Embed Size (px)
Citation preview

i
“CORRELATION OF DERMATOGLYPHIC AND CHEILOSCOPIC PATTERNS,
ALONG WITH ASSESSMENT OF PREVALENCE OF DENTAL CARIES AND
SKELETAL MALOCCLUSION IN CHILDREN OF AGE GROUP 6-14 YEARS”
By
Dr. ANNAT VARGHESE
Dissertation
Submitted to the Rajiv Gandhi University of Health Sciences,
Karnataka, Bangalore
In partial fulfilment of the requirements for the degree of
MASTER OF DENTAL SURGERY
In
PEDIATRIC AND PREVENTIVE DENTISTRY
Under the guidance of
Dr. SHIVAPRAKASH.P.K.
Professor & Head
DEPARTMENT OF PEDIATRIC AND PREVENTIVE DENTISTRY,
P.M.N.M DENTAL COLLEGE AND HOSPITAL,
BAGALKOT-587103, KARNATAKA
2020

Scanned by CamScanner

Scanned by CamScanner

iv
ACKNOWLEDGEMENT
This venture would not have been possible without God’s grace and spiritual
guidance. I bow before the Almighty who with his immense bountiful nature showered
blessings on me.
With profound sense of gratitude and respect, I express my most cordial and
humble thanks to my guide, Dr.Shivaprakash P.K., Prof. and Head, Department of
Pediatric & Preventive Dentistry, P.M.N.M. Dental College and Hospital, Bagalkot,
for his unparalleled and excellent guidance, constant inspiration, unlimited patience
and encouragement for which my mere expression of thanks likewise does nothing to
suffice.
It is my immense pleasure to thank my respected co-guide Dr. Mahantesha T.
for inspiring and encouraging me to achieve beyond my set limits and always being
supportive that showed me the path to success, for which I am extremely grateful.
Expressions are inadequate to convey my immense gratitude to Professor Dr.
Hina Noorani and senior lecturers Dr.Rashmi G. Chour, Dr.Prashant Jalannavar,
and Dr.Hiranmayi Brid for their keen interest, moral support and encouragement
throughout my studies.
I am extremely indebted to Prof. Dr.Shreenivas.S.Vanaki, Principal, P.M.N.M
Dental College and Hospital, Bagalkot for providing me the opportunity to utilize all
the facilities available in this institution for the completion of the study.
Above all, I would like to thank my family and friends…
Dr. ANNAT VARGHESE

v
LIST OF ABBREVIATIONS
ABBREVIATIONS FULL NAME
ANB angle A point, Nasion, B point angle
ANOVA Analysis of variance
CPITN Community Periodontal Index of Treatment Need
CVG+RG Complete vertical grooves + Reticular grooves
deft Decayed-Extracted-Filled Teeth
DMFT Decayed-Missing-Filled Teeth
IG+RG Intersecting grooves + Reticular grooves
PVG+RG Partial vertical grooves + Reticular grooves
SPSS Statistical Package for Social Sciences
WHO World Health Organisation

vi
LIST OF TABLES
SERIAL
NO.
TABLES PAGE
NO.
1. Sample size
25
2. Study parameters
25
3. Age and Gender distribution among study subjects
27
4. Comparison of different types of Lip Print Patterns among
study subjects between three skeletal malocclusions using
Chi Square Test
27
5. Comparison of different types of Finger Print Patterns
among study subjects between three skeletal malocclusions
using Chi Square Test
27
6. Comparison of mean DMFT / deft scores between different
types of Skeletal malocclusion using Kruskal Wallis Test
28
7. Multiple comparison of mean difference in the DMFT/deft
scores b/w different skeletal malocclusions using Mann
Whitney Post hoc Test
28
8. Comparison of prevalence of Skeletal Malocclusion based
on different age and gender of study subjects using Chi
Square Test
28

vii
9. Correlation between different Lip and Finger Print Patterns
in Skeletal Class I Malocclusion using Chi Square Test
29
10. Correlation between different Lip and Finger Print Patterns
in Skeletal Class II Malocclusion using Chi Square Test
29
11. Correlation between different Lip and Finger Print Patterns
in Skeletal Class III Malocclusion using Chi Square Test
30
LIST OF GRAPHS
SERIAL
NO.
GRAPHS PAGE
NO.
1. Age-wise distribution of study subjects 30
2. Gender-wise distribution of study subjects 31
3. Lip Print Patterns among study subjects between three
skeletal malocclusions
31
4. Finger Print Patterns among study subjects between three
skeletal malocclusions
32
5. Mean DMFT/deft scores between different types of Skeletal
malocclusions
32

viii
6. Age-wise Prevalence of different types of skeletal
malocclusions
33
7. Gender-wise Prevalence of different types of skeletal
malocclusions
33
8. Correlation between different lip and finger print patterns in
Skeletal Class I Malocclusion
34
9. Correlation between different lip and finger print patterns in
Skeletal Class II Malocclusion
34
10. Correlation between different lip and finger print patterns in
Skeletal Class III Malocclusion
35

ix
LIST OF FIGURES
SERIAL
NO.
FIGURES PAGE NO:
1. Suzuki and Tsuchihashi’s
classification system
23
2. in Dermatoglyphic patterns 24
3. Armamentarium 60
4. Obtaining informed consent 60
5. Applying child safe lipstick with
brush
61
6. Lip print being collected through
scotch tape
61
7. Lip print collected and transferred to
paper
62
8. Applying black duplicating ink with
cotton
62
9. Finger print being collected 63
10. Finger print collected on paper
63

xi
ABSTRACT
TITLE: “CORRELATION OF DERMATOGLYPHIC AND CHEILOSCOPIC
PATTERNS, ALONG WITH ASSESSMENT OF PREVALENCE OF DENTAL
CARIES AND SKELETAL MALOCCLUSION IN CHILDREN OF AGE
GROUP 6-14 YEARS.”
BACKGROUND & OBJECTIVES:
To record and compare lip prints and finger prints in children with skeletal
malocclusion (I, II, III) of age group 6-14 years.
To determine the prevalence of dental caries and type of skeletal malocclusion
in children of age group 6-14 years.
METHODS:
90 children of age group of 6 - 14 years reporting to the Department of
Pediatric and Preventive Dentistry, P.M.N.M. Dental College and Hospital, Bagalkot
were divided into 3 groups, by examining the lateral cephalograms obtained from
them, as:
Group A - consisting of 30 children with skeletal Class-I malocclusion.
Group B - consisting of 30 children with skeletal Class-II malocclusion.
Group C - consisting of 30 children with skeletal Class-III malocclusion.

xii
For the groups:
Lip-prints were taken using child safe lipstick-scotch tape method on the bond
paper and classified according to Suzuki and Tsuchihashi’s classification
system.
Finger prints (right and left) of the subjects were recorded using black
duplicating ink on the bond paper and classified as arch, whorl and loop
patterns.
Presence of dental caries were assessed by deft/DMFT index.
RESULTS:
Unique lip prints and finger prints were obtained for different skeletal
malocclusions.
Prevalence of dental caries were as follows: Class III>Class II>Class I.
INTERPRETATION AND CONCLUSION:
This study highlights the scope of early diagnosis of skeletal malocclusions
through the chelioscopic and dermatoglyphic patterns which are unique for each
individual and the prevalence of dental caries which also must be considered as an
entity to be sorted out with the preventive and therapeutic measures.
Key words: Malocclusion; Lip print; Finger print; Dental caries.

Introduction
P.M.N.M Dental College, Bagalkot 1
“CORRELATION OF DERMATOGLYPHIC AND
CHEILOSCOPIC PATTERNS, ALONG WITH ASSESSMENT OF
PREVALENCE OF DENTAL CARIES AND SKELETAL
MALOCCLUSION IN CHILDREN OF AGE GROUP 6-14
YEARS.”
INTRODUCTION
Malocclusion is defined as an irregularity of the teeth or a malrelationship
between the dental arches beyond the range of what is accepted as normal. It is one of
the most common dental problems like dental caries, periodontal disease, and dental
fluorosis. In addition, mal-occluded dentition can cause disturbances in oral function
and psychosocial problems due to impaired dento-facial esthetics. The etiology of
malocclusion is multifactorial and can be a combination of hereditary factors
including some stimulus during the formation and development of orofacial structures
and environmental factors such as oral habits, social characteristics, and diet1.
Malocclusion can be classified into skeletal malocclusion and dental
malocclusion. The occlusion in which there is a malrelationship between the arches in
any of the planes is skeletal malocclusion and in which there are anomalies in tooth
position beyond the normal limits is dental malocclusion2. Based on cephalometric
analyses, skeletal malocclusion can be classified as: Class I Skeletal Pattern, Class II
Skeletal Pattern and Class III Skeletal Pattern. Understanding the skeletal pattern is
essential for choosing the proper treatment mechanics.
The relationship between the skeletal malocclusions (Class I, II and III Skeletal
Patterns) and soft tissue facial morphology has been an arena of vast research in

Introduction
P.M.N.M Dental College, Bagalkot 2
contemporary orthodontics. The lip prints are unique to an individual just like the
fingerprints and shows strong hereditary pattern3.
Lip prints consist of normal lines and fissures in the form of wrinkles and
grooves present in the zone of transition of human lip between the inner labial mucosa
and outer skin. The study of lip prints is referred to as Cheiloscopy. It can be defined
“as a method of identification of a person based on the characteristic arrangements of
lines appearing on the red part of lips or as a science dealing with lines appearing on
red part of the lips”.
Lips form an important component of the orofacial soft tissue profile. So they
play an important role in orthodontic diagnosis and treatment planning. Establishing a
correlation between sagittal jaw relation and lip prints would benefit the clinician by
predicting the type of malocclusion4. The pattern of wrinkles on the lips has
individual characteristics as fingerprints5. Similarly, in recent past several research
studies had established that lip prints can be used as evidence in personal
identification and criminal investigation in forensic dentistry3.
Dermatoglyphics as coined by Cummins and Midlo refers to the study of the
intricate dermal ridge configurations on the skin covering the palmar and plantar
surfaces of hands and feet and has been investigated extensively by many researchers.
Etymologically this term is a harmonious blend of two words derma, i.e., skin; and
glyphe, i.e., carve, giving the impression that something has been carved out of the
skin. The dermal patterns once formed remain constant throughout life6.
Through decades of scientific research, the hand has been recognized as a
powerful tool in the diagnosis of psychological, medical and genetic conditions6. The
use of finger prints in personal identification and in criminal investigation is accepted

Introduction
P.M.N.M Dental College, Bagalkot 3
part of forensic science3. It has proved to be a helpful adjunct to other diagnostic
methods in identifying specific syndromes of genetic origin6.
Determining the relationship between the lip prints, finger prints and respective
skeletal malocclusions can facilitate early diagnosis of the developing jaw relation
and can also be helpful as a forensic tool. There exists a deficiency in studies carried
on samples of pediatric age groups.
Dental caries is the localized destruction of susceptible dental hard tissues by
acidic by-products from bacterial fermentation of dietary carbohydrates7. The
relationship between malocclusions and prevalence of dental caries is an important
concept. This association is due to the increased susceptibility to plaque retention
among the crowded teeth, which results in caries development8.
Dental caries has been compared with malocclusion and some authors reported
a positive association between them. Moreover, conflicting results have been obtained
in studies considering a possible relationship between malocclusion and various oral
hygiene measures9.
Considering the increasing frequency of poor oral health status in children
having malocclusion, it is required to conduct a study to investigate the
dermatoglyphics and cheiloscopic patterns, along with assessment of prevalence of
dental caries and type of skeletal malocclusion in boys and girls of age group 6-14
years.

