Embed Size (px)
DESCRIPTION
Join SUSP Affinity Groups! Learn from experts and other SUSP hospital teams who are working on what you’re working on . Click this link SUSP Affinity Group Registration Link to register for an affinity group by Tuesday, May 20 th ! . Thomas Varghese Jr. MD, MS, FACS. - PowerPoint PPT Presentation
Citation preview

DRAFT – final pending AHRQ approval
Join SUSP Affinity Groups!Learn from experts and other SUSP hospital teams who are working on what you’re working on
Early recovery protocol (ERP)
Preop care coordination
SCIP measures Environmental management
Pain management, fluid management, postop mobility
Glucose control, bowel prep, oral antibiotics
Antibiotic prophylaxis, normothermia, skin prep
OR traffic, sterile technique, surface contamination
Traci Hedrick, MDUniversity of Virginia
Melanie Morris, MDUniversity of Alabama
Skandan Shanmugan, MDUniversity of Pennsylvania
Mariana PeharJohns Hopkins Hospital
Coaching calls every other month Quarterly Coaching Calls
Click this link SUSP Affinity Group Registration Link to register for an affinity group by Tuesday, May 20th!

Thomas Varghese Jr. MD, MS, FACS

Objectives of Strong For Surgery
• Identify and evaluate evidence-based practices to optimize the health of patients prior to surgery
• Outline key factors in pre-surgical care that can improve post-operative outcomes
• Apply quality improvement tools to implement best practices toward optimizing patient health

Funding
• Agency for Healthcare Research and Quality• Life Sciences Discovery Fund• Nestle HealthCare Nutrition• UW Patient Safety Innovation Program• UW Department of Surgery

Our Shared Project Goals
To achieve significant reductions in surgical site infection and surgical complication rates
To achieve significant improvements in safety culture

Why is Your SUSP Work Important?
1 in 25 people will undergo surgery
7 million (25%) complications follow in-patient surgeries
1 million (0.5 – 5%) deaths follow surgery
50% of all hospital adverse events are linked to surgery AND are avoidable


Problems
Every year there are 210,000 Preventable Deaths• $30 billion per year
J Patient Safety Sept 2013; 9(3): 122-128

Problems
Every year there are 210,000 Preventable Deaths• ½ associated with an operation• $30 billion per year
1 in 4 colon resections readmitted within 90 days• $300 million per year
Soft Tissue Surgical Site Infections• $3 billion in direct costs
J Patient Safety Sept 2013; 9(3): 122-128Wick EC, et al. 2011; 54(12):1475-1479Eappen S JAMA. 2013;309(15):1599-1606

It takes an average of 17 years before new knowledge from randomized clinical trials is incorporated into widespread clinical practice!
JAMA 1999; 282: 1458-1465; Health Professions Education 2003J Am Med Inform 2001; 8(4):398-399N Engl J Med 2003; 348:2635-2645

Healthcare System in Washington State
QI Performance Surveillance
Translation of Research into Practice
Research and Development

• Clinician-led QI using clinical data
• Focus on quality and cost-effectiveness data
• Impacts behavior through:• Benchmarking• Education• Standard orders• Checklists

BeforeElective Colorectal Resection, CHARS 2000-2003
17.7±38.2%

After Elective Colorectal Resection CHARS 2006-2009
9.6±29.4%

Evidence Generation
Clinical PracticePartners
Dissemination & Implementation
Clinician Offices
Long-term CareFacilities
Hospitals

Evidence Generation
Clinical PracticePartners
Dissemination & Implementation
Healthcar
eData
Patient Voices
StakeholderInput
Clinician Offices
Long-term CareFacilities
Hospitals

Evidence Generation
Clinical PracticePartners
Dissemination & Implementation
Healthcar
eData
Patient Voices
StakeholderInput
Clinician Offices
Long-term CareFacilities
Hospitals

