 0.04 0.12 0.005 0.05 0.16 -0.01Obesity 0.03 0.08 -0.008 0.15 0.15 0.05 0.15 -0.005PriorSSTI 0.005 0.17 0.12 0.12 0.11 0.16 0.15 -0.02PVD -0.005 0.24 0.11 0.22 0.01 -0.01 -0.005 -0.02 DM=diabetesmellitus;TBSA=totalbodysurfacearea;MRSA=priormethicillinresistantStaphylococcusaureus(MRSA)colonizationorinfection;PriorSSTI=cellulitiswithinthepast12months;PVD=peripheralvasculardisease
InterpretationofthePhicoefficientwasasfollows:strongpositiveassociation(0.7
to1.0);weakpositiveassociation(0.3to0.7);littleornoassociation(-0.3to0.3);
weaknegativeassociation(-0.7to-0.3);andstrongnegativeassociation(-1.0to-
0.7).Therewerenostrongpositiveornegativeassociations.Becausetherewasno
highdegreeofcollinearity,wedidnotneedtoconsiderexclusionofanyofthe
categoricalvariablesinTableB2.
CorrelationbetweencontinuousvariablesInTableB3thecorrelationbetweencontinuousvariablesusingthePearson
correlationcoefficient(r)areprovided.ThesamerangesforthePhicoefficientwere

134
usedtointerpretthePearsoncorrelationcoefficients.Therewerenostrongpositive
ornegativelinearassociationsbetweenthecontinuousvariables,asnoneofthe
Pearsoncorrelationcoefficientsapproached+1or-1.
TableB3.CorrelationBetweenContinuousVariablesUsingPearsonCorrelationCoefficient(r)
Pearsonrcoefficient
Age SBP HR Temp RR SaO2
Age 1 0.12 -0.23 -0.001 0.07 -0.24SBP 0.12 1 -0.07 -0.05 -0.04 -0.01HR -0.23 -0.07 1 0.25 0.20 0.03Temp -0.008 -0.05 0.25 1 0.28 -0.08RR 0.07 -0.04 0.19 0.28 1 -0.08SaO2 -0.24 -0.01 0.03 -0.08 -0.09 1SBP=systolicbloodpressure;HR=heartrate;Temp=temperature;RR=respiratoryrate;SaO2=oxygensaturation
LogisticRegressionAnalysis
UnivariateAnalysisFollowingtheexploratoryanalysis,therewere18variables(5continuousand13
categorical)thatwefeltmeritedconsiderationaspotentialpredictorsbasedon
clinicalsensibility.
Forthe5continuousvariables,weconsideredclinicallymeaningfulcutoffsand
performedunivariatelogisticregression.Inaddition,wedidexplorearangeof
cutoffstodetermineiftherewereanytrends.Wedeterminedage≥65yearstobe
themostclinicallyrelevant,whichisthedefinitionemployedbythemostrecent
geriatricEDguidelines.4Forthetriagevitalsigns,thefollowingcutoffswere
selected:systolicbloodpressure<90mmHg(clinicallyrelevanthypotension);heart

135
rate≥100beatsperminute(clinicaldefinitionoftachycardia);respiratoryrate>20
breathsperminute(clinicaldefinitionoftachypnea);andtemperature≥38.0°C
(clinicaldefinitionoffever).Theunivariatelogisticregressionanalysisofthe
continuousvariablesatprespecifiedcutoffsaresummarizedinTablesB4–B8.
Thesecutoffswereselectedbasedonstandarddefinitionsandclinicalreasoning
andareshownwithvariousothercutoffstoshowanypotentialtrends.
TableB4.UnivariateLogisticRegressionforAgeasaPredictorofOralAntibioticTreatmentFailure
PredictorVariable
Estimate PValue OR 95%CI
Age≥50 0.40 0.21 1.49 0.80–2.75Age≥55 0.38 0.20 1.46 0.82–2.62Age≥60 0.35 0.21 1.42 0.82–2.43Age≥65* 0.21 0.42 1.24 0.74–2.06Age≥70 0.02 0.95 1.01 0.61–1.69Age≥75 0.15 0.57 1.16 0.69–1.95Age≥80 0.22 0.44 1.25 0.71–2.18Age≥85 0.25 0.44 1.29 0.67–2.46
*SelectedasthemostclinicallyrelevantcutoffOR=oddsratio;CI=confidenceintervalTableB5.UnivariateLogisticRegressionforSystolicBloodPressureasaPredictorofOralAntibioticTreatmentFailure
PredictorVariable
Estimate PValue OR 95%CI
SBP<85 0.90 0.53 2.45 0.15–39.64SBP<90* 0.90 0.52 2.45 0.15–39.64SBP<100 0.04 0.95 1.04 0.26–4.14SBP<110 -0.36 0.49 0.70 0.25–1.96
*SelectedasthemostclinicallyrelevantcutoffSBP=systolicbloodpressure;OR=oddsratio;CI=confidenceinterval