Objectives
P.M.N.M Dental College, Bagalkot 4
OBJECTIVES
1. To record and compare lip prints and finger prints in children with skeletal
malocclusion (I, II, III) of age group 6-14 years.
2. To determine the prevalence of dental caries in children with skeletal
malocclusion of age group 6-14 years.
3. To assess the prevalence of the type of skeletal malocclusion in boys and girls
of age group 6-14 years.

Review of Literature
P.M.N.M Dental College, Bagalkot 5
REVIEW OF LITERATURE
A study was conducted by Shivani et al to find pre-dominant lip print pattern in
skeletal class-III malocclusion. A total of 30 patients were taken with skeletal class III
malocclusion. On the basis of ANB angle and wits appraisal patients were categorized
into skeletal class III malocclusion. Digital soft copies of their lateral cephalograms
were taken and lip prints were taken using lipstick-cellophane method on the bond
paper. Brand of Lipstick used was LAKME enrich satins 461. Descriptive statistical
analysis was used to find the prevalence of lip prints patterns among sagittal class III
skeletal malocclusions. CVG+RG, PVG+RG, IG+RG types of lip prints were
predominant in skeletal class III group of individuals10.
A study was conducted by Raghav et al to explore the possible association of
lip prints with skeletal malocclusion. A sample of 114 subjects in the age group of
18‑30 years, from North Indian adult population were selected on the basis of skeletal
class I, class II and class III malocclusion, each comprising of 38 subjects with equal
number of males and females. Lip prints of all the individuals were recorded and
digital soft copies of lateral cephalograms were taken. Lip prints were compared
between different skeletal malocclusions. It was found that branched lip pattern was
most common in North Indian adult population with no sexual dimorphism. The
Z‑test for proportion showed that the prevalence of vertical lip pattern was
significantly higher in subjects having skeletal class III malocclusion. A definite
co‑relation of vertical lip patterns with skeletal class III malocclusion was revealed3.
Kaushal et al conducted a study to explore the possible association of lip prints
with Skeletal Class I and Class II malocclusions with varying growth patterns. A
sample of 90 subjects in the age group of 18‑30 years, from District Solan (H.P.),
population were selected. Subjects were divided into two groups group I (Skeletal

Review of Literature
P.M.N.M Dental College, Bagalkot 6
Class I) and group II (Skeletal Class II). Lip prints of all the individuals were recorded
and compared between Skeletal Class I and Class II malocclusions with varying. It
was found that Branched lip pattern was most common in District Solan population
with no sexual dimorphism. No statistically significant association of lip prints with
Skeletal Class I and Class II malocclusion was revealed4.
A study was conducted by Sharma et al to determine whether there is any
association of lip print patterns with malocclusion. 300 subjects were recruited, out of
them 234 subjects including males and females were found to be fit for the study
having dental malocclusion with age range of 18-25 years. The subjects were
classified into three groups according to Angle’s classification of malocclusion into
Class-I, Class-II and Class-III malocclusions. A thin film of lipstick was applied onto
cleaned and dried lips and left for 3 minutes. The impressions of lips were taken on
the self-adhesive cellophane tape and then immediately transferred onto the bond
sheets. The analysis of these lip print patterns was done with the help of magnifying
lens. For analysis of lip prints, classification proposed by Tsuchihashi was used. Data
was then tabulated in various classes of lip print patterns and malocclusions and then
analyzed statistically. The statistical analysis with chi square test showed that lip print
patterns were found to have highly significant (p<0.001) association with
malocclusion11.
Ponnusamy et al conducted a study to assess the strength of association between
lip patterns and skeletal class I and II malocclusion. Lip prints of 25 subjects with
skeletal Class I and 25 with skeletal Class II malocclusion (age group of 18-35years)
were recorded. Statistically significant difference between the two malocclusions
were observed in the Vertical and Branched patterns while the intersected, reticular
and undermined patters showed no difference. This was evident in the female gender

Review of Literature
P.M.N.M Dental College, Bagalkot 7
while the male gender showed differences in the vertical pattern only. Since sagittal
jaw and dental relationships get established before lip prints, lip print assessment may
aid the clinical orthodontist by predicting the type of malocclusion12.
A study was conducted by Vignesh et al to assess the correlation between
different cheiloscopic patterns with the terminal planes in deciduous dentition. Three
hundred children who are 3–6 years old with complete primary dentition were
recruited, and the pattern of molar terminal plane was recorded in the proforma. Lip
prints of these children were recorded with lipstick‑cellophane method, and the
middle 10 mm of lower lip was analyzed for the lip print pattern as suggested by
Sivapathasundharam et al. The pattern was classified based on Tsuchihashi and
Suzuki classification. Type II (branched) pattern was the most predominant
cheiloscopic pattern. The predominant patterns which related to the terminal planes
were as follows: Type IV (reticular) and Type V (irregular) pattern for mesial step,
Type IV (reticular) pattern for distal step, and Type I (complete vertical) pattern for
flush terminal plane. No significant relationship was obtained on gender comparison.
Lip prints can provide an alternative to dermatoglyphics to predict the terminal plane
in primary dentition13.
A study was conducted by Tikare et al to assess the relationship between finger
prints and malocclusion. Six hundred and ninety six children aged twelve to sixteen
years were selected. Their fingerprints were recorded using duplicating ink and
malocclusion status was clinically assessed using Angle’s classification. A statistical
association was revealed between whorl patterns and classes 1 and 2 malocclusion.
Dermatoglyphics might be an appropriate marker for malocclusion and further studies
are required to elucidate an association between fingerprint patterns and
malocclusion14.

Review of Literature
P.M.N.M Dental College, Bagalkot 8
Sonika et al conducted a study to assess the relationship between fingerprint
patterns and skeletal malocclusion. Fingerprint patterns were collected using the ink
method from 90 subjects who were divided into skeletal class I, II, and III
malocclusion groups of 30 subjects each. The loop pattern was more frequent in
patients with skeletal class I and II malocclusion, and the whorl pattern was more
frequent in those with class III malocclusion. The present study attempted to assess
the relationship between dermatoglyphic patterns with skeletal malocclusion to use as
an indicator of developing malocclusion at an early age15.
A study was conducted by Neda et al to compare the dermatoglyphic
characteristics of different malocclusions. In this cross-sectional study, 323 patients
who were referred to Orthodontic Department of Mashhad Dental School were
recruited. The participants were classified into three groups according to Angle´s
classification, i.e., Skeletal Class 1 (n = 163), Skeletal Class 2 (n = 111), and Skeletal
Class 3 (n = 49). For all participants, they recorded the total ridge counts of each
finger (TRC), atd angles, a-b ridge counts, and types of fingerprint patterns. Right-
and left-hand asymmetry scores were calculated. The chi-squared test was used to
compare the dissimilarity of the types of patterns for each finger. Asymmetry of other
parameters was analyzed statistically using the ANOVA or Kruskal-Wallis tests. P-
values greater than 0.05 were considered to be significant. A significant difference
was determined between Class I and Class III patients in terms of left a-b ridge count
(p=0.049). Loop was the most frequent pattern in the three groups, whereas the arch
pattern occurred with the lowest frequency. No significant difference was found in the
other parameters that were studied. Although there were some slight differences in
dermatoglyphic peculiarities of different skeletal malocclusions, most of the palm and
fingerprint characteristics failed to indicate any significant differences16.

Review of Literature
P.M.N.M Dental College, Bagalkot 9
Baswaraj et al conducted a study on 60, 9-12 years old, healthy children, with
mixed dentition. Their left and right handprints were recorded on a paper, and the
fingerprints were studied to find the frequency of occurrence of different types of
patterns. Based on the dental aesthetic index, malocclusion was graded into four
groups and then was correlated with the patterns’ frequency. Loops were found to
increase and while the whorls decreased, with increasing severity of malocclusion. In
this study, loop pattern is a more common in the thumb and middle finger. Whorl
pattern is a more common in the ring finger and index finger17.
A study was conducted by Divyashree et al to determine the relation between
dermatoglyphics and malocclusion. 40 individuals cephalometrically confirmed as
Skeletal Class I and Skeletal Class II based on Downs and Steiner analysis between
the age group of 15 – 30 years were selected. Fingerprint patterns of the study
subjects were recorded using ink and paper method and the finger prints were studied
to find the frequency of occurrence of different types of patterns. The pattern
distribution is significantly different between both the groups. Increased frequency of
whorls were found both in right & left hands in Skeletal Class I pattern group.
Increased frequency of ulnar loops was found in the right hand of Skeletal Class II
pattern group18.
A study was conducted by George et al to assess the correlation between
dermatoglyphic patterns and sagittal skeletal discrepancies. A total of 180 patients,
aged 18-40 years, were selected from those who attended the outpatient clinic of the
Department of Orthodontics and Dentofacial Orthopedics, Mar Baselios Dental
College, Kothamangalam, Kerala, India. The fingerprints of both hands were taken by
ink and stamp method after proper hand washing. The patterns of arches, loops and
whorls in fingerprints were assessed. The total ridge count was also evaluated. Data

Review of Literature
P.M.N.M Dental College, Bagalkot 10
was also sent to the fingerprint experts for expert evaluation. The sagittal jaw relation
was determined from the patient’s lateral cephalogram. The collected data was then
statistically analyzed using Chi-square tests, ANOVA and Post-hoc tests and a
Multinomial regression prediction was also done. A significant association was
observed between the dermatoglyphic patterns exhibited by eight fingers and the
sagittal skeletal discrepancies (p<0.05). An increased distribution of whorl pattern
was observed in the skeletal Class II with maxillary excess group and skeletal Class II
with mandibular deficiency group while an increased distribution of loop pattern was
seen in the skeletal Class III with mandibular excess group and skeletal Class III with
maxillary deficiency group. Higher mean of total ridge count was also seen in the
groups of skeletal Class II with maxillary excess and skeletal Class II with mandibular
deficiency. Multinomial regression predicting skeletal pattern with respect to the
fingerprint pattern showed that the left thumb impression fits the best model for
predicting the skeletal pattern19.
A study was conducted by Charles et al to evaluate and compare the
dermatoglyphic patterns with various skeletal malocclusions. The study was carried
out on 40 outpatients reported with an age group of 18–20 years divided into four
groups as follows: Group: I – 10 (Class I occlusion), Group: II – 10 (skeletal Class I
malocclusion), Group: III – 10 (skeletal Class II malocclusion), and Group: IV – 10
(skeletal Class III malocclusion). The fingerprints were recorded using scanner
exclusively designed for diagnostic purpose of the study. The collected data were
analyzed using SPSS statistics software Version 23.0 to find which groups had
significant differences. Increased frequency of arch pattern was present in participants
with Class I malocclusion, and loop patterns were observed in those with Class I

