Embed Size (px)
Citation preview
12/3/2011
1
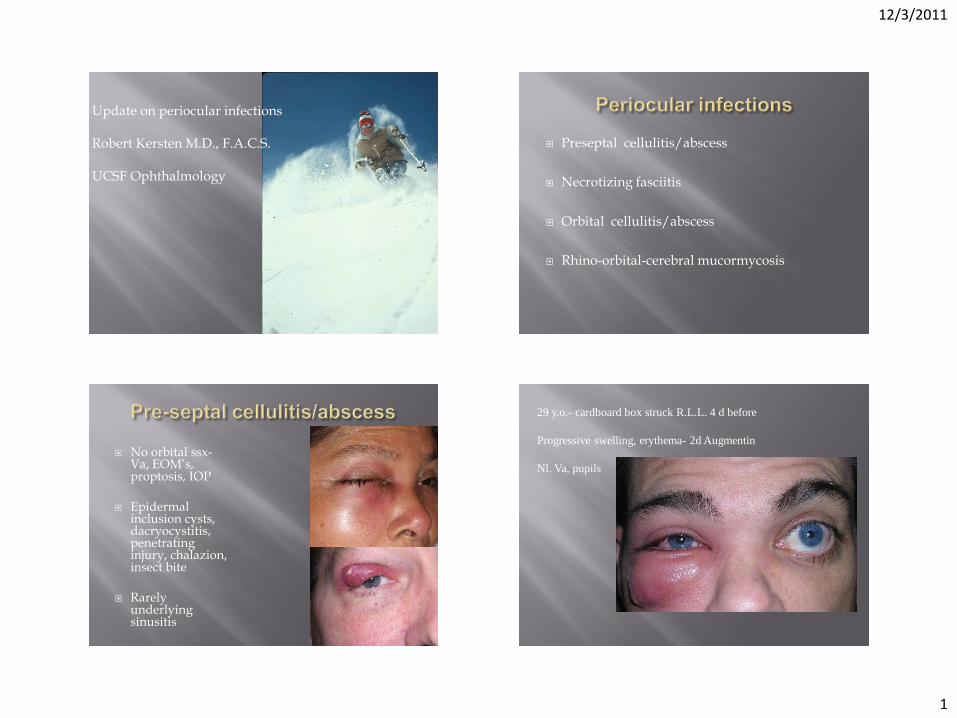
Update on periocular infections Robert Kersten M.D., F.A.C.S. UCSF Ophthalmology
Preseptal cellulitis/abscess
Necrotizing fasciitis
Orbital cellulitis/abscess
Rhino-orbital-cerebral mucormycosis
No orbital ssx- Va, EOM’s, proptosis, IOP
Epidermal inclusion cysts, dacryocystitis, penetrating injury, chalazion, insect bite
Rarely underlying sinusitis
29 y.o.- cardboard box struck R.L.L. 4 d before
Progressive swelling, erythema- 2d Augmentin
Nl. Va, pupils
12/3/2011
2
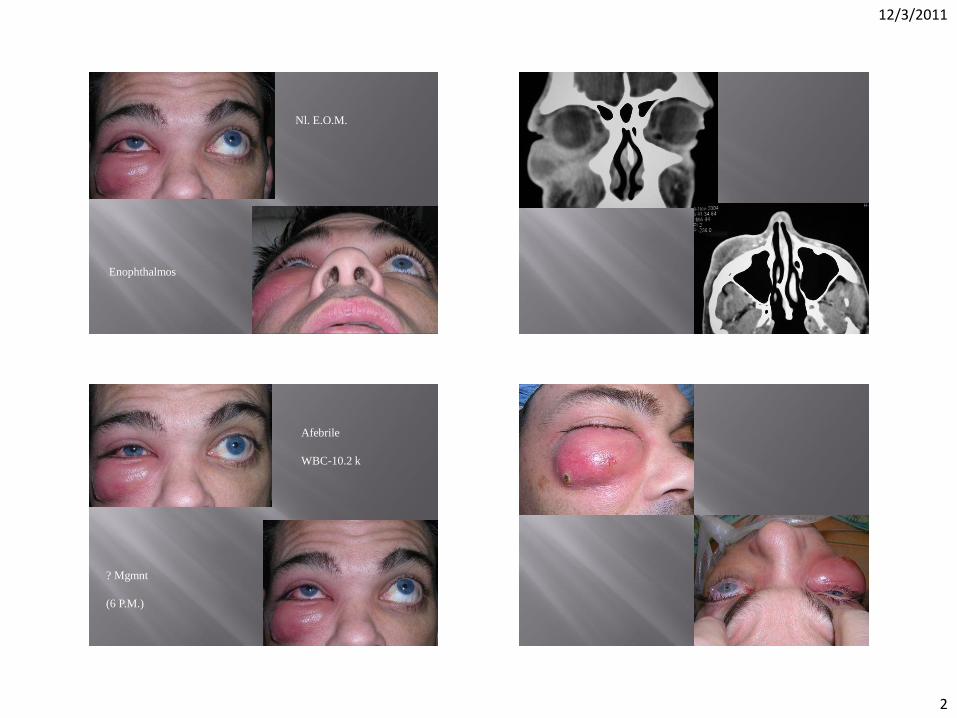
Nl. E.O.M.
Enophthalmos
Afebrile
WBC-10.2 k
? Mgmnt
(6 P.M.)

12/3/2011
3
Culture-MRSA
I.V.-Vancomycin
Packing advanced
Home with PICC line, 2 wks Vanc.