Focus on Decision Making
PATIENT
DOCTOR’S OFFICE
OPERATING ROOM

PATIENT
DOCTOR’S OFFICE
OPERATING ROOM

PATIENT
DOCTOR’S OFFICE
OPERATING ROOM
Focus on Decision Making in Clinic


What is Strong for Surgery?
Public health campaign focused on surgeons, patients and other important stakeholders
• Interactive tools to help optimize patients prior to surgery
• Messaging• Surveillance, data feedback, public reporting

Current Checklists
Nutrition• Screening for malnutrition• Albumin test for risk stratification• Immunonutrition supplementation
Smoking• Smoking habits and history• Establish and document quit plan
Blood Sugar• Diabetes risk screening• Blood sugar control screening• Perioperative glucose management
Medications• Identify drugs that could cause
bleeding and cardiac risks• Herbal medication reconciliation
See full version of the checklists at www.strongforsurgery.org

Why Blood Sugar?• Hypergycemia doubles the risk of SSI
• In some studies 47% of hyperglycemic episodes were in nondiabetics!
Latham. Inf Contr Hosp Epidemiol. 2001;22:607Dellinger. Inf Contr Hosp Epidemiol. 2001;22:604

Why Blood Sugar?• Hypergycemia doubles the risk of SSI
• In some studies 47% of hyperglycemic episodes were in nondiabetics!
• 470 million people worldwide will have prediabetes by 2030
• 35% of US adults older than 20 yrs of age and 50% greater than 65 years had prediabetes in 2005-2008
Latham. Inf Contr Hosp Epidemiol. 2001;22:607Dellinger. Inf Contr Hosp Epidemiol. 2001;22:604Lancet 2012; 2279-22902011 US Department of Health and Human Services

• > 65 years• 1 in 4 will have diabetes• 2 in 4 are prediabetic
2011 US Department of Health and Human Services
Why Blood Sugar?

Why Medications?
• Some medications and herbal remedies increase risk of bleeding• Echinacea, Garlic, Ginkgo, Ginseng, Kava, Saw
Palmetto, St. John’s Wort, Valerian ↑ risk
• Aspirin can be safely continued
Chest 2012; 141:e326S-e350S; JAMA 2008; 300(24):2867-2878; Ann Surg 2012; 255(5):811-819

Why Medications?
• Some medications and herbal remedies increase risk of bleeding• Echinacea, Garlic, Ginkgo, Ginseng, Kava, Saw
Palmetto, St. John’s Wort, Valerian ↑ risk• Aspirin can be safely continued
• Beta-blocker continuation associated with fewer cardiac events and mortality
Chest 2012; 141:e326S-e350S; JAMA 2008; 300(24):2867-2878; Ann Surg 2012; 255(5):811-819; Arch of Surg 2012; 147(5):467-473

Why Nutrition?
• Malnutrition is prevalent in surgical patients• Best determinant of surgical outcome

Why Nutrition?
• Malnutrition is prevalent in surgical patients• Best determinant of surgical outcome
• Modifiable with appropriate intervention• Immunonutrition may improve recovery

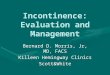
SCOAP: Albumin & ComplicationsElective colon/rectal procedures 2011
<2.0 2.0-2.4 2.5-2.9 3.0-3.4 3.5-3.9 4.0+0.0%
3.0%
6.0%
9.0%
12.0%
15.0%
Re-operation Death
Albumin Levels (g/dL)
Adve
rse
Out
com
e Ra
tes

Arginine Depletion
T-Cell Dysfunction
Risk of INFECTION
Surgery and trauma patients are immune suppressed making them more susceptible to infection due to arginine depletion.
Popovich 2006; McClave 2009; Zhu 2010

Arginine Depletion
T-Cell Dysfunction
Risk of INFECTION
Surgery and trauma patients are immune suppressed making them more susceptible to infection due to arginine depletion.
Immune- modulating formulas Arginine + Ω-3 fatty acids + Nucleotides 5 to 7 day regimen, 3 times daily
Popovich 2006; McClave 2009; Zhu 2010