Review of Literature
P.M.N.M Dental College, Bagalkot 11
occlusion and Class III malocclusion and whorl patterns in Class II malocclusion with
P < 0.0520.
Smitha et al conducted a study to explore an association if any, between the
dermatoglyphic patterns and type of malocclusion among the Malaysian dental and
medical students. A total of 104 Malaysian dental and medical students were included
in the study. The fingerprints and palm prints were recorded to analyze the type of
pattern. Occlusion status was clinically assessed using Angle’s classification of
malocclusion. Statistically significant association was seen between the left thumb
ridge pattern and type of malocclusion. Individuals with loop ridge pattern on their
left thumb showed high frequency of Class I normal occlusion and Class III
malocclusion, and those with whorl ridge pattern were witnessed to have Class I
malocclusion. Dermatoglyphics serves to strengthen the diagnostic impression of
malocclusion at an early age and hence can aid in predicting malocclusion and plan
preventive and interceptive orthodontics in pediatric patients21.
A study was conducted by Matilda et al to assess the prevalence of
malocclusion and its association with socio-demographic characteristics, caries
experience and level of oral hygiene in 12-14 year old school children residing in
Tanzania. A total of 1601 children attending 16 primary schools in Kinondoni and
Temeke districts. Chi-square and multiple logistic regression models were used.
Malocclusions were prevalent in Tanzanian children investigated and were associated
with environmental factors in terms of caries experience and residing in a less affluent
district9.
A study was conducted by Sajith et al to determine the association of
malocclusion with dental caries. This cross-sectional study included 243 children with
various mental disabilities with or without physical infirmities. The Dental Aesthetic

Review of Literature
P.M.N.M Dental College, Bagalkot 12
Index (DAI) and the dentition status were recorded using the World Health
Organization Oral Health Surveys – Basic Methods (1997) Pro-forma. The Decayed
(D), Missing (M) and Filled (F) components of the DMF index were calculated using
the Dentition Status and Treatment Need (DSTN). A Chi-square test, ANOVA, and t-
test were used to derive inferential statistics. The mean DAI score ± standard
deviation was 39.0 ± 12.3. A total of 123 (50.6%) participants (74 males and 49
females) had DAI scores of 36 and above, which indicated a handicapping
malocclusion requiring mandatory orthodontic treatment. Sixty-nine (28.4%)
adolescents (36 males and 33 females) had DAI scores between 31 and 35, which
indicated severe malocclusion, for which orthodontic intervention was desirable.
Incisal segment crowding (84.8%) was the most common aspect of the malocclusion.
The mean DMFT score was 4.36 ± 3.81, and 82.8% of the participants had a DMFT
score > 0. There was no statistically significant correlation between the mean DAI and
DMFT scores (r = 0.090, p = 0.15). Only 16 (6.6%) of the adolescents had minor or
no anomaly not needing orthodontic treatment. The prevalence of malocclusion and
dental caries was found to be high22.
Jennifer et al conducted a study to evaluate the relationship between caries and
malocclusion in the early and late mixed dentition in a population of children of
Chinese migrant workers in Shanghai. Dental charts were obtained for 646 children in
the mixed dentition, aged between 6 and 13 years old. The decayed, missing, and
filled teeth (DMFT) index and interproximal tooth structure lost due to caries (ITSLC)
were evaluated. In the early mixed dentition, overbite was more likely to be ideal in
subjects with DMFT > 0. In the late mixed dentition, crowding in both arches was
greater in subjects with DMFT > 0. In the total sample, crowding in the lower arch
only was greater in subjects with DMFT > 0. In the early mixed dentition, upper

Review of Literature
P.M.N.M Dental College, Bagalkot 13
crowding was lower in subjects with ITSLC in the upper arch and in both arches and
the rate of anterior cross-bite was higher in subjects with ITSLC in the upper arch. In
the late mixed dentition, overjet was more likely to be ideal in subjects with ITSLC in
the upper arch and upper crowding was greater in subjects with ITSLC in both arches.
In the total sample, overjet was more likely to be ideal in subjects with ITSLC in the
upper arch and lower crowding was greater in subjects with ITSLC in both arches. A
relationship exists between caries and malocclusion, and between ITSLC and
malocclusion, and some relationships may change with dental age23.
A study was conducted by Monika et al to associate the dental caries,
malocclusion and oral habits with the quality of life of preschool children. Cross-
sectional study with 93 children from three to five years of age who have or have not
been affected by untreated carious lesions were selected. Parents answered the
questionnaire on oral habits and quality of life instrument related to oral health
denominated Early Childhood Oral Health Impact Scale (B-ECOHIS). A pediatric
dentist assessed the severity of the carious lesions and the presence of occlusal
disorders. The level of significance used was 5%. The B-ECOHIS demonstrated
impact on quality of life with increasing age in the fields of symptoms, psychological
aspects, self-image and social interaction and family function. Dental caries were
shown to have an impact on the quality of life of children and their families,
especially in relation the domains of symptoms and limitations. There was no
association between malocclusion and quality of life related to oral health24.
A study was conducted by Roshan et al to assess the malocclusion status,
dentition status, and treatment needs of 15‑year‑old school children of Mangalore. A
cross‑sectional study of 1001 school children aged 15‑year‑old was conducted in
Mangalore. Their malocclusion status, dentition status, and treatment needs were

Review of Literature
P.M.N.M Dental College, Bagalkot 14
recorded using the WHO oral health assessment pro-forma. Statistical analysis was
done using Statistical Package for Social Sciences version 17. Descriptive statistics
was obtained and Chi‑square test was used. The level of significance was set at 0.05.
Decayed teeth were prevalent in 45.5% of the study subjects. Malocclusion was
present in 30% of the study subjects. Teeth missing due to caries and those requiring
extraction and prosthetic rehabilitation were significantly higher in government
schools (P < 0.05). Malocclusion and treatment need was significantly higher in
government schools (P < 0.05)25.
A study was conducted by Saurabh et al to find the relationship of orthodontic
malocclusion with periodontal status, dental caries, and sociodemographic factors.
The study population comprised 400 school‑going children of age 11–14 years. The
severity of malocclusion was determined by Treatment Priority Index. The
sociodemographic factors were evaluated using a questionnaire that enquired about
age, gender, parents’ monthly income, and their educational status. Periodontal status
was assessed using Community Periodontal Index of Treatment Need (CPITN) index.
To know about dental caries, decayed, missing, filled teeth (DMFT) index was used in
this study. Spearman’s rank correlation coefficients were used to find an association
between variables. The effect of sociodemographic factors on treatment priority index
(TPI) scores was examined using Chi‑square test. Student’s t‑test (to compare TPI
scores of different genders) and analysis of variance (to compare TPI scores among
different age groups) were used in this study. Out of a total of 400 children included
in the study, 19.5% students had normal occlusion whereas a majority of them
(80.5%) showed some sort of malocclusion. CPITN scores revealed that 3.1% pupils
had no sign of the disease, 57.5% showed gingival bleeding after gentle probing, and

Review of Literature
P.M.N.M Dental College, Bagalkot 15
39.4% had supra or subgingival calculus. No statistically significant correlation was
found between the orthodontic treatment need, periodontal status, and
sociodemographic factors while a significant relation is observed of TPI with
DMFT26.
Disha et al conducted a study to establish the prevalence of malocclusion and
its association with caries experience in 8–9‑year‑old children of Davangere city,
South Indian region. The study design was a cross‑sectional survey. A total of 800
children from 350 schools (both males and females) were randomly selected for the
study. t‑test and Chi‑square test were used for statistical analysis. The overall
prevalence of malocclusion among 8–9‑year‑old children was 40.9%. The most
prevalent malocclusion was crowding (11.5%), followed by excessive overjet (9.4%),
deep bite (6.8%), spacing (6.5%), crossbite (4.5%), and open bite (3.2%). Class I
molar relationship prevailed in 95.5% of children. The prevalence of malocclusion in
our study was in accordance with the other studies reported in India, which ranged
from 19.6% to 90%. Furthermore, correlation of malocclusion and dental caries in the
primary dentition, although nonsignificant, presented children with malocclusion to
have a higher caries experience than children without malocclusion27.
A study was conducted by Assad et al to assess the prevalence of malocclusion
and dental caries in school children, using Index of Orthodontic Treatment Need
(Dental Health Component) IOTN (DHC) and Decayed, Missing, Filled, Teeth
(DMFT) score. Also to evaluate any relationship between malocclusion/ orthodontic
treatment need and dental caries. This study was carried out on 574 school children
aged 11 to 16 years having permanent dentition, no history of orthodontic treatment
and no dental anomalies. Each student’s number of DMFT was computed and the
IOTN (DHC) was recorded based on contact point displacement only. Results of the

Review of Literature
P.M.N.M Dental College, Bagalkot 16
current study which comprised of 574 school children, with 320 males and 254
females, exhibited a mean IOTN grade of 2.4 ± 1.016 and a mean DMFT score of
2.57 ± 2.7. The prevalence of malocclusion was found to be 75.6% while the
prevalence of dental caries was 64.6%. The Pearson correlation coefficient found a
significant correlation between IOTN and DMFT scores. The brushing frequency and
gender did not correlate with DMFT scores, while sugar intake, age and SES had a
significant correlation with DMFT. Taking IOTN into consideration, age and diet
showed no correlation with it, whereas gender and Socio Economic Status (SES)
status displayed a significant correlation with IOTN grades28.
A study was conducted by Roopa et al to assess the prevalence of malocclusion
and its gender distribution among Indian school children. A cross-sectional
epidemiological survey was conducted in all the 30 districts of Karnataka, India.
School children in the age group of 10-16 years were the target population. Population
proportionate technique was employed for the sample size estimation. A total sample
of 9505 was randomly selected from 102 schools all over Karnataka, India.
Ackermann-Proffit classification of malocclusion was used to record the
malocclusion. Statistical analysis used was simple descriptive statistics. Results
obtained were: prevalence of crowding is 50.4% in boys and 51.4% in girls. Cross-
bite was reported in 17.8% and 18.3% in boys and girls, respectively. Angle’s class I
malocclusion was reported in 78.4% of boys and 80.2% of girls. Angle’s class II
malocclusion was reported in 21.5% of boys and 19.8% of girls and class III
malocclusion was observed in 0.1% of boys29.
Ciuffolo et al conducted a study to describe the prevalence and distribution, by
gender, of occlusal traits in a sample of Italian students aged 11–14 years (mean 13 ±
1 years). Using standardized and validated recording criteria, a single operator

Review of Literature
P.M.N.M Dental College, Bagalkot 17
measured the overjet, overbite, open bite, anterior and posterior crossbites, crowding,
coincidence of the upper and lower midlines, and diastema, in 810 secondary school
students (53.6 per cent males). Chi-square, t-test statistics, and odds ratios (ORs) with
95 per cent confidence intervals (CI) were used to investigate the relationship between
gender and malocclusion characteristic. Logistic regression was used to further
analyse the independent association between gender and each outcome measure.
Ninety-three per cent of the subjects showed at least one occlusal trait, with one or
two anomalies recorded in 63 per cent of children. The prevalence of occlusal traits
ranged from 1.1 (negative overjet) to 54 per cent (upper and lower midlines not
coincident). Males were more likely than females to show both an increased overbite
and an increased overjet, although the latter result was not confirmed by logistic
regression (P = 0.05). Multivariate analysis showed a negative association between
overbite and misalignment of the lower incisors and lack of coincidence of the upper
and lower midlines, whereas subjects with an increased overbite were more likely to
have an increased overjet (all P < 0.01)30.
Tiziano et al conducted a study which evaluated gender differences in the
cephalometric records of a large-scale cross-sectional sample of Caucasian subjects
with Class III malocclusion at different developmental ages. The purpose also was to
provide average age-related and sex-related data for craniofacial measures in
untreated Class III subjects that are used as reference in the diagnostic appraisal of the
patient with Class III disharmony. The sample examined consisted of 1094
pretreatment lateral cephalometric records (557 female subjects and 537 male
subjects) of Caucasian Class III individuals. The age range for female subjects was
between 3 years six months and 57 years seven months. The male subject group
ranged from 3 years three months to 48 years five months. Twelve age groups were