Central eschar granulated
Dual life style
Colonizer, commensal, normal flora
Virulent pathogen
Tendency to relapse or recur
5-25% treatment failure rate
Antibiotic resistance
Penicillin resistance 90% of all strains
Methicillin resistance (beta-lactam class resistance) 50-75% of hospital strains, 25-50% of community strains
<5% in 1990’s- large majority HA-MRSA CA-MRSA first reported in 1990’s
41.9% soft tissue infections by 2005 Univ of Cincinnati
2000- no cases mrsa 2006- 60% preseptal soft tissue infections
2010- routine culture Olson et al 2011
Conjunctiva 12.1% MRSA Eyelid 15.3% MRSA
12/3/2011
4
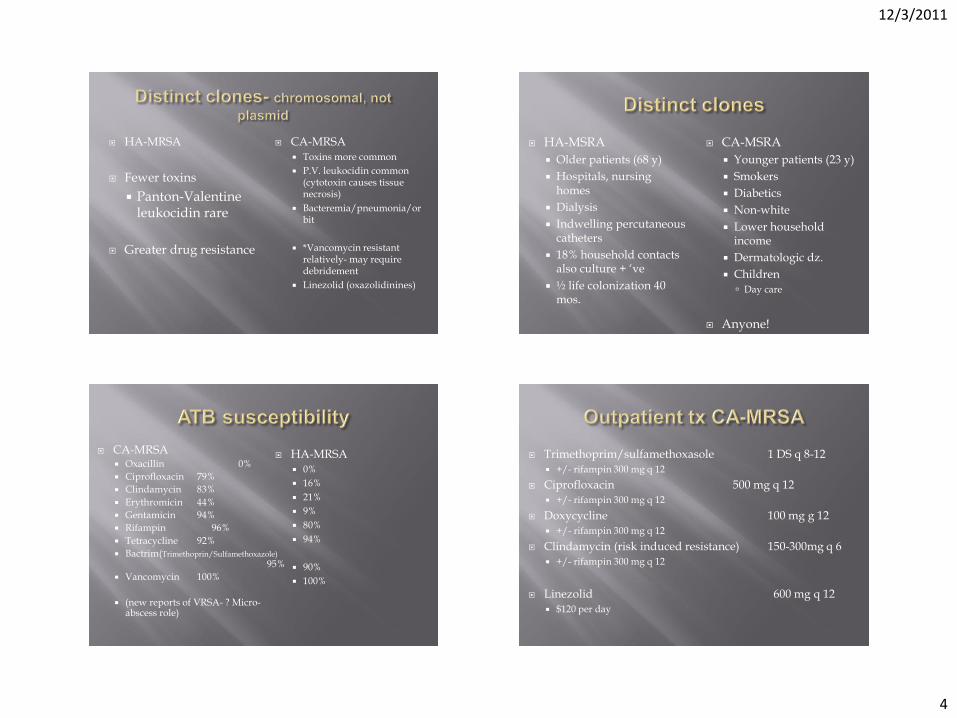
HA-MRSA
Fewer toxins
Panton-Valentine leukocidin rare
Greater drug resistance
CA-MRSA Toxins more common
P.V. leukocidin common (cytotoxin causes tissue necrosis)
Bacteremia/pneumonia/orbit
*Vancomycin resistant relatively- may require debridement
Linezolid (oxazolidinines)
HA-MSRA
Older patients (68 y)
Hospitals, nursing homes
Dialysis
Indwelling percutaneous catheters
18% household contacts also culture + ‘ve
½ life colonization 40 mos.
CA-MSRA
Younger patients (23 y)
Smokers
Diabetics
Non-white
Lower household income
Dermatologic dz.
Children Day care
Anyone!
CA-MRSA Oxacillin 0%
Ciprofloxacin 79%
Clindamycin 83%
Erythromicin 44%
Gentamicin 94%
Rifampin 96%
Tetracycline 92%
Bactrim(Trimethoprin/Sulfamethoxazole) 95%
Vancomycin 100%
(new reports of VRSA- ? Micro-abscess role)