136
TableB6.UnivariateLogisticRegressionforHeartRateasaPredictorofOralAntibioticTreatmentFailure
PredictorVariable
Estimate PValue OR 95%CI
HR≥90 -0.14 0.61 0.87 0.50–1.50HR≥100* 0.33 0.35 1.39 0.70–2.77HR≥110 0.59 0.22 1.80 0.70–4.66HR≥120 0.90 0.16 2.46 0.69–8.74
*SelectedasthemostclinicallyrelevantcutoffHR=heartrate;OR=oddsratio;CI=confidenceintervalTableB7.UnivariateLogisticRegressionforTemperatureasaPredictorofOralAntibioticTreatmentFailure
PredictorVariable
Estimate PValue OR 95%CI
T≥38.0* 1.14 0.09 3.13 0.82–11.98T≥38.5 2.01 0.08 7.44 0.76–72.6
*SelectedasthemostclinicallyrelevantcutoffT=temperature;OR=oddsratio;CI=confidenceintervalTableB8.UnivariateLogisticRegressionforRespiratoryRateasaPredictorofOralAntibioticTreatmentFailure
PredictorVariable
Estimate PValue OR 95%CI
RR≥20 0.14 0.70 1.15 0.57–2.30RR>20* 1.78 0.004 5.95 1.78–19.91RR≥22 1.78 0.004 5.95 1.78–19.91RR≥24 3.05 0.004 21.19 2.60–172.3
*SelectedasthemostclinicallyrelevantcutoffRR=respiratoryrate;OR=oddsratio;CI=confidenceintervalAtourchosencutoffof65years,agewasnotassociatedwithoralantibiotic
treatmentfailure.ThesamewastrueforavarietyofothercutoffsasshowninTable
4.Hypotensionandtachycardiawerealsonotassociatedwiththeprimaryoutcome
(TablesB5andB6).However,feverandtachypneawereassociatedwiththe

137
primaryoutcome(TablesB7andB8),andthesevariableswereselectedforthe
multivariablemodel.
TableB9showstheunivariatelogisticregressionfor13categoricalvariables.We
foundfivevariablesthatwereassociatedwiththeprimaryoutcome(p-value≤0.10):
chroniculcers;chronickidneydisease;diabetesmellitus;ahistoryofMRSA
colonizationorinfection;andpriorcellulitisinthepast12months.
TableB9.SimpleUnivariateLogisticRegressionforCategoricalVariables
PredictorVariable Estimate PValue OR 95%CIMale 0.09 0.72 1.10 0.66–1.83
ChronicUlcers 1.62 0.0009 5.06 1.94–13.17Surgicalsiteinfection 0.27 0.58 1.31 0.50–3.41
TBSA>5% 0.34 0.35 1.40 0.69–2.86Coronaryarterydisease 0.59 0.14 1.80 0.82–3.95Congestiveheartfailure 0.70 0.16 2.01 0.76–5.27Chronickidneydisease 1.07 0.04 2.91 1.02–8.30Diabetesmellitus 0.68 0.03 1.98 1.08–3.65Lymphedema 0.30 0.60 1.35 0.44–4.14
HistoryofMRSAcolonizationorinfection
1.77 0.001 5.89 1.98–17.51
Obesity 0.37 0.62 1.45 0.34–6.20Priorcellulitisinlast
12months1.02 0.004 2.79 1.39–5.59
Peripheralvasculardisease -0.005 0.99 0.99 0.34–2.92TBSA=totalbodysurfacearea;MRSA=methicillinresistantStaphylococcusaureus;OR=oddsratio;CI=confidenceinterval
Insummary,followinganexploratoryanalysisandunivariatelogisticregression
analysis,weidentifiedsevenvariableswithap-value≤0.10thatwechosetoinclude
inamultivariablelogisticregressionmodel:

138
1. Fever(temperature≥38.0°C)
2. Tachypnea(respiratoryrate>20breaths/minute)
3. Chroniculcers
4. Chronickidneydisease
5. Diabetesmellitus
6. PastMRSAcolonizationorinfection
7. Priorcellulitisinthepast12months
Giventhattherewere85identifiedcasesoforalantibiotictreatmentfailure,testing
7variableswouldsatisfytheruleof10.5-7
AssessingforInteractionWhereitseemedclinicallyplausible,weassessedforpossibleinteractionbetween
thesevenpotentialpredictorvariables.Investigationforpotentialinteractionterms
issummarizedinTableB10.Noneoftheinteractiontermswassignificant(defined
asp≤0.05),andsonointeractiontermswerebroughtintoamultivariablemodel.
TableB10.AssessmentofPossibleInteractionTerms
PredictorVariable Estimate PValueDiabetes*CKD -0.26 0.82
ChronicUlcers*Diabetes 13.60 0.99ChronicUlcers*PVD 1.32 0.37
ChronicUlcers*Lymphedema 0.06 0.96Priorcellulitis*MRSAhistory 0.36 0.79Priorcellulitis*Lymphedema -1.86 0.17
Priorcellulitis*PVD 15.13 0.99Priorcellulitis*Diabetes -1.57 0.08
Fever*Tachypnea 13.66 0.99CKD=chronickidneydisease;PVD=peripheralvasculardisease;MRSA=methicillinresistantStaphylococcusaureus;PVD=peripheralvasculardisease

139
MultivariableLogisticRegression:PreliminaryModelWeperformedmultivariablelogisticregressionincludingsevenpotentialpredictor
variableswithp≤0.10intheunivariateanalysis.TableB11showsthepreliminary
model.
TableB11.MultivariableLogisticRegressionModelofPredictorsAssociatedwithOralAntibioticTreatmentFailure(N=288)
PredictorVariable Estimate PValue AdjustedOR 95%CITachypnea(RR>20) 1.64 0.01 5.15 1.41–18.86Chroniculcers 1.57 0.004 4.80 1.64–14.04HistoryofMRSA
colonizationorinfection1.56 0.008 4.78 1.49–15.31
Priorcellulitisinlast12months
0.76 0.06 2.14 0.96–4.74
Chronickidneydisease 1.08 0.08 2.94 0.89–9.70Diabetesmellitus 0.53 0.13 1.70 0.86–3.63Fever(T≥38.0) 0.82 0.34 2.26 0.42–12.24
TheHosmer-Lemeshowchi-squaretestyieldedap-valueof0.938(chi-squared=0.409,degreesoffreedom=3).C-statistic=0.710.
RR=respiratoryrate;MRSA=methicillinresistantStaphylococcusaureus;T=temperature;OR=oddsratio;CI=confidenceinterval
TableB12showsthebackwardsselectionlogisticregressionmodelincludingthe
samesevenvariableswithaninclusioncriteriasetasap-value≤0.15.The
backwardsselectionmodeldroppedonevariable(fever).

140
TableB12.MultivariableLogisticRegressionModelUsingBackwardsSelectionofPredictorsofOralAntibioticTreatmentFailure(N=288)
PredictorVariable Estimate PValue AdjustedOR 95%CITachypnea(RR>20) 1.80 0.005 6.08 1.74–21.31Chroniculcers 1.56 0.004 4.74 1.63–13.84HistoryofMRSA
colonizationorinfection1.55 0.009 4.70 1.47–15.01
Chronickidneydisease 1.05 0.08 2.87 0.87–9.46Priorcellulitisinpast
12months0.78 0.06 2.17 0.98–4.82
Diabetesmellitus 0.55 0.11 1.74 0.88–3.43TheHosmer-Lemeshowchi-squaretestyieldedap-valueof0.611(chi-squared=
1.819,degreesoffreedom=3).C-statistic=0.710.RR=respiratoryrate;MRSA=methicillinresistantStaphylococcusaureus;T=temperature;OR=oddsratio;CI=confidenceinterval
Asafinalstep,theremaining6variablesfromthebackwardsselectionmodelwere
placedintoamultivariablelogisticregressionmodel.Thefinalmodelisshownin
TableB13.
TableB13.FinalMultivariableLogisticRegressionModelofPredictorsAssociatedwithOralAntibioticTreatmentFailure(N=288)
PredictorVariable Estimate PValue AdjustedOR 95%CITachypnea(RR>20) 1.84 0.004 6.31 1.80–22.08Chroniculcers 1.59 0.004 4.90 1.68–14.27HistoryofMRSA
colonizationorinfection1.58 0.008 4.83 1.51–15.44
Priorcellulitisinpast12months
0.80 0.05 2.23 1.01–4.96
Chronickidneydisease 1.59 0.10 2.60 0.82–8.22Diabetesmellitus 0.53 0.12 1.70 0.87–3.32
TheHosmer-Lemeshowchi-squaretestyieldedap-valueof0.604(chi-squared=1.853,degreesoffreedom=3).C-statistic=0.709.
TheHosmer-Lemeshowgoodnessoffit(p=0.604)indicatesnoevidenceofpoorfit
andtheC-statistic(0.709)suggestthemodelhasgoodfit.Thevariablesthat