Review of Literature
P.M.N.M Dental College, Bagalkot 18
identified. Skeletal maturity at different age periods also was determined using the
stage of cervical vertebral maturation. Gender differences for all cephalometric
variables were analyzed using parametric statistics. The findings of the study
indicated that Class III malocclusion is associated with a significant degree of sexual
dimorphism in craniofacial parameters, especially from the age of 13 onward. Male
subjects with Class III malocclusion present with significantly larger linear
dimensions of the maxilla, mandible, and anterior facial heights when compared with
female subjects during the circum-pubertal and post-pubertal periods31.
A study was conducted by Ibrahim et al to describe the prevalence of
malocclusion in a population of Central Anatolian adolescents in relation to gender.
The sample comprised 2329 teenagers (1125 boys and 1204 girls), aged between 12
and 17 years (mean age: 14.6 yrs). Occlusal anteroposterior relationships were
assessed using the Angle classification. Other variables examined were overjet,
overbite, crowding, midline diastema, posterior crossbite, and scissors bite. The
results showed that about 10.1% of the subjects had normal occlusions, 34.9% of the
subjects had Class I malocclusions, 40.0% had Class II Division 1 malocclusions,
4.7% had Class II Division 2 malocclusions and 10.3% had Class III malocclusions.
Over 53.5% had normal overbites, and 18.3%, 14.4%, 5.6%, and 8.2% had increased,
reduced, edge-to-edge or anterior open bite values, respectively. Overjet relationship
was normal in 58.9%, increased in 25.1%, reversed in 10.4%, and edge-to-edge in
5.6%. A posterior crossbite registered in 9.5% and scissors bite in 0.3%. Anterior
crowding was present in 65.2% of the sample and midline diastema in 7.0%. No clear
gender differences were noted, except for normal overbite (most frequent in girls,
P<.001) and increased overbite (most frequent in boys, P<.05). Class II Division 1

Review of Literature
P.M.N.M Dental College, Bagalkot 19
malocclusion is the most prevalent occlusal pattern among the Central Anatolian
adolescents and the high values (25.1% and 18.3%) of increased overjet and overbite
were a reflection of the high prevalence of Class II malocclusion32.
A study was conducted by Yuko et al to describe the prevalence and perform a
gender comparison of malocclusion requiring orthodontic treatment in Japan. On the
basis of the index of orthodontic treatment need, occlusal characteristics of a
population-based sample of adolescents (ages 12-15 years) were evaluated by
orthodontists. A total of 821 adolescents participated in this study. The prevalence of
malocclusion was 46.5%. Multivariate logistic regression indicated that girls were
1.56 times more likely than boys to develop malocclusion, particularly with anterior
crossbite and upper and lower crowding33.
Mridula et al conducted a study to assess the prevalence of malocclusion and
orthodontic treatment needs among 12‑15 years old school children of Udaipur, India.
A cross‑sectional descriptive survey was conducted among 887 subjects aged 12‑15
years. The prevalence of malocclusion and orthodontic treatment needs was assessed
using dental aesthetic index (World Health Organization, 1997). General information
on demographic data was also recorded. Chi‑square test, analysis of variance and
Scheffe’s test were employed for statistical analysis. Malocclusion and orthodontic
treatment need was reported among 33.3% of the study subjects. A significant age and
gender difference depicting preponderance among younger age group and a male
proclivity was experiential. A significant improvement in anterior crowding and
largest anterior maxillary irregularity with age was documented. Males had a
significantly higher prevalence of anterior crowding, midline diastema and largest
anterior maxillary irregularity than females. The prevalence of malocclusion and

Review of Literature
P.M.N.M Dental College, Bagalkot 20
orthodontic treatment needs among school children of Udaipur city, Rajasthan, India
was found to be 33.3%34.
A study was conducted by Bushra et al to explore the relationship of ABO
blood groups with classes of malocclusion and relative prevalence of these characters
in males and females of a defined population. The current study was performed on
500 individuals with an age range of 15 to 45 years, along with permanent dentition
only, reporting to the department of orthodontics of Punjab dental hospital, Lahore.
Complete details about the classes of malocclusion and blood group of the subjects
were noted in accordance with the ABO blood group system. The sample was divided
into three groups, i.e., Class I, Class II, and Class III. Data were analyzed statistically
by using SPSS 21.0. Pearson Chi-square was used as statistical analysis to get the
association of classes of malocclusion with blood group type. A significant difference
between the prevalence of classes of dental malocclusion in relation to blood group
types was found among both genders. There was gender wise association difference
between the classes of dental malocclusion and blood group types. The study also
covered the gender wise prevalence of dental malocclusion in all the four blood
groups which are A, B, AB and O35.

Methodology
P.M.N.M Dental College, Bagalkot 21
METHODOLOGY
SOURCE OF THE DATA
Data regarding 90 children of both sexes, of the age group 6 to 14 years, those
who reported to the Department of Pedodontics and Preventive dentistry, P.M.N.M
Dental College, Bagalkot was taken after obtaining written consent from parents.
GENERAL INCLUSION AND EXCLUSION CRITERIA
Inclusion criteria:
1. Children willing to participate in the study.
2. Normal healthy children visiting for routine dental treatment.
3. Written consent was obtained from the Parents/ Guardians
4. Children of the age group 6 to 14 years.
5. Children without history of any systemic disorder, infectious diseases.
Exclusion criteria:
1. Children who were not willing to participate in the study.
2. Children suffering from any systemic disease or with any history of illness.
3. Children whose parents were not willing to give the written consent.

Methodology
P.M.N.M Dental College, Bagalkot 22
MATERIALS:
Mouth mirror and probe
Lipstick
Child safe lipstick-scotch tape
Black duplicating ink
Cotton swab
White bond paper
Clipping board
Magnifying glass lens
METHODS OF COLLECTING DATA:
Ninety children of age group of 6 - 14 years reporting to the Department of
Pediatric and Preventive Dentistry, P.M.N.M. Dental College and Hospital, Bagalkot
for routine dental check-up and treatment were considered for the study. After
obtaining the consent from the parents, these children were grouped based on
examining lateral cephalograms obtained from them. ANB angle, WITS appraisal and
Beta angle were calculated for each cephalograms to assess the anteroposterior jaw
position. Keeping the norms into consideration, the children were grouped as:
Group A - consisting of 30 children with skeletal Class-I malocclusion.
Group B - consisting of 30 children with skeletal Class-II malocclusion.
Group C - consisting of 30 children with skeletal Class-III malocclusion.

Methodology
P.M.N.M Dental College, Bagalkot 23
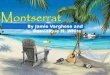
Lip prints in each group were taken using child safe lipstick-scotch tape
method. Magnifying glass lens was used for the analysis of lip prints. The field of
observation was restricted to middle thirds of both upper and lower lips. All lip print
analyses were done by an observer who was blinded in relation to clinical
examination and cephalometric analysis of the patient. The lip print patterns were
classified according to the Suzuki and Tsuchihashi’s classification system10, 36. The lip
print pattern was determined by counting highest number of lines in the study area
having similarity to the Suzuki Tsuchihashi classification.
Figure 1: Suzuki and Tsuchihashi’s classification system
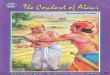
Finger prints (right and left) of the subjects were recorded using black
duplicating ink, which was applied on the fingers with cotton swab. First, the
subjects’ hands were cleaned with soap and water prior to recording their fingerprints
to remove dirt, oily secretions, and sweat and then dried with a towel. In taking the
rolled impressions of the individual fingers, the fingertip was placed at right angles to
the surface of the plate. Next, the finger was rolled or turned until the tip faced the
opposite direction. The finger was then placed on white paper and rolled in the same
manner to obtain a clean rolled impression of the finger pattern. The finger print

Methodology
P.M.N.M Dental College, Bagalkot 24
patterns were analyzed for various dermatoglyphic patterns including the arch, loop,
and whorl patterns.
Figure 2: Dermatoglyphic patterns
Prevalence of dental caries was measured by DMF teeth index (DMFT) which
was introduced by Klein, Palmer and Knutson in 193837.
The criteria for DMFT score included 3 components:
1) D component: Used to describe Decayed teeth
2) M component: Used to describe Missing teeth due to caries
3) F component: Used to describe Filled teeth due to caries
Then DMFT score of an individual will be calculated by a formula:
DMFT = D + M + F
Maximum score: DMFT = 32; Minimum score = Zero
Prevalence of the type of skeletal malocclusion in boys and girls were evaluated
and compared.

Sample size estimation
P.M.N.M Dental College, Bagalkot 25
SAMPLE SIZE ESTIMATION
Analysis: Descriptive and analytical statistics will be done. The normality of data will
be tested by Shapiro-Wilk test. If the data followed normal distribution parametric
tests (one-way ANOVA) will be used and if the data does not follow normal
distribution non-parametric test (Kruskal-Wallis) will be used. The chi-square test
will be used to check differences in proportions.
Statistical Software: SPSS (Statistical Package for Social Sciences) Version 20.1
(IBM Corporation, Chicago, USA)
Sample Size Calculation Software: N Master, V.2.0, CMC Vellor, India
Sample Size Calculation:
Minimum sample size calculated for your study is 23 in each of the three groups –
Class I, II and III. You can take sample size of 30 in each group considering loss of
data or follow up. The sample size calculations according to Divyashree et al (2016)
are as follows:
Table-1: Sample size
Sample size
Group I 23
Group II 23
Total 46
Table-2: Study parameters
Study parameters
Mean, Group I 107.85
Mean, Group II 138.8
Alpha 0.05
Beta 0.2
Power 0.8