HA-MRSA 0%
16%
21%
9%
80%
94%
90%
100%
Trimethoprim/sulfamethoxasole 1 DS q 8-12 +/- rifampin 300 mg q 12
Ciprofloxacin 500 mg q 12 +/- rifampin 300 mg q 12
Doxycycline 100 mg g 12 +/- rifampin 300 mg q 12
Clindamycin (risk induced resistance) 150-300mg q 6 +/- rifampin 300 mg q 12
Linezolid 600 mg q 12 $120 per day
12/3/2011
5
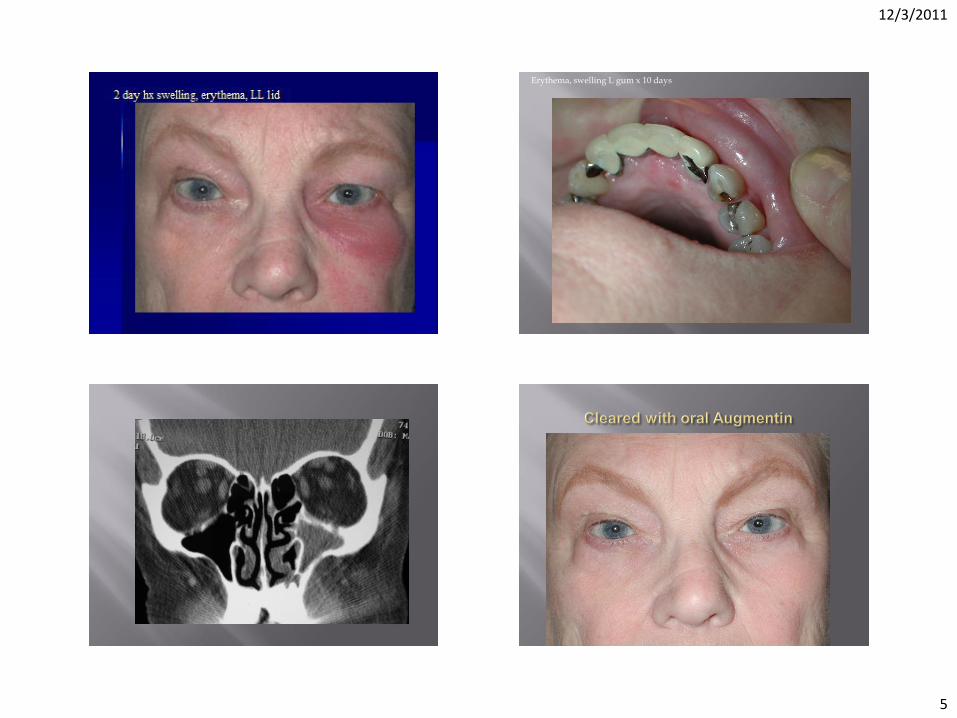
Erythema, swelling L gum x 10 days
12/3/2011
6
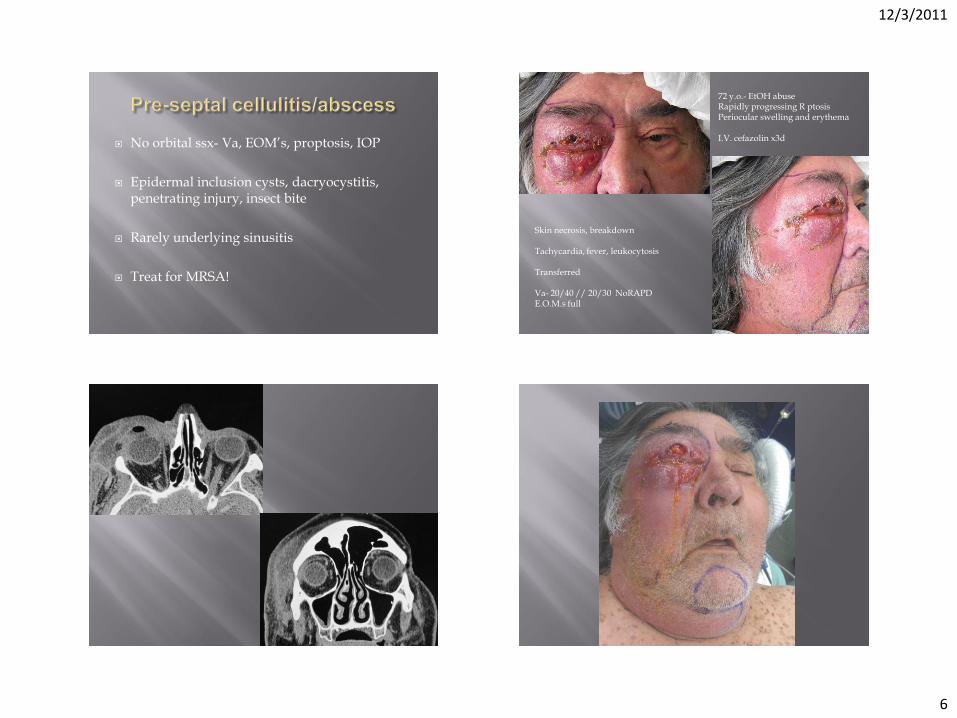
No orbital ssx- Va, EOM’s, proptosis, IOP
Epidermal inclusion cysts, dacryocystitis, penetrating injury, insect bite
Rarely underlying sinusitis
Treat for MRSA!
72 y.o.- EtOH abuse Rapidly progressing R ptosis Periocular swelling and erythema I.V. cefazolin x3d
Skin necrosis, breakdown Tachycardia, fever, leukocytosis Transferred Va- 20/40 // 20/30 NoRAPD E.O.M.s full

12/3/2011
7
Cultures- Group A strep Klebsiella Responded to Debridement and I.V. Unacin/Clindamycin
12/3/2011
8
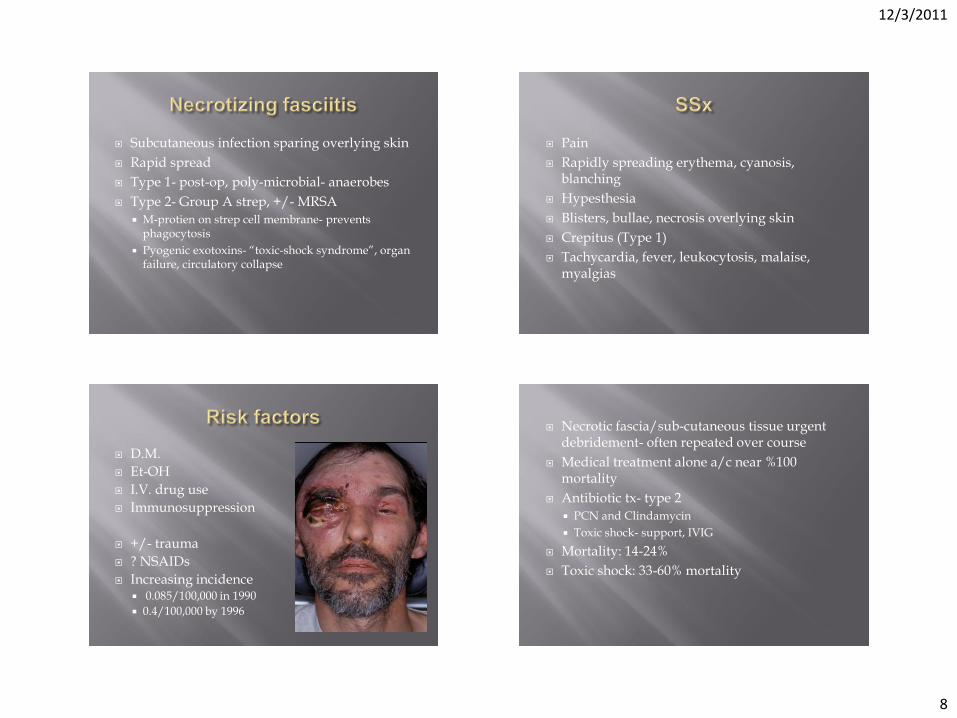
Subcutaneous infection sparing overlying skin
Rapid spread
Type 1- post-op, poly-microbial- anaerobes
Type 2- Group A strep, +/- MRSA
M-protien on strep cell membrane- prevents phagocytosis
Pyogenic exotoxins- “toxic-shock syndrome”, organ failure, circulatory collapse
Pain
Rapidly spreading erythema, cyanosis, blanching
Hypesthesia
Blisters, bullae, necrosis overlying skin
Crepitus (Type 1)
Tachycardia, fever, leukocytosis, malaise, myalgias
D.M.