Literature Review• Systematic Review
N=3,43835 studies focused on elective surgeryProcedure types
25 GI: 18 upper; 2 lower; 5 mixed 10 non-GI
• 23 – used arginine-based supplementsPre-Op Use: ↓ Infectious complications 43%
Drover JW, et al.JACS 2011; 212 (3):385-399

All Patients Neurosurgery Orthopedic0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
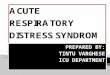
Never SmokerPrior SmokerCurrent Smoker
Why Smoking?
Mary T Hawn et al., “The Attributable Risk of Smoking on Surgical Complications,” Annals of Surgery 254, no. 6 (December 2011): 914–920.
Adju
sted
Odd
s Rati
oCo
mpl
icati
ons A
ssoc
iate
d w
ith S
mok
ing

Post-Operative Outcomes by Pack-Years Smoked
Surgical Site Infection Pulmonary 30-day Mortality0.8
1
1.2
1.4
1.6
1.8
2
0 1-20 21-40 41-60 >60
Adju
sted
Odd
s Rati
o
Mary T Hawn et al., “The Attributable Risk of Smoking on Surgical Complications,” Annals of Surgery 254, no. 6 (December 2011): 914–920.

Checklists






Raising Awareness
Changing Practice

Raising Awareness

Public Health Campaign
• Understanding clinic and patient needs• Checklists• Tracking outcomes• Strategic partnerships
• Community Engagement• Outreach events• Website content
www.strongforsurgery.org


Publications
OR MANAGER

By Laura Landro



Collaborators
• Washington State Medical Association• Washington State Hospital Association• Washington State Nurses Association• Washington State Academy of Nutrition and Dietetics• Washington Patient Safety Coalition• Washington State Society of Anesthesiologists• Washington St. Chapter – American College of Surgeons• Qualis Health• American Lung Association

Social Media Presence
2014 to date• 2,375 Total Hits• 1,803 Unique
Hits
• 126 “Likes”• Frequency 2-3
posts/week
• Discussion post 1-2/month
www.strongforsurgery.org
Implementation Guide requests 2013: 113 sites, 34 states, 7 countries
• 14.1 K Tweets• 2,678 Followers• 2,495 Following• Frequency
~70/week
@Strong4Surgery@TomVargheseJr

Changing Practice

The SUSP Team
Understands that patient safety culture is LOCAL
Composed of engaged frontline providers who take ownership of patient safety
Includes staff members who have different levels of experience
Tailored to include members based on clinical intervention

SUSP Teams’ Group Processes
Effective Group
Processes
Norms
Role Clarity
Effective Team Communication
Conflict Resolution
Education and
Engagement
Leadership Buy-in and
Support

Site Expectations
• Change team formation and support champion• Commitment through post-implementation• Checklist adoption• Data abstraction and sharing• Stakeholder calls attendance• Feedback for improvement

Site Activities
• Pre-Assessment• Workflow Mapping• Assessment of Resource Needs• Feedback – clinicians and staff• Post-Assessment

For More Information
• Visit the website: http://www.strongforsurgery.org• Review the literature• View our checklists• Request the implementation guide
• E-mail us: [email protected]
@TomVargheseJr@Strong4SurgeryStrongforSurgery

DRAFT – final pending AHRQ approval
Join SUSP Affinity Groups!Learn from experts and other SUSP hospital teams who are working on what you’re working on
Early recovery protocol (ERP)
Preop care coordination
SCIP measures Environmental management
Pain management, fluid management, postop mobility
Glucose control, bowel prep, oral antibiotics
Antibiotic prophylaxis, normothermia, skin prep
OR traffic, sterile technique, surface contamination
Traci Hedrick, MDUniversity of Virginia
Melanie Morris, MDUniversity of Alabama
Skandan Shanmugan, MDUniversity of Pennsylvania
Mariana PeharJohns Hopkins Hospital
Coaching calls every other month Quarterly Coaching Calls
Click this link SUSP Affinity Group Registration Link to register for an affinity group by Tuesday, May 20th!