Sample size estimation
P.M.N.M Dental College, Bagalkot 26

Results
P.M.N.M Dental College, Bagalkot 27
RESULTS
Table 3: Age and Gender distribution among study subjects
Table 4: Comparison of different types of Lip Print Patterns among study
subjects between three skeletal malocclusions using Chi Square Test
Comparison of different types of Lip Print Patterns among study subjects between 03 skeletal
malocclusions using Chi Square Test
Lip Print Patterns
Class I Class II Class III
c2 Value P-Value n % n % n %
Type I 10 33.3% 1 3.3% 1 3.3%
26.400 0.009*
Type II 14 46.7% 21 70.0% 25 83.4%
Type III 0 0.0% 2 6.7% 1 3.3%
Type I & II 3 10.0% 2 6.7% 0 0.0%
Type I & III 0 0.0% 1 3.3% 2 6.7%
Type II & III 2 6.7% 3 10.0% 1 3.3%
Type I, II, III & IV 1 3.3% 0 0.0% 0 0.0%
Note: Multiple Lip patterns have been distributed in Upper and Lower Lips
*-Statistically Significant
Table 5: Comparison of different types of Finger Print Patterns among study
subjects between three skeletal malocclusions using Chi Square Test
Comparison of different types of Finger Print Patterns among study subjects between 03 skeletal
malocclusions using Chi Square Test
Finger Print Patterns
Class I Class II Class III
c2 Value P-Value n % n % n %
Arch 0 0.0% 0 0.0% 1 3.3%
26.781 0.003*
Loop 9 30.0% 3 10.0% 16 53.5%
Whorl 11 36.7% 18 60.0% 4 13.3%
Arch & Loop 1 3.3% 0 0.0% 4 13.3%
Loop & Whorl 8 26.7% 8 26.7% 4 13.3%
Arch, Loop & Whorl 1 3.3% 1 3.3% 1 3.3%
*-Statistically Significant
Age and Gender distribution among study
subjects
Variables Category n %
Age 6-9 yrs 16 17.8%
10-13 yrs 74 82.2%
Mean SD
Mean & SD 10.9 1.7
Range 6 - 13
Sex Males 57 63.3%
Females 33 36.7%

Results
P.M.N.M Dental College, Bagalkot 28
Table 6: Comparison of mean DMFT / deft scores between different types of
Skeletal malocclusion using Kruskal Wallis Test
*-Statistically Significant
Table 7: Multiple comparison of mean difference in the DMFT/deft scores b/w
different skeletal malocclusions using Mann Whitney Post hoc Test
Multiple comparison of mean difference in the DMFT/deft scores b/w
different skeletal malocclusions using Mann Whitney Post hoc Test
(I) Groups (J) Groups
Mean Diff.
(I-J)
95% CI for the
Diff.
P-Value Lower Upper
Class I Class II -0.27 -1.25 0.71 0.79
Class III -1.80 -2.78 -0.82 <0.001*
Class II Class III -1.53 -2.51 -0.55 0.001*
*-Statistically Significant
Table 8: Comparison of prevalence of Skeletal Malocclusion based on different
age and gender of study subjects using Chi Square Test
Comparison of prevalence of Skeletal Malocclusion based on different age and gender of study subjects using
Chi Square Test
Variables Categories
Class I Class II Class III
c2 Value P-Value n % n % n %
Age Group 6-9 yrs 8 50.0% 2 12.5% 6 37.5% 4.257 0.12
10-13 yrs 22 29.7% 28 37.9% 24 32.4%
Sex Males 15 26.3% 19 33.3% 23 40.4% 4.593 0.10
Females 15 45.5% 11 33.3% 7 21.2%
Comparison of mean DMFT / deft scores between different types of Skeletal
malocclusion using Kruskal Wallis Test
Sk. Malocclusions N Mean SD Min Max P-Value
Class I 30 1.80 1.27 0 5
<0.001* Class II 30 2.07 1.36 0 5
Class III 30 3.60 2.03 0 10

Results
P.M.N.M Dental College, Bagalkot 29
Table 9: Correlation between different Lip and Finger Print Patterns in Skeletal
Class I Malocclusion using Chi Square Test
Correlation between different Lip and Finger Print Patterns in Skeletal Class I Malocclusion
using Chi Square Test
Lip Print Patterns Arch Loop Whorl
Arch &
Loop
Loop &
Whorl
Arch, Loop &
Whorl
Type I 0 5 2 0 3 0
Type II 0 3 7 1 2 1
Type III 0 0 0 0 0 0
Type I & II 0 0 1 0 2 0
Type I & III 0 0 0 0 0 0
Type II & III 0 0 1 0 1 0
Type I, II, III & IV 0 1 0 0 0 0
Χ2 Value - 12.326; P-Value - 0.72
Table 10: Correlation between different Lip and Finger Print Patterns in
Skeletal Class II Malocclusion using Chi Square Test
Correlation between different Lip and Finger Print Patterns in Skeletal Class II
Malocclusion using Chi Square Test
Lip Print Patterns Arch Loop Whorl
Arch &
Loop
Loop &
Whorl
Arch, Loop &
Whorl
Type I 0 0 1 0 0 0
Type II 0 3 13 0 4 1
Type III 0 0 1 0 1 0
Type I & II 0 0 0 0 2 0
Type I & III 0 0 1 0 0 0
Type II & III 0 0 2 0 1 0
Type I, II, III & IV 0 0 0 0 0 0
X2 Value - 8.998; P-Value - 0.88

Results
P.M.N.M Dental College, Bagalkot 30
Table 11: Correlation between different Lip and Finger Print Patterns in
Skeletal Class III Malocclusion using Chi Square Test
Correlation between different Lip and Finger Print Patterns in Skeletal Class III
Malocclusion using Chi Square Test
Lip Print Patterns Arch Loop Whorl
Arch &
Loop
Loop &
Whorl
Arch, Loop &
Whorl
Type I 0 1 0 0 0 0
Type II 1 13 3 3 4 1
Type III 0 1 0 0 0 0
Type I & II 0 0 0 0 0 0
Type I & III 0 0 1 1 0 0
Type II & III 0 1 0 0 0 0
Type I, II, III & IV 0 0 0 0 0 0
X2 Value - 8.400; P-Value - 0.98
Graph 1: Age-wise distribution of study subjects

Results
P.M.N.M Dental College, Bagalkot 31
Graph 2: Gender-wise distribution of study subjects
Graph 3: Lip Print Patterns among study subjects between three skeletal malocclusions

Results
P.M.N.M Dental College, Bagalkot 32
Graph 4: Finger Print Patterns among study subjects between three skeletal
malocclusions
Graph 5: Mean DMFT/deft scores between different types of Skeletal
malocclusions

Results
P.M.N.M Dental College, Bagalkot 33
Graph 6: Age-wise Prevalence of different types of skeletal malocclusions
Graph 7: Gender-wise Prevalence of different types of skeletal malocclusions

Results
P.M.N.M Dental College, Bagalkot 34
Graph 8: Correlation between different lip and finger print patterns in Skeletal
Class I Malocclusion
Graph 9: Correlation between different lip and finger print patterns in Skeletal
Class II Malocclusion

Results
P.M.N.M Dental College, Bagalkot 35
Graph 10: Correlation between different lip and finger print patterns in Skeletal
Class III Malocclusion
1. Distribution and Comparison of age and gender among various study subjects
(Table 3, Graph 1 & 2)
A total of 90 children were taken for the study and they were divided into 3 groups of
30 members each. Age of the children were categorized into 6-9 years and 10-13
years, respectively. The number of children in 6-9 years group was 16 and the number
of children in 10-13 years group was 74. This was due to the inclusion of children
who visited the department for the treatment. The mean age of children considered for
the study was 10.9 with a standard deviation of 1.7, of which 57 were males i.e.
63.3% and 33 were females i.e. 36.7%.

Results
P.M.N.M Dental College, Bagalkot 36
2. Comparison of different types of Lip Print Patterns among study subjects
between three skeletal malocclusions using Chi Square Test (Table 4, Graph 3)
Among 30 children grouped under Class I malocclusion: Type I lip pattern was shown
by 10 (33.3%), Type II lip pattern was shown by 14 (46.7%), Type I & II lip pattern
was shown by 3 (10%), Type II & III was shown by 2 (6.7%) and Type I,II,III & IV
was shown by 1 (3.3%).
Among 30 children grouped under Class II malocclusion: Type I lip pattern was
shown by 1 (3.3%), Type II lip pattern was shown by 21 (70%), Type III lip pattern
was shown by 2 (6.7%), Type I & II lip pattern was shown by 2 (6.7%), Type I & III
lip pattern was shown by 1 (3.3%) and Type II & III was shown by 3 (10%).
Among 30 children grouped under Class III malocclusion: Type I lip pattern was
shown by 1 (3.3%), Type II lip pattern was shown by 25 (83.4%), Type III lip pattern
was shown by 1 (3.3%), Type I & III lip pattern was shown by 2 (6.7%) and Type II
& III was shown by 1 (3.3%).
Multiple lip print patterns have been distributed in upper and lower lips with a p-value
of 0.009 showing statistical significance.
3. Comparison of different types of Finger Print Patterns among study subjects
between three skeletal malocclusions using Chi Square Test (Table 5, Graph 4)
Among 30 children grouped under Class I malocclusion: 9 (30%) showed loop
pattern, 11 (36.7%) showed whorl pattern, 1 (3.3%) showed arch and loop pattern, 8
(26.7%) showed loop and whorl pattern and 1 (3.3%) showed arch, loop and whorl
pattern.

Results
P.M.N.M Dental College, Bagalkot 37
Among 30 children grouped under Class II malocclusion: 3 (10%) showed loop
pattern, 18 (60%) showed whorl pattern, 8 (26.7%) showed loop and whorl pattern
and 1 (3.3%) showed arch, loop and whorl pattern.
Among 30 children grouped under Class III malocclusion: 1 (3.3%) showed arch
pattern, 16 (53.5%) showed loop pattern, 4 (13.3%) showed whorl pattern, 4 (13.3%)
showed arch and loop pattern, 4 (13.3%) showed loop and whorl pattern and 1 (3.3%)
showed arch, loop and whorl pattern.
The p-value obtained was 0.003 showing statistical significance.
4. Comparison of mean DMFT / deft scores between different types of Skeletal
malocclusion using Kruskal Wallis Test (Table 6 & 7, Graph 5)
Thirty children grouped under Class I malocclusion showed a mean DMFT/deft score of 1.8
with a standard deviation of 1.27, 30 children grouped under Class II malocclusion showed a
mean DMFT/deft score of 2.07 with a standard deviation of 1.36 and 30 children grouped
under Class III malocclusion showed a mean DMFT/deft score of 3.6 with a standard
deviation of 2.03.
The P-value obtained was <0.001 showing statistical significance.
5. Comparison of prevalence of Skeletal Malocclusion based on different age and
gender of study subjects using Chi Square Test (Table 8, Graph 6 & 7)
Among children grouped under 6-9 years: 8 (50%) showed Class I malocclusion, 2
(12.5%) showed Class II malocclusion and 6 (37.5%) showed Class III malocclusion.
Among children grouped under 10-13 years: 22 (29.7%) showed Class I
malocclusion, 28 (37.9%) showed Class II malocclusion and 24 (32.4%) showed
Class III malocclusion. P-value obtained was 0.12, showing statistical insignificance.

Results
P.M.N.M Dental College, Bagalkot 38
Among 90 children: 15 (26.3%) males; 15 (45.5%) females showed Class I
malocclusion, 19 (33.3%) males; 11 (33.3%) females showed Class II malocclusion
and 23 (40.4%) males; 7 (21.2%) females showed Class III malocclusion. P-value
obtained was 0.10, showing statistical insignificance.
6. Correlation between different lip and finger print patterns in Skeletal Class I
Malocclusion (Table 9, Graph 8)
Among 10 children having Type I lip print pattern, the finger print pattern was: 5 had loop
pattern, 2 had whorl pattern and 3 had loop and whorl pattern.
Among 13 children having Type II lip print pattern, the finger print pattern was: 3 had loop
pattern, 7 had whorl pattern, 1 had arch and loop pattern, 2 had loop and whorl pattern and 1
had arch, loop and whorl pattern.
Among 3 children having Type I & II lip print pattern, the finger print pattern was: 1 had
whorl pattern and 2 had loop and whorl pattern.
Among 2 children having Type II & III lip print pattern, the finger print pattern was: 1 had
whorl pattern and 1 had loop and whorl pattern.
1 child having Type I,II,III & IV lip print pattern, showed loop finger print pattern.
P-value obtained was 0.72, showing statistical insignificance.
7. Correlation between different lip and finger print patterns in Skeletal Class II
Malocclusion (Table 10, Graph 9)
1 child having Type I lip print pattern, showed whorl finger print pattern.
Among 21 children having Type II lip print pattern, the finger print pattern was: 3 had loop
pattern, 13 had whorl pattern, 4 had loop and whorl pattern and 1 had arch, loop and whorl
pattern.