Et-OH
I.V. drug use
Immunosuppression
+/- trauma
? NSAIDs
Increasing incidence 0.085/100,000 in 1990
0.4/100,000 by 1996
Necrotic fascia/sub-cutaneous tissue urgent debridement- often repeated over course
Medical treatment alone a/c near %100 mortality
Antibiotic tx- type 2
PCN and Clindamycin
Toxic shock- support, IVIG
Mortality: 14-24%
Toxic shock: 33-60% mortality
12/3/2011
9
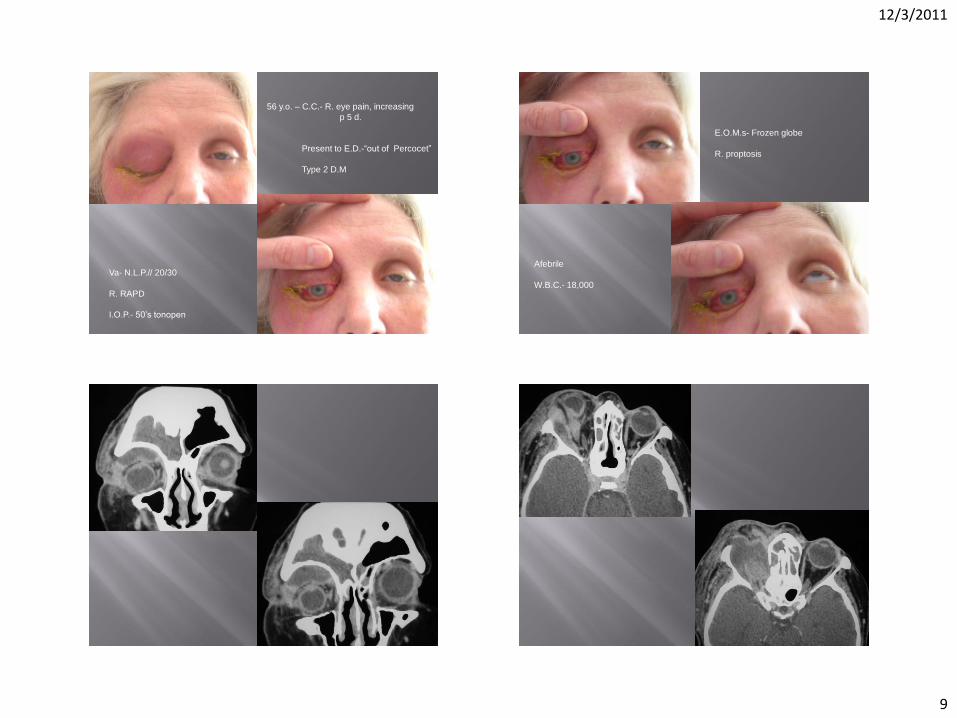
56 y.o. – C.C.- R. eye pain, increasing
p 5 d.
Present to E.D.-“out of Percocet”
Type 2 D.M
Va- N.L.P.// 20/30
R. RAPD
I.O.P.- 50’s tonopen
E.O.M.s- Frozen globe
R. proptosis
Afebrile
W.B.C.- 18,000
12/3/2011
10
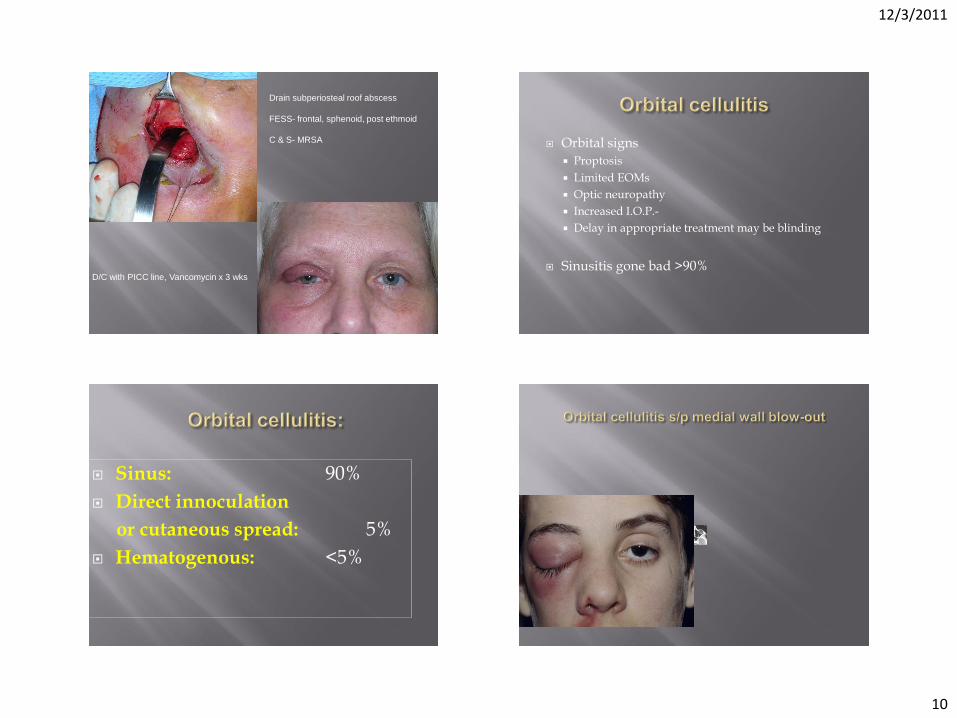
Drain subperiosteal roof abscess
FESS- frontal, sphenoid, post ethmoid
C & S- MRSA
D/C with PICC line, Vancomycin x 3 wks
Orbital signs
Proptosis
Limited EOMs
Optic neuropathy
Increased I.O.P.-
Delay in appropriate treatment may be blinding
Sinusitis gone bad >90%
Sinus: 90%