141
remainedsignificant(p≤0.05)inthemultivariablemodelwere:tachypnea,chronic
ulcers,historyofMRSAcolonizationorinfection,andpriorcellulitisinthepast12
months.Sincediabeticsarepronetodevelopinglowerextremityulcers8-10,asafinal
step,wecheckedforpossibleinteractionbetweendiabetesmellitusandchronic
ulcers.Thisyieldedap-value=0.99,indicatingnosignificantinteractionbetween
thesevariables.
SecondaryAnalysis(ComparingOralvs.IntravenousTreatmentGroups)Weconductedasecondaryanalysiscomparingtheoralantibiotictreatmentgroup
(N=288)andintravenousantibiotictreatmentgroup(N=212).Theresultsare
summarizedinTablesB14andB15.

142
TableB14.SecondaryAnalysisComparingOralversusIntravenousAntibioticGroupsforCategoricalVariablesforall500Patients
Variable(n)
OralAntibioticGroupFrequency,n(%)
(n=288)
IVAntibioticGroupFrequency,n(%)
(n=212)
PValue*
Male(279) 158(54.9) 121(57.1) 0.62
ChronicUlcers(56) 20(6.9) 36(17.0) 0.0004SurgicalSiteInfection(30)
20(6.9) 10(4.7) 0.30
Bite(12) 8(2.8) 4(1.9) 0.52
>5%TBSA(99) 39(13.5) 60(28.3) <0.0001
Coronaryarterydisease(58)
29(10.1) 29(13.7) 0.21
Congestiveheartfailure(48)
18(6.2) 30(14.1) 0.003
Chronickidneydisease(35)
15(5.2) 20(9.4) 0.07
Chronicvenousinsufficiency(10)
8(2.8) 2(0.9) 0.20
Diabetesmellitus(126)
55(19.1) 71(33.5) 0.0002
HepaticDisease(37) 17(5.9) 20(9.4) 0.14HIV(8) 2(0.7) 6(2.8) 0.08IVDU(14) 4(1.4) 10(4.7) 0.02Lymphedema(33) 14(4.9) 19(9.0) 0.07MRSAHistory(43) 16(5.6) 27(12.7) 0.005Obesity(27) 8(2.8) 19(9.0) 0.002Priorcellulitis(87) 38(13.2) 49(23.1) 0.004PVD(40) 17(5.9) 23(10.8) 0.04*UsingChi-SquaredorFisher’sExactTestIV=intravenous;TBSA=totalbodysurfacearea;HIV=humanimmunodeficiencyvirus;IVDU=intravenousdruguse;MRSA=methicillinresistantStaphylococcusaureus;PVD=peripheralvasculardisease

143
TableB15.SecondaryAnalysisComparingOralversusIntravenousAntibioticGroupsforContinuousVariablesforall500Patients
Variable(n)
OralAntibioticGroup
Frequency,n(%)(N=288)
IVAntibioticGroup
Frequency,n(%)(N=212)
PValue*
Age(mean±SD) 64.4±20.0 64.3±16.9 0.95SystolicBP(mean±SD) 139±23 131±25 0.0007Heartrate(mean±SD) 84±16 90±21 <0.0001Temperature(mean±SD) 36.4±0.8 36.8±1.2 <0.0001RespiratoryRate(median,IQR)
16(16–18) 18(16–20) 0.02
SaO2(median,IQR) 97(96–98) 97(96–98) 0.88WBCcount(median,IQR) 8.2(6.6–11.2) 10.4(7.7–14.7) <0.0001*Usingt-testsfornormallydistributedvariables,Wilcoxontestsfornon-normallydistributedvariablesSD=standarddeviation;IQR=interquartilerange;IV=intravenous;BP=bloodpressure;HR=heartrate;SaO2=oxygensaturation;WBC=whitebloodcell
Patientsweremorelikelytoreceiveintravenousantibioticsiftheyhadchronic
ulcers,largeareaofinvolvement(totalbodysurfacearea>5%),congestiveheart
failure,diabetes,injectiondruguse,ahistoryofMRSAcolonizationorinfection,
priorcellulitisinthepast12monthsandperipheralvasculardisease.Patients
treatedwithintravenousantibioticsalsohadahighermedianrespiratoryrateand
highermeansystolicbloodpressure,heartrateandtemperature.Theseresults
suggestthatemergencyphysiciansappeartobemorelikelytoadminister
intravenousantibioticstopatientswithtriagevitalsignsorcomorbiditiesthatwere
associatedwithtreatmentfailureinthefinalmodel(TableB13).
DiscussionOurstudyidentifiedpotentialriskfactorsassociatedwithoralantibiotictreatment
failureforadultspresentingtotheEDwithnon-purulentSSTIs.Thenumberof