Results
P.M.N.M Dental College, Bagalkot 39
Among 2 children having Type III lip print pattern, the finger print pattern was: 1 had whorl
pattern and 1 had loop and whorl pattern.
Among 2 children having Type I & II lip print pattern, the finger print pattern was loop and
whorl pattern.
1 child having Type I & III lip print pattern, showed whorl finger print pattern.
Among 3 children having Type II & III lip print pattern, the finger print pattern was: 2 had
whorl pattern and 1 had loop and whorl pattern.
P-value obtained was 0.88, showing statistical insignificance.
8. Correlation between different lip and finger print patterns in Skeletal Class
III Malocclusion (Table 11, Graph 10)
1 child having Type I lip print pattern, showed loop finger print pattern.
Among 25 children having Type II lip print pattern, the finger print pattern was: 1 had arch
pattern, 13 had loop pattern, 3 had whorl pattern, 3 had arch and loop pattern, 4 had loop and
whorl pattern and 1 had arch, loop and whorl pattern.
1 child having Type III lip print pattern, showed loop finger print pattern.
Among 2 children having Type I & III lip print pattern, the finger print pattern was: 1 had
whorl pattern and 1 had arch and loop pattern.
1 child having Type II & III lip print pattern, showed loop finger print pattern.
P-value obtained was 0.98, showing statistical insignificance.

Discussion
P.M.N.M Dental College, Bagalkot 40
DISCUSSION
Malocclusion is one of the most common dental problems like dental caries,
periodontal disease, and dental fluorosis9. If a malocclusion is identified early, simple,
preventive and interceptive measures can alleviate a developing malocclusion. The
incidence of various categories of malocclusion in a particular population is necessary
to provide a basis for planning preventive and interceptive orthodontics29.
In 1950, Synder reported in his book Homicide Investigation that the
characteristics of the lips formed by lip grooves are as individually distinctive as the
ridge characteristics of finger prints38. Suzuki, in 1967, made detailed investigations
of the measurement of the lips, the use and color of rugae, and the method for its
extraction to obtain useful data for practical forensic application39. McDonell in 1972
conducted a study on lip prints between two identical twins and reported that two
identical twins seemed to be indistinguishable by every other means but their lip
prints were different40. Lip prints are established at a very early period in comparison
to sagittal jaw relation and dental relation41, 42. Establishing a correlation between
sagittal jaw relation and lip prints would benefit the clinician by predicting the type of
malocclusion and can also provide additional information on individual personal
identity12.
Cummins and Midlo (1929) defined dermatoglyphics as the study of the
intricate dermal ridge configuration on the skin covering the palmar and plantar
surfaces of the hands and feet43. Dermal configurations appear during the 12th week
of intrauterine life and are completely established by the 24th week and remain
constant throughout life, except for overall size44, 45. Finger and palm prints and facial
structures such as the lip, alveolus, and palate develop during the same embryonic
period. Therefore, any factor causing changes in the lip, alveolus, and palate may also

Discussion
P.M.N.M Dental College, Bagalkot 41
cause different patterns in the appearance of finger and palm prints. Fingerprint
patterns and other characteristics of dermal ridges offer distinct advantages and may
be used as a screening tool to detect early malocclusion15.
Dental caries is an important dental public health problem, and it is the most
prevalent oral disease among children in the world. The prevalence pattern of dental
caries not only varies with age, sex, socioeconomic status, race, geographical location,
food habits, and oral hygiene practices but also within the oral cavity46. Dental caries
is the most prevalent dental affliction of childhood. Despite credible scientific
advances and the fact that caries is preventable, the disease continues to be a major
public health problem47. The relationship between caries and malocclusion has been
debated for decades. Despite ongoing research, no definitive studies have been
performed48, 49. The relationship between caries and specific types of malocclusion is
even more poorly defined. A better understanding of this potential relationship would
be beneficial to orthodontists, pediatric dentists and general dentists which would aid
in the diagnosis and treatment of malocclusion23.
Malocclusions are the result of orofacial adaptability to various etiological
factors50, which result in various implications such as psychosocial problems related
to impaired dento-facial aesthetics, disturbances of oral function, such as mastication,
swallowing and speech and greater susceptibility to trauma and periodontal disease9.
A number of studies have demonstrated its impact on quality‑of‑life51, 52. Since the
public equates good dental appearance with success in many pursuits and societal
forces define the norms for acceptable, normal and attractive physical appearance, an
individual with malocclusion might develop a feeling of shame about their dental
appearance and may feel shy in social situations or lose career opportunities.
According to World Health Organization (WHO), the main oral diseases should be

Discussion
P.M.N.M Dental College, Bagalkot 42
subjected to periodic epidemiological surveys. The epidemiological data on
orthodontic treatment need is of interest for dental public health programs, clinical
treatment, screening for treatment priority, resource planning and third party
funding50. Appraisal of gender-wise distribution of malocclusion in childhood can
facilitate efforts to prevent such a disorder and its consequences and make it possible
to reduce the complexity of costly orthodontic treatment. Furthermore, this knowledge
might help to minimize or eliminate future treatment need34.
The mixed dentition is the time of greatest opportunity for occlusal guidance,
especially in cases of malocclusion. As uninterrupted growth might further complicate
the condition in the permanent dentition, an appropriate diagnosis at an early stage
becomes necessary. Any relation between the dermatoglyphic, cheiloscopic patterns
and skeletal jaw relation might aid in the early diagnosis and interception of the
condition and also might be helpful in future forensic research. There exists a
deficiency in studies carried on samples of pediatric age group, hence it is necessary
to conduct a study to investigate the dermatoglyphic and cheiloscopic patterns, along
with assessment of prevalence of dental caries and type of skeletal malocclusion in
boys and girls of age group 6-14 years.
In this study, 90 children of age group of 6 - 14 years reporting to the
Department of Pediatric and Preventive Dentistry, P.M.N.M. Dental College and
Hospital, Bagalkot for routine dental check-up and treatment were selected and
divided into 3 groups, by examining the lateral cephalograms obtained from them, as:
Group A - consisting of 30 children with skeletal Class-I malocclusion.
Group B - consisting of 30 children with skeletal Class-II malocclusion.
Group C - consisting of 30 children with skeletal Class-III malocclusion.

Discussion
P.M.N.M Dental College, Bagalkot 43
For the groups:
Lip-prints were taken using child safe lipstick-scotch tape method on the bond
paper, without any distortion.
Finger prints (right and left) of the subjects were recorded using black
duplicating ink, which were applied on the fingers with cotton swab. The
digits were guided and pressed firmly against the white bond paper clipped on
to a board.
The lip print patterns were classified according to Suzuki and Tsuchihashi’s
classification system10, 36 and finger print patterns were classified into arch,
whorl and loop patterns.
Presence of dental caries were assessed by deft/DMFT index.
Prevalence of the type of skeletal malocclusion in boys and girls were
evaluated.
In the course of the present study it was observed that the full thickness of the
lips could not always be recorded in patients with various malocclusions due to the
skeletal prognathism or retrognathism. Therefore, both upper and lower lips were
studied for each patient. This is in contrast with the study conducted by
Sivapathasundharam et al., (2001) in which they suggested to study the lip print
pattern in the middle part of lower lip up to 10 mm wide53. Mamandras A. H et al.,
(1988) observed the lips reach their maturity in late adolescence54. Therefore in the
present study the field of observation was restricted to middle thirds of both upper and
lower lips.
In this study, Type II (branched) pattern was the most predominant lip print
pattern and multiple lip print patterns have been distributed in upper and lower lips

Discussion
P.M.N.M Dental College, Bagalkot 44
with a p-value of 0.009 showing statistical significance (Table 4, Graph 3). This was
in accordance with the studies conducted by Pradeep Raghav et al3 and Vignesh et
al13. This was in contrast with the study conducted by Sujatha Ponnusamy et al12
which showed that vertical pattern was the most prevalent lip print pattern among
Class-I and Class-II skeletal malocclusions. This might be due to the reason that the
parameters considered in the present study were different from the above mentioned
contrast study.
In the present study, predominant lip print patterns which related to the
skeletal malocclusions were as follows: Type I (vertical) pattern for Class-I
malocclusion, Type II (branched) and Type III (intersected) pattern for Class-II
malocclusion and Type I (vertical) and Type III (intersected) pattern for Class-III
malocclusion (Table 4, Graph 3). This was in accordance with the study conducted
by Pradeep Raghav et al3. This was in contrast with the study conducted by Shivani et
al10 who concluded that combination of lip print patterns were predominant in skeletal
class III group of individuals. This contrast might be due to the reason that the above
mentioned study had only considered the Class-III skeletal malocclusion and
compared its correlation with lip print patterns.
In this study, whorl pattern was the most predominant lip print pattern among
Class I and Class II malocclusion and loop pattern among Class-III malocclusion with
a p-value of 0.003 showing statistical significance (Table 5, Graph 4). This was in
accordance with the studies conducted by Susha et al19 and Smitha et al21.
In the present study, predominant finger print patterns which related to the
skeletal malocclusions were as follows: Loop pattern for Class-I malocclusion, Loop
and Whorl pattern for Class-II malocclusion and Whorl pattern for Class-III

Discussion
P.M.N.M Dental College, Bagalkot 45
malocclusion (Table 5, Graph 4). This was in contrast with the studies conducted by
Sonika et al15, who concluded that loop pattern was more frequent in patients with
skeletal Class I and II malocclusion, and the whorl pattern was more frequent in those
with Class-III malocclusion. This might be because the previous study was based on
Angle’s classification of malocclusion and in the current study skeletal malocclusion
was considered.
In the present study it was also noticed that the correlation of cheiloscopic
patterns with the skeletal malocclusion is more comparable than the dermatoglyphic
patterns obtained among the study groups (Table 9,10,11; Graph 8,9,10). Hence, by
obtaining these patterns, it is easier to predict the type of skeletal malocclusions and
an early intervention can be achieved. Collection of the data containing cheiloscopic
and dermatoglyphic patterns can be also used in forensics in the future.
In this study, DMFT scores and standard deviations obtained for each group
are as follows: 1.8 and 1.27 for Class-I malocclusion; 2.07 and 1.36 for Class-II
malocclusion; 3.6 and 2.03 for Class-III malocclusion. P-value obtained was <0.001,
which was statistically significant (Table 6 & 7, Graph 5). This proves that as the
malocclusion becomes severe, there is increased prevalence of dental caries. This was
in accordance with the studies conducted by Assad et al28 and Patil et al27, who
concluded that children with malocclusion, have a higher caries experience than
children without malocclusion. This is due to the occlusal mishaps caused by the
skeletal malocclusions. Hence maintaining of oral hygiene becomes more
cumbersome, leading to increased susceptibility to dental caries.
In the present study, age of the children were categorized into 6-9 years and
10-13 years, respectively. Among these two age ranges, 6-9 years showed increased