Direct innoculation
or cutaneous spread: 5%
Hematogenous: <5%
12/3/2011
11
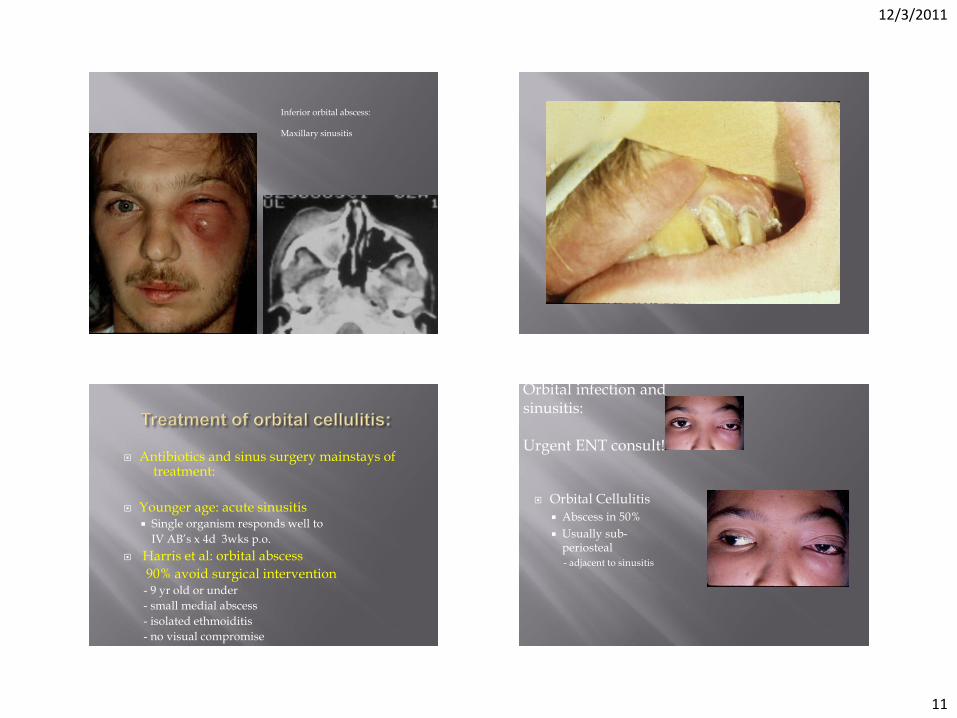
Inferior orbital abscess: Maxillary sinusitis
Antibiotics and sinus surgery mainstays of treatment:
Younger age: acute sinusitis Single organism responds well to
IV AB’s x 4d 3wks p.o.
Harris et al: orbital abscess
90% avoid surgical intervention - 9 yr old or under
- small medial abscess
- isolated ethmoiditis
- no visual compromise
Orbital Cellulitis
Abscess in 50%
Usually sub-periosteal - adjacent to sinusitis
Orbital infection and sinusitis: Urgent ENT consult!
12/3/2011
12
Initial medical therapy IF: Less than 10 y.o. “not large” medial sub- periosteal abscess Isolated acute ethmoid sinusitis No optic neuropathy
3rd generation cephalosporin
Ampicillin- sulbactam
MRSA- Vancomycin
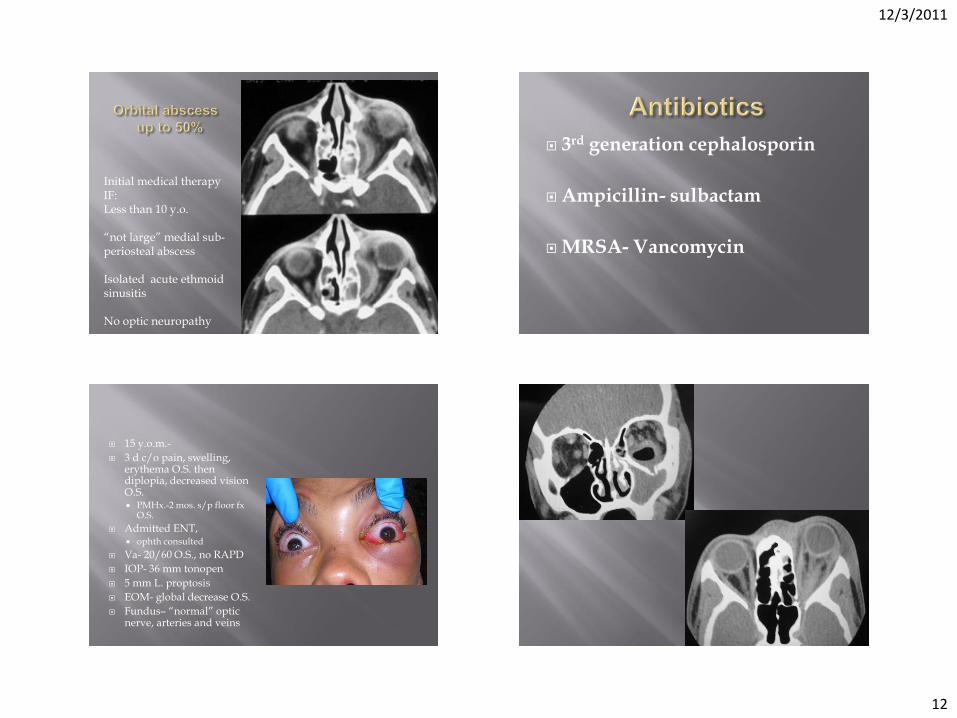
15 y.o.m.-
3 d c/o pain, swelling, erythema O.S. then diplopia, decreased vision O.S. PMHx.-2 mos. s/p floor fx
O.S.