144
variablesunderconsiderationwasreducedbyeliminatingvariableswith>20%
missingdataorwithsparsedistributions.Wechosetoonlyincludevariableswhere
itwasclinicallyplausiblethattheymaybeassociatedwiththeprimaryoutcome.We
didnotidentifyahighdegreeofcollinearitybetweenvariables.Followingthe
exploratoryanalysis,univariatelogisticregressionidentifiedsevenvariables
associatedwiththeprimaryoutcome.
Wethendevelopedafinalmultivariablelogisticregressionmodelthatincludedsix
variables.Fourvariableswereindependentlyassociatedwithoralantibiotic
treatmentfailure:tachypnea;chroniculcers;ahistoryofMRSAcolonizationor
infection;andpriorcellulitisinthepast12months.TheHosmer-Lemeshow
goodness-of-fitsuggestsnoevidenceofpoorfitandtheC-statisticindicatesthatthe
modelhasgoodfit.Wealsolookedatpossibleinteractionbetweenindependent
variablesbutdidnotidentifyanysignificantinteractionterms.
Oneimportantlimitationtoourapproachwasthatthedatamightbeoverfitted.
However,asthiswasahealthrecordsreview,thepurposewastotryandidentify
potentialassociationswithoralantibiotictreatmentfailure.Weplantoconduct
futureprospectivestudiesincorporatingfewervariablestodevelopamodel.
ConclusionToourknowledge,thisisthefirststudytoidentifypredictorvariables
independentlyassociatedwithoralantibiotictreatmentfailure.Emergency

145
physiciansshouldconsidertheseriskfactorswhenselectingtheappropriateroute
ofantimicrobialtherapyforapatientwithanon-purulentSSTI.Futureprospective
studieswillbeconductedthatassessfewervariablesbasedonthefindingsofthis
study.

146
References1. HettiaratchyS,DziewulskiP.ABCofburns:pathophysiologyandtypesof
burns.BMJ.2004;328(7453):1427-1429.
2. WachtelTL,BerryCC,WachtelEE,FrankHA.Theinter-raterreliabilityofestimatingthesizeofburnsfromvariousburnareachartdrawings.Burns.2000;26(2):156-170.
3. BreaughJ.Effectsizeestimation:factorstoconsiderandmistakestoavoidJournalofManagement.2003;29(1):79-97.
4. Geriatricemergencydepartmentguidelines.AnnEmergMed.2014;63(5):e7-25.doi:10.1016/j.annemergmed.2014.1002.1008.
5. ConcatoJ,PeduzziP,HolfordTR,FeinsteinAR.Importanceofeventsperindependentvariableinproportionalhazardsanalysis.I.Background,goals,andgeneralstrategy.JClinEpidemiol.1995;48(12):1495-1501.
6. PeduzziP,ConcatoJ,FeinsteinAR,HolfordTR.Importanceofeventsperindependentvariableinproportionalhazardsregressionanalysis.II.Accuracyandprecisionofregressionestimates.JClinEpidemiol.1995;48(12):1503-1510.
7. PeduzziP,ConcatoJ,KemperE,HolfordTR,FeinsteinAR.Asimulationstudyofthenumberofeventspervariableinlogisticregressionanalysis.JClinEpidemiol.1996;49(12):1373-1379.
8. SinghN,ArmstrongDG,LipskyBA.Preventingfootulcersinpatientswithdiabetes.JAMA.2005;293(2):217-228.doi:210.1001/jama.1293.1002.1217.
9. LevyL,ZeichnerJA.Dermatologicmanifestationofdiabetes.JDiabetes.2012;4(1):68-76.doi:10.1111/j.1753-0407.2011.00151.x.
10. ForbesJM,CooperME.Mechanismsofdiabeticcomplications.PhysiolRev.2013;93(1):137-188.doi:110.1152/physrev.00045.02011.