Discussion
P.M.N.M Dental College, Bagalkot 46
prevalence of Class-I malocclusion followed by Class III and II malocclusions,
whereas 10-13 years showed increased prevalence of Class-II malocclusion followed
by Class III and I malocclusions. P-value obtained was 0.12 (Table 8, Graph 6). This
showed that, only as the age increases the skeletal pattern becomes more evident.
Hence an early diagnosis with the specific chelioscopic and dermatoglyphic patterns
of skeletal malocclusion can allow the clinician to plan the treatment at an early stage.
This was in accordance with the study conducted by Tiziano et al31, who concluded
that malocclusion is associated with a significant degree of sexual dimorphism in
craniofacial parameters, especially from the age of 13 onwards. The results obtained
in this present study was in contrast with the study conducted by Mridula et al34, who
concluded that a significant improvement in anterior crowding and largest anterior
maxillary irregularity is seen with increase in age. This might be because the previous
study considered more parameters like crowding, spacing, etc. compared to the
present study which only focused on skeletal malocclusion.
In the current study gender prevalence of skeletal malocclusion was also taken
as a parameter and the results showed that males had an increased prevalence of Class
II and III malocclusions compared to females (Table 8, Graph 7). This was in
accordance with the study conducted by Fabio et al30. This was in contrast with the
study conducted by Komazaki et al33, who concluded that Multivariate logistic
regression indicated that girls were 1.56 times more likely than boys to develop
malocclusion. This might be because the previous study considered parameters like
anterior crossbite, upper and lower crowding, etc. which were not considered in the
present study.
This study highlights the scope of early diagnosis of skeletal malocclusions
through the chelioscopic and dermatoglyphic patterns which are unique for each

Discussion
P.M.N.M Dental College, Bagalkot 47
individual and the prevalence of dental caries which also must be considered as an
entity to be sorted out with the preventive and therapeutic measures. This study also
brought out the prevalent patterns observed among each group of skeletal
malocclusions which can group out children at an earlier stage, even before the
clinical manifestations arise. Hence, early diagnosis and treatment planning can give a
clinician with ways of treating such malocclusions at a faster rate.
The limitations of the study was smaller sample size which can be rectified by
further research with a larger sample size and taking into consideration the varied
ethnic background for conclusive results regarding association of chelioscopic and
dermatoglyphic patterns with different skeletal malocclusions.

Conclusion
P.M.N.M Dental College, Bagalkot 48
CONCLUSION
Ninety children of age group of 6 - 14 years reporting to the Department of
Pediatric and Preventive Dentistry, P.M.N.M. Dental College and Hospital, Bagalkot
for routine dental check-up and treatment were considered for the study. After
obtaining the consent from the parents, these children were grouped based on
examining lateral cephalograms obtained from them. ANB angle, WITS appraisal and
Beta angle were calculated for each cephalograms to assess the anteroposterior jaw
position. Keeping the norms into consideration, the children were grouped as:
Group A - consisting of 30 children with skeletal Class-I malocclusion.
Group B - consisting of 30 children with skeletal Class-II malocclusion.
Group C - consisting of 30 children with skeletal Class-III malocclusion.
For the groups:
Lip-prints were taken using child safe lipstick-scotch tape method on the bond
paper, without any distortion.
Finger prints (right and left) of the subjects were recorded using black
duplicating ink, which were applied on the fingers with cotton swab. The
digits were guided and pressed firmly against the white bond paper clipped on
to a board.
The lip print patterns were classified according to Suzuki and Tsuchihashi’s
classification system10, 36 and finger print patterns were classified into arch,
whorl and loop patterns.
Presence of dental caries were assessed by deft/DMFT index.

Conclusion
P.M.N.M Dental College, Bagalkot 49
Prevalence of the type of skeletal malocclusion in boys and girls were
evaluated.
The results obtained were grouped, tabulated, compared and subjected to
appropriate statistical evaluation.
Within the limitations of this study, the following conclusions were drawn:
1. Predominant lip print patterns which related to the skeletal malocclusions were
as follows: Type I (vertical) pattern for Class-I malocclusion, Type II
(branched) and Type III (intersected) pattern for Class-II malocclusion and
Type I (vertical) and Type III (intersected) pattern for Class-III malocclusion.
2. Predominant finger print patterns which related to the skeletal malocclusions
were as follows: Loop pattern for Class-I malocclusion, Loop and Whorl
pattern for Class-II malocclusion and Whorl pattern for Class-III malocclusion.
3. The caries experience was significantly more in children having severe
malocclusions (Class-III>Class-II>Class-I).
4. Males had an increased prevalence of Class II and III malocclusions compared
to females and as the age increases the skeletal pattern becomes more evident.

Summary
P.M.N.M Dental College, Bagalkot 50
SUMMARY
The mixed dentition is the time of greatest opportunity for occlusal guidance,
especially in cases of malocclusion. As uninterrupted growth might further complicate
the condition in the permanent dentition, an appropriate diagnosis at an early stage
becomes necessary. Any relation between the dermatoglyphic, cheiloscopic patterns
and skeletal jaw relation might aid in the early diagnosis and interception of the
condition and also might be helpful in future forensic research. There exists a
deficiency in studies carried on samples of pediatric age group, hence it is necessary
to conduct a study to investigate the dermatoglyphic and cheiloscopic patterns, along
with assessment of prevalence of dental caries and type of skeletal malocclusion in
boys and girls of age group 6-14 years.
Ninety children of age group of 6 - 14 years reporting to the Department of
Pediatric and Preventive Dentistry, P.M.N.M. Dental College and Hospital, Bagalkot
for routine dental check-up and treatment were considered for the study. After
obtaining the consent from the parents, these children were grouped based on
examining lateral cephalograms obtained from them. ANB angle, WITS appraisal and
Beta angle were calculated for each cephalograms to assess the anteroposterior jaw
position. Keeping the norms into consideration, the children were grouped as:
Group A - consisting of 30 children with skeletal Class-I malocclusion.
Group B - consisting of 30 children with skeletal Class-II malocclusion.
Group C - consisting of 30 children with skeletal Class-III malocclusion.

Summary
P.M.N.M Dental College, Bagalkot 51
For the groups:
Lip-prints were taken using child safe lipstick-scotch tape method on the bond
paper, without any distortion.
Finger prints (right and left) of the subjects were recorded using black
duplicating ink, which were applied on the fingers with cotton swab. The
digits were guided and pressed firmly against the white bond paper clipped on
to a board.
The lip print patterns were classified according to Suzuki and Tsuchihashi’s
classification system10, 36 and finger print patterns were classified into arch,
whorl and loop patterns.
Presence of dental caries were assessed by deft/DMFT index.
Prevalence of the type of skeletal malocclusion in boys and girls were
evaluated.
The results obtained were grouped, tabulated, compared and subjected to
appropriate statistical evaluation.
Within the limitations of this study, the following conclusions were drawn:
1. Predominant lip print patterns which related to the skeletal malocclusions were
as follows: Type I (vertical) pattern for Class-I malocclusion, Type II
(branched) and Type III (intersected) pattern for Class-II malocclusion and
Type I (vertical) and Type III (intersected) pattern for Class-III malocclusion.

Summary
P.M.N.M Dental College, Bagalkot 52
2. Predominant finger print patterns which related to the skeletal malocclusions
were as follows: Loop pattern for Class-I malocclusion, Loop and Whorl
pattern for Class-II malocclusion and Whorl pattern for Class-III malocclusion.
3. The caries experience was significantly more in children having severe
malocclusions (Class-III>Class-II>Class-I).
4. Males had an increased prevalence of Class II and III malocclusions compared
to females and as the age increases the skeletal pattern becomes more evident.

Bibliography
P.M.N.M Dental College, Bagalkot 53
BIBLIOGRAPHY
1. Akbari M, Lankarani KB, Honarvar B, Tabrizi R, Mirhadi H, Moosazadeh M.
Prevalence of malocclusion among Iranian children: A systematic review and
meta-analysis. Dent Res J (Isfahan) 2016; 13(5): 387-95.
2. Shivakumar KM, Chandu GN, Subba Reddy VV, Shafiulla MD. Prevalence of
malocclusion and orthodontic treatment needs among middle and high school
children of Davangere city, India by using Dental Aesthetic Index. J Indian
Soc Pedod Prev Dent 2009; 27(4): 211-8.
3. Raghav P, Kumar N, Shingh S, Ahuja NK, Ghalaut P. Lip prints: The barcode
of skeletal malocclusion. J Forensic Dent Sci 2013; 5(2): 110-7.
4. Kaushal B, Mittal S, Aggarwal I. Association of Lip Print Patterns with
Saggital Malocclusions in District Solan Population. Int J Res Health Allied
Sci 2018; 4(1):75-81.
5. Prabhu RV, Dinkar AD, Prabhu VD, Rao PK. Cheiloscopy: Revisited. J
Forensic Dent Sci 2012; 4(1): 47–52.
6. Anitha C, Konde S, Raj NS, Kumar NC, Peethamber P. Dermatoglyphics: A
genetic marker of early childhood caries. J Indian Soc Pedod Prev Dent 2014;
32(3): 220-4.
7. Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet 2007; 369(9555): 51-9.

Bibliography
P.M.N.M Dental College, Bagalkot 54
8. Cirulli N, Cantore S, Ballini A, Perillo L, Giannico OV, Tafuri S, De Vito D.
Prevalence of caries and dental malocclusions in the apulian paediatric
population: an epidemiological study. Eur J Paediatr Dent 2019; 20(2): 100-4.
9. Mttaya M, Brudvik P, Astrom AN. Prevalence of malocclusion and its
relationship with socio-dermatographic factors, dental caries, and oral hygiene
in 12 – 14 year old Tanzanian school children. Eur J Orthod 2009; 31(5): 467-
76.
10. Shivani Y, Thukral R, Makhija PG, Bhardwaj A. Predominant lip prints in
skeletal class III malocclusion group. National Journal of Dental Sciences &
Research 2015; 3(1): 17-9.
11. Ruchi S, Kuldeep S, Dhruv Y, Abhilasha C, Vijay A. Association of lip print
patterns with malocclusion in Jaipur population. Indian Journal of
Contemporary Dentistry 2015; 3(2): 25-9.
12. Ponnusamy S, Vijayalakshmi K, Premkumar KS and Sumalatha S. Lip print’s
correlation coefficient with skeletal class I & II malocclusion. Int J of Inov and
App 2017; 5(5): 76-81.
13. Vignesh R, Rekha CV, Annamalai S, Norouzi P, Sharmin D. A comparative
evaluation between cheiloscopic patterns and terminal planes in primary
dentition. Contemp Clin Dent 2017; 8(4): 522-5.
14. Tikare S, Rajesh G, Prasad KW, Thippeswamy V, Javali SB.
Dermatoglyphics-A marker for malocclusion? Int Dent J 2010; 60(4): 300-4.