Admitted ENT, ophth consulted
Va- 20/60 O.S., no RAPD
IOP- 36 mm tonopen
5 mm L. proptosis
EOM- global decrease O.S.
Fundus– “normal” optic nerve, arteries and veins
12/3/2011
13
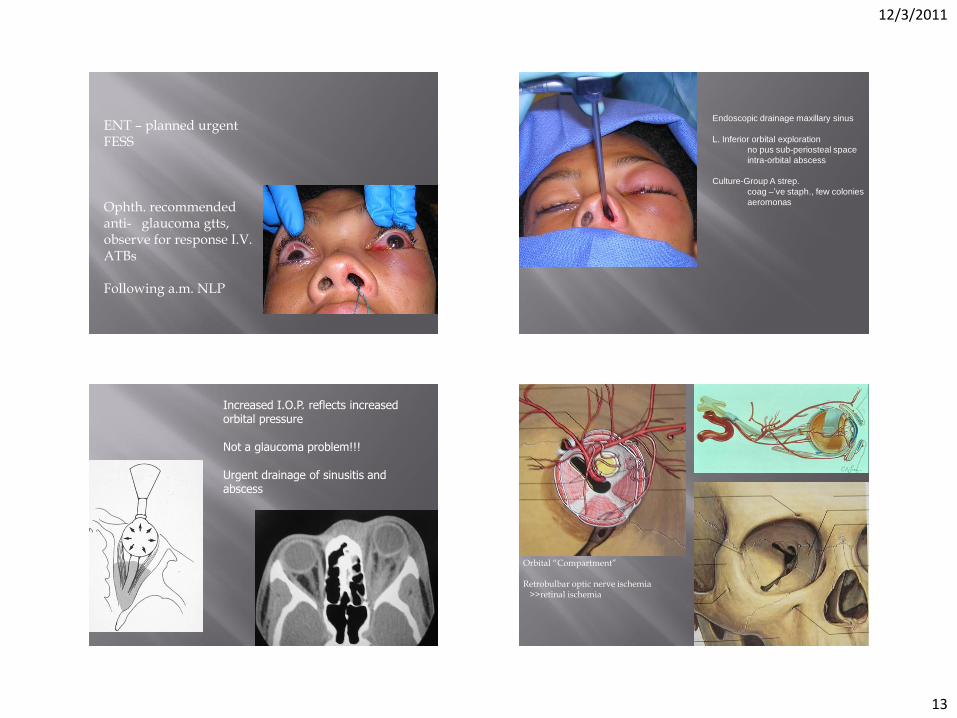
ENT – planned urgent FESS Ophth. recommended anti- glaucoma gtts, observe for response I.V. ATBs Following a.m. NLP
Endoscopic drainage maxillary sinus
L. Inferior orbital exploration
no pus sub-periosteal space
intra-orbital abscess
Culture-Group A strep.
coag –’ve staph., few colonies
aeromonas
Increased I.O.P. reflects increased orbital pressure Not a glaucoma problem!!! Urgent drainage of sinusitis and abscess
Orbital “Compartment” Retrobulbar optic nerve ischemia >>retinal ischemia

12/3/2011
14
16 y.o.f.- “fell” and bumped head (repeatedly) on kitchen table “bruising , swelling L.U.L.” diplopia maximal 2 days post injury- stable despite 2 weeks of oral ampicillin Increasing pain, transferred to UCSF V.A.- 20/100, but no RAPD, motility globally limited, intact sensation V1 I.O.P.- 21/18 Hertel- 21/13mm
Image!
Culture Polymicrobial- gm +’ves, anaerobes
12/3/2011
15
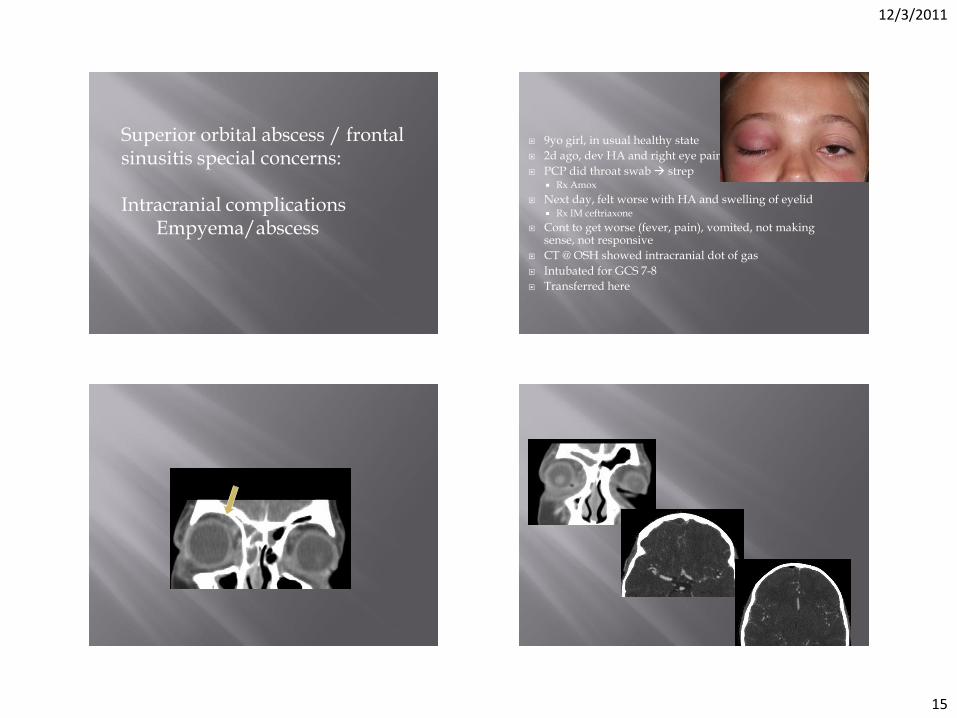
Superior orbital abscess / frontal sinusitis special concerns: Intracranial complications Empyema/abscess
9yo girl, in usual healthy state
2d ago, dev HA and right eye pain
PCP did throat swab strep Rx Amox
Next day, felt worse with HA and swelling of eyelid Rx IM ceftriaxone
Cont to get worse (fever, pain), vomited, not making sense, not responsive
CT @ OSH showed intracranial dot of gas
Intubated for GCS 7-8
Transferred here
12/3/2011
16
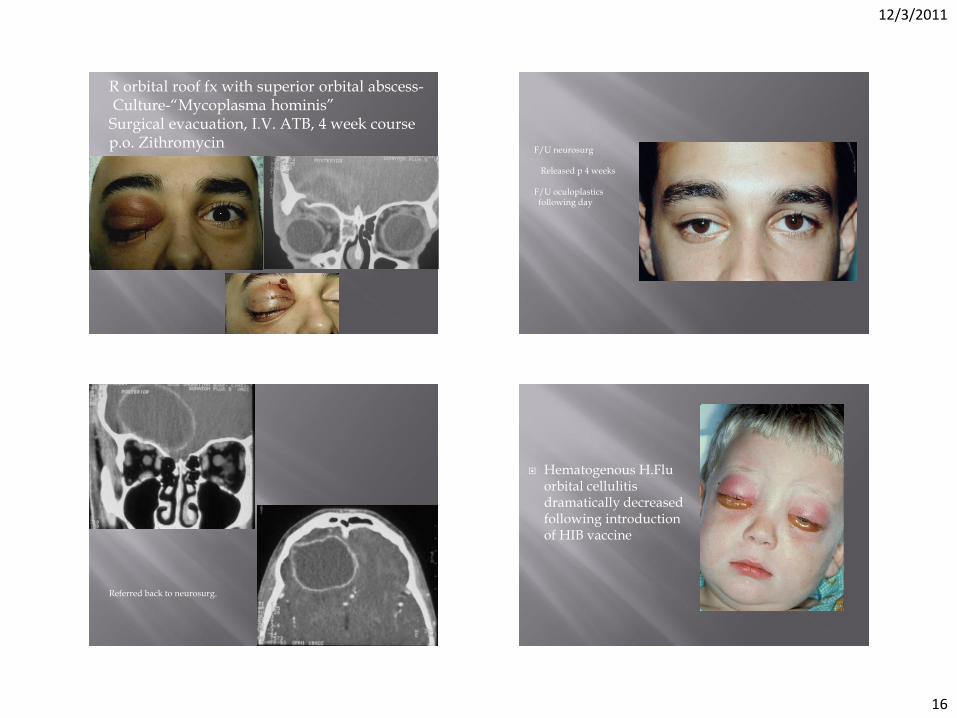
R orbital roof fx with superior orbital abscess- Culture-“Mycoplasma hominis” Surgical evacuation, I.V. ATB, 4 week course p.o. Zithromycin
F/U neurosurg Released p 4 weeks F/U oculoplastics following day
Referred back to neurosurg.
Hematogenous H.Flu orbital cellulitis dramatically decreased following introduction of HIB vaccine
12/3/2011
17
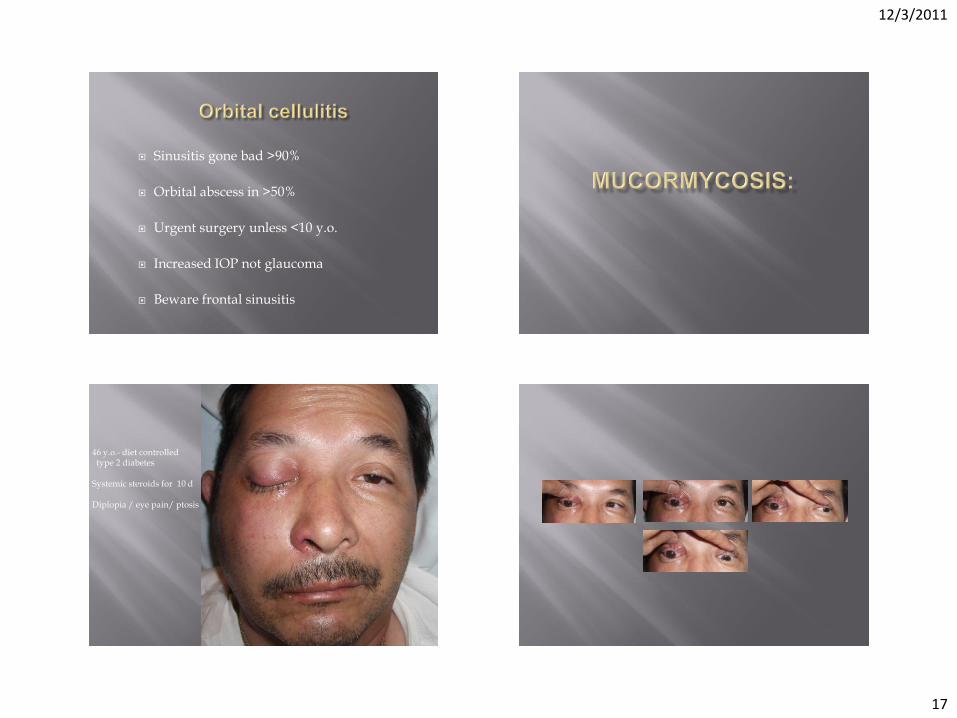
Sinusitis gone bad >90%
Orbital abscess in >50%
Urgent surgery unless <10 y.o.