Bibliography
P.M.N.M Dental College, Bagalkot 55
15. Achalli S, Patla M, Nayak K, B, Bhat M. Assessment of dermatoglyphic
patterns in malocclusion. J Dent Indones 2018; 25(2): 104-7.
16. Eslami N, Jahanbin A, Ezzati A, Banihashemi E, Kianifar H. Can
dermatoglyphics be used as a marker for predicting future malocclusions?
Electron physician 2016; 8(2): 1927-32.
17. Baswaraj H, Lalakiya H, Mashru K, Modi H, Patel U, Ramani A.
Dermatoglyphics and malocclusion. J Int Oral Health 2016; 8(8): 865-9.
18. Divyashree, Suhas AS, Sharmada BK, Tayeepriyanka. Dermatoglyphic
patterns and their co-relation with skeletal malocclusions. IOSR Journal of
Dental and Medical Sciences 2016; 15(3): 101-4.
19. George SM, Philip B, Madathody D, Mathew M, Paul J, Dlima JP. An
assessment of correlation between dermatoglyphics patterns and sagittal
skeletal discrepancies. J Clin Diagn Res 2017; 11(3): ZC35-ZC40.
20. Charles A, Ramani P, Sherlin HJ, Dilip S, Srinivas S, Jayaraj G. Evaluation of
dermatoglyphic patterns using digital scanner technique in skeletal
malocclusion: A descriptive study. Indian J Dent Res 2018; 29(6): 711-5.
21. Shetty SS, Li GS, Babji NA, Yusof LS, Yang NN, Jun TD, et al.
Dermatoglyphics: A prediction tool for malocclusion. J Datta Meghe Inst Med
Sci Univ 2019; 14: 27-30.
22. Vellappally S, Gardens SJ, Kheraif AA, Krishna M, Babu S, Hashem M, et al.
The prevalence of malocclusion and its association with dental caries among
12-18-year-old disabled adolescents. BMC Oral Health 2014; 14: 123.

Bibliography
P.M.N.M Dental College, Bagalkot 56
23. Caplin JL, Evans CA, Begole EA. The relationship between caries and
malocclusion in Chinese migrant workers’ children in Shanghai. Chin J Dent
Res 2015; 18(2): 103-10.
24. Carminatti M, Lavra-Pinto B, Franzon R, Rodrigues JA, Araújo FB, Gomes E.
Impact of dental caries, malocclusion and oral habits on the oral health-related
quality of life of preschool children. Audiol Commun Res 2017; 22(1801): 1-
8.
25. Shetty R, Hegde V, Shetty PJ. Assessment of malocclusion status, dentition
status, and treatment needs among 15-year-old school children of Mangalore.
Indian J Dent Res 2018; 29(1):109-16.
26. Goel S, Singh A, Chaudhary G, Kalsi S, Sood A, Marria G. The relationship
of malocclusion with periodontal status, dental caries, and sociodemographic
factors in school children of Ludhiana. Indian J Dent Sci 2018; 10(2): 87-91.
27. Disha P, Poornima P, Pai SM, Nagaveni NB, Roshan NM, Manoharan M.
Malocclusion and dental caries experience among 8–9-year-old children in a
city of South Indian region: A cross-sectional survey. J Edu Health Promot
2017; 6: 98.
28. Abbas A, Syed IB, Abbas H, Malik F. Malocclusion and its relationship with
dental caries in a sample of Pakistani school children. Pakistan Oral & Dental
Journal 2015; 35(4): 615-9.
29. Siddegowda R, Satish RM. The prevalence of malocclusion and its gender
distribution among Indian school children: An epidemiological survey. SRM J
Res Dent Sci 2014; 5: 224-33.

Bibliography
P.M.N.M Dental College, Bagalkot 57
30. Ciuffolo F, Manzoli L, D’Attilio M, Tecco S, Muratore F, Festa F, et al.
Prevalence and distribution by gender of occlusal characteristics in a sample
of Italian secondary school students: A cross-sectional study. Eur J Orthod
2005; 27(6): 601-6.
31. Baccetti T, Reyes BC, McNamara JA. Gender differences in Class-III
malocclusion. Angle Orthod 2005; 75(4): 510–20.
32. Gelgor IE, Karaman AI, Ercan E. Prevalence of malocclusion among
adolescents in Central Anatolia. Eur J Dent 2007; 1(3): 125-31.
33. Komazaki Y, Fujiwara T, Ogawa T, Sato M, Suzuki K, Yamagata Z, et al.
Prevalence and gender comparison of malocclusion among Japanese
adolescents: A population-based study. Journal of the World Federation of
Orthodontists 2012; 1: e67-e72.
34. Tak M, Nagarajappa R, Sharda AJ, Asawa K, Tak A, Jalihal S, et al
Prevalence of malocclusion and orthodontic treatment needs among 12-15
years old school children of Udaipur, India. Eur J Dent 2013; 7: SO 45-53.
35. Tariq B, Habib K, Riaz S, Ilyas M. Gender Wise Association between Dental
Malocclusion Classes and ABO Blood Group System. Dentistry 2019; 9: 532.
36. Prabhu RV, Dinkar A, Prabhu V. Digital method for lip print analysis: A new
approach. J Forensic Dent Sci 2013; 5(2): 96–105.
37. Soben peter. Essentials of Public Health Dentistry. 5th edition; New Delhi
Arya Medi: 2013.

Bibliography
P.M.N.M Dental College, Bagalkot 58
38. Lucas T, Henneberg M. Are human faces unique? A metric approach to
finding single individuals without duplicates in large samples. Forensic Sci Int
2015; 257: 514.e1-6.
39. Kapoor N, Badiye A. A study of distribution, sex differences and stability of
lip print patterns in an Indian population. Saudi J Biol Sci 2017; 24(6): 1149-
54.
40. George R, Nora Afandi NS, Zainal Abidin SN, Binti Ishak NI, Soe HH, Ismail
AR. Inheritance pattern of lip prints among Malay population. J Forensic
Legal Med 2016; 39: 156-60.
41. Adamu LH, Taura MG, Hamman WO, Ojo SA, Dahiru AU, Sadeeq AA,
UmarKB. Study of lip print types among Nigerians Homo 2015; 66(6): 561-9.
42. Kanematsu N, Yoshida Y, Kishi N, Kawata K, Kaku M, Maeda K, et al. Study
on abnormalities in the appearance of finger and palm prints in children with
cleft lip, alveolus, and palate. J Maxillofac Surg 1986; 14(2): 74-82.
43. Cummins H, Midlo C. “The topographic history of the volar pads (walking
pads) in the human embryo.” Embryol Carnig Int Wash 1929; 20: 103-9.
44. Mulvi hill JJ, Smith DW. The genesis of dermatoglyphics. J Pediatr 1969; 75:
579-89.
45. Walker NF. Inkless methods of finger, palm and sole printing. J Pediatr 1957;
50(1): 27-30.
46. Saravanan S, Madivanan I, Subashini B, Felix JW. Prevalence pattern of
dental caries in the primary dentition among school children. Indian J Dent
Res 2005; 16(4): 140‑6.

Bibliography
P.M.N.M Dental College, Bagalkot 59
47. Mahesh Kumar P, Joseph T, Varma RB, Jayanthi M. Oral health status of 5
years and 12 years school going children in Chennai city – An epidemiological
study. J Indian Soc Pedod Prev Dent 2005; 23(1): 17‑22.
48. Hafez HS, Shaarawy SM, Al-Sakiti AA, Mostafa YA. Dental crowding as a
caries risk factor: A systematic review. Am J Orthod Dentofacial Orthop 2012;
142(4): 443–50.
49. Jackson A. Insufficient evidence to determine an association between dental
crowding and caries. J Am Dent Assoc 2014; 145(1):78–9.
50. Brito DI, Dias PF, Gleiser R. Prevalence of malocclusion in children aged
9‑12 years old in the city of Nova Friburgo, Rio de Janeiro state, Brazil. Rev
Dent Press Ortod Ortop Facial 2009; 14: 118‑24.
51. Marques LS, Ramos‑Jorge ML, Paiva SM, Pordeus IA. Malocclusion: Esthetic
impact and quality of life among Brazilian school children. Am J Orthod
Dentofacial Orthop 2006; 129(3): 424‑7.
52. Bernabé E, Flores‑Mir C, Sheiham A. Prevalence, intensity and extent of oral
impacts on daily performances associated with self‑perceived malocclusion in
11‑12‑year‑old children. BMC Oral Health 2007; 7: 6.
53. Sivapathasundharam B, Prakash PA, Sivakumar G. Lip prints (Cheiloscopy).
Indian J Dent Res 2001; 12(4):234-7.
54. Mamandras AH. Linear changes of the maxillary and mandibular lips. Am J
Orthod Dentofacial Orthop 1988; 94(5):405-10.

DEPARTMENT OF PEDIATRIC AND PREVENTIVE DENTISTRY,
P.M.N.M DENTAL COLLEGE AND HOSPITAL,
BAGALKOT-587103, KARNATAKA
INFORMED CONSENT FOR DISSERTATION
Name:
Age/sex:
Address:
Phone no. :
I, , the undersigned, as the legally responsible
parent/guardian/care-taker of have been explained the whole
procedure of the dental examination to be performed by Dr. Annat Varghese, (Post graduate
student ,Department of Pediatric and Preventive Dentistry, P.M.N.M Dental College &
Hospital, Bagalkot) on my child which includes dental examination, radiographic
examination, dactylographic and cheiloscopic examination.
I, hereby grant my consent for the above procedures being performed on my child.
Place:
Date:
Signature
(Parent / legal guardian)


Scanned by CamScanner

DEPARTMENT OF PEDIATRIC & PREVENTIVE DENTISTRY
B.V.V.S P.M.N.M DENTAL COLLEGE & HOSPITAL, BAGALKOT – 587103,
KARNATAKA
1. Suzuki and Tsuchihashi’s classification system
2. Dermatoglyphic patterns

3. deft / DMFT Scoring Index:
Name:
Age:
Sex:
Type of skeletal malocclusion:
55 54 53 52 51 61 62 63 64 65
17 16 15 14 13 12 11 21 22 23 24 25 26 27
47 46 45 44 43 42 41 31 32 33 34 35 36 37
85 84 83 82 81 71 72 73 74 75
DMFT Score = deft Score =

Scanned by CamScanner

Scanned by CamScanner

Scanned by CamScanner

Annexure
P.M.N.M Dental College, Bagalkot 60
ANNEXURE
FIGURE 3: ARMAMENTARIUM
FIGURE 4: OBTAINING INFORMED CONSENT

Annexure
P.M.N.M Dental College, Bagalkot 61
FIGURE 5: APPLYING CHILD SAFE LIPSTICK WITH BRUSH
FIGURE 6: LIP PRINT BEING COLLECTED THROUGH SCOTCH TAPE

Annexure
P.M.N.M Dental College, Bagalkot 62
FIGURE 7: LIP PRINT COLLECTED AND TRANSFERRED TO PAPER
FIGURE 8: APPLYING BLACK DUPLICATING INK WITH COTTON

Annexure
P.M.N.M Dental College, Bagalkot 63
FIGURE 9: FINGER PRINT BEING COLLECTED
FIGURE 10: FINGER PRINT COLLECTED ON PAPER