Increased IOP not glaucoma
Beware frontal sinusitis
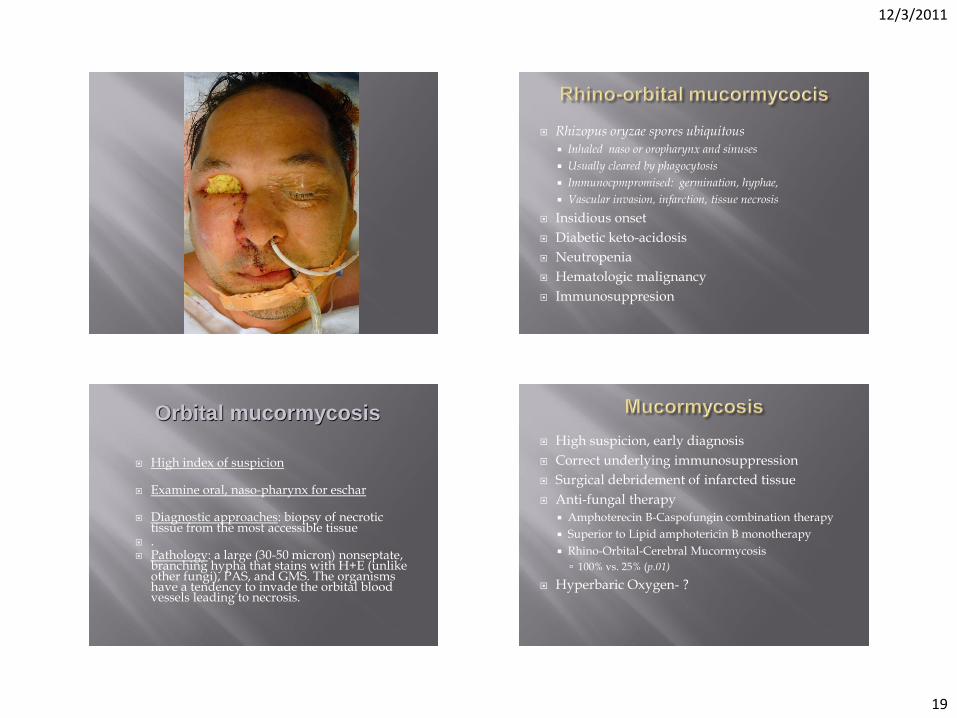
46 y.o.- diet controlled type 2 diabetes Systemic steroids for 10 d Diplopia / eye pain/ ptosis

12/3/2011
18
12/3/2011
19
Rhizopus oryzae spores ubiquitous
Inhaled naso or oropharynx and sinuses
Usually cleared by phagocytosis
Immunocpmpromised: germination, hyphae,
Vascular invasion, infarction, tissue necrosis
Insidious onset
Diabetic keto-acidosis
Neutropenia
Hematologic malignancy
Immunosuppresion
High index of suspicion
Examine oral, naso-pharynx for eschar
Diagnostic approaches: biopsy of necrotic tissue from the most accessible tissue
. Pathology: a large (30-50 micron) nonseptate,
branching hypha that stains with H+E (unlike other fungi), PAS, and GMS. The organisms have a tendency to invade the orbital blood vessels leading to necrosis.
Orbital mucormycosis High suspicion, early diagnosis
Correct underlying immunosuppression
Surgical debridement of infarcted tissue
Anti-fungal therapy
Amphoterecin B-Caspofungin combination therapy
Superior to Lipid amphotericin B monotherapy
Rhino-Orbital-Cerebral Mucormycosis
100% vs. 25% (p.01)
Hyperbaric Oxygen- ?
12/3/2011
20
> 46 y.o
Febrile
Frontal sinus involvement
Non-diabetic (4 x mortality)
Extent of disease (Rhino-cerebral 3x > rhino-orbital)
Anti-fungal treatment
Exenteration better survival Case-by-case: (patients w fever)
Treatment:
- Treat the underlying metabolic disorder or neutropenia.
- Antifungal: Amphotericin B (lipid formulation) alone or combined with echinocandins (e.g. caspofungin)
- Wide surgical debridement (excise until presence of freely bleeding tissue) and orbital exenteration done on case by case basis.
Reed C, Bryant R, Ibrahim AS, Edwards J Jr, Filler SG, Goldberg R, Spellberg B. Combination polyene-caspofungin treatment of rhino-orbital-cerebral mucormycosis. Clin Infect Dis. 2008;47(3):364.
Orbital mucormycosis
12/3/2011
21
Sinusitis gone bad >90%